Embed Size (px)
Citation preview
Issu
e 20
10
Aerosol-Journal TodayAerosol-Journal TodayAerosol-Journal TodayAerosol-Journal TodayAerosol-Journal TodayAerosol-Journal Today
Editorial 2
Inhalation in practice• The scientifi c argument for use of 3
nebulisers by children
• Case report: Current case from 5
paediatric care
• Treatment with eFlow® rapid 6
for lung transplant patients
• Expanding the range of treatments 7
for cystic fi brosis?
• Don‘t vaporise, nebulise! 9
• COPD: Nebulisers support 10
selfmanagement
Scientifi c News• New series: Inhalational medications 11
in research and development.
Part 1: Asthma
• Congress-News 13
• Poorly controlled asthma – Empirical 16
treatment rarely helps against refl ux
News in Brief• Update to DGP coughing guideline 17
• New guideline for mixing compatibility 17
of nebuliser solutions
• On the technique, practice and traps 18
in inhalation therapy
News from PARI• 3% saline solution for acute bronchiolitis 19
• Inhaling hypertonic saline for bronchectases? 20
• eFlow® rapid now with pause function 20
• The PARI Service Center 21
• The new instructions for PARI products 21
• User video for the eFlow® rapid 22
• PARI runs for CF patients 22
Conference Dates 23

Since saline solutions in various con-centrations have shown their effective-ness in a range of applications, from moistening to intensive mobilisation of secreta, they have become an es-tablished element of respiratory tract therapy. On the other hand, most of the general public still does not under-stand that saline solutions need to be nebulised or administered in aerosol form, they cannot simply be vaporised in a saucepan – there is a crying need for education here!
In this issue, we also present an es-sential part of the PARI organisation, which is becoming even more impor-tant as the company‘s liaison function with the public – the PARI Service Cen-ter. It manages in the region of 100,000 contacts with physicians, pharmacies, authorised dealers and patients every year and is ready to answer questions of whatever nature: expert, fast, and personal.
As always, we hope that you will find this issue of Aerosol Journal today in-formative and interesting.
With warmest regards
Dr. Johann ZimmermannManaging Director, PARI GmbH
Editorial
Dear Reader
Nebulisers remain a central element in treatment of the respiratory tract, and not only in Germany: Dr. Ahmad Kantar, Medical Scientific Director of the High Altitude Paediatric Asthma Centre in Misurina, Italy reports on the many and various advantages of nebu-liser treatment, particularly in asthma emergency cases. Our interview with him appears on page 3. In a guest con-tribution, Prof. C.P. Bauer describes one such case of early childhood asth-ma with atopy.
Nebuliser treatment is also becoming more and more important for the up-per respiratory tract. The efficacy of treatment for sinusitis using a pulsed aerosol via PARI SINUS is currently the subject of a number of studies invol-ving CF patients. Dr. Jochen Mainz from Jena presented the latest study data with Pulmozyme at ECFC 2010.
Two major advantages of administe-ring medications via nebulisers are the ease with which usable solutions can be produced and the simplicity of their administration. Accordingly, the topi-cal application is often used in nebu-lisers when medications are being tes-ted for the first time. One of the main reasons for this is to minimise adverse side effects. This is shown in examples from the drug pipeline for treating asthma and studies with antibiotics for bronchiectasis patients. In the lat-ter case, hypertonic saline solution can also help with mucus clearance.
2

Inhalation in practice
PARI:Dr. Kantar, you are the Medical Scientific Director of the Paediatric Asthma Centre in Misurina, Italy. In your opinion, why are nebulisers still such an important part of inhalation therapy when there are so many other devices on the market?
Kantar: Yes, that is correct: nebulisers are still used in inhalation therapy very often. And it is especially true for the new generation of devices, the mesh and membrane nebulisers, despite the wi-despread availability of metered dose inhalers and dry powder inhalers.
I think that one of the main reasons is their „universal“ applicability: almost all classes of medication can be administered via nebulisers, whether the patients are still mobile or if they have to be ventilated mechanically [1].
Nebulisers are typically manufactured as „open“ systems. This means that the doc-tor can use a large number of active ingre-dients of various medications according to his best judgment and on his own initia-tive. This is not true for MDIs and DPIs, in which the device is tied directly to the ac-tive substance – as a rule, this then places the responsibility for the combination of
medication and inhalation device firmly in the hands of the medication manufactu-rer.
The regulatory authorities have now had a chance to respond to this difference in handling: in 2009 the European Medical Agency EMEA published a guideline pa-per on „clinical documentation for orally inhaled products“ [2]. It covered MDIs, DPIs, spacers and nebulisers. According to this guideline, the insert in the medication packaging should identify the nebuliser that was used for the clinical studies. It should also include appropriate warnings if data on use with other systems is not available and the results achieved may differ. This makes people more aware that not all nebulisers are created equal.
PARI:Why do you think nebulisers are especial-ly beneficial for children?
Kantar: Nebulisers have a distinct advantage over other devices because of the particular, unique way in which the active agent is delivered – although this is not often ta-ken into account when prescribing inhala-tion treatment for children.
• An aerosol cloud forms and is then per-fused very slowly. This low speed red-uces impaction of the particles as they travel through the respiratory tract. This means that more of the active agent penetrates deep into the lungs. We also have a higher rate of deposition in the peripheral areas of the lungs and less in the pharyngeal cavity.
• The active agent is released over a longer period of time. Children often breathe irregularly, and this helps to avert the risk of too little medication reaching the lungs because the inha-lation manoeuvres are too short.
• The active agent is delivered in the form of an aqueous solution. The
advantage of this is that, due to exi-sting surface tensions, water drop-lets in the lungs tend to spread out towards the distal regions. As a con-sequence, the active agent is „car-ried“ to these regions as well, by the water.
• This leads directly to our next point: this mechanism prevents the respira-tory tract from becoming dried out, or at least reduces the effect.
• Inhalation requires only minimal co-ordination on the part of the pati-ent.
In my opinion, these 5 points constitute an excellent argument for using nebulisers to treat children.
PARI:You insist on the use of nebulisers to tre-at acute asthma attacks at your centre – what led you to this decision?
Kantar: There are many factors involved in setting up the optimum inhalation treatment programme: the physical aerosol charac-teristics, the patient‘s breathing pattern, the active agent, the nature and severity of the disease, the „target region“ within the lung, and the age of the patient to mention just a few.As an example, let us consider targeting with salbutamol as a representative of the class of beta-2-agonists. This has a critical role in the event of an acute asthma at-tack. It is beyond dispute that good tar-geting can maximise therapeutic respon-se. For beta-2-agonists, deposition in the central regions of the lungs is key. Not in the alveolar regions and also not total de-position.
In fact Usmani et al. demonstrated that larger salbutamol droplets result in gre-ater bronchodilation [3] – providing ad-ministration is conducted correctly. Then the deposition site matches the available
agent receptors on the smooth muscula-ture.When I say larger droplets, they mean droplets with a diameter between 3 and 6 µm – that is to say droplets from the upper respirable range, and small droplets have a diameter of about 1.5 µm.
The authors succeeded in modulating cli-nical effects simply by modifying the size of the droplets. For me, this is evidence that it makes sense to use „smart“ inha-lation devices, which produce droplets of exactly the right size. Our first choice when working with acute asthma suffe-rers are the new generation nebulisers, like the eFlow rapid. The PARI TurboBoy is also called on.
PARI:Can you explain what algorithm you use to decide on the correct device for your asthma patients?
Kantar: Yes, this question is often asked in clini-cal practice. There are pros and cons with regard to every device. What is available for selection? There are various nebuli-sers, MDIs, with and without spacers, and a wide variety of DPIs. Current reviews of inhalation devices for beta-2-agonists to treat asthma have shown that nebuli-sers and MDIs plus spacers are essentially equally effective [4,5]. The primary finding of the largest meta-analysis conducted by Dolovich et al. was that all inhalation de-vices can provide effective treatment in the most dramatically different life situ-ations, as long as the patient inhales cor-rectly [4]. It should not be inferred from this that the choice of inhalation device for a specific patient is of no importance. I mean rather: this study reveals that all de-vices can function well if the patient has mastered the inhalation equipment. And this is an extremely important point: after all, most clinical studies only include pati-ents who are able to perform the inhala-tion manoeuvre without difficulty or who are instructed until they can. This scenario is not consistent with real life.Dolovich‘s work only considered the effici-ency of the devices in the context of clini-cal studies. It is not very helpful in resol-ving questions like: who can operate one
or other of these devices properly? Which one will he really use regularly? Perhaps simply because he trusts it more? Which device is available, or will be provided?For example, infants would find it very dif-ficult to use an MDI without a spacer or a DPI correctly.Another key issue emerging from the review of Dolovich‘s work is that diffe-rences within the device groups were not discussed categorically. So no clear state-ments are made about the various types of DPIs or nebulisers. The meta-analysis placed them all on the same level, even though several studies have shown that there are significant differences between the devices within a category. In this con-text, one might mention the comparisons between nebulisers conducted by Barry & O‘Callaghan with salbutamol and budeso-nide as test substances [6,7]. Subsequent studies – such as the one conducted by Rau et al. in 2006 – repeatedly confirmed the differences between devices [8]. Inci-dentally, it was Rau again who showed that the dosage variations for MDI/spa-cer are of similar magnitude [9]. So this applies not only for nebulisers, but for all systems: devices within the same category are also not equivalent, and what is true for one is by no means necessarily true for another.
PARI:
What must one bear in mind most parti-cularly when using nebulisers with asth-ma patients?
Inefficient inhalation devices in asthma therapy have simply been put up with si-lently for far too long. Even though the-re is now a larger selection available, too many nebulisers are now being brought onto the market without the support of sufficient evidence-based data. Paediatri-cians then do not have enough informa-tion on which to make a professionally informed choice. Accordingly, they are of-ten guided more by financial expediency or even just habit.
Nebulisers are used to deliver active agents both topically and systemically. But the delivery of medications via the „pul-monary route“ is a complex process. Many
The scientific argument for use of nebulisers
in children – by Dr. Kantar, Italy
parameters are involved: the principle of aerosol generation, the device itself, the formulation of the agent, the patient‘s breathing pattern, and much more.
In the last 10 years, nebulisers have be-come more efficient systems. But this does no good unless doctors also insist that their patients receive treatment with the latest technology. From a purely techno-logical point of view, there is no reason why nebuliser therapy should not be used to deliver active agents to the lung with outstanding efficiency. But of course there are financial arguments against this form of treatment – from my perspective peop-le are obliged to use poorly designed, che-ap nebulisers, as is unfortunately the case in many centres in Italy.
Sources:
1 Hess DR, 2000, Respir. Care 2000:45;609-
622
2 www.emea.europa.eu/pdfs/human/
ewp/415100enfin.pdf
3 Usmani OS, Biddiscombe MF, Bar-
nes PJ, Am. J. Respir. Crit. Care Med.
2005:172;1497-1504
4 Dolovich MB, American College of
Chest Physicians/American College of
Asthma, Allergy and Immunology. Chest
2005:127;335-371
5 Cates CC, Bara A, Crilly JA, Rowe BH,
Cochrane Database Syst. Rev. 2009
6 Barry PW, O‘Callaghan C. Eur. Eur. Respir. J.
1999; 13: 1164-1169
7 Barry PW, O‘Callaghan C. J. Allergy Clin.
Immunol. 1998; 104: 1168-1173
8 Rau JL, Ari A, Restrepo RD, Respir. Care
2004: 49;174-179
9 Rau JL, et al. Respir. Care 2006 May:
51;503-10
Dr. Ahmad Kantar
3 4

Inhalation in practice
A five-year-old boy has suffered from recurring obstructive breathing dif-ficulties since infancy. He also has mild atopic eczema. The symptoms occur mainly during infections and when he comes into contact with cats. Symptoms are most pronounced in au-tumn and winter, the best season for the boy is summer; during this time he is largely symptom-free. The family has no pets, but the father apparently smokes (not in the house). According to mother‘s information, the boy also does not respond well to strenuous exercise, and upon running vigorously is subject to bouts of coughing.
According to the report by the fami-ly doctor, in the last few months the results of auscultation of the young patient have alternated between un-remarkable respiratory sounds, mild wheezing, and exacerbated breathing noise.
During the current clinical examinati-on, mild basal wheezing was detected bilaterally depending on how deeply the boy was breathing. No rhoncus was detected and the results of auscul-tation were otherwise normal. With regard to lung function, mild to moderate obstructive ventilator im-
Inhalation in practice
Case report: Current case from paediatric care
By Prof. Dr. Bauer, Gaißach
pairment was observed (FEV1: 77%, MEF 50: 48%). After bronchospasmo-lysis, the FEV1 increased by 33% and the MEF 50 by 59% . Accordingly, the young man responded significantly to administration of a beta mimetic (Fig. 1).
According to allergy testing (RAST), the patient showed positive reactions to cat dander (rating 5), grass pollen, birch pollen, horse epithelia, and dog dander (rating 2). The overall IgE level was 263 kU/l.Immunoglobulin and IgG subclass de-termination revealed no abnormali-ties. A chest X-ray showed a mild to moderate increase in peripronchial streaking in both lower lung fields, otherwise normal.
Sweat test and ciliary function exami-nation were normal.
The results of these tests indicate possi-ble early childhood Asthma bronchiale with atopy. For the treatment, it was emphasised again that the patient must not be exposed to the effects of passive smoking under any circumstan-ces, and it was recommended to avoid all contact with animals to minimise the occurrence of allergic reaction. The anti-inflammatory treatment was also stepped up, to include moist inhala-tions 3 times daily consisting of 0.5 mg
pulmicort in combination with 8 drops salbutamol after an intensive course of instruction (inhalation using LC Sprint Junior nebuliser together with mouth-piece). Peak flow measurement was also begun.
With this course of treatment, the young patient showed significant im-provement and stabilisation of the clinical picture after 1 week. As a re-sult, after this time the beta mimetic could be discontinued and budesonide inhalation could be reduced to two sessions per day. As the clinical picture remained stable for a further 14 days, the patient was switched from „PARI inhalations“ to a 200 µg budesonide metered dose inhaler using a vortex twice a day, with the recommendation that at the onset of an infection the patient return to 3 daily sessions with PARI moist inhalations of 0.5 mg bu-desonide in combination with 8 drops salbutamol.
Univ.-Prof. Dr. C. P. Bauer
Source: PARI GmbH
Treatment with eFlow®rapid for lung transplant patients
– an LTX recipient reports
Ms. Beate Basista, a former support base manageress for the German self-help group Sauerstoff-Langzeit-Therapie (LOT) e.V. (Long-term Oxygen Therapy) received a new lung in No-vember 2007. PARI Pharma asked Ms. Batista how she feels now after recei-ving a lung transplant and about using eFlow®rapid as part of her treatment.
PARI:Ms. Batista, please tell us how you feel today, after your lung transplant ope-ration (LTX).
Frau Basista:Having been diagnosed with idiopathic pulmonary fibrosis, I underwent a trans-plant of my left lung in November 2007. I came through the operation very well, and also recovered very quickly.
You cannot imagine what it means to me to be able to breathe „freely“ again. But the greatest dangers still lurk „eve-rywhere“. They are called „risk of infec-tion“ and „overexertion“ (due to the medications that I must take for the rest of my life to prevent my immune system from rejecting the foreign lung).Today, after two-and-a-half years, I still look upon the transplant as a gift, alt-hough I have now been receiving long-term oxygen therapy for a year again since I suffered a serious infection. But I am feeling well – of course I am working very hard to make sure that I continue to feel well.
PARI:How often must a lung transplant recipient visit the doctor, and what tests must he or she undergo?
Frau Basista:That depends on the patient‘s gene-ral health at the time of the visit. I go to my family doctor, a pulmonary specialist and the transplant centre. In the early days after my transplant, the centre kept a very close eye on me. Now I have a regular appoint-ment every 3 months. I visit my other two doctors „on an as needed basis“.
The monitoring appointments at the transplant centre are usually a „triathlon“: first they take a blood sample in a number of little vials, so that they can check my blood valu-es and the level of immunosuppres-sant drugs in my blood. Then I have an ECG, and finally they test my lung function. The lung function measu-rements are tiring, but necessary to enable the doctors to get a better idea. One‘s own impression of whe-ther the lung is working better or
Source: PARI GmbH
worse is highly subjective. They also carry out a blood gas analysis (BGA) (regardless of whether oxygen is indi-cated). Then I discuss the results with my doctor and we talk about how the therapy might be modified if neces-sary.
PARI:What role does physiotherapy play in tour treatment?
Frau Basista:I can‘t imagine treatment without a physiotherapy element. My brea-thing is still strained, so my muscles, including my respiratory muscles, quickly „seize up“. These muscles must be loosened in special brea-thing exercise sessions at least twice a week. I wouldn‘t like to imagine what the state of my health would be without these sessions. I compare it to the cyclists in the Tour de France: where would they be without physio-therapy. Except that the cycle race is over after 3 weeks. My breathing is laboured like that 24 hours a day, 365 days a year.
eFlow® rapid and physiotherapy:
important treatment elements for an LTX patient
5 6

Inhalation in practice
PARI:What are the difficulties and challen-ges you face during your therapy?
Frau Basista:Making time for everything. Eve-rything is important, even my walk to the fitness studio, as well as meeting with friends and activities and trips if that is possible. That is a challenge every day, and means that I have to plan everything perfectly.
PARI:How important is the eFlow®rapid as part of your treatment?
Frau Basista:When my physiotherapist introduced me to the eFlow®rapid in early 2009, I was rather sceptical at first. But her arguments persuaded me, and I tried it. From the first inhalation session, I had a very pleasant feeling, I could feel the mucus quite simply breaking up and that I was getting more air as a result. For me, the difference is that with other inhalation devices I am in-haling „dry“. For example, I can feel the saline solution penetrating deep into my bronchi, and the mucus being cleared so that I can cough it up wit-hout straining – that is a very good feeling. Inhalation sessions with the eFlow®rapid are short, quiet, and I
can disinfect all of the nebuliser parts quickly and easily.
For me, inhaling is one of the most important tasks of the day – I call it „my internal shower“. And I also re-lax when I am inhaling because I am concentrating on my breathing and I can breathe „freely“ when my lungs are clear.
PARI:How often do you inhale with the eFlow®rapid, and what medications do you inhale?
Frau Basista:I use the eFlow®rapid to inhale once or twice a day. I inhale sultanol and atrovent as well as 6% MucoClear.
PARI: Is there anything else that needs spe-cial attention in the treatment pro-gramme for lung transplant patients?
Frau Basista:Hygiene – that is why my dream is to own a small disinfecting device (sui-table for the eFlow®rapid), that I can take with me when I travel.
PARI:Do you have any personal advice for lung transplant recipients that would
make their treatment significantly easier and more effective?
Frau Basista:Not really – anyone who has under-gone a lung transplant is already very familiar with the issues. Everyo-ne experiences and feels the „gift of time“ in his or her own way. Different things are of concern to them, and that must be respected. In my expe-rience, I find self-discipline, thinking positively and a healthy dose of curi-osity are my guiding lights.
Source: Fotolia.com
Diseases of the upper respiratory tract are particularly common du-ring the „cold season“. Rhinitis and sinusitis together are among the most common illnesses suffered by humans generally. According to one prospective cross-sectional study, in a 12-week period in the winter of 2000/2001, an estimated 14.5 mil-lion Germans were treated by the doctors for sinusitis [1]. 80% of these were suffering from acute sinusitis, the other 20% were suffering chro-nic symptoms. That is equivalent to about 21.5% of the population of the Federal Republic aged over 16.
Cystic fibrosis (mucoviscidosis) is a di-sease that mainly affects the lungs. But since the cause of cystic fibrosis – a chloride canal impairment – invol-ves the entire organism, it concerns the digestive system, the pancreas and the upper respiratory tract as well as the lungs. Viscous mucus cau-ses chronic coughing and frequent respiratory tract infections, disrup-ted secretion of the digestive enzy-mes causes gastrointestinal problems and underweight.
The lungs and the intestinal tract are particularly important for diagnosis and treatment, because these are the sites where quality of life is most sig-nificantly impaired. The upper respi-ratory tract was neglected for many
years, even though inflammation of the tract is a standard symptom of CF patients. A cross-sectional study of chronic rhinosinusitis among CF suf-ferers revealed that more than 40% of the patients studied had already undergone operations of the upper respiratory tract at least once; in over 45% of patients who present with a Pseudomonas aeruginosa infection of the lungs, the bacteria is also pre-sent in the upper respiratory tract. In one patient, P. aeruginosa was de-tected in the upper respiratory tract even though the lungs were not in-fected [2]. This suggests strongly that the upper respiratory tract may be an entry portal for pathogenic bacteria such as P. aeruginosa, which is to say primary infection may begin in the nose.
It follows, therefore, that the upper respiratory tract should be monito-red constantly in cystic fibrosis pati-ents. It may be possible to prevent a lung infection by suitable measures even if the bacteria have already co-lonised the tract. Ideally, the appro-priate medications and active agents can be delivered directly to where they are needed – the paranasal si-nuses. Since this topical therapy for the paranasal sinuses does not work with conventional aerosols, the PARI SINUS system is used to transport the particles to these unventilated cavi-
ties by means of a vibrating aerosol. In a recently published study [3], for example, it was shown that Pulmozy-me can be applied successfully and effectively in this way.
The work to refine treatment options for cystic fibrosis is so important be-cause even the smallest step can help to alleviate the symptoms and im-prove the patients‘ quality of life. If inhaled substances that are conven-tionally used to treat the lungs can also be applied successfully to the upper respiratory tract, this may re-present a significant advance in the treatment of the disease. The PARI SI-NUS is helping to close an important gap in the treatment of cystic fibro-sis – other ongoing studies are also considering other medications that are significant for cystic fibrosis, and their efficacy when they are applied with the PARI SINUS.
Expanding the range of treatments for cystic fibrosis?
Sources:
1 Elies et al. Häufigkeit und Therapie der
Sinusitis. Chemotherapie 16.2007, 5,
167-175
2 Mainz et al. Poster for CF Congress,
Würzburg 2008
3 Mainz et al. Poster for ECFC, Valencia
2010
Figure 1a: Ventilation without vibration.
Möller et al. 2007
Figure 1b: Ventilation with vibration.
Figure 2: PARI SINUS
Inhalation in practice
7 8
Inhalation in practice Inhalation in practice
Don‘t vaporise, nebulise!
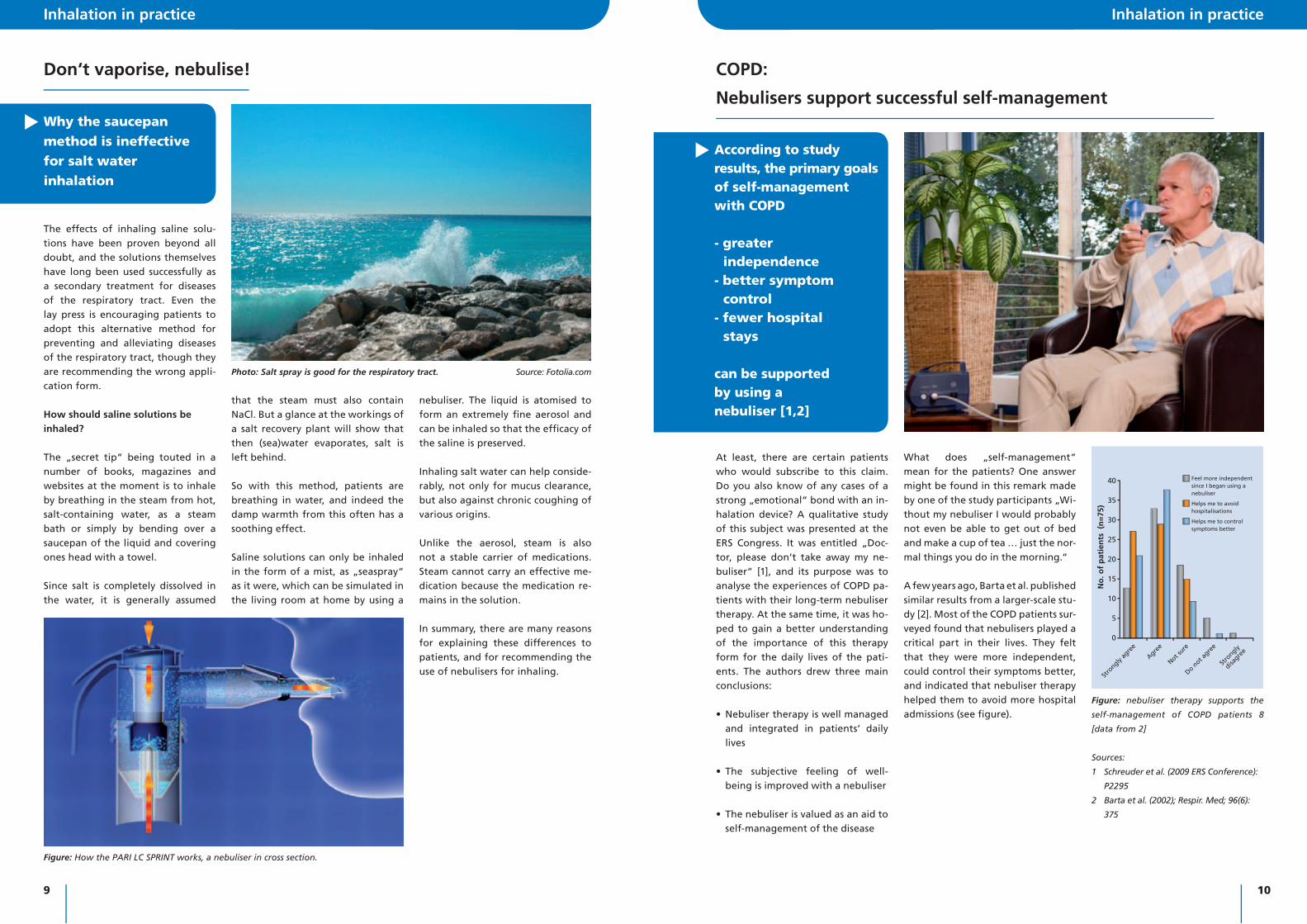
The effects of inhaling saline solu-tions have been proven beyond all doubt, and the solutions themselves have long been used successfully as a secondary treatment for diseases of the respiratory tract. Even the lay press is encouraging patients to adopt this alternative method for preventing and alleviating diseases of the respiratory tract, though they are recommending the wrong appli-cation form.
How should saline solutions be inhaled?
The „secret tip“ being touted in a number of books, magazines and websites at the moment is to inhale by breathing in the steam from hot, salt-containing water, as a steam bath or simply by bending over a saucepan of the liquid and covering ones head with a towel.
Since salt is completely dissolved in the water, it is generally assumed
Why the saucepan method is ineffective for salt water inhalation
that the steam must also contain NaCl. But a glance at the workings of a salt recovery plant will show that then (sea)water evaporates, salt is left behind.
So with this method, patients are breathing in water, and indeed the damp warmth from this often has a soothing effect.
Saline solutions can only be inhaled in the form of a mist, as „seaspray“ as it were, which can be simulated in the living room at home by using a
Figure: How the PARI LC SPRINT works, a nebuliser in cross section.
nebuliser. The liquid is atomised to form an extremely fi ne aerosol and can be inhaled so that the effi cacy of the saline is preserved.
Inhaling salt water can help conside-rably, not only for mucus clearance, but also against chronic coughing of various origins.
Unlike the aerosol, steam is also not a stable carrier of medications. Steam cannot carry an effective me-dication because the medication re-mains in the solution.
In summary, there are many reasons for explaining these differences to patients, and for recommending the use of nebulisers for inhaling.
Photo: Salt spray is good for the respiratory tract. Source: Fotolia.com
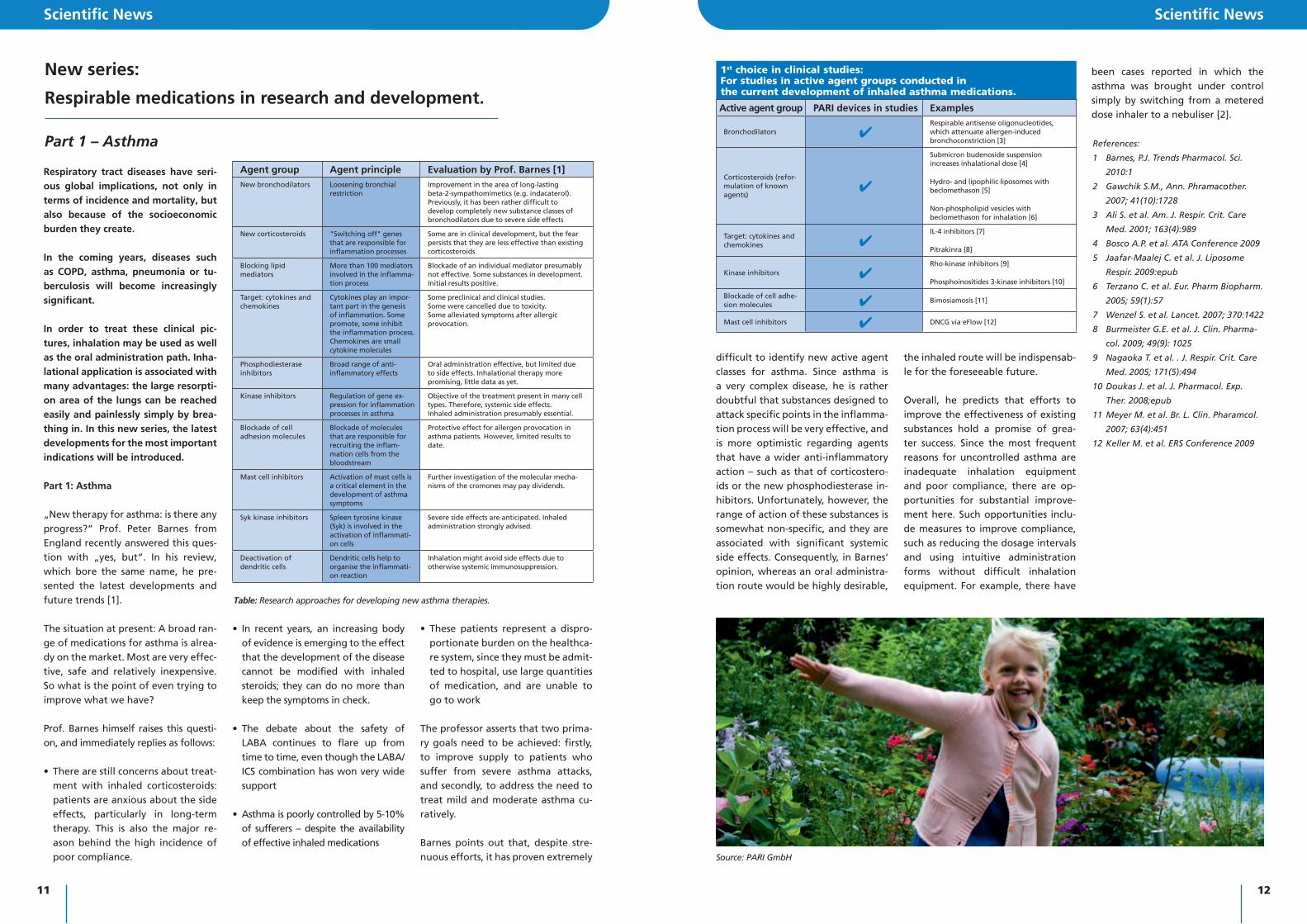
According to study results, the primary goals of self-management with COPD
- greater independence- better symptom control- fewer hospital stays
can be supported by using a nebuliser [1,2]
COPD:
Nebulisers support successful self-management
At least, there are certain patients who would subscribe to this claim. Do you also know of any cases of a strong „emotional“ bond with an in-halation device? A qualitative study of this subject was presented at the ERS Congress. It was entitled „Doc-tor, please don‘t take away my ne-buliser“ [1], and its purpose was to analyse the experiences of COPD pa-tients with their long-term nebuliser therapy. At the same time, it was ho-ped to gain a better understanding of the importance of this therapy form for the daily lives of the pati-ents. The authors drew three main conclusions:
• Nebuliser therapy is well managed and integrated in patients‘ daily lives
• The subjective feeling of well-being is improved with a nebuliser
• The nebuliser is valued as an aid to self-management of the disease
What does „self-management“ mean for the patients? One answer might be found in this remark made by one of the study participants „Wi-thout my nebuliser I would probably not even be able to get out of bed and make a cup of tea … just the nor-mal things you do in the morning.“ A few years ago, Barta et al. published similar results from a larger-scale stu-dy [2]. Most of the COPD patients sur-veyed found that nebulisers played a critical part in their lives. They felt that they were more independent, could control their symptoms better, and indicated that nebuliser therapy helped them to avoid more hospital admissions (see fi gure).
Sources:
1 Schreuder et al. (2009 ERS Conference):
P2295
2 Barta et al. (2002); Respir. Med; 96(6):
375
Figure: nebuliser therapy supports the
self-management of COPD patients 8
[data from 2]
40
35
30
25
20
15
10
5
0
No
. of
pat
ien
ts (
n=
75)
Stro
ngly ag
ree
Agree
Do not a
gree
Stro
ngly
disagre
e
Not sure
Feel more independent since I began using a nebuliser
Helps me to avoid hospitalisations
Helps me to control symptoms better
9 10
Respiratory tract diseases have seri-ous global implications, not only in terms of incidence and mortality, but also because of the socioeconomic burden they create.
In the coming years, diseases such as COPD, asthma, pneumonia or tu-berculosis will become increasingly significant.
In order to treat these clinical pic-tures, inhalation may be used as well as the oral administration path. Inha-lational application is associated with many advantages: the large resorpti-on area of the lungs can be reached easily and painlessly simply by brea-thing in. In this new series, the latest developments for the most important indications will be introduced.
Part 1: Asthma
„New therapy for asthma: is there any progress?“ Prof. Peter Barnes from England recently answered this ques-tion with „yes, but“. In his review, which bore the same name, he pre-sented the latest developments and future trends [1].
The situation at present: A broad ran-ge of medications for asthma is alrea-dy on the market. Most are very effec-tive, safe and relatively inexpensive. So what is the point of even trying to improve what we have?
Prof. Barnes himself raises this questi-on, and immediately replies as follows:
• There are still concerns about treat-ment with inhaled corticosteroids: patients are anxious about the side effects, particularly in long-term therapy. This is also the major re-ason behind the high incidence of poor compliance.
Scientific News Scientific News
New series:
Respirable medications in research and development.
Part 1 – Asthma
• In recent years, an increasing body of evidence is emerging to the effect that the development of the disease cannot be modified with inhaled steroids; they can do no more than keep the symptoms in check.
• The debate about the safety of LABA continues to flare up from time to time, even though the LABA/ICS combination has won very wide support
• Asthma is poorly controlled by 5-10% of sufferers – despite the availability of effective inhaled medications
• These patients represent a dispro-portionate burden on the healthca-re system, since they must be admit-ted to hospital, use large quantities of medication, and are unable to go to work
The professor asserts that two prima-ry goals need to be achieved: firstly, to improve supply to patients who suffer from severe asthma attacks, and secondly, to address the need to treat mild and moderate asthma cu-ratively.
Barnes points out that, despite stre-nuous efforts, it has proven extremely
Agent group Agent principle Evaluation by Prof. Barnes [1]New bronchodilators Loosening bronchial
restrictionImprovement in the area of long-lasting beta-2-sympathomimetics (e.g. indacaterol). Previously, it has been rather difficult to develop completely new substance classes of bronchodilators due to severe side effects
New corticosteroids "Switching off" genes that are responsible for inflammation processes
Some are in clinical development, but the fear persists that they are less effective than existing corticosteroids
Blocking lipid mediators
More than 100 mediators involved in the inflamma-tion process
Blockade of an individual mediator presumably not effective. Some substances in development. Initial results positive.
Target: cytokines and chemokines
Cytokines play an impor-tant part in the genesis of inflammation. Some promote, some inhibit the inflammation process. Chemokines are small cytokine molecules
Some preclinical and clinical studies. Some were cancelled due to toxicity. Some alleviated symptoms after allergic provocation.
Phosphodiesterase inhibitors
Broad range of anti-inflammatory effects
Oral administration effective, but limited due to side effects. Inhalational therapy more promising, little data as yet.
Kinase inhibitors Regulation of gene ex-pression for inflammation processes in asthma
Objective of the treatment present in many cell types. Therefore, systemic side effects. Inhaled administration presumably essential.
Blockade of cell adhesion molecules
Blockade of molecules that are responsible for recruiting the inflam-mation cells from the bloodstream
Protective effect for allergen provocation in asthma patients. However, limited results to date.
Mast cell inhibitors Activation of mast cells is a critical element in the development of asthma symptoms
Further investigation of the molecular mecha-nisms of the cromones may pay dividends.
Syk kinase inhibitors Spleen tyrosine kinase (Syk) is involved in the activation of inflammati-on cells
Severe side effects are anticipated. Inhaled administration strongly advised.
Deactivation of dendritic cells
Dendritic cells help to organise the inflammati-on reaction
Inhalation might avoid side effects due to otherwise systemic immunosuppression.
Table: Research approaches for developing new asthma therapies.
difficult to identify new active agent classes for asthma. Since asthma is a very complex disease, he is rather doubtful that substances designed to attack specific points in the inflamma-tion process will be very effective, and is more optimistic regarding agents that have a wider anti-inflammatory action – such as that of corticostero-ids or the new phosphodiesterase in-hibitors. Unfortunately, however, the range of action of these substances is somewhat non-specific, and they are associated with significant systemic side effects. Consequently, in Barnes‘ opinion, whereas an oral administra-tion route would be highly desirable,
References:
1 Barnes, P.J. Trends Pharmacol. Sci.
2010:1
2 Gawchik S.M., Ann. Phramacother.
2007; 41(10):1728
3 Ali S. et al. Am. J. Respir. Crit. Care
Med. 2001; 163(4):989
4 Bosco A.P. et al. ATA Conference 2009
5 Jaafar-Maalej C. et al. J. Liposome
Respir. 2009:epub
6 Terzano C. et al. Eur. Pharm Biopharm.
2005; 59(1):57
7 Wenzel S. et al. Lancet. 2007; 370:1422
8 Burmeister G.E. et al. J. Clin. Pharma-
col. 2009; 49(9): 1025
9 Nagaoka T. et al. . J. Respir. Crit. Care
Med. 2005; 171(5):494
10 Doukas J. et al. J. Pharmacol. Exp.
Ther. 2008;epub
11 Meyer M. et al. Br. L. Clin. Pharamcol.
2007; 63(4):451
12 Keller M. et al. ERS Conference 2009
1st choice in clinical studies:For studies in active agent groups conducted in the current development of inhaled asthma medications.
Active agent group PARI devices in studies Examples
Bronchodilators 4Respirable antisense oligonucleotides, which attenuate allergen-induced bronchoconstriction [3]
Corticosteroids (refor-mulation of known agents)
4
Submicron budenoside suspension increases inhalational dose [4]
Hydro- and lipophilic liposomes with beclomethason [5]
Non-phospholipid vesicles with beclomethason for inhalation [6]
Target: cytokines and chemokines 4
IL-4 inhibitors [7]
Pitrakinra [8]
Kinase inhibitors 4Rho-kinase inhibitors [9]
Phosphoinositides 3-kinase inhibitors [10]
Blockade of cell adhe-sion molecules 4 Bimosiamosis [11]
Mast cell inhibitors 4 DNCG via eFlow [12]
the inhaled route will be indispensab-le for the foreseeable future.
Overall, he predicts that efforts to improve the effectiveness of existing substances hold a promise of grea-ter success. Since the most frequent reasons for uncontrolled asthma are inadequate inhalation equipment and poor compliance, there are op-portunities for substantial improve-ment here. Such opportunities inclu-de measures to improve compliance, such as reducing the dosage intervals and using intuitive administration forms without difficult inhalation equipment. For example, there have
been cases reported in which the asthma was brought under control simply by switching from a metered dose inhaler to a nebuliser [2].
Source: PARI GmbH
11 12

Scientifi c News
In vitro tests revealed significant advantages of the lightweight PARI BOY® mobile S. Compared to the other systems, PARI BOY® mobile S produced more respirable droplets for inhalation into the deep lungs and nebulised the test substance in the shortest time.
Two US scientists evaluated the per-formance characteristics of four of the most popular portable nebuliser systems in their lab. First, the aero-sol droplet size was measured. This is an important measure; to reach the deep lungs small droplets need to have diameters smaller than 5µm (thousandth part of a millimetre). Three of the four devices fulfilled this quality feature.
Further measurements were obtained using breath simulation: The nebu-lisers were connected to a breathing
Congress news
Comparison of four portable jet nebuliser systems:
PARI BOY® mobile S performed best
simulator to represent actual pati-ent breathing conditions to measure the amount of test drug that would reach the lungs.
PARI BOY® mobile S significantly out-performed the three other devices. Three times more respirable drug was produced compared to the lowest performing device and 30% more respirable drug dose was delivered to the “lungs” of the simulated patient compared to the second best perfor-ming device.
The “S” in PARI BOY® mobile S stands for “SPRINT” and it lives up to its reputation, considering the amount of drug that is released per minute at the mouthpiece – i.e. a sort of nebulising velocity – the PARI BOY® mobile S was six times faster than the slowest performing device and had
a notably, 50% faster rate than the runner-up.
The scientists presented these results at this year’s Congress of the American Thoracic Society (ATS) in New Orleans. They report that the big differences in performance bet-ween the nebuliser systems might be clinically significant. Their conclusion: The decision for or against a speci-fic nebuliser device should be made carefully. Once efficient therapy is established in a patient, system chan-ging is not recommended.
Source:
Tiffi n & Zeman ATS conference 2010:
poster 1494
Scientifi c News
A Russian workgroup compared stan-dard therapies with a course of treat-ment using PARI SINUS for infantile viral and allergic rhinitis. The standard therapy for allergic rhinitis was mon-teleukast or a glucocorticoid nasal spray. The standard therapy for viral rhinitis was not specifi ed. The children (aged 5-14) in the „PARI SINUS group“ nebulised either a combination of be-denoside, oxymetazoline and ambro-xol for allergic rhinitis or cefamyzin, oxymetazoline and acetyl cysteine for viral cold symptoms.
All patients who received treatment with the pulsed aerosol from the PARI SINUS device showed faster recovery from their symptoms than the pati-ents using the standard therapy.
Children with rhinosinusitis benefi t from
treatment with the PARI SINUS device
Source: Geppe et al. Poster at the ERS
Conference 2009
Figure: Reduction of the average symptom
score for viral rhinitis following treatment with
PARI SINUS vs. Standard Therapy
3
2,5
2
1,5
1
0,5
0
Ave
rag
e sy
mp
tom
sco
re f
or
vira
l rh
init
is(0
=ke
ine,
3=
sch
wer
e Sy
mp
tom
e)
Before treatment
Day 3 Day 7
Standard treatment
Treatment with PARI SINUS
6
5
4
3
2
1
0
% s
olid
s in
ASL
CF <3 yr (n=2)
CF 5-12 yr (n=10)
CF adults (n=9)
COPD adults (n=?)
Healthy adults
(n=29)
CF
Disease monitoring
Healthy subjects
Uncontrolled asthma attacks
>30% fall in FEV1 on2 consecutive days
Emergency treatment
Start of oral steroid therapy
Use of emergency medications
Nocturnal waking
0 0,5 1 1,5 2
Ratio of occurrence frequency: esomeprazol group / placebo group6
5
2
3
2
1
0
Spu
tum
wei
gh
t [g
]
Physio-therapy
alone
Physio-therapy
+isotonic
saline
Physio-therapy
+hypertonic
saline
Faster improvement
with PARI SINUS
Cystic fi brosis: Does hypertonic saline improve nutritional status?
Results were presented at this year’s European Cystic Fibrosis Conference from a study in which BMI had signi-ficantly increased for 14 cystic fibro-sis patients after inhaling hypertonic saline for at least 18 months.
Due to their poor nutritional status, cystic fi brosis patients are mostly underweight and have to take dietary supplements every day. Hence, an Italian group of phy-sicians chose the body mass index (BMI) as a quantifi able parameter for the over-all state of health in this disease [1].
The authors compared the baseline BMI to values during therapy, which were measured every six months. Patients’ average age was 17 years and they had
been on hypertonic saline for a mean of 32 months. In those participants that did not require dietary supplements, the mean BMI increased from 18,2 to 20. In the group of patients requiring daily nu-tritional supplementation the mean BMI rose from 17,8 to 19,5.
The physicians’ conclusion: “Long-term HS has a positive effect on nutritional status in adolescent patients with mild to moderate CF lung disease.” However, investigators also stated that studies with more patients would be necessary to con-fi rm these preliminary results.
Hypertonic saline is often used in cystic fi brosis patients to improve mucocilia-ry clearance. Many studies have shown
that inhaling hypertonic saline is a very benefi cial treatment in CF: it facilitates airway clearance, patients experience improved lung function, and suffer less from exacerbations2. Quality of life ques-tionnaires report that patients on the whole feel a lot better when they are on inhaled hypertonic saline therapy [2].
Sources:
1 Fogazzi et al. 2010 J Cyst Fibr 9
(suppl 1):S64
2 Wark & McDonald 2009 Cochrane Databa-
se Syst Rev: CD001506
PARI LC SPRINT:
nebuliser of choice for clinical trials with inhaled antibiotics
The main advantage of inhaled anti-biotic therapy is that the drug directly reaches the site of action and reduces adverse events for the entire organism. Recent results from ongoing clinical trials with ciprofloxacin – an antibiotic with a broad antibacterial spectrum – were presented at the ATS conference in New Orleans. This drug is currently commercially available for oral or intra-venous administration only, but is now being tested as an inhaled drug. The active substance has been specifically reformulated for patient-friendly use with once daily administration via the PARI LC® SPRINT nebuliser.
According to the study investigators, the reason for selecting the PARI LC® SPRINT nebuliser was that many pati-ents with cystic fi brosis or bronchiectasis have similar systems at home and are very familiar with its use and inhalation technique.
The lungs of people suffering from cy-stic fi brosis or bronchiectasis are often persistently colonised with bacteria. This leads to an infl ammatory process,
mucus overproduction and severe tissue damage in this vital organ. Pseudomo-nas aeruginosa, a prevalent organism, is of particular concern in this population. Only certain antibiotics are suitable to destroy it -ciprofl oxacin is one of them. It is a well-established drug availab-le since the 1980’s which is currently available as tablets, drops, or solution for infusion or injection.
Inhaling this substance directly into the lungs may greatly increase the benefi t to risk ratio for patients – that is the fi rm belief of the scientists at Aradigm Corporation. The company specializes in products for severe lung disease. Re-searchers at Aradigm managed to pack ciprofl oxacin into nanoparticles. This leads to a slow release of the active substance in the lungs and a concomi-tant long duration of action. The great advantage: the drug has to be adminis-tered only once daily. Cystic fi brosis pa-tients will appreciate this, as their treat-ment burden is very high – often taking more than one hour per day.
The current state of development was
presented during the annual confe-rence of the American Thoracic Society (ATS). Study results so far, demonstrate that the number of bacteria in mucus that patients coughed up could be re-duced by a factor of 1000 to 10000. No serious adverse events occurred.
These encouraging results promote further development of the drug pro-duct and „will support inclusion of young CF patients in our future pivotal trials,“ said Dr. Paul Bruinenberg, the Company‘s Medical Director. In May, the FDA gave the “go-ahead” for further clinical studies.
Sources:
Bilton et al. ATS conference 2010:
poster E49
Bruinenberg et al. ATS conference 2010:
poster E50
13 14

Scientifi c News Scientifi c News
Chronic rhinosinusitis is a complex condition that is quite common and considerably compromises the quali-ty of life in cystic fibrosis patients. In a study conducted with the mucoly-tic drug dornase alfa via PARI SINUS, cystic fibrosis patients with chronic rhinosinusitis had significant impro-vement in symptoms after only 4 weeks of therapy. They reported im-proved quality of life and physicians acknowledged a significant reduction of complaints.
The average participant age was 22 years in the randomized, placebo con-trolled cross-over study. Patients were randomly assigned to two treatment groups. The fi rst group received dor-nase alfa via PARI SINUS for 28 days, the second group a placebo treat-ment. After a 4 week washout peri-od, patients crossed over to the other group.
PARI SINUS and dornase alfa:
an effi cient tandem team in treating chronic rhinosinusitis
Quality of life was assessed with a standardised questionnaire at base-line and at the end of each treatment period. Symptoms and lung function were also evaluated. All parameters signifi cantly improved during therapy with dornase alfa via PARI SINUS com-pared to placebo treatment. The the-rapy was well tolerated and no severe adverse events occurred.
These results were presented at this year’s European cystic fi brosis confe-rence in Valencia. The workgroup led by Jochen Mainz (PHD) from Jena, Germany, concluded: “Even in the short period of 4 weeks of treatment the new method of sinonasal inhala-tion of dornase alfa led to signifi cant reduction of sinonasal symptoms in CF-patients”.
Whereas the nose is easily reached with simple nasal sprays or irrigations, therapy for the paranasal sinuses
poses much more of a problem. The “gate” into these cavities is very nar-row and fl uids or aerosol administe-red conventionally are unable to gain access. The PARI SINUS is a ground-breaking device, which sends a pulsa-ting aerosol into the nose – using fast and small impulses, the drug mist can also penetrate the paranasal sinuses (refer also to Aerosol Journal Today 1/2009 p.6).
Source:
Mainz et al. 2010 J Cyst Fibr 9(suppl 1): 23
The fraction of solids in the airway surface liquid (ASL) was used as a re-ference parameter for dehydration of the respiratory tract. This value was quantifi ed gravimetrically from spu-tum specimens or from endoscopic biopsies. The material was supplied by cystic fi brosis patients „disease monitoring procedures“ (asthma and COPD patients as well as people with primary ciliary dyskinesia) and healthy subjects. Up to the time of publication, only a few participants could be studied (see chart for exact numbers), so the results must be con-sidered preliminary. However, the-re was a clear trend towards severe ASL dehydration even among very young CF patients (<3 years old). „Dry respiratory tracts“ were also experi-enced by adult patients with mode-
„Dry respiratory tracts“ for cystic fi brosis patients
evident at early age
Figure: The fraction of solids in the airway
surface liquid (ASL) was signifi cantly higher
for cystic fi brosis or COPD patients than for
healthy study participants.
3
2,5
2
1,5
1
0,5
0
Ave
rag
e sy
mp
tom
sco
re f
or
vira
l rh
init
is(0
=ke
ine,
3=
sch
wer
e Sy
mp
tom
e)
Before treatment
Day 3 Day 7
Standard treatment
Treatment with PARI SINUS
6
5
4
3
2
1
0
% s
olid
s in
ASL
CF <3 yr (n=2)
CF 5-12 yr (n=10)
CF adults (n=9)
COPD adults (n=?)
Healthy adults
(n=29)
CF
Disease monitoring
Healthy subjects
Uncontrolled asthma attacks
>30% fall in FEV1 on2 consecutive days
Emergency treatment
Start of oral steroid therapy
Use of emergency medications
Nocturnal waking
0 0,5 1 1,5 2
Ratio of occurrence frequency: esomeprazol group / placebo group6
5
2
3
2
1
0
Spu
tum
wei
gh
t [g
]
Physio-therapy
alone
Physio-therapy
+isotonic
saline
Physio-therapy
+hypertonic
saline
Source:
Ramanathan et al. Poster at NACF
Conference 2009
rate COPD, though the symptom was less pronounced in these cases (Ra-manathan et al. p. 48).
Poorly controlled asthma –
Empirical treatment rarely helps against refl ux
The link between asthma and reflux is a close one. 20-80% of asthma pa-tients also suffer from „GERD“*. Yet this association is highly complex and has not yet been adequately in-vestigated. There are recommenda-tions for using empirical medications against reflux by patients with un-controlled asthma [1], even if there are no symptoms of GERD. However, the justification for this clinical prac-tice has largely been discredited by an ongoing US study entitled „SARA“ [2]
412 asthma patients were included in this „Study of Acid refl ux in Asthma“ (SARA). The disease was not adequa-tely controlled even with the use of inhaled steroids, but there were no symptoms of refl ux. The study parti-cipants received 40 mg esomeprazol against acid refl ux or a placebo twice a day throughout the 24-week study.
Everyone kept a journal for this time, in which they recorded their peak fl ow values, intensity of incidents, and their use of bronchodilators. Af-ter every four weeks, this data was analysed and a spirometry was also carried out.
Figure 1: Empirical treatment of asthma patients with anti-refl ux medication brought no
signifi cant improvement.
3
2,5
2
1,5
1
0,5
0
Ave
rag
e sy
mp
tom
sco
re f
or
vira
l rh
init
is(0
=ke
ine,
3=
sch
wer
e Sy
mp
tom
e)
Before treatment
Day 3 Day 7
Standard treatment
Treatment with PARI SINUS
6
5
4
3
2
1
0
% s
olid
s in
ASL
CF <3 yr (n=2)
CF 5-12 yr (n=10)
CF adults (n=9)
COPD adults (n=?)
Healthy adults
(n=29)
CF
Disease monitoring
Healthy subjects
Uncontrolled asthma attacks
>30% fall in FEV1 on2 consecutive days
Emergency treatment
Start of oral steroid therapy
Use of emergency medications
Nocturnal waking
0 0,5 1 1,5 2
Ratio of occurrence frequency: esomeprazol group / placebo group6
5
2
3
2
1
0
Spu
tum
wei
gh
t [g
]
Physio-therapy
alone
Physio-therapy
+isotonic
saline
Physio-therapy
+hypertonic
saline
A comparison of the placebo and ve-rum groups with regard to emotional strain caused by the uncontrolled na-ture of the disease revealed no signi-fi cant differences (see Figure 1).
For practical purposes, these results have the following signifi cance: pa-tients with poorly controlled asthma, but who are receiving treatment with appropriate „controller“ medica-tions, should not receive antacids if GERD is suspected: other causes of the inadequate asthma control should be sought: are other comorbidities pre-sent, such as aspergillosis, sinusitis, allergic rhinitis or a vocal cord disor-der? Or is the cause simply improper use of the inhalation equipment? In this case, all the patient may need is some instruction, or to change to an inhalation device that is easier to coordinate – such as a nebuliser – in order to feel better (see our report in Aerosol Journal 2/2008, P. 17).
*GERD Gastro esophageal refl ux disease
Sources:
1. Riscili, Cleveland Clinic Journal of Me-
dicine, 3/2010
2. National Asthma education and
Prevention Program, J. Allergy Clin
Immunol. 2007
Source: PARI GmbH
15 16

News in Brief News in Brief
Update to DGP coughing guideline
The new guideline for diagnosing and treating adults suffering from acute or chronic cough has been published in the June edition of the technical magazine Pneumologie (Pneumology). This update became necessary due to scientific advances in the last five years.
One addition since the 2004 version is that the „GRADE“ system (Grades of Recommendation, Assessment, Development and Evaluation) has been used for recommendations – it contains 4 levels of evidence and two levels of recommendation and is thus considerably easier and clearer than the previous SIGN system (Center of
Evidence Based Medicine 1999). It has now also been recognised as the in-ternational standard.
The number of recommendations has been reduced from 42 to 37. For ex-ample, the explicit recommendation to use intravenous antibiotics against persistent coughing has been omit-ted, while the recommendation for treatment with inhaled antibiotics has been reformulated: in the case of bronchiectases with resistant coug-hing, this method is now generally „strongly“ recommended.
The clinical pictures that were treated in a separate CPH item (chronic per-
sistent coughing) in the 2004 version have now been integrated in the ca-tegory „chronic coughing“.
The new version devotes greater at-tention to PEP breathing and PEP coughing. Both are considered as an option to assist secretion mobilisation and for learning coughing avoidance technique.
Besides antibiotic inhalation, the plant-based active agent combinati-on of thyme-ivy-primrose now also enjoys a „stronger“ recommendation as a treatment for acute coughing.
To mix or not to mix? The medical team led by Professor Darko at the SUNY Upstate Medical University Hospital observed in its own routine work that nurses and other healthca-re staff often do not know enough about whether certain nebuliser so-lutions can be mixed.
In this hospital, for example, the only information available was a single sheet of paper listing the most com-mon medications and the notation „Yes“ or „No“. There were no ex-planatory notes about the evidence on which the notation was based. Reason enough to carry out another thorough review of mixability. Af-ter carefully analysing the available
data from scientific literature, from package inserts and commercial da-tabases, the authors compiled a com-prehensive chart in table form and published it in the American Journal of Health-System Pharmacy [1]. The most important innovation was that they not only considered purely phy-sicochemical compatibility, but also drew on clinical experience with cer-tain mixtures.
New guideline for mixing compatibility of nebuliser solutions
Table 1: Clinically tested nebulised medication mixtures [1]
Active agent
Can be mixed with*
Acetyl X + + + - + - -
Budesonide + X - - - + + -
Colistin + - X - - + -
DNCG + + - X + + + -
Epinephrine - - - + X - - -
Ipratropium - + - + - X + +
Salbutamol - + + + - + X +
Tobramycin - - - - - + + X
Acety
l cys
tein
e
Budesonid
e
Colistin
DNCGEp
inep
hrine
Salb
utam
ol
Tobra
myc
in
Ipra
tropiu
m
Mixing is possible: The latest medication mixtures tested in clinical studies.
Source:
1 Burchett et al. 2010 Am J Health-Syst
Pharm 67(1):227-30
* Please review the corresponding
technical information.
On the technique, practice and traps in inhalation
therapy
Paediatricians find time and again that one of their young asthma pati-ents is not responding to treatment. When that happens, it is time to start looking for the reason: is there something wrong with the diagnosis, or is there a fault with the inhalation device after all, is the patient inha-ling properly, or are they not comp-lying fully with the programme?
At the end of a workshop during the 16th annual meeting of the Westdeutsche Arbeitsgemeinschaft für Pädiatrische Pneumologie und Allergologie e.V. (WAPPA) ( West German Work Group on Paediatric Pneumology and Allergology), pri-vate lecturer Dr. Kamin wanted to impart to his audience some useful advice from his immense experience. He pointed out that if „therapy is not working“ it is usually worth looking for technical errors in the inhalation therapy.
For example, if a holding chamber is to be attached in front of the spray, consider what it is made of: electro-static charging of plastic spacers can cause dosage losses of as much as 80%.
It is also very important to ensure that masks are fitted properly on the face, because even tiny gaps may result in almost no medication being delivered to the lungs. In general, patients should switch to inhaling with a mouthpiece as soon as possi-ble, because oral inhalation is up to ten times more effective than with a mask.
Another stumbling block might be the prescription of different inha-lers for the same asthma patient: even with good instruction, patients are usually only able to retain one inhalation technique – rapid inha-lation for the powder inhaler – and even this is forgotten by children and adolescents within a few months. Therefore, it is essential to repeat the instruction in inhalation technique again and again.
As always before, PD Dr. Kamin placed considerable emphasis on inhalation therapy. He recalled that one of the great advantages of this form is that different sized droplets can be produced depending on the indication and the age of the patient. And the expert advised his listeners
that it is also very important to use the psychological advantages of the system.
He was referring to a principle that was described several years ago as the „feelgood factor“ [1]. Dr. Brownlee sums it up: „A nebuliser that […] quietly hisses away in the background can do away with an awful lot of anxiety…“.
Indeed, parents often have a great deal of faith in nebuliser therapy when they use it to give their child-ren medication [1]. Many COPD pati-ents find that a nebuliser helps them to breathe better than other inhalers, and also that it contributes to impro-ving their overall quality of life [2-5].
Sources:
1 Brownlee et al. 1997; Eur. Respir. Rev.:
177
2 Barta et al. 2002; Respir. Med 96(6):
375
3 Tashkin et al. 2007; Am. J. Med
120(5):435
4 Santana et al. 2006: ERS Conference:
poster E469
5 Schreuder et al. 2009 ERS Conference:
poster P2295
Source: PARI GmbH
17 18

Would you send the parents of an infant suffering from bron-chiolitis back home, evenafter giving them instructions on care? With-out a prescription of any kind, whether for refundable or privately bought medication?
This is what happens according to the guidelines – antibiotics, steroids, bron-chodilators, all are therapy forms that have not passed scrutiny by the Cochra-ne Collaboration, and therefore are not to be administered [1,2,3].
Yet the clinical picture of bron-chiolitis is often severe. These small patients (and accordingly their parents as well) are sufferingconsiderably.
But now a new treatment option has made an appearance: nebulised 3% sa-line solution – on its own or in conjunc-tion with bronchodilators. In 2008, the effi cacy of this therapy form was cer-tifi ed by a Cochrane Review [4]. Since then it has been adopted in a growing variety of updated treatment recom-mendations [5,6,7].
3% saline solution for acute bronchiolitis
News from PARI News from PARI
To date, 7 randomised, blind clinical studies have been carried out invol-ving just under 600 patients, and eve-ry one of them has confi rmed the po-sitive effect of 3% saline solution as a treatment for bronchiolitis [8-14].
The more severe the clinical picture, the more pronounced was the bene-fi t.
For both outpatients and inpatients, the symptoms began subsiding im-mediately after inhalation [8,10] (see fi gure 1).
A comparison was made of the point values for the severity of sym-ptoms over the 3-day treatment period. It indicates clearly that the positive effect of hypertonic sali-ne solution helps reduce the symp-toms of a bronchiolitis attack. [8,12] (see fi gure 2).
In severe cases of bronchiolitis that necessitated hospitalisation, treat-ment led to a much shorter hospital stay – this result was recorded in 4 dif-ferent studies [8,9,11,12]. (see fi gure 3).
Fig. 1: Young bronchiolitis sufferers began fee-
ling much better just 30 minutes after inhaling
3% saline solution (n=52, Ø age = 2.9 ± 2.1
months). The difference compared with the
placebo was signifi cant. [Data from 10].
Fig. 2: Treatment with inhaled hypertonic
saline solution helped to alleviate the severi-
ty of symp-toms over the course of the illness
(93 patients, Ø age = 5.8 ± 4.4 months). [Data
from 12].
MucoClear 3% offers a handy, sterile solution – free from preservatives. In the UK it is available on prescription from November 2010.
Literature:
1 Gadomski & Bhasale Cochrane Data base
Syst Rev. 2006(3): CD001266
2 Patel et al. Cochrane Database
Syst Rev. 2004(3): CD004878
3 Spurling et al. Cochrane Database
Syst Rev. 2007; 24(1):CD005189
4 Zhang et al. Cochrane Database
Syst Rev. 2008; 8(4): CD006458
5 NHS choices – Bronchiolitis treatment:
http://www.nhs.uk/Conditions/Bronchioli-
tis/Pages/Treatment.aspx
6 Gonzales de Dios et al. An Pediatr
(Barc). 2010:epub
7 Wainwright et al. Paediatr Respir
Rev. 2010; 11(1):39
8 Sarell et al. Chest. 2002; 122(6): 2015
9 Tal et al. Isr Med Assoc J. 2006; 8(3): 169
10 Mandelberg et al. Chest. 2003; 123(2): 481
11 Kuzik et al. J Pediatr. 2007; 151(3): 266
12 Luo et al. Pediatrics International. 009:1
13 Anil et al. Pediatr Pulmonol. 2010; 45(1):41
14 Grewal et al. Arch Pediatr Adolesc Med .
2009; 163(11):1007
Day 2 Day 3Day 1
8
7
6
5
4
3
2
1
0
Tren
d of
sym
ptom
sco
re
Day 1 Day 2 Day 3Baseline
Control group
3% saline solution
10
9
8
7
6
5
4
3
2
1
0
Day
s in
hos
pita
l
Kuzik 2007
Tal 2006
Mandelberg2003
Luo 2009
Control group
3% saline solution
Reduction of time in hospital
0
-2
-4
-6
-8
-10
-12
Acu
te r
educ
tion
in s
ympt
om s
core
follo
win
g in
hala
tion
(%)
Control group
3% saline solution
Measurement of symptom improvement
Fig. 3: Shorter hospital stays were recor-
ded following treatment with inhaled saline
solution in 4 different clinical studies [Data
from 8, 9, 11,12].
Day 2 Day 3Day 1
8
7
6
5
4
3
2
1
0
Tren
d of
sym
ptom
sco
re
Day 1 Day 2 Day 3Baseline
Control group
3% saline solution
10
9
8
7
6
5
4
3
2
1
0
Day
s in
hos
pita
l
Kuzik 2007
Tal 2006
Mandelberg2003
Luo 2009
Control group
3% saline solution
Reduction of time in hospital
0
-2
-4
-6
-8
-10
-12
Acu
te r
educ
tion
in s
ympt
om s
core
follo
win
g in
hala
tion
(%)
Control group
3% saline solution
Measurement of symptom improvement
Day 2 Day 3Day 1
8
7
6
5
4
3
2
1
0
Tren
d of
sym
ptom
sco
re
Day 1 Day 2 Day 3Baseline
Control group
3% saline solution
10
9
8
7
6
5
4
3
2
1
0
Day
s in
hos
pita
l
Kuzik 2007
Tal 2006
Mandelberg2003
Luo 2009
Control group
3% saline solution
Reduction of time in hospital
0
-2
-4
-6
-8
-10
-12
Acu
te r
educ
tion
in s
ympt
om s
core
follo
win
g in
hala
tion
(%)
Control group
3% saline solution
Measurement of symptom improvement
eFlow® rapid now with pause function
With immediate effect, the eFlow®rapid is available with a pause function. The user can thus take a short break from inhaling without having to switch the device off completely. In this way, the function reduces medication waste if the patient needs to take a short rest from inhaling.The procedure is easy and uncomplicated:
1. Inhaling begins as normal by pres-sing the ON/OFF button. Aerosol is generated.
2. The Pause function can be used af-ter operating for 5 seconds.
3. To activate the Pause function, the ON/OFF button is pressed and held down for about 1 second.
4. Pause mode is activated when the LED flashes green.
5. To resume inhaling, the ON/OFF but-ton is pressed and held for about 1 second again.
For more information, please visit www.pari.de on the internet, or call the PARI Service Center at +49 (0)8151-279 279
Inhaling hypertonic saline for bronchiectases?
The term „bronchiectases“ literally means „bronchial enlargements“. These enlargements particularly af-fect the medium sized and small bronchi. Cardinal symptoms of this disease are chronic coughing, increa-sed mucus production, and recurring infections of the respiratory tract.
The advance of the disease is closely associated with sputum retention in the respiratory tract, which causes in-fl ammations, which in turn stimulate further sputum production.
It has been known for some time that hypertonic saline (HS) is able to improve mucociliary clearance. In 2005, Kellett and associates investiga-ted whether bronchiectasis patients might also benefi t from inhalation therapy with HS.
Among other things in this small-scale, double-blind study, they compared inhalation of isotonic and 7% saline solutions, each combined with physio-therapy, and with physiotherapy on its own. They were able to show that inhaling either isotonic or hypertonic saline both increased sputum clearance and reduced sputum viscosity signifi -cantly more than physiotherapy alone. In this context, the best results were achieved when inhaling hypertonic sa-line (see chart).
As a second endpoint of the study, the FEV1 was calculated for all of the diffe-rent treatment regimens. Here, a trend was revealed toward improvement of FEV1 when inhaling hypertonic saline. However, signifi cance could not be de-monstrated because of the small num-ber of probands (24 patients).
Chart: Sputum ejection. The study included
24 patients aged from 50 to 70.
3
2,5
2
1,5
1
0,5
0
Ave
rag
e sy
mp
tom
sco
re f
or
vira
l rh
init
is(0
=ke
ine,
3=
sch
wer
e Sy
mp
tom
e)
Before treatment
Day 3 Day 7
Standard treatment
Treatment with PARI SINUS
6
5
4
3
2
1
0
% s
olid
s in
ASL
CF <3 yr (n=2)
CF 5-12 yr (n=10)
CF adults (n=9)
COPD adults (n=?)
Healthy adults
(n=29)
CF
Disease monitoring
Healthy subjects
Uncontrolled asthma attacks
>30% fall in FEV1 on2 consecutive days
Emergency treatment
Start of oral steroid therapy
Use of emergency medications
Nocturnal waking
0 0,5 1 1,5 2
Ratio of occurrence frequency: esomeprazol group / placebo group6
5
2
3
2
1
0
Spu
tum
wei
gh
t [g
]
Physio-therapy
alone
Physio-therapy
+isotonic
saline
Physio-therapy
+hypertonic
saline
Further studies will be needed to show to what extent inhaling hypertonic sa-line can benefi t patients suffering from bronchiectases and improve infection rates and the FEV1.
19 20

News from PARI News from PARI
User-friendly, understandable, legible:
the new instructions for PARI products
Even good products are only as good as the way they are used.
Only if the user knows how they work and is prepared to learn how to ope-rate them properly will they do their job and provide help. In this way, compliance and effectiveness are in-creased, and patient satisfaction is reinforced, so that those who suffer from respiratory tract diseases obtain the maximum possible benefit from their aids.
This is why PARI goes to great lengths to make sure the instructions for using our products are as clear as pos-sible. At the moment, all instructions for use are being reviewed with re-spect to certain criteria, which have been tested beforehand in extensive user surveys.
The results have led to a number of major changes, which have already been implemented for the LC SPRINT instructions, and will be introduced progressively for all of our products:
1. Two sets of instructions for use for each productSome instructions that may be hel-pful to doctors only confuse patients. Information that patients understand is too long-winded and detailed for medical professionals. In order to be able to retain language and format that is appropriate for the general public and reduce content to just what the patients need, in future a separate set of instructions will be prepared and distributed correspon-dingly for each of these two groups.
User video for the eFlow® rapid
To ensure that first time users can be-gin inhaling with the eFlow®rapid as quickly, easily, and safely as possible, patients can now see a video on using the eFlow®rapid inhalation system. Inhalation with the eFlow®rapid is ex-
PARI runs for CF patients
Every year, several PARI GmbH and PARI Holding GmbH employees place their active commitment on public - and very active - display by taking part in charity runs to benefit cystic fibrosis patients.
In cooperation with the Christiane Her-zog Foundation, and the „CF Initiative aktiv – Aid for cystic fibrosis“, the race team hits the road on behalf of child-ren and adults suffering from the di-sease who receive treatment at the CF centres in Bavaria.
As a registered charity, the CF initiative makes donations to fund social security payments for families that are expe-riencing financial difficulty as a result of cystic fibrosis. The fund finances treatment courses, advanced training events, therapy facilities, counselling centres and much more.
In the autumn of 2009 the race team‘s efforts were rewarded with high ran-kings at the „Brombachsee Running“, at which 3,700 euros were received in donations.
In July 2010, four PARI team runners and an enthusiastic dog took their marks for the CF charity team at the start of the 25th Altmühlseelauf. With 42 men and women, this was the lar-gest team in the half-marathon group, and it succeeded in running down about 3500 euros for the CF foundati-on.
In the Everyman‘s Run and Half-Mara-thon, the PARI team delivered a stor-ming run in the truest sense of the word, winning high places and many hearts.
2. Booklets instead of wallpaper The days of instructions printed on sin-gle sheets of large-format paper will soon be over: in future, these will be largely replaced by small pamphlets and booklets with a table of contents and page numbering so that readers can quickly find what they are looking for, instead of folding and refolding unwieldy sheets.
3. Focus on relevant content The contents for patients have been re-duced considerably, because, for examp-le, information on hygiene when chan-ging patients does not concern them.
4. Better legibility This reduction in content has been used to make space for a larger typeface and more spacious page layout.
5. Pictures instead of words We have also tended to dispense with text when an illustration will serve equally well. This takes up a little more space, but is very important for hel-ping with comprehension by speakers of different languages. This in turn encourages compliance. Diagrams, ta-bles, and overviews illustrate quickly and clearly how a product is assem-bled, used, or cleaned.
6. Linguistic optimisation Simple language, clear instructions, unambiguous messages – that was the aim of this revision. More than half of the patients surveyed agree: the result is „very good“, all other respondents find that comprehensibility is „good“.
In the future too, PARI will continue to make all of our informational materials simpler and easier to un-derstand. If you have any questions, wishes or suggestions, please send an e-mail to: [email protected].
plained and demonstrated clearly in German and English on our website at www.pari.de. The instructions cover all aspects of the device, from assembly to inhaling to hygiene.
The PARI Service Center: Your contact for all questions
+49 (0)8151-279 279. Of course you know this number: it is on every piece of printed material, all an-nouncements and correspondence you receive from PARI, it is on our website, and of course on all our instructions for use, for PARI service is more than just an indispensable part of our business.
The PARI Service Center was set up with telephone number 279 279 in January 2001, and ever since then it has served as a reliable source of information for all customer enquiries, the volume of which grows in line with the range of products we offer. An office that was originally staffed by 3 employees from order processing, repairs, and user ser-vice has blossomed into a fully fledged department of 12, who make sure all your calls are answered from Monday to Friday, from 8 am until 6 pm.
The PARI Service Center handles over 100,000 contacts by telephone, fax or e-mail per year, and this number is on the rise. From orders and requests for informational literature to help with choosing the right product and ques-tions about which medications can be nebulised, the stream of questions and requests is received from pharmacies,
authorised dealers, patients, physicians, physiotherapists and hospitals.
At the same time, our highly trained personnel work closely with our field technicians and is well informed about the market, knows the current needs and concerns of the patients or prescri-bers, and forwards more complex enqui-ries to the product managers or medical scientific department. The goal and gui-ding principle of our department is to ensure that not a single caller goes away without a satisfactory answer. The fact that the Service Center has now become an important part of the pro-duct offered by our company is attested to in feedback from doctors, patients
and dealers or pharmacies, which often turn to the company even for general advice and help in all aspects of respi-ratory tract disease treatment, knowing they are relying on a company with more than a century of experience in the field.
In our constant efforts to be able to of-fer even more personalised advice and more technical expertise, PARI places great importance on continuous trai-ning and advanced education for its employees. Precisely because the health-care environment is changing constant-ly, professional advice is becoming more and more important.
21 22

Date/Meeting location Conference or training session title
October 08. - 09.10.2010 24th annual conference of the Southern Work Group Heidelberg of Paediatric Allergists (AGPAS)
07. - 09.10.2010 Annual conference of the Austrian PneumologyGraz Society
16.10.2010 5th pneumology advanced training dayLinz
22. - 23.10.2010 24th advance training days for the South GermanNuremberg Pneumology Society
28. - 30.10.2010Mannheim 44th ENT Congress
November05. - 06.11.2010 XV German Aerosol Therapy Seminar Marburg / Lahn
12. - 13.11.2010 13th German Cystic Fibrosis Conference Würzburg
ImprintPublisher: PARI GmbHMoosstr. 3 • D-82319 Starnberg Phone: +49 (0) 8151 279-0 • Fax: +49 (0) 8151 279-101 www.pari.de • E-mail: [email protected]
Authors: Dr. Susanne Merk and guest contributors Editor: Petra Kaden • Layout: Christian Hedrich
Conference and Advanced Training Dates
© P
AR
I Gm
bH
– S
pez
ialis
ten
fü
r ef
fekt
ive
Inh
alat
ion
041
D04
35ºı
Iss
ue
2010