Embed Size (px)
Citation preview

SECTION 1
ACUTE BRONCHIOLITIS

IntroductionCommon disease of lower
respiratory tract in infantsCommon age group: 1-3
monthsCommon during winter

Etiology Viral RSV - >50% Para influenza 1,2,3Adeno virus
Non-viralMycoplasma
No bacterial etiology

Epidemiology 100,000-126,000 children
<1 yr - hospitalized annually in the US because of RSV infection
Males – non breast fed babies
Older family members (LRTI) – common source

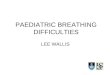
Pathophysiology

Pathophysiology Bronchiolar obstructionMinor bronchial wall
thickeningResistance α
Air trapping & overinflation Atelectasis
1
radius4

Clinical featuresHappy wheezerPreceded by URTI, Mild to
mod. fever(101-2°F)Gradual onset of wheezy
cough, dyspneaTachypnea interfere feeds,
apnea in very young infants

Wheezy cough

Clinical featuresPhysical examinationsTachypnea doesn’t correlate
to the lung findingsIncreased work of breathingHyperinflated chestPredominant wheezePalpable liver & spleen

Bronchiolitis

Investigations Chest – X – Ray:Hyperinflated lungs with
patchy atelectasis
Flat diaphragm
Increased peri-hilar bronchovascular markings


Investigations WBC count: Normal
(without lymphopenia) Diagnosis:Healthy infant first t ime
wheeze during winter

Differential diagnosis
Bronchial asthma- family history atopy
CCF- suck rest suck cycleFB aspiration- sudden
onset, choking episodeBacterial pneumonia- sick
child

Course & PrognosisHighest risk (cough &
dyspnea) – first 48 to 72 hrsDeath is due to Uncompensated respiratory
acidosisApneaSevere dehydration

Course & PrognosisRisk factors for severe
disease- age <12 wk, preterm birth, or underlying comorbidity such as cardiovascular, pulmonary, neurologic, or immunologic disease

TreatmentHospitalize - hypoxia,
inability to take oral feedings, apnea, extreme tachypnea
Supportive therapy- IV fluids, humidified oxygen, careful monitoring
No sedation- clear upper airways

Treatment options available
1. Inhaled epinephrine: some clinical improvement
2. Inhaled bronchodilators – no use
3. Inhaled anti-cholinergics- no use
4. Hypertonic saline nebulization- some clinical improvement
5. Steroids- No role
6. Antibiotics – no role, Mycoplasma suspected- Macrolides
7. Antiviral- Palivizumab, Ribavirin- underlying CHD, immunodeficiency

Prevention Meticulous hand washing

STRIDOR AND ALTB
Section 2

StridorHarsh, high-pitched
respiratory sound, which is usually inspiratory but can be biphasic- sign of upper airway obstruction

Causes Acute Onset
ALTB
Epiglottitis
Foreign body
Retropharyngeal abscess
Bacterial trachiitis
Peritonsillar abscess
ChronicVascular ring
Laryngomalacia
Vocal cord dysfunction

ALTB Causes- Viruses-
Parainfluenza virus 1,2,3Inflammation of Larynx,
trachea and bronchus

C/F Upper respiratory tract infection-
rhinorrhea, pharyngitis, mild cough, and low-grade fever for 1-3 days
Characteristic “barking” cough, hoarseness, and inspiratory stridor- worse at night and often recur with decreasing intensity for several days and resolve completely within a week
Agitation and crying- aggravate Not ill looking

Croup

Investigations X ray- Steeple signCroup is a clinical
diagnosis and does not require a radiograph of the neck

Steeple sign

TreatmentNebulized Adrenaline- moderate or
severe croup- used as often as every 20 min
Oral dexamethasone used a single dose of 0.6 mg/kg, a dose as low as 0.15 mg/kg may be just as effective
Intramuscular dexamethasone and nebulized budesonide have an equivalent clinical effect

Complications 15% children with croup- complications Hypoxia and low oxygen saturation only
when complete airway obstruction imminent
Child who is hypoxic, cyanotic, pale, or obtunded- immediate airway management
Bacterial tracheitis in some

EpiglottitisBends
forwardTripod
positionDroolingToxic child

Epiglottitis

Thumb sign

Croup vs epiglottitis
Inflammation of LTB- Caused by virus- Parainfluenza
Usually mild No fever at
presentation- non toxic child
X ray neck AP- Steeple sign
Treatment- Nebulized adrenaline, Steroids, humidified oxygen
Inflammation of epiuglottis- Caused by bacteria- H.influenzae
Serious illness High fever at
presentation- toxic child
X ray neck lateral- Thumb sign
Treatment- may need airway management, ventilation, Antibiotics