Embed Size (px)
Citation preview
Advocating for Abortion Access:
Eleven Country Studies
Copyright: Women’s Health Project 2001.The publication may be reviewed, abstracted or reproducedin part when fully referenced, but not for sale or for use inconjunction with commercial purposes.
Published by:The Women’s Health ProjectSchool of Public HealthUniversity of the WitwatersrandJohannesburgSouth Africa
P O Box 1038 Johannesburg 2000 South AfricaFax: 27 11 489 9922Telephone: 27 11 489 9917E-mail: [email protected]: www.sn.apc.org/whp/
Project managed by Zanele Hlatshwayo
Publication edited by Barbara Klugman and Debbie Budlender
Copy edited and proof-read by Cheryl Hunter
Layout by ITL Communication and Design
Cover photograph taken by Daniela Colombo during a rallyin Rome in 1977. The women carry placards with names ofwomen who had died after undergoing clandestine abortions.
Printed by Witwatersrand University Press, Johannesburg
ISBN No 1-86383-283-4
Also available in Spanish
AcknowledgementsThe Johannesburg Initiative is funded by the Government ofthe Netherlands and the Swedish International DevelopmentCooperation Agency (Sida). The South African case study wassupported by the Health Systems Trust.
We thank them all for their willingness to support a ‘south-based’ initiative and one which seeks to explore this contro-versial yet critical issue for women’s rights and health.
We would like to thank all the participants in this Initiative fortheir commitment to this endeavour. We would like to thankour colleagues at Women’s Health Project (WHP) includingour financial officer, Lynn Reynolds, operations managerJennifer Harris and administrator Thandi Mosiane, for man-aging the logistics of the Initiative.
We would like to thank Debbie Budlender for her insights,pace, positive working style with all authors, and commitmentto producing a fine publication.
DedicationThis publication is dedicated to all the women who have hadunsafe abortions and as a result have been criminalised, hu-miliated and can no longer have children. It is dedicated tothose who have died because they were denied the right tochoose whether or not they wanted to have a child.
Advocating for Abortion Access: Eleven Country Studies
Produced through the collective input of participants in the JohannesburgInitiative:
Ana Cortes Mexico
Antonietta Cillumbriello Italy
Barbara Klugman South Africa
Cait Calcutt Australia
Chantal Birman France
Esmeralda Kuliesyte Lithuania
Fred Nunes Guyana
Friday Okonofua Nigeria
Hailemichael Gebreselassie Ethiopia
Halida Hanum-Akhter Bangladesh
Katini Nzau-Ombaka Kenya
Maria Gutierrez Argentina
Marlene Gerber Fried United States of America
Martha Rosenberg Argentina
Noeleen Hartigan Ireland
Sanjani Varkey South Africa
Sarah Pene Fiji
Shelia Clarke United States of America
Sunita Bandewar India
Wanda Nowicka Poland
Wilza Villela Brazil
Zanele Hlatshwayo South Africa
CONTENTSPreface ............................................................................................. vi
Glossary ..........................................................................................xiv
Conceptual framework ...................................................................... 1
Strategy and action for abortionaccess: a comparative analysis .......................................................... 7
The Australian Pro-Choice Movement andthe Struggle for Legal Clarity, Liberal Laws and LiberalAccess: Two Case Studies ............................................................... 41
Current Status of Policy and Accessto Abortion: The Bangladesh Experience ........................................ 71
Expanding Women’s Access toAbortion: The Brazilian Experience ................................................ 87
Implementing a Liberal AbortionLaw in Guyana: Experiences and Lessons ..................................... 109
Abortion Legislation and Access to SafeAbortion Care Services: The Indian Experience ............................ 135
The Fight for Reproductive Rights in Italy .................................... 157
Alternative Access to Abortion ServicesUnder Restricitive Law: The Kenyan Experience .......................... 173
August 2000 Reforms to Mexico CityAbortion Legislation: The Long, Hard Struggle ............................. 199
Struggles For and Against LegalAbortion in Poland ........................................................................ 223
From Policy Development toPolicy Implementation: The South AfricanChoice on Termination of Pregnancy Act .................................... 251
Expanding Abortion Access:The US Experience ........................................................................ 283

Preface
vii
PREFACE
This publication is the result of work undertaken in phase oneof ‘The Johannesburg Initiative’. This is the name given byparticipants to an international project of which the full title is“Capacity building for advocacy on expanding abortion policyand access: sharing of national experiences between countriesfrom diverse regions.”
Background to the initiativeThe initiative was the Women’s Health Project’s response torepeated questions by activists from all over the world: ‘Howdid South Africa win such a liberal abortion law?’ We realisedthat the political and social context that had created the spacefor legal change was very specific to South Africa and that itwas simplistic to think that telling our story would help activistselsewhere. For this reason, we thought we might learn moreby comparing abortion advocacy experiences from differentparts of the world. Would this comparison, for example, showus that under certain circumstances it was impossible to changethe law? Or that all countries which had been successful hadtaken specific actions or had a certain context?
After we had begun to shape an idea for this research, activistsfrom Poland (Wanda Nowicka) and Colombia (Maria IsabelPlata) heard our analysis of the contextual factors and activiststrategies which had resulted in the legal victory in South Africa.They suggested that it would be helpful not just to read analysesfrom different countries, but also to engage in a process ofinteraction between activists in different countries. With theirinput, and that of Marlene Fried in the United States of America(USA), this initiative was shaped and funds raised.
To identify potential participating countries, we sent out a callvia actors in the field of reproductive rights in different parts ofthe world. We asked them to assist in identifying non-govern-
The Johannesburg Initiative
Advocating for abortion access
viii
mental organisations that have worked or currently are work-ing in abortion advocacy in their own countries, rather than atan international level. As names came in, we looked for a mixof countries from all regions of the world and with diverse ex-periences of abortion advocacy.
The aim of the initiative is to build capacity amongst those ofus engaged in advocacy for improving abortion access, whetherthrough legal change or by increasing access to and quality ofservices. By providing case studies of different experiences,activists can interrogate the strategies used by other activists indifferent countries and learn from their successes and mistakes.The project also aimed to provide an example of southern-initiated activism that builds bridges and facilitates learningbetween regions and countries of the north and south.
One particularly dynamic aspect of the initiative was havingpeople from countries in the north and south, as well as coun-tries in transition, working together as equals. This approachallowed not only for a collective analysis of the different coun-try studies, but also for the inclusion of countries that were notinitially part of the initiative or the research group. To facilitatethis, some researchers in the initiative drew fewer funds thanwere originally allocated for individual country studies in or-der to release funds to incorporate additional studies.
Eighteen countries participated in the Johannesburg Initiative.Of these, ten conducted research and documented their coun-try experiences. Their reports are carried in this publication.The other participants contributed actively to the research de-sign and analysis in order to ensure that this research talked totheir concerns and experiences and would be helpful in sup-porting activists in their own countries. The publication there-fore is not only a product of the authors, but of all those in theinitiative.
Participants were invited as representatives of their NGOs. Ina few cases, however, the NGOs contracted an activist re-searcher to represent them and do the research. In two cases,participants had been key players in their countries’ abortionstruggles but the organisational impetus was over. Neverthe-
Preface
ix
less, we felt the stories needed to be shared. The overall inten-tion, however, was for participation in this project to strengthenNGO advocacy efforts.
The participants are:Argentina, Foro por los Derechos Reproductivos, MarthaRosenberg, Maria Gutierrez
Australia, Abortion Rights Network of Australia, Cait Calcutt
Bangladesh, Bangladesh Institute of Research for Promotion ofEssential & Reproductive Health and Technologies, HalidaHanum-Akhter
Brazil, Feminist Health and Sexuality Collective, Wilza Villela
Ethiopia, IPAS, Hailemichael Gebreselassie
Fiji, Fiji Women’s Crisis Centre, Sarah Pene
France, Chantal Birman
Guyana, Fred Nunes
India, Centre for Enquiry into Health and Allied Themes, SunitaBandewar
Ireland, Irish Family Planning Association, Noeleen Hartigan,
Italy, AIDOS, Antonietta Cillumbriello
Kenya, IPAS, Katini Nzau-Ombaka
Lithuania, Family Planning and Sexual Health Association,Esmeralda Kuliesyte
Mexico, GIRE, Ana Cortes
Nigeria, Women’s Health and Action Research Centre, FridayOkonofua
Poland, Federation for Women and Family Planning, WandaNowicka
South Africa, Women’s Health Project, Sanjani Varkey
United States of America, National Black Women’s HealthProject, Shelia Clarke, and the National Network of AbortionFunds and the Civil Liberties and Public Policy Program, Hamp-shire College, Marlene Gerber Fried
The Johannesburg Initiative
Advocating for abortion access
x
Why abortion?Abortion has always been one means for women to take con-trol of their lives. In times past, all cultures had ways of provid-ing abortion to women who, for whatever reasons, did notwant children. In recent centuries, however, society has increas-ingly sought to limit women’s ability to control their reproduc-tive capacity themselves. On the one hand population poli-cies have sought to make decisions for women about whetherthey should have more or fewer children. On the other, themedical profession has sought to professionalise reproductivehealth, undermining the role of traditional midwives andwomen themselves in the reproductive health sphere. In addi-tion, in a number of countries, religious institutions have soughtto apply more limited rulings to the circumstances, if any, un-der which abortion is acceptable.
The Johannesburg Initiative is based on the recognition thatindividuals have the right to control their own bodies, theirsexuality and their reproductive capacity, free of coercion, dis-crimination and violence. Nevertheless, throughout the world,women, men and adolescents are denied this opportunity. Insome cases this is the result of lack of access to services, suchas protection from and treatment of sexually transmitted dis-eases, contraceptives and abortion. In others it is because so-ciety does not recognise the need for equality between womenand men. Unwanted pregnancy is one of the indicators of thisinequality; when women are denied the right to decide withwhom and when they want sexual relations and whether ornot they want a child. Coupled with the lack of access to serv-ices, this leads to high rates of illegal and frequently unsafeabortions. Where abortion is illegal or inaccessible, the searchfor abortion humiliates women and undermines their self-re-spect and dignity. Such abortions may result in criminalisation,infertility, or death.
Abortion represents a woman’s moment of last resort. In thecontext of gender inequality, where sexuality and reproduc-tion are frequently not issues over which women are able toexercise control, abortion serves as a way out. Likewise in con-
Preface
xi
texts of limited availability of contraception or contraceptivefailure. In the long term, we hope to build a society in whichevery person has, as the Beijing Platform of Action asserts,“The right to have control over and decide freely and respon-sibly on matters related to their sexuality, including sexual andreproductive health, free of coercion, discrimination and vio-lence”. There is a long and difficult road to cover before weshall achieve this end.
At the present moment, the right to choose and access abor-tion is an absolute prerequisite for women to be able to exer-cise their human rights. Without abortion access, women can-not exercise their freedom and cannot live as full citizens. Forthis reason, the struggle for abortion rights sits at the heart ofthe women’s rights and health movement. This initiative servesto strengthen that movement.
What is meant by “abortionaccess”?Full access is a key concept in The Johannesburg Initiative.In this publication ‘access’ is described in relation to the law;health services; information, education and communication(IEC); health service providers; and the public domain. All ofthese are perceived to be potential gatekeepers to women ac-cessing abortion services. Achieving full abortion access means:
In relation to the law. Abortion should be decriminalised.No punitive measures should be taken against any individualor organisation that provides abortion services. Women whoseek and have abortions should not be criminalised.
In relation to health services. Women should have thepower to make decisions regarding a termination of pregnancywithout negative interventions from gatekeepers.
All restrictions such as on the basis of age, or requirements forparental or spousal consent should be removed. Requirementsfor multiple doctor approval before an abortion can be con-ducted should be removed. The gestation period should not
The Johannesburg Initiative
Advocating for abortion access
xii
be a deterrent. Likewise, bans on medically appropriate pro-cedures should be removed and so should mandatory coun-selling and all religious and socio-culturally based restrictions.
Full access means that services are free or readily affordable,of good quality care and assured privacy and confidentiality.They should be accessible in all geographical locations and atthe primary level of care.
Management should be accountable for making sure that pro-cedures used by women are appropriate, current and safe.Research institutions and national governments should givepriority to developing and providing methods which womencan control.
In relation to information, education and communica-tion (IEC). Women need to know their rights under the law,as well as how to access abortion services and what optionsare available to them for the procedure. All available choicesshould be accompanied by information facilitating women’sability to choose what is best for them rather than being co-erced with a population control agenda. Educational oppor-tunities should foster peer education and materials should sup-port this approach and be written in appropriate language.Sites for education should be expanded to include the formaland informal and should focus on health and rights.
In relation to health-care providers. Teaching and trainingin abortion provision and care should be institutionalised. Insti-tutional policies must ensure that there are adequate providers.In addition, the bio-medical approach to health care, whichplaces authority in the hands of doctors as opposed to othermedical professionals, such as midwives, should be challenged.
Health service providers should provide the service with thesame diligence as any other service. While respecting the pro-viders’ right to choose, training institutions should help pro-viders to clarify the distinction between their personal viewsand their responsibility for providing a service. Providers shouldnot attempt to limit women’s right to choose abortion whetherby imposing their personal views on abortion, by providing
Preface
xiii
biased information or by putting bureaucratic obstacles in theway of women receiving prompt and responsive attention.
In relation to the public domain. Abortion should bedestigmatised. Strategies should be put in place to counter anti-abortion movements whose main activity is to prevent accessto abortion care and services.
Structure of the Johannesburg InitiativeThe initiative is divided into three phases:
Phase 1: December 1999 – June 2001. The research designwas developed in an interactive process between participants;building on a conceptual framework used by the Women’sHealth Project in analysing the South African experience inwinning the abortion legislation. Eleven countries were cho-sen to document country experiences using the framework.Activists in each of the countries had at some point engaged inadvocacy to increase abortion access. After developing the con-ceptual framework, the NGOs and researchers in the elevencountries used it to undertake policy research and record theirfindings. Five months later the participants reconvened to dis-cuss the findings. They conducted a collective analysis of thestrategies employed by the different countries and examinedthe emerging themes. This analysis formed the basis of thesynthesis that appears in this volume.
Each participant peer reviewed a number of the papers, pro-viding authors with further questions to explore or ideas onhow to strengthen the quality of the papers. A unique featureof the initiative is that all the researchers investigated their ownfield of work – abortion advocacy. This presents a number ofcomplexities such as researcher bias. Nevertheless, we wantedto break the pattern of the actors being researched by others,since the aim of the initiative is to support activists reflectingon their experiences and on the experiences of others withsimilar goals. Interviews with other actors and the process ofpeer review served to balance the authors’ subjectivity.
Phase 2: March 2001 – December 2001 aims to strengthenthe capacity of activists to undertake effective campaigns for
The Johannesburg Initiative
Advocating for abortion access
xiv
the liberalisation of abortion legislation and improvement ofaccess to abortion services by sharing the lessons learnt in phaseone. During this phase, they will also identify any need forinformation, training or resources they may have if they wantto pursue ideas generated in the workshop. These could bemet in phase 3. Phase 2 will be undertaken not only by thosewho did country-studies, but also by the additional six NGOsthat participated in Phase 1 and a number of NGOs in othercountries that are conducting abortion advocacy and are keento draw on the lessons learnt in Phase 1.
Phase 3: June 2001 – June 2002. The final phase of theinitiative will focus on mobilising resources to support countrybased activities. The different countries will identify the type ofresource they need, such as building specific advocacy skills;engaging with the media; training in coalition building andmaintenance of coalitions; building capacity to engage effec-tively with diverse religious and cultural perspectives on abor-tion; building the capacity of local lawyers or human rightsgroups to use international law; or building the knowledgebase of health activists regarding methods for safe abortionservices.. The project will support national NGOs in meetingthese needs, either through in-country expertise or throughthe international abortion rights community.
This publication marks the end of Phase one. It explores strat-egies through which activists in different countries have soughtto make abortion services accessible to women needing themand looks at factors which improve or impede advocacy foraccess to abortion services and care. The Johannesburg Ini-tiative hopes that readers will find the publication informativeand useful. In addition, the initiative is producing materials forworkshops based on this publication. It is also translating thispublication into a number of languages. For further informa-tion, please contact the Women’s Health Project.
Zanele Hlatshwayo and Barbara KlugmanWomen’s Health ProjectApril 2001
Glossary
xv
GLOSSARY
AAP Abortion Access Project
ACOG American College of Obstetricians andGynaecologists
ACT Australian Capital Territory
AIWC All India Women’s Conference
ALP Australian Labour Party
ALRA Association for Legal Rights to Abortion
AMA American Medical Association
ANC African National Congress
ARAG Abortion Reform Action Group
AWS Solidarity Election Action
BBS Bangladesh Bureau of Statistics
C.A.R.E.2000 Campaign for Access and ReproductiveEquity
CARE Campaign for Abortion andReproductive Equity
CBD Community-based distributor
CCR Citizenship and ReproductionCommittee
CESA Committee to End Sterilisation Abuse
CFEMEA Centro Feminista de Estudos eAssessoria
CMO Chief medical officer
DENOSA Democratic Nursing Association ofSouth Africa
The Johannesburg Initiative
Advocating for abortion access
xvi
DPP Director of Public Prosecutions
FEBRASGO Brazilian Federation of Gynaecologyand Obstetrics
FIDA-K International Federation of WomenLawyers, Kenya
FPACT Family Planning Australian CapitalTerritory
FPAG Family Planning Association of Guyana
FPAK Family Planning Association of Kenya
FWV Family welfare visitor
GIRE Information Group on ReproductiveChoice
GMA Guyana Medical Association
GPC Catholic Parliamentary Group
GRPA Guyana Responsible Parenthood Association
HIG Health Industry Group
HLI Human Life International
IBGE Geographic and Statistics Brazilian Institute
ICPD International Conference on Populationand Development
IMSS Mexican Social Security Institute
IWES Institute for Women and Ethnic Studies
KDHS Kenya Demographic and Health Survey
KIMET Kisumu Medical Educational Trust
KOGS Kenya Obstetrical and GynaecologicalSociety
Glossary
xvii
MCH Mother and Child Health
MCWH Mother, Child and Women’s Health
MOHFW Ministry of Health and Family Welfare
MP Member of parliament
MR Menstrual regulation
MRTSP Menstrual regulation Training andServices Program
MTP Medical termination of pregnancy
MVA Manual vacuum aspiration
NAF National Abortion Federation
NARAL National Abortion and ReproductiveRights Action League
NOW National Organisation of Women
PAC Post-abortion care
PAISM Programa de Atenção Integral emSaúde da Mulher
PAN National Action Party
PNC People’s National Congress
PPNWK Private Providers Network of WesternKenya
PPP People’s Progressive Party
PRD Democratic Revolution Party
PRG Pro-Reform Group
PRI Institutional Revolutionary Party
REDESAUDE Brazilian National Network for Healthand Reproductive Rights
The Johannesburg Initiative
Advocating for abortion access
xviii
RHRU Reproductive Health Research Unit
RHS Reproductive Health Service
RRA Reproductive Rights Alliance
SIDA Swedish International DevelopmentCo-operation Agency
SLD Democratic Left Alliance
STD Sexually transmitted disease
TBA Traditional birth assistant
US United States
USAID United Stated Agency for InternationalDevelopment
UW Freedom Union
WA Western Australia
WEL Women’s Electoral Lobby
WHP Women’s Health Project
WLRC Women’s Legal Rights Centre
WSS Women’s Section of Solidarity
NotesAbortifacient: Usually a drug or compound which causesthe termination of an ongoing pregnancy.
Cannula: Small tube or pipe for insertion into the body.
Curretage: Surgical scraping or cleaning.
D&C – Dilatation and Curretage: A procedure to emptythe uterus of its contents (usually performed for diagnostic rea-sons, to carry out an abortion or to ensure a spontaneous orincomplete abortion is complete).
Glossary
xix
Depo-provera: Injectable progestin-only contraceptive thatis highly effective for 3 months.
Dilatation: Stretching or widening an organ of the body,often used to refer to procedures to open the cervix or to allowaccess to the uterus (dilation – the noun – usually refers to theamount by which the cervix has been opened).
Menstrual regulation: Intervention (either surgical or medi-cal) to bring on a woman’s menses soon after a missed period.
Misoprostol: A prostaglandin registered in more than 80countries for the treatment/prevention of gastric ulcers.Misoprostol is also commonly used in conjunction withmifepristone (usually taken 2 days later) for medical abortion.
MVA: Manual vacuum aspiration. A procedure to empty theuterus of its contents that uses a hand-held syringe and a can-nula inserted into the uterus. A vacuum in the syringe leads tonegative pressure and the contents of the uterus are drawninto the syringe.
Norplant: Trade name of a contraceptive implant that con-sists of small silicone rods inserted in the upper arm that re-lease progestins. It is considered highly effective for 5 years.
RU 486: This is the commercial identifier for the compoundmifepristone which is an antiprogestin that is used most com-monly for medical abortion in conjunction with a prostaglan-din (see misoprostol).
xx
M E D I A I M A G E S
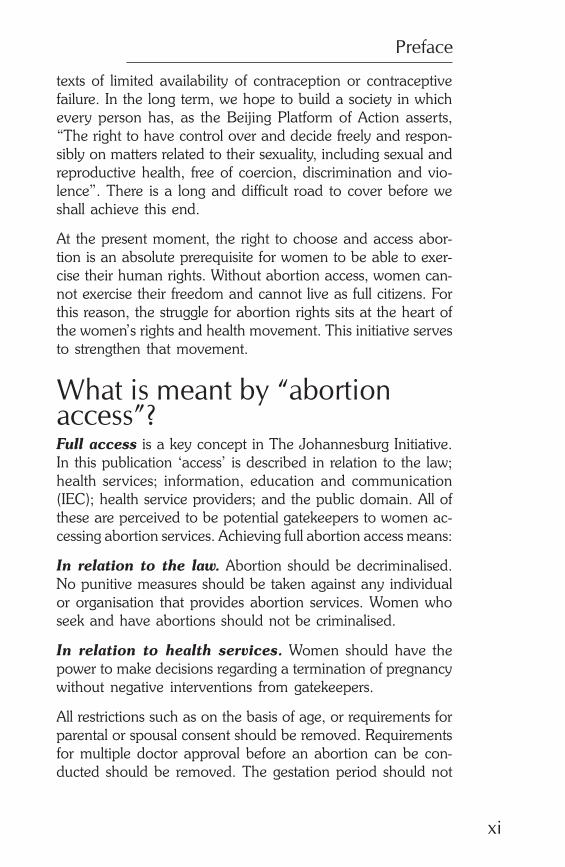
Courtesy: Cehat
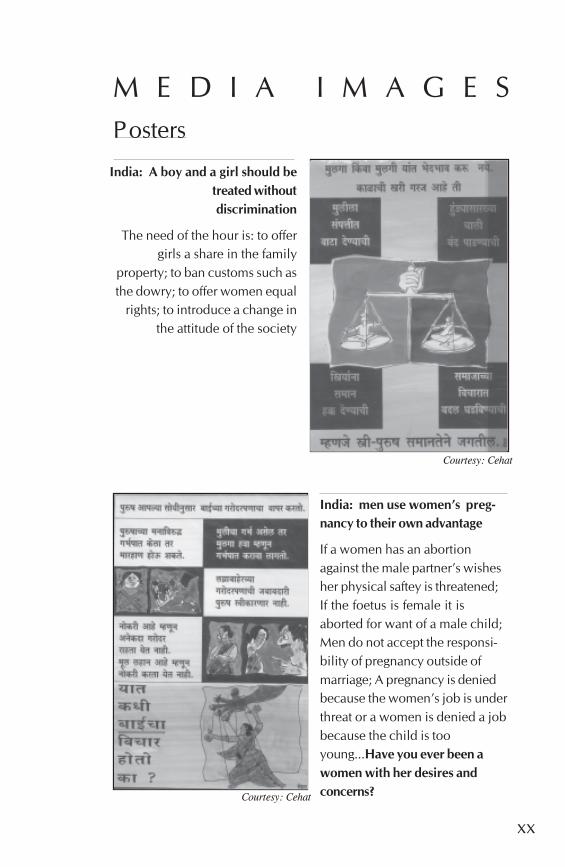
India: men use women’s preg-nancy to their own advantage
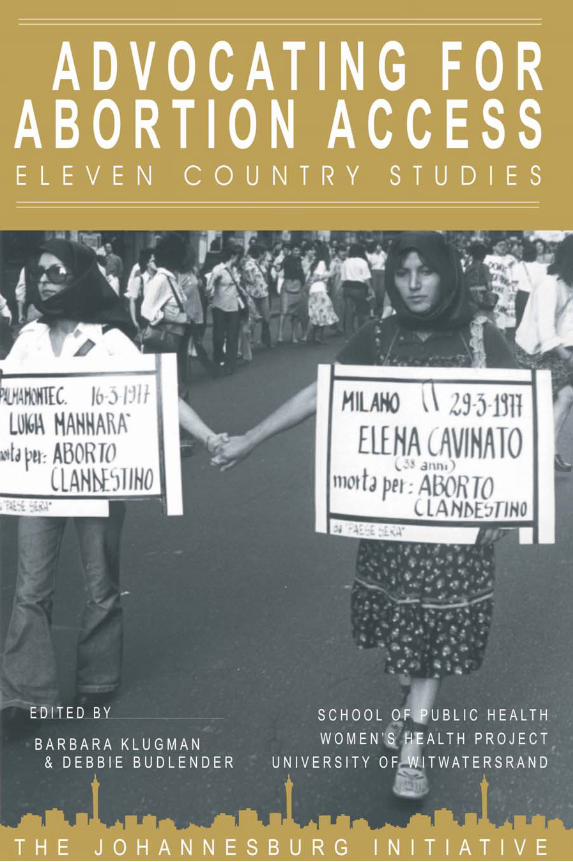
If a women has an abortionagainst the male partner’s wishesher physical saftey is threatened;If the foetus is female it isaborted for want of a male child;Men do not accept the responsi-bility of pregnancy outside ofmarriage; A pregnancy is deniedbecause the women’s job is underthreat or a women is denied a jobbecause the child is tooyoung...Have you ever been awomen with her desires andconcerns?
Posters
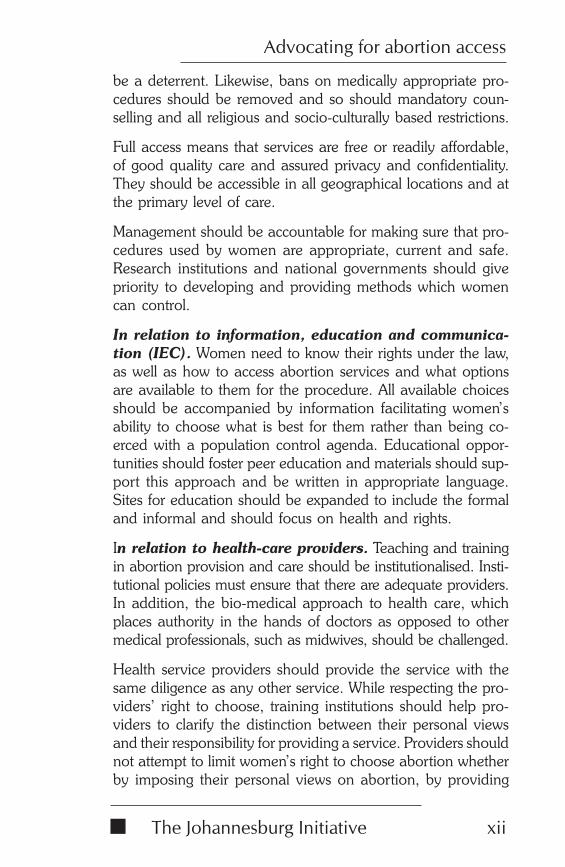
Courtesy: Cehat
India: A boy and a girl should betreated withoutdiscrimination
The need of the hour is: to offergirls a share in the family
property; to ban customs such asthe dowry; to offer women equal
rights; to introduce a change inthe attitude of the society
xxi
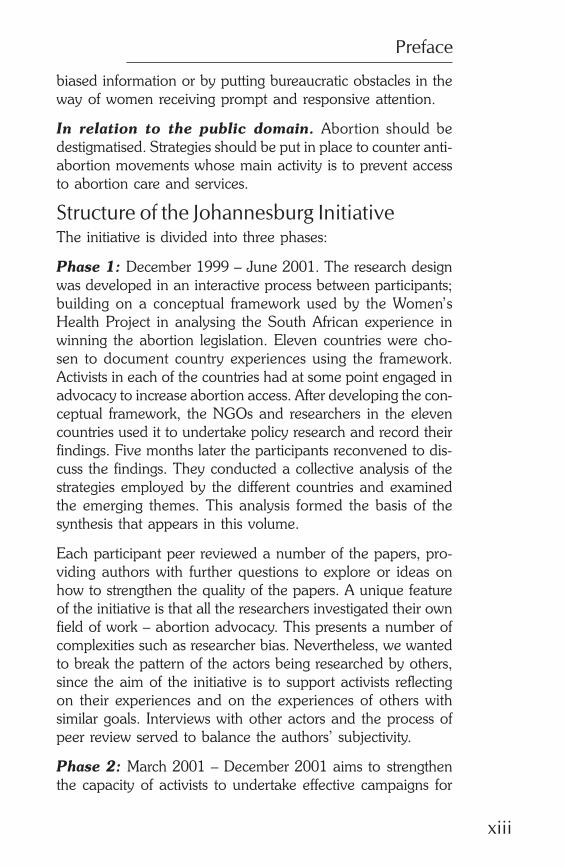
Courtesy: Abortion Access Project
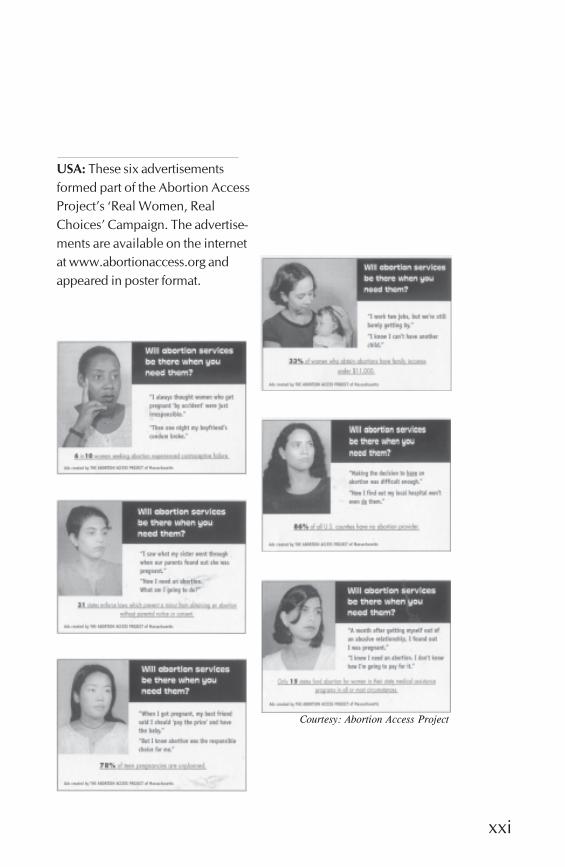
USA: These six advertisementsformed part of the Abortion AccessProject’s ‘Real Women, RealChoices’ Campaign. The advertise-ments are available on the internetat www.abortionaccess.org andappeared in poster format.
xxii
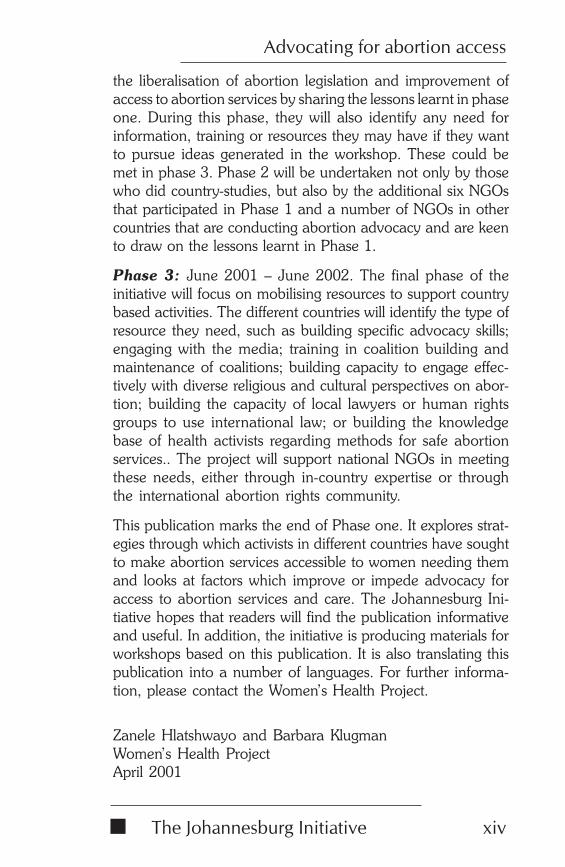
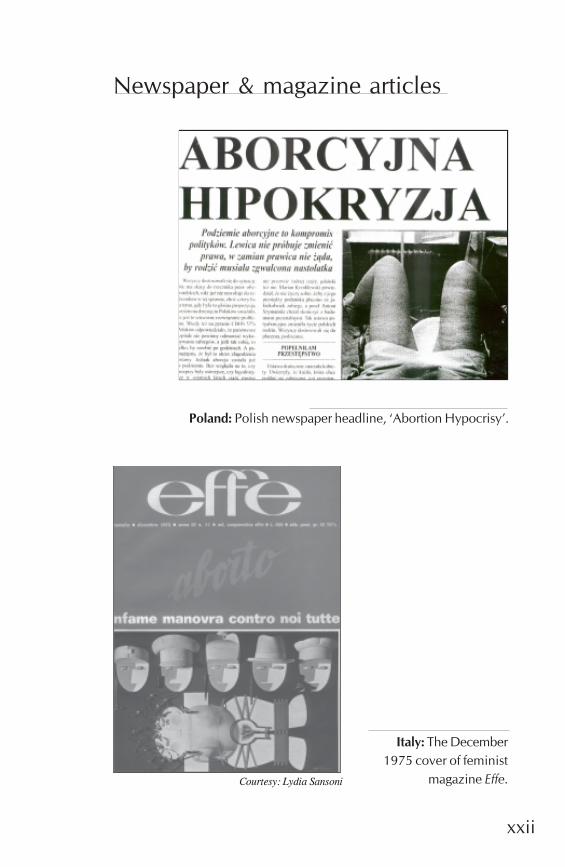
Courtesy: Lydia Sansoni
Italy: The December1975 cover of feminist
magazine Effe.
Newspaper & magazine articles
Poland: Polish newspaper headline, ‘Abortion Hypocrisy’.
xxiii
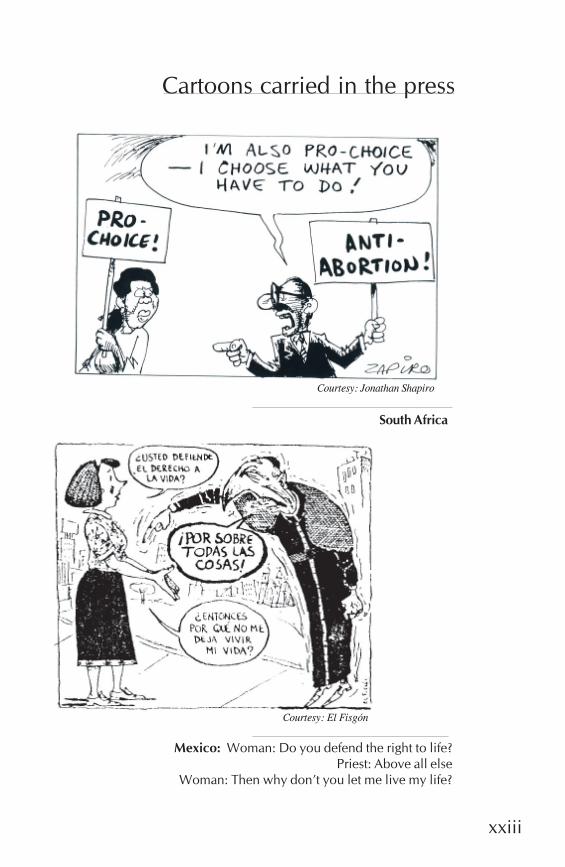
Cartoons carried in the press
South Africa
Courtesy: Jonathan Shapiro
Courtesy: El Fisgón
Mexico: Woman: Do you defend the right to life?Priest: Above all else
Woman: Then why don’t you let me live my life?
xxiv
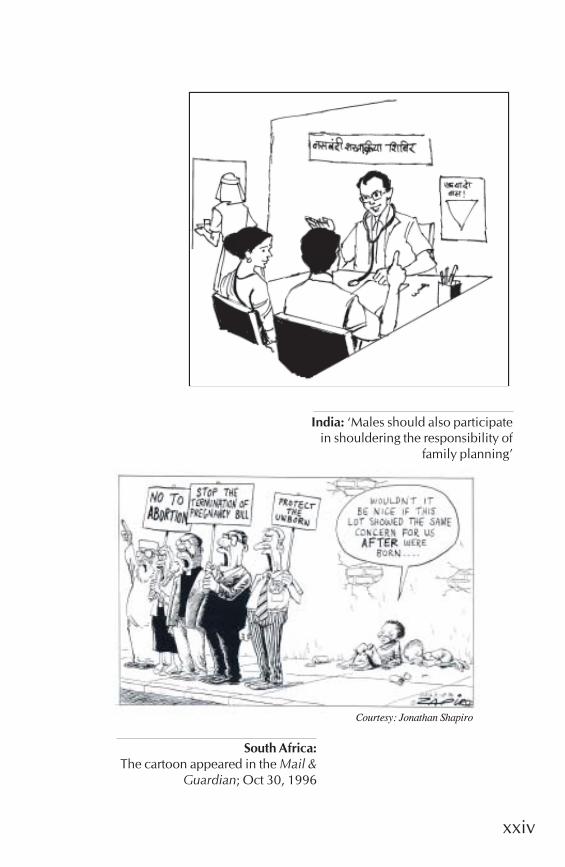
India: ‘Males should also participatein shouldering the responsibility of
family planning’
South Africa:The cartoon appeared in the Mail &
Guardian; Oct 30, 1996
Courtesy: Jonathan Shapiro

xxv
Courtesy: Jóse Hernández
Guyana: This cartoon,designed by the Pro-
Reform Group,appeared in The
Starbroek News onSaturday, May 6, 1995,
once the law waspassed.
Courtesy: Paul Harris
Mexico: “Women are toblame...They dress
indecently...How can theyexpect us not to rape
them?”
xxvi
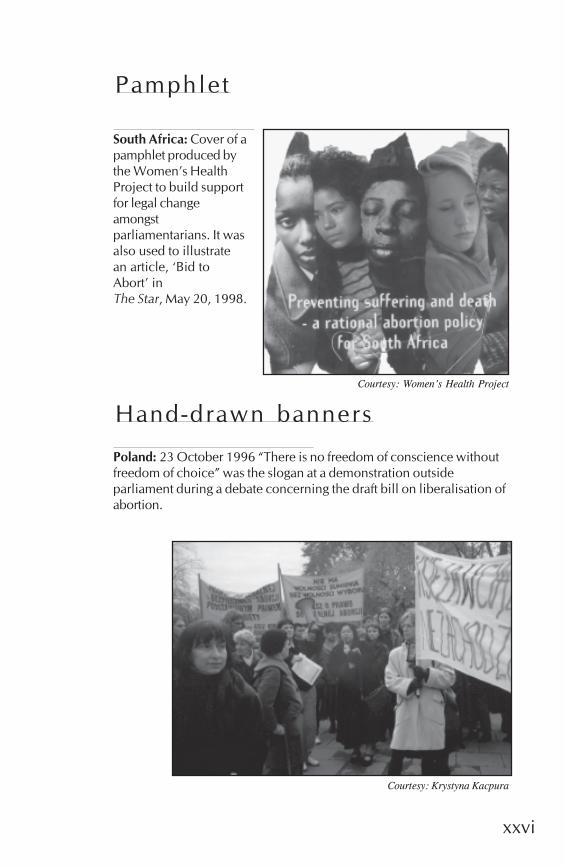
Pamphlet
Hand-drawn banners
Poland: 23 October 1996 “There is no freedom of conscience withoutfreedom of choice” was the slogan at a demonstration outsideparliament during a debate concerning the draft bill on liberalisation ofabortion.
Courtesy: Krystyna Kacpura
South Africa: Cover of apamphlet produced bythe Women’s HealthProject to build supportfor legal changeamongstparliamentarians. It wasalso used to illustratean article, ‘Bid toAbort’ inThe Star, May 20, 1998.
Courtesy: Women’s Health Project
Methodology
1
CONCEPTUAL FRAMEWORK FORANALYSING ABORTION ADVOCACY
Barbara Klugman
From description to analysisThe intention of the Johannesburg Initiative is to build capac-ity for advocacy for abortion access. The first step in this proc-ess is to learn lessons from the experience of activism in differ-ent parts of the world. In order to achieve this, the papers hadto ask similar questions, so that they would be comparable.More importantly, they had to move beyond a description of‘what happened’ to a reflection on why this happened.
The field of policy analysis provides a range of approaches toexploring how and why policies change and what factors in-fluence their implementation. The Women’s Health Project hassynthesised some of these into a framework that is presentedbelow. At the first meeting of the Johannesburg Initiative, weasked participants to identify all of the factors which have in-fluenced abortion access in their experience. We then groupedthese factors into the different components of the policy analy-sis framework – the broad contextual factors, the actors in-volved, the nature of the political process or implementationprocess and the strength or weakness of a pro-choice activistmovement. Through this process, we developed a shared un-derstanding of what questions we wanted to ask about eachcountry’s experience. By asking similar questions, we hopedto gain insights for activism in diverse countries.
In the literature, there is a distinction between analysis ‘of’ policyand ‘for’ policy. Phase one of this initiative is about analysis‘of’ policy – that is retrospectively trying to understand the fac-tors which influenced changes in law or in access to services.The purpose of the initiative, however, is to support activism‘for’ policy change – the belief that policy activism can be
The Johannesburg Initiative
Advocating for abortion access
2
strengthened through analysis. The more activists choose theirstrategies based on a thorough analysis of the factors facilitat-ing and constraining change, the more likely it is that they willsucceed in reaching their goals. Thus the aim of this initiativeis not only to analyse past experience, but to build capacity inthe methodology of policy analysis and strategic planning –identifying opportunities and barriers in advance of a cam-paign and then working out strategies to address them.
The studies in this book provide a wealth of ideas about mis-takes that can be made and strategies that can be used. Thecomparative analysis draws out some of the lessons learntacross the papers. This short paper describes the methodologyunderlying the papers – the questions the initiative chose toask in order to unravel the lessons that could be learnt fromeach country experience.
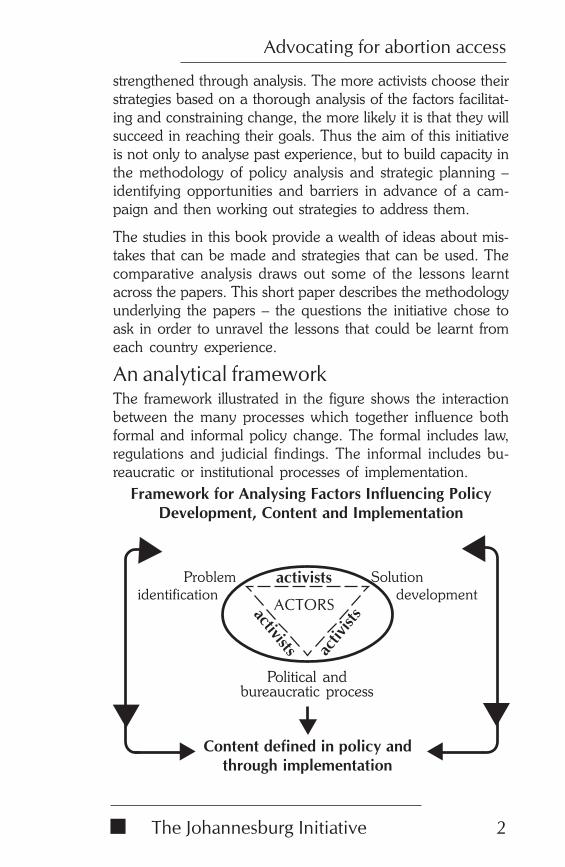
An analytical frameworkThe framework illustrated in the figure shows the interactionbetween the many processes which together influence bothformal and informal policy change. The formal includes law,regulations and judicial findings. The informal includes bu-reaucratic or institutional processes of implementation.
Framework for Analysing Factors Influencing PolicyDevelopment, Content and Implementation
Content defined in policy andthrough implementation
Solutiondevelopment
Political andbureaucratic process
ACTORS
activists
activ
istsactivists
Problemidentification
Methodology
3
The context is seen as the overarching factor influencing policyand its implementation because it shapes what is possible. Apoor economic context may account for poor accessibility ofcontraceptive services, for example, thus contributing to wom-en’s recourse to abortion. A poor economic context will like-wise make it difficult to introduce costly services. A politicaldictatorship will make it almost impossible for public activismfor legal change. A change in government might provide themomentum for activism for legal change. The existence of afunctioning public health sector may suggest a goal of provi-sion of abortion within the public health sector. If the publicsector is weak, a strategy to increase the safety and availabilityof abortions through the private sector may be more effective.Thus the context helps define the problem and shapes the typesof policy options which may be attainable.
The framework presents problem identification, solution de-velopment and political and bureaucratic processes as threeseparate spheres. The framework recognises that the world hasmany problems that never get onto the policy agenda. Indeedabortion is a good example of such a problem. Despite thefact that abortion is a major cause of maternal mortality andmorbidity in many parts of the world, some governments donot want to consider it as a policy or service delivery issue.They prefer to avoid it because they fear the political backlashfrom taking steps to address the issue.
Likewise, the world has many solutions, generated by aca-demic institutions, bureaucracies, think-tanks of political par-ties or private companies. The existence of a solution does notmean that it will be taken up by decision-makers to address aproblem. The example of medical abortions using misoprostoland mifepristone is a case in point. Despite the existence ofthis technology for some years, few governments respondedto its development by exploring how it could be registered andused to cut the costs for both health providers and women inproviding safe abortions.
Political and bureaucratic processes have their own motivat-ing forces, which may have little to do with addressing specificproblems. Concern about winning an election, for example,
The Johannesburg Initiative
Advocating for abortion access
4
may motivate a politician to take up a specific issue. A bu-reaucrat may choose not to implement or to implement onlycertain components of policy because this is easiest, or strength-ens his or her position within the bureaucracy. Policy only getsonto the agenda when the problem connects with the con-cerns of the political or bureaucratic actors.
Using this framework, the research on abortion advocacysought to identify who defined the problem, how and why?What sorts of solutions were put forward, by whom and why?What were the interests and motivations of politicians, bureau-crats and other implementers, for example health profession-als? The framework shows activists linking the three spheres.The studies asked what activist strategies were used to makethe linkages? In doing so, they also had to explore the strate-gies of those against abortion access since here, too, activistswere seeking to define the problem and solutions and to winpolitical or bureaucratic support for these. Advocacy for abor-tion access has to take account of other actors in the field, theirresources and levels of influence and power.
All of these dynamics ultimately influence the policy contentdefined in law and regulations and through implementation.The framework illustrates this interaction and serves as a re-minder to policy researchers of the diverse issues they need toexplore in order to understand how and why change comesabout. The two-way arrows around the framework are thereto remind us that this is not a linear process. No sooner has alaw been made than new problems emerge about whetherand how to implement. Diverse solutions may be available,but what decides which, if any of these, are taken up?
By unravelling strategy in this way, activists can ensure thattheir targets, messages and solutions are clear and realistic atany particular time, given the range of forces at work. Theconceptual framework serves as a model to remind activists ofthe range of factors which influence change. It helps both inanalysing what has happened and why and in preparing forfuture advocacy, strengthening the chances of its success.

Methodology
5
ReferenceThe conceptualisation of problems, solutions and the politi-cal and bureaucratic process as separate spheres is adaptedfrom Kingdon, J, Agendas, Alternatives and Public Policies,United States: Harper Collins, 1995.

The Johannesburg Initiative
Advocating for abortion access
6
Comparative Analysis
7
STRATEGY AND ACTION FORABORTION ACCESS: A
COMPARATIVE ANALYSIS
Barbara Klugman and Zanele Hlatshwayo1
Women’s Health Project
The papers in this collection demonstrate the enormous diver-sity of advocacy strategies for promoting abortion accessthroughout the world. The ways in which activists have de-fined the problem, the goals they have established, and themethods they have used to achieve these are diverse and in-novative. Yet the differences are seldom there by chance. To alarge extent, the options available to activists have been shapedby the context in which they find themselves. This article ex-plores why activists took up different strategies and under whatconditions these were effective.
None of the countries included in this compilation haveachieved full abortion access. For this reason activists fromthese countries, as well as from others not represented in thisbook, can continually learn from one anothers’ experiences.Also, the descriptions of each country’s strategies are based onan analysis by activist researchers and those they interviewedin each country. They therefore cannot be seen as compre-hensive or the only possible view. The issues drawn out ineach paper and in this synthesis are shaped by activists’ per-ceptions of what is interesting and worth sharing from theircountry’s experiences.
1We would like to acknowledge inputs from participants in theJohannesburg Initiative both through our collective analysis at oursecond workshop and specific responses to earlier drafts of this paper.

The Johannesburg Initiative
Advocating for abortion access
8
A goal to match to realisticoptionsWhile the ultimate goal is full access, as defined in the prefaceto this book, this is very difficult to achieve. Its achievementrequires long-term commitment and many different phases.Sometimes victories are lost, so it can be a case of movingforwards and backwards. Thus in Poland a liberal abortionlaw was in place, then lost, then won, then lost again. Eachdevelopment was linked to a change in political party, so thefocus is currently on winning legal reform. In contrast, therehas been a liberal abortion law in India for decades, but withlimited access. Indian activists are focusing on seeing the lawimplemented by ensuring access to quality services. In Brazilthe law limits access in the case of rape or maternal risk, soactivists are focusing on making abortion available to the ex-tent of the law, since even that is not available at present. Theymeanwhile retain a longer-term goal to improve the law. Theseexamples show that one cannot assume that the first goal willbe liberalisation of law, followed by efforts at implementation.
In some cases a number of different goals are being pursuedin one country at the same time, sometimes by different group-ings, sometimes by single groupings operating a multi-prongedstrategy. In Kenya for example, the focus for some is on equip-ping private sector providers to perform safe and cheap abor-tions despite the illegality. For others it is on improving thequality of post-abortion care in public health institutions. Inthe United States of America (USA) one focus is to hold ontothe legal rights which are under threat. Another is to improveaccess for poor women and women of colour by changingfunding regulations, health professionals’ attitudes and otheraccess oriented strategies. Likewise in South Africa, while somegroups are focusing on holding onto the law which is beingchallenged in the constitutional court for the second time, oth-ers are focusing on building clinical skills and yet others onstrengthening the capacity of the public health system.
Hence the goal of abortion advocacy is to some extent framed
Comparative Analysis
9
by the context in a particular country at a particular time.However, it also reflects activists’ priorities and their under-standing of the problem.
Framing a messageControlling women or women controlling theirbodies?This raises questions about how the problem should be framed.Studies in different countries show very diverse approaches todescribing the problem and hence the goal. This is shapedpartly by the overall ideological environment – how other so-cial players are or are not addressing the issue of abortion.The pro-choice position argues women’s right to control theirfertility and thus makes access to abortion an issue of humanrights and choice.
But this presentation of the problem can be inadequate orconfusing, especially in a context where other groupings areproposing fertility control for demographic purposes. India isone example where abortion is legal, not because of any re-productive rights ideology, but rather because of a desire bothfor population control and to reduce maternal mortality. Forthis reason, pro-choice activists have difficulty winning sup-port from mass-based organisations for working on abortionaccess as abortion is linked in people’s minds with the govern-ment’s population control strategy.
Other countries show similar dynamics. The USA case, forexample, illustrates how black women activists found it hardto take on pro-choice activities when a range of populationcontrol oriented policies, including sterilisation programmes,have undermined their control over their bodies. To supportabortion in this context meant having to simultaneously chal-lenge a population control ideology. The paper describes howthe failure of many feminists to distance themselves from thosewho support eugenics has deepened racial divisions withinadvocacy movements. While groups focusing on the legal rightto abortion use the language of ‘choice’ and ‘privacy’, they
The Johannesburg Initiative
Advocating for abortion access
10
frequently do not take on problems of access even within thelaw, such as the removal of funding obligations for abortion.As a result, they communicate only with those who have somedegree of choice and fail to build a support base amongst themajority of women.
The concept of ‘choice’ is itself open to interpretation. In In-dia, many women have resorted to sex-selective abortions,which both reflect and reinforce the low value of women inIndian society. Thus abortion is used to perpetuate gender in-equality. Some of those favouring the right to sex selectionframe it as a women’s choice issue, subverting the feministdemand for women’s right to choose. In order to win supportfor advocacy to increase abortion access, pro-choice activistswould also need to address the issues of sex selection and ofpopulation control.
The concept of choice has also been used by those opposingthe right to abortion. In Mexico, anti-choice activists arguedthat abortion was part of an international population controlcampaign and should therefore not be supported. Likewise inPoland, anti-choice groupings used the country’s declining birthrate as an argument against abortion. Carrying this further,they compared abortion with concentration camps and be-trayal of the Polish nation, drawing on powerful emotionaland psychological forces in the creation of a post-communistPolish nation.
Thus the traditional call of abortion rights activists – the call forwomen’s right to choose – hides many complex questions andmay not be an adequate argument to mobilise women’s sup-port. It may, on the one hand, be subverted by those againstreproductive rights. On the other hand, it may be inadequateif it focuses only on the legal right to choose and not on all thepractical obstacles to abortion choice such as availability, costsand quality of services.
Moral debate or data driven public healthdebate?Another obstacle to the ‘women’s rights’ argument in manycountries is the prevailing view that the national morality, as
Comparative Analysis
11
represented in ‘tradition’ or ‘culture’, is against abortion. Thisis is a relatively new view. In countries as diverse as SouthAfrica and the USA abortion was carried out for generationswithout any legal interference until roughly the middle of the19th century. Over the past century religion, particularly Ca-tholicism, has become an organised force against abortion.(Unfortunately, the absence of more papers from countries withan Islamic tradition means that the force of Islam as a socialinstitution has not been adequately covered in this collection.)Yet the papers show that this force is not always all-powerful.The Polish case illustrates how abortion was not a politicalissue under communism and their liberal 1956 law was takenfor granted by the Catholic population. Likewise, the religioussector did not raise any objections to the passing of a liberallaw in India. In Kenya, by contrast, where only 28% of thepopulation is Catholic, the church exerts a disproportionateinfluence on reproductive health policies. The paper describeshow some potential opposition to abortion services by churchleaders was prevented when providers made clear that theyhad performed services for family members of religious lead-ers.
In particular, where there is not a clear divide between churchand state or where the church has supporters in key institu-tions of state, such as parliament, education structures or themedia, religious institutions become a much more powerfulforce in undermining access to abortion. This is specificallyillustrated by the Polish and Mexican cases. In contrast, theItalian case illustrates how the ideological force of feminismand socialism in the 1970s, coupled with women’s limited ac-cess to contraception and increased desire to control fertility,collectively undermined the power of the catholic church whichhad, until then, prevented access to both contraception andabortion. This shows the importance of pro-choice activiststaking account of and trying to influence the cultural and ideo-logical context.
Organised religion and related anti-choice lobbies have some-times mounted an ideological attack against the ‘women’s rightto choose’ position by presenting themselves as being at the
The Johannesburg Initiative
Advocating for abortion access
12
forefront of concern for women’s rights and health. The Aus-tralian case describes anti-choice health professionals arguingfor anti-choice information to be given to pregnant women inthe name of ‘informed consent’ in order to position themselvesas being concerned about women’s well-being and not onlyabout foetuses. They likewise promoted the concept of ‘postabortion syndrome’, which claims that women suffer long-termpsychological distress after an abortion. They did this despitethe lack of scientific evidence for this concept. These terms areused in an effort to define the problem in an apparently neu-tral way by using pseudo-medical terminology and in terms ofmeeting women’s needs. The strategy is often sophisticatedenough to confuse an audience and hide the fact that group-ings are against abortion under any circumstances. Similarly,such language has been introduced into Polish official language– the word ‘conceived child’ has replaced the word foetus inthe Polish Criminal and Civil Codes and a pregnant womanhas become a ‘mother of a conceived child’.
These experiences reinforce the need for pro-choice activiststo frame their messages in ways that resonate with the publicat large. It has led many to move from a ‘rights’ and ‘women’schoice’ platform to a public health platform which can be sup-ported by data. Thus in Guyana, instead of describing the prob-lem as one of women’s lack of reproductive choice, activistsframed it entirely in public health terms. Using data as thebasis of their approach, they argued that a liberal abortion lawwould reduce the number of abortions, improve women’shealth and save public health resources that were being spenton treating victims of unsafe abortion. South African activistsinitiated research into the costs and public health impact ofunsafe abortion as a means of focusing the debate away fromquestions of morality. At the same time, they identified keystakeholders who challenged the idea that abortion was againstAfrican tradition and provided historical evidence and per-sonal testimonies to the contrary. They also ensured that pro-choice religious figures spoke in favour of liberalised abortionlaw, thus developing a mix of messages to address the diver-sity of anti-choice arguments. In contrast, Brazilian activists
Comparative Analysis
13
have moved from a health message to the right to citizenship,reflecting their recognition of openings in the political discourse.
These cases illustrate strategic approaches to the public fram-ing of a problem and its possible solutions that take account ofthe contextual environment and shape messages which aremost likely to overcome obstacles to change. In all cases theoverall aim of activists is the same, only the approach differs.
Windows of opportunity forchangeA number of the case studies illustrate how major social up-heavals or specific moments in history can play a significantrole in facilitating or undermining abortion access.
National eventsSpecific events have directly influenced national willingnessto change abortion laws. In South Africa the arrival of democ-racy created a moment in time when politicians wanted todemonstrate their commitment to gender equality, to endingrace discrimination and to public health. A new bill of rightswas developed which insists on gender equality and on theright to health, including reproductive health. This created aclear window of opportunity for activists to mobilise for liber-alisation of the abortion law. In Bangladesh, the mass rape ofwomen by the army during the War of Liberation led govern-ment to facilitate access to abortion despite its illegality. Bydoing so, it shifted the national approach to abortion and laida foundation for activists to introduce services that continueuntil today. The victory of Solidarity in Poland and the asso-ciation of the Catholic Church with this victory at the sametime as a Pole became Pope, created an ideological link be-tween religion and freedom from communism. As a result, acountry and medical profession that was previously comfort-able with abortion suddenly reframed itself as anti-abortion,thus closing down both abortion access and opportunity forpro-choice activism.
The Johannesburg Initiative
Advocating for abortion access
14
ElectionsElections are a key moment when politicians are vulnerableand may open or close opportunities for activism. In the caseof Guyana, an anti-abortion rally discouraged Cabinet fromapproving an abortion law prior to the elections for fear oflosing electoral support. In a Mexican example, a pro-choiceparty would not put forward liberal legislation for fear of influ-encing their chances in the presidential elections. After losingthose elections, however, they were willing to introduce thechange in the one-month window in which their party wouldmaintain the majority in the house. In Brazil, abortion servedas the key difference in the municipal elections. The Braziliancase shows how a strong public pro-choice movement can helpa candidate on an abortion rights platform win votes, as hap-pened with a feminist candidate during the Sao Paulo Cityelections.
An election can also change the national climate. In the caseof the USA, the election of a pro-choice President created op-portunities for expanding abortion access. It also led someactivists to focus on the federal level. The recent return of ananti-choice President puts pro-choice activists on the defen-sive again and removes the possibility of successful activism atthe federal level.
All activities around changing abortion law or service provi-sion take place within specific contexts as described above.Activists, whether pro- or anti-choice adopt their strategies onthe basis of the opportunities or barriers established by thecontext. Windows of opportunity open and close. The impor-tance of being prepared so as to take advantage of opportuni-ties like these emerged repeatedly as a lesson for activists. Boththe Australian and Mexican cases show how activists had gath-ered the necessary information and built their coalitions andthe like, so that when opportunities arose they could take ad-vantage of them. The Brazilian case shows how activists madeabortion access an election issue, with positive results. In otherstudies pro-choice activists have not been able to shape thedebate, and have had to be responsive instead because anti-choice activists had made abortion an election issue.
Comparative Analysis
15
Choice of strategy to achieve aspecific goalOnce the specific goal of abortion advocacy is clear and themessage resolved, there remain diverse options for strategies.One of the questions is whether there are opportunities to con-duct advocacy within the political or bureaucratic / institutionalsystem and whether these are likely to achieve the desired goal.Alternatively, is working from the outside, or from a positionof opposition to the existing political or bureaucratic system,the better option, or indeed the only option?
Working from the inside: the political systemNot all activists are in a position to work from within the sys-tem, but where the context has made this possible, there havebeen substantial victories.
Opportunities for civil society interventionThe nature of the political system to some extent shapes op-tions for activism. The extent to which the political system al-lows civil society engagement will determine strategic options.In Italy, for example, citizens can compel parliament to debatea bill by gathering 50 000 signatures. In South Africa there arepublic hearings in parliament at which individuals and organi-sations can present their views. Interest groups in Brazil canpresent their perspectives in the Senate and House of Repre-sentatives where the principle of hearing both sides ensuredthat, for example, the pro-choice organisation Catholics for aFree Choice gained a platform when the church hierarchyspoke.
In some countries political party members can vote accordingto their individual beliefs. In others they must vote with the party.In certain cases, the approach changes, depending on the is-sue. This ruling can determine the success or failure of pro-choicelegislation. In the South African case, for example, substantialactivism went into ensuring that those in the ruling party de-cided that its members of parliament had to vote en bloc, sincethis guaranteed the passing of the liberal abortion bill.
The Johannesburg Initiative
Advocating for abortion access
16
Location of policy-makingThe site of activism ‘within the system’ will also be shaped bynational law. Abortion laws in Australia, for example, are de-fined at state rather than federal level and it is here that activ-ism must occur. Thus activists need to understand the struc-ture of political decision-making and the nature of the policy-making process in order to work out where and how to inter-vene.
Orientation of political leadershipThe existence of one or more political parties that are explic-itly pro-choice or which are at least not expressly against it isoften an important determinant of whether or not abortionlegislation can be liberalised. However, a pro-choice perspec-tive does not guarantee that politicians will choose to addressabortion. Election support and internal party dynamics seemto be of greater significance. Nevertheless, where someone whois part of the women’s movement or pro-choice movementbecomes a politician, they are frequently able to play catalyticroles because of their location ‘on the inside’. The Australiancase, for example, describes how a member of parliament,who was also a long term member of a pro-choice group, putforward a repeal bill to remove anti-choice legislation. On theother hand, anti-choice parliamentarians can prevent pro-choice legislation or put forward restrictive legislation, as boththe Mexican and Polish cases illustrate.
Activists supporting politiciansWorking on the inside does not always require having pro-choice activists who are parliamentarians or other official de-cision-makers. The South African case illustrates the advan-tage of activists and the ruling party having close relationshipsso that activists can help shape the parliamentarian’s consulta-tive strategies, reports and monitoring systems.
Working from the inside may require compromises and cancreate very complex dynamics for pro-choice activists. TheAustralian cases illustrate the advantages and difficulties ofworking with pro-choice parliamentary political leadership. A
Comparative Analysis
17
close relationship between pro-choice activists and pro-choiceparliamentarians allowed the activists to understand the sys-tem and identify both opportunities for advancing and timeswhen compromise was necessary. On the other hand, someactivists felt that an alliance with those inside the political sys-tem sometimes resulted in unnecessary compromises.
The Mexican case illustrates the complexity of operating onthe inside and outside at the same time. In one situation, ac-tivists succeeded in getting four of a package of five women’srights proposals to be presented to the parliament by an alliedlegislator. The legislator excluded the fifth proposal, that onabortion, with the knowledge and consent of advocates. Inthe meantime, activists demonstrated their support outside theparliament building, leading to confusion among parliamen-tarians inside who thought that the controversial abortion pro-posal was also being presented. The legislator was obliged toretract the presentation of the proposals. This seriously dam-aged relations between activists and their allies from the strong-est pro-choice party.
Working from the inside: the bureaucraticsystemLiberal law does not guarantee implementation. The natureof the health system and the scope for control within the bu-reaucracy are additional and important variables. Moreover,even when a law allows for abortion in limited circumstances,these provisions may not be implemented and abortion maynot be readily available. For this reason, advocacy for serviceprovision may have to be a goal in itself.
Location of decision-making in health systemWhere political leadership directly controls the health system,politics can directly influence whether or not abortion servicesare implemented. This can be seen in the greater provision ofabortion services in states with democratic city government inBrazil.
Where decision-making resides at the level of service man-agement, greater opportunities exist to lobby that level. In these
The Johannesburg Initiative
Advocating for abortion access
18
cases, success is likely to depend on the personal views of thehospital board or manager. The Bangladesh case describeshow the senior decision-maker within government supportedthe menstrual regulation initiative and how this played a deci-sive role in its acceptance. The USA paper illustrates positiveexamples of hospital-level activism to improve access. It alsoillustrates, however, that local level service providers can bethe focus of attention for anti-choice activism, with pro-choiceactivists finding themselves having to defend existing services,rather than being able to extend them. Guyana shows publichealth hospitals refusing to make decisions at hospital level toprovide services. They did this on the basis of the lack of clearinstructions from the Ministry, despite clear legislation. TheSouth African case shows an internal contradiction within thehealth system where those responsible for implementing abor-tion policy – Maternal, Child and Women’s Health (MCWH)programme officers – are not in charge of managing serviceprovision so they cannot insist on implementation. These ex-amples illustrate how the target of advocacy needs to be cho-sen based on an understanding of both the nature of the deci-sion-making structures and the perspectives of decision-mak-ers.
The Brazilian paper illustrates how much can be achieved inwinning positive women’s health policy, technical guidelinesfor service provision and high quality services when the abor-tion advocates are employed in management roles within thepublic health system. The activist strategy of ensuring that theywere positioned in this way and then bringing on board moresympathetic health professionals as volunteers, has allowedinstitutionalised changes in the public health system – althoughonly in specific geographic areas. The sites of high quality serv-ices are now being used as a model for service guidelines else-where in the country. This strategy has been backed by majornational mobilisation for legal change.
Bringing health providers on boardOne of the difficulties with advocacy from the inside is that thebarrier to service provision may not be somewhere in the sys-
Comparative Analysis
19
tem that can be targeted for advocacy. It may be at the level ofthe individual providers. Whatever the law, health profession-als play a critical role in interpretation. The Kenyan case studydescribes how certain health professionals do not provide abor-tion to the extent that the law allows. The Italian case showsdoctors choosing to make women wait a week after first re-questing abortion, despite the fact that this is not a require-ment. Alternatively, they use the conscience clause to refuse todo abortions when they are overwhelmed by the demand,rather than for actual reasons of conscience. The Indian caseshows doctors demanding husbands’ consent when it is notlegally required. In contrast, the Australian case shows doctorsand clinic staff actively resisting legal requirements to showpictures to women of stages of foetal development when ob-taining informed consent for an abortion.
These examples raise questions about what types of advocacymight influence health providers’ attitudes. The Kenyan caseshows an NGO initiative that wins doctors’ and nurses’ enthu-siasm and commitment to provide safe services despite theillegality. The Indian case shows an advocacy interventionbased on research that brought together both health providersand the state administration, getting both involved in identify-ing opportunities for improving quality of care. The USA pa-per illustrates an initiative to engage with medical students whilestill in training to win their understanding of and commitmentto provide quality abortion services. In these initiatives ‘work-ing from the inside’ implies working with providers, but notnecessarily only within a public health system. These initia-tives work within the private sector too.
Partnerships to increase public health accessA number of the country studies on increasing service accessdescribe partnerships between government, NGOs and theprivate sector, sometimes with the support of donors. Whilethe dynamics of partnerships are always complex, they pro-vide innovative ideas about what is possible. In the Kenyancase, while the network of providers was established as an NGO,many of the providers worked in the public health system and
The Johannesburg Initiative
Advocating for abortion access
20
the government-run teaching hospitals hosted the training. Inan effort to ‘mainstream’ this experience, another NGO hasworked with the National Nurses’ Association of Kenya to ex-tend post abortion care services to rural areas. In addition, theMinistry of Health has reviewed its policies and regulationsand is now planning to train mid-level providers in post abor-tion care in all district hospitals. In this way, an initiative thatbegan on the outside has impacted on the system as a whole.In the case of Bangladesh, NGOs conduct the training of bothgovernment and private practitioners and government man-ages the entire system.
The key challenges in these cases appears to be where owner-ship and control lies and how to ensure that all parties believethat their own goals are being met through the partnership.The value of partnership is that it draws on the strengths ofdifferent players, without which services would often not bedelivered. As illustrated in the South African case, however,NGO partnerships with government and donor support forpublic health initiatives can reinforce tendencies towardsverticalisation – failing to integrate abortion services with otherprimary care services and hence limiting the overall healthsystem’s responsibility for abortion service provision.
These examples illustrate advocacy strategies that work fromboth outside and inside. In many cases, working ‘on the out-side’ is done as a means of bolstering efforts of those insidethe political system or bureaucracy. This is discussed in thefollowing section.
Working from the outsideIn some situations pro-choice activists have no points of ac-cess to the political or bureaucratic systems. There are no win-dows of opportunity. In this situation, activists have to operatetheir strategies outside of these formal structures. Again thereare strategic choices to make in this space, depending on thesocial and political context and the range of interest groups,the extent of opposition and other factors specific to each coun-try and each moment in time.
Comparative Analysis
21
Even where activists are working from within, they, or othersworking towards the same goal, may also operate strategiesfrom the outside.
Popular mobilisation to pressure for changeA number of country studies illustrate how public mobilisationplayed a key role in achieving intended goals.
In the case of Italy, mass mobilisation in the 1970s aimed atliberalisation of the law. After a successful challenge to theCatholic Church on divorce, the women’s movement consoli-dated around abortion. Women networked in collectives atgrassroots level throughout the country, without centralisedleadership but with the clear goal of winning abortion reform.Because of this mass-based approach, they were able to mo-bilise demonstrations of up to 50 000 people and collectenough signatures to bring a bill to parliament. Women in tradeunions joined up with them and left wing political parties feltpressure from their women members and ultimately succumbedin order not to lose this constituency. One of the parties – theCommunist Party – was in a conservative coalition with theChristian Democrats and closed parliament rather than allowthe abortion debate. But within a few years the pressure wastoo much and they conceded. The mobilisation took placeover a decade. At first contraception advertising was legalised,then contraceptives were made available and family healthcounselling centres established and, finally, voluntary termi-nation of pregnancy legalised. Such was the strength of themovement that when the pro-life movement held a referen-dum against the new law, 68% of votes were against abolish-ing it. This illustrates that mass mobilisation can impact di-rectly on legislation, but its depth and tenacity are critical.
Context also played a role in the success story. The collision offeminism with Catholicism occurred in a social context wherepeople wanted greater control over their fertility and contra-ceptives were not available. Many families saw the negativeimpact of women having to seek and undergo unsafe abor-tion. Thus the moment was right and the women’s movement
The Johannesburg Initiative
Advocating for abortion access
22
gave voice to what had become widespread public opinion,thereby challenging one of the fundamental institutions ofpower in the country – the Catholic church.
In the Brazilian case, mobilisation aimed firstly at the creationand extension of quality services within the limits of the law.Secondly, it aimed at building legitimacy for public debate onabortion to create an environment conducive to legal reform.Rather than building a grassroots movement, NGO activists inthe feminist movement targeted diverse sectors in order to buildwide ranging support for change. The sectors included profes-sionals in health, law, education and communication, as wellas the public at large. The activists used seminars, debates,public hearings and the media. The strategic nature of the Bra-zilian goal – to improve services within the limits of the lawwhile simultaneously creating an enabling environment forabortion discussion as a precursor to working for legal reform– is helpful in recognising that in countries where there is deep-seated opposition to abortion rights, it may take many yearsto achieve broad access. In these circumstances, short termstrategies should aim to change these contextual factors. Thestrategy of feminist groups in Brazil recognises that society keepsabortion hidden and that the first step in a long-term strategyis to bring it into the public eye.
In the case of the USA, mobilisation was used to gain legalabortion in the first place. Some groups are currently mobilis-ing individuals and communities for the goal of ensuring fi-nancial access to abortion for poor women. Over the years ofstruggle a number of different mobilisation strategies have beenused. These include grassroots organising in Congressionaldistricts to lobby members of Congress to motivate the state topay for abortions, a strategy which was coupled with winningthe support of five female senators for this issue. This cam-paign created links between pro-choice groups and those work-ing on economic justice for women. At this stage it has influ-enced a number of appropriations bills to allow funding forabortion in case of rape, incest or danger to the life of themother. The Hospital Access Collaborative supports commu-nity-based activism to convince hospitals to change their rules
Comparative Analysis
23
and procedures, including increasing hospital based abortionservices. Another mobilisation strategy towards this goal is theNational Network of Abortion Funds which has more than 77grassroots-based groupings in local communities in 36 statesthat provide direct assistance to women in need and advocatefor public funding of abortion. A further mobilisation goal inthe USA is to build community-level activism to protect abor-tion clinics and providers against violence. There are initia-tives to this end, for example, to build student and youth net-works.
The existence of a mobilised public voice for abortion accessstrengthens other forms of advocacy. For example, if politi-cians are aiming to liberalise law or if service managers wantto include abortion amongst their services, it is easier for themto challenge their opponents when they can show that there ispublic support for their position. There are many barriers topopular mobilisation for abortion rights, however. A numberof cases argue that poor economic contexts are not conduciveto pro-choice activism. Whether in Kenya or India, women’srights activists have tended to focus more on issues of eco-nomic empowerment or political participation. Within indi-vidual countries, abortion rights are more likely to be the focusof attention of middle-class groupings, despite the fact that it ispoor women who are most likely to suffer from limited legalaccess or the high costs of services and therefore resort to un-safe abortions.
In addition, those directly affected by the need for abortionmay well feel unable to speak publicly on the issue in order toprotect their privacy or because of their sense of shame ortheir fear of legal or family repercussions. Thus the economicand cultural context may influence the capacity of pro-choiceactivists to mobilise a broad constituency of support, particu-larly of those who are poor, from an ethnic minority or other-wise marginalised. In these contexts, strategies that link abor-tion rights to broader demands, whether for health services ingeneral or for full citizenship for all women, may have a widerappeal.
The Johannesburg Initiative
Advocating for abortion access
24
Providing alternative services or securing fund-ing for services.A number of country studies contain examples of service pro-vision outside of a public health system or the private ‘for profit’health sector. These are often referred to as abortion‘undergrounds’. They involve women learning abortion skillsfor themselves and, in this way, ensuring that poor womenhave access to safe services. This is described in the early his-tory of abortion activism in the USA and Italy. The other formof ‘underground’ strategy is setting up of networks to providewomen with information about where to get legal abortions inother countries, where to find sympathetic doctors who will dosafe abortions despite their illegality and, in some cases, pro-viding funds to women who cannot afford abortions so thatthey can pay for them in the private sector or travel to otherstates or countries where they are legal or safe.
The balance between organisationalmobilisation and individual agencyWhile it is frequently assumed by activists that mass mobilisa-tion is a requirement for success, a number of country studiessuggest otherwise. In particular, charismatic leadership canprovide the catalyst role.
In the Kenyan case, the problem identified was the high levelsof maternal mortality and morbidity from unsafe abortion inthe context of a deteriorating public health system as a resultof structural adjustment policies. In this context, activists real-ised that the public health system would not provide a goodentry point for attempting to provide abortion services. Moreo-ver, abortion is illegal except on ‘grounds of necessity’ andactivists, who were themselves doctors, did not see any shortterm likelihood of being able to challenge the law. The gov-ernment was, however, committed to providing post abortioncare. For these reasons, the solution identified by activists wasto train and build the willingness of health professionals, in-cluding nurses, in the private sector to provide safe services,stretching the definition of the law to its absolute limits. Themessage of ‘post abortion care’ could be used to create a ve-
Comparative Analysis
25
neer of legality to the initiative. In addition, realising the great-est problem was amongst poor women, the organisers includeda requirement that providers not turn poor women away, or atleast refer them elsewhere.
The primary strategy used to achieve this goal was charismaticleadership by a key figure in the gynaecological establishmentin Kenya, coupled with winning commitment from interna-tional donors to support the rather risky initiative. The leader-ship figure was well placed to make institutional decisions suchas introducing training in manual vacuum aspiration at a na-tional teaching hospital. As the chairperson of the Kenya Medi-cal Association, the leader influenced the views and approachof health professionals.
The Guyana case likewise demonstrates the role of charismaticleadership in forging alliances across ideological positions, inthis case for legal reform.
In both cases, the shifting role of the charismatic leadershiphas influenced the impact of the intervention. In Guyana, with-out an active advocate for implementation of the new law, thevarious mechanisms established for this end have not takenon their allocated tasks. The Advisory Board established tomonitor whether access to safe abortions ultimately leads toreduced figures for abortion has not analysed the availabledata nor used it to address gaps and problems in provision. InKenya, the new leaders of the Medical Association do not haveformal links with the abortion initiative, so the Association hasnot played a role in advocacy for the growth and expansion ofthe network since the initial advocate left this position.
While these are extreme cases of the role of charismatic lead-ership, most of the country studies illustrate the importance ofagency – the initiatives of one or two NGOs and, by implica-tion, of individuals within these – in developing advocacy ini-tiatives, building a support-base for them and maintaining themover time. Whereas grassroots mobilisation is not necessarilya prerequisite for achieving abortion access, in all cases barIndia, individual or NGO tenacity appears to have been es-sential. Whilst in some cases their strategies include working
The Johannesburg Initiative
Advocating for abortion access
26
on the inside, all of them have a range of advocacy strategieswhich involve building support outside of the political or serv-ice-delivery system.
Building blocks for successfuladvocacyIs media support essential?Some country studies illustrate how the media can be under-stood as the voice of the public and therefore be influentialboth on politicians and the public. This is so even when theirposition is not matched by actual public opinion polls. Theanti-choice position of much of the media in Poland, for ex-ample, presents ‘public opinion’ that is not matched by themajority public support for abortion shown in polls. The me-dia is one of the primary sites of attention of the anti-choicemovements. The Australian case illustrates how anti-choiceactivists usually have substantially greater resources to carryadvertisements and other direct messages than do the pro-choice movement. Given their limited resource base, pro-choice activists need to identify approaches to winning bothmedia understanding and media support that do not rely onbuying media space.
The papers give a diverse range of examples. These includecreating events such as demonstrations which fit media con-cepts of ‘newsworthiness’; hosting media conferences to com-municate new research findings such as opinion polls; alertingmedia to human drama stories, for example of a young girlwho has been raped and is then refused a legal abortion. Insome cases, pro-choice activists have created their own news,for example by presenting famous and socially ‘respectable’individuals who publicly say they have had abortions or whoare willing to say they support the right to abortion. A numberof studies illustrate the importance of developing personal trustwith targeted journalists and maintaining ongoing communi-cation with them.
The lessons drawn from the papers are that no amount ofwork building media relationships or establishing a media-
Comparative Analysis
27
liaison person guarantees that the media will cover an activ-ist or NGO’s events or perspectives. The media are their ownauthors and one cannot assume a shared view on what con-stitutes a ‘major story’. Further, they will not always chooseto interview the media ‘spokesperson’ whom the pro-choiceorganisations would prefer them to interview. Nor can oneassume that the media will carry factual information if theythink this information may turn their advertisers away, if thisinformation goes against the values of their owners, or if theirpaper is allied to a particular political party which holds anti-choice views.
Finally, the general political and social climate will influencehow openly supportive the media are willing to be, irrespec-tive of the power of the information or message presented. Forthis reason, gaining media support is easiest when there is ahighly mobilised pro-choice movement. The Italian case illus-trates how pro-choice activists achieved a range of coverage,all the way to carrying a TV series on how to perform manualvacuum extraction. The movement convinced the station tocarry regular contributions by feminist journalists, both of docu-mentaries and women’s stories on abortion. The Mexican case,in contrast, shows NGOs mobilising media without a majormass movement behind it. Here key NGOs made media theirbusiness. They prepared the necessary information at the righttime and gave it to the correct media contacts, keeping abor-tion in the media for an extended period of time. In this waythey managed not only to ensure public awareness and buildpublic anger against anti-choice efforts to restrict the law fur-ther in one state, but also to create tension between nationalleadership and ultra-conservative legislators.
The media are usually a target of anti-choice activism, to theextent, in the Polish case, that media managers and individualjournalists had their credibility and professional competencequestioned and were threatened with court cases. In this coun-try the Pope publicly criticised the media as being ‘anti-church’.The Church may also establish its own media, thus giving itdirect access to the public. While pro-choice activists do nothave the same institutional capacity, the country studies show
The Johannesburg Initiative
Advocating for abortion access
28
that development of their own newsletters targeting key fig-ures, such as in Brazil, can make an impact.
These examples do not, however, mean that media supportdetermines success. While politicians and other decision-mak-ers would prefer the support of the public and while ‘the pub-lic’ is frequently assumed, incorrectly, to be the perspectivepresented by the media, it is not the only force for change.While some cases illustrate the positive or negative impact ofthe media, innumerable other advocacy strategies may bal-ance its impact.
Power of coalitionsMost country studies illustrate the power of coalitions for pro-choice activism. Mexican activists brought together 40 NGOsto put women’s rights proposals to parliament. Between themthey incorporated a range of very diverse skills – organisa-tional, information and advocacy skills. The Coalition for Le-gal Abortion in Western Australia went beyond abortion rightsNGOs to include members of parliament and religious, medi-cal, professional, lawyers, workers and public health organisa-tions. Pro-choice medical practitioners and their representa-tive groups also formed a separate pro-choice coalition. Thesetypes of coalitions extend the legitimacy of abortion advocacy,since it is clear to the public that there is widespread support.
The Australian experience specifically noted that the presenceof the medical profession within a pro-choice coalition maymake politicians and media take it more seriously. Such a broadcoalition also brought in a wide range of expertise and insight,which strengthened the strategic planning and resource baseof the coalition. On the other hand, the wider the coalition,the more likely it is to have to make compromises. For exam-ple, bringing in the religious sector in some countries may meanlimiting the shared goal to abortion in the case of danger tothe women’s health or rape. However, many country studiesshow the enormously positive impact of just a few religiousfigures joining with pro-choice alliances and going public ontheir pro-choice perspective.

Comparative Analysis
29
Some country studies illustrate the power of alliances – whereorganisations collaborate without being in a formalised coali-tion. Through alliances, diverse resources can be mobilised ina way that single NGOs, especially those not operating at na-tional level, are unable to do. The Mexican case describes howexperienced organisations operating at the national level gavestate-based activists not only strategic support, but also themedia coverage they needed when that state’s governmentwas attempting to restrict the law further. Moreover, they coulduse the state-specific experience to wring commitments fromnational leadership that they would not perpetrate similar laws,strengthening the national context for abortion law reform.
Since health professionals are frequently the gatekeepers ofservice provision, alliances with them seem to play a key rolein improving access. Likewise, as discussed under ‘working onthe inside’, partnerships between NGOs, the private sector,government and donors may be key to facilitating the adequatetraining of service providers and the extension of access toservices. One of the dangers of working in close allegiancewith medical practitioners and health workers can be that theinterests of women’s groups seeking to expand safe abortionaccess can conflict with practitioners’ and health workers’ de-sire to hold onto their gate-keeping role.
Yet since health workers and health worker organisations arekey to service access, the advantages of coalitions or allianceswith them may outweigh the disadvantages. A theme whichruns through most papers is the power of the medical profes-sion when it chooses to mobilise. A number of cases, such asAustralia and Poland, show doctors organising on an anti-choice platform, although often under a more neutral guise ofproviding ‘technical’ information. Other cases, however, showmedical associations actively supporting both legal reform andservice access, including by training mid-level providers.
Training of mid-level providers does not, however, appear tomark a change in the conventional doctor/nurse hierarchy. Ifanything, the idea that nurses can do manual vacuum aspira-tion, leaving doctors to take on more complex or second tri-
The Johannesburg Initiative
Advocating for abortion access
30
mester cases, reinforces this divide. Nursing Associations aremajor gatekeepers here, as illustrated by the length of timethat it took the Nursing Council in South Africa to promulgateregulations allowing midwives to perform abortions after le-galisation. In that case, there had been a deliberate strategynot to establish mechanisms for widespread consultation withnurses before changing the law, for fear that they would op-pose it.This has meant that advocacy with nurses is now nec-essary since they are contributing to the slow pace of imple-mentation. The Kenyan case illustrates the success of a strat-egy which brought the Nurses Association on board early, inthis case including post abortion care as part of the nursingcurriculum.
The lesson for activists is that the orientation of medical andnursing associations is seldom towards human or women’srights. Rather, their purpose includes securing legal protectionfor health professionals or extending the range of services theyare able to offer and from which they profit. By drawing theminto a pro-choice platform, their orientation will need to beincorporated into the overall goals. Both coalitions and alli-ances going beyond abortion advocacy groups and medicalprofessionals can substantially strengthen the resources avail-able for advocacy work as well as the perceived legitimacy ofthe goals.
Identifying and using informationInformation is essential at all stages of the advocacy process.For example, unless the group initiating advocacy is a mass-based organisation which has generated its demands throughparticipation of poor and marginlised women, it needs to en-sure that the specifics of its goals match the needs of thesewomen. The Indian and Australian papers show that womengive priority to privacy over geographic closeness of a facility.This information would need to be factored into demands forabortion access at nearby health facilities.
A number of country strategies describe how information wasgenerated for use in winning the support of specific constituen-cies or decision-makers. Different kinds of information may be
Comparative Analysis
31
necessary for influencing different constituencies. Thus in SouthAfrica, decision-makers concerned about costs and health sys-tem capacity found epidemiological research generated by theMedical Research Council showing estimated incidence and coststo the public health system of backstreet abortions particularlyconvincing. This research was initiated by a pro-choice NGOthat made the strategic decision to persuade the Council to ac-tually host the research to give it greater credibility. Other politi-cians were more influenced by different kinds of information.For example, those politicians most concerned with ending dis-crimination were more convinced by personal stories of poorblack women who had been criminalised for having abortions.Some years after the legal change, activists persuaded parlia-ment to hold a hearing on achievements and barriers to imple-mentation and presented a wide range of research findings thathelped to shape the agenda of health system managers.
The Brazilian example of identifying well known women whohad had abortions and were willing to say so publicly in apopular magazine was effective in influencing public percep-tion and legitimising public discussion of abortion as a com-mon occurrence and a right. In India, in-depth qualitative andquantitative research findings have been used as the basis fordeveloping a series of advocacy strategies. They have, for ex-ample, been used as a means of persuading state administra-tors to improve the registration procedure for abortion facili-ties. They also shaped an NGO strategy to build women’sknowledge of their right to services.
In addition to data or individual cases, the country papers il-lustrate other imaginative uses of information. In Guyana, ac-tivists gathered editorials from political party newspapers ofthe 1960s and 1970s and used the collection to show howthey had continually considered addressing abortion. This strat-egy was an effort to influence decision-makers by drawing ontheir own history and showing abortion was not a new issuefor the country.
Some country studies portray the use of information to coun-ter anti-choice positions, often using the media as a vehicle for
The Johannesburg Initiative
Advocating for abortion access
32
disseminating the information. In Brazil, three newspapersconducted opinion polls on abortion that they published fourdays before the Pope’s visit, thus closing some of the advo-cacy space that this visit would have offered anti-choice activ-ists. Similarly, but in order to impact at the political rather thanservice level, activists in Brazil published lists of how membersof Congress voted at different stages in the hope of embarrass-ing them into supporting a growing body of public opinion forabortion rights.
Pro-choice activists must also be prepared to counter antago-nists’ use of information that is wrong or ill-informed. TheAustralian case describes the anti-choice movement’s claim ofa link between induced abortion and breast cancer, despitethe lack of scientific agreement on the issue. They also claimedthat women needed to see foetal pictures in order to make aninformed decision. The pro-choice movement was not pre-pared for a message which appeared to show concern forwomen, yet was based on unfounded premises. The paperconcludes that both an academic rebuttal on statistical groundsand a personal response, would have been powerful counterstrategies. In respect of the latter, for example, a pro-choiceactivist could have expressed her personal distress as a breastcancer sufferer in having her tragedy used as a means for anti-choice ends.
Importantly, however, the papers also show the lack of utilisa-tion of information. The Mexican case depicts activists’ sur-prise when data was not used by politicians. The Guyana caseshows how an analysis of reporting forms on legal abortionsprovides critical information both to rebut media claims – forexample to show that more than 99% of abortions are donefor Guyanese women resident in the country thus rebuttingclaims of abortion tourism – and to identify weaknesses in serv-ice delivery such as low contraceptive use and high relianceon dilatation and curettage. Yet those tasked with using thisinformation are not doing so.
These experiences suggest that generating and presenting in-formation to decision-makers does not mean they will use it.
Comparative Analysis
33
Political interests, personal values and contextual factors willinfluence whether or not they use it and these factors maychange over time. In addition to the information-gatheringexercise, substantial thought needs to go into how to dissemi-nate information in a way that will give it maximum impactwith the public, with decision-makers and with implementers.The source of information affects its credibility to decision-makers, hence generating research from a source which is seento be neutral may be a necessary strategy. While some deci-sion-makers will want ‘hard data’, for example on maternalmortality, others will be more influenced by human-intereststories, particularly of those they consider their constituency.
Recourse to international resources
Learning lessons from other countries’ policyexperienceThe papers show many cases of ‘policy transfer’ – of one coun-try either voluntarily drawing on policy ideas from another, orof pressure by one country on another to change its policy. InIndia, the content of the abortion law was drawn directly fromBritish law, a reflection of the colonial legacy. The combina-tion of national concern about population control and inter-national interest both in population control and in new abor-tion technology in Bangladesh facilitated the introduction ofmenstrual regulation. Despite the fact that the internationalpopulation control ideology is antithetical to women’s repro-ductive rights, service providers managed to establish a highquality service which gives priority to meeting women’s needsand created at least one avenue for them to exercise repro-ductive choice. Ironically, USAid later dropped all abortion-related funding in a direct attempt at forcing policy change.The services nearly collapsed until another donor stepped in.This case shows direct efforts at influencing national policyand programming from an external country.
The efforts of an international agency attempting to influencenational policy are most apparent in the case of the CatholicChurch as a global institution. Whether in Poland or Mexico,
The Johannesburg Initiative
Advocating for abortion access
34
Italy or Kenya, the studies show that the Catholic Church’sglobal access to information, funds and experience in anti-abortion politics allows it to play a very sophisticated role innational struggles. The Church provides some of the clearestexamples of efforts directed at policy transfer, attempting toensure that all countries hold to its policy position of no legalabortion under any circumstances.
International financial transfersFinancial resources play a key role in abortion activism, bothpro-choice and anti-choice. Many case studies illustrate reli-ance on international donor funds for pro-choice activism,predominantly from the USA or Europe. Without these, manypro-choice activist strategies would not be possible.
Citing and influencing United Nations consensusagreementsTwo papers provide examples of activists threatening to em-barrass political leadership by revealing that they are not keep-ing to international consensus agreements. Mexican activiststhreatened to take the issue of the withholding of the right toabortion from a young girl who had been raped to the UnitedNations and the Inter-American Court. Polish activists submit-ted research findings on the impact of unsafe abortion to theUnited Nations Committee on Economic, Social and CulturalRights and to the Human Rights Committee.
But it is not only a case of national activists drawing on inter-national institutions. National activists have also influencedinternational debates and consensus agreements. The chang-ing context of the abortion debate in Brazil allowed Braziliandelegates to the Cairo +5 meeting at the United Nations toplay a leading role in winning support for a paragraph argu-ing that governments need to take steps to improve healthworker training to ensure that abortion is safe and accessible.
Comparative Analysis
35
Drawing on activists from other countriesThe Guyana case describes local actors drawing on interna-tional activists and concludes that such expertise is only usefulif it builds local expertise. This method is also used by the anti-choice movement. A number of cases note the involvement ofanti-choice activists from the USA. In Mexico, the Ministry ofForeign Affairs fined the anti-choice organisations and sanc-tioned the foreigners for trying to influence national politics.This suggests that drawing attention to such interference maybe an effective strategy of pro-choice activists.
Drawing on lessons learnt in other countriesThe South African case describes legal activists engaging withpro-choice lawyers elsewhere in the world and studying theconstitutions and laws in other countries to learn from theirexperience. It also describes health activists arranging a fieldtrip for government officials to see menstrual regulation serv-ices in Bangladesh to build a health worker voice in support ofliberalising the law and the right of nurses to conduct abor-tions. The Kenyan case describes the international pro-choiceNGO Ipas providing technical input for the introduction oftraining in manual vacuum aspiration.
The Johannesburg Initiative, which has produced the papersfor this book, is itself a strategy to share advocacy experiencesbetween pro-choice activists in different countries. Two of theNGOs participating in this Initiative, from Kenya and Ethio-pia, were established by Ipas, but are run by local staff.
Thus the international arena provides a potential resource forpolicy content, for ideas on strategy and for active support ofboth pro-choice and anti-choice activism.
Comparing strategic optionsThe following tables summarise the range of strategies andtheir possible advantages and disadvantages. In each case,these will be shaped by the specific context. The table sharessome of the specifics of actions undertaken in different coun-tries as a way of illustrating strategies more concretely.
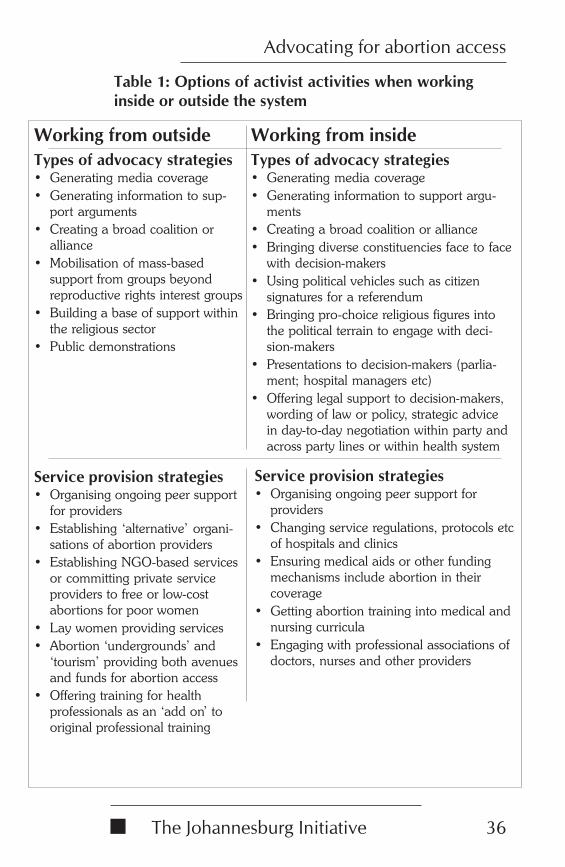
The Johannesburg Initiative
Advocating for abortion access
36
Working from outsideTypes of advocacy strategies• Generating media coverage• Generating information to sup-
port arguments• Creating a broad coalition or
alliance• Mobilisation of mass-based
support from groups beyondreproductive rights interest groups
• Building a base of support withinthe religious sector
• Public demonstrations
Working from insideTypes of advocacy strategies• Generating media coverage• Generating information to support argu-
ments• Creating a broad coalition or alliance• Bringing diverse constituencies face to face
with decision-makers• Using political vehicles such as citizen
signatures for a referendum• Bringing pro-choice religious figures into
the political terrain to engage with deci-sion-makers
• Presentations to decision-makers (parlia-ment; hospital managers etc)
• Offering legal support to decision-makers,wording of law or policy, strategic advicein day-to-day negotiation within party andacross party lines or within health system
Service provision strategies• Organising ongoing peer support
for providers• Establishing ‘alternative’ organi-
sations of abortion providers• Establishing NGO-based services
or committing private serviceproviders to free or low-costabortions for poor women
• Lay women providing services• Abortion ‘undergrounds’ and
‘tourism’ providing both avenuesand funds for abortion access
• Offering training for healthprofessionals as an ‘add on’ tooriginal professional training
Service provision strategies• Organising ongoing peer support for
providers• Changing service regulations, protocols etc
of hospitals and clinics• Ensuring medical aids or other funding
mechanisms include abortion in theircoverage
• Getting abortion training into medical andnursing curricula
• Engaging with professional associations ofdoctors, nurses and other providers
Table 1: Options of activist activities when workinginside or outside the system
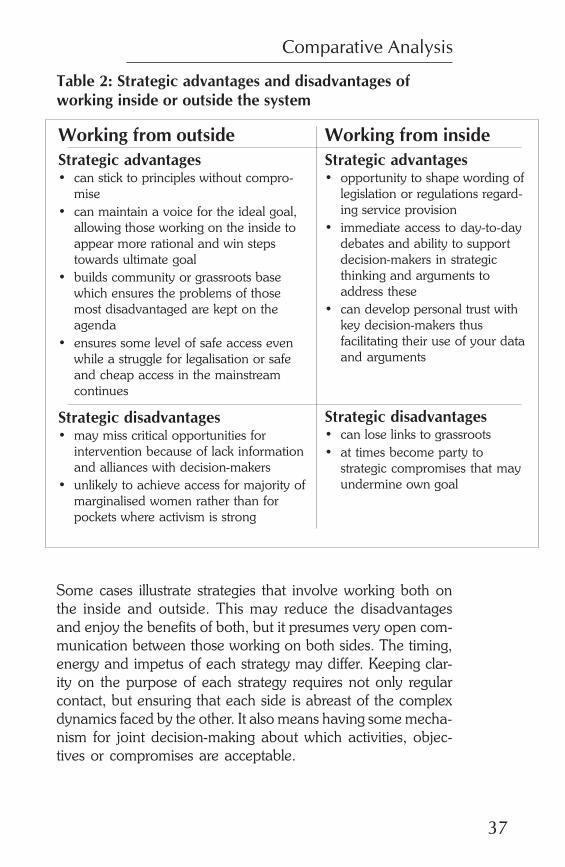
Comparative Analysis
37
Table 2: Strategic advantages and disadvantages ofworking inside or outside the system
Some cases illustrate strategies that involve working both onthe inside and outside. This may reduce the disadvantagesand enjoy the benefits of both, but it presumes very open com-munication between those working on both sides. The timing,energy and impetus of each strategy may differ. Keeping clar-ity on the purpose of each strategy requires not only regularcontact, but ensuring that each side is abreast of the complexdynamics faced by the other. It also means having some mecha-nism for joint decision-making about which activities, objec-tives or compromises are acceptable.
Working from outsideStrategic advantages• can stick to principles without compro-
mise• can maintain a voice for the ideal goal,
allowing those working on the inside toappear more rational and win stepstowards ultimate goal
• builds community or grassroots basewhich ensures the problems of thosemost disadvantaged are kept on theagenda
• ensures some level of safe access evenwhile a struggle for legalisation or safeand cheap access in the mainstreamcontinues
Strategic disadvantages• may miss critical opportunities for
intervention because of lack informationand alliances with decision-makers
• unlikely to achieve access for majority ofmarginalised women rather than forpockets where activism is strong
Working from insideStrategic advantages• opportunity to shape wording of
legislation or regulations regard-ing service provision
• immediate access to day-to-daydebates and ability to supportdecision-makers in strategicthinking and arguments toaddress these
• can develop personal trust withkey decision-makers thusfacilitating their use of your dataand arguments
Strategic disadvantages• can lose links to grassroots• at times become party to
strategic compromises that mayundermine own goal
The Johannesburg Initiative
Advocating for abortion access
38
ConclusionThe studies in this book were commissioned as part of a broaderproject to build capacity for abortion advocacy. We hoped thatby comparing and contrasting experiences in advocacy forabortion access in different countries we would be able to de-termine whether there were any shared criteria for success. Itis difficult to draw a simple conclusion on this, especially wherecircumstances dictate that pro-choice abortion activism has andmust have very different goals and strategies in different partsof the world.
Where abortion is a site of political struggle and anti-choiceperspectives hold sway in institutions of power, pro-choiceactivism tends to be defensive. In this context, the options opento activists are very different from those where there is a win-dow of opportunity for change – whether through a change inpolitical leadership or through the opportunity to build agroundswell of public support for change. Likewise, if the bu-reaucracy of the health system has no entry points for publicengagement, then gaining entry to persuade management tochange policies or procedures, or to build capacity of healthproviders may not be possible.
Even in situations where there is limited scope, however, thepapers show a variety of innovative approaches to increasingaccess, mostly operating outside of the system, be it the politi-cal system or the public health service delivery system. Thispoints to an area of weakness in abortion activism - the lack ofexperience of activists in engaging with public health systems.Activists are more comfortable in the field of legal reform whichusually requires targeted bursts of energy, rather than the veryslow, incremental pace of change of health systems. Activiststend to avoid grappling with how to support health systemreform to ensure that quality abortion services are available.They are more likely to resort to encouraging or providingabortion services in the private or NGO sector than findingways to improve access within major health institutions.
The case studies suggest, too, that while struggles for legal re-form may more easily attract the interest of activists, the inter-
Comparative Analysis
39
ests of poor and marginalised women will only be served whenabortion activism takes on questions of service accessibility.The papers illustrate how activist fatigue can set in once legalstruggles are won. Yet the need for advocacy only begins withthe legal victory. From this point, strategies both to retain legalvictories and to move from law to implementation need tena-cious and sustained efforts.
What all papers have in common is the lessons learnt aboutthe need to link strategies to a sophisticated analysis of thefactors supporting and constraining abortion access. So, forexample, a public march will not be effective when one can-not mobilise larger numbers than the anti-choice movementor where the police response will demoralise participants. Simi-larly, where service providers are reticent to perform abortions,failure to address this barrier will undermine any other advo-cacy efforts. The original research framework for these stud-ies, presented at the start of this book, provides a template foractivists to analyse their changing contexts and continuallyrevisit their problem definitions and solutions. It also remindsthem to continually assess how the political and bureaucraticsystem will respond to these and should be targeted. The coun-try studies provide a wealth of ideas of what to try and whereto take care.
The central theme through all the case studies is the tenacityof activists and their ability to review their situation and op-tions continually. Activism both in mobilising public and com-munity support for the right to choose abortion and in win-ning legitimacy for this position by decision-makers and serv-ice providers is ongoing. Victories can become losses and lossescan be overturned. The struggle will not end until all womenare able to access safe and legal abortions if and when they sochoose.
AuthorsBarbara Klugman was Director of the Women’s Health Projectduring phase one of this Initiative and is currently a senior
The Johannesburg Initiative
Advocating for abortion access
40
specialist there. She is a social anthropologist working in gen-der and policy analysis, and advocacy on gender equality,human rights, the new population policy paradigm, and sexualand reproductive rights and health. She is on the editorial boardof Reproductive Health Matters, the women’s health advisorycommittee of the Medical Research Council and the govern-ment’s Essential National Health Research Committee.
Zanele Hlatshwayo is currently the Executive Officer, Advocacy,at the Women’s Health Project, School of Public Health,University of the Witwatersrand. She has worked as an HIV/AIDS activist and policy researcher in Swaziland and SouthAfrica. Zanele currently works on gender, policy analysis andsexual rights. She is manager of the Johannesburg Initiative.
Australia
41
THE AUSTRALIAN PRO-CHOICEMOVEMENT AND THE STRUGGLE
FOR LEGAL CLARITY, LIBERAL LAWSAND LIBERAL ACCESS:TWO CASE STUDIES
Leslie Cannold with Cait Calcutt
For Children by Choice and the Australian ReproductiveHealth Alliance
Population size
Women of reproductiveage (15-44)
% population living inurban area
Gross domestic productper capita
Literacy rate of womenaged 15+
Human developmentindex
% hospital births
Maternal mortality rate
Religious affiliation
Abortion legal status
18.7 million
5.1 million
86%
US$ 20,640
0.922
99%
N/A
5 per 100,000 live births
Catholic 27%, Anglican 22%,other Christian 22%
Terms and conditions underwhich abortion is legal differin each state
The Johannesburg Initiative
Advocating for abortion access
42
IntroductionSignificant legislative changes in relation to abortion occurredin two Australian states – Western Australia (WA) and the Aus-tralian Capital Territory (ACT) – in 1998. Australia has a fed-eral political system and state governments generally regulateabortion law and practice, so when two WA doctors were crimi-nally charged for performing a termination, pro-choice legisla-tion was introduced into the WA State Parliament. Prior to this,safe and affordable abortion had been available since the early1970s, despite abortion still being classed as illegal under theWA Criminal Code. In May 1998, after three months of debateand when the proposed legislation had been significantlyamended, arguably the most liberal abortion laws in Australiawere finally passed by both houses of parliament. (This view ofthe WA law change as positive for women is still contestedamongst Australian pro-choice advocates as some view the newclauses regarding informed consent, post-twenty week restric-tions and parental notification for girls under sixteen as too re-strictive.)
A bill was introduced into the ACT parliament in August 1998that proposed severe restrictions to women’s access to abor-tion. Women in the ACT had enjoyed relatively good accesssince 1992, despite the fact the abortion was still regarded as acrime in the ACT Crimes Act. After initial community outrage,the bill was withdrawn and an amended version introducedand passed. The following months saw struggles around theimplementation of the new law, in which pro-choice advo-cates were able to limit some of the negative effects of thelegislation in practice.
This paper will discuss aspects of both these law reform cam-paigns, focussing on how final outcomes were influenced bypro-choice and anti-choice activism. The analysis has been
Australia
43
organised thematically, with a short chronological summaryof major events beginning each case study. The paper is basedon interviews with pro-choice advocates, members of parlia-ment, and resource material drawn from both campaigns.
The context of abortion inAustraliaLegalAbortion laws in Australia are determined by state govern-ments, not the federal government, and therefore differthroughout the nation. In each state and territory in the coun-try, abortion appears in the relevant Crimes Act or criminalcode, but in all states and territories amending legislation orjudicial decisions define the terms and conditions under whicha legal abortion can be performed.
In the ACT, abortion is defined within the Crimes Act of 1900and the health regulations. Under the Crimes Act, abortion isstrictly defined as lawful only if the medical practitioner be-lieves, in good faith, that the woman’s life is at risk. Womencan be prosecuted for obtaining an abortion, but this law re-mains untested in ACT courts. A judicial decision on similarlaws in another Australian state which allows for abortion onmedical, social and economic grounds has meant that authori-ties in the ACT have been reluctant to prosecute.
The Health Regulation (Maternal Health Information) Act of1998 affirms the Crimes Act definition of lawfulness. Impor-tant provisions of the Act are:
• Five years’ imprisonment for the performance of abor-tions by non-doctors. The abortion must be performedin an approved facility.
• Consulting doctors are required to give a balanced state-ment of medical advice, to estimate the probable age ofher foetus, to offer the woman the opportunity for coun-selling and to present the woman with approved writtenmaterials that include foetal photographs.
The Johannesburg Initiative
Advocating for abortion access
44
• Consulting doctors must then obtain the woman’s signa-ture on a declaration certifying that she had been of-fered or provided with this information.
• There must be a 72-hour ‘cooling off’ period betweenthe woman’s signing of the declaration and the carryingout of the termination procedure.
• A ‘conscientious objection’ clause specifies that no per-son is under an obligation to act in relation to an abor-tion.
In WA, prior to 1998, abortion was only legal according to theCriminal Code if the person performing the abortion believedit was done to save the woman’s life. This law remained un-tested following the liberal judicial interpretations of similarlaws in other Australian states.
The new Acts Amendment (Abortion) Act introduced a newclause in the WA Health Act 1911 (WA). This Act specifiesthat a lawful abortion is one in which a woman freely givesher informed consent to the procedure or has other social,personal or health related reasons for wanting an abortion.Informed consent means a medical practitioner other thanthe one performing the abortion has provided or offered orreferred the woman to counselling. After twenty weeks of preg-nancy, two medical practitioners from a panel of six appointedby the Minister must agree that the mother or unborn childhas a severe medical condition. These abortions can only beperformed at a facility approved by the Minister. No person,hospital, or other institution is obliged to perform an abor-tion.
The Acts Amendment (Abortion) Act 1998 repealed four sec-tions of the criminal code and enacted a new section whichstates that abortion must be performed by a medical practi-tioner in good faith and with reasonable care and skill. A medi-cal practitioner performing an unlawful abortion may be finedAUS$50,000, while a non-medical person performing an abor-tion is subject to a maximum penalty of five years’ imprison-ment. The woman is no longer at risk of legal sanction.
Australia
45
Girls under sixteen years of age must inform one of her par-ents that an abortion is being considered and the parent mustbe given the opportunity to participate in the counselling andmedical processes. This requirement can be waived by theChildren’s Court, however.
Service availability and accessibilityIn the ACT there is one not-for-profit clinic. Under the 1998regulations, the Minister for Health must approve all facilities.In WA there is one owner-operated clinic and one not-for-profit operated by Marie Stopes International. There is limitedpublic hospital provision, mainly for women terminating preg-nancies for foetal indications. In practice, terminations beyondtwenty weeks are available in approved facilities when the foe-tus or woman has a severe medical condition that their doctorbelieves warrants a termination and the doctor is willing tosupport the woman through the prescribed legislative process.
Approximately seven in every eight terminations are done inprivate specialised clinics, in day surgery units or by privatepractitioners in private or public hospitals. Since 1974, thenational health rebate has reduced women’s expenses. Con-cerns about privacy mean that approximately 10% of eligiblewomen do not submit claims, however. In addition, becausethe rebate has not been substantially increased since its intro-duction and does not cover theatre fees, women still face sub-stantial out-of-pocket costs. The average out-of-pocket cost fora first trimester abortion is around AUS$200. Poorer women,public patients in hospitals, rural women, indigenous womenand women from non-English speaking backgrounds are alldisadvantaged in seeking timely, affordable, confidential andculturally appropriate advice, counselling and termination serv-ices.
Attitudes towards abortionPolls appear to show that 60%-80% of Australians believe thata woman should have access to a safe, (by which many peo-ple mean ‘medically provided’) legal termination if she requestsone after counselling and in consultation with her doctor. FewAustralians believe that women should have an unrestricted
The Johannesburg Initiative
Advocating for abortion access
46
‘right to choose’ and even fewer that abortion should be ille-gal in all circumstances.
Australian political parties and abortionThe dominant political parties at State and federal level arethe Liberal Party of Australia and the Australian Labour Party(ALP). Both parties generally allow their state and federalmembers of parliament to have a ‘conscience’ vote on abor-tion issues.
The Liberal Party has no policy position on abortion, but it iscurrently in power at the federal government level and has aconservative stance on most social issues. While it has not actedto remove the partial health insurance rebate for abortionsperformed in private clinics and hospitals for fear of a back-lash within its own ranks, it has taken several decisions thatare detrimental to Australian women’s access to abortion.
The ALP has better record on abortion but its recent historyon this issue has been disappointing. The ALP policy is pro-choice. The Federal ALP government introduced the partialhealth insurance rebate for abortion in 1974. This rebate isone of the key factors allowing women to access safe abortionprovided by medical practitioners in Australia. A motion waspassed to in 1984 however, which allows ALP members ofparliament to ignore whatever decisions are taken in state orfederal ALP forums on the issue in order to vote according totheir consciences. In 1996, federal ALP and Liberal party mem-bers of parliament voted in support of anti-choice SenatorHarradine’s motion to restrict importation of mifepristone.
Case study 1: Australian CapitalTerritorySummary of eventsIndependent Member of Parliament (MP) Paul Osborne intro-duced a bill into parliament on 26 August 1998 to restrict ACTwomen’s access to abortion. The ACT pro-choice movementquickly organised a public campaign to attempt to defeat thebill. One pro-choice group also attempted to negotiate pro-
Australia
47
choice changes to the bill with the Health Minister. Seeing thathis bill did not have majority parliamentary support, Osbornewithdrew his original bill and introduced a substitute. The sub-stitute contained fewer direct attacks on women’s access, butretained the indirect attacks embodied in requirements regard-ing informed consent. The second bill passed, although de-bate continued over the content of the information womenhad to receive under the new act. While the government even-tually passed a regulation requiring women to view foetal pic-tures, service providers and activists have had some success infrustrating the implementation of the new law.
Ground Zero: The situation before the processof change beganThe ACT government consists of only one house, the legisla-tive assembly. There is no upper ‘house of review’. Therefore,the ACT is a good place for activists to attempt legislativechange because the outcomes of such attempts are easier topredict and manage.
Pro-choice activism had reached its peak in the ACT in thefirst six months of 1992 when activists successfully campaignedto repeal the restrictive 1978 Termination of Pregnancy Act. Anew, less restrictive bill was introduced, but abortion remaineda crime under the ACT Crimes Act. Activists rightly saw therepeal and the consequent establishment of the ReproductiveHealth Service (RHS) clinic as a victory and many saw thebattle for women’s reproductive freedom as largely won. Con-sequently, groups that had been active in the ACT during therepeal battle had largely disintegrated or become inactive.
In May 1998, inspired by legal change in WA, pro-choice ALPMP Wayne Berry had begun exploring the possibility of pass-ing a repeal bill in the ACT. Liberal Kate Carnell was ChiefMinister of a minority government while the Health MinisterMichael Moore was a progressive Independent with solid pro-choice credentials. The balance of power was held by two con-servative Independents. One was Paul Osborne, a retired foot-baller and Catholic father of four.
The Johannesburg Initiative
Advocating for abortion access
48
Osborne’s introduction of his anti-choice bill into the Legisla-tive Assembly surprised the pro-choice movement. This wasnot only because he contravened legislative convention byintroducing it without notice, but because many in the pro-choice movement saw the repeal of the Termination of Preg-nancy Act and the consequent establishment of the clinic asvictories that could not be undone.
Pro-choice organisingA loose and informal coalition of ACT pro-choice forces be-gan meeting weekly soon after Osborne presented his originalbill. These meetings included representatives from WayneBerry’s office, grassroots feminist activists from the democraticsocialist leaning group Pro-Choice, the Women’s ElectoralLobby (WEL), the Australian Reproductive Health Alliance,the Women’s Legal Centre and the Women’s Centre for HealthMatters and Family Planning ACT (FPACT). Representativesfrom the medical profession, although seen to be supportive,did not attend these meetings. They did liaise regularly with arepresentative of FPACT, who did attend. All members wereinvolved in lobbying Assembly politicians as well as organis-ing rallies and press conferences and other actions.
Early in the campaign, the pro-choice team saw both the HealthMinister and Chief Minister as supportive. Both had voted torepeal the Act in 1992 and supported legislation necessary toestablish the RHS clinic. In addition, both spoke at the firstand largest pro-choice rally held just after the introduction ofOsborne’s original bill. There were reasons to have been sus-picious of the Chief Minister’s position, however. Since 1994,Berry’s office had a copy of a questionnaire she had filled infor the ACT Right to Life Association in 1992. She had an-swered affirmatively to the question ‘Would you oppose anymoves to liberalise the present abortion laws of the ACT?’ aswell as to the question ‘Would you oppose the provision ofany additional facilities (government or private) for abortionsin the ACT?’
Australia
49
Legislative strategiesThe pro-choice group’s initial strategy was to oppose the origi-nal bill. This strategy would likely have met with success be-cause of the bill’s extremism, the discomfort MPs had with theway it was introduced and the inept way in which it was writ-ten.
Despite being part of the pro-choice campaign team trying tostop the bill in its entirety, FPACT/RHS began negotiatingamendments to the bill with the Health Minister. Moore’s con-tention that the original bill could pass had convinced FPACT/RHS that the safest strategy was to assist with amendmentsthat would ensure the clinic’s survival. Thus, FPACT/RHS/RHSnegotiated with Moore throughout the process of legislativechange. Indeed, up until Moore began working towards over-riding the Advisory Panel’s recommendations against includ-ing foetal pictures in the approved materials, FPACT/RHS sawthe negotiations as positive for abortion service providers inthe territory. Later FPACT/RHS’s view of Moore as ‘pro-choice’and their belief that he had tried to get them the best dealpossible changed. Moore made many unacceptable compro-mises, said one, and had ‘sold them out’. Other team mem-bers were convinced that FPACT/RHS’s actions went againsttheir strategy of uncompromising opposition to the entire bill.
On 18 November, Osborne gained permission from the speaker– again without notice – to withdraw his original bill and sub-stitute a second one. Osborne’s strategy of focusing on infor-mation rather than access in the substituted version of his billwas an unexpected anti-choice strategy and may have caughtpro-choice activists off-guard. The high level of pro-choice con-cern about losing ‘their clinic’ and the confirmation the firstbill provided of pro-choice beliefs about anti-choice ‘extrem-ism’ may also have distracted pro-choice activists from thenuances in anti-choice strategy. These factors seem to haveled pro-choice forces to ignore the bill’s informed consent con-tent.
The informed consent strategy sought to reduce the numberof terminations in two ways:
The Johannesburg Initiative
Advocating for abortion access
50
• By disclosing ‘information’ to women designed to deterthem from consenting to a termination; and
• By deterring medical staff from referring or providingterminations by making the informed consent processunduly complicated and by falsely intimating that medi-cal staff involved in abortion provision are likely to besuccessfully sued by women who decide – after the fact– that they had not been adequately informed about theprocedure.
Assessing the campaignMany activists believed that private meetings to lobby politi-cians were among the most important strategies at their dis-posal to achieve a pro-choice outcome. Several activists em-phasised the importance of presenting oneself as a crediblesource of information by dressing conservatively and present-ing non-emotive arguments in a calm, rational, methodicaland ‘academic’ way. One activist said that while FPACT/RHSwas seen as a credible source of information, the democratic-socialist leaning Pro-Choice group mob were seen to be moresuspect. Another activist with experience as an adviser to afederal politician said that doctors and other professionals areeffective lobbyists because they are more mainstream and ‘like’politicians. In her view, the more an activist group is perceivedto be a bunch of ‘ratbag activists’ or ‘feminists’ – unlike politi-cians and divorced from the mainstream – the more their viewsare dismissed.
In contrast, a ProChoice activist argued that the inside agita-tion strategy was a mistake in the 1998 campaign because itput activists in the position of supplicants – asking politiciansfor things, rather than demanding things from them. This, shefelt, exposed activists and those they represented to ridicule by‘power-lording’ politicians. In addition, she says, the pursuitby FPACT/RHS of private negotiations with the Health Minis-ter in an attempt to save the clinic undermined the effective-ness of both inside and outside agitation strategies. She be-lieves that if pro-choice forces had refused to negotiate withthe Minister, the fight would have continued over the originalbill, which she contends would never have passed.
Australia
51
Activists’ experience and knowledge of the ACT political land-scape and previous experience campaigning on the issue inthe ACT did not necessarily benefit pro-choice activists or strat-egy. One activist argues that her lack of previous experiencecampaigning on the issue in the ACT may have increased hereffectiveness because, unlike those with more knowledge, shedid not expect the fight to be easy. Similarly, academic GinaAnderson also believes that activists without specific knowl-edge about the abortion issue were extremely effective duringthe campaign. She qualifies this observation with the beliefthat it was important that at least one or two did know theirway around the issue. FPACT/RHS’s representative felt that‘being in the industry forever’ made her a credible source ofinformation, as well as ensuring her access to politicians, al-though she felt that the politics of the situation made it difficultto influence the way politicians voted. Moreover, given whatwe now know to be the failure of the negotiations FPACT/RHS was conducing with Moore, FPACT/RHS’s access to ACTpoliticians may be viewed as something less than an advan-tage.
The fact that FPACT/RHS’s representative was such a knownquantity may have worked against the pro-choice cause inother ways. One activist suggested that one of the things theHealth Minister took advantage of in his ‘divide-and-rule’ strat-egy was FPACT/RHS’s representative’s known dislike of ‘con-flict and being in the public eye’. He capitalised on his knowl-edge that she was not someone who wanted to play hardballin public, but would be drawn to a backroom negotiated strat-egy.
The media was generally seen to be on the side of the pro-choice movement. One activist’s unhappiness with the politi-cal outcome made her cynical about the impact the mediacan have on the debate, although she notes the importance ofthe media after the event to put a positive spin on the out-come. Another noted that the media had little interest in whothe campaign team had nominated to speak on their behalf.Instead the media themselves chose whom they would seekout and question on a given day or topic.
The Johannesburg Initiative
Advocating for abortion access
52
Activists said that no formal discussions were had or explicitagreements made about the language that would be used andthe way the issue would be framed during the campaign. In-stead, an unspoken consensus prevailed about these issues.Thus in rally speeches and advertisements for protest actionsas well as letters and opinion pieces in the newspaper, rightsand choice discourse was interwoven with a public healthdiscourse that focused on the dire consequences of abortiondenied. To this was added a sprinkling of feminist anti-maleand anti-patriarchal language.
Thus a range of familiar women’s rights-based slogans ap-peared in the advertisements of public meetings and ralliesand in speeches and leaflets distributed at this time. Theseincluded: ‘Support women’s rights and the right of every childto be a wanted child’; ‘A woman’s body – A woman’s choice!’;and ‘Keep Abortion Safe and Legal’.
‘Rights’ and ‘choice’ discourse was used throughout the cam-paign. It was particularly dominant in the early stages whenactivists were on the offensive against the original Osbornebill. Rights-based arguments were also seen in numerous let-ters to the editor of the Canberra Times. The Women’s LegalResource Centre (WLRC) provided a legal rationale for abor-tion as a universal political right. In a piece in the CanberraTimes (dated 7.11.98), WLRC argued that Osborne’s origi-nal legislation infringed on women’s human rights as guar-anteed in a number of international covenants to which Aus-tralia is a party.
A woman’s performance group that collected donations ofcoat hangers and assembled them into a large sculpture atan early pro-choice rally expressed the public health argu-ment. Opinion pieces and letter-writers to the Canberra Timesalso spoke of the public health consequences of abortion de-nied.
Some pro-choice activists and letter writers introduced thepatriarchal arguments when they contended that abortion wasa woman’s decision into which men – particularly middle-aged
Australia
53
ones in the Assembly – should not intrude. A pro-choice Can-berra Times opinion piece made a scathing reference toOsborne as one of a band of men worldwide ‘who know best’about the needs of women. A pro-choice ‘fact and fallacy’ leafletreferences the cartoon in which a wife comforts her anti-choicehusband by using her words in a tag line at the bottom: ‘Againstabortion? Don’t have one.’
A few activists avoided ‘rights talk’ and pursued the ‘healthissue’ line in their representations to Assembly members. Theysaw the anti-choice movement as having been more success-ful in making discursive shifts that were in tune with currentvalues. In contrast, the pro-choice movement had, as one ac-tivist said: ‘kind of gotten stuck in the 1970s ‘biology is des-tiny’ [arguments]…The heavy emphasis on a woman’s rightto choose – while I think it worked really well earlier – doesn’tsit quite as comfortably in a world that has a better idea thatyou can’t necessarily be that individualistic.’ However, mostACT pro-choice activists refused to shift their discourse. Olderones, having had success with rights talk previously, were re-luctant to abandon it, while the radical agitators refused toentertain any practical moderation of the argument becausethey saw it as giving the anti-choice side a win.
Several anti-choice activists sought to invert the rights claimsof the pro-choice movement and particularly the legal rightsdiscourse articulated by the WLRC. The activists asserted thatfoetuses as well as women have rights, citing the ‘scientificevidence’ for this claim and the same international covenantscited by WLRC.
Many, although not all, ACT anti-choice activists and organi-sations followed the newer strategies of their US counterpartsand explicitly refused to identity as anti-choice. For example,the movement circulated a treatise designed to discouragedoctors from performing or referring for abortions under theneutral-sounding Doctors’ for Legal Safeguards Group. The1998 booklet explicitly claims not to be ‘either ‘pro-choice’ or‘pro-life’ but instead a ‘credible’ source of medical and legalinformation.
The Johannesburg Initiative
Advocating for abortion access
54
In the latter half of the campaign activist focus turned to thecontent of the approved information that would be disclosedto women considering an abortion. During this time, the anti-choice movement went on the offensive with its informed con-sent strategy. While their strategy included claims about therisk abortion poses to women’s mental health and future fertil-ity, in the ACT the majority of the claims were around a claimedlink between induced abortion and breast cancer. The essenceof the anti-choice strategy was that the disclosures made towomen seeking terminations were inadequate and that wom-en’s lack of relevant information, combined with the preda-tory and financial motives of the ‘abortion industry’, coercedwomen into having abortions they did not really want andwere not freely choosing.
There was division among the anti-choice movement. Tradi-tionalists like the Pope and Human Life International arguedagainst the morality of the informed consent approach inOsborne’s bill because it condoned abortion in some cases.Local groups like ACT Right to Life responded by brandingthis perspective ‘out of step’.
Most media attention was directed to the claims around breastcancer and the claim that women need to see foetal pictures inorder to make an informed decision. Anti-choice activists ar-gued that women should receive as much information as pos-sible from the medical profession and that women, not the‘experts,’ should decide what information was relevant to theirdecision. The rational-sounding strategies served to avoid the‘extremist’ tag that US anti-choice research showed leads manyin the public to ‘turn off’ to anti-choice arguments (Swope,1998:31-35). The informed consent message was also designedto resonate with feminist sensibilities, having been taken whole-sale from radical feminist discourses opposing women’s use ofassisted reproductive technologies and mifepristone. Further,the strategy allowed the anti-choice movement to appear tocare about women, instead of just foetuses. The absence ofthis element was a weakness in their previous strategies thatthe pro-choice movement had successfully exploited.
Australia
55
The pro-choice response to this complex and unfamiliar anti-choice strategy was ad-hoc, defensive, literal and severed froma larger ‘integrated’ feminist analysis. For example, a lengthyflyer for a rally in December 1998 called for readers to ‘rejectanti-abortion information packages’ but offered no argumentsas to why they were not really ‘information.’ So ‘distressing’did one activist find the unfamiliar breast cancer strategy, thatit took her until after the issue died down to reflect on otherways she might have responded to the anti-choice claims. Shenow believes it might have been best to have coupled the lit-eral academic response she made to the legitimacy of anti-choice statistical claims with her personal distress as a breastcancer sufferer in having her tragedy used as a means for pro-choice ends. This would have questioned the integrity of anti-choice claims to be concerned about the adequacy of informedconsent because they truly care about women, rather than asa means to achieve anti-choice ends.
The validity of breast cancer data and its claim to be includedin disclosures made to women considering abortion, is un-likely to excite the interest of large numbers in the wider pub-lic. However the larger question of whether women shouldhave more information and who should decide what informa-tion is relevant – as well as suspicions about those arguing torestrict their informational access – is likely to have emotionalbite. This is particularly true in respect of the educated femi-nist-inclined women of childbearing age at which it is targeted.
Once Osborne’s original legislation was introduced, however,the ACT pro-choice movement had a crisis on its hands. Therewas no time to analyse anti-choice informed consent strate-gies and to develop responses consistent with feminist analy-ses of reproductive politics. This sort of work needed to havebeen done prior to the crisis.
The ACT anti-choice movement’s tactics were relatively subtleand restrained. Capitalising on longstanding discomfort amongpoliticians and in the wider community about the quality ofwomen’s decision-making around unplanned pregnancy, theyused feminist health advocate arguments to contend that gov-
The Johannesburg Initiative
Advocating for abortion access
56
ernmental legislation was required to ensure women were giventhe information they needed to make an informed decision.Their discussion of ‘post-abortion syndrome’ was carefullycrafted, subtle and allowed them to kill several birds with onestone. To depressed or angry women who have experiencedan abortion, it provided an explanation for their symptomsand a target for blame. To those considering abortion, it sug-gested that, however confident they feel about their decision,they are vulnerable to later regret and emotional upheaval.
The public health discourse – raising the spectre of unsafe abor-tion – fell flat in the ACT campaign because of the ACT’s geo-graphical location. The ACT is sandwiched between two stateswith liberal laws and access and there is a recent history ofACT women crossing the border to obtain services. Early in1998 a new book on abortion had inspired intense debateamong activists about the refocusing of pro-choice argumentsaround women’s moral agency. They argued that pro-choiceadvocates should not disregard the morality within in whichwomen frame their decision around abortion and that theyshould move away from a public women’s rights discourse.The explicit rejection by ACT Pro-Choice of such areconfiguration of pro-choice arguments and their decision tore-embrace the old rights/choice discourse deprived the pro-choice campaign of an effective framework to meet the im-plied and explicit claims of the newer anti-choice informedconsent strategy. This is not to say that the uniform adoptionof such discourse would have changed the outcome in theACT this time. The outcome was largely a foregone conclu-sion because of parliamentary numbers and the politicalagenda of the Chief Minister. Public views about abortion willhave some influence on the success of future activist endeav-ours, however, including the current goal of electing pro-choicecandidates at the next election.
FundingThe lack of funding was an issue for all pro-choice activistsand organisations in the debate. They were specifically con-
Australia
57
cerned about the lack of funding to present the pro-choiceposition in the media and to use direct mail or other methodsto make the electorate aware of the abortion issue and theirrepresentative’s position. Fundraising took up time and en-ergy that could have been used more productively elsewhereand funds often came out of the pockets of individual activists.Some money was raised during the campaign, but most of itwent to fund the legal advice required by service providersregarding the implications of the Osborne bill. When Osbornesubstituted the second bill for the original, precious resourceswere lost on what became useless advice.
The impact of legislative change on accessThe FPACT and RHS say that the impact of the legislation ontheir operations has been moderate. This is a consequenceboth of the active resistance of referring doctors and clinic staffto implementing aspects of the legislation and the capacity ofclinic staff to minimise its impact on women through theirmanner of implementation. For example, in the quarterly re-ports the RHS now has to submit to the government under theregulation, they give only two reasons for granting termina-tions – for the mother’s health and for ‘other medical reasons’.In a footnote they explain that this minimal amount of detail,less than required by the legislation, is necessary to protect thewomen’s identities.
The biggest threat the legislation poses to ACT women’s ac-cess to terminations is the prescribed 72-hour waiting periodbetween the time the woman signs the client declaration andthe time the termination is performed. This requirement hasproved onerous mainly to rural women who find it difficultand expensive to make two trips to the clinic. Consequently,many of these women now seek services across the New SouthWales border in the town of Queenbeyan. This has meant anapproximately 10% decline in client numbers for the RHS clinic.The Queenbeyan clinic has also sought to attract women byadvertising itself as free from the restrictive legislative require-ments under which RHS now operates.
The Johannesburg Initiative
Advocating for abortion access
58
Case study 2: Western AustraliaSummary of eventsIn February 1998, two doctors were charged with the unlawfulperformance of an abortion. The routine abortion had beenperformed in 1996 at one of the two major private abortionclinics in Western Australia. WA police and prosecuting au-thorities had spent most of the last twenty five years turning ablind eye to abortion, but the Director of Public Prosecutions(DPP) now advised police to lay charges.
The WA Association for the Legal Right to Abortion (ALRA)responded by launching a campaign to repeal abortion lawsfrom the WA criminal code. Pro-choice MP Cheryl Davenportintroduced a repeal bill, the Acts Amendment (Abortion) Bill,into the upper house of the WA parliament. At the same time,the state government introduced a bill into the lower housethat retained abortion in the criminal code but gave MPs fourchoices regarding the grounds on which women could accessabortions. On 1 April the Davenport bill passed through theupper house with a new section in the Health Act allowingwomen to access abortions of pregnancies up to twenty weekson the basis of informed consent. Abortions performed aftertwenty weeks had to be approved by two medical practition-ers who were members of a six-member panel appointed bythe Health Minister. The government bill passed through thelower house on the following morning with similar provisions,but was contained in the criminal code rather than the HealthAct.
On 8 April the President of the upper house rejected the bill.The Davenport bill was then the only one still before parlia-ment. Davenport entered into a long series of negotiations withthe anti-choice lobby and wavering MPs. Several anti-choiceamendments were added to the bill before it was passed bythe lower house and returned for consideration to the upperhouse. On 22 May the Davenport bill was passed into law bythe upper house without further amendments. The chargesagainst the two doctors were dropped.
Australia
59
Ground Zero: The situation before the processof change beganSince the 1970s, most WA women had enjoyed access to safe,clinical abortions at two private clinics operating in Perth, thecapital city of Western Australia. Virtually all terminations per-formed in WA are performed before the 12th week of preg-nancy, with the clinics providing services up to the 15th week.Abortions beyond this time were available at the major teach-ing hospital in Perth, but only if the woman or foetus had aserious medical condition or the foetus had a severe geneticabnormality.
ALRA was founded in the late 1960s and was the main grassroots group active in WA around abortion prior to 1998. Theywere an unusual group in a number of ways. They had a clearagenda to reform the law. They rejected the common practicein political and activist circles of separating the legality andaccess issues and weighed the benefits of achieving one againstthe possible risks to the other. ALRA had been active since1969 and had been planning a campaign at the time of thecrisis in February 1998. As part of this planning, the grouphad researched successful strategies employed by other pro-choice organisations around the world. It had also achievedconsensus about the language and strategies to be employedduring campaigning. The group rejected rights-based argu-ments for abortion and phrases like ‘pro-abortion’ and ‘abor-tion on demand’. Instead, they described abortion as a healthissue and a decision about motherhood and described them-selves as ‘pro-choice’.
In September 1997 long-time ALRA member and now MPCheryl Davenport presented the ALRA Committee with a pro-posal for law reform. The draft bill sought to straddle Daven-port’s beliefs about compromise with her continuing desire toimplement some positive changes to abortion laws. Theamendment would involve the insertion of an additional sec-tion that sought to clarify the law by defining legal abortion.Davenport had planned to move on the bill in early 1998, butwas overtaken by the charging of the two doctors and she
The Johannesburg Initiative
Advocating for abortion access
60
began to consider the option of putting forward a repeal billrather than the amendment proposal.
Pro-choice organisingWA activists coalesced under two new banners after the doc-tors were charged. The first group was the Coalition for LegalAbortion, including the Public Health Association, Family Plan-ning Western Australia, WEL, ALRA, Women Lawyers, Cen-tre for Sexual Health, the Christian Coalition and representa-tives from the Trades and Labor Council.
The Coalition monitored debate in parliament, wrote to poli-ticians, conducted a poll of voters in two anti-choice seats,kept in daily contact with the media, lobbied politicians andwrote and disseminated the much-utilised ‘Resource Materialfor Politicians.’ Dr Judy Straton from the Department of Pub-lic Health at the University of Western Australia became thecoalition’s chief spokesperson as well as the key liaison personbetween the Coalition and the Health Industry Group (HIG),the other main pro-choice lobbying group. Straton was alsothe main player briefing, consulting with and supporting CherylDavenport and Diana Warnock, the key politicians steeringthe bill through the parliament. She also, in the final days be-fore the bill’s passage, wrote responses to anti-choice amend-ments and lobbied politicians not to support them.
The idea of forming a new organisation with a new name hadbeen formulated by ALRA during their research of successfulpro-choice campaigns. They subsequently decided to supportthe newly formed Coalition for Legal Abortion and joined thegroup. They also decided to continue as a separate organisa-tion, however. One ALRA member described their motivationfor wanting to remain separate as a desire to ensure that their‘agenda was not diluted’. The coalition was happy that ALRAremained separate. As one of the members explained, this al-lowed them to pursue a more realistic approach to achievinglegislative reform and to escape ALRA’s sense of ‘ownership’of the abortion issue.
Australia
61
The second group was the Health Industry Group (HIG). TheHIG included the Australia Medical Association, the RoyalAustralian College of General Practitioners, the Royal Austral-ian College of Obstetricians and Gynaecologists, the RoyalAustralian and New Zealand College of Psychiatrists, Austral-ian Faculty of Public Health Medicine of the Royal Australa-sian College of Physicians, the Public Health Association, Fam-ily Planning WA and the Health Consumers Council. Thesewere mostly organisations that represented medical profession-als and had a history of political conservatism. The HIG wroteto politicians, issued press releases and responded to mediainterviews. The HIG also organised, made announcements andkept the public abreast of the medical profession’s publiclystated intention to refuse to provide terminations in the ab-sence of legislative clarification of the law.
Legislative strategyIn the first stage of the campaign, the pro-choice movementwas on the offensive, having seized the opportunity the arrestshad provided to push for full repeal. Public and political anxi-ety about the DPP’s decision to enforce the law, coupled withthe medical profession’s decision to restrict access to termina-tions, contributed to Davenport’s decision to pursue repealrather than proceed with her pre-arrest plans to amend thecriminal code. ALRA supported this decision and launched acampaign that offered repeal as the solution to the crisis.
The government decided to sponsor their own staged bill thatkept abortion in the criminal code because some more liberalmembers of the government thought it would be good elec-tion politics. Key government members supported the reten-tion of abortion in the criminal code and a staggered approachas the means to finding a moderate solution to the problem.
Davenport decided not to support the government’s bill forreasons that may have included the government’s withdrawalof promised support for her bill and pressure from minor partyMPs and activist groups to pursue repeal. However, going italone meant that Davenport’s bill was disadvantaged by a lackof government support.
The Johannesburg Initiative
Advocating for abortion access
62
The turning point in the campaign was the decision of the Coa-lition for the Defence of Human Life to release confidential in-formation about women having terminations. This informationincluded the ages of the women and the gestational ages oftheir foetuses, each of which was given a name by the anti-choice agitators. The information was announced on the eve ofthe resumption of debate in the lower house. Many anti-choiceMPs were appalled by the invasion of privacy and gratuity ofthe stunt and believed that the banner headlines that resultedensured that all four options of the government bill passed itssecond reading. The bill was transmitted to the upper house.
This was the high point of the campaign for the pro-choicemovement: two pro-choice bills passed by two house of par-liament, each of which allowed abortion if a woman gave herinformed consent. Of the two, Davenport’s bill remained moreliberal.
To facilitate a reasonably smooth passage of her bill throughthe lower house, Davenport had agreed by 8 April to a numberof amendments. These included a penalty of five years’ im-prisonment for an abortion performed by a non-registeredmedical practitioner, the removal of the word ‘economic’ inthe consequences for the woman making an abortion allow-able and the inclusion of the lower house’s definition of ‘in-formed consent’.
The government bill was ruled out of order in the upper houseon the same day pro-choice MP Diana Warnock introducedDavenport’s concessions to the lower house. The ruling againstthe government bill put Davenport under further pressure tosmoothe the ruffled feathers of those in the lower house whoresented losing ‘their bill’. It is here that things fell apart. Overthe next month, Davenport agreed to the return of unjustifiedabortion into the criminal code, to restrictive dependant mi-nor provisions and to the addition of an information clause.On 21 May, the Davenport bill became law.
The period after each house had passed their respected abor-tion bills was extremely stressful for pro-choice activists. Dur-ing April, anti-choice forces began working around the clock,
Australia
63
trolling United States statute books for possible amendmentsto undermine the informed consent justification. Straton wouldarrive at Parliament House each morning to confront a newlist of proposed anti-choice amendments. In retrospect, shebelieves it would have helped if pro-choice forces had antici-pated possible amendments and had responses prepared.
Several factors appeared to auger well for the passage of theDavenport bill with its fundamental features intact. Davenportand other MPs knew that MPs risked community outrage shouldthey fail to produce some sort of resolution to the crisis engulf-ing WA. Since the announcement of the arrest of the two doc-tors, several women had been admitted to hospitals withbotched self-attempted abortions. The polls were showing 82%support for treating abortion as a private decision a womanmakes in consultation with her doctors, with 65% of electorsstrongly agreeing with this statement.
Given this, it remains unclear why Davenport felt under somuch pressure to negotiate so many compromising amend-ments to her bill. On 6 April, Straton penned a letter to allgovernment MPs pointing out that both bills had accepted in-formed consent as adequate grounds for legal abortion andpushing MPs to remove all abortion sections from the criminalcode except those referring to non-medical abortion provision.
Yet, just a few days later, with her bill the only one still in town,Davenport seemed to be making the sort of compromises thatwould only be made when a bill is really in trouble. Davenportfirmly rejects any suggestion that she got a worse outcomethan she needed to. She argues that the bill would have beendefeated in the final stage without every single one of the com-promises she made.
Negotiations may not have been helped by the fact that nei-ther Davenport nor Straton appeared to have agreed on clear‘bottom lines.’ Davenport says that her bottom line was thataborting women had to be free from the threat of prosecu-tion and that all mention of abortion had to be removed fromthe Criminal Code. Given that this latter criteria was not ob-tained, however, and that Davenport was earlier prepared to
The Johannesburg Initiative
Advocating for abortion access
64
put forward an amendment that only added to the CriminalCode, it is unclear how non-negotiable this ‘bottom line’ re-ally was. Straton claims that she and Davenport didn’t havea bottom line position, because they did not have ‘that sortof power.’
While Davenport insists that the bill would not have left thelower house without the amendments, Straton suggests thatthey may have been able to beat back or amend the informedconsent provision so ‘counselling’ was better defined had theamendment not come up in the middle of the night. Anotherinformant suggests that the informed consent provision was agood-faith gesture, a give-away designed to demonstrate the‘reasonableness’ of pro-choice negotiators.
Grassroots strategiesMPs appreciated the purple ribbons worn by ALRA in the par-liamentary gallery. Several reported that they found it reassur-ing to look up and to know that someone was ‘on their side’,particularly when the debate grew acrimonious. Several activ-ists expressed frustration, however, convinced that that thepoliticians were not ‘using’ them enough or as effectively asthe anti-choice politicians were using their grassroots support-ers. ALRA felt they were overlooked as lobbyists of waveringpoliticians and as providers of visible support inside the par-liament to bolster the confidence of pro-choice MPs. One MPspecifically cited this lack of visible support and presence assomething that increased her sense of being under siege.
A lack of inside knowledge of how parliamentary lobbyingworked could have contributed to ALRA’s difficulty in ensur-ing that MPs heard their arguments. Also, politicians saw ALRAas one ‘side’ of the issue. This meant that when they sought toreassert control over the internal debate by following the coa-lition and putting out their own briefing guide for MPs, theirefforts were largely unsuccessful.
There were a variety of tensions between the Davenport/Stratonteam and ALRA. These included ‘personality clashes’ and theteam’s perception that certain ALRA members believed they
Australia
65
‘owned’ the abortion issue. The team perceived ALRA’s resist-ance to any restrictions on gestational limits and their refusalto compromise on repeal as being out of touch with the politi-cal realities of the situation. The Coalition, on the other hand,accepted that repeal was not ‘politically feasible’, a view expe-rience had led Straton to share.
While some ALRA activists were distressed at being sidelinedfrom inside agitation activities within the parliament, some didnot feel such activities were the main part of ALRA’s brief, orwhere their power lay. Instead, these activists saw their role asworking from the outside to influence public opinion and toensure they did so in a way that supported those with realpower working on the inside. They felt they did this success-fully by keeping ALRA’s public health message the same asthe public health message being put forward by Davenport,Straton and their supporters in the parliament. Because ALRAwas working externally, they were not forced to compromiseon the other message that mattered to them – women’s deci-sion-making around motherhood. This message, unlike therights/choice one, had the advantage of not contradicting thepublic health message being used by those working internally.
Many of the activists in ALRA and the coalition, as well as MPsDavenport and Warnock, had been active in the pro-choicemovement for many years. Whether this was a positive thingdepends very much on whether the outcome in WA is seen asa success or an unacceptable compromise. Long-time involve-ment in the movement as activists or politicians seemed tocorrelate with increased clarity about the compromises thatwould be necessary, and an increased willingness to make thosecompromises in order to achieve some sort of outcome. It isunclear whether such ‘realistic views’ assisted or hindered themin achieving the best possible pro-choice outcome.
As in the ACT, the impression of most activists was that themedia was generally pro-choice and that coverage was mostlyfavourable. ALRA monitored and sought to intervene in themedia. Howard Sattler, the traditional scourge of the left andan extremely popular talkback radio host, was pro-choice. He

The Johannesburg Initiative
Advocating for abortion access
66
allowed anti-choice advocates onto his show but was dismiss-ive of their arguments. The major daily newspaper had twoeditorials on the issue, both of which supported repeal of theold abortion laws.
The HIG, the coalition, politicians and ALRA were firmly wed-ded to a discourse of public health. The public health discoursewas closely linked with discourse about the importance of keep-ing the procedure legal. Such a link appeared in ALRA pressreleases and ALRA went to some trouble to obtain copies ofthe Public Health Association booklet, which also links healthand legal issues, in order to distribute them.
ALRA took the issue of discourse and strategy so seriously theyhired media consultants. All members agreed this was one ofthe best decisions they made. The consultants were well con-nected in the small town of Perth and provided specific adviceon how ALRA activists ought to present their case and them-selves to the best effect.
Davenport, the coalition and ALRA characterised abortion asa difficult and complex decision that women undertake re-sponsibly and with due seriousness. In a letter to MPs, theCoalition rejected the media’s blithe use of the phrase ‘abor-tion on demand’ to describe ‘the complex and difficult deci-sion-making process engaged in by a woman faced with anunwanted pregnancy’. ALRA also stressed how the private anddifficult nature of abortion decision-making not only affectedwomen, but couples and families.
As noted, the medical profession was largely on side with thepush for repeal, although their motives and thus aspects oftheir arguments differed at times from those used by pro-choiceactivists. Their presence in the coalition resulted in increasedattention and seriousness from both media and politicians tothe abortion issue and to pro-choice arguments. These ben-efits may explain the lack of objections activists made to self-interested medical insistence that all abortion restrictions belifted except those restricting provision to medicos. One activ-ist notes that she has never been able to get a politician to take
Australia
67
the idea of having no restrictions on abortion seriously. Shenotes that arguments against removing all restrictions clusteraround the need to protect women from unscrupulous practi-tioners.
A number of young female lawyers come forward to tell oftheir personal experiences of abortion. All on the pro-choiceside saw this strategy as extremely effective. The stories of dif-ficult and sad decisions that resulted in non-pathological out-comes for contemporary women contrasted sharply with anti-choice discourse that sought to make the minority experienceof women ‘hurt by abortion’ the representative modern-dayabortion experience.
The bulk of anti-choice discourse was of the traditional sortthat confirmed the extremism of the anti-choice movement.Anti-choice forces asserted the rights of foetuses and demonisedwomen and service providers as murderers. The Coalition forthe Defence of Human Life sent plastic foetal kits to every MPand imported a recanting American abortion doctor from theUS. Anti-choice groups also used television adverts that showeda foetus in the womb with the sound of a heartbeat that sud-denly stops. They took out similar style advertisements on ra-dio stations, but one station pulled the advert after receivingcomplaints from listeners.
In particular, the pro-choice movement benefited from the anti-choice decision to release confidential medical records ofwomen who had abortions, along with the gestational ages ofthe women’s foetuses, to the press. The stunt divided the anti-choice movement and pushed wavering politicians and mem-bers of the public towards the pro-choice position.
The impact of legislative change on accessSince the laws have been passed, most women’s access to infor-mation and services has improved. Plans are underway for aclinic to begin providing access beyond 15 weeks and possiblyup to eighteen weeks. In addition, there is now a process – al-beit an extremely restrictive one – for women to obtain post-twenty week terminations that they had to obtain interstate in

The Johannesburg Initiative
Advocating for abortion access
68
the past. Because clinics were always restrictive in their provi-sion of abortions to girls under sixteen and the judicial bypassappears to be working smoothly, access for minors may havebeen improved.
The Western Australian government’s Health Department hasproduced and disseminated counselling guidelines to practi-tioners and a balanced easy-to-read information booklet forwomen. These discuss the possible emotional consequencesof abortion and the risk of the procedure to fertility. No men-tion of breast cancer is made.
Conclusion - Lessons learned from recentAustralian pro-choice experience• Activist groups should aim to meet regularly, even when
the issue is not politically centre-stage. This will allowthem to analyse and evaluate the political players andscene, anti-choice discourse and strategy and to formu-late and agree on the language and strategies they willuse when campaigning.
• Forming coalitions with other pro-choice supporters andgiving those coalitions fresh names for a campaign areproven strategies. Coalitions with the medical professionoffer numerous strategic benefits. However, activists mustremain aware of the differences that are likely to existbetween feminist pro-choice values and goals and thoseof the medical profession. Mistaken assumptions aboutsimilarities in values and goals between seemingly like-minded groups provide ‘divide and rule’ opportunitiesto the opposition.
• Grassroots activists must be wary of the assumptions theymake about, and the trust they give to, politicians. Activ-ists should not assume that politicians running with theabortion issue share their ‘bottom lines’.
• Activist groups should analyse and debate the meaning,effectiveness, acceptability and relevance of older andnewer pro-choice discourses and strategies to the gen-eral Australian situation and the specific conditions in
Australia
69
their state. Discourse and strategy effective in the pastmay not be effective when conditions or times havechanged.
• The large well-funded and well-organised US anti-choicemovement supports the smaller Australian movementwith financial and informational resources as well aspersonnel. Activists can anticipate some of the newerstrategies used by the Australian movement by watchingfor changes in the US movement’s strategies and pro-choice responses to these.
• Both inside and outside agitation may be effective andcan – when used in tandem – be mutually beneficial.Inside agitation tends to involve more compromise, butis also more likely to achieve an outcome. Outside agi-tation allows activists to remain committed touncompromised ideals that can serve to remind thoseworking from the inside of the necessary limits to com-promise. Inside agitators may benefit from the percep-tion of moderation and rationality that results from con-trasts of their methods and positions with those on theoutside.
• The anti-choice movement has borrowed depictions ofwomen as victims who lack moral agency and real choicefrom radical feminist arguments of the 1980s and havemanipulated the feminist concept of informed consentto serve their anti-feminist ends. This borrowing and ma-nipulation is an attempt to appeal to feminist-orientedwomen and to undermine the effectiveness of feministarguments and strategies. In constructing pro-choice strat-egy and tactics, activists must attempt to anticipate waysin which their arguments can be used against feministends. They may need either to reclaim the notion of in-formed consent or to construct a new phrase to replaceit.
The Johannesburg Initiative
Advocating for abortion access
70
ReferencesSwope P (1999) ‘Abortion: A failure to communicate’ in ACTRight to Life Association Newsletter, First Quarter, 82, April31-35.
IntervieweesRebecca Albury, Gina Anderson, Lindsay Beaton, WayneBerry, Scott Blackwell, Margot Boetcher, Dorothy Broom,Barbara Buttfield, Cait Calcutt, Natasha Cica, Cheryl Daven-port, Stan Doumani, Judith Dwyer, Ruth Greble, DavidGrundmann, Susan Kelly, Carmen Lawrence, Sandy Macken-zie, Dianne Proctor, Lara Pullen, Sue Robinson, Judy Stratonand Diana Warnock.
AuthorsLeslie Cannold is a director at Strategic Data consulting firmand a fellow at the Centre for Philosophy and Public Ethics atthe University of Melbourne. She is the author of numerousacademic and general audience publications on aspects ofwomen’s health and ethics and in the area of HIV/AIDS. In1998, Leslie’s book ‘The Abortion Myth: feminism, moralityand the hard choices women make’ was published to wide-spread critical acclaim. The book grounds arguments for newpro-choice language and strategies to expand women’s repro-ductive freedom in women’s experiences of abortion.
Cait Calcutt is currently the Coordinator of the Children byChoice Association and National Coordinator of AbortionRights Network of Australia. She was a key member of theAssociation for the Legal Right to Abortion (WA) campaignteam during the 1998 WA abortion law reform campaign. Caitis also a committee member of the Australian ReproductiveHealth Alliance, which, along with Children by Choice, co-sponsored the research for the Australian contribution to thisstudy.
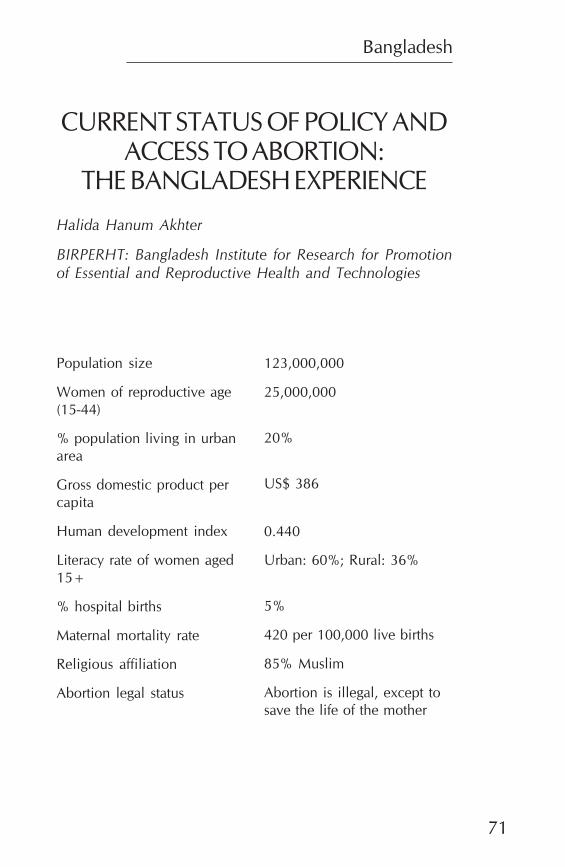
Bangladesh
71
CURRENT STATUS OF POLICY ANDACCESS TO ABORTION:
THE BANGLADESH EXPERIENCE
Halida Hanum Akhter
BIRPERHT: Bangladesh Institute for Research for Promotionof Essential and Reproductive Health and Technologies
Population size
Women of reproductive age(15-44)
% population living in urbanarea
Gross domestic product percapita
Human development index
Literacy rate of women aged15+
% hospital births
Maternal mortality rate
Religious affiliation
Abortion legal status
123,000,000
25,000,000
20%
US$ 386
0.440
Urban: 60%; Rural: 36%
5%
420 per 100,000 live births
85% Muslim
Abortion is illegal, except tosave the life of the mother
The Johannesburg Initiative
Advocating for abortion access
72
IntroductionThe population of Bangladesh is now over 123 million, withan estimated annual growth rate of 1.6% (Bangladesh Bureauof Statistics (BBS), 1998). Forty-three percent of the popula-tion is below the age of fifteen years and early marriage is stillthe norm, in that more than 60% of women are married bythe age of fifteen. The median age at first birth is around eight-een years (Mitra et al, 1997). Just over half (54%) of all cou-ples use contraception and the majority use temporary meth-ods. Although the total fertility rate has declined considerably,it is still high, at 3.3. The maternal mortality rate of 420 per100,000 live births (BBS, 1997) is a major concern. This highrate is a result of poor availability as well as low utilisation ofservices and a general lack of information. The low status ofwomen is a major determining factor for the high mortalityand morbidity burden women face.
The Bangladesh National Population Policy was drafted in1976. The draft policy included various measures to increasethe accessibility and availability of mother and child health(MCH) services throughout the country. It also proposedstrengthening the supervision system.
In terms of legal measures, the policy proposed liberalisationof the law on abortion. Under the Penal Code of 1860, abor-tion is permissible only to save the life of the expectant mother.In all other cases abortion, self-induced or otherwise, is acriminal offence punishable by imprisonment or fines. Thepolicy proposed that medical termination of pregnancy (MTP)by a qualified medical practitioner within twelve weeks ofpregnancy would not be punishable, provided that thewoman, with the consent of her husband or legal guardian,voluntarily submits for MTP for socio-economic or medical
Bangladesh
73
reasons. For the purposes of the law, socio-economic rea-sons would include unintentional pregnancy, rape, desertionby the husband or extreme penury. Medical reasons wouldinclude risk to life or grave danger to the physical and men-tal health of the women or risk that the child be born with acongenital abnormality.
The draft policy was, however, not approved as the nationalpopulation policy. The main aim of the policy had been toachieve the demographic goal of the country. This objectiveremained an important one for the government despite therejection of the 1976 proposals. Thus, in 2000 a new Na-tional Population Policy was formulated which reflected theneed for the prevention of unsafe abortion. Similarly, theobjectives of the Ministry of Health under the Fourth FiveYearPlan were to create public awareness of the seriousness ofthe population problem and to integrate family welfare intothe development programmes. Better maternal and childhealth care was planned to reduce infant, maternal andneonatal mortality. During the Third and Fourth Health andPopulation projects, maternal and child health family plan-ning strategies were developed to achieve a reduction inmaternal mortality and promotion of women’s health serv-ices through nutrition and prevention of ill health. Subse-quent programme formulation and implementation havelargely followed these strategies.
Nevertheless, abortion remains illegal in Bangladesh. Thispaper looks at how, through delivery of menstrual regulation(MR) services, many women in Bangladesh have enjoyed ac-cess to a way in which to avoid unwanted pregnancies, whilethe government has found a way of, at least partly, addressingits population concerns. The paper is based on a literaturereview, the personal experience of the author as the first MRservice provider and interviews with senior government pro-gramme managers and an NGO executive.

The Johannesburg Initiative
Advocating for abortion access
74
Introduction of menstrualregulation in the nationalprogrammeHistoryIn 1972, the law on abortion was waived for women raped bymembers of the army during the War of Liberation. Duringthis period abortions, some carried out very late in the preg-nancy, were performed in a few district hospitals under theguidance of expert teams from home and abroad. In 1974 MRwas initiated in an isolated urban model clinic where newermethods were being introduced to study the feasibility of large-scale introduction in the country.
The model clinic was funded by the Pathfinder Funds as a partof a national postpartum programme. Those responsible hopedthat the introduction of modern contraceptives and menstrualregulation procedures in the same clinical facilities would en-hance the ability of the programme to achieve its desired de-mographic goals. They hoped that it would help with fertilitycontrol by providing backup services to lessen the effects ofcontraceptive failure (Khan et al, 1984).
Menstrual regulation involves a surgical procedure to inter-rupt the course of a suspected pregnant status within 14 daysof the expected onset of the missed menstrual period. Duringthe first 14 days of a missed period, currently available tech-nological tools can not establish pregnancy conclusively. Thusany simple procedure to interrupt a suspected status of preg-nancy can be described as a means of ensuring that the womanis not pregnant, or a treatment for delayed menstruation, ratherthan as an induced abortion. The procedure is carried out byvacuum aspiration. The source of the vacuum is usually a 50ccplastic syringe and occasionally an electric vacuum aspirator.Depending on the length of gestation, a flexible plastic can-nula of varying dimensions is used.
The author was the first physician in the model clinic. TheBangladesh government encouraged the introduction of MR
Bangladesh
75
services in a few isolated family planning clinics. In 1978, anMR Training and Services Programme (MRTSP) was initiatedin seven government medical colleges and two governmentdistrict hospitals.
The initiatives of 1974 cannot be isolated from other develop-ments after the war of 1971. Government leadership, in par-ticular, must be commended for its support of the introductionof MR. One of the prominent leaders was an entrepreneurialsecretary of health with a foreign wife; both of whom had PhDs.His leadership, enthusiasm and commitment to women’s healthwere key factors promoting the establishment of these specialprojects with innovative activities.
Who defined the problem?The Director of Service Delivery had a doctorate in publichealth and was also a researcher. He made an important con-tribution to the definition of the problem. As a technocrat atthe Directorate level, he provided leadership in planning, im-plementing and facilitating these innovative programmes. In-ternational support and initiative in the early phase of the familyplanning programme facilitated the initiative. The leadershipand initiative of providers in undertaking new ventures werealso key in the successful implementation of the methods aswell as in the introduction of paramedics to the program.
All in all, there was an able group at the ministry and directo-rate level who, when the donors approached them, respondedwell to the idea of creating new types of organisations, inno-vative activities and model clinics.
International assistanceFunding and technical assistance from Family Health Interna-tional, an organisation situated in North Carolina, USA, sup-ported research, including clinical trials on contraceptives inthe clinic. The first clinic where MR was initiated was fundedby Pathfinder Fund under the auspices of the Ministry of Health.In about 1974, experts involved in the development of manualvacuum aspiration (MVA) with a plastic cannula came to Bang-ladesh under the auspices of the US Agency for International
The Johannesburg Initiative
Advocating for abortion access
76
Development. The experts delivered lectures and demonstratedthe use of MVA at the clinic.
Until 1983 external funds were available from the United StatesAgency for International Development (USAID), the PathfinderFund and the Population Crisis Committee. Due to the USgovernment’s stance on abortion, however, almost all non-government programmes stopped providing MR services inorder to protect their access to USAID funds in 1983-4. Donoragencies such as the Ford Foundation and Swedish Interna-tional Development Cooperation Agency (SIDA) stepped into provide bridging support. Donor interest was primarily inachieving demographic goals through fertility control. Theywere motivated by public health concerns rather than a con-cern with women’s rights.
At national levelThe doctors at the model family planning clinic learned themethod first and began performing the procedures. Some fe-male paramedics were then trained by the doctors on a trialbasis in the MR procedures. These paramedics then startedproviding services at this and other non-governmental organi-sation (NGO) clinics under the supervision of doctors. Withthis experience, paramedics were increasingly asked to pro-vide MR services in the NGO sector.
The professional obstetrics and gynaecology practitioners atthe medical college and MR training centres were responsiblefor both training the paramedics and then employing them.Unlike in other countries, there was no apparent resistanceamong the practitioners to utilising paramedics.
It was an opportune time. Intra-uterine devices, the lippes loopand the condom were the only contraceptive methods avail-able in 1965. Injectibles arrived around 1978. The lack of avail-ability of adequate and appropriate contraceptive methodsfacilitated the introduction and expansion of MR.
Many studies on abortion at hospitals corroborated the needfor such methods. The Ford Foundation and local expertsshowed the extent of mortality due to induced abortion. Com-
Bangladesh
77
plications of induced abortion were identified as one of thefive main causes of maternal mortality.
Despite the fact that abortion was still illegal the governmentincluded MR services in the national family planning pro-gramme in 1979 and encouraged doctors and paramedics toprovide MR services in all government hospitals, health andfamily planning complexes. A memorandum from the Popu-lation Control and Family Planning Division of the Ministry ofHealth quotes a report from the Bangladesh Institute of Lawand International Affairs (1979) to the effect that MR does notcome under the prohibition contained in the Penal Code inthat pregnancy cannot be established. Under the law, preg-nancy is an essential element of the crime of abortion. TheMR method makes it virtually impossible for the prosecutor tomeet the required proof as in Bangladesh MR is performedonly until the tenth week following a missed menstrual period.After that patients are referred to as abortion cases. MR is rec-ognised as an interim method of establishing non-pregnancyfor the woman who is at risk of being pregnant. Whether ornot she is, in fact, pregnant is not an issue.
The government memorandum states that MR is part of offi-cial policy and that the necessary logistic support for MR serv-ices and training will be provided by the Division. AnotherDivision memorandum of 1980 states that MR can be per-formed by an MR-trained, registered medical practitioner orby a Family Welfare Visitor (FWV) who has specific training inMR. It also specifies that an FWV should perform MR only upto eight weeks from the last menstrual period and must do sounder the supervision of a physician. Any case of longer dura-tion must be referred to a trained doctor. In many govern-ment-supported clinics, the procedure is now performed byparamedics.
The current situationIn 1985 bans were imposed on using USAID funds for MR.Several organisations that had been receiving USAID fundsstopped providing services. Nevertheless the procedure con-tinued to be offered within the government service network
The Johannesburg Initiative
Advocating for abortion access
78
where people were trained and willing to perform the proce-dure.
When USAID money was discontinued, the Ford Foundationprovided bridging funds. The Swedish International Develop-ment Cooperation Agency (SIDA) then began funding theNGO network to support FWV refresher training and research.The SIDA support continues today. USAID now provides sup-port for post abortion care. The Health and Population Sec-tion Programme for 1998 to 2003 of the Ministry of Healthand Family Welfare includes menstrual regulation as part ofthe Reproductive Health Care Package.
Existing information suggests that each year about 2.8% of allpregnancies undergo MR and about 1.5% undergo inducedabortion. A significant number are conducted in public facili-ties, but under unsafe conditions. Although about 12,000 doc-tors and paramedics have received formal training in MR andthe rate of complications and side effects have been reducedover time, the unsafe termination of pregnancies continues tooccur due to inadequately trained personnel and insufficientlogistical support. In addition, many women do not know of aprovider or are not aware of time limits. Access to legal MRservices is also inferior in rural areas compared to urban ar-eas.
Discussion on strategyWhy not the legal route?Most other case studies in this publication describe the strug-gle for liberal laws. In Bangladesh significant access to termi-nation of pregnancy has been achieved despite restrictivelaws.A legal solution to abortion was never seriously on theagenda once MR had been introduced in Bangladesh. Mostactors and advocates of MR are content with the way theservice is being provided. Improved quality and accessibilityare the issues to be addressed rather than legality. Paramedicsare currently providing services, government provides logis-tics and NGOs do the training. The programme thus repre-sents good networking between government and NGOs and
Bangladesh
79
there is widespread support for protecting and promoting theprogramme.
Resistance – or the lack of itThe programme, located in the family planning division of theMinistry of Health, encountered virtually no resistance fromdoctors. The doctors, who mostly work in the health division,were not concerned about the availability of the method orabout the involvement of paramedics. Initially thoseparamedics involved were family planning paramedics namedLady Family Planning Visitors. Their name was later changedto FWVs and they were given additional midwifery training.There was no opposition from obstetricians and gynaecolo-gists to this. Rather there were referrals of MR cases from theobstetricians and gynaecologists to the centre. The specialistswere at that time performing D&C abortions in their privatepractices, but were happy to have the paramedics performMR.
Political and religious groups also raised no objections to theinitiative, perhaps because they did not know about it.
In a country like Bangladesh there could be several reasonsfor this lack of resistance. One reason, which explains theoverwhelming influence of donors, is the focus on populationobjectives (this sentence is not self-explanatory). The focus onthe public health and population control perspective ratherthan the women’s rights perspective or women’s socio-eco-nomic status would also have avoided opposition from otherquarters. Thirdly, health NGOs were sensitised to women’shealth care needs and some NGOs were interested in provid-ing MR services. This provided a fertile ground for the govern-ment-NGO collaboration that characterises the programme.The women NGOs feel that if they talk loudly about abortion,there could be problems. It is more important for them thatservices are provided through government clinics and thatgovernment trained personnel, both doctors and paramedics,perform the procedure. Further, both pre- and post-counsel-ling is given. The service thus constitutes a good ‘package’,with fees ranging from nominal to modest.
The Johannesburg Initiative
Advocating for abortion access
80
Another possible reason for the lack of resistance is that thecountry’s leadership were educated and enlightened as to whatwas happening in the western world and had contact with in-ternational groups. Bangladesh was not the first country inwhich MR was introduced. Funding agencies were alreadyimplementing the programme in other countries. Bangladeshhad the requisite leadership and a pressing population issue.None of the available contraceptives were foolproof in pro-tecting women from unwanted pregnancy. It was made clearthat MR is not a contraceptive method, it is rather a backup forthe ineffective use of contraceptives. The impetus for its intro-duction thus came from scientists, government and interna-tional leadership rather than from those concerned with wom-en’s rights.
How the service worksProvidersMR training and service facilities were extended in phases andservices are now available throughout the country. There arenearly 8,000 doctors and 6,500 paramedics trained in MR whoare posted in government clinics at national, district, thanaand union levels. (The thana is an administrative unit, cover-ing between 250 000 and 300 000 people, while the lower-level union covers about a tenth of this number of people.)Services are also provided privately by doctors and paramedics.
About half of the doctors who obtain MR training are internsin the medical college hospitals. The remainder are alreadyemployed in medical posts. Many private physicians also ob-tain training and provide MR services in their private prac-tices.
The FWVs are an important component of the service in bothin government facilities and in their private capacity, espe-cially in rural areas. The FWVs have at least ten years of for-mal schooling prior to their 18-month course in family plan-ning and MCH. They learn to insert IUDs during this courseand MR techniques are taught with additional training in fresherand refresher courses. There are two main reasons MR tech-
Bangladesh
81
niques are not taught during the basic training. Firstly, it is feltthat they need to gather experience in assessing uterus sizebefore performing theprocedure and secondly, not all basictraining centres are adequately equipped to train paramedicson MR procedures and the related management issues.
FWVs are posted in almost all Thana Health Complexes andall the Family Welfare Centres. In addition to MR services, theyprovide counselling and follow up to their clients. FWVs arealso posted in most of the 4,500 unions in the country. EachFWV attends satellite clinics twice a week, extending their serv-ices to the peripheral level. The FWVs are vital in minimisingthe number of cases in which MR is not possible becausewomen arrive at the rural clinics too late, more than four weeksafter missing their menstrual period. The FWVs help to mini-mise this because they come in contact not only with the womendemanding clinical services but also with others who visit thesatellite clinics.
TrainingThe government provides considerable support in the form ofclinic space, salaries, and equipment for MR training and serv-ices. At present three programmes, one government and twonon-government, train government health personnel in theMR procedure.
Most MR training is carried out at centres by NGOs, workingunder the supervision of the university medical colleges. TheMR training and service organisations use three standardisedtraining protocol and curricula: first time training for doctors,first time training for FWVs and refresher training for FWVs.To be certified, each doctor trainee has to perform at leasttwenty MR cases independently and counsel twenty clients,every new FWV trainee has to perform at least twenty-five MRcases independently and counsel twenty-five clients and everyrefresher FWV trainee has to perform ten MR cases independ-ently and counsel ten clients. MR training covers counsellingand infection prevention. Films on contraceptives and men-strual regulation are shown during training and alecture onsafety and comfort is part of the curriculum.
The Johannesburg Initiative
Advocating for abortion access
82
Regulatory proceduresThe MR programme is guided by a National Technical Advi-sory Committee headed by the Director General, Directorateof Family Planning. The members come from the Directorateof Family Planning and four non-government organisationswhich play a prominent role in the implementation of the pro-gramme and training.
Effects of the illegal status ofabortionWhile MR provides access to termination of pregnancy formany women in Bangladesh, the illegal status of abortioncauses a range of problems.
Lack of dataThe number of MRs officially reported to the Directorate ofFamily Planning, including reports from MR training and someservice centres, was approximately 120,000 for a twelve monthperiod spanning 1998/9. MR procedures are also performedprivately by doctors and FWVs, by other medical personneland by traditional practitioners without formal training. De-pendable estimates of the annual number of MR proceduresperformed in the country are not available due to under-re-porting of the MR procedures performed in private practice.Estimates of induced abortion procedures based on interviewswith practitioners are in the range of 400,000-500,000 in oneyear (Singh et al, 1997).
Utilisation of MR services and lack of knowl-edgeThe Bangladesh Demographic and Health Survey of 1996/97(Mitra et al, 1997) shows that almost four in five women whoare or have been married know about MR, while the level ofknowledge among currently married men is low. On average,3-4% of women reported that they had undergone MR at somepoint. The proportion of those who have had MR is highestamong respondents who are currently in their late 20s and30s.
Bangladesh
83
In spite of the widespread availability of MR services, utilisa-tion of MR thus remains low, especially among high parity,less educated, rural women. There could be a number of rea-sons for this. Firstly, MR is not well publicised. Women learnabout MR services mainly through word of mouth, throughthe family planning field workers, from FWAs, or from tradi-tional birth assistants (TBAs). The FWAs are a particularly im-portant source of information. They visit households and edu-cate women on mother and child health and family planning.One FWA covers about 800 households and there are about23,500 FWAs in the country.
A second possible reason for the under-utilisation is thatparamedics are not able to reach all women as they can onlyperform MR up to eight weeks. MR beyond eight weeks is doneby doctors in relatively larger centres at district level. Becauseof a lack of information, many women do not know that theymust have the procedure before eight weeks. As they are illit-erate, they do not have access to written materials and sur-veys show that even those who have had MR, do not knowwhat it is.
Marie Stopes has roadside advertisements informing peopleabout the availability and location of MR services. While gov-ernment and NGO clinic staff and fieldworkers are free to com-municate with people in the community, MR publicity is notpermitted in any formal media, probably because of the socialstigma still attached to abortion.
Inappropriate use of MVA equipmentThe highest proportion of abortion complications is reportedwhen providers are FWVs, Kabiraj (herbal healers) and selfinduced. Traditional birth attendants and village doctors areanother group of providers for whom complications are re-ported.
It has been reported that MR syringes are used by paramedicsto induce abortion. The paramedics then refer the woman toa hospital where she receives treatment by D&C. The guide-lines state that the MR syringe can be used for a uterus of lessthan eight weeks’ size and that only the appropriate cannula
The Johannesburg Initiative
Advocating for abortion access
84
should be used beyond this date. Research shows that the useof the MR syringe beyond nine weeks’ gestation results in com-plications, particularly in incomplete abortions.
There is, however, a positive side to this situation. In the pre-MR period these women would go to an indigenous providerwho would place sticks inside the uterus. This would often re-sult in infection and death. The trained paramedic uses amethod which is approved, but uses it beyond the recom-mended period. Thus women have access to a facility wheretheir lives can be saved through lessened risk from the compli-cations.
Rejected MRIn the training centres, MR is performed during the 6-8 weekperiod by FWVs and doctors using MVA. In the 8-10 weekperiod, it is performed by doctors using electric vacuum aspi-ration. A study in 1990 (Kamal et al, 1993) found that nearlyone-third of women seeking MR services were rejected. Mostof the rejections were due to pregnancy durations of longerthan eight weeks as this is the period in which rural paramedicsare permitted to perform the operation by means of a plasticsyringe. At larger facilities, MR can be performed with vacuumaspiration machines up to eight weeks. Here again, reportingto the clinics when the pregnancy is too advanced was foundto be the most common reason for rejection for MR. Therewere a variety of reasons for clients attending late at the clinic.
Many of the rejected MR clients resort to dangerous indigenousmethods of abortion and about one-fifth of maternal mortal-ity is attributed to traditional unsafe abortions.
Drainage of hospital and family resourcesThe complications of illegal abortion affect not only individualwomen and their families, but also medical institutions andsociety as a whole. Treating these complications consumessubstantial quantities of scarce resources such as hospital beds,blood for transfusions, costly medicines and the time of medi-cal personnel which could be better utilised treating othermedical conditions. Studies showed that the mean duration of
Bangladesh
85
a hospital stay for post-abortion care is about six nights (Khanet al, 1984). Cases with associated surgery usually need tostay for more than eleven nights (Akhter, 1998).
Conclusion: The effect of MRservices on abortion seekingpractices and consequencesWhile the liberalisation of abortion laws goes a long way to-ward preventing morbidity and death from unsafe procedures,Bangladesh provides an alternative example of a way to ar-rive at a socially acceptable and workable compromise whichprovides access without a change in law. The introduction ofthe menstrual regulation programme in Bangladesh is signifi-cant because it occurred despite restrictive laws around thetermination of pregnancy.
The Bangladesh example suggests that commitment is one ofthe most important requirements when one wants to increaseaccess to safer abortion services and thus save women’s lives.In Bangladesh this commitment resulted in the formation of agovernment-NGO partnership that provided effective leader-ship to protect, promote and lobby for greater access to abor-tion care through influencing both policy and the wider com-munity.
ReferencesAkhter HH (1998) Abortion in Bangladesh in P Sachdev (ed)International Handbook on Abortion, Connecticut: GreenwoodPress.
Bangladesh Bureau of Statistics (1998) Statistical Yearbook ofBangladesh, Dhaka.
Bangladesh Institute of Law and International Affairs (1979)Dhaka Report on Legal Aspects of Population Planning in Bang-ladesh, Dhaka.
The Johannesburg Initiative
Advocating for abortion access
86
Khan AR, Begum SF, Covington DL, Janowitz B, James S andPotts M (1984) ‘Risks and Costs of Illegally Induced Abortionin Bangladesh’ in Journal of Biosocial Science, December.
Kamal H, Hossain A, Begum SF and Kamal GM (1993) Pros-pects of menstrual regulation services in Bangladesh, (Bang-ladesh Association for Prevention of Septic Abortion, Publica-tion no 9,) Dhaka.
Mitra SN, Sabir AA, Cross AR and Jamil K (1997) BangladeshDemographic and Health Survey 1996-1997. National Insti-tute of Population Research and Training, Dhaka: Mitra andAssociates and Maryland: Macro International Inc.
IntervieweesDr Atiqur Rahman Khan and Dr Shafiqur Rahman Khan (sen-ior programme managers when MR first introduced), andAbdur Rouf (senior NGO executive).
AuthorDr Halida Hanum Akhter began her career as a Medical Of-ficer in an Urban Family Planning Clinic. She later worked forthe Training-cum-Research Institute and Mohammadpur Fam-ily Planning Model Clinic in Dhaka. After obtaining her doc-toral degree in public health, Halida worked in the Reproduc-tive Health Division of the Centres for Disease Control, At-lanta. She then worked for Ford Foundation, Dhaka, as a pro-gramme officer in MCH for two years. In July 1985, she joinedthe World Bank, Washington, as an MCH-family planning spe-cialist. Halida has produced a large number of publicationsand presentations in international and national forums.
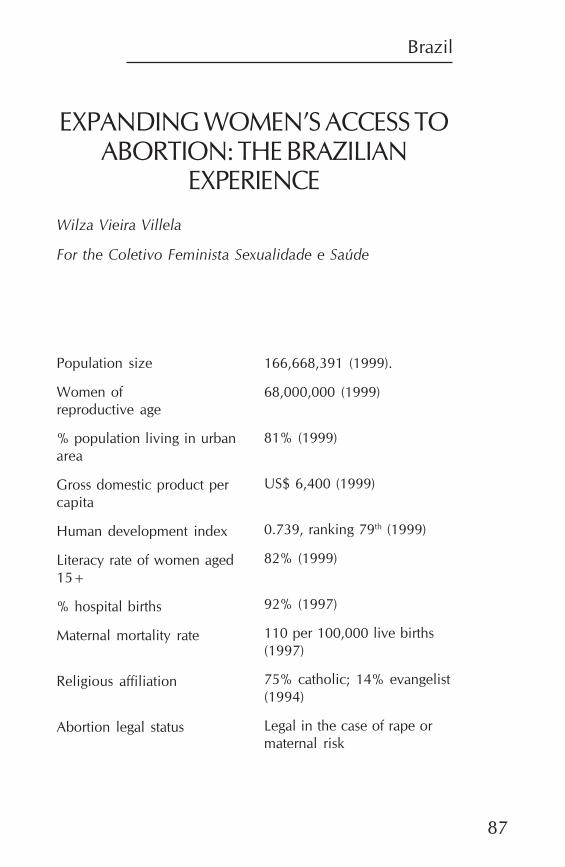
Brazil
87
EXPANDING WOMEN’S ACCESS TOABORTION: THE BRAZILIAN
EXPERIENCE
Wilza Vieira Villela
For the Coletivo Feminista Sexualidade e Saúde
Population size
Women ofreproductive age
% population living in urbanarea
Gross domestic product percapita
Human development index
Literacy rate of women aged15+
% hospital births
Maternal mortality rate
Religious affiliation
Abortion legal status
166,668,391 (1999).
68,000,000 (1999)
81% (1999)
US$ 6,400 (1999)
0.739, ranking 79th (1999)
82% (1999)
92% (1997)
110 per 100,000 live births(1997)
75% catholic; 14% evangelist(1994)
Legal in the case of rape ormaternal risk
The Johannesburg Initiative
Advocating for abortion access
88
IntroductionBrazil is the largest and most populous country in LatinAmerica. It is also the country with the greatest social inequal-ity in the world. Available statistics suggest that the richest 10%of the population have an average per capita income approxi-mately 56 times greater that the poorest 10% (Citizen Observa-tory, 2000).
The Brazilian official public health system is based on univer-sal access. The national Health Ministry plays a regulatory role.
There has never been an explicit population policy in Brazil.Since the 1960s, however, there has been a marked reductionin the average growth rate of the population – from 2.9% perannum to 1.9% in the 1980s. At the same time the fertility ratedropped from 5.6 in the 1960s to 2.5 in 1996, with a variationfrom 2.3 to 3.5 depending on the region (Geographic andStatistics Brazilian Institute (IBGE), 1996).
Even without a population policy, private family planning or-ganisations became active in the 60s. The organisations fo-cused on offering oral contraceptives and female sterilisation.The Brazilian government only began offering contraceptivesin public health clinics in 1983 through the Programme forComprehensive Women’s Health (Programa de Atenção Inte-gral em Saúde da Mulher, PAISM). This initiative provided thefirst opportunity for feminists and the Health Ministry to worktogether.
Today contraceptive use in the country is widespread. Surgi-cal sterilisation predominates. In 1996, 40% of all women liv-ing with men were sterilised. Sterilisation is followed by theuse of the pill, with 21% of all women living with men usingthis method (Demographic Health Survey, 1996).
Brazil
89
Since 1940, abortion has been considered a crime under theBrazilian Penal Code except in cases of pregnancy resultingfrom rape or if there is no other way to save the life of thepregnant woman. Very few women and health professionalsknew about this legal possibility for performing abortion until1990. This fact, allied to the refusal of professionals to performthe procedure and a strong moral rejection by the public ofthe voluntary interruption of pregnancy, made this legal per-mission a ‘dead letter’. Thus, until 1990, it was practically im-possible for a woman to obtain a voluntary interruption ofpregnancy in the public heath service, even when this proce-dure had legal protection.
The illegality of abortion in Brazil led to the expansion of anetwork of clandestine abortion clinics, in which the degree ofsecurity and sanitation was directly related to the price charged.Thus, women with greater purchasing power managed to ne-gotiate relatively safe abortions, while the poor had access onlyto low quality clinics. This put their health and even their livesat risk. In the safer clinics, the prices were high, causing manywomen to resort to other abortion practices, such as the intro-duction of objects into the uterus or the ingestion of substancesconsidered to be abortifacient. These practices are of ques-tionable efficacy and have great potential for undesirable sideeffects and consequences (Costa, 1999).
Besides the consequences for women’s health, the illegality ofabortion and the multiplicity of means used to realise it made itdifficult to study the practice with any precision. Yet differentstudies, while disagreeing on the rates, all suggest that the numberof induced abortions in Brazil is high. According to the AllanGutmacher Institute, for example, in 1990 there were 39 abor-tions for every 1,000 women (Allan Gutmacher Institute, 1998).
Between 1991 and 1993, abortion accounted for 11% of ma-ternal deaths in the country (Costa, 1999). In 1998, abortionwas the fifth most common reason for hospital admission inthe public health network and was responsible for 9% of ma-ternal deaths and 25% of the cases of sterility for tubal reasons(Ministerio de Saude, www.saude.gov.br).
The Johannesburg Initiative
Advocating for abortion access
90
Early political actionSince the 1970s the struggle for the right to abortion has beenone of the main causes of the feminist movement in Brazil.There has been heated discussion among feminists as towhether to advocate decriminalisation or legalisation. Thusfeminists discussed whether abortion should be a woman’sright, reflecting her autonomy and self-determination, orwhether it should be performed for women only under pre-determined circumstances. The latter arguments were basedon the rates of female morbidity and mortality due to its clan-destine nature and the potential social, psychological andhealth risks for women and their children. The former argu-ment was based on the idea of the right of a woman over herbody. As feminists have affirmed since the 1970s: ‘Our bodiesbelong to us!’
In 1989, with the election of a democratic city government, analliance between local government, the women’s movementand health professionals committed to social change managedto establish the first service for legal abortions in a public hos-pital. The service was located in a poor, densely populatedregion in São Paulo City. São Paulo is the most populous Bra-zilian city and the main economic centre of the country. Whathappens there has strong repercussions around the country.Thus the inauguration of the Service for Legal Abortion of theMunicipal Hospital of Jabaquara was intentionally accompa-nied by discussions with different social actors to stimulatedebate on abortion rights throughout the country. In the firstyears of functioning, the service probably inspired as muchdiscussion as procedures, operating as a reference for debateon abortion in different spheres. Such discussions were pro-moted by organised feminists in alliance with progressive doc-tors.
For five years, Jabaquara Legal Abortion Service was the onlyalternative for women who did not want to continue a preg-nancy resulting from an act of sexual violence. In 1994 thetime was ripe for expansion. The International Conference onPopulation and Development (ICPD) in Cairo, activities of the
Brazil
91
women’s movement, more positive public opinion and sup-port from health professionals and the judiciary provided thestimulus. In that year a second public hospital in São Paulobegan to perform legal abortions as part of the activities of-fered by the Services for Women Victims of Sexual Violence ofthe Reference Centre for Women’s Health. This second serv-ice was the result of an alliance between feminists and doctorseager to find a way to perform legal abortions that was moreintegrated in the overall public health framework.
Since then there has been a significant increase in legal abor-tion services. Today there are more than 20 services in thecountry equipped to provide this type of care. The distributionis unequal and insufficient in that six of the services are in SãoPaulo state and four in Porto Alegre, a southern city with atradition of 12 years under a progressive government. Never-theless, the expansion of legal abortion services has allowedthe discussion of abortion to enter the daily lives of women,health professionals and members of the legislature. Abortionis currently the theme of legislative proposals being consid-ered throughout the country and a frequent issue in the Brazil-ian media and in academic, technical or political debates re-lated to the health and autonomy of women.
This article outlines some post-1994 Brazilian initiatives aimedat broadening women’s access to abortion. It focuses, in par-ticular, on alliances and partnerships between civil society andthe state. The article draws on a Brazilian bibliography on thetopic as well as interviews with key informants.
The establishment of legal abortion services: apolitical strategyThe establishment and expansion of legal abortion servicesmeets three objectives. Firstly, it guarantees women’s right tointerrupt pregnancy in cases where the law permits. Secondly,it brings discussion about abortion into the open. Thirdly, itstimulates the participation of the population, especiallywomen, in the debate and monitoring of laws that regulatetheir daily lives.
The Johannesburg Initiative
Advocating for abortion access
92
Since 1989, the establishment of services has involved the fol-lowing steps (Castanheira, 2000):
• Activities of feminist and women’s organisations aimedat sensitising public opinion and local spheres of gov-ernment to the issue of abortion permitted by law;
• Discussion with different social sectors, especially themedical, juridical and police sectors;
• Consultation by feminist organisations and feministhealth professionals within the public health service withthe hospitals of the municipal network around the choiceof location for establishment of the service;
• Organisation of a programme team through voluntaryparticipation by technicians from different professionalareas. Preferably, each team should include, at a mini-mum, doctors, nurses, social workers and psychologists;
• Discussion of the operational norms for the service withthis team;
• Publication of a city regulation to establish the service inthe chosen hospital. The regulation specified parameterssuch as the documentation required by the women, timelimit for the realisation of the procedure, and so on;
• Training of the technical team, done in partnership withIPAS for training in manual vacuum aspiration; and
• Establishing the workflow and recording instruments.
How the services functionReferral to a legal abortion service can be done by the ap-proximately 170 Women’s Police Stations that are spreadthroughout the country. These stations are staffed by profes-sionals who have received specialised training to deal with thespecific problems women face when they are violated. Womencan also be referred by non-specialised police stations, the LegalMedical Institute (coroner’s office), support services for womenvictims of violence and other health services. A woman can
Brazil
93
also arrive at the service without passing through these refer-ral agencies, although this rarely occurs.
The technical criteria for inclusion in the programme vary acrossthe different services. The great majority of services set a 12-week limit for the interruption of pregnancy in cases of sexualviolence or maternal risk. The only document required by lawfor the legal interruption of pregnancy is the consent of thepregnant woman or her legal representative if the pregnantwoman is a minor or incapacitated. However, the majority ofhospitals require a document from the police attesting to sexualviolence. In cases of maternal risk, the technical report of threeprofessionals is required.
The establishment of services for women victims of violencehas followed a route similar to that of the legal abortion serv-ices in that they were also based on intense discussion be-tween the police, judicial authorities and non-governmentalorganisations. Every effort is directed towards facilitating thevictim’s use of services as quickly as possible, with the aim ofinstituting immediate protective measures such as preventionof pregnancy and sexually transmitted diseases (STDs) andtreatment of lesions or contusions, as well as protection andthe necessary emotional support.
No proof or documentation is necessary for the victim to re-ceive treatment at these services since violence can be provenby clinical examination. If, however, the woman needs a legalabortion but does not arrive at the service within the 72 hourperiod after the violence during which emergency contracep-tion would be effective, documents are required. These includea written police report and the written consent of the patientor her representative. The woman must also sign a declara-tion of informed consent stating that she is aware of differentoptions and rights with regard to the termination of pregnancyresulting from rape, namely interruption, acceptance or puttingthe child up for adoption (Drezett, 2000).
Despite the similar routine, the political process of lobbyingfor implementation of a service for women victims of sexual
The Johannesburg Initiative
Advocating for abortion access
94
violence is distinct from support for legal abortion services.The existence of sexual violence shifts the discussion aboutthe right to interrupt pregnancy to the prevention and treat-ment of the consequences of sexual violence. A well function-ing service for victims of sexual violence with good access forthe community theoretically reduces the need for legal abor-tions through the availability of emergency contraception. Ittherefore encounters less resistance even in more conserva-tive social circles. It is perhaps for this reason that ten of the 15functioning services offering legal abortion in the country in1998 were services for women victims of violence.
In the first six years of their existence, the services for womenvictims of violence at the São Paulo Women’s Violence Refer-ence Health Centre saw 1,118 women and performed 201 le-gal interruptions of pregnancy (Drezett, 2000). The ratio of con-sultations to interruptions of pregnancy varies across services,as does the number of women seeking the services. For exam-ple, the Women’s Violence Reference Health Centre in JoaoPessoa, a very conservative city in the North-east, saw only 70women in the first 18 months of functioning and performedonly six interruptions of pregnancy (REDESAUDE, 2000a).
The majority of the services offering legal abortion interruptthe pregnancy in cases of serious foetal malformation. In thesecases there is a legal limit in terms of gestation time and judi-cial authorisation is necessary. However, these legal require-ments have not been a real barrier since the early 1990s whena new generation of more progressive people entered the ju-dicial system. In the last ten years there have been approxi-mately 500 abortions related to serious foetal malformation,with only three refusals.
Sensitising public opinion: ThecampaignAs noted above, the establishment of a legal abortion serviceinvolves the participation of the organised women’s movement,of medical entities such as the Brazilian Federation of Gynae-
Brazil
95
cology and Obstetrics (FEBRASGO) and of local government.These groups work together to create the technical and politi-cal conditions necessary for the services to function. Their col-laboration is facilitated by the overlap between the organisa-tions, in that there are feminist doctors within the system. Theparticipation of the women’s movement occurs throughout theprocess. Prior to implementation, they are involved with thelocal public authorities and in discussion with the population.At the time of establishment, they collaborate in the training ofthe professionals, in publicising the service to the communityand in supervising implementation. Thus the co-ordinator ofthe FEBRASGO National Committee for Legal Pregnancy Ter-mination confirms: ‘We can only guarantee the quality of theseservices insofar as the local organised feminist groups are work-ing together with us’ (Andalaft, personal interview).
Nevertheless, the activities of organised women in favour ofabortion go beyond the work done around the legal abortionservices. There has been a systematic and constant effort tokeep the discussion on abortion alive, whether through themedia, the promotion of specific events on the theme or theintroduction of the theme into events on women’s health orhealth in general.
The effort to sustain discussion on abortion has gained newimpetus since 1991, with the 28 September Campaign – theInternational Day of Struggle for the Decriminalisation of Abor-tion. The campaign is an effort by Latin American and Carib-bean feminists in 14 countries to promote mobilisation forabortion in the region. In 2000, the Brazilian National Net-work for Health and Reproductive Rights (REDESAUDE) tookon the coordination of the campaign for the following two years.
The campaign attempts to align the struggle for thedecriminalisation of abortion within the broader agenda ofhealth and reproductive rights. In Brazil the campaign has beenmarked by activities in the media, with the legislature and theMinistry of Health. The chief demands are that care in respectof legal abortion be available in all the public health servicesin the country and that this provision be of the same quality as
The Johannesburg Initiative
Advocating for abortion access
96
in the services currently in operation. These demands are thetheme of a legislative proposal that has been under considera-tion since 1991. Technical norms for care of women and ado-lescent victims of sexual violence have been under considera-tion since 1999.
The Campaign Coordination Report of 2000 lists the priorityactivities of the campaign as follows (REDESAUDE, 2000b):
• The maintenance and strengthening of the visibility ofthe issue of unsafe abortion as a public health and socialjustice issue;
• The consolidation and updating of arguments on theright to decide about abortion as a question of humanrights and democracy;
• The broadening of the base of support for the campaignthrough the strengthening of ties with legislators, law-yers and medical associations;
• The mapping of the main forces against the right to abor-tion and their strategies and activities; and
• An increase in the campaign’s ability to act in the field ofcommunications through the creation of a campaign siteon the Internet, the creation of a database on the issueof abortion and publications.
The Campaign has steadily expanded since its inception inBrazil in 1991 and has succeeded in placing the abortion issueon the Brazilian political agenda. In 2000, a range of informa-tive material was produced for different sectors of the public.There was a pamphlet for the population in general, a specialedition of REDESAUDE’s electronic bulletin for the network’smembers, a special edition of the REDESAUDE newspaperfor health professionals, researchers and women’s organisa-tions and a dossier for legislators. In addition, electronic pan-els carrying this year’s theme: ‘Abortion is not a sin. Abortionis a health right, the right to choose and the right to citizen-ship’, were placed at the busiest crossroads in São Paulo.
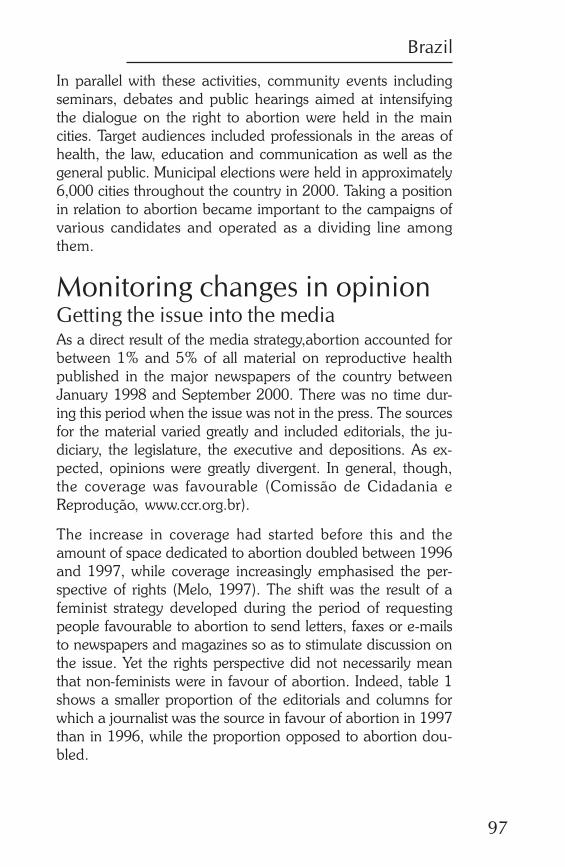
Brazil
97
In parallel with these activities, community events includingseminars, debates and public hearings aimed at intensifyingthe dialogue on the right to abortion were held in the maincities. Target audiences included professionals in the areas ofhealth, the law, education and communication as well as thegeneral public. Municipal elections were held in approximately6,000 cities throughout the country in 2000. Taking a positionin relation to abortion became important to the campaigns ofvarious candidates and operated as a dividing line amongthem.
Monitoring changes in opinionGetting the issue into the mediaAs a direct result of the media strategy,abortion accounted forbetween 1% and 5% of all material on reproductive healthpublished in the major newspapers of the country betweenJanuary 1998 and September 2000. There was no time dur-ing this period when the issue was not in the press. The sourcesfor the material varied greatly and included editorials, the ju-diciary, the legislature, the executive and depositions. As ex-pected, opinions were greatly divergent. In general, though,the coverage was favourable (Comissão de Cidadania eReprodução, www.ccr.org.br).
The increase in coverage had started before this and theamount of space dedicated to abortion doubled between 1996and 1997, while coverage increasingly emphasised the per-spective of rights (Melo, 1997). The shift was the result of afeminist strategy developed during the period of requestingpeople favourable to abortion to send letters, faxes or e-mailsto newspapers and magazines so as to stimulate discussion onthe issue. Yet the rights perspective did not necessarily meanthat non-feminists were in favour of abortion. Indeed, table 1shows a smaller proportion of the editorials and columns forwhich a journalist was the source in favour of abortion in 1997than in 1996, while the proportion opposed to abortion dou-bled.
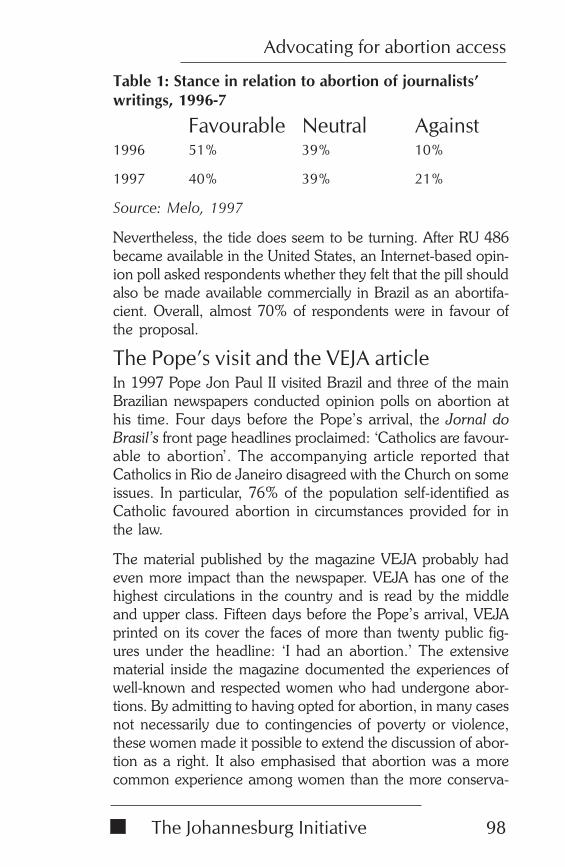
The Johannesburg Initiative
Advocating for abortion access
98
Table 1: Stance in relation to abortion of journalists’writings, 1996-7
Favourable Neutral Against1996 51% 39% 10%
1997 40% 39% 21%
Source: Melo, 1997
Nevertheless, the tide does seem to be turning. After RU 486became available in the United States, an Internet-based opin-ion poll asked respondents whether they felt that the pill shouldalso be made available commercially in Brazil as an abortifa-cient. Overall, almost 70% of respondents were in favour ofthe proposal.
The Pope’s visit and the VEJA articleIn 1997 Pope Jon Paul II visited Brazil and three of the mainBrazilian newspapers conducted opinion polls on abortion athis time. Four days before the Pope’s arrival, the Jornal doBrasil’s front page headlines proclaimed: ‘Catholics are favour-able to abortion’. The accompanying article reported thatCatholics in Rio de Janeiro disagreed with the Church on someissues. In particular, 76% of the population self-identified asCatholic favoured abortion in circumstances provided for inthe law.
The material published by the magazine VEJA probably hadeven more impact than the newspaper. VEJA has one of thehighest circulations in the country and is read by the middleand upper class. Fifteen days before the Pope’s arrival, VEJAprinted on its cover the faces of more than twenty public fig-ures under the headline: ‘I had an abortion.’ The extensivematerial inside the magazine documented the experiences ofwell-known and respected women who had undergone abor-tions. By admitting to having opted for abortion, in many casesnot necessarily due to contingencies of poverty or violence,these women made it possible to extend the discussion of abor-tion as a right. It also emphasised that abortion was a morecommon experience among women than the more conserva-
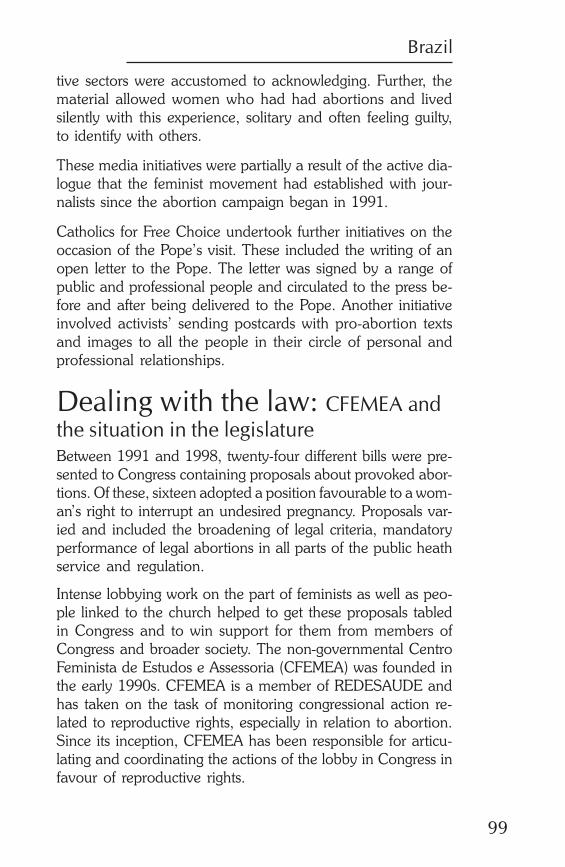
Brazil
99
tive sectors were accustomed to acknowledging. Further, thematerial allowed women who had had abortions and livedsilently with this experience, solitary and often feeling guilty,to identify with others.
These media initiatives were partially a result of the active dia-logue that the feminist movement had established with jour-nalists since the abortion campaign began in 1991.
Catholics for Free Choice undertook further initiatives on theoccasion of the Pope’s visit. These included the writing of anopen letter to the Pope. The letter was signed by a range ofpublic and professional people and circulated to the press be-fore and after being delivered to the Pope. Another initiativeinvolved activists’ sending postcards with pro-abortion textsand images to all the people in their circle of personal andprofessional relationships.
Dealing with the law: CFEMEA andthe situation in the legislatureBetween 1991 and 1998, twenty-four different bills were pre-sented to Congress containing proposals about provoked abor-tions. Of these, sixteen adopted a position favourable to a wom-an’s right to interrupt an undesired pregnancy. Proposals var-ied and included the broadening of legal criteria, mandatoryperformance of legal abortions in all parts of the public heathservice and regulation.
Intense lobbying work on the part of feminists as well as peo-ple linked to the church helped to get these proposals tabledin Congress and to win support for them from members ofCongress and broader society. The non-governmental CentroFeminista de Estudos e Assessoria (CFEMEA) was founded inthe early 1990s. CFEMEA is a member of REDESAUDE andhas taken on the task of monitoring congressional action re-lated to reproductive rights, especially in relation to abortion.Since its inception, CFEMEA has been responsible for articu-lating and coordinating the actions of the lobby in Congress infavour of reproductive rights.
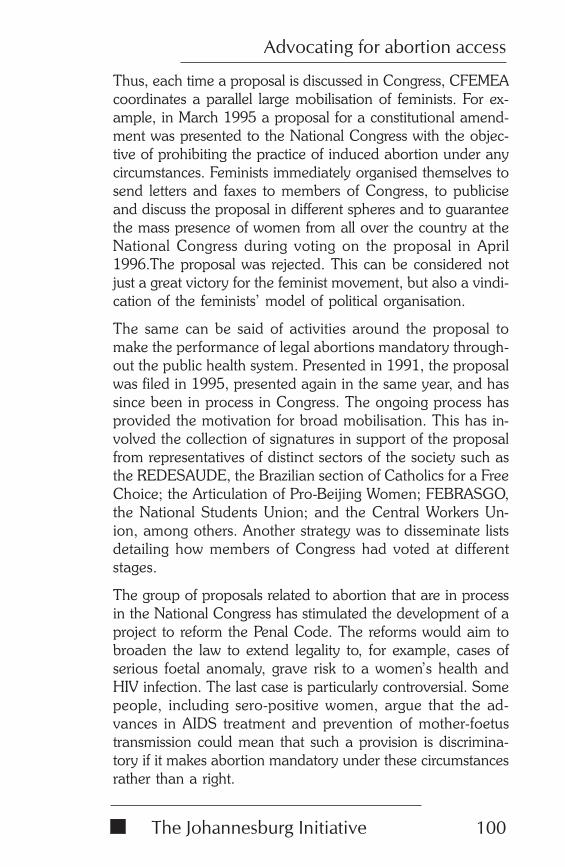
The Johannesburg Initiative
Advocating for abortion access
100
Thus, each time a proposal is discussed in Congress, CFEMEAcoordinates a parallel large mobilisation of feminists. For ex-ample, in March 1995 a proposal for a constitutional amend-ment was presented to the National Congress with the objec-tive of prohibiting the practice of induced abortion under anycircumstances. Feminists immediately organised themselves tosend letters and faxes to members of Congress, to publiciseand discuss the proposal in different spheres and to guaranteethe mass presence of women from all over the country at theNational Congress during voting on the proposal in April1996.The proposal was rejected. This can be considered notjust a great victory for the feminist movement, but also a vindi-cation of the feminists’ model of political organisation.
The same can be said of activities around the proposal tomake the performance of legal abortions mandatory through-out the public health system. Presented in 1991, the proposalwas filed in 1995, presented again in the same year, and hassince been in process in Congress. The ongoing process hasprovided the motivation for broad mobilisation. This has in-volved the collection of signatures in support of the proposalfrom representatives of distinct sectors of the society such asthe REDESAUDE, the Brazilian section of Catholics for a FreeChoice; the Articulation of Pro-Beijing Women; FEBRASGO,the National Students Union; and the Central Workers Un-ion, among others. Another strategy was to disseminate listsdetailing how members of Congress had voted at differentstages.
The group of proposals related to abortion that are in processin the National Congress has stimulated the development of aproject to reform the Penal Code. The reforms would aim tobroaden the law to extend legality to, for example, cases ofserious foetal anomaly, grave risk to a women’s health andHIV infection. The last case is particularly controversial. Somepeople, including sero-positive women, argue that the ad-vances in AIDS treatment and prevention of mother-foetustransmission could mean that such a provision is discrimina-tory if it makes abortion mandatory under these circumstancesrather than a right.
Brazil
101
To date, all the legislative proposals that have come up forvote and which aimed to restrict the right to abortion havebeen filed or rejected. This is a direct result of the intense mo-bilisation on the part of forces favourable to the right to abor-tion.
Further, even though abortion is considered to be a crime, it israre for the Brazilian judicial system to condemn women forthis act. Even in the period 1970-1989, before there was in-tense mobilisation favourable to abortion, of a total of 765abortion cases coming to court in the city of São Paulo, only102 went to trial. Of these, only 32 – or 4% of the total – re-sulted in convictions (Ardaillon, 1998).
Confronting religious discourse:Catholics for a Free ChoiceThree-quarters of the Brazilian population is Catholic. Never-theless, a large percentage of Catholics are in favour of abor-tion, both in the cases foreseen by law and even uncondition-ally. There is also a high prevalence of the use of contracep-tive methods among the Catholic population, even thoughthis is a practice the church rejects.
Yet the fact that many people who claim to be Catholic do notfollow religious prescriptions does not reduce the social powerof the church and its influence over the mass media and thepublic in general, whether Catholic or non-Catholic. It hasparticular power over the legislators.
The power of the Church in Congress is especially visible inthe activities of the Catholic Parliamentary Group (GPC), agroup of legislators from different political parties who identifywith the official positions of the Church. The GPC organisesmeetings where they make speeches and debate issues relatedto the themes proposed by the Church. Their aim is to arriveat collective approaches to the issues. The vice-president ofthe Republic is a member of the group.
Despite not being formally linked to the Catholic Church, theGPC maintains close contact with the Confederation of Bish-
The Johannesburg Initiative
Advocating for abortion access
102
ops of Brazil and with the pro-life groups, defending the invio-lability of human life from conception. Nonetheless, womencongress members who participate in the GPC sometimes showgreater flexibility in their approach to abortion. For example,some Catholic women representatives voted in favour of themotion that sought to oblige public hospitals to perform abor-tions in the cases permitted by law (REDESAUDE, 2000a).
The best example of the fact that even inside the Church thereare different positions in relation to abortion was given by Sis-ter Ivone Gebara in 1993, when she gave an interview to apopular magazine stating that she was in favour of abortionon ethical and religious grounds. Although Sister Gebara wasseverely punished for her stance, her attitude allowed manyCatholics and Christians to review their own position. She thusfacilitated a more open debate rather than simple religiousdogmatism.
Sister Gebara’s controversial interview took place at a timewhen Brazilian feminists were attempting to reach progressivesectors within the Church. The initiative resulted in the crea-tion of a Brazilian section of Catholics for a Free Choice. Catho-lics for a Free Choice participated alongside members of theChurch hierarchy in debates in the Senate and the House ofRepresentatives. They introduced a discourse based on doc-trine and religious ethics that pointed to different conclusionsthan those previously considered hegemonic. They showedthat, historically, the Church has not always condemned abor-tion as a defence of life. Rather, in the early days of Christian-ity, abortion was condemned because it could hide adultery.Similarly, until just a few centuries ago, there was an intensedebate with respect to the moment in which the foetus be-came human. Clearly the interruption of pregnancy can onlybe considered as an attempt against life after this moment,since before the entrance of the soul there is no human lifeand therefore neither crime nor sin (Nunes, 1999).
The elaboration of counter-arguments by Catholics for a FreeChoice has a broad target audience. In particular, the organi-sation targets religious leaders linked to popular movements.
Brazil
103
Through these leaders the organisation hopes to reach the ul-timate target – people from poorer and uninformed sectors ofthe population.
The alliance between feminists and the Church meant that themore radical stance of some feminist causes had to be sof-tened. For example, it was implicitly agreed that, while manyfeminists were materialists, they would not openly questionthe dogmas of faith. This pragmatic approach to the allianceeffectively increased the possibilities for introducing new ideasand ways of thinking to sectors of the population who are lesslikely to be reached by ‘traditional’ feminist militancy.
In recent years, the Catholic Church in Brazil has lost oppo-nents to abortion through members who have opted to joinevangelical groups. In particular, the Universal Church of theReign of God has positioned itself publicly in favour of abor-tion. Its stance has included the publication in its newspapers ofinterviews with and articles on well-known Brazilian feminists.
The position of the Ministry ofHealthCollaboration between the Ministry of Health and the feministmovement began with the joint elaboration of the Programmefor Comprehensive Women´s Health in 1983. In 1996 the Min-istry of Health invited a feminist doctor to be part of the tech-nical team in the area of women’s health. The doctor con-cerned was a long-standing and active member of one of themost recognised feminist organisations in Brazil. Thereafteradditional health professionals who identified with feministpositions were invited. In less than a year the entire team inthis area of government activity was made up of public sectorhealth professionals who had worked directly or indirectly withthe Brazilian feminist movement.
These women took on the technical area of women’s health inthe Ministry with a firm commitment to implementing policiesand providing heath services to women based on reproduc-tive rights.
The Johannesburg Initiative
Advocating for abortion access
104
Thus, in 1998 technical norms for attending to women victimsof sexual violence were elaborated which included the techni-cal procedures for interrupting pregnancy. The document cameup for discussion in Congress, where a proposal was set inprocess for its suspension. However, with the mobilisation ofwomen and health professionals committed to the cause ofabortion, the proposal for suspension was voted down in theHouse of Deputies. The technical norms in respect of care forhigh-risk pregnancy include provision for the interruption ofpregnancy. This approach reinforced the directive that publichealth services should be delivered in a broad and multi-disci-plinary way that provides for abortion in those case contem-plated in the law.
At the CAIRO +5 meeting in New York in 1999 the officialBrazilian delegation announced itself firmly in support of theparagraph suggesting that national governments shouldbroaden women’s access to abortion. This stance of the Brazil-ian government positively influenced the delegations fromother countries in the region, most of which generally adopteda more restricted approach.
The present situation andconclusionsDespite the victories, we still have many problems to face:
Firstly, legal interruptions of pregnancy account for approxi-mately 1% of the hospitalisations related to abortion complica-tions. We must therefore consider further strategies to broadenthe coverage of abortion services. It is also important to thinkabout the ongoing illegal abortions provided by thousands ofdoctors in private clinics. These will continue, given the currentinequalities in access to health services in Brazil. On the otherhand, if the expansion of legal abortion reduces the profit ofprivate doctors, some could take a stance against the expansionof the right to legal abortion performed through public services.
Secondly, until the approval of the law forcing public servicesto perform legal abortions, and perhaps even after this, we
Brazil
105
need to put considerable effort into ensuring the expansion ofthese services so as to achieve better coverage around thecountry. Further, the services need to be part of an effectivenetwork involving all services which can operate as entry pointsso as to guarantee a real referral system.
At the same time, we need to consider that rape and abortionare hidden problems and that society still has a strong preju-dice against both. Consequently, when a woman is raped, sheoften feels guilty and is too ashamed to search for help. Toconvince people that rape is a crime and that a pregnancy isnot payment for a sin, is a big task. The task must includestrategies to keep the discussion alive, as well as special strate-gies to reach poor, young and illiterate women.
We are thus still far from guaranteeing the right to interrupt apregnancy when the woman decides to do so. Nevertheless,the gradualist strategies adopted in the country have shownthemselves to be efficient in ensuring that women can exercisea right foreseen by the law but neglected for fifty years. Thevictories are still fragile. We stand to lose the gains given theups and downs of Congress process. This fragility points to theneed for continuous mobilisation and flexibility in playing thepolitical game.
The Brazilian gradualist strategy has also shown itself to beefficient in bringing the matter into public debate. Throughdiscussion, it has introduced and disseminated new argumentson abortion rights. In Brazil today the right to abortion hasbecome an issue in the media and on the agenda of organisa-tions that deal with women’s health. Defence of abortion rightswas one of the most important elements that helped a feministcandidate win the 2000 elections for the government of SãoPaulo City.
Traditionally, the discussion on abortion in Brazil has empha-sised the social drama of poor women who have little accessto information and reproductive health services and who be-come pregnant without being able to care for or do not wantmore children. Thus the arguments in favour of abortion have
The Johannesburg Initiative
Advocating for abortion access
106
framed it as a public health issue. The expansion of the femi-nist discourse during the 1980s provoked a shifting of the de-bate from the field of health to that of law, emphasising theresponsibility and autonomy of women (Costa, 1998). Thisshift inspired the demand for decriminalisation, although thereis still much discussion as to whether there should be totaldecriminalisation, partial decriminalisation or whether the mostadequate strategy is to struggle for the broadening of the legalcriteria.
The alliance of feminists with health professionals andFEBRASGO for the implementation of legal abortion servicesbore fruit that went beyond the defence of women’s rights tothe interruption of an unwanted pregnancy. The alliance hasmade possible a rich and broad dialogue around sexual andreproductive rights and ways of implementing them, given thecurrent political and technical positions. In the same way thearticulation of the discussion of abortion with the discussion ofviolence against women has given better visibility to this prob-lem that today has reached epidemic proportions in the coun-try. The articulation made it possible for the problem to beframed in terms of the autonomy of women in a way thatincluded not just the right to self-determination but also theright to physical and psychic integrity.
Thus, the experience in the struggle to legalise abortion andfor sexual rights in Brazil has taught us that in seeking allies forradical measures we should count on a reconfiguration of theactors between the progressive and conservative camps(Barsted, 1997). The feminist movement’s actions have beenfundamental to impeding legislative backsliding and in puttingthe abortion debate on the agenda based on the right to choose,the right to health and to citizenship. Nevertheless, these vic-tories would not have been possible had we not been pre-pared to negotiate and make joint proposals with other seg-ments of society, even though this sometimes implies a retreatin relation to more radical stances.
While the use of gradualist strategies can be difficult for manyof us who would like to see immediate attention to these de-
Brazil
107
mands, the Brazilian experience of broadening access to abor-tion has taught us that often this is the better route.
ReferencesAndalaft J (1999) ‘Dez anos de Serviços de Aborto Legal’ inJornal da RedeSaúde, 18.
Ardaillon D (1998) O tratamento do Aborto na Justica,Programa de Estudos em Saude Reprodutiva e Sexualidade,NEPO, UNICAMP.
Barsted LL (1997) ‘O movimento Feminista e aDescriminalização do Aborto’ in IFCS/UFRJ, Revista de EstudosFeministas, 5(2), 397-402.
Castanheira, ER (2000) Boas práticas em gestão de saúdeReprodutiva. Estudo do serviço de aborto legal do HospitalMunicipal do Jabaquara. Programa de AdministracaoHospitalar e Saude.
Costa S (1999) Aborto Provocado: A dimensão do problemae a transformação da prática in K Giffin and S Costa (eds)Questões de Saúde Reprodutiva. Fundacao Oswaldo Cruz, Riode Janeiro.
Demographic Health Survey (1996) Bemfam, Rio de Janeiro.
Drezett J (2000) ‘Aspectos psicossociais do atendimento amulheres vítimas de violência’, paper presented at a seminaron Health and Violence, Instituto de Saúde, Sao Paolo.
IBGE (1998) Pesquisa Nacional de Amostra por Domicílio.Cdrom.
IBASE (2000) Observatório de Cidadania. IBASE, Rio deJaneior.
Melo J (1997) ‘A polemica do Aborto na Imprensa’ in Institutode Filosofia e Ciencias Sociais, Revista de Estudos Feministas,5(2), 406-12.
Nunes MJR (1997) ‘O tratamento do Aborto pela IgrejaCatólica’ in Instituto de Filosofia e Ciencias Sociais,
The Johannesburg Initiative
Advocating for abortion access
108
Universidade Federal do Rio de Janiero, Revista de EstudosFeministas, 5(2), 413-417.
REDESAUDE (2000a) Jornal da REDE 21.
REDESAUDE (2000b) Boletim da Campanha, Sao Paolo.
AuthorWilza Villela is doctor, PhD in Social Medicine, Director Assist-ant at the Health Institute (Instituto de Saúde), São Paulo, Brazil.In this project she worked on behalf of Sexuality and HealthFeminist Collective (Coletivo Feminista Sexualidade e Saúde),an NGO based in São Paulo, Brazil, which since 1983 hasprovided assistance and conducted research on reproductivehealth and rights within a feminist approach.
Guyana
109
IMPLEMENTING A LIBERALABORTION LAW IN GUYANA:EXPERIENCES AND LESSONS
Fred Nunes
Population size
Women of reproductive age(15-44)
% population living in urbanarea
Gross domestic product percapita
Human development index
Literacy rate of women aged15+
% hospital births
Maternal mortality rate
Religious affiliation
Abortion legal status
772,755
211,013
38%
US$ 746
0.701
98%
93%
126 per 100,000 live births
57% Christian (including 6%Roman Catholic), 33%Hindu, 9% Muslim
Legal on request up to 8weeks; broad indications upto 16 weeks; to preserve lifeand health of woman after 16weeks.
The Johannesburg Initiative
Advocating for abortion access
110
IntroductionFive years after Guyana introduced a liberal abortion law in1995, the government had failed to give any sustained leader-ship in implementing that law. How can one explain the factthat, after a copybook campaign of extensive ministerial andparliamentary consultation, so little has been done by way ofexecutive action? In the clear vision of hindsight, it seems thatthe seeds of the poor record of implementation were carefully,if unintentionally, sewn during the successful campaign. Thefundamental error was a singularly strong engagement betweenthe Pro-Reform Group (PRG) and the Minister of Health, GailTeixeira, who showed an unequivocal commitment to wom-en’s reproductive rights. The PRG’s focus on the Minister failedto include and engage the small but critical cadre of seniortechnicians in the Ministry of Health.
This group, which was aloof and perhaps alienated during thecampaign, remained disinterested and disconnected from theissue prior to 2000. They contended that unsafe abortion wasnot a health priority. The net result was that no public hospitalin Guyana provided terminations under the law. Worse, eventhough every government hospital continued to admit andprovide services for women with complications of abortion,just as they had done before 1995, they submitted no reportson those services to the Ministry of Health as required underthe new law. The Ministry of Health seemed to be contemptu-ous of a law enacted in the name of strengthening public health.What benefits women have derived from the law were duelargely to the work of private medical practitioners and a smallNGO established at the time of the new law to provide com-prehensive reproductive health services, including abortions.Of course, the actions of the Ministry of Health must be seenin the context of a system of public administration that has a

Guyana
111
generally poor record of implementation in almost every sphereof government. In turn, that poor record must be understoodto prevail in a political system characterised by weak socialorganisations in a generally timid civil society.
This paper seeks to focus on the challenges of implementa-tion. It does not address the process of law reform. After asection setting out the context of the law, the account is pre-sented in chronological order and in terms of the different ac-tors.
BackgroundThe story of the campaign for a liberal abortion law in Guy-ana has been reported elsewhere (Nunes & Delph, 1995). Herewe provide only the basic background necessary to appreci-ate the problems of implementation.
Preparing the groundThe People’s Progressive Party (PPP) that won the general elec-tions of October 1992 had been the opposition party for 27years. Almost none of its members had any experience in gov-ernment, far less in leading a ministry. The period from themid-1960s to the early 1990s were years of a strong autocraticgovernment. During those decades much of Guyana’s middleclass emigrated to North America and the Caribbean. Bothcivil society and government services grew weaker. For mostof that period the press and other media had been greatlyrestrained. The Roman Catholic Church, while being the churchof only 6% of the population, had a disproportionate influ-ence on the country’s political process. In the 1960s, it playeda pivotal role in the removal of the communist-oriented leaderof the PPP Dr Cheddi Jagan and his party from government.In the 1990s, it played an equally significant role in calling forthe free and fair elections which led to Jagan’s assumption ofthe presidency in 1992.
In 1985, toward the end of its long regime, the Peoples Na-tional Congress (PNC) which had formed the governmentcontinuously since December 1964, initiated discussions on a
The Johannesburg Initiative
Advocating for abortion access
112
Medical Termination of Pregnancy (MTP) Bill. The govern-ment’s draft was a faithful copy of the Barbados MTP Act of1983. The Barbados Act was relatively liberal and permittedterminations where there was risk to the mother’s life or health,in the case of rape and for socio-economic conditions. In thefirst 12 weeks one medical practitioner could respond to a re-quest, from 13-20 weeks two practitioners had to agree, andafter 20 weeks, three practitioners were required to concur.
In Guyana, between 1985 and 1989 there had been somepublic consultation on the proposed abortion law. During thisprocess, the compact first draft grew into a complex instru-ment laden with controls. Although the bill had Cabinet ap-proval, it was not sent to the National Assembly because thegeneral elections were scheduled for 1990 and the bill wasconsidered too contentious. It was shelved instead. At leastone factor leading to that action was a public rally by a funda-mentalist Christian, anti-abortion group. While small, the in-tensity of the rally was sufficient to persuade the Senior Minis-ter in the Ministry of Health, who was also the Prime Minister,not to take further action at that time. It proved to be the PNC’slast opportunity as they lost the elections of October 1992.
Twenty years earlier, in 1971, the PNC had appointed a Spe-cial Select Committee to examine the need for an abortionlaw. Although there was vibrant public debate with severalpublic sessions, the Committee failed to report before the endof the parliamentary session and so its work was null and void.
The approach to abortion law reform is typically characterisedby a great clash of values – the rights of the foetus to life againstwomen’s right to choose. The PRG sought to avoid that di-chotomy. Instead, it adopted an approach that was highly re-liant on empirical research. It fashioned a case for abortionlaw reform predicated on making the issue a dialogue aboutpublic health, not a debate about rights. In 1991, septic abor-tion was the third highest cause of admission to hospitals andincomplete abortion was the eighth highest cause. The PRGargued that the old, restrictive law was doing nothing to con-tain the number of abortions. The group contended that a

Guyana
113
liberal law could reduce the number of abortions and radi-cally improve women’s health. They claimed that the new lawwould save public health resources that were being spent ontreating victims of unsafe abortions.
The PRG did extensive research in the national archives andidentified editorials supportive of abortion law reform that hadappeared in the party newspapers in the 1960s and 1970s.They used this information to persuade both parties to sup-port the need for a new, liberal law. The group tried unsuc-cessfully to stimulate professional groups to engage in the de-bate. But the PRG failed to get the Guyana Bar Association orthe Guyana Association of Women Lawyers to participate. Italso failed to convince the Guyana Medical Association to takea stand. The group did win support from individual membersin those associations, however, and took advantage of globalmeetings at the time of its campaign, in particular the run-upto the Cairo and Beijing meetings, to mobilise internationalsupport and to bring that focus to the local campaign.
On the local front, frustrated by the intransigence of technicalofficers within the Ministry of Health, it abandoned its effort toengage them. The PRG worked with the energetic Ministerand ignored her technical and administrative officers. Thisapproached served the short term objective of law reform, butwas to prove a recipe for disaster for the long-term matter ofimplementation.
5 May 1995: Passing the lawThe bill was debated on 5 May 1995. The tension that Teixeirahad carried virtually alone for more than two years, as the solepublic champion of the need for law reform, was evident themoment the vote was counted. It had been a tense event. Itlacked the certainty of a majority party vote as it was Guy-ana’s first conscience vote. Unable to contain her relief at thesuccessful outcome, the resolute minister shed tears of reliefand triumph in the National Assembly.
The bill which the National Assembly approved was more so-cially liberal than the Barbados Act and yet more medically
The Johannesburg Initiative
Advocating for abortion access
114
conservative. It permitted abortion on request for the first eightweeks. It was permitted for a wide range of reasons, includingcontraceptive failure, up to the sixteenth week. It was explicitthat minors could have abortions without parental knowledgeor consent. Similarly, married women did not need their part-ner’s knowledge or consent. Terminations after the sixteenthweek and at any stage of pregnancy were permitted to savethe woman or the foetus from grave harm.
Yet in respect of the medical conservatism, doctors who wishto conduct terminations after eight weeks’ gestation, must be‘authorized’ and these terminations must be done in ‘approved’institutions. These cautions were deemed appropriate in viewof the poor quality of care with which some practitioners hadallegedly performed abortions before the law was passed. Inan attempt to ensure easy access, the Act makes provision forterminations up to 12 weeks to be done by ‘any assistant’ un-der the supervision of an authorised medical practitioner.Consistent with the concern to reduce the high incidence ofrepeat abortion, there was provision for mandatory counsel-ling and a 48 hour waiting period designed to facilitate thatcounselling.
The day after the bill was debated in the National Assembly,its successful passage was reported in the local newspapers inhuge headlines. The following day two women went to theGeorgetown Public Hospital seeking lawful terminations. Theywere turned away. The women did not know that the passageof a bill did not make it law. The Hospital Administrator didnot know what to do in the circumstances. He had receivedno instructions from the Ministry of Health.
Once a bill receives majority support in the National Assem-bly, it must be sent to the President for his assent. Until thePresident signs it and until there is formal public notice of hissignature by way of the Act appearing in the Gazette, it is notthe law of the land. Indeed, even after the parliamentary vote,adversaries firmly believed that they would be able to frustratethe process of lawmaking by persuading the President not tosign the bill into law.
Guyana
115
But President Cheddi Jagan had no wish to protract a debatethat had already raged without respite for two years. He signedthe bill into law on 17 June 1995, just one month after it hadbeen passed by the National Assembly. Since there was nocommencement clause giving a future date, the Act took im-mediate effect.
The President’s prompt action was the last effective act in re-spect of making provision for the safe, legal, medical termina-tion of pregnancy. So much for the law.
At the time of writing, five years later, poor women know thatthey cannot lawfully terminate pregnancies at any public hos-pital in Guyana because no abortion service is provided. TheHospital Administrators are still uncertain of their authority toprovide abortions in accordance with the law, so they do not.This situation has resulteds in abuse. Some doctors in publichospitals provide abortions and charge women for them. Therehave been public charges and formal investigations of suchcomplaints. Intimidated by strong traditions of bureaucracy,Hospital Administrators have waited for instructions from theMinistry before providing any service. They give greater weightto Ministerial instructions than to the law of the land.
The PRG had urged the Minister of Health to declare a three-month moratorium between the passage of the law and itscommencement. The idea was to allow all parties affected bythe law an opportunity to prepare and adjust to the new re-quirements. The Ministry had to prepare forms for doctors tosubmit reports, the Medical Council had to consider applica-tions from doctors wanting to conduct terminations after eightweeks and the Council had to develop a curriculum for doc-tors it considered in need of special training. A curriculum forpre- and post-abortion counselling had to be developed andcounsellors had to be trained and certified. There was a strongwish to train doctors in manual vacuum aspiration (MVA) andto encourage a shift from dilatation and curettage (D&C) andgeneral anaesthesia.
The Johannesburg Initiative
Advocating for abortion access
116
After the law was passed14 October 1995: Regulations issued – finallyA law without regulations is of little effect. The specific guide-lines for making the law operational must be developed andmade available to all concerned. Aware of this need, the samemulti-party parliamentary committee that had prepared thebill, had also prepared the regulations that were essential forgiving effect to the law. The idea was that the regulations wouldbe submitted immediately after the bill was approved, therebyavoiding any delay in giving life to the law. For no apparentreason those regulations were not set before parliament untilOctober, four months after the law had been enacted.
There is no evidence of any extenuating circumstances thatwould have led the Minister of Health to consciously delay theregulations for this duration. The effect was to prevent privatehospitals from applying for recognition as approved institu-tions to do abortions because they had no notice of the needto do so. Nor did they know specifically what equipment thelaw required them to have to qualify for such standing. Thisdelay diminished any sense of urgency.
But these were minor inconveniences in the context of thelarger significance of the delay. The delay exposed a measureof ambivalence on the part of the Ministry’s leadership. ThePRG had succeeded in its objective of getting a new law onthe books and it knew that the regulations had been thoroughlyprepared. The group therefore turned its attention to publiceducation and mounted radio spots. For the first time in morethan two years, the Minister was on her own on the abortionissue. If she turned to her technicians for advice, they wouldscarcely have treated the regulations as a matter of urgency,since they had not been involved in the previous discussions.
Once the regulations were laid before the National Assembly,the PRG assisted the Chief Medical Officer in converting thecomprehensive reporting requirement into a layout that couldbe easily completed by physicians. The group had learnedthat the failure to make the reporting forms readily available
Guyana
117
in Barbados was a main cause of the non-reporting there, inspite of the legal requirement. Anticipating the likelihood ofresistance to complying with the reporting requirement, thegroup persuaded a leading gynaecologist to make a publicstatement of the importance of this data. The strategy worked.In the first month in Guyana, there were more reports submit-ted than in the entire 13 years under the Barbados Act.
In November 1995, a full year after the bill had been availablefor comment and five months after it had been debated andenacted into law, the Guyana Medical Association (GMA) fi-nally showed an interest in it. The GMA made a constructivesubmission to the Minister, pointing to the need for some revi-sions. The GMA was opposed to the waiting period and man-datory counselling and expressed grave concern about therestriction to non-surgical methods of abortion in the first eightweeks of gestation. The intent of the phrase ‘other than a sur-gical method’ was to encourage MVA in place of D&Cs as thedrafters had been led to regard MVA as a non-surgical proce-dure. The matter was discussed in the media from time to timebut the Ministry took no steps to address it. The net result wasand is that doctors continue to do D&Cs in technical breach ofthe law. Minister Teixeira passed the GMA’s submission to theAdvisory Board (discussed below). In four years, the AdvisoryBoard has not replied to the GMA.
31 December 1995: First indication of impactIn spite of the lack of direction from the Ministry of Health,private practitioners responded constructively to the new law.The opponents of the new law had claimed that it would makeno difference since many of the complications entering publichospitals were the result of services by medical practitioners.The high incidence of incomplete abortions that were admit-ted to public hospitals also raised the prospect that some agents,backstreet and registered practitioners alike, may have beeninducing abortions, collecting their fees and then sending thepatients to public hospitals to have the treatment completed atpublic expense. Clearly, making the service legal would havea radical impact on any such sub-standard service. Market
The Johannesburg Initiative
Advocating for abortion access
118
forces resulting from legalisation would eliminate any suchproviders. They would have to improve their service or loseclients.
Immediately after the law was passed a number of practition-ers got together and decided to make a concerted effort toimprove the quality of their services. They agreed to adminis-ter antibiotics as a prophylactic. This action, as well as themarket pressure mentioned above, were perhaps major causesof the dramatic improvement noted by December 1995. ThePRG compared the last three months of hospital admissionsfor 1994, the year before the law, with the last three months of1995 and found a 42% reduction in the number of admis-sions. This was the first clear indication of the impact of thenew law on women’s health and its potential for public sav-ings.
February 1996: Baseline dataIn Guyana, a primary driver of the legal campaign was thelocal research data that was used by the PRG throughout thecampaign. Because of the centrality of the empirical approachto the character and thrust of the reform movement, this sec-tion deals in some detail with this issue.
The crucial need following the passing of the new law for reli-able baseline data against which to measure trends could havebeen substantially addressed had the Ministry simply enforcedthe reporting requirement for doctors providing abortion serv-ices. The form developed for this purpose was a comprehen-sive one. It included substantial demographic informationabout the woman, the medical aspects of the procedure aswell as pre- and post-abortion counselling and post-abortioncontraceptive decisions. Yet the form was not introduced intouse until March 1996, eight months after the law was in place,and then for only a handful of practitioners.
Keen to generate some baseline data, , a researcher conducteda one-week survey of ten providers and three private hospi-tals in February 1996, just before the Ministry finally issued thereporting form to the medical practitioners (Nunes, unpub-
Guyana
119
lished). Respondents were asked to give the survey to allwomen seeking abortions during that week. In that period,there were 316 terminations of pregnancy. Only two were non-residents of Guyana and one was under 15 years of age. Ex-trapolating from the remaining 313, the number of total abor-tions for a year would be 16,276. Given a female population(15-44) of 204,792, this gives an abortion rate of 79.5 per1,000 women between 15-44 per year. Given 22,500 birthsper year, that gives an abortion ratio of 42 per 100 knownpregnancies.
By working with women who reported this to be their first abor-tion, we were able to calculate the age-specific rates for thisgroup. We then extrapolated for a cohort of 1,000 womenthroughout their reproductive life to see how many would haveat least one abortion. The result, which we called ‘lifetime ortotal abortion risk’, was 720. The pattern shows a steep in-crease to age 24, but afterage 29 the slope is more gradual.The figures have great significance for public policy. They trans-form the paradigm of abortion from being a marginal experi-ence to a predominant, mainstream one for most women inpoor countries. Access to safe abortion is therefore a matter ofparamount public health importance for women’s reproduc-tive health. In all likelihood, a similar proportion of adult menwould probably have shared a sexual relationship resulting inat least one abortion. In other words, at least one abortionepisode is a majority experience among sexually active adults.
The measure, lifetime abortion risk, is only concerned withwomen having a first abortion. It does not count that womanagain if or when she has another abortion. Data from doctors’reports suggest that about two-thirds of the women in Guyanawho have one abortion will have at least one other abortion.
The social profile of data from the small study may be skewedsince it relied on private providers who were mostly based inurban areas. The results are nevertheless instructive, especiallysince the government in 2000 still does not provide an abor-tion service. The first observation is that 51% of the womenwho had abortions were married and another 22% were in
The Johannesburg Initiative
Advocating for abortion access
120
common law unions. These data challenge the stereotype thatwomen seeking abortions are careless, single and young. Sin-gle women were 46% of the population 15-44, but only 21%of those who had abortions. About 56% of the women whohad abortions had at least secondary education. This washigher than the general population where only 37% have thatmuch education. Less than 9% of those who had terminationswere teenagers. Women in their 20s accounted for 51% of theabortions, and 18% of the women who had terminations were35 or older. Since it is unlikely that a woman who voluntarilyseeks an abortion at or after 35 plans to have further children,the prospect of permanent contraception, especially for herpartner, needs to be a central part of counselling for these oldercouples. Some 14% of the women who had abortions had nochildren and 61% had two or fewer children. This suggeststhat delaying first birth or spacing is a major consideration forthese women.
Only 21% of the women were using contraceptives at thetime they became pregnant. Among this group of 65 women,48% were using the pill, and 34% were using a male con-dom. The need for transition to longer lasting, non-user de-pendent methods such as injectables, intra-uterine contra-ceptive devices, implants or surgery needs to be a consciouspart of contraceptive education. Yet knowledge of contra-ceptive methods was not the issue for these women. Theyknew an average of 3.4 methods and 32% knew five or moremethods. Yet 42% had never used any method. Learningmore about the factors that militate against use thus remainsa major challenge and is the path to reducing repeat abor-tions. Two thirds of the women (67%) who had terminationsin the week of the study reported that they had had previousinduced abortions. And 13% of the group had had at leastthree previous abortions.
Form F: Reporting by practitionersThe above data relate to information collected privately, fromoutside the bureaucacy and law. The reports that medicalpractitioners submit to the Ministry of Health (Form F) are
Guyana
121
clearly one of the successes of the period of implementation.They constitute a source of ongoing institutional data.
Immediately after the regulations appeared in the Gazette, thethen Chief Medical Officer (CMO) worked to get the modifiedforms printed. He distributed them to providers and urged themto comply with the requirement. That CMO left the Ministryshortly after that. The new CMO has shown little or no interestin the abortion law. He regards Form F as onerous and anundue burden on the practitioners. Further, some doctors be-lieve that reports of terminations may be used by the IncomeTax Department to assess their earnings and to investigate themfor the underpayment of taxes, which makes them reluctant tocomply. The new CMO has been sympathetic to these con-cerns and has not encouraged reporting.
In spite of the generally low level of compliance, the data aresignificant – as much for what they reveal as for the questionsthey raise. Firstly, they show that the fear of ‘abortion tourism’is unfounded. Almost all abortions (typically more than 99%)are for Guyanese women resident in the country. Second, ta-ble 1 reveals that only about 13% of all abortions are for teen-agers. Of these, almost 9% are for young women 18-19 yearsold. Women 20-29 routinely account for 53-55% of all abor-tions. Women in stable unions account for more abortions thansingle women. Most women who have abortions have sec-ondary education (more than 60%). The ethnic and religiouspatterns are a close mirror of the society. The vast majority ofreports (75%) of women having abortions are from the urbanarea containing the country’s capital city, Georgetown. In everyyear the majority of abortions are repeat abortions. About athird of the women who had abortions in any one year re-ported having had an abortion in the previous year.
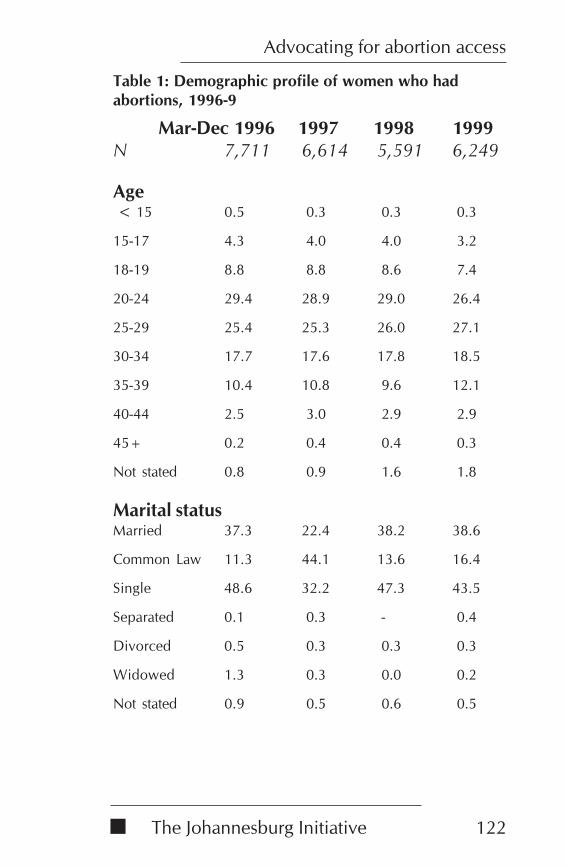
The Johannesburg Initiative
Advocating for abortion access
122
Table 1: Demographic profile of women who hadabortions, 1996-9
Mar-Dec 1996 1997 1998 1999N 7,711 6,614 5,591 6,249
Age < 15 0.5 0.3 0.3 0.3
15-17 4.3 4.0 4.0 3.2
18-19 8.8 8.8 8.6 7.4
20-24 29.4 28.9 29.0 26.4
25-29 25.4 25.3 26.0 27.1
30-34 17.7 17.6 17.8 18.5
35-39 10.4 10.8 9.6 12.1
40-44 2.5 3.0 2.9 2.9
45+ 0.2 0.4 0.4 0.3
Not stated 0.8 0.9 1.6 1.8
Marital statusMarried 37.3 22.4 38.2 38.6
Common Law 11.3 44.1 13.6 16.4
Single 48.6 32.2 47.3 43.5
Separated 0.1 0.3 - 0.4
Divorced 0.5 0.3 0.3 0.3
Widowed 1.3 0.3 0.0 0.2
Not stated 0.9 0.5 0.6 0.5
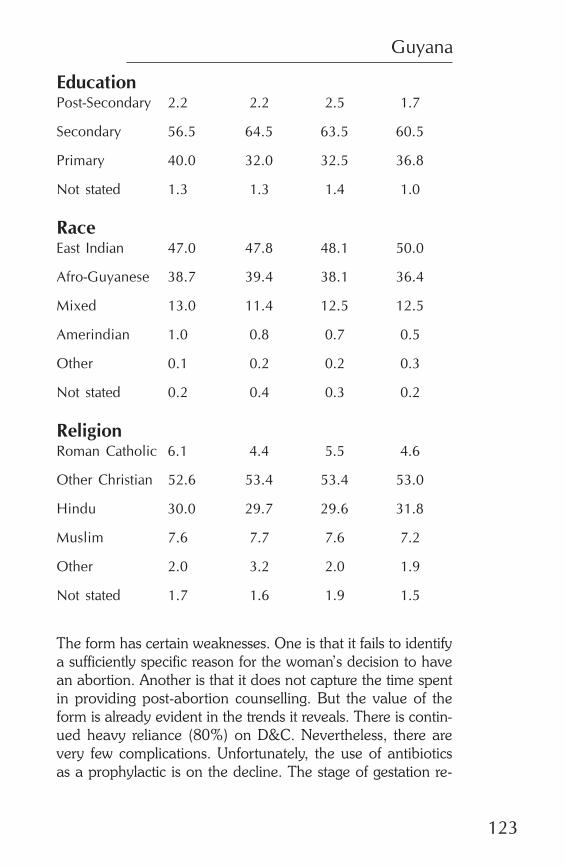
Guyana
123
EducationPost-Secondary 2.2 2.2 2.5 1.7
Secondary 56.5 64.5 63.5 60.5
Primary 40.0 32.0 32.5 36.8
Not stated 1.3 1.3 1.4 1.0
RaceEast Indian 47.0 47.8 48.1 50.0
Afro-Guyanese 38.7 39.4 38.1 36.4
Mixed 13.0 11.4 12.5 12.5
Amerindian 1.0 0.8 0.7 0.5
Other 0.1 0.2 0.2 0.3
Not stated 0.2 0.4 0.3 0.2
ReligionRoman Catholic 6.1 4.4 5.5 4.6
Other Christian 52.6 53.4 53.4 53.0
Hindu 30.0 29.7 29.6 31.8
Muslim 7.6 7.7 7.6 7.2
Other 2.0 3.2 2.0 1.9
Not stated 1.7 1.6 1.9 1.5
The form has certain weaknesses. One is that it fails to identifya sufficiently specific reason for the woman’s decision to havean abortion. Another is that it does not capture the time spentin providing post-abortion counselling. But the value of theform is already evident in the trends it reveals. There is contin-ued heavy reliance (80%) on D&C. Nevertheless, there arevery few complications. Unfortunately, the use of antibioticsas a prophylactic is on the decline. The stage of gestation re-
The Johannesburg Initiative
Advocating for abortion access
124
ported at termination suggests that two-thirds of all cases oc-cur in the first eight weeks. The high figure (67%) for earlyterminations could reflect women’s positive response to thelaw, which permits terminations ‘on request’ at that stage. Al-ternatively, it could represent an effort by practitioners to labelas ‘eight weeks,’ some that are in fact nine or more, in order tobe able to provide the service in their offices, as terminationsafter eight weeks must be done in an ‘approved institution’.
Analysis of the data on the source, method, duration and con-tent of counselling suggests that until there is an adequate cadreof trained counsellors, so that doctors are no longer the mainproviders of this service, the likelihood of satisfactory counsel-ling will remain minimal. In respect of contraceptive uptake, afull 27% of the women refused and in 1999 there was no reportfor 20%. This extent of non-reporting is indicative of the lack ofdiscipline and commitment to counselling by providers and theabsence of any effort at enforcement from the Ministry.
Among the practitioners who submit reports, there is a heavyreliance on hospitals (85%). If this is not representative, therecould be a whole legal service of office-based abortions that islargely outside of these benign reports. Of the reported cases,almost all (95%) are day cases. Yet the high reliance on D&Calso typically means an equally high reliance on general an-aesthesia. A switch to MVA could avoid this further risk.
Among those reporting, almost everyone (96%) provided serv-ices in Georgetown. The Ministry has not reached out to pro-viders across the country to submit reports. There has been noeffort by the Ministry to encourage all providers to report, orto encourage them to report all their terminations. Even at thetime of writing, the number of providers who report has neverexceeded 17, about half of the total believed to be deliveringservices. Further, if a doctor reports a single abortion for theyear, he or she shows up as a provider. We have no reason tobelieve that all of those who are reporting are duly reportingevery procedure they perform. We estimate that less than aquarter of the terminations actually performed, are being re-ported.
Guyana
125
The good news is that the Health Statistics Unit of the Ministryof Health has consistently produced quarterly compilations ofthe medical practitioners’ reports. These are made availableto the members of the Advisory Board and on special request– and with much reluctance – to researchers. The very sadnews is that, in spite of the powerful data that resides in thesetables, the Advisory Board is yet to make a single recommen-dation to the Minister, despite routinely receiving these tables.
Perhaps the most glaring weakness on the part of the Ministryis its failure to report on the services provided in public hospi-tals for women receiving treatment for complications of abor-tion. The reporting form for doctors specifically seeks informa-tion on procedures that are ‘to complete only’. These data areparticularly important for the short-term assessment of theimpact of the law. Indeed, the genesis of the law lay in thealarming incidence of admissions for abortion complications.That the government should fail to supply these data is a veryclear indicator of its disconnection from any objective assess-ment of its own venture into social engineering. The reluc-tance of the principal public institutions to conform to require-ments that the Act has imposed on private practitioners is aclear example of the Ministry’s disregard for the social impor-tance of its own law.
The need for these data are all the more important in a periodin which women have gained easy access to Cytotec(misoprostol) and are using it without the benefit of any proto-col. This is a situation in which both the Ministry and the Ad-visory Board should be taking the initiative in providing infor-mation to pharmacists and doctors and engaging in publiceducation. Women’s reproductive health is clearly not seen asa health priority by a male-dominated Ministry.
Advisory boardA major provision in the Act, which was given specific formin the regulations, was the creation of an Advisory Board.The body was to serve at least three purposes. One was toserve as a mechanism for ongoing monitoring of the impactof the law and of the conduct of medical practitioners under
The Johannesburg Initiative
Advocating for abortion access
126
the law. This would permit the body to advise the Minister ofthe need for any policy adjustments. Thus, rather than hav-ing to wait for a long period and an expensive commission,the ministry could readily learn what was working and whatneeded attention.
The second purpose was to create a forum for ongoing dia-logue between advocates and adversaries of the new law. Thiswas explicitly defined through the membership of the bodythat was to be composed entirely of non-governmental repre-sentatives from religious, medical and legal groups. The goalwas to continue the transparency of the debate, which was allabout intent and promise, into the period of implementationin order to allow for all parties to learn the reality of the situa-tion in operation. Would the liberal law result in an explosionof abortions? Would the net result be more harm to women’sreproductive health? Would the law have a devastating im-pact on the morals of young children? Would it result in adecline of interest in family planning? Would it result in publichospitals being swamped by women seeking terminations ofpregnancy? Or would it result in a reduction in the number ofadmissions for complications of abortion? Would women makeeven greater reliance on legal abortion as a method of fertilityregulation? And, above all, would the pre- and post-abortioncounselling introduced with a liberal abortion law result in adecline in reliance on abortion? The Board was designed tobe a forum in which persons with very different perspectivescould see the common data and learn from one other. It wasan opportunity for them to speak with passion andacquireinformation.
The third objective was that the Board would serve as a cen-tral point for information to be available to the public and fordiscourse with the public. As an autonomous and independ-ent body, it would command a certain measure of legitimacyand each representative would have considerable influenceamong their own constituencies. The Board would thereforebe a source for ongoing and informed dialogue with variouspublic groups.
Guyana
127
This critical body could not be established and these vital serv-ices could not begin until the regulations were in effect. Theloss of momentum was debilitating to the effect that, in its fiveyears of operation, it has failed to fulfil its purpose. The gov-ernment was tardy in following up on the enactment of thelaw. The four-month delay in issuing the regulations was acritical period during which the excitement of the debate dissi-pated. When The Minister finally attempted to convene theBoard, she met with resistance from religious groups. With oneor two exceptions, she was unable to attract the calibre of per-sons who could give stature and credibility to the Board.
In a political culture that is unschooled in dialogue, the pros-pects for the success of the body were small. The preference isfor central, top-down control. The dominant political currencyis power. The untidiness of dialogue with the need for flexibil-ity and the exercise of influence in the process of collabora-tion, are all novel constructs in the political arena even withinthe parties, let alone between them and civil society. It is notsurprising, then, that the Minister was slow to convene thisBoard. It met for the first time more than a year after the lawpassed.
But the delay was not all of the Minister’s making. She actedwith courage and determination once she decided to put it inplace. One appointment was particularly significant in that shewas successful in attracting onto the Board a strong and ar-ticulate female leader of the opposition party. As a shadowMinister of Health Dr Faith Harding had been a strong critic ofthe Minister, but nevertheless agreed to serve on the Board.Both women held women’s health needs above their partisandifferences
The problem lay elsewhere, with the far right religious groupthat was hostile to the very notion of sitting and learning to-gether. Those adversaries worked hard to discourage religiousleaders whom the Minister invited to join the Advisory Boardfrom accepting her invitations. And they succeeded. This wasa major loss. The real challenge to law reform had come formthe religious right. That was the source that challenged the
The Johannesburg Initiative
Advocating for abortion access
128
PRG’s data and countered it with references to data from othercountries. It was the religious right that organised two largestreet demonstrations. Any advisory body without a substan-tial presence of the religious leadership known to oppose thelaw would lack legitimacy. Without the energy of oppositionfrom high profile religious adversaries, the Board has nevercommanded either the authenticity or the credibility it neededto gain any meaningful public stature.
The Advisory Board was finally convened in mid-1996. Ex-cept for the former Shadow Minister of Health, Faith Harding,none of the personalities that had given spark to the debatewere on the Board. It was slow to get going and from the out-set was marred by poor attendance. Further, in spite of re-quests for secretarial and budgetary support, the Board re-ceived neither for its first four critical years. Only in 2000 did itreceive some limited secretarial support for its monthly meet-ing. In 2001, for the first time, the Ministry’s budget made someprovision for its operation.
The Ministry left the Board to find its own way. It struggled formonths over the simple question of whether it could reportonly to the Minister of Health or had the capacity to makepublic statements on its own behalf. The body was torn be-tween those who felt strictly obligated to the Minister and oth-ers who saw their role on a far broader scale. Just as the Boardwas beginning to find its way, its first chairperson suffered anuntimely death.
Her death precipitated the Board’s first real crisis. How shoulda successor chairperson be chosen? The regulations containedno guidelines on this important matter. Some members felt itshould be left to them to make that determination, but theMinister of Health insisted on selecting the chair. For at leasttwo members, that was their last meeting. The new chairper-son Frederick Cox was the head of the local affiliate of theInternational Planned Parenthood Federation, the GuyanaResponsible Parenthood Association (GRPA). That body hadbarely participated in the campaign for the new law and haddone nothing to provide services since the law. Cox has not
Guyana
129
managed to give leadership to the Board. He travels frequentlyand does not allow the Board to meet in his absence. It isunder his stewardship that the Board has, for four years, hadan unblemished record of not making a single recommenda-tion to the Minister of Health.
The Advisory Board thus remains a pivotal body, but unless itcan attract a medical representative and conservative, religiousleadership, it is unlikely to approach the purposes for which itwas created.
The Board was an early casualty of the loss of momentum.Initially, the plan was to train the members in the skills of con-ducting meetings, interpreting statistics, listening skills, meet-ing with stakeholders, hearing their own constituents, dealingwith the media and so on. None of this was done. The Boardmembers were ‘named’ and that was that. Largely lacking skillsfor the task, with a few notable exceptions, they have oftenbeen far out of their depth.
The Board lacks the skills to address the complex task it faces.This is clearly evident in its incapacity to make any use of therich data it receives routinely from the Ministry’s Health Statis-tics Unit. In four years of meetings, the Board has been unableto have discourse with a single group.
Family Planning Association of GuyanaIn spite of the weak performance of the government, and per-haps because of it, a small NGO has been able to providecomprehensive reproductive services, including an abortionservice. The body was created in April 1995, a few weeks be-fore the new law was passed, in accurate anticipation that nei-ther the Ministry nor the long-established GRPA would takeaction to provide abortion services to poor women. At the timeof writing, that assumption remains, unfortunately, accurate.
The Family Planning Association of Guyana (FPAG), with for-eign funding, has trained more than 30 counsellors and seventraining counsellors to train others. It has trained doctors inMVA. It boasts an uptake of post-abortion contraception ofalmost 100%. It provides an outreach community-based dis-
The Johannesburg Initiative
Advocating for abortion access
130
tribution service in squatter areas around Georgetown. And ithas met or exceeded all its service targets in the last year interms of new clients, continuing clients, and abortion services.On a small scale, it is doing what the Ministry should be doing.But there is no way that a tiny NGO can take the place of animportant public institution. One measure of FPAG’s progressis that it has had to move from its original location because ithad outgrown its first home. All the terminations done by FPAGare provided by MVA and under local anaesthetic.
Political fortunesPresident Cheddi Jagan died before the general elections ofDecember 1997. His wife and life-long political ally, JanetJagan took leadership of the party. In the 1960s, she hadbeen Minister of Health. It was a matter of public knowledgethat there was more than a passing tension between the firstlady, Janet Jagan and Gail Teixeira, the Minister of Health.While Cheddi led the party and the country, he was a sourceof temperance between the two. Following the contentiouselection of 1997, Janet Jagan assumed the Presidency andGail Teixeira was reassigned to the Ministry of Youth, Sportsand Culture. A political scientist, Dr Henry Jeffrey, was ap-pointed Minister of Health. Unlike Teixeira, who clearly hada definite commitment to women’s need for access to safeabortion, Jeffrey seems quite indifferent and evidently regardsthe noise about abortion as a mere nuisance. Service deliv-ery appears secondary to his grand interests in health sectorreform. Besides, Jeffrey is also Minister of Labour. And inthat role he was deeply involved in a protracted civil servicestrike that ended in bitter arbitration. Abortion has simplynot been on his agenda.
Even before the PPP administration took office in 1992, therehad been feuding between the Guyana Medical Associationand the Ministry of Health. Those lines of combat were accen-tuated during Teixeira’s tenure and have hardened into legalwarfare under Jeffrey. It is not surprising that the AdvisoryBoard has functioned without any medical representative forat least a year.
Guyana
131
With the demise of the PRG, no other civil group has takenany interest in being vigilant about making the law work. Indi-vidual members of the former PRG still write strong letters tothe press and a supportive media gives coverage to their ef-forts, but the Ministry’s intransigence persists. The culture ofthe institution is one of passive resistance. There seems to bean abiding faith that inertia overcomes all things. Where therewere officers who might have exercised some leverage, theywould disappear to study abroad for several months. In a smallMinistry, those absences were crucial.
The small group of people who constituted the PRG wereemotionally and financially exhausted by a campaign that hadlasted for longer than they had ever expected. They had stuckdoggedly to the task of winning a new law. Once that wassecured, they soon lost sight of the larger purpose of a civil law– to provide access to safe abortion for all women. Sensingvictory in winning the new law, they too readily abandonedtheir advocacy for access to safe services. The emigration of afew key members was enough to end the vitality of the PRG.
Lessons learnedThe main lessons for implementation can be expressed as fol-lows:
• During the process of law reform, advocates were notsufficiently mindful of the allies they would need duringimplementation. They did not appreciate how much thecharacter of the campaign would shape the character ofimplementation.
• While the process of law reform was inevitably political,it was essential to engage the administrative and techni-cal cadre of the implementing (Health) or other relevantministries (for example, Education, or Women’s Affairs)as part of an effective strategy. The PRG did not makeadequate efforts in this area.
• Leaving implementation of a major new initiative to analready resource-strained administrative system is haz-ardous. It would have been prudent to assign responsi-
The Johannesburg Initiative
Advocating for abortion access
132
bility for implementation to a specific, small, multi-skilledproject team, complete with budget, planning scheduleand reporting responsibilities.
• Given the resource scarcity in Guyana, in the early stagesof implementation it would have been wise to select spe-cific targets for effective action – for example, a singlehospital or a single nursing school - from which manag-ers can have quick wins and whose lessons can be repli-cated.
• The wisdom of the religious right in withdrawing fromthe public arena once the law was passed removed theclear need for the PRG to work at consolidating the law,or for the government to ensure that the law deliveredas it had promised. The PRG should not have been soeasily lulled. The PRG needed to persist with the politi-cal work necessary for consolidating the law into the so-cial consciousness. The absence of active religious op-position was not sufficient reason for the PRG to relax itsefforts.
• The optimistic presumption that a new law would changethe social dynamic and unleash new energies ofvoluntarism was without foundation. The failures ofmobilisation during the campaign persisted to haunt theprocess of implementation. A corollary of this observa-tion is the need for members of the PRG to commit them-selves to work beyond the formal enactment of law,through the long process of implementation towards thebroad social justice goal of real access to safe services forall women.
• Political leaders, however charismatic and committed,are seldom the sole agents of their own destiny. Advo-cates should be mindful of the risks of putting all theireggs on such a fragile political platform. That risk shouldbe avoided or at least hedged by contingency plans.
• International networking was an invaluable source oftechnical expertise and resources during the campaign

Guyana
133
for law reform. But these resources should have beenharnessed to build local capacity. Because this was notdone, their impact ended with the campaign, and advo-cates in Guyana were left vulnerable. Failing to invest indeveloping international linkages for the less glamoroustasks of implementation and service provision was alsoa mistake.
ReferencesNunes F & Delph Y (1995) ‘Making Abortion Law ReformHappen in Guyana: A Success Story’ in Reproductive HealthMatters 6:12-23.
Nunes F (unpublished) Contraceptive knowledge and behav-iour among women seeking legal abortions in Guyana, in 1996.
AuthorFred Nunes is a researcher and advocate for safe motherhood.He was a central activist in the 1993-95 campaign for abor-tion law reform in Guyana. He considers himself ‘pro-life, pro-choice and pro-reform’ and contends that liberal laws are onepath for reducing the incidence of abortion.

The Johannesburg Initiative
Advocating for abortion access
134
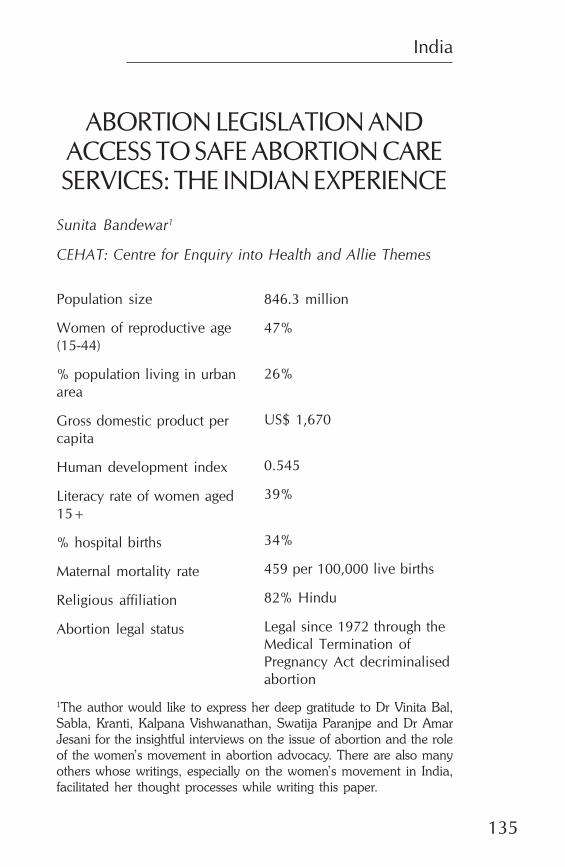
India
135
ABORTION LEGISLATION ANDACCESS TO SAFE ABORTION CARESERVICES: THE INDIAN EXPERIENCE
Sunita Bandewar1
CEHAT: Centre for Enquiry into Health and Allie Themes
Population size
Women of reproductive age(15-44)
% population living in urbanarea
Gross domestic product percapita
Human development index
Literacy rate of women aged15+
% hospital births
Maternal mortality rate
Religious affiliation
Abortion legal status
846.3 million
47%
26%
US$ 1,670
0.545
39%
34%
459 per 100,000 live births
82% Hindu
Legal since 1972 through theMedical Termination ofPregnancy Act decriminalisedabortion
1The author would like to express her deep gratitude to Dr Vinita Bal,Sabla, Kranti, Kalpana Vishwanathan, Swatija Paranjpe and Dr AmarJesani for the insightful interviews on the issue of abortion and the roleof the women’s movement in abortion advocacy. There are also manyothers whose writings, especially on the women’s movement in India,facilitated her thought processes while writing this paper.
The Johannesburg Initiative
Advocating for abortion access
136
IntroductionThe Medical Termination of Pregnancy (MTP) Act was passedin India in 1971. The Act, implemented in 1972, decriminalisedabortion. The manner in which the Act is implemented re-mains inadequate, however, and the quality of care availableto women seeking abortion care at institutions and elsewhereis very poor. This chapter presents a critique of the legislation,examines the process through which the Act came into being,provides information about current access and documents ad-vocacy efforts aimed at improving access to safe, legal andaffordable abortion care services.
The chapter is primarily a documentation of the abortion ad-vocacy initiative of the group to which the author belongs andso relies considerably on personal knowledge and experience.Earlier writings on the MTP legislation and women’s move-ment provided background material. Additional informationon the role of the women’s movement was obtained throughinterviews with representatives of women’s organisations.
The MTP actThe content and the critiqueTwo aspects of the Act are particularly noteworthy. Firstly, theIndian legislation represented the first time in the world thatabortion was made legal in cases of the failure of contracep-tion. Secondly, the legislation did not require the husband’sconsent for abortion. Despite these strengths, the Act can becriticised for the power it gives medical practitioners. Otherweaknesses are described below:
The Act stated that a termination up to twelve weeks had to beapproved by a single registered medical practitioner, while it

India
137
needed the approval of two medical practitioners betweentwelve and twenty weeks. The practitioners had to testify thatcontinuing the pregnancy would place the life or physical ormental health of the woman at risk, or that there was signifi-cant risk that the child would suffer from serious physical ormental abnormalities. Within these definitions, a pregnancycaused by rape was considered to pose a serious threat to themental health of the woman, as was the failure of contracep-tion.
While the Act was relatively liberal in its clauses, it establishedmedical practitioners as the ultimate gatekeepers. Further, thefact that failure of contraception was only considered a justcause for married women was evidence of a moralistic posi-tion concerning women’s sexuality which links the use of con-traception with her marital status. This linkage precludes allother situations in which a woman may express her sexualityleading to an unwanted or unintended pregnancy.
The Act is open to differing interpretations by medical provid-ers engaged in abortion care services. To date the interpreta-tion of the law has been liberal. This could partly reflect thegovernment’s preoccupation with population control or themedical profession’s commercial motivation. Nevertheless, thepossibility remains that the Act could be interpreted restric-tively without a singleword of the text being altered (Jesaniand Iyer, 1993).
Few abortion care facilities are ‘stand-alone’. Most are situ-ated either in the general health care service facilities or inmaternity care centres. The MTP Act specifies the need forabortion-specific instruments. The standards do not cover theother minimum physical standards at the health care facilitiesat which abortion care services are situated.
The only medical legislation which covers general minimumstandards is the Bombay Nursing Home Act of 1949 whichcovers the urban area of the state of Maharashtra and otherprovincial legislation, such as the Tamil Nadu Private ClinicalEstablishments Regulation Act of 1997. In the absence of any
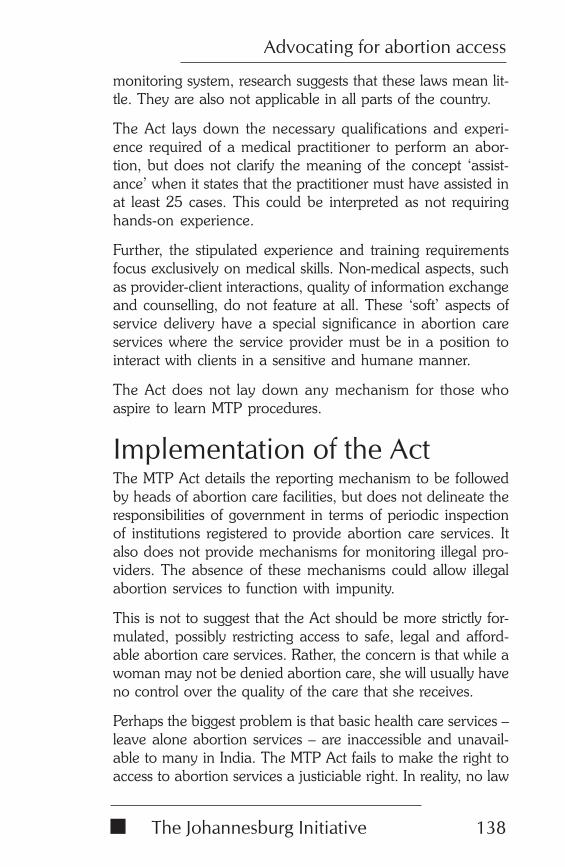
The Johannesburg Initiative
Advocating for abortion access
138
monitoring system, research suggests that these laws mean lit-tle. They are also not applicable in all parts of the country.
The Act lays down the necessary qualifications and experi-ence required of a medical practitioner to perform an abor-tion, but does not clarify the meaning of the concept ‘assist-ance’ when it states that the practitioner must have assisted inat least 25 cases. This could be interpreted as not requiringhands-on experience.
Further, the stipulated experience and training requirementsfocus exclusively on medical skills. Non-medical aspects, suchas provider-client interactions, quality of information exchangeand counselling, do not feature at all. These ‘soft’ aspects ofservice delivery have a special significance in abortion careservices where the service provider must be in a position tointeract with clients in a sensitive and humane manner.
The Act does not lay down any mechanism for those whoaspire to learn MTP procedures.
Implementation of the ActThe MTP Act details the reporting mechanism to be followedby heads of abortion care facilities, but does not delineate theresponsibilities of government in terms of periodic inspectionof institutions registered to provide abortion care services. Italso does not provide mechanisms for monitoring illegal pro-viders. The absence of these mechanisms could allow illegalabortion services to function with impunity.
This is not to suggest that the Act should be more strictly for-mulated, possibly restricting access to safe, legal and afford-able abortion care services. Rather, the concern is that while awoman may not be denied abortion care, she will usually haveno control over the quality of the care that she receives.
Perhaps the biggest problem is that basic health care services –leave alone abortion services – are inaccessible and unavail-able to many in India. The MTP Act fails to make the right toaccess to abortion services a justiciable right. In reality, no law
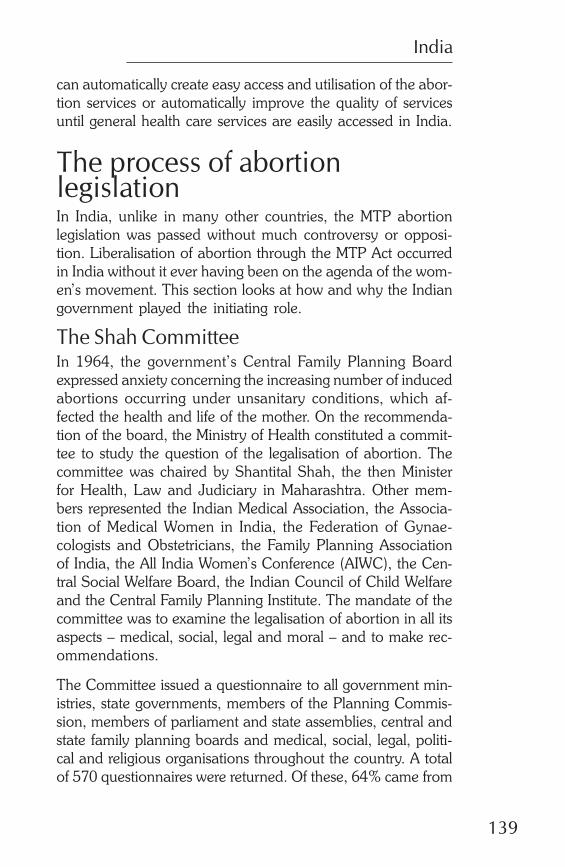
India
139
can automatically create easy access and utilisation of the abor-tion services or automatically improve the quality of servicesuntil general health care services are easily accessed in India.
The process of abortionlegislationIn India, unlike in many other countries, the MTP abortionlegislation was passed without much controversy or opposi-tion. Liberalisation of abortion through the MTP Act occurredin India without it ever having been on the agenda of the wom-en’s movement. This section looks at how and why the Indiangovernment played the initiating role.
The Shah CommitteeIn 1964, the government’s Central Family Planning Boardexpressed anxiety concerning the increasing number of inducedabortions occurring under unsanitary conditions, which af-fected the health and life of the mother. On the recommenda-tion of the board, the Ministry of Health constituted a commit-tee to study the question of the legalisation of abortion. Thecommittee was chaired by Shantital Shah, the then Ministerfor Health, Law and Judiciary in Maharashtra. Other mem-bers represented the Indian Medical Association, the Associa-tion of Medical Women in India, the Federation of Gynae-cologists and Obstetricians, the Family Planning Associationof India, the All India Women’s Conference (AIWC), the Cen-tral Social Welfare Board, the Indian Council of Child Welfareand the Central Family Planning Institute. The mandate of thecommittee was to examine the legalisation of abortion in all itsaspects – medical, social, legal and moral – and to make rec-ommendations.
The Committee issued a questionnaire to all government min-istries, state governments, members of the Planning Commis-sion, members of parliament and state assemblies, central andstate family planning boards and medical, social, legal, politi-cal and religious organisations throughout the country. A totalof 570 questionnaires were returned. Of these, 64% came from
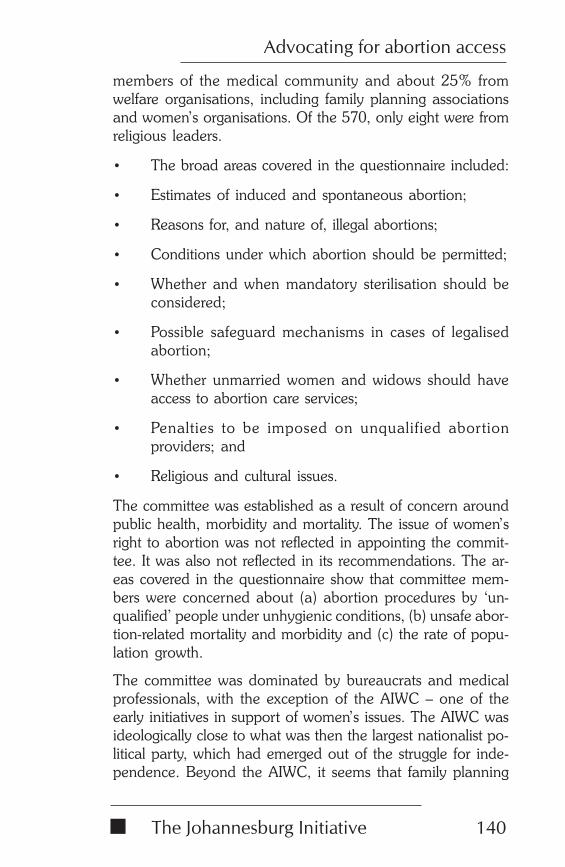
The Johannesburg Initiative
Advocating for abortion access
140
members of the medical community and about 25% fromwelfare organisations, including family planning associationsand women’s organisations. Of the 570, only eight were fromreligious leaders.
• The broad areas covered in the questionnaire included:
• Estimates of induced and spontaneous abortion;
• Reasons for, and nature of, illegal abortions;
• Conditions under which abortion should be permitted;
• Whether and when mandatory sterilisation should beconsidered;
• Possible safeguard mechanisms in cases of legalisedabortion;
• Whether unmarried women and widows should haveaccess to abortion care services;
• Penalties to be imposed on unqualified abortionproviders; and
• Religious and cultural issues.
The committee was established as a result of concern aroundpublic health, morbidity and mortality. The issue of women’sright to abortion was not reflected in appointing the commit-tee. It was also not reflected in its recommendations. The ar-eas covered in the questionnaire show that committee mem-bers were concerned about (a) abortion procedures by ‘un-qualified’ people under unhygienic conditions, (b) unsafe abor-tion-related mortality and morbidity and (c) the rate of popu-lation growth.
The committee was dominated by bureaucrats and medicalprofessionals, with the exception of the AIWC – one of theearly initiatives in support of women’s issues. The AIWC wasideologically close to what was then the largest nationalist po-litical party, which had emerged out of the struggle for inde-pendence. Beyond the AIWC, it seems that family planning
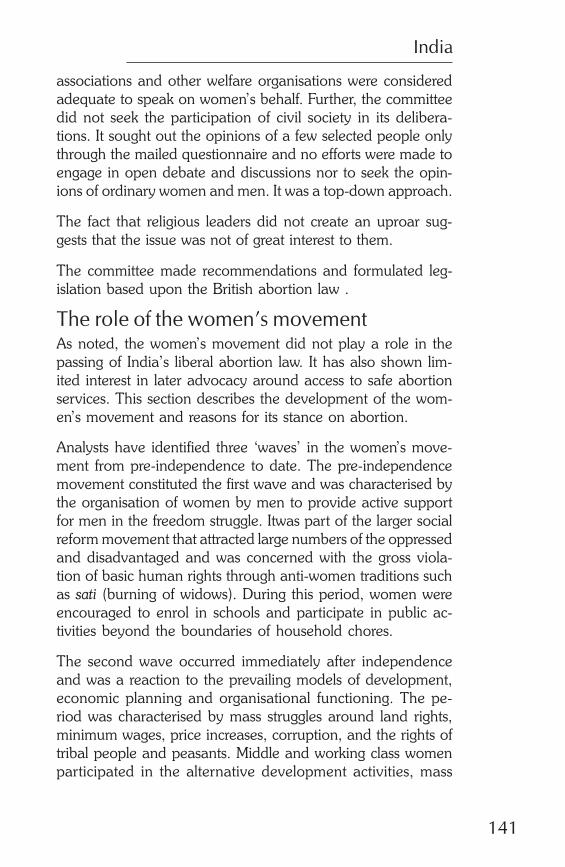
India
141
associations and other welfare organisations were consideredadequate to speak on women’s behalf. Further, the committeedid not seek the participation of civil society in its delibera-tions. It sought out the opinions of a few selected people onlythrough the mailed questionnaire and no efforts were made toengage in open debate and discussions nor to seek the opin-ions of ordinary women and men. It was a top-down approach.
The fact that religious leaders did not create an uproar sug-gests that the issue was not of great interest to them.
The committee made recommendations and formulated leg-islation based upon the British abortion law .
The role of the women’s movementAs noted, the women’s movement did not play a role in thepassing of India’s liberal abortion law. It has also shown lim-ited interest in later advocacy around access to safe abortionservices. This section describes the development of the wom-en’s movement and reasons for its stance on abortion.
Analysts have identified three ‘waves’ in the women’s move-ment from pre-independence to date. The pre-independencemovement constituted the first wave and was characterised bythe organisation of women by men to provide active supportfor men in the freedom struggle. Itwas part of the larger socialreform movement that attracted large numbers of the oppressedand disadvantaged and was concerned with the gross viola-tion of basic human rights through anti-women traditions suchas sati (burning of widows). During this period, women wereencouraged to enrol in schools and participate in public ac-tivities beyond the boundaries of household chores.
The second wave occurred immediately after independenceand was a reaction to the prevailing models of development,economic planning and organisational functioning. The pe-riod was characterised by mass struggles around land rights,minimum wages, price increases, corruption, and the rights oftribal people and peasants. Middle and working class womenparticipated in the alternative development activities, mass
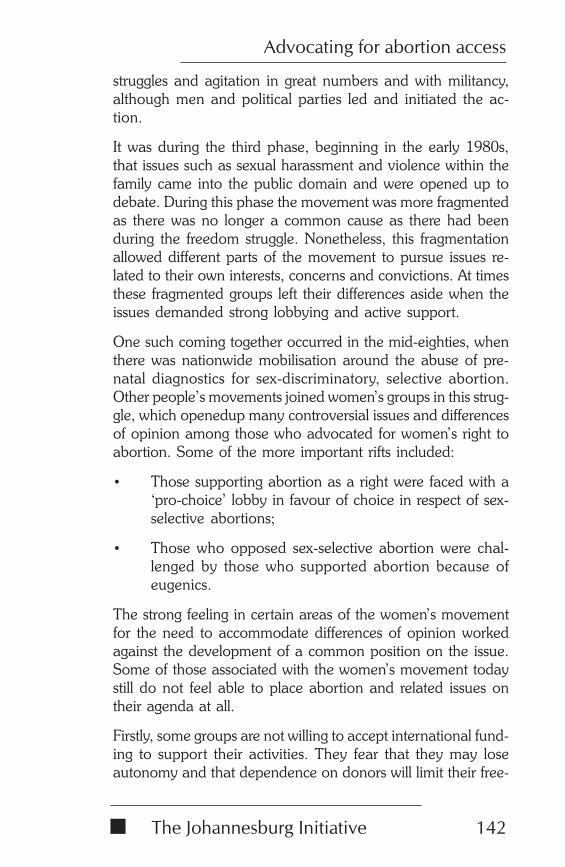
The Johannesburg Initiative
Advocating for abortion access
142
struggles and agitation in great numbers and with militancy,although men and political parties led and initiated the ac-tion.
It was during the third phase, beginning in the early 1980s,that issues such as sexual harassment and violence within thefamily came into the public domain and were opened up todebate. During this phase the movement was more fragmentedas there was no longer a common cause as there had beenduring the freedom struggle. Nonetheless, this fragmentationallowed different parts of the movement to pursue issues re-lated to their own interests, concerns and convictions. At timesthese fragmented groups left their differences aside when theissues demanded strong lobbying and active support.
One such coming together occurred in the mid-eighties, whenthere was nationwide mobilisation around the abuse of pre-natal diagnostics for sex-discriminatory, selective abortion.Other people’s movements joined women’s groups in this strug-gle, which openedup many controversial issues and differencesof opinion among those who advocated for women’s right toabortion. Some of the more important rifts included:
• Those supporting abortion as a right were faced with a‘pro-choice’ lobby in favour of choice in respect of sex-selective abortions;
• Those who opposed sex-selective abortion were chal-lenged by those who supported abortion because ofeugenics.
The strong feeling in certain areas of the women’s movementfor the need to accommodate differences of opinion workedagainst the development of a common position on the issue.Some of those associated with the women’s movement todaystill do not feel able to place abortion and related issues ontheir agenda at all.
Firstly, some groups are not willing to accept international fund-ing to support their activities. They fear that they may loseautonomy and that dependence on donors will limit their free-
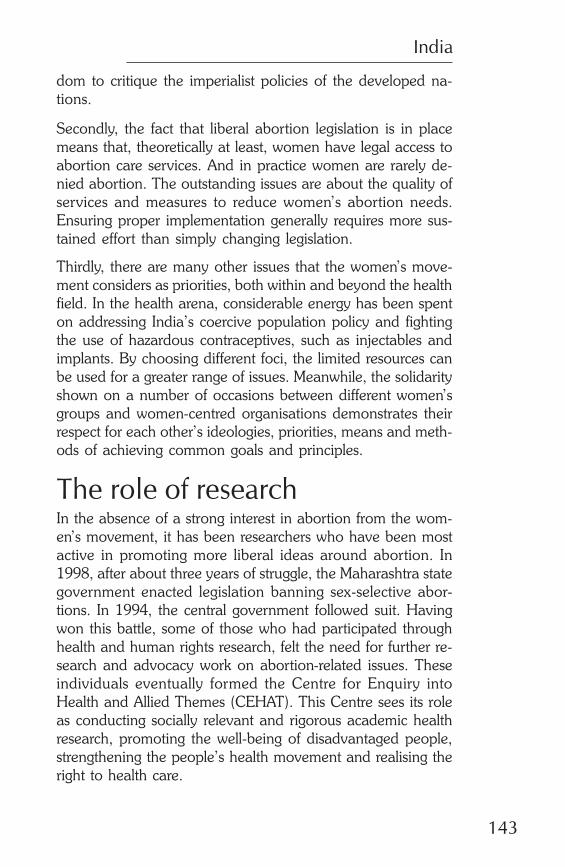
India
143
dom to critique the imperialist policies of the developed na-tions.
Secondly, the fact that liberal abortion legislation is in placemeans that, theoretically at least, women have legal access toabortion care services. And in practice women are rarely de-nied abortion. The outstanding issues are about the quality ofservices and measures to reduce women’s abortion needs.Ensuring proper implementation generally requires more sus-tained effort than simply changing legislation.
Thirdly, there are many other issues that the women’s move-ment considers as priorities, both within and beyond the healthfield. In the health arena, considerable energy has been spenton addressing India’s coercive population policy and fightingthe use of hazardous contraceptives, such as injectables andimplants. By choosing different foci, the limited resources canbe used for a greater range of issues. Meanwhile, the solidarityshown on a number of occasions between different women’sgroups and women-centred organisations demonstrates theirrespect for each other’s ideologies, priorities, means and meth-ods of achieving common goals and principles.
The role of researchIn the absence of a strong interest in abortion from the wom-en’s movement, it has been researchers who have been mostactive in promoting more liberal ideas around abortion. In1998, after about three years of struggle, the Maharashtra stategovernment enacted legislation banning sex-selective abor-tions. In 1994, the central government followed suit. Havingwon this battle, some of those who had participated throughhealth and human rights research, felt the need for further re-search and advocacy work on abortion-related issues. Theseindividuals eventually formed the Centre for Enquiry intoHealth and Allied Themes (CEHAT). This Centre sees its roleas conducting socially relevant and rigorous academic healthresearch, promoting the well-being of disadvantaged people,strengthening the people’s health movement and realising theright to health care.
The Johannesburg Initiative
Advocating for abortion access
144
When CEHAT was formed, most of the existing research onabortion had focused on the extent to which the legislationhad contributed to fertility reduction and to understanding thesocio-economic and demographic profile of women seekingabortion care services. There was little or no attention paid inresearch to improving the quality of services or the extent towhich the legislation safeguarded women’s health by prevent-ing exposure to unsafe abortion services.
Indications that the legislation was not being properly imple-mented prompted CEHAT to start with a scenario analysis ofinduced abortions in India and of the health care system moregenerally. The second focus was a critical examination of thecontent of the legislation to ascertain why it was not providingthe hoped-for benefits for women.
CEHAT’s examination of the health care system exposed:
• the inadequacy of services provided to the rural popula-tion by both the public and private health care sectors;
• the inadequate equipping in terms of staff and infrastruc-ture of the primary health centres which constitute thelowest level of the state health care delivery system inIndia;
• the fact that, in the absence of adequate public healthservices, many people were seeking health care fromprivate providers who were charging exorbitant fees;
• the lack of regulation of private sector provision.
The research into abortion services found that the number ofMTP institutions increased about fivefold between 1972 and1997. The number of MTPs performed at these institutionsover the same period increased by only about 40%, suggest-ing more widespread access, but fewer abortions performedper institution.
Despite the increase, there is still far less provision than therecould be. There were over 22,010 primary health centres, 2,662community health centres, and 13,692 hospitals in India in1997 (Ministry of Health and Family Welfare (MOHFW)), all
India
145
of which were eligible under the MTP Act to offer MTP facili-ties. Yet only 8,891, or 23%, of these were approved MTPinstitutions. The institutions each conducted, on average, 61legal induced abortions every year. If these institutions were toconduct all the estimated 4.7 million induced abortions (Jesani& Iyer, 1993) in the country, they would be required to per-form an average of 529 abortions each year. Such a nine-foldincrease in work would seriously compromise the quality ofcare unless something is done to increase the number of regis-tered institutions. To make matters worse, the available serv-ices are distributed unequally within the states, between pri-vate and public sectors, and between rural and urban.
The findings of CEHAT’s examination of the legislation aresummarised in the critique of the legislation above.
As CEHAT took forward its abortion research and advocacyagenda in the 1990s, other groups also pursued research thatcontributed to understanding the abortion issue. The initia-tives included a national level study on illegal abortion con-ducted by the governmental Indian Council for Medical Re-search, a community-based study of induced abortion con-ducted by King Edward Memorial Hospital Research Centrein Pune and an assessment of the quality of institutional-basedabortion care conducted by the Centre for Operation Researchand Training.
Combining research and advocacyThe research process helped CEHAT identify the constituen-cies which could be influenced by the proposed advocacy ini-tiative. The most important constituencies were the state ma-chinery, the medical community and ordinary women andmen. Given limited resources, CEHAT decided to limit its ad-vocacy efforts to the state or provincial level. The discussionwhich follows describes, chronologically, what CEHAT stud-ied and how it embarked on advocacy in respect of each.
Women’s needsCEHAT utilised a community-based, qualitative approach. Theresearch was woman-centred, and removed from the popula-
The Johannesburg Initiative
Advocating for abortion access
146
tion control perspective that dominated abortion research forthe two decades after legalisation. The research revealed thatwomen were largely unaware of the fact that abortion islegaland provided free of charge at public health care facili-ties, including PHCs. When the legislation and situation wasexplained to them, most were in favour of universal access toabortion care services.
Their concerns in seeking abortion care were not identical toconcerns in other health-seeking situations. While womenopted for abortion in a range of situations, they were not freeof moral dilemmas and feelings of guilt about doing so. Aseven talking about abortion remained taboo, CEHAT foundthat women attached considerable importance to confidenti-ality, speed of service and the husband’s signature not beingcompulsory (Gupte et al, 1999). The fact that many womenappeared willing to trade safety and quality of care considera-tions for assured confidentiality helps explain why the privatesector is often the preferred source for abortion care services.
Advocacy: Issues and strategiesCEHAT chose as its advocacy goals the development of amechanism for building awareness in society about abortionlegislation and for changing attitudes. The organisaiton pre-pared a booklet and slideshow in the local language, whichcovered the medical, legal, socio-cultural and political aspectsof abortion. The materials were prepared with the participa-tion of the women from the community and drew heavily onthe insights gained in the research. To date, about 3,000 cop-ies of the booklet have been disseminated.
While 3,000 is a small number for dissemination to the popu-lation, the materials have reached larger numbers through theuse of networks. For example, the materials have been used ina ‘Women and Health’ initiative, which brings together a state-wide network of NGOs working on women’s health and re-lated issues. Middle-level health workers in these NGOs un-derwent a year-long training programme on gender-sensitivewomen’s health care. The workers are members of the com-
India
147
munities in which they work and thus ideally placed to takethe message further.
The booklet was launched at a public function that was openedby the Deputy Director of Health Services in the state and towhich CEHAT invited NGOs and women’s groups, activists,people’s organisations, office-holders of medical associations,leading gynaecologists and the press. A gynaecologist, wom-en’s activists, and the Deputy Director shared the platform toexpress their views about women’s health and women’s abor-tion needs. The public function served as an expression ofsolidarity among the groups and a collective commitment tothe cause.
CEHAT also attempted to provide the resource material toservice providers constituting the upper cadre of the state’spublic health sector. These were the civil surgeons who are thechief medical officers in districts and officials at the state-rundistrict hospital who are responsible for overseeing MTP per-formance and approval of centres in their districts. There wasalso some outreach to grassroots health workers from the pub-lic health care sector. Unfortunately, despite their attempts,CEHAT was unable to use the official Information, Educationand Communication (IEC) Bureau to disseminate the book-let. It seemed that CEHAT would have to pay for this facilityand perhaps also contribute in terms of labour. The organisa-tion chose instead to devote its energies to disseminating thematerial through the NGO networks.
The slideshow was designed for illiterate and newly literatepeople and contained visuals as well as text. It was primarilyused in training programmes, especially to train trainers. Dis-semination was constrained by the need for a slide-projector,basic training for animators and the costs involved in these. Itwas thus comparatively less accessible than the booklet de-spite its tremendous educational potential. The NGOs whichserved as anchors for large networks of smaller grassrootsgroups were able to use the slideshow in combination with thebooklets.
The Johannesburg Initiative
Advocating for abortion access
148
The above efforts to disseminate the booklet and slideshow weregeared to the large rural population. For the urban population,CEHAT made use of the mass media, especially the local press.The organisation wrote articles for daily and weekly newspa-pers and received some positive response from readers.
Expansion of abortion servicesGiven the inadequacy of current service provision, CEHAT’sresearch:
• Explored ways of accommodating medical profession-als other than the practitioners of allopathy who are cur-rently the only ones legally allowed to provide abortioncare services;
• Explored the feasibility of introducing abortion methodssuch as manual vacuum aspiration (MVA) andmisoprostol (RU486); and
• Explored the feasibility of involving paramedics in abor-tion service provision.
The research looked at both legal and medical feasibility anddrew on the experience of other countries, both with similarandcontrasting health care systems and health status. The re-search also examined the capacities and skills that existingmedical and nursing courses impart, particularly to studentsof Indian systems of medicines.
Advocacy: Issues and strategiesIn conducting this research over a four-year period, CEHATinteracted with women’ groups and grassroots organisations,health activists, the medical community, the nursing andparamedic community and state administrators. This interac-tion gave visibility to the issue and built awareness.
CEHAT organised a state level consultation in 1998 for whichit prepared background discussion papers. The organisationalso invited representatives of other constituencies to share theirperspectives on alternative methods for expanding abortion
India
149
care services. Invitees included medical officers from the pub-lic health care sector, office-holders of the medical and nurs-ing association, women’s groups involved in running trainingprogrammes for grassroots level health workers and middle-level health workers engaged in service provision. CEHATdecided not to invite state representatives as they feared it mighthinder open dialogue among the other representatives.
As anticipated, many of the issues were not resolved as par-ticipants held often divergent views about them. The allopathswere against any expansion on the grounds that MVA is not amethod with acceptable efficacy. The allopaths also did notapprove of the idea of accommodating medical practitionersfrom other systems of medicine for abortion service provision.
As regards paramedics, CEHAT had thought that impartingskills would help to change the power relationship betweenthem and those with more formal qualifications. Paramedicswere not willing to take on any additional duties, however,given their responsibility for all the work in the state’s FamilyWelfare Programme.
Only the women’s health activists were prepared to explorethe involvement of paramedics in MVA. They were also infavour of promoting other medical methods of menstrual regu-lation such as misoprostol. However, they emphasised thatimproving the existing public health care system was essential.They cautioned that, in the absence of an improved and ac-countable health care system, introducing such methods wouldonly add to women’s suffering.
The different opinions highlighted the conflicting interests ofthe constituencies. The consultation also gave CEHAT, as ad-vocates, greater clarity as to which issues to tackle in the short,medium and longer term. For example, expansion of servicesseems to present a tougher challenge for advocacy purposes,especially as it is still in the conception phase. It is perhapseasier to concentrate on those issues related to improvementof the quality of existing abortion services.
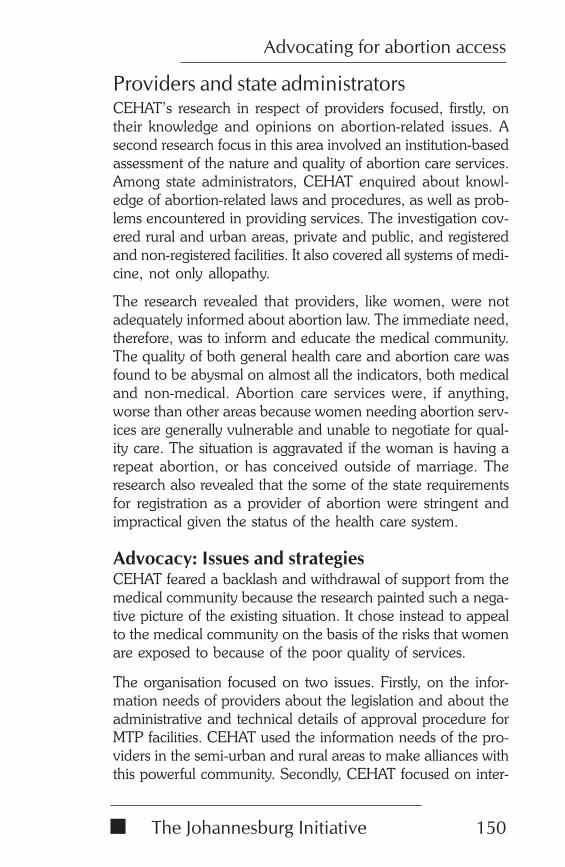
The Johannesburg Initiative
Advocating for abortion access
150
Providers and state administratorsCEHAT’s research in respect of providers focused, firstly, ontheir knowledge and opinions on abortion-related issues. Asecond research focus in this area involved an institution-basedassessment of the nature and quality of abortion care services.Among state administrators, CEHAT enquired about knowl-edge of abortion-related laws and procedures, as well as prob-lems encountered in providing services. The investigation cov-ered rural and urban areas, private and public, and registeredand non-registered facilities. It also covered all systems of medi-cine, not only allopathy.
The research revealed that providers, like women, were notadequately informed about abortion law. The immediate need,therefore, was to inform and educate the medical community.The quality of both general health care and abortion care wasfound to be abysmal on almost all the indicators, both medicaland non-medical. Abortion care services were, if anything,worse than other areas because women needing abortion serv-ices are generally vulnerable and unable to negotiate for qual-ity care. The situation is aggravated if the woman is having arepeat abortion, or has conceived outside of marriage. Theresearch also revealed that the some of the state requirementsfor registration as a provider of abortion were stringent andimpractical given the status of the health care system.
Advocacy: Issues and strategiesCEHAT feared a backlash and withdrawal of support from themedical community because the research painted such a nega-tive picture of the existing situation. It chose instead to appealto the medical community on the basis of the risks that womenare exposed to because of the poor quality of services.
The organisation focused on two issues. Firstly, on the infor-mation needs of providers about the legislation and about theadministrative and technical details of approval procedure forMTP facilities. CEHAT used the information needs of the pro-viders in the semi-urban and rural areas to make alliances withthis powerful community. Secondly, CEHAT focused on inter-
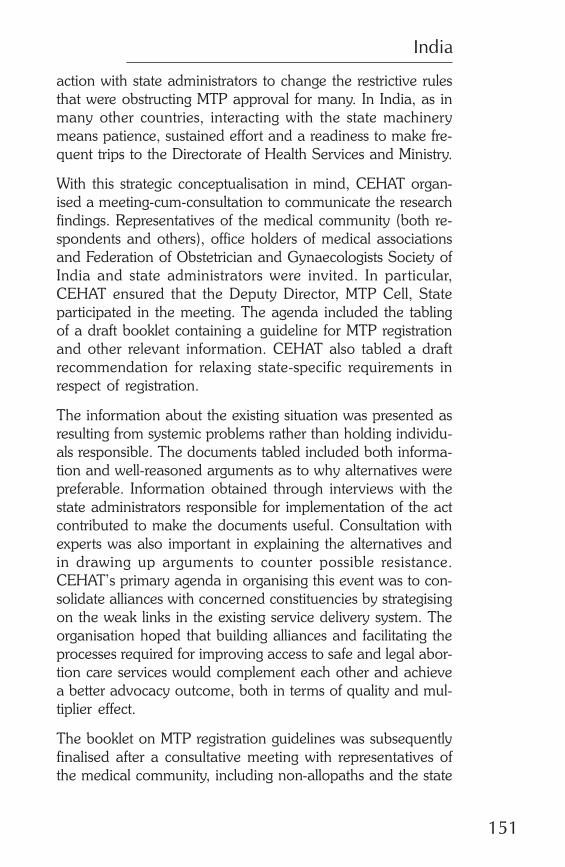
India
151
action with state administrators to change the restrictive rulesthat were obstructing MTP approval for many. In India, as inmany other countries, interacting with the state machinerymeans patience, sustained effort and a readiness to make fre-quent trips to the Directorate of Health Services and Ministry.
With this strategic conceptualisation in mind, CEHAT organ-ised a meeting-cum-consultation to communicate the researchfindings. Representatives of the medical community (both re-spondents and others), office holders of medical associationsand Federation of Obstetrician and Gynaecologists Society ofIndia and state administrators were invited. In particular,CEHAT ensured that the Deputy Director, MTP Cell, Stateparticipated in the meeting. The agenda included the tablingof a draft booklet containing a guideline for MTP registrationand other relevant information. CEHAT also tabled a draftrecommendation for relaxing state-specific requirements inrespect of registration.
The information about the existing situation was presented asresulting from systemic problems rather than holding individu-als responsible. The documents tabled included both informa-tion and well-reasoned arguments as to why alternatives werepreferable. Information obtained through interviews with thestate administrators responsible for implementation of the actcontributed to make the documents useful. Consultation withexperts was also important in explaining the alternatives andin drawing up arguments to counter possible resistance.CEHAT’s primary agenda in organising this event was to con-solidate alliances with concerned constituencies by strategisingon the weak links in the existing service delivery system. Theorganisation hoped that building alliances and facilitating theprocesses required for improving access to safe and legal abor-tion care services would complement each other and achievea better advocacy outcome, both in terms of quality and mul-tiplier effect.
The booklet on MTP registration guidelines was subsequentlyfinalised after a consultative meeting with representatives ofthe medical community, including non-allopaths and the state
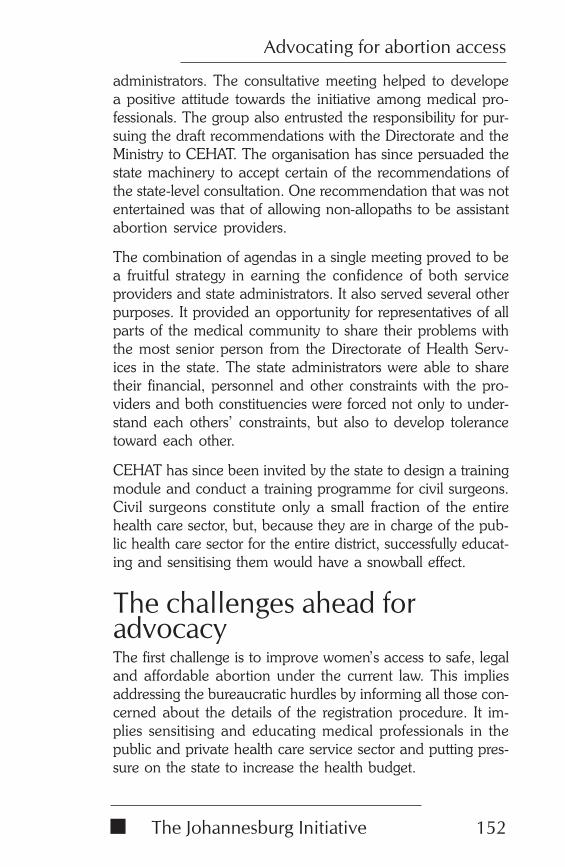
The Johannesburg Initiative
Advocating for abortion access
152
administrators. The consultative meeting helped to developea positive attitude towards the initiative among medical pro-fessionals. The group also entrusted the responsibility for pur-suing the draft recommendations with the Directorate and theMinistry to CEHAT. The organisation has since persuaded thestate machinery to accept certain of the recommendations ofthe state-level consultation. One recommendation that was notentertained was that of allowing non-allopaths to be assistantabortion service providers.
The combination of agendas in a single meeting proved to bea fruitful strategy in earning the confidence of both serviceproviders and state administrators. It also served several otherpurposes. It provided an opportunity for representatives of allparts of the medical community to share their problems withthe most senior person from the Directorate of Health Serv-ices in the state. The state administrators were able to sharetheir financial, personnel and other constraints with the pro-viders and both constituencies were forced not only to under-stand each others’ constraints, but also to develop tolerancetoward each other.
CEHAT has since been invited by the state to design a trainingmodule and conduct a training programme for civil surgeons.Civil surgeons constitute only a small fraction of the entirehealth care sector, but, because they are in charge of the pub-lic health care sector for the entire district, successfully educat-ing and sensitising them would have a snowball effect.
The challenges ahead foradvocacyThe first challenge is to improve women’s access to safe, legaland affordable abortion under the current law. This impliesaddressing the bureaucratic hurdles by informing all those con-cerned about the details of the registration procedure. It im-plies sensitising and educating medical professionals in thepublic and private health care service sector and putting pres-sure on the state to increase the health budget.
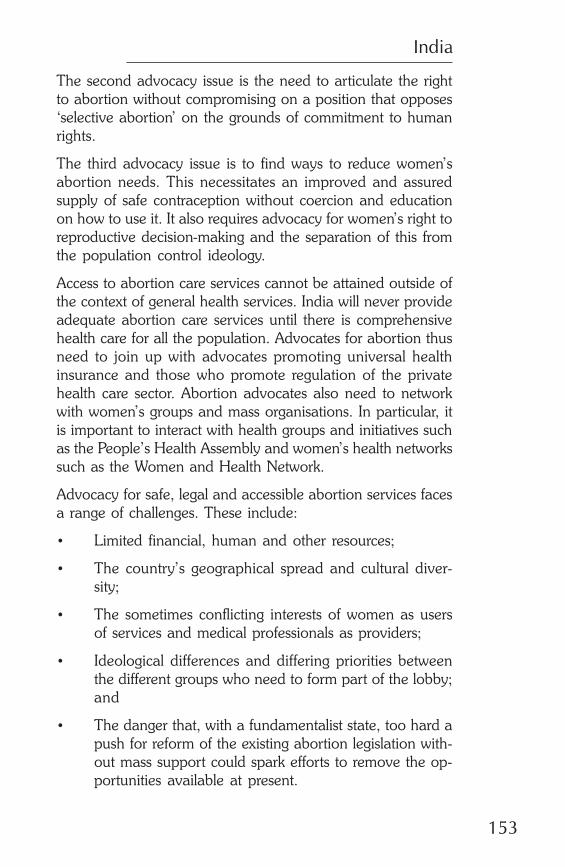
India
153
The second advocacy issue is the need to articulate the rightto abortion without compromising on a position that opposes‘selective abortion’ on the grounds of commitment to humanrights.
The third advocacy issue is to find ways to reduce women’sabortion needs. This necessitates an improved and assuredsupply of safe contraception without coercion and educationon how to use it. It also requires advocacy for women’s right toreproductive decision-making and the separation of this fromthe population control ideology.
Access to abortion care services cannot be attained outside ofthe context of general health services. India will never provideadequate abortion care services until there is comprehensivehealth care for all the population. Advocates for abortion thusneed to join up with advocates promoting universal healthinsurance and those who promote regulation of the privatehealth care sector. Abortion advocates also need to networkwith women’s groups and mass organisations. In particular, itis important to interact with health groups and initiatives suchas the People’s Health Assembly and women’s health networkssuch as the Women and Health Network.
Advocacy for safe, legal and accessible abortion services facesa range of challenges. These include:
• Limited financial, human and other resources;
• The country’s geographical spread and cultural diver-sity;
• The sometimes conflicting interests of women as usersof services and medical professionals as providers;
• Ideological differences and differing priorities betweenthe different groups who need to form part of the lobby;and
• The danger that, with a fundamentalist state, too hard apush for reform of the existing abortion legislation with-out mass support could spark efforts to remove the op-portunities available at present.
The Johannesburg Initiative
Advocating for abortion access
154
Lessons learnt• It remains a challenge to fight for quality abortion serv-
ices even once seemingly liberal abortion legislation isin place.
• It is difficult to mobilise the masses around the singleissue of abortion when the majority of the populationlacks access to the means to satisfy their basic needs.
• As a consequence, it is difficult to motivate people’s or-ganisations to participate actively and in a sustained wayin abortion advocacy campaigns. Their efforts and pri-orities are concentrated around people’s basic needs forsurvival.
• Because the potential of enactment of liberal abortionlegislation is viewed too optimistically and because oflimited resources in terms of human energy and finances,abortion advocacy has a low priority on the agenda ofthe women’s movement.
• Liberal legislation, if not complemented by an adequateimplementation plan, will not achieve what it is meantto achieve. The plan must include strategies for aware-ness building among the concerned constituencies, suchas service providers, women and their families, imple-menters and bureaucrats.
• CEHAT’s abortion advocacy initiative, although domi-nated by non-medical people, earned credibility throughrigorous research and by giving due weight to the prob-lems faced by both service providers and state adminis-trators.
• The unregulated and dominant private health sector isdifficult to target with conventional methods of advo-cacy given the power and monopoly they enjoy in healthcare service provision in India.
• A broad-based advocacy campaign is an appropriatestrategy in the initial phase to make the issue visible at
India
155
different levels and among different constituencies, butCEHAT still has to find strategies to sustain the initiative,to extend it geographically, and to develop mechanismsto assess its usefulness to women.
ReferencesGupte M, Bandewar S & Pisal H (1999) ‘Women perspectiveson the quality of general and reproductive health care: Evi-dence from rural Maharashtra’ in M Koenig and ME Khan(eds), Improving quality of care in India’s Family Welfare Pro-gramme: The Challenge Ahead, New York, Population Coun-cil, 117-39.
Jesani A and Iyer A (1993) ‘Women and Abortion’ in Eco-nomic and Political Weekly, November 27, 2591-4.
Ministry of Health and Family Welfare (1997) Annual Report.New Delhi.
AuthorSunita Bandewar is an anthropologist by training and has adoctorate in development communication. She currently worksas a senior research officer at CEHAT. She has been engagedin abortion research and advocacy work since 1994 andheaded a three-year project aimed at improving women’s ac-cess to safe and legal abortion. She is currently responsible fora large-scale, community-based abortion research project thatis part of the national abortion assessment initiative being jointlyco-ordinated by CEHAT and Health-Watch.

The Johannesburg Initiative
Advocating for abortion access
156
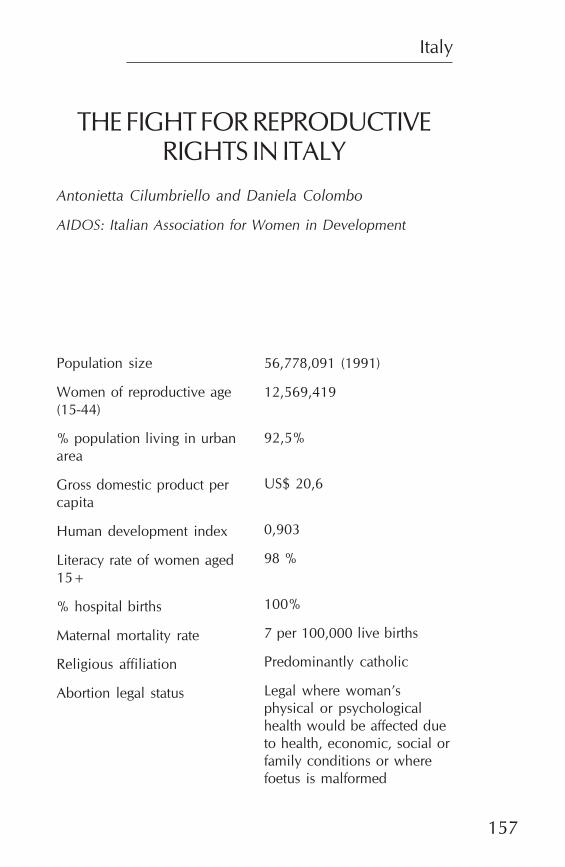
Italy
157
THE FIGHT FOR REPRODUCTIVERIGHTS IN ITALY
Antonietta Cilumbriello and Daniela Colombo
AIDOS: Italian Association for Women in Development
Population size
Women of reproductive age(15-44)
% population living in urbanarea
Gross domestic product percapita
Human development index
Literacy rate of women aged15+
% hospital births
Maternal mortality rate
Religious affiliation
Abortion legal status
56,778,091 (1991)
12,569,419
92,5%
US$ 20,6
0,903
98 %
100%
7 per 100,000 live births
Predominantly catholic
Legal where woman’sphysical or psychologicalhealth would be affected dueto health, economic, social orfamily conditions or wherefoetus is malformed
The Johannesburg Initiative
Advocating for abortion access
158
A brief history of the secondfeminist movement in ItalyThe fight for reproductive rights and the abortion bill in Italy inthe 1970s is closely linked with the history of the second femi-nist movement. One cannot understand why a catholic coun-try such as Italy passed one of the most advanced abortionbills in the world without knowing a little about what happenedin civil society, and especially in the women’s movement, inthose years.
When the Italian feminist movement began in the early 1970s,it launched a movement for social change that promised toalter some of the fundamental values governing Italian soci-ety. For this reason, when feminists decided to come out in theopen – whether in Rome, Milan or Trento – they were metwith hostility that broke out into violence on the slightest pre-text. The attacks were not only perpetrated by helmeted po-lice in full combat gear, carrying shields and heavy truncheons,nor only by the right wing. They were also initiated by menfrom the left parties and the students’ movement.
The violent reaction served to create greater solidarity amongthe women and helped the movement to grow more rapidly.In 1971, there were two main organised groups. The Movimentodi liberazione della donna (MLD, or Women’s Liberation Move-ment) was associated with the Radical party, a small, liberal,anti-clerical and anti-communist party which was not repre-sented in Parliament until 1975. The MLD immediately estab-lished political objectives that included the struggle for divorce,abortion, and non-sexist education. The Lotta Femminista(Feminist Struggle) was strongest in Northern Italy. It foughtfor wages for housework and had international connections in
Italy
159
England, the United States of America (USA) and Canada.
In addition to these groups, there were ultra-left collectives.For the collectives, the solution to women’s problems shouldbe found through a correct interpretation of Marxism. Mostcollective members were women who emerged from revolu-tionary extreme left groups and parties such as Lotta Con-tinua, il Manifesto, and Avanguardia Operaia. For thesewomen, feminism created a problem similar to that of militantblack women in the USA – they had to find a way to reconcilefeminism with the sacred texts of the extreme left. Many of thewomen eventually quit the extreme left groups.
The majority of the broader feminist movement worked insmall, loose, informal, consciousness-raising groups, active ata local level. The energy of the movement came from the bot-tom, not from the top. The day-to-day direction was derivedfrom conditions close to the lives of the women most involved.The movement did not depend on any kind of leadership. Infact, any women who emerged as natural leaders were op-posed. Women took decisions collectively and concepts likehierarchy, power, and delegation were rejected as products ofa male culture.
A profound feeling of belonging to a unique community unitedthe women working in different local settings. Unity incorpo-rated women from the more advanced North as well as thosefrom the developing South, where the crimes of honour killingand abduction were still considered part of ‘traditional norms’.A feeling of sisterhood, of sharing a common struggle and com-mon discovery characterised the movement. The number ofgroups operating in the country at any one time was not known,but in every small town there was at least one feminist group.In addition, for a movement without centralised structures, therewas an enormous amount of informal communication andmobilisation through magazines, newsletters and other me-dia.
Over time, women from different social and economic back-grounds started responding to feminist ideas. In 1975 the first
The Johannesburg Initiative
Advocating for abortion access
160
feminist groups within trade unions were formed in the maincities and soon the movement spread to women workers allover the country. This development forced women from thesocialist and communist parties into a different view of femi-nism and motivated them to join forces and fight in Parlia-ment for some of the most advanced legislation on a range ofissues of interest to the women’s constituency.
An early example centred on the divorce law. In March 1974 anumber of Catholic organisations called for a referendum onthe abolition of the divorce law that had been approved byParliament. They did this in line with the provision in Italywhereby any organised group can call for a referendum toabolish a piece of legislation if it collects the signatures of 500000 Italian citizens within a period of three months. The femi-nist movement decided to campaign in favour of divorce and,for the first time in the political history of the country, insteadof addressing people from the top, feminists chose differentmethods – street theatre, songs, puppets, magic boxes.
When the catholic referendum was defeated, it was clear thatfor the first time Italian women had made an independentchoice, rather than listening to the church. It was also clearthat feminism was speaking to the reality of contemporary so-ciety. Even if feminists were still far in advance of what mostwomen were willing to accept, they had a substantial audi-ence ready to receive the message. It was at this time that thestruggle for the liberalisation of abortion became the unifying,nationwide issue on which all the different groups becameactive.
Eight years of struggle for theliberalisation of abortionThe legal backgroundIn Italy, the first regulation concerning abortion was includedin the penal code of 1889. The code stated that abortion wasa crime against the right to life of the embryo. The code of1930 went further. It included abortion among the crimes
Italy
161
‘against the integrity and the health of the race’. The penaltieswere severe – imprisonment in jail for two to five years forboth the woman who had undergone an abortion and theperson who had intervened. Publicity connected with contra-ceptives was also forbidden and was punishable by imprison-ment of up to one year and a fine of 400,000 lire, a largeamount of money at the time.
Clandestine, unsafe abortion, performed by unskilled personsusing hazardous techniques in unsanitary conditions was thusthe primary means of contraception. The condom was expen-sive and only available in pharmacies. Women from the up-per middle class were the only ones who could afford an abor-tion in a clinic abroad or by a gynaecologist. The latter werereferred to as ‘golden spoons’ because of the high fees theyasked on the basis of the risk involved in performing the op-eration.
In the early 1970s, an estimated 800,000 abortions were tak-ing place every year. It is not possible to calculate how manywomen died because of illegal, unsafe abortion or how manywere left with permanent disabilities as the cause of complica-tions was never declared in death certificates because of thedanger to the woman and the practitioner. The extent of abor-tion was so large, that it was not possible to apply the repres-sive legislation. Only about one in every 10,000 illegal abor-tions came to trial and these cases were dragged through thecourts for several years.
Tackling the issue in ParliamentIn February 1970, the issue of abortion was raised for the firsttime at the initial national congress of the MLD. The congresslaunched a campaign to collect signatures for presentation ofa ‘people’s bill’ in Parliament. This was possible under the Ital-ian provision whereby any organisation which collects 50,000signatures, certified by a notary, on the text of a bill, can presentit for discussion in Parliament.
On 7 June 1971, the first bill for therapeutic abortion was pre-sented by a group of parliamentarians from the socialist party.
The Johannesburg Initiative
Advocating for abortion access
162
During the years which followed, further bills were presentedby different political forces. Some of these bills were progres-sive. For example, in 1973 Loris Fortuna, a socialist who hadsigned the first bill on divorce, together with other socialist MPs,presented a bill in the House of Deputies with which the radi-cal party and the MLD also agreed. The bill called fordecriminalisation and liberalisation of abortion. Other bills werereactionary. A group of catholic MPs, for example, presenteda bill aiming to help a woman through pregnancy so that shecould give the baby up for adoption.
Despite these bills, the non-confessional forces could not findagreement on a single text. The Communist party in particu-lar, adopted a reactionary position, as it was seeking a govern-ment alliance with the Christian Democratic Party. These weredifficult political years, with no stable majority and coalitiongovernments of four and five parties and the terrorism of thered brigades raged throughout the country. For pro-abortioncampaigners, this meant that each time Parliament was dis-solved, the political battle around legislation had to start allover again.
StrategiesIt was the feminist movement and the Radical Party that ulti-mately organised the pressure from civil society that obligedParliament to legislate. A successful strategy of the Radical Partywas to collect signatures for a referendum for the abolition ofthe provision in the penal code criminalising abortion. An-other strategy was that its leaders fasted during crucial mo-ments of the Parliamentary debate. No other political force,except the Socialist Party, wanted the referendum as it wasclear that the Radical Parties would win and that the debatebefore the vote would create more divisions in the country.
Several polls were conducted by magazines and research in-stitutions. These showed that close on two-thirds of the publicthought that Parliament should deal with the issue. They alsoshowed that three in five women felt that abortion should be amatter of concern only for the woman and her conscienceand that the church and state should not be involved. Some of
Italy
163
the media with the largest circulations in the country took astand in favour of abortion. L’Espresso, a progressive liberalweekly magazine, placed the photo of a crucified, pregnant,naked woman on its cover and evoked a wave of discussionaround the country. The magazine subsequently dealt withthe issue every week until legislation was approved.
Meanwhile the feminist movement organized ‘soccorso rosa’(pink assistance), a form of mutual aid in which, two or threetimes a week, women who wanted to have an abortion couldmeet in the office (or cellar) of a feminist group and be helped.Various methods were used. A medical doctor in Florence, DrCrociani, who was a member of the Radical Party, performedone abortion at low cost, using the Karman suction methodand local anaesthesia. When Dr Crociani was arrested, in Janu-ary 1975, together with two leaders from the Radical Party,feminists in Rome started organising clandestine task forceswho performed abortions using the Karman method in pri-vate homes. Several feminist doctors went for training in thismethod in England and the United States.
The equipment was kept in different homes and the groupswould meet in a different place each time. By organising abor-tions in this way, women from the feminist movement wantedto show their solidarity with women who wanted to have aprivate abortion, but without being subjected to unskilled per-sons in the poorer districts who operated on the kitchen tableor having to pay high prices to the ‘golden spoons’. Abortionswere performed collectively, with the conscious participationof the patient, in a relaxed ambience. Charter flights were alsoorganised to London clinics.
Soccorso rosa started in Rome, but the example of the femi-nist movement of Rome was copied in other cities. Many ofthe groups working on the abortion issue subsequently joinedtogether in a coordinating body called CoordinamentoRomano Contraccezione Aborto (CRAC). CRAC organisedseveral rallies at crucial moments of the political debate. InDecember 1975 50,000 women marched through the streetsof Rome demanding the liberalisation of abortion.
The Johannesburg Initiative
Advocating for abortion access
164
When a young woman, Gigliola Pierobon, was arrested inPadua, her trial became a political statement. At a certainmoment, all the women in the court who had come from vari-ous cities cried “We all have undergone an illegal abortion”.In the confusion that followed, three were arrested and werelater put on trial for having disturbed the court procedure. Thewoman who underwent the trial later wrote a book “Il processodegli angeli. Storia di un aborto” (The trial of the angels: his-tory of an abortion). This was one of the many books thatwere published on the issue at the time.
The feminist monthly magazine EFFE published photographsof the full sequence of the Karman method. These photographshad been taken in Washington in the summer of 1973 by DanielaColombo. In each issue of the magazine there were articles andnews about the discussions in Parliament and the struggle aroundthe country. A special issue on abortion was published in De-cember 1975 at the time of the Rally organized by CRAC. In1976, a weekly television programme on women’s issues, titled‘Si dice donna’ (We say women), was started by a group ofprogressive producers at the Italian national public televisionRAI 2, with contributions from feminist journalists. The pro-gramme soon began broadcasting documentaries and wom-en’s stories on abortion. It was, however, stopped in 1981 at thetime of the abortion referendum called by the catholics becauseof its strong feminist position on the issue.
The catholic forces, meanwhile, were divided, even withinparties. While the pro-life movement was organised by youngmales, women and older men were generally in favour of leg-islation allowing abortion to be carried out in public hospitalsunder certain conditions. In a country which was supposed tobe almost 100% catholic there were many families in which amother, sister or daughter had undergone an unsafe, clandes-tine operation.
The law changesIn March 1971 the Constitutional Court abolished article 553of the penal code that prohibited the advertisement of contra-ceptives. However, contraceptives could only be sold to regu-
Italy
165
late menstruation. Italian women had to wait until 1975 forlaws which permitted contraception and created family healthcounselling centres (HCCs). The 1975 law was an attempt bythe government to put a stop to the abortion discussion. Itprovided for the creation of services with an integrated, holis-tic approach to the reproductive health of women and men,including family planning and social assistance to families. Theservices could be created by municipalities, within the nationalhealth system, as well as by private groups. By 1998, therewere 2,227 public HCCs – 1.6 for every 10,000 women agedbetween 15 and 49 years. There were also 161 private HCCs.
In 1976, Parliament was dissolved because conservative po-litical forces – in particular the Christian Democrats and Com-munists – did not want to have the referendum for which theRadical party had collected signatures. Two years later, how-ever, Communist Party women who had been influenced byfeminist ideals succeeded in changing their party’s position onthe issue and a compromise was made. Law 194 of 1978,‘Norms for the social protection of motherhood and on thevoluntary termination of pregnancy’ (VTP), was approved on22 May 1978. It was not the best law in Europe, but it wascertainly not the worst one.
Law 194 provided, among others, that:
• VTP was available within the first 90 days of pregnancyfor any women requesting this on the grounds that herphysical or psychological health would be affected dueto health, economic, social or family conditions, or wherethe foetus was expected to be malformed;
• After 90 days, a VTP could be performed where thewomen’s life was at risk, or where there was a problemwith the foetus which constituted a serious hazard to thephysical and psychological health of the woman;
• To obtain an VTP, a woman needed a certificate from aphysician at a counselling centre or other social healthfacility or her general practitioner;
The Johannesburg Initiative
Advocating for abortion access
166
• A woman under 18 required approval either from herguardian or a judge;
• Health staff had the right to refuse to take part in VTPson the basis of a formal declaration of conscientiousobjection; and
• All VTP procedures would be covered by the nationalhealth system and provided free of charge in public hos-pitals.
After the legislation was passedAdvocacy for and againstThe pro-life movement quickly began collecting signatures fora referendum to abolish the law. The referendum was held inNovember 1981 and the pro-life movement was badly de-feated, with 68% of the votes against abolishing the law.
Many feminists were not satisfied with the law, but fought todefeat the referendum. However, their dissatisfaction withthe law partly explains their subsequent relative inactionon the issue. 1981 also marked a profound change in thefeminist movement in Italy, which had reached its peak inthe late 1970s. Feminism in Italy had never been a well-structured ideology and the movement did not have a clearpolitical programme apart form the abortion struggle. Bythe early 1980s, feminism had been accepted by some ofthe political forces, especially the socialist and the commu-nist parties, but they had accepted it in a way that was un-critical of their existing practices. They thus made it coexistwith the existing principles of hierarchy and rigid organisa-tion. Many laws were approved during the 1970s, however,that helped to change women’s lot in Italy, including a veryprogressive family law passed in 1975 that put husband andwife on equal footing.
Among ordinary citizens, the economic crisis was preventingyoung women from finding a job when they finished school.The older feminists who had started the movement ten years
Italy
167
before, and for this reason are called ‘historical feminists’, hadestablished better lives for themselves and in many instanceshad decided to retreat from the public sphere. Very few ofthem entered the ‘women’s machineries’ and equality com-missions that were created at national and local level. Mostpreferred to work in small groups concerned with specialisedissues such as women and literature, women and history,women and music, women and arts, women and economics,women and health, career women and women and develop-ment. None of these groups took forward the work on theabortion law and mobilisation to ensure quality implementa-tion was left to the women in the institutions.
In 1995, however, when the abortion law was under severeattack by the pro-life movement and there was a risk that dis-cussions on a new bill would resume in Parliament, thousandsof middle-aged and younger women marched again in thestreets of Rome, with the same spirit of sisterhood as in the1970s. The women did not want to lose something for whichthey had fought so hard, but this was the last episode of na-tional mobilisation.
Trends in VTPs conductedThe annual reports of the Minister of Health and the monthlysurveys of the National Bureau of Statistics (ISTAT) on VTPscarried out at health facilities authorised by the law provide awealth of information that facilitates analysis of VTP in Italyover the last twenty years. From a quantitative point of view,Law 194 can be considered a success story. During the lastseventeen years, the number of VTPs performed on womenresident in Italy increased from 213,310 in 1980 to 233,976 in1983 and then decreased to 138,357 in 1998. These and otherstatistics suggest that abortion is no longer widely used as ameans of contraception.
The current more or less constant rate of VTPs is the result ofthree factors:
• the institutional change, as the introduction of legisla-tion has affected illegal abortions and in several cases
The Johannesburg Initiative
Advocating for abortion access
168
the problem could be directly faced and prevention strat-egies could be put in place;
• a cultural change, which was already taking place whenthe Law was approved, that is different models for ma-ternity and more efficient contraception;
• a demographic change, mainly determined by the de-lay in the average age of marriage and first birth.
The largest decreases in abortion rates have been recorded inthose geographical areas where reproductive health servicesand support to prevent abortion have been most efficientlydeveloped. The rate of post-abortion complication in Italy islow compared with other European countries. This is at leastpartly due to the fact that VTP is generally performed in hos-pitals.
Some critical issues in implementation
CertificationTo obtain a VTP, the woman must obtain certification thatattests to the duration of the pregnancy and the presence ofdanger for the psychological or physical health of the woman.Despite the existence of the HCCs, which are named in thelaw as one of the main services which will support imple-mentation, women still experience difficulties in using theseservices for obtaining the certificate. In 1998 only 27% ofwomen seeking a VTP went to a HCC. Reasons include thelack of integration between this service and the referral facili-ties where VTP can be performed, insufficient HCCs in theSouthern regions, conscientious objection by many gynae-cologists and the fact that they work only a few hours at theHCC.
The certificate is therefore more often given by a private doc-tor, generally a gynaecologist. According to data from the min-isterial report of 1998, in 30% of cases it is given by the obstet-ric/gynaecological service where the VTP is performed. Thissuggests that a policy of support, reception and planning thatshortens the time between the certificate and the operation is
Italy
169
appreciated by women as it diminishes the psycho-social im-plications that the VTP can have.
Data for 1998 from the few regions for which data was avail-able show that 67% of VTPs were performed within 14 days ofthe date of the certificate. The situation becomes urgent if thepregnancy has reached the tenth or eleventh week as inter-vention depends both on the availability of gynaecologists –who, even if they are not objectors, can raise conscientiousobjection only during this stage of pregnancy – and on thewaiting list in the hospital facilities. In this situation womenmust often resort to private clinics that perform the operationat a high cost.
Conscientious objection of medical andparamedical staffIn 1998, the rate of conscientious objection stood at more than60% for gynaecologists, 50% for anaesthetists and 56% forparamedical personnel. In many regions, especially in theCentre and the North, the problem has been addressed throughservices provided by private clinics with authorisation fromthe regional authorities. In the South, with the exception ofApulia, this alternative of private clinics is not available. Thiscould be an important cause of ongoing illegal abortions, longerwaiting times and women resorting to a VTP in another prov-ince or region (ISTAT, 2000:105).
Where doctors are obliged to give the certificate, because nosubstitute is available, they can use one of the clauses of thelaw which authorises the doctor to invite the woman to waitfor one week and then to come back to communicate her de-cision again. The use of this clause represents an attempt bymedical professionals to exercise a power that is cultural andnot scientific. The paramedic staff, for their part, especiallyduring the hours following the intervention when the womanis still feeling the effect of the anaesthesia and the difficulty ofthe situation, exercise a subtle conscientious objection, for ex-ample by obliging her to listen to information on natural meth-ods of family planning.
The Johannesburg Initiative
Advocating for abortion access
170
Abortions among minors
The number of VTPs among minors is relatively low and de-creasing. Data for 1998 shows that authorisation was given byparents in 70% of the cases and by a judge in 29%. This lowrate accords with other characteristics of VTPs in Italy in thatmost are performed on women who already have children. InItaly, young women generally have their first sexual intercourseat an older age than in other countries.
Most operations on minors are performed on young singlewomen, who are students in secondary schools. This suggeststhat prevention could be effected in schools if sexual educa-tion were permitted.
ConclusionsNo political party has asked for the reintroduction of a puni-tive abortion law. The pro-life movement seems stronger to-day than it was in the 1970s, but in Italy it has chosen to usemore subtle methods, such as encouraging conscientious ob-jection of medical and paramedical staff, rather than act vio-lently. For example, a woman is often left alone to face a VTP.
The waiting time between certification and the intervention,the limited time that the medical team responsible for the VTPsspend in hospitals, the inadequate integration between theservices that certificate pregnancy and those that perform theintervention and the limited availability of the services - espe-cially in the South - are all manifestations of how widespreadconscientious objection is among medical and paramedicalstaff.
There is also some ‘abortion fatigue’ among gynaecologistsand paramedics who are members of teams performing VTPs.Recently, some of them have used conscientious objection asa way of protesting against the fact that they are obliged tospend all their working time in hospital performing abortions.
Italy
171
Since Italy has one of the lowest fertility rates in the world, thediscussion on bio-ethics and the juridical rights of the foetussurfaces quite often, even within the most progressive politicalforces.
In this context, the concept of free choice for women, whichwas the basis for the women’s struggle in the 1970s, has beenundermined by many organisational difficulties. Instead of fight-ing against the system and mobilising to ensure correct appli-cation of the law, it seems that women have preferred to or-ganise themselves in a different way. As was the case whenabortion was illegal, women pass information by word of mouthon where to go. This informal system of communication onwhere to get the certificate, who the best doctors are and wherethe waiting list is shortest, is relatively efficient and is concealedin the women’s world where some prefer to act, rather than tomobilise to obtain legislation which ensures good operationeverywhere.
The prospects if the centre right wins the elections in May 2001are not good. We had an indication of what might happenwhen, on 30 October 2000, pharmacies started selling emer-gency contraception. The sales were possible because the prod-uct had been approved by the French government and thisallowed other European countries to sell it. Approval for thesales by the Ministry of Health raised strong objections fromcatholics that reached as far as Parliament. Thus far the Minis-ter of Health has been firm in defending this decision, but.public authorities in those regions where centre right politicalparties are in power have asked that the pharmacists shouldbe allowed to refuse on the basis of conscientious objection.
The pro-choice forces have not taken these attacks lying down.There has been some reaction in the press, some declarationsby women parliamentarians and lists of friendly pharmacistshave started to circulate. We hope that if the centre right wins
The Johannesburg Initiative
Advocating for abortion access
172
nationally, pro-choice forces will fight back firmly.
ReferencesISTAT (2000) Induced abortion in Italy: a socio-demographicand health view since the legalisation until now, Essay no 5,Italian National Bureau of Statistics.
AuthorsDaniela Colombo is a development economist and presidentof AIDOS, the Italian Association for Women in Development.In the 1970s she was actively involved in the feminist movementof Rome, co-founder and editor of the monthly feministmagazine EFFE and member of the team of journalists whoworked for the programme “Si dice donna”, contributingdocumentaries on abortion
Antonietta Cilumbriello is a gynaecologist who has alsospecialised in Chinese medicine, and who works in one of themost advanced birth centres in Rome, “Il melograno”. Shehas been collaborating with AIDOS in the implementation ofprojects in developing countries that aim at the creation ofhealth counselling centres with an holistic approach to repro-ductive health.
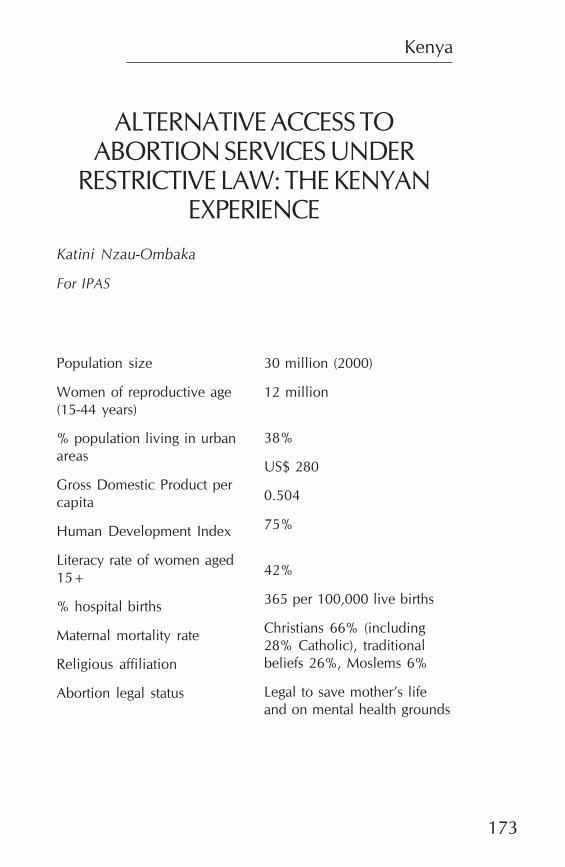
Kenya
173
ALTERNATIVE ACCESS TOABORTION SERVICES UNDER
RESTRICTIVE LAW: THE KENYANEXPERIENCE
Katini Nzau-Ombaka
For IPAS
Population size
Women of reproductive age(15-44 years)
% population living in urbanareas
Gross Domestic Product percapita
Human Development Index
Literacy rate of women aged15+
% hospital births
Maternal mortality rate
Religious affiliation
Abortion legal status
30 million (2000)
12 million
38%
US$ 280
0.504
75%
42%
365 per 100,000 live births
Christians 66% (including28% Catholic), traditionalbeliefs 26%, Moslems 6%
Legal to save mother’s lifeand on mental health grounds
The Johannesburg Initiative
Advocating for abortion access
174
IntroductionBackgroundHigh maternal mortality rates are found in those countrieswhere the law prohibits non-medical reasons for induced abor-tion. Kenya, where abortion is permitted by law to save thepregnant woman’s life and on ‘grounds of necessity’, is onesuch country. Despite the restrictive law, many abortions con-tinue to be performed clandestinely with serious socio-eco-nomic and health outcomes. Changing the legal status of abor-tion thus remains fundamental to improving women’s repro-ductive health.
In Kenya, certain doctors, particularly gynaecologists, havebeen the primary supporters of a more liberal abortion law. Atthe 1993 Annual Scientific Conference of the Kenya Obstetri-cal and Gynaecological Society (KOGS), the organisation’smembers reiterated their stand on this issue. They passed aresolution asking the Minister of Health to present a cabinetpaper on abortion as a health issue, highlighting social, eco-nomic and health costs to the country. They asked for a moreliberal law, but nothing resulted from their efforts. KOGS’ stancewas largely the product of strong leadership by the then chair-person, who had been proactive in advocating on adolescentreproductive health and abortion issues.
Unlike the gynaecologists, other doctors and health personnelcontinue to hold more conservative attitudes toward abortionlaw reform (Rogo, 1993). Further, the Church, especially theCatholic Church, remains a bastion of opposition to abortionin Kenya. Although only 28% of the population are Catholic,the Catholic Church exerts disproportionate influence on thereproductive health policies in the country.
Kenya
175
Until recently, women’s groups and non-governmental organi-sations (NGOs) generally remained silent on the issue of abor-tion. A number of NGOs have begun to show an interest inthe advocacy of reproductive rights, including the InternationalFederation of Women Lawyers, Kenya (FIDA-K), the FamilyPlanning Association of Kenya (FPAK), the Africa Regionaloffice of the International Planned Parenthood Federation(IPPF-Africa), the Kenya Medical Association, and Ipas. Thepredominant national women’s organisations have, however,not been very vocal on reproductive rights or abortion in par-ticular. After the Beijing Conference most women’s organisa-tions focused on gender concerns in political participation andeconomic empowerment,while remaining less vocal on healthmatters.
Meanwhile, the magnitude of unsafe abortion and its conse-quences has become a public health emergency in Kenya. In1993 an estimated 252,800 induced abortions occurred amongschoolgirls in Kenya. Sixty percent of all gynaecological ad-missions and up to 5% of total hospital admissions are due toabortions (Rogo, 1993.) It is evident from the large number ofwomen seeking abortions that the restrictive legislation onabortion does not receive much respect in practice. Yet, whilethe law is interpreted liberally by doctors whenever they arekeen to help women in need of services, most clinicians havenot been providing abortion for the full range of reasons per-mitted within the current law. In the prevailing atmosphere it isunlikely that any major liberal change in the law will occur.Emphasis must therefore be put on the fullest possible inter-pretation of existing law, which permits abortion under ‘groundsof necessity’, interpreted to include abortions performed onphysical or mental health grounds (UN Population Division,1999.)
This paper looks at a unique initiative by private health pro-viders in the western part of Kenya to make sure safe abortionservices are available to the fullest extent of the law. Whilestrategies for changing the law on abortion are the focus of theoverall project, the Kenyan experience highlights the possibili-
The Johannesburg Initiative
Advocating for abortion access
176
ties within restrictive laws to ensure access to safe abortionservices. Because the western Kenya initiative did not origi-nally intend to change the law, it would be unfair to evaluate itin terms of its success or failure to do so. Instead, it is evaluatedas a way of achieving one aspect of the ‘broader’ picture inexpanding access to abortion services, i.e. creating a pool ofwell trained and skilled, willing providers.
The paper draws on interviews with approximately thirty indi-viduals, including public, private and non-governmental serv-ice providers and officials and other representatives of the in-stitutions and organisations concerned with reproductive healthand abortion services.
The Private Providers Network of WesternKenyaIn late 1996, a network of private health providers trained toprovide comprehensive, affordable post-abortion care (PAC)and family planning was started by a local NGO - the KisumuMedical Educational Trust (KIMET). The Network was namedthe Private Providers Network of Western Kenya (PPNWK)and it’s philosophy was to realise the potential contribution ofprivate practitioners to abortion care and reproductive healthcare more generally. The hypothesis was that there was nohostility to abortion services at the community level and thatthese services had been performed through the decades byunskilled community members who are accepted and toler-ated. By setting up the Network, community confidence inlocal services for abortion and post-abortion care would im-prove because services would now be provided by skilled healthprofessionals. This support might ultimately contribute to build-ing a supportive environment for legislative change.
The project was initiated in response to the deterioration ofthe health service delivery system in Kenya. Cost sharing hadbeen introduced in respect of most health services, includingreproductive health. Quality of care had become an issue andsome women chose to seek private services which they per-ceived to be of better quality.
Kenya
177
PAC encompasses emergency treatment for abortion compli-cations, counselling and provision of family planning infor-mation, and links to other reproductive health services. In par-ticular, in Kenya PAC was interpreted to include manualvacuum aspiration (MVA) for incomplete abortion, menstrualregulation and legal abortion as well as family planning coun-selling and services, emergency contraception, condom pro-motion and treatment of sexually transmitted infections (STIs).The PPNWK aimed to expand outlets for the provision of arange of reproductive health services by recruiting and train-ing private providers. Trainees learnt that they could use thesame technology used in PAC to provide abortion servicesand the choice as to whether to do so was left to the indi-vidual. The project was based in western Kenya because thisregion had fertility rates above the national average and highmaternal mortality due to unsafe abortion. The contraceptiveprevalence rate was one of the lowest in the country (Rogo etal, 1998).
Involving private providers was seen as a rapid and cost effec-tive way of expanding PAC services to the community andhence significantly reducing the incidence of unsafe abortion,unnecessary deaths and the competition for services, staff andresources which often occurs in public hospitals. The Networkinitially comprised physicians, but later expanded to includemid-level providers and community health workers, and com-munity based distributors (CBDs) for contraception. The phy-sicians did not object to this expansion as they felt that theyhad received adequate personal benefits through the trainingand, at a societal level, through the hoped-for reduction inmaternal mortality. Linkages with, and the role of, other pri-mary health workers such as herbalists and local women’sgroups are currently being explored (Rogo, Bohmer, Ombaka1999).
The Network also connects private individual health care pro-viders, corporate providers such as Marie Stopes and govern-ment facilities at the district and provincial levels as it trainsproviders from all of these institutions. here is a strong referral
The Johannesburg Initiative
Advocating for abortion access
178
system set up through the Network as a result and membersgain access to the support of physicians and other Networkproviders who serve as sources of referrals and professionalconsultants.
The training is provided free. While it is available to all thatare qualified, the Network specifically targets public facilityproviders. By incorporating key public sector providers asmembers, the Network has been able to function without muchinterference.
The Network shares some characteristics of a franchise. Oncompletion of training, the Network members are given aninitial free MVA kit and undertake to provide high quality care,improve their facilities where required and not send any clientaway for lack of money. They also submit monthly reports oftheir activities, including details of abortion services provided.The Network coordinator makes follow-up advisory visits andmembers meet annually to share experiences.
The charges for services range from free to US$100 with gy-naecologists’ bills in the top bracket and nurses in the lowerrange. As noted, no client is supposed to be sent away for lackof money and providers use a sliding scale mechanism tocharge fees. When a provider is not able to offer a service,they refer the woman to another Network member for care.The fact that the nurse providers have larger caseloads sug-gests that they may be more accessible in terms of both fi-nances and locality. Analysis of the quality of care offered bythe different providers shows that women are satisfied with theservices provided by nurses (Bradbury, 2000).
The Network is into its fourth year and has a total of about100 active members spread throughout the region but con-centrated around Kisumu town. Since its existence, evidenceshows that the number of abortion cases at the provincialhospital has decreased and complicated cases and deathsfrom abortion are now rare. It may also be that since theintroduction of user fees in public facilities and because ofprivacy concerns, many women now opt to seek services inthe Network.
Kenya
179
The contextHealth services in KenyaThere are fewer than 5,000 physicians and about 40,000 nursesand clinical officers (mid-level providers) in Kenya. The doc-tors are located mainly in large towns while the majority ofmid-level providers are to be found in smaller towns and ruralsettings. Curative services are provided primarily through gov-ernment facilities, which serve 57% of the population. Theremaining 43% use the private sector (Kenya Demographicand Health Survey (KDHS, 1998). For the last ten years thegovernment has allowed the licensing of mid-level providersfor private practice. The number of private health facilities hasincreased threefold over this period. This was in line with thegovernment’s plan to decentralise health care managementand financing through community participation, cost sharing,and involvement of NGOs and the private sector.
Since 1989, only certain categories of health services are pro-vided free in public sector facilities, such as services for chil-dren under five years and some infectious diseases like tuber-culosis. With the introduction of structural adjustment pro-grammes and the subsequent reduction in government spend-ing for public health services, these services are increasinglybecoming inaccessible to many Kenyans. Many women, be-cause of their low socio-economic status, do not have accessto quality health care. The government has identified unsafeabortion as a major cause of maternal mortality and morbid-ity, however, and is addressing this through a recently adoptedPAC strategy. Expansion of PAC to include all governmentfacilities at the district level is currently ongoing.
Access to legal induced abortion services in public facilities isrestricted and very few procedures are done. Denial of care byhealth professionals is common in public hospitals (Rogo etal, 1998). Yet, despite restrictive laws, safe abortion servicesare easily obtainable in Kenya for a fee. This implies that theservices are only accessible to middle and upper class womenand explains the relatively low reporting of abortion compli-cations from public hospitals.
The Johannesburg Initiative
Advocating for abortion access
180
Legal and policy issuesIssues of reproductive health and rights are addressed in theframework of the national health and population policies. Therecently adopted National Population Policy for SustainableDevelopment (May 2000) shows evidence of the influence ofthe Cairo International Conference on Population and Devel-opment in terms of women’s empowerment and reproductiverights. While articulating the issue of reproductive rights, how-ever, these rights do not include the right to abortion serviceson request. The document does clearly state that no womenor girl will be denied services for post-abortion care. The un-written message is clear: ‘If you start the abortion, we will com-plete it.’
With regard to abortion laws, there is no statutory classifica-tion of abortion into therapeutic, induced or other categoriesin Kenya. Cases of termination of pregnancy on demand areusually recorded as menstrual regulation. The latter term isnot commonly used in Kenya (Rogo, 1993). Most people there-fore do not associate it with abortion or termination of preg-nancy. While the term is understood by gynaecologists, it re-mains foreign to most doctors, nurses and the general popula-tion.
The constitution of Kenya spells out the right to life of all peo-ple within its borders. The abortion law thus permits abortiononly for ‘the preservation of the women’s life’. The interpreta-tion of this clause and of the ‘grounds of necessity’ ruling havenot been uniform in medical circles. The lack of clarity hasoffered an opportunity to expand the range of conditions un-der which abortion can be considered permissible within thelaw.
Such broad interpretation is not without risk, however. Ken-yan statutory law recognises three felonies and one misde-meanour that bear on the act of abortion. Although the PenalCode contains restrictive provisions relating to abortion, thescope of these laws remains unclear. Prosecutions under thissection are few and are generally for causing the death of thewoman rather than for procurement of the abortion. The pen-
Kenya
181
alties for procuring an abortion are seven years’ imprisonmentfor the woman seeking services and 14 years for the serviceprovider (Lema et al, 1992).
Socio-cultural perspectivesMany communities in Kenya still maintain a traditional patri-archal system in which men are the primary decision-makersin family and social relationships. Women internalise this op-pression, keep their place within the community and eventu-ally earn the respect due to a mother or an elder. The tradi-tional arrangements of gender roles reinforce men’s sense ofpower and competence. In times of external challenges, as inAfrica’s current socio-economic climate, control over womenoffers men of relatively low status a position of power deniedin other spheres of their lives. Despite this, men’s roles andrealities are changing in parts of Kenya (Silberschmidt, 1999).Their paternal authority is weakening due to changing circum-stances, including land fragmentation, increased migration tocities, stronger local women’s groups and children’s expecta-tions as a result of education.
Traditionally, pregnancies in unmarried girls elicited commu-nity disapproval and punishment. Very strong social pressurecontinues to exist that condemns pregnancy outside marriage.The blame for pre-marital pregnancy is unilaterally heapedon the woman in the absence of any corresponding sanctionon pre-marital fatherhood. These micro-prejudices are the pil-lars of denial of women’s right to choice.
Due to their poor economic status, many of the women seek-ing abortion services through the Network relied on men topay for the services. Traditionally women went to communityproviders. The transaction was ‘woman-to-woman’ and it wasusually the aunt who took her niece to the abortionist andsettled the bill. It seems from the current relatively liberal stanceof these western Kenyan men in regard to abortion servicesand contraception that there is a new thinking about repro-ductive health matters. Perhaps this is due to the harsh eco-nomic realities and the pressure on men to provide for theirown immediate families as well as extended families. This may
The Johannesburg Initiative
Advocating for abortion access
182
also explain why many couples, particularly Catholic couples,sought these services repeatedly. The experience in westernKenya revealed that abortion is not just a problem for the un-married, young girl.
In western Kenya and elsewhere in Kenya, communities havedealt with unwanted pregnancy at the community level de-spite the law. There have always been known providers ofabortion services within the community and traditional meth-ods of terminating pregnancies are documented in many soci-eties (Lema & Njau, 1990). While traditionally abortion wasexclusively procured with herbal medicines, today it has be-come a business and a variety of people are involved. Manyhave inadequate training, knowledge and skills, especially atthe rural community level.
The impact of religion on the lives of communities in Kenya issubstantial. The Catholic Church, in particular, continues tohave immense influence on reproductive health policies inKenya. The state has often adopted the Catholic Church’sposition on reproductive health matters. More recently, how-ever, the President of Kenya challenged the Church’s positionon the use of condoms to fight the AIDS pandemic. This is adeparture from the state’s conservative stance on matters re-lated to the family and specifically reproductive health issues.The AIDS pandemic has had far-reaching consequences onpreviously held norms and beliefs. The issue of gender powerrelations in negotiating sexual relations and the consequencesof such relations are now the subject of heated debate in Kenya.There is no doubt that the AIDS crisis has brought to the forethe fundamental connection between women’s right to repro-ductive health and socio-economic development.
Key findingsFactors that influenced the PPNWK initiativeThe 1990s saw a shift in the way PAC services were providedin Kenya. Following the Cairo Conference in 1994 and itsemphasis on the need for post-abortion care, the government
Kenya
183
welcomed efforts to mobilise the private sector’s involvementin reproductive health services. Service delivery for abortionand contraception remained a sensitive area in public facili-ties, however, because of the restrictive law and perceivedpolicies. The need to maintain privacy and confidentiality fur-ther complicated the expansion of abortion-related serviceswithin the public sector. In the private sector no-one other thanthe provider and assistant had to know that the woman hadan induced abortion. In the public sector, it was more difficultfor women – and especially girls – to keep the matter out ofthe public eye. Broadening the service delivery base for abor-tion could be done cost effectively in the private sector withlinks to public facilities. The PPNWK project is one such at-tempt to address this issue. Network members enjoyed thesupport and collaboration of local public hospitals for trainingand referral.
The project concept was based on the assumptions that:
• Private physicians were already providing a significantproportion of safe post-abortion care services but wereout of reach of most women due to cost;
• Many private practitioners were willing and had themeans to provide high quality abortion care; and
• Trained well and sensitised to the responsibilities in-volved, many of these providers would agree to providecomprehensive reproductive health services, includingPAC and other abortion-related services at an afford-able cost.
The international NGO donor agency that funded the projectwas initially sceptical about the feasibility of the initiative, butagreed to fund the project because of its interest in abortionservice delivery and its support for women’s and abortion rights.The donor must also have been motivated to fund the projectgiven the unmet need for family planning in the region. Beinga risk-taking organisation with interest in funding areas thatothers do not fund, the donor agreed to support the project.
The Johannesburg Initiative
Advocating for abortion access
184
Within this background, the PPNWK case illustrates the im-portance and impact of leadership and commitment to an is-sue as evidenced by the physician who initiated the project.The physician had consistently advocated for a liberal law onabortion over the years. He was the chair of the KOGS in1993 when the first attempt to liberalise the law was made. In1987 with technical input from Ipas, he spearheaded the in-troduction of MVA training at the national teaching hospital.As the chair of the KMA at the time the project was launched,he was able to intensify the fight to reduce maternal mortalitydue to unsafe abortion. He used his advantaged and respectedposition as a health professional and expert in reproductivehealth matters in Africa and risked the consequences of theNetwork operating under the current laws on abortion. Hiswillingness to be a vocal advocate for better services influencedhis peers in the region.
The fact that Network members were themselves local provid-ers made them more responsive to the plight of women in theirown region. The members of the Network had deep trust andrespect for the physician’s commitment to reduce maternalmortality in the region, which also happened to be his ancestralland. Coupled with the high maternal mortality in western Kenya,the region has one of the highest fertility rates and one of thelowest contraceptive prevalence. The unmet need for contra-ception was obvious. PAC became an entry point to compre-hensive reproductive health services and community membersand donors recognised that an intervention at this level wouldreduce maternal mortality and prevent unwanted pregnancy.
Health providers’ motivation to offer abortionservicesEven though this part of the country contains a significant Chris-tian population and the Catholic Church is strong, there seemsto be little or no community opposition to the functioning ofthe Network. Many of the providers seem unaware of any threatto their services and only one or two members have receivedwarnings of possible closure of their clinics from local healthsystem officials.
Kenya
185
To short-cut any opposition from church leaders, some of theNetwork members reported providing services to family mem-bers of religious leaders in order to gain their support. In addi-tion, the Catholic Mission Hospital facilities are utilised by theNetwork for training and a staff doctor is a key trainer for theNetwork. There thus appears to be some level of tolerance forthe Network activities in Catholic institutions in the region, al-though it was not clear why this was so when Catholic institu-tions elsewhere in the country remain very conservative.
With little resistance to their services, the health providers havecontinued to offer safe abortion services with minimal compli-cations. In fact, the Network has been able to advertise abor-tion care services and the providers are seeing increasing num-bers of clients. One provider located in a town on the borderhad seen about 1,040 cases for abortion services in the threemonths preceding this study. He had been arrested severaltimes but had always been released after paying some moneyto the police, demonstrating a level of acceptance of the Net-work by the law enforcement agents in this town.
Many providers said that they were motivated to continue of-fering services because of the training they received, the sub-sequent improvement in the quality of care and their contri-bution to decreasing maternal mortality and morbidity. Thistranslated into an increased caseload and ultimately an in-crease in their income. The monetary incentives were impor-tant to most of the providers interviewed.
Other providers said that being a member of the Network haddeveloped their confidence, solidarity and given ‘a sense ofprotection’ from prosecution by the law enforcers. A nurse pro-vider had her clinic closed down for providing illegal abortionservices after she refused to bribe a health official. With assist-ance and support from the Network, she was able to restarther services and claims to have been empowered by this inci-dent to deal with similar situations. She reiterated her deter-mination to continue her services after this ordeal.
The Johannesburg Initiative
Advocating for abortion access
186
The most notable motivation was among the mid-level healthprofessionals who felt empowered and proud that they couldperform procedures previously considered the sole domain ofdoctors. The referral system that the Network created amongproviders was also seen as a motivation to improve the qualityof care offered.
Significantly, from a ‘rights’ perspective, not even the femaleproviders mentioned that they were motivated by the need topromote women’s right to reproductive choice. Only one maleprovider talked about a ‘rights’ approach and the need to in-tegrate advocacy work in the Network. His statement is, nev-ertheless, significant and his leadership has been key in thedecline of maternal mortality at his hospital since the start ofthe Network. He has a proactive stand on abortion rights andis a Catholic. He has used his influence and power at the pro-vincial hospital to effect changes in abortion care. As a mem-ber of the Network, he acts as a consultant and referral pointfor complicated cases.
Impact of expansion of abortion services onadvocacySeveral other activities in Kenya complement the work of thePPNWK and may ultimately result in more accessible abor-tion-related services and a pool of advocates who are willingto argue for abortion law reform. For example, in 1997, giventhat there are many more nurses than doctors who are will-ing to work in under-serviced areas, a pilot project to expandPAC training opportunities for mid-level health profession-als was created by the USAID-funded PRIME project. Theproject was carried out in the Central, Rift Valley and Nai-robi regions, areas not covered by the PPNWK. The launch-ing of the PRIME project proceeded smoothly because of leg-islative and administrative support from the Nursing Counciland the Ministry of Health. The project itself included advo-cacy activities designed to raise awareness and build policysupport and acceptance among providers for PAC. This sup-port ultimately led to more mid-level providers joining theNetwork in western Kenya.
Kenya
187
The project confirmed that nurse-midwives could competentlyand economically provide safe, high quality PAC services.Nurses had previously watched in frustration as women diedfrom complications of unsafe abortions. They could have savedthose lives, but their hands were tied by policies and regula-tions that prevented their offering the much-needed services.The training provided them with the skills and technology withwhich, if they so chose, they could provide abortion serviceswhile still referring to what they were doing as PAC.
Recently, the Ministry of Health has reviewed the policies andregulations and plans are underway to train mid-level provid-ers in PAC in all district hospitals. The National Nurses Asso-ciation of Kenya is very supportive of including PAC as part ofthe nurse-midwife curriculum. The review to effect this is cur-rently underway.
In another effort, utilising findings from a community-basedand other studies on abortion in Kenya, the KMA in collabo-ration with FIDA-K and other stakeholders for advocacy onabortion have undertaken a project to expand legal policy andaccess to abortion services. The project is in its initial stages.
Critique of the KenyanexperienceInvolving womenAn overall analysis of the strategies used in the establishmentof the PPNWK reveals an emphasis on expanding accessthrough a medical focus, rather than direct advocacy for policychange. The key players were health professionals motivatedmainly by the benefit of improving access to better qualityabortion services through training and the accompanyingmonetary gains. When asked specifically about including thewomen seeking services into the Network, the providers ex-pressed the need for their involvement. There was, however, alack of connection between the services the providers gaveand the need for their involvement in advocacy work aroundthe abortion issue.
The Johannesburg Initiative
Advocating for abortion access
188
Women’s struggle for better reproductive and sexual health isa political struggle for control over their bodies and not merelya demand for adding to services (Ravindran, 1995). Yet thestruggle for reproductive rights is not visible in the women’smovement of Kenya even after the Cairo conference and the1995 Fourth World Conference on Women in Beijing. What isvisible in the case study presented here is the leadership andentrepreneurship of a highly distinguished male physician.Even the Kenya Medical Women’s Association, a professionalorganisation committed to women’s health and with potentialto promote women’s reproductive rights, has not seized thisopportunity and remains relatively conservative and non-com-mittal on the issue.
Earlier efforts to liberalise the law by the KOGS may havefailed due to the lack of political pressure for change amongthe public and key constituencies. In particular, the voices ofwomen – those affected most directly by unsafe abortion - weremissing in that effort. Today these voices are still largely miss-ing from the debate. A valuable role for the Network to play inthe legal reform process would be to position the issue of un-safe abortion as less of a health sector problem and to pro-mote community responsibility and ownership for both theproblem and the solution. Forming alliances between Networkmembers and women’s organisations could have a positiveimpact on law reform.
It is important to plan from the local level up, to respect wom-en’s knowledge and perspectives of their health needs and toadopt a holistic and integrated approach to solutions that takeinto account the social, political and economic causes of illhealth. Involvement of women in conceptualising the projectmight have identified the need for an advocacy component ofthe Network at its inception. Omitting this, the women’s agendato achieve the right to make decisions on their reproductivehealth appears to have been lost in the focus on service deliv-ery. The danger in this strategy without an accompanying po-litical mobilisation is the possibility that service providers anddelivery points will be targeted if opposition to the Networkmounts. Yet there seems to have been little strategising on the
Kenya
189
part of Network members in regard to the opposition to theirservices.
A ‘public health’ or a ‘rights’ approach?Central to the workings of the PPNWK is the assumption thatordinary women will be able to pay for services. The widelyused argument for provision of safe abortion is the public healthand equity one which recognises that abortions are widespreadand that criminalisation increases maternal mortality throughunsafe abortions, mainly among low-income women. Middleand upper income women can generally pay for access to safe,clandestine services. In this context we must ask whether thePPNWK initiative to expand abortion access discriminatesagainst poor women.
Although PPNWK members agreed not to turn away anywoman requiring services, it is difficult to guarantee that thisdid not happen. The efforts to create a strong referral systemand to include in the Network mid-level professionals, whocharge less than physicians, were geared toward addressingthis possibility. A soon-to-be released evaluation of the Net-work will give better insight into access to services for poorwomen (Montagu et al, forthcoming). A significant finding ofthis study is that many of the clients of the Network were eithermarried or women with their own economic base, which sug-gests that poorer women are not able to access the service.The challenge for the Kenyan experience, therefore, is to dem-onstrate that all women, whatever their socio-economic situa-tion, can access the services of the Network.
The ‘public health approach’ might be appropriate for Kenyain the short run. The medical profession can perhaps, withsustained support for access to services, offer the leadershiprequired to achieve legislative change. There is no general‘rights framework’ in Kenya at present for one to use for abor-tion rights. For the success of a ‘rights approach’ to achievingreproductive health, Kenya must first lay a foundation for a‘rights framework’. The current review of the constitution of-fers an opportunity to articulate this agenda. While focusingon the delivery of services, the PPNWK may need to build
The Johannesburg Initiative
Advocating for abortion access
190
capacity in skills for activism at community level and to serviceproviders, to enhance the opportunity to address reproduc-tive rights in our constitutional review.
Should the silence be broken?Since its inception, the PPNWK seems to have chosen the‘quiet’ advocacy approach through its focus on access as op-posed to ‘loud and visible’ legal advocacy. This may have beena strategic approach to reduce the high political costs attachedto efforts for reform (Shepard, 2000). In some cases, publicdebate can lead to increased repression and limits on the in-formal mechanisms that expand choice. Thus, there are ad-vantages to continuing the silence.
Yet the disadvantages of semi-official clandestine systems likethe PPNWK cannot be ignored. When unofficial solutions toexpand reproductive choices are dependent on the judgmentof individual health providers, no-one is guaranteed access tothese solutions and no-one can ensure consistent quality. Thehealth and legal risks then usually fall disproportionately onlow-income or marginalised women as informal mechanismsare safer and more commonly available as one climbs the socio-economic ladder. The fact that those higher up on the ladderare also the sectors with the most influence on policy decisionscan result in a lack of political will to defend abortion rights.Hence, the ‘escape valve’ created by the PPNWK may weakenthe will of political actors in both government and civil societyto address the issue in an efficient and unified manner.
The fact that only one physician mentioned women’s rights toabortion services identified a gap that could be used in de-signing the next phase of intervention with the Network mem-bers. Currently the Network members are all clearly on-boardwith a better access and quality of care approach. Making theconnection with the ‘rights approach’ is a process and doesnot have to happen at once. However, to have the Networkalso function as an advocacy body for legal reform, this issuewould need to be addressed.
Kenya
191
Conclusion and lessons learntThe PPNWK addresses a very important constituency in win-ning the battle for liberalising the law on abortion by winningthe support of health care providers in an ongoing and sys-tematic manner and by training doctors and nurses in safeclinical techniques. This will be key to the implementation ofany legislative change on abortion. The PPNWK experiencenow needs to be expanded to impact on the national policymaking processes. While an interview with the current chair-person of Kenya Medical Association indicates support for theNetwork, there is need to develop more formal linkages forthe growth and expansion of the Network countrywide. Al-though the previous chairperson of KMA, who started theNetwork, gave credibility to the project, the links between theNetwork and KMA were not institutionalised and once the in-dividual left, the ties loosened.
In summary, an analysis of the PPNWK reveals the followingstrengths and weaknesses:
StrengthsIncreased provider willingness to deal with abortion;
• By creating a Network of carefully-selected providers inprivate practice, Network members are given a piece ofthe economic ‘pie’, thus eliminating some of the com-petition. This, in turn, defuses practitioners’ willingnessto report their colleagues to the police;
• A strong referral system allows providers to refer womento other Network members if they cannot offer the serv-ices themselves;
• By utilising government facilities for training in PAC,some of the providers in the government institutions arelinked to the Network as members and act as referralpoints for complications. Having a supportive publichealth facility is key to the success of the PPNWK;
The Johannesburg Initiative
Advocating for abortion access
192
• The change in Ministry of Health policy to train mid-level providers in PAC services as part of the PRIMEproject means that more mid-level providers will be ableto join the Network.; and
• There is interest from other countries in the PPNWK as amodel for cost-effective delivery of reproductive healthcare through a network of private providers.
Weaknesses• Lack of clarity as to whether clients are turned away for
lack of money. The economic factor is an issue that can-not be ignored for poor women;
• Difficulty in ensuring close and consistent supervision ofproviders. This could compromise quality of care. Thesustainability and potential growth or replication of thePPNWK will depend upon its ability to ensure the qual-ity of services being offered by member providers;
• Absence of an advocacy strategy for access and a needfor outreach and information programmes to informwomen about the Network’s services and about strate-gies to reduce the need for abortion. According to a re-cent evaluation, although into its fourth year, the Net-work was not very well known by the women in the com-munity;
• There are no clearly defined linkages between thePPNWK and professional bodies like KMA and FIDA-K.The Network could benefit from a broader understand-ing and support of its activities among other professionalgroups;
• There is over-concentration of the providers in andaround Kisumu town; and
• The ‘rights perspective’ to the abortion issue appears tohave received little attention and will need to be ad-dressed if the Network is to function as an advocacy bodyfor legal reform.
Kenya
193
In conclusion, the PPNWK initiative utilises quiet action foraccess as against loud advocacy for law reform. Earlier at-tempts at law reform by the KOGS and recent public state-ments by a key government policy-maker have met with dis-approval and lack of political will for change. To change thelaw on abortion requires political mobilisation of many ac-tors, which could take years. The PAC enterprise offers a ‘safe’entry point for expanding access to abortion services sincethe government has adopted the PAC strategy to address thepublic health and women’s health dimensions of unsafe abor-tion. Hence the PPNWK is operating within the acceptedgovernment policy framework for comprehensive reproduc-tive health services.
Finally, in respect of replicating the Network within Kenya, thededication, commitment, leadership and entrepreneurship ofthe male physician who has ensured the success of the projectmay be difficult to attain elsewhere. Expansion of the Networkwould require the involvement of local providers in each re-gion and mobilisation of each community to own the problemand solutions of unsafe abortion. The role of the medical pro-fessionals, both doctors and mid-level providers, in this ex-pansion needs to be well defined. The enthusiasm of the Nurs-ing Association in providing PAC services needs to be nur-tured so to avoid conflict with physicians. It would also be im-portant to develop alliances with other key players in the fieldof abortion in Kenya.
The mobilisation and incorporation of women and their com-munities in the expansion of the Network cannot be over-em-phasised. As the Network expands to other parts of the coun-try, it will be important to involve local women in conceptual-ising and informing the design of Network services in order tominimise any resistance.
Lessons learnt• The choice between adopting a ‘rights approach’ or a
‘public health approach’ when advocating for safe abor-tion can be difficult. The dilemma can be philosophical,but the choice should be strategic. Are the two ap-
The Johannesburg Initiative
Advocating for abortion access
194
proaches mutually exclusive? Providers argue that, on apractical level, a woman’s right to abortion is only possi-ble if services are provided rather than simply talkedabout. In our fight to change legislation on abortion, wemust not lose sight of the issue of access to services. Wesometimes become too easily consumed by the middleclass passion for the abstractions of ‘rights’ and misledby the egoistic desire for the visibility of battle.
• It is unlikely that the law will change soon in Kenya’spresent socio-economic and political climate. There areother major social justice and development issues likeAIDS and poverty alleviation that will undermine mobi-lisation on abortion. There are, however, several activi-ties that can be undertaken immediately, which cangreatly benefit those who need abortion services. ThePPNWK is an initiative that is responding to the need fortraining and expansion of safe abortion services.
• In countries where the abortion law is restrictive, there isan opportunity to be creative. PAC or other ‘safe’ issuesmay be the best way to get people interested in this sen-sitive issue. From this ‘safe’ base, one can expand toother services, including abortion.
• The medical profession in Kenya, with committed lead-ership on the issue of abortion, is in a unique position topush the legal provisions to increase access to services.To achieve legal reform, linkages with the women’s move-ment and community mobilisation are necessary. Womencould be allies of the medical profession and use the‘public health’ perspective to change the law. A ‘rights’approach may invite too much attention and inflameadversaries. It accentuates dichotomies and fuels con-flict. It could also alienate some of the current allies, thedoctors and mid-level providers who are taking a risk inoffering services under the restrictive law.
• The acceptance of the PPNWK in western Kenya pro-vides evidence of sympathy on the part of lawyers, thepolice, religious leaders and others to the issue of abor-

Kenya
195
tion. We often do not appreciate the extent to which theseplayers are sympathetic.
• Understanding and addressing the interests of providersis essential in expanding access to abortion services. Profitcan be a major factor in abortion service delivery. Fearor loss of economic gains available under restrictive lawsmay restrict support for liberalisation of the abortion laws.On the other hand, empowering the mid-level providersto do procedures that have been the preserve of doctorsmay have motivated many of them to provide abortionservices.
• Where the women’s movement is weak on the issue ofreproductive rights, it is important to be strategic in form-ing alliances for reproductive choice. In Kenya, the cur-rent discussion on abortion is spearheaded by men onboth sides. Men still have political power in Kenya andchanging the law is a political process. There will thusneed to be serious consideration of alliances with malegroups and individuals.
• It is not clear what the foregoing fact means for women’sorganising on the issue. Experience in Kenya has shownthat it has been difficult to win legislation that is specificto women’s needs. In a recent interview, the chairpersonof FIDA-K, a professional women’s organisation that hashad experience with legislative advocacy, said: ‘Wom-en’s issues must be translated into national issues. Womenmust not be portrayed as victims. An approach of a senseof justice is more likely to succeed.’
ReferencesBradbury K (2000) Report of the PPNWK Evaluation, unpub-lished.
Kenya Demographic and Health Survey (1998) Central Bu-reau of Statistics, Ministry of Planning and National Develop-ment, Nairobi. Macro International, Washington DC.
The Johannesburg Initiative
Advocating for abortion access
196
Lema VM & Kamau K, Rogo K (1989) Epidemiology of Abor-tion in Kenya, Centre for the Study of Adolescence. Nairobi.
Lema VM & Kabeberi-Macharia J (1992) A Review of Abor-tion in Kenya, Centre for the Study of Adolescence, Nairobi.
Lema VM & Njau PW (1990) Abortion in Kenya: TraditionalApproach to Unwanted Pregnancy. Centre for the Study ofAdolescence, Nairobi.
Montagu D, Rogo K, Bradbury K, Oguttu M & Orero S(forthcoming) Networking Private Providers to Improve Clini-cal Family Planning Services in Western Kenya.
Ravindran S (1995) ‘Women’s Health Policies: Organising forChange’ in Reproductive Health Matters 6, 7-11.
Rogo K (1993) ‘Induced Abortion in Kenya’, Centre for theStudy of the Adolescence, Nairobi. Paper prepared for the In-ternational Planned Parenthood Federation, October.
Rogo K, Bohmer L and Ombaka C (1999) ‘Developing Com-munity Based Strategies to Decrease Maternal Mortality andMorbidity Due to Unsafe Abortion: Intervention Research Re-port’ in East African Medical Journal 76, 11 (supplement).
Rogo K, Orero S and Oguttu M (1998) ‘Preventing UnsafeAbortion in Western Kenya: An Innovative Approach throughPrivate Physicians’ in Reproductive Health Matters, 6, 77-83.
Shepard B (2000) ‘The “Double Discourse” on Sexual andReproductive in Latin America: The Chasm between PublicPolicy and Private Actions’ in Health and Human Rights 4(2).
Silberschmidt M (1999) ‘Women Forget that Men are the Mas-ters: Gender Antagonism and Socio-economic Change in KisiiDistrict, Kenya’ in Men’s Roles and Changing Realities State ofthe World Report 2000, UNFPA.
United Nations Population Division (1999) World AbortionPolicies 1999.

Kenya
197
AuthorKatini Nzau-Ombaka is a gynaecologist, reproductive healthconsultant and women’s health activist from Kenya. For thepast five years, she has worked with women’s rights organisa-tions in reproductive health policy advocacy both locally andinternationally. Recently, she briefly taught the politics of wom-en’s health in the Women’s Studies Programme at the Univer-sity of Wisconsin, Madison. She is currently engaged as a policyconsultant for Ipas-Kenya.

The Johannesburg Initiative
Advocating for abortion access
198
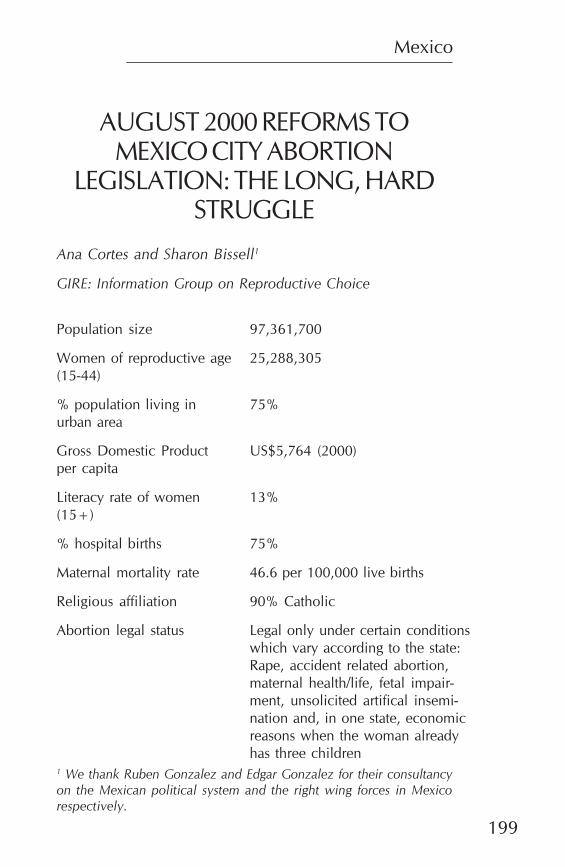
Mexico
199
AUGUST 2000 REFORMS TOMEXICO CITY ABORTION
LEGISLATION: THE LONG, HARDSTRUGGLE
Ana Cortes and Sharon Bissell1
GIRE: Information Group on Reproductive Choice
Population size
Women of reproductive age(15-44)
% population living inurban area
Gross Domestic Productper capita
Literacy rate of women(15+)
% hospital births
Maternal mortality rate
Religious affiliation
Abortion legal status
97,361,700
25,288,305
75%
US$5,764 (2000)
13%
75%
46.6 per 100,000 live births
90% Catholic
Legal only under certain conditionswhich vary according to the state:Rape, accident related abortion,maternal health/life, fetal impair-ment, unsolicited artifical insemi-nation and, in one state, economicreasons when the woman alreadyhas three children
1 We thank Ruben Gonzalez and Edgar Gonzalez for their consultancyon the Mexican political system and the right wing forces in Mexicorespectively.
The Johannesburg Initiative
Advocating for abortion access
200
IntroductionThe first concerted effort by women’s organisations to liberal-ise abortion legislation in Mexico began in early 1999 in re-sponse to the planned creation of new penal and civil codesfor Mexico City. A coalition of forty feminist non-governmen-tal organisations (NGOs) presented a legislative proposal onabortion to the Mexico City Parliament, taking advantage ofthe favourable political climate within the greater context ofdemocratic transition and the fact that a party that supportsvoluntary motherhood held the majority in the house. De-spite the coalition’s analysis that the time was right, the pro-posal faced major political obstacles, the most important ofthese being the July 2000 presidential elections and the par-ties’ desire to reach consensus on the new penal and civil codes.These difficulties blocked possibilities for advancing on the topicof abortion as the local parliament and political leaders avoidedaddressing the controversial topic at all costs.
That the coalition’s failure to secure legislative change in 1999was due to external political factors was confirmed in August2000, when the Mexico City Parliament passed legislation onlyslightly different from the original proposal that they had re-jected in 1999. The favourable political context in Mexico atthat time facilitated the reform’s passage, as well as a nationalmedia debate in which diverse sectors of Mexican society firmlyrejected an attempt to revoke legal abortion for rape survivorsin the state of Guanajuato. This paper describes the August2000 abortion law reform in Mexico City.
The Mexican political systemFor the last 70 years, political power in Mexico has been heldnationally by the Institutional Revolutionary Party (PRI). It wasnot until the late 1980s and 1990s that other parties started to
Mexico
201
gain power. The most important of these were the NationalAction Party (PAN), a centre-right party, and the DemocraticRevolution Party (PRD), a centre-left party. Before the PANwon the 2000 presidential elections, the opposition had al-ready governed 46% of the population through municipalpresidencies compared to only 2% in 1988.
The Mexican political system is characterised by a strong cen-tralisation of power in the executive branch and vertical deci-sion making, with a lack of effective division between the ex-ecutive, legislative and judicial branches. This is expected tochange with the new PAN government and parallel democra-tisation processes. Unprecedented political activity in recentyears has favoured an increase in civil participation in the leg-islative processes, which is a new area of activity, particularlyfor women’s groups.
Party stances on abortion differ. The PRI, as the governingparty, has historically made all legislation on abortion, from itsinclusion in state penal codes in the 1930s to modest liberali-sation in the 1970s, 1980s and 1990s. These changes occurredwithin the broader effort to implement the National FamilyPlanning Programme, introduced in 1974 (Ortiz-Ortega, 2001).The PRD’s platform supports voluntary motherhood, repro-ductive rights and the state’s obligation to recognise these rights.The PAN is a strong opponent of abortion. Party principlesstate that that human life begins at the time of conception andthat abortion should be legally penalised (GIRE, 1997).
Reproductive health and abortion in MexicoAlthough the Mexican constitution guarantees the right tohealth, many Mexicans do not have access to services. Healthservices are provided by the Mexican Social Security Institute(IMSS) for the employed population and by the public healthsystem for those who are unemployed or work in the informalsector. According to official statistics for 1995, the IMSS cov-ered only 40% of the population, mostly urban workers (Wom-en’s Environment and Development Organisation, 1999). Thepublic health system provides for about 30% of the popula-tion with extremely limited funding. The rest of the population
The Johannesburg Initiative
Advocating for abortion access
202
has access to basic services through rural clinics (ComisiónNacional de la Mujer, 2000) and limited access to secondaryhealth care in the public health system. Private services areexpensive and inaccessible to the majority of the population.Approximately three million Mexicans have no access to medi-cal services.
Officially, 96% of all women have access to basic reproductivehealth services. However, government actions continue to fo-cus principally on demographic goals rather than quality ofcare. According to government statistics, almost 70% of womenof reproductive age use contraceptives, but the average is con-siderably lower for young couples. There are no statistics forsingle women or men and there are approximately 455,000births every year among young women between 15 and 19years old. Births to this age group account for 16% of all birthsin the country (Poder Ejecutivo Federal, 1995).
Abortion is officially recognised as the third or fourth leadingcause of maternal mortality. Estimates of abortion vary exces-sively due to its clandestine nature. Different sources give 110(Consejo Nacional de Población, 1996), 533,100 (AlanGuttmacher Institute, 1994) and 850,000 (Mexican Safe Moth-erhood Committee, 1994) per year. Access to legal abortionservices is practically nil, with only one hospital in Mexico Cityopenly offering legal abortion services.
Feminist groups have struggled for legalisation for over thirtyyears. Despite the public health authorities’ recognition of abor-tion as a public health problem on several occasions and un-der differing political scenarios, the government has neverdesigned public policy or legislation to resolve the problemscreated by unsafe abortion.
Abortion legislation varies from state to state. None of the coun-try’s 32 states penalises abortion for pregnancy through rape,28 do not penalise for accident-related abortion, 30 for dan-ger to the woman’s life, 11 for foetal impairment, eight for riskto the woman’s health, five for artificial insemination withoutthe consent of the woman and one for socio-economic rea-
Mexico
203
sons in respect of women with three or more children. The1931 Mexico City Penal Code, valid until 23 September 2000when the August reform took effect, allowed abortion for casesof rape, danger to the woman’s life and accident-related abor-tion.
Mexico City August 2000abortion law reformSeveral events laid the groundwork for the August 2000 MexicoCity Penal Code reform. In July and August of 1998, an his-torically intense three-week national media debate on abor-tion allowed reproductive and sexual rights NGOs to increasetheir visibility and strengthen their media strategies. Argumentsfor decriminalisation based on social justice, public health andethics were disseminated and taken up by the various actorswho participated in the discussion. Mexico’s leading abortionrights NGO, the Information Group on Reproductive Choice(GIRE), employed a media strategy that included a consistentpresence on the radio and television and in the press, as wellas holding press conferences and making public statements innational papers signed by recognised opinion leaders.
From 1998 to 2000, PAN legislators in three states continuedtheir party’s strategy to gradually attack abortion rights. Theyintroduced bills to amend state constitutions to protect life from‘conception’. By so doing, they brought the issue into the po-litical arena and sparked the opposition of PRI and PRD statelevel legislators. Abortion became a political issue.
The two events that played a determining role in the MexicoCity August 2000 reform were, firstly, the work of activists topass liberalising legislation in 1999 and, secondly, an attemptto revoke legal abortion for rape survivors in the state ofGuanajuato on 3 August 2000.
1999: An opportunity for justice for women?In 1998, the Mexico City Parliament began its work to createnew city penal and civil codes. Feminist NGOs thought thatthe time was right to introduce liberalising abortion law re-
The Johannesburg Initiative
Advocating for abortion access
204
form because of their close ties with the PRD, the fact that thePRD held the majority and because the city mayor Cárdenashad made campaign promises regarding issues related tohealth, including abortion.
A group of forty NGOs formed a coalition called the Cam-paign for Access to Justice for Women (the ‘Access Campaign’)and presented five proposals on women’s rights to the Parlia-ment in March 1999. The proposals were generally well re-ceived. The notable exception was the abortion proposal, writ-ten by GIRE to include legislation valid in other states allow-ing legal abortion for danger to the woman’s health, foetalimpairment and for socio-economic reasons.
The Access Campaign’s strategy was to offer information sup-porting its reform proposals to local parliament members,Mexico City government authorities, party leaders and themedia and to advocate for a wide public consultation on abor-tion. This was the first lobbying attempt for concrete legisla-tion for many Access Campaign members and the first timethat the PRD had a majority in the house. The lack of experi-ence, technical knowledge, management of procedures andpolitical relations complicated the creation of new penal andcivil legislation.
The Access Campaign’s basic supposition was that if legisla-tors had the right information, they would recognise the needto improve legislation as a means of alleviating problems ofclandestine abortion and thousands of maternal deaths andhealth-related problems. This was particularly expected of thePRD because of its favourable stance on abortion. If legisla-tors from other parties were also convinced, reform passagewould be even more likely. The Access Campaign was unableto advance its negotiations with PRI and PAN legislators, how-ever, as the PRI was not willing to risk election votes and thePAN categorically rejected any discussion on the basis of itsparty’s position on the subject.
The Campaign’s conviction that rational arguments wouldprevail is recognised today as erroneous by both the organisa-tions and legislators involved in the process. PRD legislators
Mexico
205
interviewed for this study claim that they were in completeagreement with the Access Campaign’s proposal for abortion,but were unable to include the issue on the agenda or makepublic proclamations because of the upcoming presidentialelections. The situation was further complicated by the par-ties’ desire to reach consensus across party lines on the newlegislation, which led them to delay and eventually eliminateall discussion on abortion.
As time went by, the Access Campaign realised that the PRDlegislators did not have full power as to which items would beincluded on the agenda. Orders from party leaders had sig-nificant weight in the decision-making process. The PRD leg-islators’ refusal to discuss abortion was clearly exposed as aris-ing from a belief that it would damage their possibilities in thepresidential race.
In addition to the obstacle of the upcoming presidential elec-tions, the January 2000 papal visit and the pope’s explicit ex-hortations against abortion reminded political actors of thepower of the Catholic church. None of the parties wanted tohave the Church as a political opponent at that important time,although during our interviews some legislators maintainedthat their decision was made in 1998, prior to the pope’s visit.
The mistake that ended a debate that neverbeganOn the morning of 22 April 2000, the Access Campaign or-ganised a rally of about 100 women outside the parliamen-tary building to demand legislative reforms on abortion. In-side, a PRD legislator presented four of the five Access Cam-paign’s proposals, excluding abortion. While the proposals werebeing presented, however, PRI and PAN legislators immedi-ately assumed that they included a proposal on abortion, per-haps influenced by the rally outside. Angered, they did notlisten to the presentation. The PRI began to accuse the PRD ofbreaking their previous agreement not to discuss initiatives onwhich there had not been prior consensus in the commissionthat reviewed proposals before presenting them to the plenary.
The Johannesburg Initiative
Advocating for abortion access
206
The PRI threatened to abandon the entire process of reformsto the penal and civil codes.
The press instantly latched on to the situation, gathering state-ments from PRI and PAN legislators as the presentation con-tinued. Confusion about the real content of the presentationpersists today, but the stenographic versions of the session showthat abortion was not addressed. The PRD was obliged to re-tract the proposals presented and forced to publicly acknowl-edge the presentation as a mistake, although the party main-tains that the claim that they were breaking an agreement wasunsubstantiated.
After this fiasco, the Access Campaign realised that the new pe-nal code would not carry any changes to abortion legislation.They decided to concentrate on the other four demands, leav-ing abortion to be addressed at a future time. The 1999 abor-tion debate had ended. The Access Campaign harshly criticisedthe PRD for their error. Relations between Access Campaignmembers and PRD legislators became somewhat tense.
Abortion for rape survivors becomes a topic ofnational debateAt the beginning of 2000, national outrage brought abortionback into the public arena with the uncovering of the case of athirteen year old girl who became pregnant as a result of rapeand was pressured by PAN state authorities in Baja Californiato desist from her request for a legal abortion. The case waswidely covered thanks to a media campaign spearheaded byfeminist groups. Through the ongoing public debate, it be-came clear that the media and many sectors of the populationsupported rape survivors’ right to an abortion.
Reproductive and sexual rights advocates and individuals frommany other sectors made declarations against the tendency ofPAN officials and legislators to give priority to their personalbeliefs over their duties as public servants. The abortion de-bate took on political dimensions, as the case was used by PRIofficials and legislators to criticise the fundamentalist behav-iour of PAN officials during the presidential race.
Mexico
207
Abortion was thus contextualised within a larger debate onthe separation of church and state that continues today. Theseparation, established in the mid 1800s, has been an impor-tant facet of Mexican society throughout the 20th century, de-spite a certain degree of flexibility on the part of the state andrestricted intervention by the Catholic church in social affairs.This formal division was weakened in 1992 with a constitu-tional amendment that gave legal representation to churchesand re-established relations with the Vatican. Since that time,the Catholic church hierarchy in Mexico has increased its pres-ence in political affairs, particularly with regard to reproduc-tive and sexual rights. It now exercises considerable pressureon public authorities and politicians.
On 3 August 2000, just one month after the PAN victory in thepresidential elections, an ultra-conservative group of local PANrepresentatives in the state of Guanajuato passed restrictivelegislation that revoked rape survivors’ right to legal abortion.They argued that current legislation was anti-constitutionalbecause it gave power to penal investigators, rather than judges,to determine whether a rape had been committed. They alsoargued that the country and particularly voters in the state ofGuanajuato, had expressed their overwhelming support of thePAN in the July 2000 elections and that this gave the PAN theresponsibility to legislate its party position on abortion. Thisinterpretation of the vote caused outrage, as a large portion ofthose who voted for the PAN presidential candidate were ac-tually voting against the PRI.
Mexico City pro-choice NGOs coordinated with local activistsin Guanajuato. On 6 August, they organised a protest of about200 women outside the state Congress during the governor’spresentation of his official report, including the mother of theyoung girl whose right to legal abortion had been obstructedby PAN officials in Baja California. A group of local activistsand NGOs from seven cities in the state threatened to take theissue to the United Nations and the Inter-American Court ifthe reform was not vetoed. Public condemnations of the re-form by dozens of NGOs were published in the papers through-out the month. At least 12 women’s groups from the states of
The Johannesburg Initiative
Advocating for abortion access
208
Chiapas and Veracruz published a letter to Fox, the nationalPAN president, and an organized group of Fox supportersdemanding the legalisation of abortion. Demonstrations wereorganised in several other cities, including Guanajuato, SanLuis Potosí and Chilpancingo.
On 7 August, leading reproductive and sexual rights NGOs inMexico City organised a press conference in front of the na-tional PAN party headquarters, in which some feminist lead-ers from Guanajuato were also present. Using their experi-ence in mobilising the media, they demonstrated their indig-nation and complete opposition to the reform. They proposedthree possible solutions: a veto from the state governor, a newlegislative proposal from the other political parties or a proc-ess to review the constitutionality of the reform.
Directly following this meeting, national PAN leaders andMexico City PAN legislators expressed their opposition to thereform and urged the governor to veto the reform. This dis-sent led to ruptures within the PAN, mainly against theGuanajuato legislators. A national newspaper surveyed twenty-three PAN legislators and governors. Fifteen expressed theiropposition to the reform while only eight supported it. Thegovernor of Guanajuato froze the reform and called a publicconsultation, paving the way for a veto. The public consulta-tion would serve as a means for basing his veto on public willand would protect him from criticism.
During the following weeks, legislators from all parties, politi-cal leaders, intellectuals, the media and a wide variety of civilsociety groups strongly condemned the Guanajuato reform.Opposition to the reform from PRD and PRI leaders, legisla-tors and officials ranged from charges of disregard for legisla-tive procedures, imposing house majority at the last minuteand without previous discussion, links to the Catholic church,fundamentalism and disregard for international treaties. Fed-eral officials working in women’s affairs also condemned thereform for this latter reason. PRD leaders and legislators pub-lished a declaration expressing their rejection of the reform onthe basis that it challenged secularism and violated Mexico’s
Mexico
209
commitments in international accords. Women PRI legislatorspublished a similar public declaration against the reform andthe Federal Congress sent a recommendation to the governorof Guanajuato to veto the reform.
The PRD established alliances with the PRI in opposition tothe reform only months after vehemently disassociating itselffrom the PRI during the presidential race. By doing so, it sym-bolically emerged as an opposition force to the newly empow-ered PAN and its alliances with the Church, thus respondingto the public’s concern about how the new administrationwould treat the separation of Church and state.
On the other hand, the reform received overwhelming sup-port from the Catholic church hierarchy and anti-choice groups.Priests from different parts of the country expressed extremeopposition to abortion under all circumstances, even rape.Some referred to the anti-reform efforts as part of an interna-tional population control campaign. A very small number ofprogressive priests expressed relatively liberal views towardsabortion in cases of danger to the woman’s life and arguedthat it is unjust to imprison a rape victim who chooses to abort.
A Guanajuato anti-choice NGO used the media to foster sup-port for the reform. They published anti-choice pictures andmessages in the local papers, including a full-page announce-ment offering housing, medical expenses and adoption pro-cedures for rape victims. The president of the Mexican Pro-Life Committee expressed support for the reform and took theopportunity to appropriate the word ‘homologar’ (unify). Thiswas a pro-choice term first used by GIRE in 1998 in a strategythat encouraged states with stricter abortion legislation to in-crease exceptions to legal abortion in accordance with lawsfrom other more liberal states. Using the term to his advan-tage, the Pro-Life president called all states to further restrictlegislation by unifying it with the Guanajuato reform, whichhad yet to be ratified. He also said that the Guanajuato stategovernor should not betray his party’s principle to defend lifefrom conception. He demanded that Fox amend the constitu-tion to reflect this stance and install stricter penalties for abor-
The Johannesburg Initiative
Advocating for abortion access
210
tion practitioners. Pro-Life also organised rallies in favour ofthe reform and mobilised affiliates in different states, particu-larly Mexico City and Guanajuato.
In anticipation of biased results of the governor’s poll, repro-ductive and sexual rights organisations from Mexico City or-ganised a parallel poll in Guanajuato and presented its resultsin a press conference three days before the governor publi-cised his results. The poll showed that 63% of a representativepool of Guanajuato residents were against penalising abor-tion for rape victims and that 83% believed abortion shouldbe allowed under one or more circumstances. In addition, 94%believed that polls should be carried out prior to the passageof abortion legislation.
The results of the governor’s poll, presented on 28 August,also showed majority disapproval of the reform (53%) andfavoured further discussion in the congress (68%). (Centre ofOpinion Studies, 2000). While the impact of the NGO poll onthe governor’s decision is unknown, it clearly served to showthat feminist groups were closely following developments andwould not accept any poll that showed contrary results. Thegovernor vetoed the reform on 29 August.
The role of President-elect Vicente Fox in the initiative wasquestioned immediately after the release of news of the re-form in the papers. Some believe that Fox ordered the initia-tive to test the waters for future reform attempts at the nationallevel. This was denied by Fox and his administration, whoclaim that Fox knew nothing of the proposed reform, whichthey maintain was a strictly local affair that in no way reflectedfuture national plans. Nevertheless, the reform clearly repre-sents party policy to protect life from ‘conception’ and Fox’sown personal position on abortion.
Regardless of the origin of the proposed reform, the result ofthis political mistake has been favourable to abortion rightsand damaging to the PAN. Not only did it trigger liberalisinglegislation in Mexico City; it also obliged Fox and his adminis-tration to state publicly that no such initiatives would be made
Mexico
211
at the national level under the Fox administration, despite theirparty or personal convictions. It also sparked national debatein which public opinion expressed pro-choice values as neverbefore, thus providing a basis for the subsequent Mexico Cityreform.
Legislative reform in Mexico City, August 2000In the midst of the heated debate on the Guanajuato reform,the Access Campaign requested a meeting with the mayor ofMexico City to renegotiate its abortion reform proposal. Themayor was now Rosario Robles, who took over when Cárdenasresigned to enter the presidential race. Robles had previouslytold the Access Campaign that she would introduce legislativechanges on abortion following the elections, regardless of theiroutcome, during a one-month window in which the PRD wouldmaintain the majority in the house. The PRD had been plan-ning for a special session on 18 August. Robles responded tothe Access Campaign’s request to discuss the matter and calleda meeting on 10 August in which she informed campaign rep-resentatives that she would place part of their abortion pro-posal on the agenda.
The abrupt change in Robles’ and the PRD’s position towardsliberalising abortion was in clear response to the Guanajuatoreform and the overwhelming opposition against it by politi-cal and opinion leaders and diverse sectors of civil society.These factors created favourable conditions for liberalising re-form that would have virtually no negative political costs foreither Robles or the PRD. The opportunity also came at a timewhen the PRD was working to recuperate from the profoundsetbacks it had suffered in the presidential elections. If the PRDcould use the topic of abortion wisely, it could possibly gainback some of the support it had lost from liberal sectors thatincluded feminists unhappy with the PRD’s refusal to act in1999. It would also allow Robles to strengthen her public im-age and her position within the PRD before leaving office.
The initiative was presented on 14 August with the presence,support and participation of numerous intellectuals, writers,
The Johannesburg Initiative
Advocating for abortion access
212
leaders, feminists and union members as well as legislators,politicians, local government officials and different sectors ofthe PRD. In her delivery speech, Robles proclaimed that shewas not in favour of abortion, but rather of the right to volun-tary motherhood. She called on the presidents of the PRI andPRD, both women, to support the initiative and criticised Foxfor his silence on the intolerant attitudes of the Guanajuatostate legislators.
The Access Campaign helped develop the content of the finalversion of the initiative, which eliminated sanctions for abor-tion in cases of danger to the woman’s health and foetal mal-formation. It also included specific procedures to guaranteeaccess to legal abortion services for rape survivors and obligedMexico City public health institutions to provide them. Althoughthe initiative excluded the original Access Campaign proposalto eliminate sanctions for economic reasons, the member NGOsconsidered it an important step forward and decided to give ittheir full support.
Throughout this process, the Access Campaign lobbied legis-lators, provided specialised information, helped organise thepresentation of the initiative, participated in the elaboration ofthe initiative itself, advised Robles, gathered support throughpress conferences, paid for advertisements and gave interviewsto the media. This was a continuation of the work begun in1999. The Access Campaign’s activities were an importantcounter to Pro-Life and the Catholic church’s efforts and acrucial support for Robles.
The day of the special session, 18 August, the Access Cam-paign placed several paid advertisements regarding the pro-posed abortion legislation in national papers. One was signedby women activists, artists, actresses and academics in favourof the initiative. It explained that the decriminalisation of abor-tion has been a central demand of the Mexican feminist move-ment for years.
Mexico
213
The public debateThe abortion initiative was a major topic in the newspapers,radio and television throughout the days before and after itsapproval on 18 August. This period overlapped with the ongo-ing decision-making process regarding the Guanajuato reform,which was resolved by the Governor’s veto on 29 August.
Robles and the PRD legislators faced serious political pressurefrom the other political parties, particularly the PAN. Robleswas criticised for introducing a last minute initiative in a simi-lar manner to the Guanajuato legislators and the PRI and PANopposed holding the special session. She was also accused ofexercising vertical and authoritarian practices common to thePRI. Moreover, PAN leaders in Mexico City warned her thatthe ‘polarising strategies of the PRD could endanger dialogueon the entire political reform’ and announced that the PANlegislators who were to enter office in September 2000 wouldscrutinise legislation passed by the PRD (Universal, 13 Au-gust). President-elect Vicente Fox’s ‘transition team’ also ve-hemently criticised Robles. They asked her to retract the initia-tive on the grounds that it did not have consensus among thepopulation, was unilateral, arbitrary, antidemocratic and au-thoritarian. Fox himself never made a statement on the initia-tive.
The initiative was generally supported by the PRD parlia-mentary legislators. They prioritised party interests over anydiscomfort with the manner in which they were practicallyobliged to pass the legislation only one year after avoidingintroducing discussion of the topic to protect the PRD in thepresidential election. The initiative also had the full supportof PRD party leaders, government officials and the party presi-dent. On the other hand, the PRD mayor-elect had statedduring his campaign that abortion was not on his politicalagenda. He avoided reproductive and sexual rights NGOsrequesting his support for an abortion reform and simplyclaimed to ‘respect but not share’ Robles’ position (Jornada,13 August).

The Johannesburg Initiative
Advocating for abortion access
214
The press and the Mexico City parliamentary legislators quicklypicked up on the contradiction in the sudden change in pos-ture of the Mexico City PRD. The Access Campaign refrainedfrom bringing attention to this, recognising that it was the lastchance to pass legislation before the PRD would lose its ma-jority.
The oppositionThe Catholic church’s attempt to mesh secular democratic dis-course with religious discourse as a means to cloak its interfer-ence in matters outside its field of action was the object ofridicule by press cartoonists. The Catholic hierarchy claimedthat Robles’ initiative was against God’s will and threatened toexcommunicate any person who participated in or directly orindirectly promoted abortion. They wisely excluded Robles,however, who commands a strong approval rating in the city.The Church indirectly incited followers to civil disobedience ifthe initiative were approved. The Church urged PRD legisla-tors to change their minds by praying, because one does not‘play’ with the Bible and accused the PRD of not having ana-lysed the problem ‘with the Superior’ (Jornada, 12 August).
Pro-Life first reacted with verbal attacks and unsuccessful pub-lic protests. They invited anti-choice militants, some with crimi-nal records, from the United States and Canada to their dem-onstrations. The Ministry of Foreign Affairs fined Pro-Life andsanctioned the foreigners for trying to influence national poli-tics. After the initiative’s approval, Pro-Life threatened to un-dertake a ‘war against Rosario Robles and the PRD’ and tostop paying their water bills (Jornada and Milenio, 13 August).
ProLife criticised the legalisation of abortion for foetal impair-ment and persuaded organisations for the disabled to publiclyoppose the initiative. They symbolically closed reproductivehealth clinics in Mexico City and Yucatan where they claimedillegal abortions were being performed. In what appears to bethe beginning of a new phase in Pro-Life Mexico’s strategy,they pressured police in Chiapas to raid a clinic and detainstaff in October 2000.
Mexico
215
The day of the special session, the Illustrious National Collegeof Mexican Lawyers and the Archdiocese of Mexico publishedseparate public advertisements asking legislators not to ap-prove the initiative. The Archdiocese of Mexico announcedthat the Catholic church would soon disclose more concreteactions to stop the attempts to decriminalise abortion in MexicoCity. The day after the reform passed into law, the Archdio-cese promoted a march organised by anti-choice organisa-tions. The march did not have any significant repercussions.
The legislative debate: August 18The PAN continued to pressure Robles to retract the initiativeuntil the last moment and disclosed that it would attend thesession to vote against the initiative. The PRI announced thateight of its eleven legislators would attend and vote in favour.
Pro-Life organisations, PRD affiliates and Access Campaignmembers demonstrated simultaneously outside the parliamentbuilding. Throughout the ten-hour session, legislators debatedin two blocks – the PRI and the PRD on one side and the PANon the other. In the beginning, the PAN desperately tried topostpone the debate until the next legislature in which theywould have house majority, but they were unsuccessful.
PRD legislators relied heavily on documents prepared andprovided by the main NGOs from the Access Campaign. Theyrelied particularly on GIRE, whose documents were used bylegislators, in some cases verbatim. During the previous days,GIRE had worked to produce, gather and distribute materialswith technical information that would allow the legislators topresent their positions with well-founded arguments. The workto inform legislators on the situation of abortion in Mexicohad begun the previous year, with talks and presentations ofthe Access Campaign’s demands as well as through the distri-bution of materials and participation in information-sharingmeetings.
The law reform was approved as expected. The final vote wasforty-one in favour (32 PRD, s PRI, 2 from minor parties);seven against from the PAN; and one abstention from a former
The Johannesburg Initiative
Advocating for abortion access
216
member of the PAN who later joined the PRD. The supportgiven to the reform by seven of the eleven PRI legislatorsbrought an important consensus to the approval, although itwas very clear that the whole reform process was wrought withopportunism, top-down decision making and political inter-ests.
The debate was unprecedented. For the first time in Mexicanhistory, abortion was widely discussed in parliament and re-ceived the attention it deserved, with the support of publicopinion and the participation of women’s groups as observersand supporters inside the parliament building throughout thesession.
ConclusionThis historical event in the struggle for safe legal abortion inMexico was part of a complex transition in the national politi-cal system. It is indisputable that the larger political contextplayed a fundamental role in the passage of legislation.
Obstacles and facilitating factorsThe main obstacles to abortion reform promoted by the Ac-cess Campaign in 1999 can be summarised as follows:
• The refusal of all parties to include the issue of abortionin their legislative agenda in 1999 due to the proximityof national elections.
• The PRD’s failure to inform the Access Campaign thatthey had decided not to reform abortion law in 1998.This had a big impact on the member organisations,which put much energy into their advocacy efforts andbecame disillusioned with the PRD when their demandswere not attended.
• Legislators’ fear of opposition from the Catholic Church,Pro-life groups and the PAN.
• The Access Campaign’s excessive confidence in the PRD.This was based on PRD electoral promises and platform

Mexico
217
principles that favour voluntary motherhood as well asthe deep political sympathy of some feminists for thePRD, since this party formed part of traditional left-wingsectors linked in various ways to the feminist movement.
• Feminist NGOs’ limited experience in developing multi-ple-NGO sustained advocacy strategies for legislativechange.
• The lack of explicitly expressed support from a wide con-stituency that supports abortion law reform.
• Limited data about legal abortion to provide decision-makers with solid arguments in support of liberalisation.For example, there was no or limited data on the eco-nomic costs of clandestine abortion for the public healthsystem, the different effects of clandestine abortion onlow and high income populations, or the true mortalityrate for clandestine abortion.
• Limited economic capacity of the reproductive and sexualrights movement to contract legal consultants, as well asthe lack of lawyers working in this field.
• Limited funding for major pro-choice media campaigns.
• The NGOs’ rationalist approach to legislative reform inthe beginning of their advocacy work, which made itdifficult for the movement to evaluate correctly the po-litical interests before the 2000 national elections. Politi-cians’ analysis was based on what they thought wouldbe negative costs of taking any measure to liberalise abor-tion, even when they agreed ideologically with the is-sue. These factors had far more weight than any NGOattempt to provide solutions to the problems related toclandestine abortion in Mexico.
Several factors at the macro-level influenced the Mexico City’s2000 reform. These, together with the Guanajuato veto, re-sulted in relative success for the liberal sectors of Mexico and aharsh loss for the Church, the PAN, Pro-life organisations and

The Johannesburg Initiative
Advocating for abortion access
218
conservative groups in general, which they have still not ac-cepted. The factors include the following:
• Ongoing changes in the Mexican political system thatfostered state reform, facilitating a gradual increase indemocratic elections and new possibilities for the par-ticipation of several young political parties representingdiverse sectors of society.
• The ousting of the PRI in the presidential elections.
• The fact that abortion was seen as part of a wider debateon the separation of Church and state, within the con-text of increasing participation of Catholic church hier-archy in political affairs and an uncertain future of thesecular state.
• Steadily increasing possibilities for public debate on abor-tion, seen at this time as a topic of national interest. Incontrast to previous debates (Kulczycki, 1999), the ma-jority of the media, including TV, radio and the press,gave considerable support and space to different actorssupporting the Mexico City reforms and rejecting theGuanajuato reform attempt.
• Increasing participation of civic groups, which are lessreluctant to express ideas on national political issueswithin the context of the historical defeat of the PRI.
• A persistent – yet unfruitful – struggle for liberalising abor-tion laws in Mexico by feminist individuals and organi-sations over the last 30 years.
• The existence of a range of organisations grouped in theAccess Campaign able to carry out specialised work, suchas advocacy, organisational, informative and media.
• The ability of NGOs to overcome differences and to worktowards a common goal.
• The respect won by feminist NGOs in the media throughlong and consistent work as part of an strategy that in-cluded maintaining permanent relationships with the
Mexico
219
press and responding to all their needs for informationon sexual and reproductive rights.
• A feminist discourse elaborated over several years re-garding the need for liberalising abortion laws, whichwas taken up by the media and public servants. It wasdeeply rewarding to hear the PRD legislators, RosarioRobles and other politicians using feminist informationand arguments to support their positions during the par-liamentary debates and other public speeches.
Current status of the Mexico City andGuanajuato reformsAlthough the abortion reforms were approved in the MexicoCity parliament in accordance with legal procedures, twenty-two legislators from the PAN and the Mexican Green Ecologi-cal Party made an appeal of unconstitutionality to the Na-tional Supreme Court of Justice. They argue that the reformviolates the Mexican constitutional guarantee of the right tolife and that it unlawfully permits public prosecutors to author-ise abortions in the case of rape, a faculty strictly limited tojudges.
It is not difficult to prove that the appeal lacks legal grounds,first and foremost because there is no constitutional right tolife from the moment of conception. In terms of the secondargument, if a judge were to authorise an abortion, the proc-ess would be too lengthy to be effective. A legal basis still needsto be developed to supplement this practical point, however.Appeals of this kind typically take from eight to ten months toresolve and NGOs are already working to provide the SupremeCourt judges with legal arguments.
The future of the reform may also be at risk because the PRDno longer has a strong presence in the new Mexico City parlia-ment and the PAN has much more power in national politicssince the installation of the Fox administration in December.Even so, the PRD has retained the governorship of MexicoCity and the PRD governor has the power to veto any intentto revoke the abortion reform.
The Johannesburg Initiative
Advocating for abortion access
220
With regards to improvements in access to legal abortion, theMexico City government has made no statement, campaignor programme to guarantee the implementation of the abor-tion reform. Because the reform is currently subject to appeal,it is difficult to advance in concrete areas so as to ensure thatthe reform offers real access to legal abortion for qualifyingwomen.
It is possible that the Guanajuato PAN legislators could intro-duce a reform similar to the one the governor vetoed in Au-gust, although the PAN suffered great political loss after thescandal it raised.
ReferencesCentre of Opinion Studies (2000) ‘Estudio para conocer lapercepción de la población del estado de Guanajuato sobre lapenalización de la práctica del aborto: Conclusiones’,Guadelajara University, unpublished.
Consejo Nacional de Población (1996) Indicadores Básicos deSalud Reproductiva y Planificación Familiar en México, Mexico.
Comisión Nacional de la Mujer (2000) Mexican Report onImplementation of the Beijing Platform for Action, México.
Raúl López García (1994) ‘El Aborto’ in MC Elú & A Langer(eds) Maternidad sin riesgos en México, México: InstitutoMexicano de Estudios Sociales.
Poder Ejecutivo Federal (1995) Programa de SaludReproductiva y Planificación Familiar, 1995-2000, Mexico.
Grupo de Información en Reproducción Elegida (1997)Boletín, 12.
Instituto Alan Guttmacher (1994) Aborto clandestino: Unarealidad latinoamericana, New York.
Kulczycki A (1999) The Abortion Debate in the World Arena,New York: Routledge.
Ortiz-Ortega A (2001) ‘If men would get pregnant, would abor-
Mexico
221
tion be legal?’, Mexico: Population Council–EDAMEX.
Women’s Environment and Development Organisation (1999)Riesgos, Derechos y Reformas, New York.
IntervieweesNGO representatives Orfe Castillo, Eduardo del Castillo, AnaMaría Hernández, Marta Lamas, Patricia Mercado, PilarMuriedas, Pilar Sánchez, and María Luisa Sánchez Fuentes;public legislators Martí Batres (PRD), Ángeles Correa (PRD),Angélica Luna Parra (PRI) and Octavio West (PRI); and PatriciaOlamendi (former leader of the Mexico City Women’s Insti-tute under the PRD).
AuthorsAna Cortés is a social anthropologist, member of theInterinstitutional Relations Program Area at the InformationGroup on Reproductive Choice (GIRE) and formerly memberof the Research Programme Area. She participated in the de-velopment of Mexico’s NGO Report for CAIRO+5, andBeijing+5. She participated in GIRE’s advocacy work withthe Ministry of Health for changing national regulations re-garding reproductive health services and currently also worksas a research consultant at the Population Council Office forLatin America in Mexico City.
Sharon Bissell is the Development Coordinator at GIRE, whereshe has worked since 1996. She has supported several Mexicanreproductive and sexual rights organisations in fundraising andproject development, has developed a case study on thenational network National Forum of Women and PopulationPolicy for Health, Empowerment, Rights and Accountabilityin preparation for Cairo+5 and translated the national networkMilenio Feminista´s NGO report on the implementation of theBeijing Platform for Action prior to Beijing+5.

The Johannesburg Initiative
Advocating for abortion access
222

Poland
223
STRUGGLES FOR AND AGAINSTLEGAL ABORTION IN POLAND
Wanda Nowicka
Federation for Women and Family Planning
Population size
Women of reproductive age,15-494
% population living in urbanarea
Gross domestic product percapita
Human development index
Literacy rate of women15+
% hospital births
Maternal mortality rate
Religious affiliation
Abortion legal status
38,654,000
10,215,100
65%
US$ 7,619
0,814
100%
99%
8 per 100,000 live births
95% Roman Catholic
Legal in cases of rape,maternal health or severe andirreversible damage of foetus
The Johannesburg Initiative
Advocating for abortion access
224
IntroductionJune 4, 1989 marked the victory of democratic forces in par-liamentary elections and is the symbolic date of the end ofCommunism in Poland. Since then, those favouring women’sright of choice in Poland have faced a paradox. The politicalchanges that resulted in the establishment of a democratic statehave brought about restrictions on women’s rights as an unex-pected side-effect. The abortion issue in Poland has been sub-ject to constant flux since democratisation – up, down, left,right, back and forth, to and fro – and is still far from beingresolved to anyone’s satisfaction.
The legal status of abortion in PolandAbortion was legalised in Poland in 1956. The regulations al-lowed abortion on social grounds, which meant that abortionwas available practically on demand for almost forty years.Although exact figures do not exist, it is estimated that therewere between 180,000 and 300,000 abortions per year dur-ing this period.
During the nineties, this abortion law changed several timesand current legislation states that abortion is legal only underthe following conditions:
• if the pregnancy constitutes a threat to the life or healthof a mother and the existence of a threat is confirmed bya doctor other than the one conducting the abortion;
• if pre-natal examinations or other medical analysis indi-cate a high probability of severe and irreversible dam-age to a foetus or incurable disease, threatening the life
Poland
225
of a child. Again, this must be confirmed by a medicaldoctor other than the one conducting the abortion; and
• if there is confirmed suspicion that the pregnancy is aresult of a criminal act. The termination of pregnancy inthis case is allowed if a woman is less than 12 weekspregnant. The criminal circumstances must be confirmedby a prosecutor.
In the first two instances the termination is performed in a publichospital. In the third the termination may also be carried outin a private clinic.
Effects of the anti-abortion lawThe Federation for Women and Family Planning has beenmonitoring the implementation of the law since its inception.Studies conducted by the Federation in 1999 and 2000 con-firm the results of research conducted by the organisation in1993 and 1996. The main findings are as follows:
• The anti-abortion law did not eliminate and probablydid not diminish the phenomenon of abortion. Illegalterminations are still common. The scale of the phenom-enon can be estimated at between 80,000 and 200,000abortions per year.
• Illegal abortions are conducted by doctors and are veryexpensive. The phenomenon is known as the ‘abortionunderground’.
• Some women travel abroad to have an abortion. Thisphenomenon is known as ‘abortion tourism’. It appearsto be decreasing and currently has more of an individualthan institutional character.
• Restrictive regulations have not eliminated abortions onsocial grounds. Instead they have resulted in serious limi-tations on access to legal abortion. Public hospitals ter-minate very few pregnancies. Many women who have aright to abortion according to the law, but for variousreasons cannot exercise this right, are increasingly turn-ing to the abortion underground for solutions.
The Johannesburg Initiative
Advocating for abortion access
226
• Knowledge about conditions for lawful termination ofpregnancy is highly unsatisfactory, both in the society ingeneral, as well as among medical staff.
• The anti-abortion law results in personal trauma andcauses substantial health problems for hundreds of thou-sands of women in Poland every year.
The anti-abortion law is much stricter de facto that it is de jure.Women who are entitled to legal abortion under the Act arevery often denied the termination. Since 1993 the accessibil-ity of legal abortions in public hospitals has deteriorated, withsome hospitals publicly admitting that they do not conductabortions.
StatisticsAccording to the 2000 government report on the implementa-tion of the Act on Family Planning, only 151 legal abortionswere performed in public hospitals in the entire country in1999. This is half the number of abortions performed in 1998.The numbers are particularly striking if we remember that inPoland there are more than ten million women of reproduc-tive age and contraceptionis practised only to a limited extent.Low numbers of official abortions indicate the existence ofmany barriers in service provision.
The real number of abortions in Poland was not known evenwhen the termination of pregnancy was legal and widely prac-tised. Available statistics only covered abortions performed inpublic hospitals. Most abortions were carried out in privateclinics and were thus not included in official statistics. The of-ficial number of abortions in the eighties was approximately120,000. The real figure could have been up to three timesmore.
It is currently even more difficult to determine the real numberof terminations carried out. The 1998 Act on the Protection ofPersonal Data, which restricts access to hospital registers, hasexacerbated the problem. The Federation’s 2000 Report in-cludes some estimates on underground abortion based on acomparison of demographic data in countries in Central Eu-
Poland
227
rope. The estimates suggest that the number of illegal abor-tions could be as high as 200,000. These estimates are con-firmed by a study carried out among rural women, accordingto which around 90,000 rural women, who constitute 30% ofthe women’s population, had an abortion in 1999.
The abortion undergroundThe abortion underground in Poland is well developed. Ac-cessing a private clinic in which one can obtain an illegal ter-mination is easy in big cities and towns – it simply requires thewoman to find the relevant press announcement. In small townsand villages, however, doctors are not anonymous and areafraid of stigmatisation. Further, even if it were possible to finda local doctor who performs abortions, women prefer to traveloutside of their community to be sure that the procedure re-mains confidential.
The price for an illegal abortion is usually between 1,500 PLN(US$330) and 3,000 PLN (US$675). The RU-486 pill, whichhas not been registered for sale, is offered for about 1,000 PLN(US$ 220).
Abortion tourismInformation collected by the Federation suggests that the phe-nomenon of travelling to obtain an abortion is becoming mar-ginal. Between 1995 and 1997 there were several court trialsof agencies that had organised abortions across the easternand southern borders of Poland. The trials effectively scaredoff potential organisers. For women the decrease in the prac-tice means less choice and an increase in price, because termi-nations are usually more expensive in Poland than abroad.
Struggles over abortionPhase I: Implementation of Anti-Abortion Actof 1993There was no public debate on abortion under communism.Abortion was not considered an issue, the liberal law was takenfor granted by society and was not questioned publicly by any-
The Johannesburg Initiative
Advocating for abortion access
228
one. The Roman Catholic Church was not very active on thetopic before the election of the Polish Pope in 1978. In theeighties anti-abortion ideas began developing within theChurch, the Solidarity movement and in medical and legalcommunities. The struggle for independence was a priorityfor those groups, however. Society in general , on the otherhand, was completely unprepared for anti-abortion actions. Itdid not believe in the possibility of restricting abortion and,since it did not have to defend the right to choose for almostforty years, lacked pro-choice arguments.
The first unsuccessful attempt to challenge the 1956 abortionregulations occurred in 1989, shortly before the first demo-cratic elections. The restrictive draft on the protection of theunborn child proposed to criminalise women who underwentillegal abortion and impose a punishment of up to three yearsin prison. Many members of the anti-communist oppositionbecame actively involved in the anti-abortion campaign whichwas strongly supported by the Roman Catholic Church hier-archy and had the personal backing of Pope John Paul II.
The next attempt was in 1990. Fundamentalist members ofparliament (MPs) hurried to ‘make the gift’ to the ‘SaintedFather’, John Paul II, before his visit to Poland in 1991. Duringthe parliamentary debates on abortion in 1991 the Sejm an-nounced national consultations on the anti-abortion draft.These consultations were used successfully by anti-choicegroups to give the impression that many people supported arestrictive law. The church arranged for signatures to be col-lected in churches and at schools by parents of children at-tending religious instruction. As a result, the anti-choice groupsmanaged to collect far more signatures than pro-choice groupsalthough all the opinion polls showed that the majority of thesociety was against criminalisation of abortion. Yet this bill alsofailed.
An even more restrictive bill was tabled in 1992 by membersof the Christian National Union, the most fundamentalist party.According to the draft, abortion would have been legal only tosave a woman’s life. A woman who underwent an illegal abor-
Poland
229
tion and a doctor performing such an abortion could havebeen sentenced to up to two years in prison. The draft evokedstrong opposition. Two members of parliament, Zbigniew Bujakof the Labour Union and Barbara Labuda from the Demo-cratic Union, initiated a grassroots movement called the Com-mittee for Referendum. The Committee called for a nationalreferendum on. Thousands of people across the country col-lected signatures in support of a referendum, with over1,300,000 signatures finally filling a petition. Parliament ig-nored the petition and rejected a bill proposing a national ref-erendum on abortion, but also rejected the restrictive anti-abor-tion bill. The bill was sent to the Extraordinary ParliamentaryCommission, together with a more liberal bill, which had beenproposed by the Women’s Parliamentary Group. As a result, anew, compromise bill was drafted and finally passed by parlia-ment in January 1993. The new law was called the Act onfamily planning, human embryo protection and conditions ofpermissibility of abortion. Under the Act, abortions on socialgrounds were made illegal. In practice, it meant that womenin difficult socio-economic conditions could no longer legallyhave abortions.
Phase II: Failure to liberalize the anti-abortionactIn 1994 the ‘left-wing’ parliament made an attempt to over-turn the restrictive law and passed an amendment accordingto which abortion would be legal on social grounds. Tthe Presi-dent, Lech Walesa, vetoed the bill and the initiative failed.
While fundamentalist clergy continued to oppose legal abor-tion, a lay movement was established in the nineties. The firstorganisation to become influential politically was the Pro LifeFederation, established in 1993.
Phase III: Liberalisation of the anti-abortion actIn 1996 pro-choice parliamentarians made another attemptto change the law when, as a result of presidential elections,the new pro-choice President Aleksander Kwasniewski waselected. Abortion again became a public issue. Women’s
The Johannesburg Initiative
Advocating for abortion access
230
groups, together with a group of supportive parliamentarians,cooperated closely to change the law. The Federation forWomen and Family Planning played an active role in thischange. The effects of the anti-abortion regulations were pub-lished in two reports launched by the Federation and publi-cised widely in the media and the Federation participated inthe Parliamentary Commission that formulated the final pro-visions of the new bill.
Anti-choice activists and Catholic priests also participated inthe Commission and worked closely with anti-choice MPs. Atthat time right wing forces were in the minority in the Parlia-ment and could therefore not succeed in keeping anti-abor-tion law intact. They did manage, however, to slow down theprocess and to oppose more liberal provisions proposed bypro-choice MPs.
The Extraordinary Parliamentary Commission debated theissue for over three months in early 1996. The Commissiondrafted a bill in terms of which (a)abortion would be legal ifthe woman was in difficult life circumstances; (b)sex educationwould be introduced into schools; and (c)several brands oforal contraceptives would be subsidised by the state so as toencourage widespread use of contraception. The anti-abor-tion law was amended by the Polish parliament in August 1996and was signed by President Kwasniewski. It came into forceon 4 January 1997.
Phase IV: Abortion law becomes restrictiveagainIn the two months prior to the vote, the trade union Solidaritytook a leading role in trying to defeat the bill as part of theiraspiration to leadership in the right-wing coalition during the1997 elections. Solidarity challenged the new law in the Con-stitutional Tribunal, which decided that abortion on socialgrounds was unconstitutional. It justified its decision on thegrounds that Poland is a democratic state of law, which it inter-preted as meaning that it should protect life at every stage.Article 38 of the Polish Constitution includes only the general
Poland
231
provision of legal protection for the life of every human being.The Tribunal’s decision and its justification were seen as anover-interpretation by many prominent lawyers, but the deci-sion was accepted by the new right-wing Parliament elected in1997, which comprised many anti-choice activists as MPs andsenators.
The new Constitution was finally adopted in 1997 after con-tinued debates which lasted several years. Anti-choice and pro-choice groups used the opportunity to promote their issues.Pro-choice groups tried to include a provision around repro-ductive rights by lobbying MPs and by organising a campaignto send letters to Parliament. The anti-choice lobby pushed forthe inclusion of the protection of life from the moment of con-ception to natural death. Both proposals failed. As a result,the right-wing mobilised vast protests which unsuccessfullycalled on society to reject the Constitution during the constitu-tional referendum.
Main anti-choice actorsThe primary objective of the anti-choice lobby has always beento introduce a complete ban on abortion, as proposed in thevery first drafts. They also believe that a woman who under-goes an illegal abortion should be penalised. They are there-fore dissatisfied with the present law. The most fundamentalistmembers of parliament voted against the 1993 anti-abortionlaw because it was too liberal for them and the anti-choicemovement has been putting strong emphasis on restrictingaccess to legal abortion. Many anti-choice doctors have occu-pied powerful positions in medical associations. From thesepositions, they have been able to influence official standardsand ethical and medical guidelines as well as target and in-timidate other doctors, as described below. By cooperatingclosely with the medical community, the anti-choice move-ment succeeded in limiting access to abortion on medicalgrounds. In cases of teenage pregnancy resulting from rape,the Government Plenipotentiary for Family Affairs, one of thestrongest fundamentalists, was among those who spoke pub-
The Johannesburg Initiative
Advocating for abortion access
232
licly against abortion. The anti-choice activists have been alsostruggling to pass the law to introduce limitations to prenatalexaminations that are necessary to obtain permission for abor-tion on genetic grounds. Their efforts are described below.
Solidarity movementThe Solidarity movement that led to the overturn of commu-nism comprised many opposition groupings. It was predomi-nantly a trade union though, which rooted its ideology in theRoman Catholic religion and was strongly supported by theRoman Catholic Church. The anti-choice agenda existed withinthe movement even in the eighties as one of the undercur-rents not visible to the majority of society. However, it becameone of the priority issues for Solidarity in the nineties. In 1990Solidarity committed itself to undertaking both legal and otheractivities to protect life from the moment of conception untilnatural death. In 1992 Solidarity, during its General Assem-bly, adopted a motion to support the restrictive anti-abortiondraft which was then being debated in parliament.
The position of Solidarity as a whole was opposed by theWomen’s Section of the Solidarity (WSS). According toMalgorzata Tarasiewicz, the head of the Women’s Section, thecontradictory stance of the WSS caused the closure of the sec-tion by the extreme fundamentalist Marian Krzaklewski, theSolidarity leader since 1991, member of parliament since 1996and one of the unsuccessful candidates for President in 2000.
When the anti-abortion law was liberalised in 1996, Solidarityleaders proposed civil disobedience and called on supportersnot to pay taxes since abortions in public hospitals are cov-ered by taxes. Further, Solidarity took the liberalised anti-abor-tion law to the Constitutional Tribunal and won, as reportedabove.
Solidarity Election Action (AWS) is a coalition of small rightwing parties and the trade union formed successfully byKrzaklewski before the 1997 parliamentary elections. AWSgained power in the elections, forming a coalition governmentwith the centre party, the Freedom Union. AWS had a so-called
Poland
233
‘pro-family programme’ as one of the priorities on their politi-cal agenda. The pro-family programme was opposed to abor-tion, contraception and sex education.
Since 1997 the parliament and government have systemati-cally implemented policies that effectively restrict access to le-gal abortion as well as limit access to modern contraceptionand sex education.
Roman Catholic ChurchCatholics constitute about 95% of the population and theRoman Catholic Church has always played a significant rolein the predominantly Catholic society. During the communistregime, it promoted the movement for independence and gaveshelter to opposition activists. When communism collapsed,the position of the Church increased significantly, due to thefact that the former opposition became the ruling power. Sincethen, the Church hierarchy has been exerting a strong influ-ence on legislators and the government to promote theiragenda.
The main priorities of the Church are (a)to strengthen its for-mal position within the state structure by promoting theConcordat – the agreement with the Vatican that dismantledthe separation of church and state; (b)to introduce Catholicinstruction in public schools; and (c)to restrict legal abortionand other reproductive rights.
In the early nineties the Church, supported strongly by PopeJohn Paul II, directly pressured decision-makers to introducerestrictive legislation. The Church also exerted a strong influ-ence on the medical community which introduced the contro-versial Medical Code of Ethics restricting abortion even beforethe anti-abortion law was introduced. In the third and fourthphases of the struggle against abortion, the Church changedits strategy slightly and took a less public role. It was less visiblein abortion debates than previously because of a perceiveddecrease of acceptance within society for the excessive involve-ment of the Church in public affairs. Nevertheless, the Churchcontinued to support the activities of a growing anti-choice
The Johannesburg Initiative
Advocating for abortion access
234
movement and utilised religious pulpits during Sunday massesfor anti-abortion preaching.
The pope is well known worldwide for his extreme anti-abor-tion position. He travelled to Poland four times in the ninetieswhere he often made very strong statements on abortion. Hisspeeches played a significant role in influencing society anddecision-makers. He continues to follow the debates on abor-tion in Poland closely and always publicises his judgements –critical or laudatory – on a particular event. When the Parlia-ment liberalised the law in 1996 the pope stated: ‘The nationwho kills its own children is a nation without a future.’ Duringone of his multiple visits to Poland, he thanked the Pro-LifeFederation for their efforts to build a ‘civilisation of love’ in-stead of a ‘civilisation of ‘death’.
The anti-choice movementThe first organisation to become politically influential againstliberal abortion legislation was the Pro-Life Federation, foundedin 1993. Its establishment was facilitated and supported notonly by the Church hierarchy and its national and local struc-ture and facilities, but also by anti-choice groups from abroad,particularly from the USA, where activists participated in train-ing and meetings. Also in 1993, the Federation’s activists formedHuman Life International (HLI)-Europe, based in Gdansk. HLI-Europe is very active in Central and Eastern Europe in, asthey term it, ‘building a civilisation of life’ by providing leader-ship and capacity-building and supporting the initiatives ofnational pro-life NGOs. Finally, several Catholic women’s or-ganisations came into being, the most important being theCatholic Women’s Forum.
The anti-choice organisations became visible after the 1994Cairo Conference on Population and Development and inten-sified their efforts in respect of the 1995 World Conference onWomen in Beijing. With easy access to the public and Catholicmedia, they have been quite effective in promoting the anti-choice position. They collect far more signatures on petitionsthan pro-choice groups and hold anti-choice demonstrations
Poland
235
that are much larger than those the pro-choice movement canorganise. During and since the change of anti-abortion law theyhave become more active. They put pressure on health person-nel to stop performing abortions and meet with the heads ofhospitals. In some hospitals, women referred for abortion areharassed by anti-choice activists who try to make them changetheir decision to have an abortion. They are reported to publi-cise lists of ‘bad’ doctors, allegedly on the Internet, and theyhold demonstrations in front of clinics performing abortions.
Street actions have been one of the most popular forms ofaction for and against legal abortion. In the early nineties rela-tively successful demonstrations were organised by pro-choicegroups, although they never had more than several thousandparticipants. In contrast, in 1996, the anti-choice groups man-aged to organize two demonstrations of around 30 000 and100 000 participants with the support of Radio Maryja andSolidarity structures. As a result, this form of protest has beengiven up by pro-choice groups for the time being.
Pro-choice groupsThe opposition against the restrictive law has never been verystrong, which is a paradox in a pro-choice society. The oppo-sition consists of a few non-governmental organisations (NGOs)including women’s groups, a few political parties, and indi-viduals from different backgrounds.
Civil society was almost non-existent under communism whenthere was only a single official women’s organisation. In thebeginning of the nineties, the NGO movement emerged. Itlacked skills, human and financial resources and experience,however, and was not successful in mobilising and organisinggreat numbers of supporters. It focused instead on building itsown identity and stability.
Another important barrier obstructing the activities of pro-choice groups was the existing divisions within the movementrooted in the communist past. Several women’s leaders asso-ciated with the struggle against the communist regime had dif-

The Johannesburg Initiative
Advocating for abortion access
236
ficulties in building new partnerships with the pro-choice left,which was mainly of communist background. These divisionsresulted in a pro-choice movement that was weaker than itmight have been. The differences, although much smaller, stillexist today. On the other side, the left has failed so far to de-velop credibility concerning their women’s programme andthis limits the possibility of stronger and more effective col-laboration. The need to fight simultaneously against limita-tions to family planning and sex education worsens the situa-tion significantly and overburdens the few groups involved.
In 1992 a coalition of the League of Polish Women, PolishFeminist Association, Young WomenChristian Association,Neutrum Association and Pro Femina Association founded theFederation for Women and Family Planning. The Federation’saim was to secure a liberal abortion law and to promote mod-ern contraception and sex education. Today the Federationbrings together nine groups. Among the almost 200 women’sgroups in the country, however, there are virtually no othergroups for whom abortion is a priority. Several other groupsare openly pro-choice, but very few are actively involved inabortion campaigns. The majority of the women’s groupschoose not to take a position on abortion.
Political partiesIn the nineties the political scene in Poland went through aprocess of transformation and crystallising. Although manypolitical parties emerged and played more or less significantroles over the years, the strongest groupings which finally re-mained are: the left (the Democratic Left Alliance (SLD) andLabor Union); the centre (the Freedom Union (UW)); and theright (Solidarity Election Action). It is important to recognisethe role of each of these in the abortion debate.
The rightFor the right-wing, the abortion issue was always a top priorityon their political agenda. The most fanatical leaders wouldalways speak publicly on the issue even if it meant risking theirpolitical position. The right-wing works closely with the Church
Poland
237
hierarchy and uses religious and demographic arguments suchas the sanctity of life or the low and constantly decreasing birthrate in their campaigns. They have been successful in recentyears in occupying strategic decision-making positions andhave introduced significant changes in Polish law and policythat will be hard to reverse.
The leftThe left is in principle pro-choice and takes up the issue of abor-tion when it sees the need. However, with the exception of thenot very strong internal women’s lobby, which is very active onthis issue, abortion is certainly not a priority for the core party.Some political commentators say that the left parties treat abor-tion instrumentally - that they raise abortion mainly in electoralcampaigns in order to gain support without true commitmentto fulfill their promises after elections. Besides, the SLD, whichis a transformed former communist party and was criticised bythe right for their past anti-church policy, might fear worseningits relations with the Roman Catholic Church.
The small Labor Union (the new left) was very active in abor-tion debates. However, it has never been strong and, afterhaving failed in the parliamentary elections of 1997, has lostits political significance.
The centreThe political centre has not adopted a common party positionon the issue of abortion because their members vary in ex-tremes from pro-choice to anti-choice. As a result, some pro-choice party members such as Barbara Labuda (who has nowleft the party), Zofia Kuratowska, speaker of Senate and MarekBalicki, MP, played a key role in abortion debates at somemoments of history. Although the UW as a whole was trying tomaintain neutrality on the subject, paradoxically the few ac-tive individuals of the party played a much stronger role inopposing and delaying the ban of abortion than members ofthe programmatically pro-choice left.
The Johannesburg Initiative
Advocating for abortion access
238
PhysiciansSince the early nineties the medical community, particularlyphysicians, has been influenced strongly by the Roman CatholicChurch. There are over 90,000 physicians in Poland, of whom55% are women (Kulik, 2000). Significant numbers, with novisible gender differences, became involved in anti-abortionpolicy and campaigns even before abortion was restricted bythe state law. In 1991, during the Extraordinary National As-sembly of Physicians, the Medical Code of Ethics was adoptedin spite of the strong opposition. The Code adopted a firmanti-abortion position, according to which only abortion tosave a woman’s life or health and on criminal grounds wasethically acceptable. The Ethical Code motivated public hos-pitals to stop performing abortions even before parliamentchanged the law in 1993.
Very few doctors would dare to speak openly in favour of moreliberal abortion regulations. None of them would confess pub-licly to performing abortions. However, many gynaecologistsperform abortions illegally for huge amounts of money.
The dominant idea that abortion is immoral has been pro-moted by the Association of the Polish Catholic Physicians,established in 1994. The association was instrumental in manyinitiatives towards restricting access to legal abortion. Two ofits leaders, Kazimierz Kapera and Maria Smereczynska, be-came MPs. They both subsequently held the key ministerialposition of Government Plenipotentiary for Family Affairs.
According to the Polish law adopted in the nineties, physi-cians can refuse to perform an abortion on the grounds ofconscientious objection. However, they must refer the womanto another service provider where she can access the termina-tion to which she is entitled. The conscience clause does notapply in life-threatening situations. Some Polish physicians usethe conscience clause to refuse to prescribe contraception. Inpractice, the clause constitutes a significant barrier to access tolegal abortion.
Poland
239
Numerous healthcare providers have been obstructing accessto legal abortion. When abortion on social grounds was re-legalised in 1997, many public hospitals issued statements thatthey would not provide abortion on these grounds. One byone, hospitals, cities or regions issued statements against abor-tion. The General Chamber of Physicians also stated theiropposition to abortion and the local chambers of physicianssupported it.
According to a Ministry of Health report presented to Parlia-ment on 20 February 1997, 209 obstetric/gynaecological hos-pitals out of the entire number of 435 hospitals in Poland didnot then perform abortions on social grounds. On the otherhand, in many places where abortion was not available inpublic hospitals, it was widely provided in private clinics bythe same providers who treat abortions as an important sourceof additional income.
Abortions were opposed not only by directors of hospitals orindividual gynaecologists, but also by anaesthesiologists ormiddle-level medical personnel such as midwives and nurses.Some doctors who were willing to perform abortions couldnot do so because they had no team to assist them. In somecases gynaecologists had to be ‘imported’ to a particular hos-pital. In one hospital all the anaesthesiologists refused to per-form an abortion for a woman with heart problems and socialcomplications – she already had eight children. The directorof the hospital dismissed the head of its anaesthesiology de-partment and an anaesthesiologist from another city wasbrought in to assist the operation. However, the dismissal ledto protests and criticism from the medical community.
Attitudes of the societyAccording to a Cenrum Badania Opinii Spolecznej (Centrefor Research on Public Opinion – CRPO) survey of November1996, 58% of those polled were in favour of the liberalisedabortion law. Only one third of the respondents were opposedto it. According to an Osrodek Badania Opinii Publicznej (Pub-lic Opinion Research Centre) opinion poll of the same month,
The Johannesburg Initiative
Advocating for abortion access
240
48% of respondents supported abortion on social grounds,compared to 65% in 1993, and 39% were against. Accordingto a survey conducted by the CRPO in 1998, 59% supportedabortion on social grounds, while 28% were against. Althoughthe results of opinion polls vary significantly, it is clear that themajority of the society, despite its Catholicism, did not supportthe ban on abortion, the direct involvement of the Church inthe activities against reproductive rights and, particularly, therole of Pope John Paul II, impeded the establishment of astronger, better organised and more effective pro-choice move-ment.
During the economic transformation and with high levels ofunemployment (higher among women than men), the vastmajority of the society has had to focus on making a living.The abortion issue has not been seen as a priority. The timecomponent also plays a significant role. In the early ninetiesmany people were afraid that they would be deprived of theright they had enjoyed for almost forty years and which theyhad expected to continue. After several years of the legal re-strictions to abortion, people became accustomed to the newlaw and learnt to live with it. New generations are growing upfor which the new law has become the norm, especially sincethe Church’s teachings in schools has made some impact onyoung people.
Strategies used by pro-choiceand anti-choice activistsReaching ordinary citizensThe Study on General Public Attitudes towards Abortion De-bates (Duch & Zielinska, 2000) illuminated some of the differ-ences between sub-groups of the population on the issue, aswell as what might be effective strategies to reach ordinarycitizens. Two groups of women (aged 18-25 and 30-45) andone group of men (aged 30-45) participated in the study. Al-though the majority of participants supported legal abortion,there were significant differences between the groups. Youngerwomen were neither interested in this issue, nor emotionally
Poland
241
involved. Among the group of older women, only one of ninewas against abortion. Most women were emotionally pro-choice, and their views were well-reasoned and consistent.Men, although mostly pro-choice, neither knew much aboutthe law nor expressed much interest, with the exception of twoof the eight men who were emotionally involved in anti-choiceactivities and were aware of the legal status of abortion.
The participants expressed their opinions about the main publicactors in the abortion debate. For all groups the campaignsagainst legal abortion were more visible than pro-choice cam-paigns. All the groups pointed out the Roman Catholic Churchas the main anti-choice actor. The study participants had no-ticed the anti-choice actions of the Solidarity Trade Union,Christian National Party, President Lech Walesa and RadioMaryja. The participants could name only the SLD among thepro-choice actors. They mentioned feminists but did not iden-tify any pro-choice women’s groups or individuals.
The most visible forms of campaigns were demonstrations.However, those of anti-choice groups were more visible. Thoseinterviewed mentioned demonstrations in front of the clinicsperforming abortions in particular and the presentation of ‘TheSilent Scream’ in schools. None of the interviewed groupsseems to be interested in undertaking actions to change theanti-abortion law. However, older women said they wouldsupport pro-choice initiatives, for example by signing a peti-tion or voting in a referendum. They would not participate ina demonstration. No participant believes that he or she wouldmake real impact.
The study shows that pro-choice campaigns could adopt arights-based approach aimed at women. Older women areparticularly sensitive to the issue And their pro-choice attitudeis deeply grounded in their responsibility for the future of theirchildren. Therefore, they believe a woman should have theright to make decisions. Men could be sensitive to argumentsbased on the right of a family for privacy and decision-mak-ing, but the issue of abortion is a marginal one for them incomparison with such issues as finances and industry.

The Johannesburg Initiative
Advocating for abortion access
242
Limiting access to prenatal testsLimiting access to prenatal examinations such as amniocente-sis could be seen as an important strategy to limit access tolegal abortion on genetic grounds. In the early nineties thetests were withdrawn as routine examinations for pregnantwomen over 35 years of age, despite the contradiction of sucha solution with international standards. In 1999 the possibilityof obtaining such examinations became even more limited.Despite strong opposition, the anti-choice lobby managed tointroduce regulations that impose penalties for ‘damaging thebody of a foetus or causing damage to health, threatening itslife’. The criminal penalty is currently up to two years’ impris-onment.
Some genetics institutes complain that their contracts withmedical insurance agencies do not secure full coverage of ex-amination costs. This can lead to further limitation of access.In 1999 the number of such examinations reached 2,204, upfrom 1,648 in 1998 and 1,612 in 1997. Some of the increasein 1999 can be attributed to the public debate in the media,thanks to which many women learnt about and demandedthem. The increasing trend may well not continue.
Given the limitations, it is not surprising that there are only 40-50 cases of abortion on the basis of damage to the foetus re-corded each year. In 1999, 309 cases of pathological develop-ment of the foetus were recorded, but only fifty abortions con-ducted on this basis.
Limiting access to family planning and sexeducationThe anti-choice movement struggles against modern contra-ception and sex education with equal devotion. The currentgovernment withdrew state subsidies for hormonal contracep-tion, which limits financial accessibility of family planning. Thegovernment also withdrew sex education from school curriculaand replaced it with ‘pro-family’ education which containsmisinformation concerning gender, sexuality and reproduc-tion-related issues.

Poland
243
There is no official record of contraception prevalence in Po-land. Surveys suggest that the use of modern contraception isstill relatively rare and that a large part of the society uses al-ternative methods such as the rhythm or calendar-basedmethod, or withdrawal before ejaculation. Research byZbigniew Izdebski (1997) showed that 55% of respondents ei-ther did not use any method or used the above-mentioned,ineffective methods of prevention. Condoms were used mostoften, by almost 21% of the respondents, while the hormonalpill was used by only 8% and the diaphragm by almost 5%.Sterilisation as a method of family planning is forbidden inPoland.
MediaIn the early nineties print media and radio stations were rela-tively supportive of the pro-choice position and would informthe public about abortion debates. At that stage the mediaraised the issue of abortion in the context of women’s dignity,women’s rights, the right to a free decision and women’s healthand life. They would quite often describe the cases of womenaffected by the anti-abortion law.
Over the years the situation has changed. Abortion-related is-sues are now addressed in a one-sided and biased way. Somemedia, particularly public TV, tend to ignore the abortion is-sue. Others present the pro-choice position only in relation tothe anti-choice position. They focus on ‘degenerate mothers’who abort, abandon or kill their children without any reflec-tion about the root causes of such tragedies. They present thestories of women who experience so-called post-abortion syn-drome as a result of abortion.
The media shift was evoked by the multiple strategies target-ing the media carried out by anti-choice groups and the Ro-man Catholic Church. The anti-choice lobbyists targeted bothmedia owners and individual journalists, questioning their cred-ibility and professional competence and threatening them withcourt cases. Individual anti-choice activists would visit jour-nalists to present their position and offer model foetuses, tapesor videos with foetal heartbeats and similar gimmicks. During
The Johannesburg Initiative
Advocating for abortion access
244
one of his visits, the pope advanced particular criticism of hismotherland’s public media as being allegedly anti-church.These actions made journalists cautious in tackling the topic.
On the other hand, pro-choice groups put particular empha-sis on communications with the media and succeed in pro-moting a number of supportive articles and radio programmes.However, the Federation had very little success with publicTV. A few years ago, after the multiple screenings of ‘The Si-lent Scream’, which evoked official protest from pro-choicegroups, the Federation made an unsuccessful attempt to presentDorothy Fadiman’s documentary, ‘When abortion was illegal’.Public TV first agreed but changed its decision at the last minuteafter publicising the presentation.
In the nineties the Roman Catholic Church established a net-work of Catholic media that includes over 100 magazines andnewspapers and 30 radio and TV stations, which promoteextreme anti-choice positions. The most effective and influen-tial is Radio Maryja, which has been the main organiser ofmass anti-abortion actions such as marches, demonstrations,letters of support or protest and petitions.
Infiltrating key institutionsFrom the very beginning the anti-choice groups successfullyinfiltrated key institutions and ensured the appointment of the‘right’ people within the institutions. They managed to occupyministerial positions in the key ideological ministries such asthe Ministry of Health, the Ministry of Education and the Gov-ernment Office for Family (and Women’s) Affairs in the nine-ties. The conservatives ensured that policies and programmesrelated to abortion, family planning and sex education reflectedthe anti-choice approach. During recent parliamentary elec-tions a number of anti-choice activists ran for parliament withthe support of Radio Maryja and other Catholic media andwon. Some of them occupied parliamentary, ministerial andgovernmental positions and pushed forward legislation, poli-cies and programmes for 1997-2000 that are detrimental towomen.
Poland
245
In 2000 the right-wing decision-makers were also successful inincreasing their majority in the fifteen-member ConstitutionalTribunal. They managed to appoint the Ombudsman for Hu-man Rights and the Ombudsman for Children’s Rights. Theseappointments may diminish the legal chances to challenge theanti-abortion law and other gender-insensitive policies andpractices.
New entitiesAnother important strategy used by the anti-choice lobby is tofound Catholic associations of key professional groups. Themost visible are the Association of Polish Catholic Physiciansmentioned above, the Association of Catholic Lawyers andthe Association of Catholic Pharmacists of Poland. The asso-ciations of physicians and lawyers were successful in gettingtheir members into parliament and government. In the earlynineties the Association of Pharmacists was reported to be re-fusing to sell contraceptives.
Several Catholic research institutions have been established,while the old ones have intensified their efforts to provide ‘sci-entific’ arguments for fundamentalist policies. In recent years,the network of teachers of natural family planning has beenestablished, the only one subsidised by the State. The trainingfor educators on sexuality-related issues has been monopo-lised by institutions with biased curricula. These institutionsare the only ones authorised to issue certificates necessary toteach at schools.
Multiple forms of pressureThe Roman Catholic clergy and anti-choice groups have uti-lised diverse forms of pressure on legislators, institutions andindividuals involved in the process of implementation of theanti-abortion act as well as professionals dealing with abor-tion, contraception and sex education, in particular, healthpersonnel and school teachers. Liberal members of Parliamentas well as other groups say they are exposed to multiple formsof pressure, some of them very nasty, such as naming fromchurch pulpits, threatening phone calls or letters or even thepainting of houses and cars red. The tactics are intended to
The Johannesburg Initiative
Advocating for abortion access
246
achieve the desired attitudes, such as ‘correct’ voting or re-fusal to perform abortions, prescribe contraception or providesex education. Many victims of such pressure have withdrawnfrom their former pro-choice positions and activities. Oneprominent member of the Committee for Referendum who,when he became the Minister of Health of the left Govern-ment, did not support the liberalisation of abortion law, is oneof the most striking examples.
Law enforcement institutions are another important target.They experience pressure to investigate the abortion under-ground. The Federation attributes the more pro-active policyin following up on these cases to this pressure.
Specific pro-choice strategiesAn important strategy for pro-choice groups is documentingand publicising the effects of the anti-abortion law. Nationalreports were published in 1994, 1996 and 2000 and have beenwidely used in parliamentary debates by the Federation forWomen and Family Planning. The Federation also submittedtwo reports to the United Nations Committee on Economic,Social and Cultural Rights (1998) and the Human Rights Com-mittee (1999). Both committees expressed their concern aboutthe effects of the anti-abortion law in Poland and recommendedthat the Polish government change its policies. These recom-mendations have been used extensively in lobbying and ad-vocacy activities.
Nationally, the Federation has attempted to use the PolishOmbudsman for Human Rights. In 1997 the Federation putforward a complaint concerning the withdrawal of state subsi-dies for hormonal contraceptives. Although the Ombudsmanagreed that the withdrawal constituted gender-based discrimi-nation, the Ministry of Health did not change its decision. In2000 the Federation failed in two complaints considered bythe new right-wing Ombudsman. One concerned police inter-vention in a private gynaecological clinic performing illegalabortion and the second concerned school textbooks present-ing sexuality-related issues in a biased and unscientific way.

Poland
247
One legal opportunity was missed by pro-choice groups. Whenthe restrictive law was introduced for the first time, the Federa-tion should have taken it to the Constitutional Tribunal on thebasis that women were being deprived of rights they alreadyhad. According to Polish law, no-one can be deprived of exist-ing rights. Unfortunately, this idea came too late. However,taking into account the composition of the Tribunal, it is doubt-ful the Federation would have won.
The language of anti-abortion campaignsLanguage has played a significant role in the debates on abor-tion in the nineties. Abortion has often been compared withconcentration camps, the holocaust, ‘death of civilisation’, ‘be-trayal of the Polish nation’ or simply murder. The world hasbeen divided between those who defend life and those whoare against life. Women’s right to choose or women’s repro-ductive rights are low in the anti-choice hierarchy of values,much lower than protection of the life of the unborn or con-ceived child. Liberal abortion law was presented as a remnantfrom the communist system that should be removed.
The anti-abortion law has introduced new concepts into Polishofficial language, such as the concept of a conceived child.The Polish Criminal and Civil Codes replaced the idea of afoetus with that of a conceived child. Now, even the medicalcommunity is using this term, in spite of its ideological, non-medical character. Another new expression created in the anti-abortion law and, consequently, in legal codes and other rel-evant documents, is ‘mother of a conceived child’, which meansa pregnant woman.
ConclusionIt seems probable that actions on the abortion issue will fluctu-ate in coming years and that their fate will depend largely onthe general political situation. Recent history shows that ‘right’and ‘left’ parliaments are being elected alternately, leading toalternately restrictive and liberal abortion regulations. Pro-choice forces have not yet been able to build a strong pro-
The Johannesburg Initiative
Advocating for abortion access
248
choice movement that can defend a woman’s right to elect tohave an abortion and make that right effective, independentof political circumstances.
ResearchersAleksandra Solik and Monika Tajak
InterviewerMagdalena Grabowska
IntervieweesJolanta Banach (MP, former Government Plenipotentiary forFamily and Women’s Affairs), Jerzy Borowicz, MD, MalgorzataKsiezopolska (Pro Femina Association), Izabela JarugaNowacka (League of Polish Women, Labour Union),Malgorzata Tarasiewicz (former head of Women’s Section ofSolidarity), Danuta Waniek (Democratic Union of Women, MP)
ReferencesDuch D & Zielinska A (2000) Study on General Public Atti-tudes towards Abortion Debates, Research and Unity Network,Warsaw.
Izdebski Z (1997) Pro health and sexual behaviors in an as-pect of HIV/AIDS in Poland, Warsaw: Ministry of Health andUnited Nations Development Programme.
Kulik H (2000) ‘Family or Professional Carrier of Female Doc-tor’ in Medical Journal (Gazeta Lekarska), 10.
AuthorWanda Nowicka has been specialising in the field of reproduc-tive health and rights for several years. Since 1990, she has beenactive in a nascent NGO movement in Poland and is a co-founder and member of several NGOs including the Associa-tion for Ideologically-Free State Neutrum and the Federation

Poland
249
for Women and Family Planning. She has run the Federationsince its creation, first as President and now as Executive Direc-tor. She was a member of the Gender Advisory Panel of WHO’sDevelopment and Research Training in Human ReproductionProgramme (1996-2001). She has published several articles andreports related to reproductive health and rights.

The Johannesburg Initiative
Advocating for abortion access
250
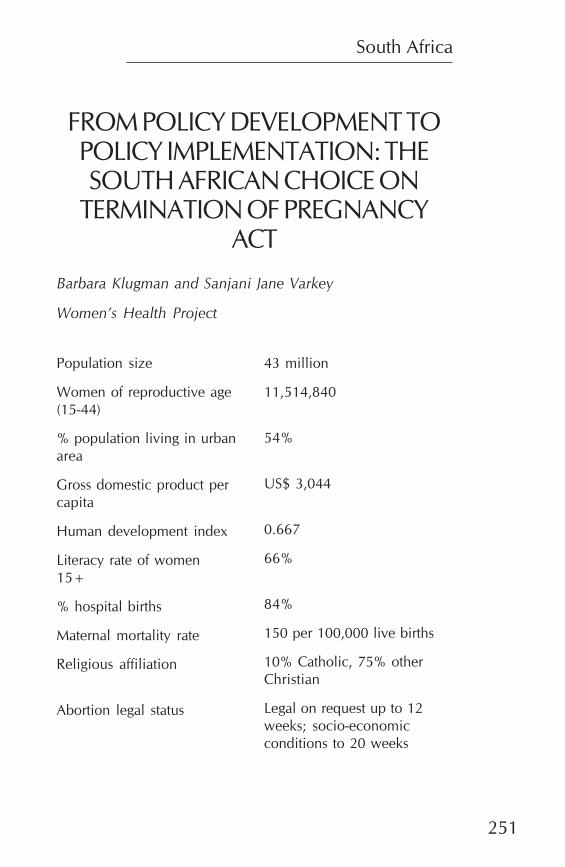
South Africa
251
FROM POLICY DEVELOPMENT TOPOLICY IMPLEMENTATION: THESOUTH AFRICAN CHOICE ON
TERMINATION OF PREGNANCYACT
Barbara Klugman and Sanjani Jane Varkey
Women’s Health Project
Population size
Women of reproductive age(15-44)
% population living in urbanarea
Gross domestic product percapita
Human development index
Literacy rate of women15+
% hospital births
Maternal mortality rate
Religious affiliation
Abortion legal status
43 million
11,514,840
54%
US$ 3,044
0.667
66%
84%
150 per 100,000 live births
10% Catholic, 75% otherChristian
Legal on request up to 12weeks; socio-economicconditions to 20 weeks
The Johannesburg Initiative
Advocating for abortion access
252
IntroductionIn the years between the start of negotiations to end apartheidand the actual elections on 27 April 1994, national mobilisa-tion of civil society shifted from the generalised goal of over-throwing apartheid, to more focused processes of debatingwhat principles and policies would shape a ‘new’ South Af-rica. Within this process, women’s rights and health were putonto the agenda. A civil society process of national network-ing took place to develop thirteen women’s health policy pro-posals, one of which concerned liberalising abortion law. Theprocess culminated in a Women’s Health Conference that ta-bled these as part of the goals for the democratisation agenda.In parallel, the African National Congress (ANC), not yet apolitical party but rather a mass movement waiting to elect itsleadership into power, set up a policy development processacross all sectors. In the health sector, abortion was put on theagenda.
The existing Abortion and Sterilisation Act of 1975 allowedfor abortion in limited circumstances, requiring, at the least,the approval of independent physicians who then could notperform the procedure. In practice this meant that only a fewthousand legal abortions were performed each year, whileestimates of illegal abortions stretched to 250 000 per year.Immediately after the elections, parliament constituted an Ad-hoc Select Committee on Abortion and Sterilisation, with pro-portional party representation, to review the existing legisla-tion and hear submissions. In 1995 and 1996, the Committeeorganised public hearings. The 1995 hearings were to assesswhether to develop a new law. The 1996 hearings were todebate a draft law. The process culminated in the passing ofthe Choice on Termination of Pregnancy Act, which was
South Africa
253
gazetted on the first of February 1997. This Act provides forabortion on request up to twelve weeks, and under a broadset of circumstances, in consultation with a health worker, upto twenty weeks. Minors (below eighteen years) do not requireparental consent. Trained midwives can do abortions.
Since the Act became law, there have been two constitutionalchallenges. In 1998 a constitutional challenge to the wholelaw was issued by three Christian groups, but failed. A subse-quent challenge was issued by the Christian Lawyers Associa-tion to contest the constitutionality of minors’ rights. This sec-ond challenge is underway at the time of writing this article.
This paper explores how the law was won, the factors whichhave facilitated or constrained implementation and, withinthese, the role of NGOs as policy and implementation activ-ists. The paper draws on documentation, analyses of the proc-ess, personal experience of the authors as participants in thisprocess, as well as interviews with key informants who havebeen involved in the policy and implementation processes. Asample of eighteen interviewees was identified to representthe different components of abortion – training, research, moni-toring, advocacy, media and legal. The paper is divided intotwo parts. The first considers the process of legislative changeand the second the implementation process. The concludingsection discusses linkages between the two processes, as wellas lessons learnt and challenges for the future.
The legislative processThree issues were central in making possible the achievementof a liberalised abortion law. They are the political and ideo-logical climate in which abortion reform was put onto the policyagenda; the interaction of civil society with the political proc-ess in the shaping of new legislation; and the influence of bothof these dynamics on the content of the new law, in particularits approach to equality and to questions of culture and reli-gion.
The Johannesburg Initiative
Advocating for abortion access
254
The political and ideological climateThe struggle to end apartheid used a human rights discoursewhich, through the negotiation process, was enshrined in abill of rights within the new constitution. It was, however, notonly the content of law that changed, but also the process.Law had been the preserve of the white electorate and, in realterms, of the white Afrikaner men who sat in Parliament. Theydid not seek the perspectives of the public. When the ANCgained power after the 1994 elections it did so on the back ofa form of participatory democracy that had been shaped bythe internal anti-apartheid movement. Its leadership, whetherin parliament or government, had no personal experience oftheir new roles. This inexperience created an opportunity forthem to shape their method of policy-making from scratch.Ministers and parliamentary committees established processesfor participation of anti-apartheid activists as well as the pub-lic at large in legal and policy change. In the case of abortion,a series of opportunities for public input were established, thusopening the way for civil society to engage in the law makingprocess.
While the ideological focus of the time was on human rights,issues of women’s rights and particularly women’s reproduc-tive rights had not been taken into the mainstream of the anti-apartheid movement prior to the 1990s. During the 1980s,the overall discourse of nationalism had made it difficult forwomen’s rights activists to get issues of reproductive rights ontothe agenda. At times young men, in particular, argued againstcontraception on the basis that women should bear ‘soldiers’for the struggle (Ritchken, 1988). Even within the black ‘estab-lishment’, this approach was evident. The National AfricanFederated Chambers of Commerce and Industry, for exam-ple, argued that blacks could not take up contraception untilSouth Africa’s political problems were solved (Keeton, 1985).
Anti-apartheid health activists were the only non-racial group-ings that put women’s right to control their own reproductionon the agenda. The Abortion Reform Action Group (ARAG),a long-standing organisation comprised predominantly of white
South Africa
255
women, had had the issue on the agenda for more than twentyyears without success. Gynaecologists, too, had supported lib-eralisation of the law for some years. A 1980 survey foundthat 82% of obstetricians and gynaecologists favoured a liber-alisation, with 32% favouring abortion on request (Domisse,1980 cited in Albertyn, 1999).
Thus despite the overall human rights discourse, women’s rightsand health activists had to develop specific strategies for giv-ing women’s experiences and reproductive needs a legitimatevoice in the transition process and in policy development inparticular. It was the political change that made it possible toget the problem of unsafe and illegal backstreet abortions onthe political agenda, as a matter of gender equality and wom-en’s rights as well as public health, despite reservations thatindividuals may have had. As one interviewee put it: ‘We hada window of opportunity with the political willingness and ac-ceptance of women’s rights.’
Civil society’s role in the shaping of newlegislationOrganisations of civil society began to prepare for policy changeand a range of mobilising interventions, such as developmentof a Women’s Charter, took place. In relation to women’s healththe most significant policy process was the mobilisation to-wards and holding of a Women’s Health Conference. This ef-fort involved a parallel process of networking with all inter-ested organisations in different regions of the country to iden-tify their concerns, while simultaneously small ‘expert’ groupsdrafted policy proposals. The proposals were then debated inthe regional networks and finalised at the conference.
The process was unique, both in taking advantage of the envi-ronment of mobilisation and helping to shape ideas about whatconsultation should mean. In the words of one participant inthe conference: ‘The conference was a breakthrough for SouthAfrican women’ (Cited in Klugman, 1997:14). The depth ofoutreach of this process, and the fact that it created opportuni-ties for women who had previously been completely
The Johannesburg Initiative
Advocating for abortion access
256
marginalised from policy processes and at the same time in-cluded people who were poised to enter senior positions ingovernment, gave it substantial legitimacy when it was usedfor advocacy once the formal legislative process began.
In parallel with this process the ANC was preparing its electionplatform. There was an overlap between actors here, as two ofthe regional representatives of the ANC’s Women’s HealthCommission were simultaneously involved in the Women’sHealth Conference process. Further, these two individuals ranorganisations – the Women’s Health Project (WHP) and theReproductive Health Research Unit (RHRU) – that played sig-nificant roles in the subsequent process of lobbying for andimplementation of a new law. Two other members of the Com-mission subsequently became the Minister of Health(Nkosazana Zuma) and the head of the Health Select Com-mittee (Manto Tshabalala Msimang) under the new govern-ment.
The group developed a range of proposals for the ANC’s HealthPlan. Significantly, the issue of abortion came onto their agendathrough grassroots membership. When Commission membersinvited representatives from all ANC branches in one regionto come to a meeting to discuss what needed to change inrelation to women’s health, some of these representatives putaccess to abortion on the table. The Commission in turn pre-sented this to the larger body of health activists collectivelyworking on the Health Plan. There was substantial argumentthere. Even within the Women’s Health Commission, somerepresentatives felt it might be easier to win commitment toliberalisation if it remained limited. Others, including the fu-ture first Minister of Health, argued that that the Women’sHealth Commission should take a strong position and try towin it, rather than admitting defeat without a battle.
Amongst health activists in general, the tension was expressedas one between their own recognition of backstreet abortionsas a public health problem and their simultaneous concernthat, if the ANC had liberalising abortion law on its agenda,this would undermine its position in the elections. However,
South Africa
257
strong arguments about both the health and rights dimensionsof the issue persuaded the meeting. It was ultimately includedin the ANC’s election platform on health in the statement that:‘Every woman must have the right to choose whether or notto have an early termination of pregnancy according to herown individual beliefs. Equally, health workers have the rightto refuse participation in termination of pregnancy, accordingto their beliefs (African National Congress, 1994:57).
This position, which committed the ANC to legal reform, wasthus a product of civil society, since at that point no electionshad taken place. It was not, however, uncontested within theANC. Ongoing advocacy was needed to keep it on the agendaand after the elections prodding from both within the newgovernment and by those outside helped to get the legislativeprocess going.
The public hearings held by the parliamentary committee onhealth, as well as those held in 2000 to monitor the implemen-tation of the Choice on Termination of Pregnancy Bill, main-tained the formal opportunities for civil society participation.But it was not only the formal policy process that created theseopportunities. Many of the players both inside and out of gov-ernment had worked together on the issue prior to the changeof government, and there were links of ‘comradeship’ whichgave people in civil society organisations easy access to thosein power. This is what Stevens describes as ‘soft boundaries’(Stevens, 2000). Moreover, the ANC had no institutionalisedresearch grouping or staff to support parliamentarians instrategising or establishing consultative processes. Thus theyturned to their erstwhile comrades. This gave those in the ‘pro-choice’ establishment much greater access than any othergroupings.
Human rights, health and development-oriented NGOs or-ganised themselves into the Reproductive Rights Alliance (RRA)and strategised diverse means of making an impact. Staff ofthese NGOs became legal advisers to parliament and later togovernment in developing regulations. Their staff advised onhow to find people to give evidence in the hearings and en-
The Johannesburg Initiative
Advocating for abortion access
258
sured that those who were poor could access parliamentaryfunds to come to speak at hearings. Many of those who gaveevidence had gained experience in talking on the issues throughthe Women’s Health Conference process. NGO staff under-took advocacy to health committees in both provincial legisla-tures and the national parliament. In characterising the link-ages between people in government and in pro-choice NGOsand research institutions, an NGO interviewee noted that ‘we’dall come from this partnership and had all developed what wewanted to achieve together, politically’.
Despite working within the RRA, different NGOs used differ-ent entry points for advocacy. Some used the human rightsdiscourse of the time, in an effort to turn around the moraldebates carried in the press. Others attempted to draw atten-tion to the public health dimensions. The most significant publichealth intervention was an initiative by a research NGO toinvolve medical schools in gaining national baseline data onmorbidity and mortality related to abortion – what a repre-sentative of the NGO described as ‘an objective epidemiologi-cal base to what we knew was going to be a political argu-ment’. The study was conducted under the auspices of the‘neutral’ Medical Research Council. The evidence from thisstudy made a major impact on politicians during the publichearings. Particularly important was its assertion that access tosafe and legal abortions would reduce costs to the health sys-tem given the existing costs of addressing complications frmunsafe abortion.
Other NGO interventions included dissemination of a pam-phlet targeting parliamentarians with information on the pub-lic health impact of unsafe abortions and the organisation of atour to Bangladesh. The latter allowed provincial departmentof health officials working in reproductive health to see howservices could be delivered at low cost and high quality throughthe ‘menstrual regulation’ programme. This built the confidenceof officials to give evidence at the hearings (Lund, 1997:8).
However, aside from the few women’s and reproductive healthinterest groups and one fledgling nurses’ organisation, Con-
South Africa
259
cerned Nurses of South Africa, progressive organisations ofhealth workers chose to put their attention elsewhere. Theyfocused, for example, on the need for overall health systemreform and more equitable financing systems to meet the needsof the majority.
Organisations of nurses, too, showed minimal interest in theabortion issue. The organisations were at that stage more con-cerned with internal transition issues as there had been sepa-rate organisations for whites and blacks and they were in theprocess of amalgamating. Possibly for these reasons, very littleattention was given to the health systems implications of theproposed new law. In addition, health service intervieweesindicated that they were aware of the legal process, but thatthere was no formal consultation with the health sector or thosewho would later have to implement.
Those who were against liberalisation of the law, and indeedagainst any legal access to abortion, were completely outsideof the process. They had no entry point except the formal hear-ings where they gave evidence. But the ideological environ-ment was against them. As one RRA organiser noted: ‘Whatimpressed us as unique to the South African experience wasthe fact that it was so many black women who … were nowsitting on the health committee and asking the questions, andattacking the wealthy white men [who gave evidence at thehearings] who were now feeling like they had no power’ (citedin Klugman 2000).
In parallel to the legal process, during 1995 and 1996 the in-terim constitution was finalised through a mixture of nation-wide calls for public input and the participation of politicalleadership and their expert advisers. In this process the ANCwas ambivalent. On the one hand, it recognised abortion asan important issue. On the other hand, it feared political divi-siveness were it to take a position. However, women’s rightsactivists were ‘within the system’ at this stage. Women consti-tuted more than 25% of elected members of parliament andthe ANC had publicly committed itself to abortion in its healthplan and to reproductive rights as one of the key gender issues
The Johannesburg Initiative
Advocating for abortion access
260
to be addressed in a post-apartheid constitution. Moreover,NGOs and research organisations had been preparing not onlyfor the legal process but also for the constitutional negotia-tions. For example, the Centre for Applied Legal Studies andthe RRA coordinator had undertaken background work andconsultations with international experts to support activistswithin the constitutional negotiations in arguing for reproduc-tive rights. The shared agenda and soft boundaries betweenthose inside and outside the negotiations facilitated daily sup-port, provision of arguments and evidence such that the finalconstitution includes clauses stating: ‘Everyone has the rightto bodily and psychological integrity, which includes the rightsto make decision concerning reproduction; to security in andcontrol over their body’ (clause 27(12)2a,b) and ‘Everyonehas the right to have access to health care services, includingreproductive health care’ (clause 27(1)a).
The influence of context and actors on thecontent of the new law
Race and gender equality and equityPro-choice NGOs focused their attention on what would mostinfluence politicians. The first argument thus related to endingthe inequalities institutionalised under apartheid. Under theprevious law, only a few thousand abortions were performedlegally each year and most of the women concerned werewhite. In addition, most white women, having greater accessto money, could either use personal contact with sympatheticgynaecologists, or pay the costs of going to Europe to securean abortion. Thus the RRA ensured that rural women whohad been criminalised for having abortions came to give evi-dence, thereby showing that it was black women who sufferedmost under the current laws. This argument was not abouteither women’s rights or public health, but about ending thediscrimination of apartheid.
In addition, women’s rights were a point of mobilisation and anumber of key points in the Act reflect the politicians’ andactivist NGOs’ commitment to achieve gender equality. Inparticular that the Act provides for abortion on request for the
South Africa
261
first trimester. This removes control from the medical profes-sion or judicial system, recognising women’s rights as individu-als to make decisions about their bodies themselves. Also thefact that the law does not include any requirement of spousalor parental consent reinforces the idea of women’s control overtheir own bodies.
The equity focus of the law is most clear in its efforts to ensurethat rural women will also be able to access abortions, by al-lowing midwives to undertake them in the first trimester. Howwas this content won? The debate began during the process ofthe Women’s Health Conference debates. At that time, ARAGhad developed a draft law as a means of giving content totheir demand for legal reform. The organisation had some-what of a medical and population control orientation. Theirdraft aimed to ensure women’s access to abortion, but wasconstrained by the assumption that this should remain thedomain of doctors. The Women’s Health Conference processbrought this lobby together with members of organisations withmore of a women’s and reproductive rights orientation. Thislatter group were less influenced by the medical profession’sattempt to keep women’s bodies under their control and moreconcerned about ensuring equity in access to abortions, par-ticularly for those reliant on public health services which, atprimary level, are run almost entirely by nurses. As a result thepolicy proposal emerging from this conference, while follow-ing the overall provisions of the ARAG draft, argued that mid-wives should also be able to perform abortions.
Questions of culture and religionThe fact that abortion was first addressed in ANC policy withinits Health Plan reflects the ANC’s recognition of abortion as acritical public health issue. In the language of its text, however,the tensions within both the ANC and society are apparent.The public discourse on rights is evident. The country hadbeaten apartheid and now everyone had a right to freedomand to choice. At the same time, health workers’ rights aregiven equal attention. This reflects the concern about electionsupport and recognition that the electorate would have moral
The Johannesburg Initiative
Advocating for abortion access
262
or cultural problems with abortion. No doubt these views werealso shared by some drafters of the Health Plan.
The concept of ‘rights’ as articulated during the anti-apartheidstruggle and within the new constitution was all encompass-ing. It included people’s right to religious freedom enshrinedalongside the right to freedom from discrimination. In a 1995national survey of 1 000 adult South Africans conducted forthe Constitutional Assembly, 34% were against abortion in allcircumstances 45% supported the existing law and 21% sup-ported women’s choice. (Everatt and Budlender, 1999). A studyof the perspectives of members of the nursing association in-dicated that 64% did not support abortion (The DemocraticNursing Organisation of South Africa, 2000:1). Since the par-liamentary hearings were public events, anyone could partici-pate. This raises the question of how it was possible to prom-ulgate the law in a country in which the majority of peopleappeared to be against liberalisation of abortion law.
There does not appear to have been a single agreed strategyon how to address the religious and cultural objections to thelaw. Collectively, however, the diverse strategies undertakenby difference players were very effective. On the one hand,some academics and legal activists interviewed argued that itwas strategically necessary to avoid engaging with health work-ers prior to winning the law, as ‘if it is broadly consulted thenwe could end up with reactionary bills, which hold up pro-gressive legislation’. Further, ‘widespread consultation withnurses or a referendum would result in a long drawn process,resulting in a very diluted Act, with limited powers for wom-en’s rights’. A number of interviewees also referred to the threatof ‘American money’ being used to mobilise anti-abortiongroupings. Thus the government and RRA believed that op-position forces would grow if the legal process were left for toolong.
At the same time there was a very pro-active strategy to builda network of pro-choice religious leaders to speak to the pressand counteract the voice of the religious anti-abortion lobby.The strategy aimed, at a minimum, to win over those who
South Africa
263
supported abortion as a choice in the case of rape. In additionto creating a public pro-choice religious voice, this approachincluded efforts to identify religious women who had had abor-tions and were prepared to testify in parliament as to why awoman might find herself opting for an abortion despite herreligious beliefs. This endeavour proved exceptionally effec-tive when a young catholic woman gave evidence that shehad become pregnant by her spiritual adviser and subsequentlyobtained an abortion that was paid for by the (catholic) church.
A similar approach was used in relation to arguments that abor-tion was against African culture. NGOs ensured that there wereblack men, in particular, who spoke for liberalising the law inan effort to undermine the argument that ‘African’ people didnot undertake abortion. This was further strengthened by pres-entation of research showing that abortions had been per-formed across culture and class in South Africa for hundredsof years (Bradford, 1991). Further, RRA members within themass democratic movement put substantial energy into get-ting the right to abortion onto the agendas and public plat-forms of organisations representing the majority, and particu-larly the Congress of South African Trade Unions, South Afri-can Communist Party and the ANC Women’s League. In con-trast to this behind-the-scenes approach, some NGOs mobi-lised public demonstrations to counter-balance those of anti-choice groupings described below.
In addition to these strategies, some pro-choice NGOs followedan active strategy to help counter negative media. This includedbuilding supportive relations with specific media representa-tives, particularly women, and training media to understandthe concept of and need for reproductive rights. One inter-viewee pointed out that the media’s interest in covering theabortion issue was strengthened by the fact that it was not onlyhealth activists raising the issue, but ‘women from all sectors’.‘When Winnie (Madikizela Mandela) says something thengrassroots women fight for it.’
While these strategies were effective, they need to be under-stood in the context of the absence of mass mobilisation of an
The Johannesburg Initiative
Advocating for abortion access
264
anti-abortion lobby. One potential anti-abortion constituencycould have been organisations of nurses. As indicated above,however, progressive health workers’ organisations were di-recting their attention elsewhere. The predominantly blackConcerned Nurses of South Africa (Conusa) was in the proc-ess of trying to amalgamate with the more conservative, white-led South African Nursing Association (SANA). While the lead-ership of Conusa aligned themselves with the values of thenew government, SANA leaders appeared to be anti-choice.Thus, despite Conusa’s evidence at the public hearings, it wasnot possible to mobilise nurses in support of a pro-choice po-sition.
While a number of the anti-choice organisations which gaveevidence at the public hearings were organisations of nursesor doctors, their spokespeople were white and they could notclaim to speak for the majority. Anti-choice health workers’organisations linked up with anti-choice religious groupings.At the time of the bill coming to parliament, over twenty anti-abortion groups united in demonstrations under the NationalAlliance for Life. While they gained a fair amount of presscoverage, they did not manage to mobilise the numbers re-quired to be taken seriously as a major constituency. The pub-lic voice for this alliance was a doctor. However, he was a whiteman, and this undermined his legitimacy. Also, a pro-choiceactivist brought to the attention of politicians that one of thepeople giving evidence for this grouping was linked to Hu-man Life International, which had been associated with right-wing political activities and arms dealing in the 1980s.
Clearly there were tensions within the ANC once the bill wasready to come to parliament on how to handle the balancebetween women’s rights and religious rights. There was a sub-stantial lobby from ANC members to allow individual voting.After major efforts by both ANC parliamentarians and NGOs,clauses which balanced health workers’ right to conscientiousobjection with the requirement that they refer clients were re-moved from the legislation in return for an agreement that allANC parliamentarians would vote as a bloc. The motivationwas once again that women’s suffering had to be kept on cen-
South Africa
265
tre stage. The fact that many of those supporting the law, suchas the Minister of Health, were themselves religious (in hercase, catholic) was significant. Thus in her speech to open thedebate on the bill, the Minister of Health said: ‘We deeply re-spect the pro-life view of our fellow Christians. Their argu-ments have some theological support and we sense a genuineconcern for the sacredness of life. Their theological explica-tion, however, is idealistic to the point where human sufferingis ignored’ (cited in Stevens, 1998:80).
How did these issues play out in the content of the law? Asnoted earlier, the ANC policy had explicitly noted the right ofhealth workers to choose not to do abortions. In the first draftsof the bill, the right to conscientious objection was retained.However, the balance of power both amongst lobbyists andwithin parliament was such that it was ultimately removed fromthe text. The final law says that health workers must informwomen about their rights in relation to the law. It does not,however, say that they have to refer clients, let alone that theyhave to perform the procedures. One interviewee was clear:‘The issue was conservatism. The political environment ofhuman rights should have been capitalised far more.’ The fail-ure to entrench the responsibility of health workers to imple-ment the law has led to a situation where despite the fact thatthis is a national law, people employed within the public healthservices do not have to refer clients and are not sanctionedwhen they do not comply. This has major implications for serv-ice provision, as discussed in the next section of the paper.
The implementation processWithin the first year of passing the Act, several actions under-taken by politicians, service implementers and activists dis-played their commitment towards the implementation of abor-tion services. As one interviewee observed: ‘If Zuma (the thenMinister of Health) decided she wanted something – she gotit.’ Some of the interventions aimed at moving from policy toimplementation were:
• The drafting of the official government regulation.

The Johannesburg Initiative
Advocating for abortion access
266
• The national group of university researchers establishedto manage the Medical Research Council slowly realignedto become the National Abortion Advisory Committee.The committee incorporated provincial governmentMother, Child and Women’s Health (MCWH) directo-rates as well as NGOs which had been involved in theprocess of legal advocacy and met fairly regularly tomonitor implementation.
• Designation of facilities to implement abortion servicesby the MCWH directorates in the provinces.
• MCWH in provinces running workshops with those re-sponsible for service provision in order to tell them aboutthe new law and promote its implementation
• ‘Values clarification workshops’ which aimed to assisthealth workers in relating their own personal value andbelief systems regarding abortion to the needs of theirclients.
• Publication of ‘Barometer’, a newsletter to monitor im-plementation, by the RRA.
• Establishment of legally designated clinics by MarieStopes.
• Research and health systems interventions looking at im-mediate issues such as women’s access to abortion andclinical protocols by diverse institutions (Varkey andFonn, 2000a and 2000b).
The next two years, in addition to continuing the processesinitiated in the first year, witnessed the introduction of theNational Abortion Care Programme, a training programmeintended to build doctors’ and nurses’ skills in manual vacuumaspiration, but also addressing broader requirements of clini-cians providing abortion. The training programme kicked offin April 1999 as the South African Nursing College approvedthe abortion curriculum only in October 1998. The curricu-lum, developed in partnership between the RHRU, the MCWH
South Africa
267
directorate and Ipas, an international NGO, was circulatedamongst different stakeholders for comments.
Through this national initiative inety-two midwives were trainedof whom twenty-two are trainers, eighty-one are fully qualifiedmidwives and sixty-nine are delivering the service (Dickson-Tetteh, 2000). Of the first ninety-two people trained, however,only sixty-nine are doing abortion procedures, with the remain-der either allocated to other services or having left the publicsector. All provincial MCWH directorates were allocatedR100,000 ($17,286) to train more midwives and to date thisfurther training has covered a total of 158 people (personalcommunication).
Three years after the Act came in, the RRA initiated parlia-mentary hearings to review the implementation of the Act. Thisprovided the first forum for discussions on a diverse range ofimplementation issues. In addition, it proved to be an impor-tant tool to keep politicians on board, especially in light of theconstitutional court challenges. It also provided substantial in-put to the bureaucracy responsible for overall policy on imple-mentation.
Results of such efforts were visible in the steady increase in thetotal number of legal abortions reported in public health facili-ties. Within three years of the reform, these reached a total of114,452 (Barometer, 2000). In the first six months of the pass-ing of the Act, there were more than double the number oflegal abortions reported in public health facilities compared tothe total number of abortions conducted legally during sevenyears (1984 to 1991) prior to the reform (Kustner, 1991). Asyet unpublished research indicates that there has been a de-cline in the incidence of incomplete abortions appearing athospitals, which suggests the success of the abortion imple-mentation process.
Although the Act has undoubtedly made abortion more avail-able, access for specific groups of women continues to be aproblem (Varkey and Fonn, 2000a and 2000b). Of the 246public health facilities designated to provide terminations, less
The Johannesburg Initiative
Advocating for abortion access
268
than a third (28%) provide the service. Of those facilities thatare operational, 99% are in centrally located hospitals (Ba-rometer, 1998) where 75% of first trimester procedures areconducted. This contradicts one of the key equity intentions ofthe Act, which was that first trimester abortions be conductedat primary health care level. In addition to these service barri-ers, studies show that only 53% of women are aware that abor-tions up to twelve weeks of pregnancy are legal (South AfricanDemographic Health Survey, 1998) with more teenagers,women without formal school education and rural womenbeing unaware of the service. A number of studies show thatproviders and community members do not support abortionon request and younger women’s right to choose (Varkey etal, 2000 and Engelbrecht et al, 1999).
This section of the paper focuses on key issues that appear tohave influenced South Africa’s experience in making abortionservices available so rapidly after the legal change, yet haveresulted in limited access for many women who require abor-tions. In particular, it considers how the structure of the healthsystem shaped implementation; how NGOs engaged with theimplementation process and the extent to which they wereable to play an activist role similar to that played during thelegal process; and the factors influencing community mobili-sation for service access.
Preparedness of the health system to implementat primary health care levelMany women approach doctors in the private sector who meettheir need for abortion. Because of the lack of appropriatetraining, quality of care issues do arise in this sector. However,this paper focuses on the public sector, given that the primaryproblem of access is for those who are poor or rural and hencedependent on the public health sector for services.
The new government inherited a public health system thatwas oriented towards tertiary level care, located in urban ar-eas. The health system was divided into separate institutionson the basis of race, geographical area and government au-
South Africa
269
thority and almost three-fifths of the total health care expendi-ture was in the private sector, which was used by less than aquarter of the population (Tollman and Rispel, 1995). At thetime of the passage of the law and up to the present, the healthsystem has been engaged in an ongoing process of funda-mental restructuring into three levels. The national level hasoverall-policy making responsibilities. The provincial leveladapts national policies into provincial policies and providestechnical support on specific programmes. The district level,which is currently being established by the provincial level,will ultimately be responsible for the integrated implementa-tion of services suitable to the needs of the communities withinits jurisdiction.
Local government boundaries were only finalised in mid-2000,at which point the process of fitting districts to local govern-ment boundaries began. Thus the scope of this restructuring isenormous and involves not only structures, but alsoreallocations of funds to promote equity and a need to reorienthealth workers from a rules-driven system into a responsive,rights-oriented service. Specific health policies such as the newabortion law had to be implemented in this context of ongo-ing changes in structures, lines of authority, and systems ofbudgeting.
The new structure has embedded within it an internal contra-diction in relation to such health policies, with those responsi-ble for policy and technical support on specific issues such asreproductive health having no authority over those, whetherat provincial or district levels, responsible for primary healthcare service delivery. Thus a tension has emerged, wherebythose in hospitals and primary level management resent thedeluge of new policies coming from national to provincial withvery little consultation. This resentment is frequently expressedin relation to funding shortages since all new policies have tobe delivered within existing or even contracting budgets.
The first step for implementation was designation of abortionservice facilities by the MCWH directorate. Its officials choseto designate hospitals so that by the end of the year 2000 legal
The Johannesburg Initiative
Advocating for abortion access
270
abortions in the public health service were available only inhospitals. Further, half of these are in the two most resourcedprovinces and only four primary health care level facilities havebeen designated (Barometer, 2000). Government interview-ees noted that by initially designating only hospitals, officialsfrom the MCWH directorate reinforced the focus on tertiarycare, thereby failing to ensure widespread services in keepingwith the intentions both of the national health system restruc-turing process and of the abortion law. In addition, the proc-ess followed for designation was in line with the top-downmanagement structure characteristic of the inherited healthsystem.
Interviewees also noted the problem of MCWH not havingconsulted with institutional managers or conducted a properanalysis of the designated facilities’ capabilities. As a result,many designated facilities did not offer services. Intervieweespointed out that this mistake is now being rectified, with MCWHofficials visiting sites rather than designating from their offices.
Designation was, however, only a starting point and an indi-cation of the problem of lines of authority for implementation.The MCWH directorates within national and provincial areonly responsible for policy making at their respective levelsand not actual implementation. Yet they had responsibility tosee the law implemented. Neither those within the provincesresponsible for district development nor the managers of dis-trict health services and institutional managers such as hospi-tal superintendents who make implementation happen weredirectly included in the process of deciding how implementa-tion would take place. They were also not involved in theNational Termination of Pregnancy Advisory Group that moni-tored implementation. As a result, they have not yet takenownership for implementation.
Given that managers of services are not directly accountableto the MCWH directorates, policy imperatives have been ig-nored. Interviewees described how doctors did not come tovalues clarification or training in MVA and the MCWH coulddo nothing about this. As one noted: ‘The previous hospitalsuperintendent did not want to start the service. When the
South Africa
271
boss does not want to do anything then nothing happens.’Likewise abortion providers in one province ranked the prob-lem of resistance from management as the greatest problem inabortion service delivery (Varkey and Robertson, 2000c).
That many managers and doctors do not want to provide serv-ices is clear from the provincial reports to the National Termi-nation of Pregnancy Advisory Group as well. Although theinitial requests for abortions were met by willing doctors, oneinterviewee confirmed that ‘active resistance’ by doctors un-dermined the ability of the services to meet the need. Anothernoted that, while the ‘value clarification workshops were veryhelpful…the doctors were left behind. They chose not to par-ticipate, as always’. This problem was not actively addressed.Interviewees suggested that part of the reason for this, is thatMCWH had no authority to address it. Had MCWH had au-thority, this would have facilitated abortion being included intothe service package and the performance criteria of facilitymanagers and doctors.
Further, interviewees noted that both the MCWH officials andmost NGOs and researchers on the Advisory Group had aclinical orientation. Thus while the problems were recognised,the solutions identified were skewed towards medical aspectsof abortion service. They failed to take into account and ad-dress other issues that are critical to abortion access. Thus eventhe initial chairperson of this group noted that ‘perhaps it wasmore successful at achieving the technical.’
The absence from the Advisory Group and the structural gapbetween those responsible for initiating and implementing thepolicy created an impasse. While the Advisory Group mademany recommendations, these were coming from outside thelines of authority that determine implementation priorities. Asa result, a number of issues that were critical to extending ac-cess could not be directly addressed. These included generichealth systems problems as identified by regional and clinicmanagers and NGOs working in strengthening health systems.For example, workshops with health workers point to the needto address problems such as improvement of supervision,management, communication, staff capacity, supply of drugs
The Johannesburg Initiative
Advocating for abortion access
272
and equipment and improvement of facilities, in order to im-prove the quality of abortion services (Varkey et al, 2000c).Another problem was difficulties faced by government in con-vincing training institutions to change curriculum. A third waslack of community outreach. These are considered in moredetail below.
While access to donor funding facilitated the implementationprocess, it also reinforced the lack of integration of abortionservices and the verticalisation of the process. Whether thiscould have been otherwise is arguable, since the overall re-structuring process perpetuated the divide between pro-grammes and implementation. Significantly, at the time ofwriting, one province – Gauteng – is attempting to do awaywith the separate ‘programme’ structures as a way of remov-ing this disjuncture.
While the impetus of donor funding and NGO initiative,partnered with MCWH, spearheaded the implementation proc-ess, the process is now facing the broader problems of institu-tionalisation which require a broader range of stakeholderparticipation. Training of health workers is one of the centralrequirements for institutionalisation, yet abortion has still notbeen integrated into the training programmes of nursing col-leges and medical schools, except into a post-graduate courseat one college in the country. Department of Health managersresponsible for liaising with colleges to ensure that training linksto policy developments indicated that they have been strug-gling to resolve a dilemma. On the one hand, they want toinclude abortion in the women’s health module. On the other,they respect nurses’ rights not to get involved in abortion. Tosome extent the problem of incorporation into the curriculumis simply one of the pace of the bureaucracy: ‘We wait to getthe policy passed. This is the institutionalised way of function-ing. We have a policy of (having) one budget year to imple-ment such expectations.’
Interviewees argued that many of the initial implementationprocesses were transitional: ‘There was an imperative to pushthis through quickly, even recognising the department of health
South Africa
273
hadn’t yet had an opportunity to completely transform itself orprepare itself.’ In this context, NGOs which had good donorcontacts were able to partner directly with government to pushfor implementation. Yet this intervention was not without prob-lems. One government interviewee argued that in this process‘because of the funds they have and the money is not seen asGovernment money, national (MCWH) has also abdicated theirrole over to the NGO’. Another felt: ‘The problem right now isthat instead of the Department driving the process of imple-mentation, it is the NGO. Staff attend national abortion co-ordination meetings, but their inputs are overturned. They lackempowerment and confidence at such meetings’.
However, both government and NGO interviewees recognisedthat, as government has strengthened, it is taking over respon-sibility. Government is attempting to understand the reasonsfor successes and failures, for example ‘instead of just knowinghow many designated institutions are functional or not, weneed to know the reasons why’. The effects of short term plan-ning are beginning to show, and the time is now ripe for as-sessment of the effectiveness of different interventions, as wellas of gaps where new interventions are required.
Research institutions and NGOs have been partnering withprovincial departments of health to deepen their understand-ing of the challenges of implementation. For example projectsin the Free State (Engelbrecht et al, 1999) and Northern Cape(Varkey et al, 2000d) look at community and health systembarriers. The Northern Cape initiative is developing a com-munity peer education intervention and a health system changemanagement tool. Other studies include one on the cost ofabortions according to level of care and qualification of pro-viders that is a useful tool for health service planning (de Pinhoand McIntyre, 1997); a study to assess the psychological ef-fects of first trimester abortion on women that begins the de-velopment of a screening tool for counselling (Faure, 1999);and descriptive research that looks at the profile of womenusing abortion services (Adanlawo, 1999 and Bennun, citedin Varkey & Fonn, 2000a). All of these will be helpful in iden-tifying which women are not accessing services and need to
The Johannesburg Initiative
Advocating for abortion access
274
be specifically targeted. The challenge will be how to incorpo-rate these findings into nationally institutionalised improve-ments in service access given the systemic and capacity prob-lems already discussed.
Community information and mobilisationOne of the notable gaps in delivery was communication withthe public about their new rights. Interviewees indicated thatthis was in fact a deliberate initial strategy and ‘that there wasa concerted effort not to prepare communities as people wereafraid of creating demands that would not be met by the sys-tem’. But three years later, besides the availability of pamphletsand a few NGO-run community workshops, government ef-forts have not yet been initiated. As a result, women do notknow their rights or how to access services.
While the government strategy of not building communityexpectations in the initial phases of implementation is under-standable, the question arises as to why, by 2000, NGOs andmass-based organisations had not begun to mobilise of theirown accord. The first reason appears to be demobilisation ofmass-based organisations as they reoriented themselves tofunctioning not as opposition, anti-apartheid groupings but asorganisations within a democracy. While they were able totake bursts of action to support the new law, they did not havethe capacity to undertake ongoing campaigns on the manyissues on which activity was needed. Moreover, abortion hasnot been a priority area for mass mobilisation, when com-pared with an issue like violence against women.
However, some NGOs had planned to deliver in this area butlargely failed to do so. Some individual NGOs took up specificactions outside of the auspices of the RRA. For example, thePlanned Parenthood Association of South Africa worked withKagiso TV to develop two videos – one for providers and onefor women – on their rights. The videos were translated anddistributed widely. Planned Parenthood also developed leaf-lets with RHRU and distributed these both through the depart-ment of health and their own networks. A recent review ofoutreach activities undertaken by the RRA indicates that there
South Africa
275
are further diverse localised processes of outreach such as acommunity training project – the Itireleng Educational Projectin the Northern Province – and the work by an individual so-cial worker at the Dora Nginza Hospital in the Eastern Cape,but no national co-ordination of these efforts (Braam, 2000).This begs the question of why, when the RRA was able to pulltogether diverse NGOs with diverse strategies in the legal re-form process, it has been unable to maintain this effort anddraw on the skills and capacity of its members in a mutuallyreinforcing way, despite having agreed to and raised the fundsto do so.
NGO interviewees noted that, after the victory, the RRA wasunable to maintain cohesion. Thus while some RRA membersdid specific pieces of work for the DoH after the passing of theAct, they did not engage with other RRA members about theprocess or content involved, so missing opportunities to gaininsights from a more diverse range of expertise. While someNGOs attended the National Abortion Advisory Committee,they did not do so as part of a concerted RRA lobby with ashared agenda for implementation and thus only the perspec-tives of those most closely aligned with the MCWH were heard.While member organisations took part in defending the con-stitutional court cases, their strategy was not conceptualisedwith other member organisations that worked on press mobi-lisation and other advocacy work outside of the formal courtcases so that strategies were not mutually reinforcing. PlannedParenthood developed the values clarification methodology.The National Progressive Primary Health Care Network, to-gether with an RRA staff member, developed materials forcommunity workshops and initially ran around twenty-oneworkshops in different parts of the country. Other memberNGOs had not participated in or had opportunity to inputinto the goals or content of these interventions and were notconfident of their appropriateness or quality. Thus this outreachwas not maintained and the networks RRA had raised fundsto establish as the base for community education were notestablished. Crucial committees such as the media committeeslowly collapsed.
The Johannesburg Initiative
Advocating for abortion access
276
Interviewees ascribed these problems to both managementproblems and the inability of the RRA to retain staff, as well asto confusion as to whether the RRA was an organisation or analliance. Activities which the RRA took upon itself, such asproduction of the monitoring journal ‘Barometer’ or facilitat-ing of the parliamentary hearings to monitor implementation,it did relatively well, except when it had no programme staff.The confusion around organisation or alliance arose specifi-cally in relation to funding. Thus one interviewee noted thatthe RRA ‘were one of the few organisations with dedicatedfunding to do the work. Certainly [my organisation] had nomoney for this and anything we did, including my time onmanagement committee which was often substantial, was fi-nanced through other projects…’ What is clear is that donorsare not overly enthusiastic about funding ‘abortion’ work andthis poses enormous challenges for organisations working inother areas of reproductive health and rights.’
Interviewees noted that since the RRA had funds, NGOs landedup competing with each other. ‘People looked at what theycould get out from the RRA rather than what they could giveto it’ rather than finding a coherent strategy for using thosefunds for member NGOs to deliver to agreed goals. In a con-text where few donors were willing to support abortion workon a national scale, NGOs with contacts made greater progressthan others in achieving their goals. The interviewees all spokeof the need for greater collaboration, but had contradictory viewsabout the extent to which this was possible. Above all, however,except for the RRA, all the other NGOs had other areas of inter-est in sexual and reproductive rights and health or even beyondthis. With the legal victory won, organisations incorporated edu-cation, advocacy or research on abortion but no longer gave itprimacy in the face of the threat of AIDS, the ongoing prob-lem of violence against women and other pressing concerns.
ConclusionThe impetus to change the abortion law was driven by thepolicy activism of diverse organisations of civil society. Theyused a range of strategies, from research to media mobilisa-

South Africa
277
tion to ensuring that the voices of both ordinary people (theconstituency of politicians) and religious people were heard insupport of women’s right to choose abortion to internal mobi-lisation within the ruling party. Their ability to mobilise fundsand to do a degree of collective strategising through the RRAallowed their interactions to be mutually reinforcing. However,the effectiveness of these diverse strategies was partly becauseof the political context, in which those in government had onlyrecently left civil society, their political party had no researchor strategic arm of its own and hence partnerships developedin the anti-apartheid and negotiations period were maintainedduring the legal process.
Implementation, in contrast, depended on a top-down ma-chinery that was slow and had its own internal structures forservice delivery. Whilst the new government worked hardwithin the MCWH directorate and made some headway, theydid not manage to address long term implementation issueswithin the first few years, given the disjunctures in account-ability for policy and for implementation within governmentand the restructuring it was going through. Again, NGOs playedkey roles, but these were no longer part of a coherent strategy.This was partly because implementation required very diverseinterventions. These needed, for example, to maintain the le-gal victory, to train health workers, to strengthen health sys-tem willingness and capacity, to build community support andknowledge and to maintain media support. Given that therewere few NGOs in the field from the start and the long-termnature of implementation challenges, it was easier for NGOsto go their own way than to have to put energy into maintain-ing the alliance, negotiating the division of donor funds andstrategising together.
Lessons learnt• Even in a conducive political and ideological context,
strategies needed to be developed to win the support ofdiverse stakeholders with diverse concerns and interests.
• Different messages work for different groups. Health man-agers and politicians concerned about resources were
The Johannesburg Initiative
Advocating for abortion access
278
more convinced by data showing that legal access wouldlower hospital costs from complications of unsafe abor-tion and address maternal mortality. Politicians con-cerned about addressing the needs of their constituencyresponded more favourably to personal stories or to themedia’s representation of public opinion
• There is value in both gaining a direct line to decisionmakers and helping them influence others from withinand working from the outside. Having both options, andkeeping very clear communication between the two,means that when there is pressure on the inside for com-promises, organisations working on the outside can takeup strategies to put pressure against such compromises.
• A liberal law does not determine increased service ac-cess. Concerted mobilisation should not end with thepassing of law.
• Mobilisation and unity for a short period with a verylimited goal and targeting a relatively focused group (poli-ticians) is much easier than long-term co-ordination andimpact on a very complex health system with multiplelevels of authority.
• Even when both government and NGOs are keen to seeimmediate results, actual institutionalisation requireslonger term, institutional planning and monitoring.
ReferencesAbortion Reform Action Group (1995) The Freedom of ChoiceAbortion Bill, Abortion Reform Action Group, Cape Town,February.
Adanlawo M (1999) Demography and social profile of womenrequesting termination of pregnancy in King Edward VIII hos-pital. Department of Obstetrics and Gynaecology, Universityof Natal, 1-19.
African National Congress (1994) A National Health Plan forSouth Africa. African National Congress. Johannesburg.
South Africa
279
Albertyn A, Goldblatt B, Hassim S, Mbatha L and Meintjes S(1999) Engendering the Political Agenda: A South African casestudy, United Nations International Institute for Research andTraining for the Advancement of Women. Dominican Repub-lic.
Barometer (1998) 2(2) Reproductive Rights AllianceJohannesburg.
Barometer (2000) 6 Reproductive Rights AllianceJohannesburg.
Braam T (2000) Overview of community IEC provision overfirst three years of implementation, Reproductive Rights Alli-ance. Johannesburg.
Democratic Nursing Organisation of South Africa (2000) Sub-mission presented at the Parliamentary Health Portfolio Com-mittee. Cape Town.
Dickson-Tetteh K (2000) Submission presented at the Parlia-mentary Health Portfolio Committee. Cape Town.
Engelbrecht M, Pelser A, Ngwenya C et al, (1999) ‘A ProjectManagement Strategy to Overcome Impediments to the Op-eration of the Choice on Termination of Pregnancy Act of 1996in the Free State: Findings from the Survey’, Centre for HealthSystems Research and Development, University of the OrangeFree State.
Everatt D and Budlender D (1999) ‘How many for and howmany against: private and public opinion on abortion’ inAgenda, 40, 101-5.
de Pinho H and McIntyre D (1997) ‘Cost analysis of abortionsperformed in the public health sector’ Department of Com-munity Health, University of Cape Town. Cape Town.
Faure SC (1999) ‘Anxiety, depression and self-efficacy in womenundergoing first trimester abortion’ Department of Psychology,University of Stellenbosch. Stellenbosch.
The Johannesburg Initiative
Advocating for abortion access
280
Guttmacher S, Kapadia F, Naude J, and de Pinho H (1998)‘Abortion reform in South Africa: a case study of the 1996Choice on Termination of Pregnancy Act’, International Fam-ily Planning Perspectives, 24(4), 191–194.
Keeton G R (1985) The Human Option Conferences. Devel-opment Southern Africa, 2:297-303.
Klugman B (1997) ‘Mobilizing and networking: what works,what doesn’t and why,’ Seminar on female empowerment anddemographic processes: moving beyond Cairo, IUSSP Com-mittee and Gender and Population and PROP, Programme onPopulation and Development, Department of Sociology, LundUniversity, Lund, Sweden, April 21-24.
Klugman B (2000) ‘Empowering women through the policyprocess: the making of health policy in South Africa’ in H Presserand G Sen (eds), Women’s Empowerment and DemographicProcesses: Moving Beyond Cairo, Oxford University Press.Oxford, 95-118.
Kola S, Budlender D, Kimmie Z and Kushlick A (1999) ‘A Gen-der Survey’ Conducted for the Commission on Gender Equal-ity. Johannesburg.
Kustner HGV (ed) (1991) ‘Epidemiological Comments’ 18(10).Department of National Health and Population Development.Pretoria.
Lund F (1997) Mid Term Review of the Reproductive HealthTransformation Project for Women’s Health Project. Johan-nesburg.
Republic of South Africa (1996) The Constitution of the Re-public of South Africa, Act No 108.
Ritchken E (1998) ‘Comrades, witches and the state’, HonoursDissertation, Department of Political Studies, University of theWitwatersrand. Johannesburg.
South African Demographic and Health Survey (1998) De-partment of Health, Medical Research Council and MACR.Preliminary report. South Africa.
South Africa
281
Stevens M (1998) ‘Factors impacting on the development of apregnancy termination bill’, A research report submitted to theFaculty of Management, University of the Witwatersrand, inpartial fulfilment of the requirement for the degree of Masterof Management. Johannesburg.
Stevens M (2000) ‘Abortion reform in South Africa’, Initiativesin Reproductive Health Policy, July, 4–6.
Tollman S and Rispel L (1995) ‘Organisation planning andmanagement’ in South African Health Review, Health SystemsTrust. Durban.
Varkey SJ and Fonn S (2000a) ‘How far are we? Assessing theimplementation of abortion services: A review of literature andwork-in-progress’, Health Systems Trust. Durban.
Varkey SJ and Fonn S (2000b) ‘Termination of Pregnancy’ inCrisp N and Ntuli A (eds.) South African Health Review, HealthSystems Trust. Durban.
Varkey SJ, Fonn S and Ketlhapile M (2000c) ‘Implementingthe abortion law in South Africa: health service barriers andsolutions’ paper presented at the World Health Organisationconsultation to develop technical and policy guidance on safeabortion for health systems. Geneva.
Varkey SJ, Fonn S and Ketlhapile M (2000d)‘The role of ad-vocacy in implementing the South African abortion law’ Re-productive Health Matters; 8 (16):103-111
Varkey SJ and Roberston ER (2000) Report on the HealthWorkers for Change – working to improve quality of abortionservices workshop to the MCWH directorate in the North WestProvince. Women’s Health Project, Department of Commu-nity Health, University of Witwatersrand.
IntervieweesGail Andrews (Director, Women’s Health, National Departmentof Health), Tamara Braam (Former co-ordinator of Reproduc-tive Rights Alliance), Kim Dickson-Tetteh (Clinical Director,
The Johannesburg Initiative
Advocating for abortion access
282
Reproductive Health Research Unit), Audrey Elster (Formerdirector of Planed Parenthood Association of South Africa),Rachel Jewkes (Director, Centre for Epidemiological Researchin South Africa, Medical Research Council, Essina Mabitsela(Deputy Director, MCWH, Northern Province), MakgoaleMagwentshu (Assistant Director, Professional Nursing ServicesDirectorate, Gauteng Province), Mia Milan, (Health Reporter,South Africa Broadcasting Corporation), Rose Mazibuko (ChiefDirector, Planning Primary Health Care & District Health Serv-ices, Northern Province), Judi Merckel (Administrator, Repro-ductive Rights Alliance), Eddie Mhlanga (Chief Director,MCWH, National Department of Health), Michelle O’Sullivan(Director, Women’s Legal Centre and former co-ordinator ofReproductive Rights Alliance), Loveday Penn-Kekana (Con-sultant during the legal and implementation process to theReproductive Rights Alliance), Dr. Perez (Doctor in charge ofO&G in Warmbath hospital, Bushveld Region, Northern Prov-ince), Cathy Pretorius (Assistant Director, Primary Health CareServices Bushveld Region, Northern Province), Helen Rees,(Director, Reproductive Health Research Unit), DoreenSenokoane (Deputy Director, MCWH, Gauteng Province), andMarion Stevens (former policy analyst of the Women’s HealthProject).
AuthorsBarbara Klugman (see page 39).
Sanjani Jane Varkey was a researcher at the Women’s HealthProject until December 2000. She is a social worker and hasworked in India and South Africa. She managed researchprojects on health systems research and policy analysis thatfocused on the implementation of the abortion law in SouthAfrica. In India she worked with women’s and children’s groupsaround their health rights.
United States of America
283
EXPANDING ABORTION ACCESS:THE US EXPERIENCE
Population size
Women of reproductive age(15-44)
% population living in urbanareas
Gross domestic product percapita
Human development index
Literacy rate of women15+
Maternal mortality rate
Religious affiliation
Abortion legal status
275,617,000
63,000,000
80%
US$6,259
0.943
99%
7.7 per 100,000
Protestant: 58% Catholic:26%
Legal but restrictions vary bystate such as requiringparental involvement,mandatory waiting periods orwhether there is state funding
Marlene Gerber FriedNational Network of Abortion Funds; Civil Liberties and PublicPolicy Program, Hampshire CollegeShelia ClarkeNational Black Women’s Health Project
The Johannesburg Initiative
Advocating for abortion access
284
IntroductionDespite twenty-seven years of legal abortion, access to abor-tion in the United States (US) is currently in a state of crisis.After almost three decades of consistent anti-abortion attackson many fronts, the political landscape has become increas-ingly hostile and there has been a steady erosion of access.The burdens of this situation are borne particularly by the mostvulnerable women – young, low-income women and womenof colour. These women often face insurmountable obstaclesin trying to obtain an abortion.
The introduction of anti-choice policies and legislation hasskyrocketed over the past few years. In the 1999 legislativesession, there were more that four hundred anti-choice meas-ures introduced and forty enacted by Congress and differentstates (National Abortion Rights and Action League (NARAL)& NARAL Foundation, 2000). Anti-choice activity has inten-sified and continues to demoralise and stigmatise women whohave abortions and abortion itself. When we add abortion clinicviolence, the murders of providers and the existing shortageof providers, we have a bleak picture of the status of abortionrights.
While the majority of Americans continue to support legalabortion, the number of people calling themselves pro-choiceis dropping and many of the supporters remain unaware ofthe threats to access. Especially with the recent approval ofMifepristone (also known as RU 486), there is a tendency tothink that access will be secured. Support for legal restrictionson abortion has grown, especially among young people. Thework of abortion rights advocates is therefore both difficult andcritical.

United States of America
285
This paper reviews the history of abortion access and advo-cacy; provides an account of the current status of access andadvocacy; maps the range of strategies in use and providesinsight into their effectiveness. The four case studies provideexamples of legislative and grassroots advocacy and organis-ing with medical facilities and with providers.
ContextThe US is a capitalist society, with significant inequalities ofrace, gender, and class. Over the past two decades, the socialwelfare supports that provided something of a safety net forpoor people have been severely curtailed. Programs have beendismantled and eligibility requirements for benefits becomemore restrictive. The impact on health care has been espe-cially serious. While there is a federal program, Medicaid, thatprovides health insurance for poor people, many poor andlow-income people do not qualify for benefits. Approximatelythirty-five million people have no health care coverage at all,including twelve million women of childbearing age.
While the US is a secular society, the Catholic church and reli-gious fundamentalist groups have significant influence overpublic policy and legislation, both directly and indirectly. Since1980 fundamentalist Christians have wielded tremendouspower within the Republican party. They have had a particu-lar impact in the areas of reproductive and sexual politics. Theparty’s official platform is explicitly opposed to abortion.
Race, class and reproductive rightsThe battle over abortion dominates reproductive politics inthe US. Mainstream pro-choice organisations have had thenarrow focus of defending the legal right to abortion. In con-trast, abortion as a single issue has not emerged with the samevigour in low-income communities and communities of col-our. Women of colour suffer disproportionate rates of poverty,lack access to health care information and services, lack insur-ance coverage and lack access to contraceptive services. Blackwomen are three times more likely than white to have an abor-tion; Latina women are twice as likely (AGI, 2000). The socio-

The Johannesburg Initiative
Advocating for abortion access
286
economic conditions manifest themselves in disproportionaterates of HIV/AIDS, sexually transmitted infections, reproduc-tive cancers and poorer overall reproductive health. The ma-ternal mortality rate for black women is four times that for whitewomen. The rate for Hispanic women is nearly twice that ofwhite women. Given this situation, women of colour organi-sations have necessarily placed abortion within a broader con-text of reproductive health and rights and have urged themainstream movement to do so as well. Unfortunately, untilrecently, this message has not been absorbed. Thus the his-tory of reproductive rights advocacy in the U.S. has been oneof division, based not only on class and race divisions, butalso on the failure of the pro-choice movement to appreciatehow those differences mediate women’s reproductive lives.
Underlying the political divisions are divergent understandingsof reproductive rights, which are themselves grounded in dif-ferent class and race experiences. Dorothy Roberts, AfricanAmerican activist and legal scholar, argues that the AfricanAmerican women’s narrative of reproductive rights is dramati-cally different from the mainstream story of increasing repro-ductive control through legalising contraception and abortion.African American and other women of colour and low-incomewomen have experienced a history of dehumanisation, abuseand coercion through policies that attempt to control them bycontrolling their reproduction. Eugenics has been a persistenttheme. For example, between 100,000 and 150,000 poorwomen, half of them African American, were sterilised annu-ally under federally sponsored mass involuntary sterilisationlaws and programs in the 1970s (Roberts,1997:90).
More recently, punitive welfare ‘reform’ policies that restrictbenefits for women who have more children while receivingpublic assistance, the coercive use of reproductive health tech-nologies such as Norplant and Depo-Provera by the medicaland criminal justice community and privately funded programssuch as CRACK (a national, private organisation that payswomen who are addicted to drugs $200 to be sterilised or touse long-acting contraceptives) all target the fertility of low-income women (Fried, 2000: 184-187).
United States of America
287
For middle class women, legal abortion brought greater ac-cess. For low-income women, access has not followed legali-sation. Instead, they have borne the brunt of the restrictionson access to abortion and to all other aspects of reproductivehealth care.
Historical context: Abortion in the 19th
centuryUntil the middle of the 19th century, termination of pregnancywas legal in the US under common law until ‘quickening’ (ap-proximately the fourth month) and only minimally regulated.A campaign to criminalise abortion began in the 1870s. Bythe 1880s it was illegal in every state and remained so until1973 except in cases where it was necessary to save the life ofthe woman. Contraception was also illegal throughout muchof the same period. Birth control for married women was notlegalised until 1966 and for unmarried women until 1972. Il-legal abortion was widely used, however. Although estimatesvary, an American Medical Association (AMA) committee con-cluded that in 1872, 20% of all pregnancies were deliberatelyaborted, and that nine out of ten premarital pregnancies wereaborted in the 1930s (Reagan, 1997: 23).
The 19th century criminalisation campaign was initiated by theAmerican Medical Association (AMA). This was part of an ef-fort to win professional power, control medical practice andrestrict competition, especially from homeopaths and midwives.The campaign was waged as a moral crusade (Petchesky, 1990:80). Although the doctors argued that abortion was medicallydangerous, the attack on abortion came when abortion hadbecome a safer procedure.
Gender, racial and class anxieties were also integral to the AMAcampaign. Before 1840, it was poor, unwed and socially des-perate women who had the majority of abortions. After 1840,abortion was the systematic practice of ‘respectable women’ –married, middle or upper class, native-born Protestants whocould afford doctors. As a result, the white Anglo-Saxon birthrate declined. Immigrants had entered the country in largenumbers and there was a fear that the newcomers would soon

The Johannesburg Initiative
Advocating for abortion access
288
outnumber native-born whites and threaten their politicalpower (Reagan, 1997:11).
The harshest impact of criminalisation was in the high rates ofwomen’s mortality and morbidity, linked closely to race andclass. In the 1960s in New York City, 80% of the deaths fromillegal abortion were black and Puerto Rican women (Ross,1998:161). Overall mortality was estimated at 1,000 to 5,000deaths annually, with hundreds of thousands more injured.Abortion deaths accounted for half of the maternal deaths ofwomen of colour, compared to 25% of white deaths.
Advocacy strategies 1950s-1973: Changing the lawWhile there were scattered calls for legal change, there was noserious attempt to overturn these laws until the late 1950s.There was also no public discussion of the issue. Kristin Luker(1984) explains this in terms of the doctors’ success in secur-ing medical ownership of abortion. Female ignorance was pit-ted against technical knowledge available only to physicians.Further, therapeutic abortion was frequent and illegal abor-tion was an accepted part of reproductive life.
Why did this change? Rosalind Petchesky explains it in terms ofthe confluence of social need, feminist activism and populationcontrol politics. There had been important social changes – latermarriage and childbearing among young women, increasinglevels of college attendance, rising labour force participation ofyoung women, rising divorce rates and an increase in the numberof female-headed households. At the same time, other condi-tions endured including ‘a sexual division of labour makingwomen primarily responsible for children; a lack of commitmentto government funded social services, especially child care andhealth care; and the need of all women to avoid unwanted preg-nancy for reasons of health, sexual self-determination, and so-cial self-actualization’ (Petchesky, 1984:103-4).
Initial advocacy efforts were among small groups of profes-sionals – public health officials, attorneys and prominent phy-
United States of America
289
sicians. They took a cautious, behind-the-scenes approach.Later abortion became a ‘woman’s issue’. The early advocatessaw abortion as a public health, a doctor’s, or a populationcontrol issue, not as a woman’s right. Organisations and coali-tions who were not grounded in the women’s liberation move-ment arose which were sometimes at odds with that move-ment. Even in the re-emerging mass women’s movement, abor-tion was controversial. The National Organisation for Women(NOW), the largest feminist organisation, endorsed abortionlaw repeal, but there was internal disagreement. There weremany who wanted to focus only on economic issues.
More radical feminist groups were often opposed to lobbyingand opted for more overt and confrontational political activi-ties – demonstrations and rallies. They emphasised concreteaccess to abortion. For example, an initiative from the feministmovement called for ‘Free Abortion on Demand’ while moreliberally oriented groups talked about the legal right to choose.There was also a disagreement over whether to press for legalreform or repeal.
NARAL, the first single-issue abortion rights organisation, wasfounded in 1969 at what was billed as the first national Con-ference on Abortion Laws. Although they adopted a woman’srights framework, medical and population control frameworksfor abortion have tended to dominate pro-choice politics.
NARAL’s tactics were also more traditional, especially in com-parison with the other social movements that were active, suchas the civil rights, anti-war, and women’s movement. NARALadopted a non-confrontational approach in the hope of mo-bilising professionals and mainstream Americans. The organi-sation used established channels for public education such asconventions of professional and health organisations, cultiva-tion of media contacts and letters to editors rather than tryingto attract media attention through their actions. They also usedconventional means of influence such as legislative lobbyingand litigation. These differences from other groups led to divi-sions, which have persisted in various forms through decadesof abortion rights organising.
The Johannesburg Initiative
Advocating for abortion access
290
Population control politicsPopulation control politics were prominent in the initial move-ment to change abortion laws. Individual activists who hadexperience in family planning and were from population or-ganisations such as the Association for Voluntary Sterilizationand Zero Population Growth were active. African American,feminist, pro-choice activists Angela Davis, Loretta Ross,Dorothy Roberts and others explain why this is a problem.They note that while African American women have consist-ently used abortion as a means of regulating their fertility, theyhave also opposed the population control politics that so of-ten accompany advocacy efforts for both contraception andabortion.
Loretta Ross documents the early involvement of the blackwomen’s club movement in the establishment of family plan-ning clinics in black communities and their simultaneous op-position to the racist de-population policies of population con-trol advocates. During the 1960s and 1970s, some black na-tionalist groups took the position that abortion and birth con-trol were genocide. They argued that the appropriate responsewas for black women to have more babies. The Black PantherParty was the only nationalist group to support free abortionsand contraception on demand although this was controver-sial.
The concern about genocide affected mainstream minorityorganisations as well. The National Association of ColouredPeople and the Urban League, both of which had supportedreproductive rights as a means of racial progress, distancedthemselves from this position in the 1960s. The legacy of ra-cial population control policies still pervades abortion politicstoday. The anti-choice movement has become adept at usingblack fears about genocide and has made significant in-roadswith black churches (Ross, 1998:166).
Direct action strategiesApart from the mainstream organisations, there were manygrassroots women’s groups and young women who saw abor-
United States of America
291
tion as their issue during this period. In this context, abortionreferral work – helping women wanting abortions to find pro-viders – was a key and very effective strategy even thoughsome activists criticised it as only a way of helping, rather thana political strategy.
The work helped mobilise grassroots activists and build com-mitment. It attracted media attention, provided concrete tasksfor activists and brought activists into immediate contact withwomen who were directly harmed by the laws restricting abor-tion. As one of those involved explained: ‘Everybody was in-volved in doing referrals. It was a tonic: We couldn’t have keptgoing without the constant reminders of women who neededhelp’ (Staggenborg, 1991:24). Important organisations devel-oped from this work including ‘Jane’ (see below) and TheClergy Consultation Services that brought large numbers ofclergy into the repeal movement.
The women’s health movement grew out of women’s libera-tion groups. They saw themselves as part of a larger move-ment that was challenging basic social, economic, and politi-cal institutions. The goal was to create alternative democraticparticipatory institutions. In the area of health care, this meantthat women would participate in their own health care. In con-trast to the mainstream approach, these groups by-passed es-tablished organisational channels and reached women directlythrough new forums. These included Our Bodies/Ourselvescourses and abortion speak-outs in which women who hadillegal abortions spoke about them publicly. This promotion ofopen discourse helped to break the decades of silence sur-rounding abortion.
Radical abortion activists had a confrontational style. Theytaught classes on how-to-do abortions and distributed do-it-yourself abortion kits. They saw themselves as committing civildisobedience and aimed to get arrested. In the late 1960s inCalifornia, activists pioneered self-examination and then ‘men-strual extraction’, the process which a woman or a group coulduse to remove the contents of the uterus. Their goal was not tobecome abortion providers but to empower women.
The Johannesburg Initiative
Advocating for abortion access
292
In 1969, the Jane Collective was transformed from a referralgroup to a provider. Jane was a grassroots women’s group.Members were neither health professionals nor abortionists.They were lay women who were trained by an abortion pro-vider who also was not a doctor. Between 1969 and 1973,Jane provided 11,000 abortions. Cost, quality of care andwomen’s empowerment were the key priorities.
LegalisationBy the late 1960s advocates saw that changing laws state bystate would take forever and in some states change seemedentirely hopeless. At the same time, there had been court vic-tories in certain states. Several more established and resourcedorganisations initiated the idea of a litigation strategy that wouldhave an impact throughout the country. They wanted to finda ‘test case’ that would bring the issue to the United StatesSupreme Court which usually accepts cases when differentfederal courts are at odds on the same issue. This was ulti-mately the winning strategy.It could not have succeeded, how-ever, without the other advocacy and activism. Changes inthe social conditions that shaped women’s lives and in femi-nist ideology were also relevant.
Several cases were brought in federal courts to challenge statelaws. One of these was Roe v Wade, the case that ultimatelygave US women the right to choose abortion. In 1973, the USSupreme Court, by a 7-2 vote, decided Roe v Wade whichdeclared that all the existing abortion laws were unconstitu-tional and that a woman’s right to make her own decision aboutabortion was protected under the right to privacy. The courtdid not affirm a woman’s right to bodily autonomy, however,which is what feminists had pressed for.
From a public health perspective, the legalisation of abortionhad a tremendously positive impact. As one doctor put it: ‘Thedeaths stopped overnight in 1973 and I never saw anotherabortion death in all the eighteen years after that until I re-tired’ (quoted in Miller, 1993:12).
There were also serious criticisms of Roe v Wade from femi-nists who argued that Roe was more about the rights of doc-
United States of America
293
tors to practice medicine than about women’s rights. Blackwomen, too, sounded an important cautionary note. An edi-torial supportive of Roe in the publication of the NationalCouncil of Negro Women warned:
The key words are ‘if she chooses.’ Bitter experiencehas taught the Black woman that the administration ofjustice in this country is not colourblind. Black womenon welfare have been forced to accept sterilisation inexchange for a continuation of relief benefits and othershave been sterilised without their knowledge or consent.A young pregnant woman recently arrested for civil rightsactivities in North Carolina was convicted and told thather punishment would be to have a forced abortion. Wemust be ever vigilant that what appears on the surface tobe a step forward, does not in fact become yet anotherfetter or method of enslavement (Black Woman’s VoiceII(2), Jan/Feb 1973).
Undermining and defendingabortion access, 1973-1989Anti-abortion strategiesThe legalisation of abortion galvanised its opponents. Theywere quick to test the limits of Roe by sponsoring a flurry oflegislation to restrict access. Beginning immediately in 1973,they won several legislative victories prohibiting federal fund-ing of abortions outside the US. Later they succeeded in pro-hibiting federal funding of abortions within the US. This policyprevails today with few exceptions.
The anti-abortion movement used a wide array of strategies,legal and illegal. These included election of anti-abortion can-didates and targeting pro-choice candidates for defeat; appoint-ments of anti-abortion judges; public education campaignsconducted through the churches and the media; and attackson abortion providers. Targeting clinics and providers becamea key strategy in the 1980s. There were regular clinic block-ades and picketing, bomb threats and other forms of vandal-
The Johannesburg Initiative
Advocating for abortion access
294
ism, with over 80% of family planning clinics experiencing someform of serious harassment. The use of deadly violence beganin the 1990s. There have been seven murders of doctors andothers that work in abortion clinics to date.
Abortion rights strategies
Single-issue politics: Defending Roe v WadeWhile some groups like Jane worried about the impact of le-galisation on the quality and accessibility of abortion services,most advocates seemed to feel that the battle had been wonand the abortion rights movement declined. More radical seg-ments of the movement mobilised after the federal fundingcuts, but it was not until the 1981 threat of a Human LifeAmendment to the United States constitution to protect foetallife from the moment of conception that a large-scale visiblemovement emerged.
Unlike the movement for legalisation, the pro-choice move-ment of the 1980s was shaped by the need to respond to whatwas, by then, a full blown and multi-faceted attack on abor-tion rights. The anti-abortion movement appeared to be eve-rywhere, even in the presidency. The general political contextwas conservative and anti-choice. Reagan, the new president,had been elected in part through organised efforts that includedanti-abortion organisations. Once elected, conservative, reli-gious and anti-abortion organisations had unprecedented ac-cess to political power and resources. The attacks on abortionand family planning clinics intensified during this period. Therewas also an impact on policy. Federal monies were channeledto anti-abortion counseling centers and religious organisationsto teach abstinence-only sexual education. A ‘gag rule’ waspassed prohibiting family planning clinics from even counsel-ling about abortion as an option for dealing with an unplannedpregnancy. Throughout the Reagan and subsequent Bushpresidencies, there was an accelerated undermining of the rightsof women, people of colour, and the poor through cutbacks inaffirmative action and welfare programs, as well as on abor-tion and reproductive health.
United States of America
295
In addition to the pressure to be reactive to the right wing on-slaught, there were other significant changes that had an im-pact on the movement. Protest in general had declined. Move-ment leadership was professionalised, with paid staff takingthe place of activists in organisations and structures becomingmore formalised. At the same time, there was a decline in lo-cal women’s liberation groups and more conventional interestgroup politics prevailed. Several single-issue groups were cre-ated with a focus on the political arena.
This movement was not part of a larger women’s movementand was therefore narrower than the one which had foughtfor legalisation. In the face of the anti-abortion onslaught, itfocused on defending the legal right to abortion, with appealsto ‘choice’ and ‘privacy’ rather than ‘abortion’ and ‘women’srights’. Services and access were not at the forefront of theagenda.
A multi-issue approachAlternative groups emerged that were critical of the mainstream,single-issue approach as too narrow, too conservative and ig-norant of the issues that were affecting low-income womenand women of colour. These groups had their roots in otherprogressive movements, including women’s health, civil rights,anti-war and the left. The alternative groups were multi-issueand advocated a pro-active strategy. They were also concernedwith the ways in which the abortion issue was being framed.The language of choice spoke to those in the society whothought of themselves as having choices, not to those who didnot. These groups wanted to create a multi-racial movementand saw the importance of overtly opposing population con-trol and working against sterilisation abuse and coerced abor-tion.
They were critical of the major groups for their failure to actagainst restrictions on access which affected primarily low-in-come women and women of colour. For example, in 1977,when Rosie Jimeñez, a single mother on welfare became thefirst woman known to have died from an illegal abortion after
The Johannesburg Initiative
Advocating for abortion access
296
the cut off of federal funding, none of the national organisa-tions took up the issue. Analysts suggest that the traditionalabortion groups, essentially white and middle class, felt thatRosie might not be a sympathetic figure as she was a Mexican-American, an unwed mother in a border town noted for illegaldrug trafficking and had apparently been pregnant several timesbefore (Frankfort with Kissling, 1979). Further underscoringhow little value was placed on Jimenez’ life, the illegal abor-tionist received a punishment of three days in jail and had topay a $100 fine.
New organisations were formed to oppose the attacks on thereproductive rights of women of colour. While they were smallerand lacked the resources of the large, single-issue groups, theywere effective in changing policy, raising awareness and creat-ing a more radical political pole within the movement. TheCommittee to End Sterilisation Abuse (CESA) in New YorkCity exposed the widespread practices of sterilising womenwithout their knowledge or consent. The Committee for Abor-tion Rights and Against Sterilisation Abuse was formed withthe perspective that fighting for abortion rights necessitatedfighting against population control. The strategic tactics of thesegroups included demonstrations, counter-protests at anti-abor-tion events and a petition campaign against the Hyde Amend-ment, the measure banning the public funding of abortion.
Women of colour reproductive health and rights organisationsalso formed during this time. Individual women and men ofcolour, black women’s groups, and civil rights organisationshad been part of the fight to legalise abortion. Black doctorshad been involved in providing illegal abortions and individualblack women participated in Jane and other pre-legalisationactivities. A few well known African American feminists spokeout early about racism, about the sexism within the black na-tionalist movement and in favour of a woman’s need and rightto make her own decisions about childbearing. But it was notuntil the 1980s that women of colour groups devoted to wom-en’s health and reproductive rights were organised. During the1980s, women of colour active on reproductive rights issuespursued a dual strategy. They pressured mainstream organi-
United States of America
297
sations and created separate women of colour organisationsthat would promote a broader reproductive health and rightsagenda and serve to break the silence in their own communi-ties about abortion, contraception, violence and related issues.
Intensified attacks againstaccess, 1990 onwardsThere was another shift in the advocacy landscape when theUnited States Supreme Court gave the states greater latitudeto restrict abortion access in Webster v Reproductive HealthServices in 1989. At the same time, the anti-abortion move-ment had made abortion clinics and providers the central tar-get of their protests. These events re-energised the pro-choicemovement. Thousands of younger women who had not beenactive previously were drawn to large demonstrations and to‘clinic defence’, maintaining a visible pro-choice presence atclinics to counter the anti-abortion demonstrators. In April1989, just prior to a large pro-choice march in Washington,women of colour came together for the first time to talk aboutdefending abortion rights in the Defence of Roe Conference,co-sponsored by the American Civil Liberties Union, the Reli-gious Coalition for Abortion Rights and the Women of ColourPartnership Programme.
This period of increased pro-choice activism ended just afterthe election of pro-choice president Clinton. National advo-cacy organisations endured, but had to struggle for members,resources and public attention. Strategically, organisations fo-cused on state-level organising because that is where the at-tacks were emanating from, either legislatively in the courts orin the form of clinic violence on the streets.
More recently, with the anti-abortion focus on ‘partial birth’abortion, Mifepristone, foetal tissue research and deadly vio-lence, the focus has shifted back to the national level. Theexistence of a pro-choice administration has also been relevantto this shift since pro-choice advocates have had access topower and opportunities which were closed to them duringthe Reagan/Bush years of 1980-1992.
The Johannesburg Initiative
Advocating for abortion access
298
Current strategies to expandaccessContextAs noted, since legalisation, the major anti-abortion strategyhas been to work toward the re-criminalisation of abortionprimarily through steadily chipping away at access. This hastaken its toll primarily on women who have little power, voiceor visibility in the political arena, namely low-income women,young women and women of colour. Before legalisation, theconsequences of illegal abortion to women’s lives and healthwere dramatic for all groups of women. In contrast, this slowerosion of access does not immediately burden middle classwhite women. It has therefore been difficult to mobilise largenumbers of pro-choice supporters or to muster a widespreadsense of urgency. Younger women did not feel the impendingthreat of criminalisation or loss of rights. They seemed to thinkthat abortion will always be there for those who really need it.
With the new Bush presidency, the overall political climate forabortion rights has changed. Pro-choice advocates have beengalvanised by the immediate and bold attacks on abortion andfamily planning. President Bush will have many opportunitiesto undermine abortion rights and access through executiveorders and by sponsoring restrictive legislation. He will ap-point two or three new Supreme Court justices and hundredsof federal court judges as well as the heads of various agen-cies. He has already appointed two staunch opponents of abor-tion to his cabinet, reinstated the global gag rule and asked theFederal Drug Administration to reconsider its approval of RU486.
Current pro-choice strategies are multi-faceted as they try toaddress the lack of access, as well as the political and ideologi-cal losses in support for abortion rights. In addition to ap-proaches which aim directly at increasing access, other relatedgoals include reactivating the traditional pro-choice constitu-ency; reclaiming the ideological and moral ground; drawingin new supporters; and legislative and candidate support. The
United States of America
299
listing below is an effort to provide a snapshot of the range ofstrategies and national organisations involved. Many of theorganisations work in more than the one area in which we listthem.
In brief, the strategies and the national organisations involvedare:
• Training more providers: Medical Students for Choiceand the Physician Mobilisation Project (see case studies)focus on attracting new providers, advocating for inclu-sion of teaching about abortion and reproductive healthin medical schools and training medical students. TheAmerican Women’s Medical Association, the AbortionAccess Project (AAP) and the National Abortion Fed-eration and Planned Parenthood of New York City haveall produced curricula for medical schools.
• Expanding the provider pool: The National Abortion Fed-eration and the Abortion Access Project have projects toenable nurse practitioners, nurse midwives, and physi-cian assistants. They also work to establish student pro-choice groups within the professions.
• Expanding abortion services: The 18% decrease in abor-tion services has come primarily through hospitals thathave stopped providing the services. The Hospital Ac-cess Project (see below) is working to increase abortionservices at hospitals. Merger-Watch and Catholics for AFree Choice are working to stop mergers of secular andreligious hospitals and to preserve reproductive healthservices that are often compromised when such mergersoccur.
• Providing support for existing providers: Several asso-ciations have been formed to offer support and ongoingtraining for abortion providers. These include the Na-tional Abortion Federation, National Association of Re-productive Health Professionals, Physicians for Repro-ductive Choice and Health and the National Coalitionof Abortion Providers. There are also grassroots efforts
The Johannesburg Initiative
Advocating for abortion access
300
to mobilise community support for abortion providersand against anti-abortion violence. Pro Choice ResourceCentre’s Communities United for Reproductive Safety,Refuse and Resist and the clinic violence task force ofthe Feminist Majority Foundation are two of the biggerprojects.
• Providing funding for low-income women and girls andadvocating for public funding: The National Network ofAbortion Funds has more than seventy-five grassroots-based members that provide direct assistance to womenin need and advocate for public funding of abortion.The Centre for Reproductive Law and Policy, the Re-productive Freedom Project of the American Civil Lib-erties Union and the NOW Legal Defense and Educa-tion Fund are the major groups trying to use the courtsto get states to pay for abortions.
• Broadening the agenda and mobilising new constituen-cies: The National Black Women’s Health Project, Na-tional Asian Women’s Health Organisation, Asian Pa-cific Islanders for Reproductive Health, National LatinaHealth Organisation, Native American Women’s HealthEducation Resource Centre and CARE 2000 Campaign(see below) represent groups organising communities ofcolour.
• Changing public opinion and regaining the moral highground: NARAL’s Pro Choice Public Education Projectfocuses on reaching young people through the media.
• Mobilising the religious community: The Religious Coa-lition for Reproductive Choice and Catholics for A FreeChoice work to organise the faith community on repro-ductive health and rights issues.
• Organising young women: Choice USA, the FeministMajority Fund and the Civil Liberties and Public PolicyProgramme at Hampshire College all focus on mobilis-ing college and high school students.
United States of America
301
In addition to the above targets and strategies, pro-choice or-ganisations and strategies focus on goals which are necessaryto preserve legal abortion and to increase access. The strate-gies and organisations involved include the following:
• Providing services, training, as well as advocacy and lob-bying: Because the medical establishment did not em-brace abortion care and service provision, advocacygroups have had to provide this as well as ongoing train-ing in new procedures. The Planned Parenthood Fed-eration of America and its affiliates, clinic and individualabortion providers and the National Abortion Federa-tion have taken a leading role in this.
• Challenging conscience clauses: Physicians, hospitals,medical schools and now pharmacists have all claimedconscience protection to avoid providing services andreferrals for abortion and contraception. The Reproduc-tive Freedom Project of the American Civil LibertiesUnion and the Pro-Choice Resource Centre have takenthe lead in investigating existing legislation and policyand in bringing advocates together to frame model leg-islation and mount political challenges.
Case studiesWe cannot possibly do justice to this impressive array of re-productive rights advocacy. Instead we have chosen to high-light four grassroots approaches to expanding abortion access.None primarily involves changes in law. The first three areefforts to address different aspects of the provider shortage.The last one looks at a 1994 effort to restore public funding forabortion and its revival in 2000.
Case study I: The Physician MobilisationProjectAs noted, women of colour and low-income women representa significant number of women with the most need and leastaccess to abortion services. At the same time, mobilisation of
The Johannesburg Initiative
Advocating for abortion access
302
advocates and physicians of colour has been limited. The Phy-sician Mobilisation Project addresses this problem.
The Institute for Women and Ethnic Studies (IWES) was cre-ated in 1990 by two female physicians in response to the ab-sence of African American physician voices on issues relatedto reproductive health and choice. Its mission is to ensure ac-cess to comprehensive reproductive health care for AfricanAmericans by increasing the commitment of physicians to thedelivery of such services. IWES acknowledges the importanceof having a physician group that can address and respond tothe unique concerns of women of colour and low-incomewomen.
The Physician Mobilization Project was the first project of IWES.Since 1990, IWES has instituted programmes designed to ex-pose minority physicians in training to reproductive health andrights issues. It is the only effort specifically aimed at promot-ing reproductive health and rights issues with minority practi-tioners.
The initiative includes a variety of programmes. The Interna-tional Fertility Management Programme held in conjunctionwith the University of the West Indies-Jamaica, the Universityof Edinburgh-Scotland and the Karolinska Institute-Swedenbrought together twelvestudents to do elective work focusedon RU 486. It was felt that exposure to common abortion prac-tices internationally would positively alter domestic perspec-tives of practitioners. IWES also sponsored Reproductive HealthInternships in the Office of Public Health family planning clin-ics between 1996 and 1998. Six to ten medical students ofcolour were recruited each year to participate in this rotation.Through the provision of reproductive health services in apublic health setting, students were exposed to the broad andcomplex issues affecting low-income women.
The Reproductive Health Advocacy Programme recruited mi-nority medical students to participate in a dialogue on repro-ductive health through the use of facilitated discussions. Thesediscussions included an introduction to advocacy organisations
United States of America
303
such as the National Black Women’s Health Project and Medi-cal Students for Choice. At the conclusion of the workshopsstudents were encouraged, though the provision of technicalassistance and financial support, to develop advocacy initia-tives on reproductive health on their campuses and in their or-ganisations. This strategy has been successful in its growth andoutreach to minority students. It also fosters the ability of medi-cal students to advocate within their professional organisationsand amongst their peers. The project facilitates current and fu-ture collaborative work between the advocacy and medical com-munities, which is vital in the expansion of services. An exam-ple of this collaborative work has been the involvement of ad-vocacy groups on panels of the national and regional confer-ences of the Student National Medial Association, the minoritymedical student organisation that participated in the programme.These linkages with minority medical students and organisa-tional advocates will help to establish and expand an integratedand strengthened advocacy for abortion access.
Case study II: The Hospitals ProjectThe decline in abortion services over the last twenty years hasbeen caused in part by a decrease in hospital-based abortionservices. The number of hospitals performing abortions fellfrom 1,405 in 1982 to 703 in 1996 (Abortion Access Project,1999). The number decreased by 18% between 1992 and 1996alone. Only 14% of US hospitals currently provide abortionsand many of these perform only a few procedures per year.The Alan Guttmacher Institute study also found that while in1973, 81% of all providers were in hospitals, in 1996 only36% of providers were in hospitals and less than 7% of allabortion procedures were performed in hospitals (AbortionAccess Project, 1999).
The limited provision of hospital-based abortion services re-stricts access for women who lack other options. For ruralwomen, hospitals may represent the only source of medicalcare, yet nine out of ten abortion providers are located inmetropolitan areas. Low-income women also rely on hospi-tals for care as hospitals may accept Medicaid funding which
The Johannesburg Initiative
Advocating for abortion access
304
many clinics do not and certain states provide free or indigentcare. Hospitals play an important role in access as services athospitals may enhance access for women with special medicalneeds or complications. Hospitals also perform late abortions,which many clinics are not equipped to do. Finally, a criticalrole of hospitals is to provide training sites for medical resi-dents. Hospitals that don’t provide abortions at all, or do veryfew, cannot fulfil this role (Abortion Access Project, 1999).
The Hospitals Project was initiated by the AAP, a grassrootsorganisation based in Boston, Massachusetts, in 1993 as a di-rect response to the decreasing number of hospital-based abor-tion services. Strategies used by this project are primarily grass-roots in that efforts are made to mobilise community supportand pressure. The strategies are aimed at changing policy atthe institutional rather than governmental or legislative level.Through community organising, negotiation with hospitals,public education and raising awareness about obstacles toaccess, the project pressures hospitals to offer abortion serv-ices and to make them more accessible to larger numbers ofwomen.
This is also a movement building strategy to draw in new ac-tivists. It has the potential to create broader coalitions and newallies. Having hospitals provide abortions as a service towomen, helps shift abortion into the realm of comprehensivehealth care for women as opposed to being a segregated serv-ice. AAP recently began a successful campaign to pressureCatholic hospitals in Massachusetts to offer emergency con-traception to rape victims.
In 1998 AAP co-founded the Hospital Access Collaborative,with the goal of engaging more states in the vital work of in-creasing hospital based abortion services. Currently, twenty-four states across the country are working on hospital accessprojects. The ultimate goal of the Hospital Access Collabora-tive is to increase hospital-based abortion services by dissemi-nating information about the different but complementarymodels of organising around hospital access developed bygroups around the country.
United States of America
305
In terms of capacity building for the movement, the campaignin Massachusetts has been successful in several ways whichare crucial, not just to the present period, but also in the ongo-ing battle to preserve and expand abortion rights. In the firstthree years of organising, five hospitals changed their intakeprocedures to increase the accessibility of abortion services.Two hospitals changed their policies to allow the use of freecare funds to cover abortion procedures. One hospital thatdid not previously have abortion services has started provid-ing abortions. Another religiously affiliated hospital reversedits policy prohibiting affiliated doctors from performing abor-tions. These victories have not only expanded access, theyhave also expanded people’s understanding of the importanceof the battle (Abortion Access Project, 1999).
Local activists have been involved in the advocacy efforts, withsupport and technical assistance from AAP, itself a commu-nity-based organisation. This strategy exemplifies the impor-tance of having women who are most affected in the forefrontof advocacy initiatives. With respect to challenges, translatingthe agendas of national organisations into concrete grassrootsactivities requires an understanding and appreciation of localcommunities and skills in grassroots organising in order toensure that the interests, needs and issues of that communityare prioritised. AAP uses a definition of access that makes cen-tral women’s ability to gain access. Further, the Hospital Ac-cess Collaborative and AAP support local projects, share ex-periences and organise working meetings but leave the actualorganising to people in the communities.
Case Study III: Midlevel access initiativesIn 1990, the National Abortion Federation (NAF) and theAmerican College of Obstetricians and Gynaecologists(ACOG), with foundation support, organised a symposium toidentify causes and find solutions to the pressing issue of theprovider shortage. Anti-abortion violence and harassment andthe sheer magnitude of service caseloads were identified asdisincentives to existing and potential providers. It was alsorecognised that as older physicians who provided abortions
The Johannesburg Initiative
Advocating for abortion access
306
reached retirement, there did not exist an expansive ‘pool’ ofreplacements. The decline in residency programmes offeringtraining in abortion techniques exacerbated this problem.
Utilising midlevel service providers – physician assistants, nursepractitioners and certified nurse midwives – was seen as animportant strategy for addressing the problem. Research datasubstantiated midlevels’ ability to perform first trimester abor-tions. The strategy provides an economical approach to abor-tion services. As midlevels tend to work in service areas thatare under-served, the needs of rural women could be met.
There are, however, significant barriers to this approach. Fromthe legal perspective, the majority of states have ‘physicianonly’ laws that may be interpreted to restrict midlevels’ abilityto provide abortion services. In addition, the medical commu-nity as well as patients think that only physicians can providethis procedure safely. It was important therefore, that strate-gies be developed that would address these attitudes and pro-mote the midlevel practitioner.
This initiative directly targets the medical community. Key tothe utilisation of midlevels was to have an already engagedand willing group of midlevel providers. Through collabora-tive work with the professional societies of midlevel clinicians,associations were encouraged to provide avenues and incen-tives for training in abortion care. Through advocacy with theprofessional associations and conferences of midlevels, edu-cation and awareness with respect to encouraging midlevelsto pursue training could be achieved. Education and advo-cacy on behalf of midlevel providers would better educate themedical community about their skills and abilities. Consumereducation in the form of news articles and other media wereused to educate the public about the valuable and qualifiedservices of midlevel practitioners. Collaborative work withphysicians promoted the work of midlevels as service enhance-ment and not service competition. This was seen as critical inestablishing rapport with physician practices.
With respect to the legal strategy, NAF decided that state lawshould be not be addressed though the development of a na-
United States of America
307
tional model. Instead, a state by state assessment by affiliateswas considered most appropriate due to the complex and dif-fering state laws.
This project has already had important outcomes. After theinitial symposium, a range of professional organisations rep-resenting midlevels issued statements supporting midlevels’involvement in the provision of abortion services. In 1994 theACOG endorsed a statement that encouraged programmes totrain physicians and other licensed health professionals to pro-vide abortion services in collaborative settings. This was sig-nificant in that it encouraged collaborative working relation-ships between midlevels and physicians.
In 1997, NAF developed Clinicians for Choice, an umbrellagroup for Physician Assistants for Choice, Nurse Practitionersfor Choice and Midwives for Choice. The goal of this group isto increase the education and training of midlevels and to buildsupport networks. To date, their membership is over 3,500.There are fifty-seven state chapters in the US and parts ofCanada. This core group of state contacts is a critical part ofNAF’s strategy to promote midlevel access through grassrootsactivities on the local and state level.
Case study IV: Campaign for Abortion andReproductive EquityAs noted, women of colour advocates have consistently ar-gued that in communities of colour abortion rights must bepromoted as part of a larger agenda which speaks to all thehealth, child bearing and reproductive rights and needs foraccess and services. The pro-choice movement has not beenadequately responsive to this message. Even in its single-issuepolitics, it has not focused on issues of access which especiallyburden women of colour. Thus in 1993, the Campaign forAbortion and Reproductive Equity (C.A.R.E.) campaign wascreated by the National Black Women’s Health Project to ad-dress the need for federal funding of abortion services.
CARE developed an advocacy strategy to repeal federal policythat banned the federal funding of abortion. In addition to
The Johannesburg Initiative
Advocating for abortion access
308
focusing on low-income women and women of colour, it alsoaddressed other groups of women who relied on the federalgovernment for their insurance. This included women in theDistrict of Columbia, women in federal prisons, women in themilitary, the Peace Corps and Native American women. Thetiming of the campaign was strategic in that the political cli-mate had changed with the election of President Bill Clintonin 1992, a pro-choice president.
The larger goal of the campaign was to rescind the restrictiveabortion language that limited poor women’s access to abor-tion though direct lobbying of policy-makers and grassrootsorganising of constituents. The campaign targeted five spe-cific appropriations bills that addressed the identified groupsof women. The primary strategies used were direct lobbyingof members of Congress by organisational advocates and con-stituents and grassroots organising in Congressional districts.In addition to these legislative strategies, advocates undertookinternal lobbying efforts with respect to getting mainstreamgroups to prioritise this issue and dedicate time and resourcesaccordingly.
While the attempt to repeal the Hyde Amendment (legislationprohibiting public funding of abortion) was not successful, theeffort expanded the legislative language to state that federalmonies could be used to fund abortions in the case of rape,incest and danger to the life of the mother. This language ap-plied to the five targeted bills. In addition, the campaign gainedthe support and leadership of five female Senators who be-came spokespersons and leaders on this issue. The CARE cam-paign thus demonstrated the ability to engage members ofCongress on what were deemed ‘unpopular issues’ that pri-marily affected the poor.
The organising of women of colour helped to increase the vis-ibility of women of colour and their issues in the wider move-ment. It also helped to push the issue of abortion within thecontext of reproductive health and rights. This was successfulin mobilising the grassroots on non-popular issues and it proveda point to mainstream organisations that felt that advocacy

United States of America
309
which focused on the needs of low-income women and womenof colour was not a viable strategy. It proved that with the rightamount of attention, energy and resources the rights of allwomen could be upheld.
In 1999, the National Network of Abortion Funds initiatedC.A.R.E. 2000, the Campaign for Access and ReproductiveEquity. This campaign addresses the need to embed abortionrights in a larger, broader agenda and to broaden the focusand constituencies of the pro-choice movement. It is multi-issue and multi-dimensional in its strategies. The focus is onlow-incomewomen, women of colour, and young women.
The major strategies of C.A.R.E. 2000 include building broadcoalitions at the national and local levels; grassroots organis-ing for a broad, reproductive rights and health agenda in whichaccess is prominent; developing the leadership of the womenmost affected by the lack of access; building ongoing, workingrelationships between pro-choice groups and those workingon economic justice for women; opposing legislation at thenational and state levels which restricts access; and promotinglegislation which increases access.
In its first year the Campaign has built a foundation. It hascreated a national planning group, hired a full-time campaigndirector, developed a website and an organising manual andheld national and grassroots launching events. It is currentlymoving into the next phase in which it will initiate grassrootsactivities in eleven target states.
Lessons learned• Legalisation of abortion does not bring access to all
women. Socio-economic inequalities determine accessand quality of care both before and after legalisation.
• Advocacy efforts that emphasise securing formal, legalrights are likely to leave out those without the economicor political means to make these rights operational.
The Johannesburg Initiative
Advocating for abortion access
310
• If advocacy strategies do not take into account the race,class and gender dimensions of reproductive politics,there will be divisions in the movement, or lack of par-ticipation from certain constituencies.
• Women with the least power and resources bear the bruntof restricted abortion access under both conditions ofillegality and legality.
• Large numbers of women use abortion as a method offertility control regardless of its legal status or medicalsafety.
• The legal status of abortion in the US had a significantimpact on its medical safety. Dangers to women’s livesand health resulting from self-abortion and bad provid-ers are more likely under conditions of illegality.
• One impetus for legalisation and expanding abortionaccess has been from population control advocates.When feminists do not distance themselves from thesepolitics, abortion can be used as a tool of eugenics andracial divisions within advocacy movements are deep-ened.
• Change in policy came from political advocacy and fromchanges in the socio-economic conditions shaping wom-en’s lives.
• Advocacy strategies cannot be clearly separated from pro-viding a service or helping women. Both before and af-ter legalisation, advocates have had to engage in bothin order to provide access.
• Vigilance cannot end with legalisation. Advocacy effortsare needed to monitor and to secure implementation oflegal changes. Public support for abortion rights and therights themselves are fragile. Movements and organisa-tions must have the capacity to sustain these fluctuations.
• Significant advocacy strategies derive from grassroots ac-tivism.

United States of America
311
• Alliances of providers and activists are significant for ex-panding access, especially if training and providing serv-ices have not been institutionalised or mainstreamed.
• Multi-faceted strategies complement each other. Oftenadvocates do not see this and try to impose one strategyor tactic.
ReferencesAbortion Access Project (1999) ‘Hospital Access Project.’ http://www.abortionaccess.org
Alan Guttmacher Institute (2000) ‘Facts in Brief: InducedAbortion.’http://www.agi-usa.org.
Baehr N (1990) ‘Abortion Without Apology: Radical Historyfor the 1990s,’ Massachusetts: South End Press.
Frankfort E with Kissling F (1979) ‘Rosie: Investigation of AWrongful Death,’ New York: Dial Press.
Fried, M (2000) ‘Abortion in the united states: barriers to ac-cess’ in the Journal of Health and Human Rights, 4(1)184-187.
Luke, K (1984) ‘Abortion and the Politics of Motherhood,’ Cali-fornia: University of California Press.
Miller P (1993) ‘The Worst of Times,’ New York: Harper Collins.
Naral & Naral Foundation (2000) ‘Who Decides? A State-by-State Review of Abortion and Reproductive Rights.’ http://www.naral.org.
Petchesky R (1990) ‘Abortion and Woman’s Choice: The State,Sexuality, and Reproductive Freedom, Revised Edition,’ Mas-sachusetts: Northeastern University Press.
Reagan L (1997) ‘When Abortion Was a Crime: Women, Medi-cine, and Law in the United States,’ 1867-1973, California:University of California Press.
The Johannesburg Initiative
Advocating for abortion access
312
Roberts D (1997) ‘Killing the Black Body,’ New York: Pan-theon Books.
Ross L (1998) ‘African American women and abortion’ in RSolinger (ed) Abortion Wars: A Half Century of Struggle, 1950-2000, California: California Press.
Staggenborg S (1991) ‘The Pro-Choice Movement: Organiza-tion and Activism in the Abortion Conflict,’ Canada: OxfordUniversity Press.
Weddington S (1992) ‘A Question of Choice,’ New York: Pen-guin Putnam, Inc.
IntervieweesRene Almeling (Assistant Director, Access Initiative, NationalAbortion Federation); Euna August (Executive Director, Insti-tute for Women & Ethnic Studies); Toni Bond (Executive Di-rector, Chicago Abortion Fund); Susan Dudley (Deputy Di-rector, Access Initiative, National Abortion Federation), JuliaScott (President & Chief Executive Officer, National BlackWomen’s Health Project); Laureen Tews (Access Initiative Di-rector, Access Initiative, National Abortion Federation); LeslieWatson (Director, C.A.R.E. 2000 Campaign); Susan Yanow(Director, Abortion Access Project)
AuthorsShelia Clark is the Senior Programs & Policy Associate for theNational Black Women’s Health Project (NBWHP). She holdsa masters degree in social work and in her current position shefocuses on health policy, health disparities and organising grass-roots advocacy initiatives related to the health and well beingof African American women. She serves on the Advisory Com-mittee for the Black Church Initiative convened by the Reli-gious Coalition for Reproductive Rights and is a newly ap-pointed board member of the Reproductive Health Technolo-gies Project.

United States of America
313
Marlene Gerber Fried is Director of the Civil Liberties and PublicPolicy Program at Hampshire College, where she is also Pro-fessor of Philosophy. She is a long-time activist in the repro-ductive rights movement and is currently president of the Na-tional Network of Abortion Funds and serves on the boards ofthe Abortion Access Project, the Abortion Rights Fund of West-ern Massachusetts, the Eastern Massachusetts Abortion Fund,the Committee on Women, Population and the Environmentand the Pro Choice Resource Center. She is editor of FromAbortion to Reproductive Freedom: Transforming A Movement,1990, South End Press.
![Aidos Kuneen1 Introduction Bitcoin, the once obscure cryptocurrency introduced by Satoshi Nakamoto [1] in 2008, has now begun to draw much wider attention from both the general public](https://img.pdfslide.us/doc/110x75/600e0a7a852dcd0f501f973d/aidos-kuneen-1-introduction-bitcoin-the-once-obscure-cryptocurrency-introduced.jpg)