Embed Size (px)
Citation preview
RichardS.Beaser,MDMedicalDirector,ProfessionalEducation
JoslinDiabetesCenterAssociateProfessorofMedicine
HarvardMedicalSchool
AdvancingtoInsulinReplacementTherapy:When,Why,andHow?
Update in Internal Medicine - 2016December 5, 2016
COPYRIG
HT

KeyMessages– InsulinTherapy• Insulinisahighlyeffectivediabetestreatment• Individualizetreatmentgoalsandregimens
– Considerpathophysiology,self-care,andsafety• Usepatternassessmenttoadjustdosingandadvance
therapy• TotreatType2Diabetes,considertheadvancement
sequencerecommendedbynationally-recognizedguidelinesfrombasalalonetobasal-bolusinsulintherapy
• Recognizeandaddresspatient,provider,andpractice-levelbarrierstoinsulintherapy
• Sometreatmentservicesshouldbeprovidedinthepractice,othersobtainedbyconsultation
COPYRIG
HT
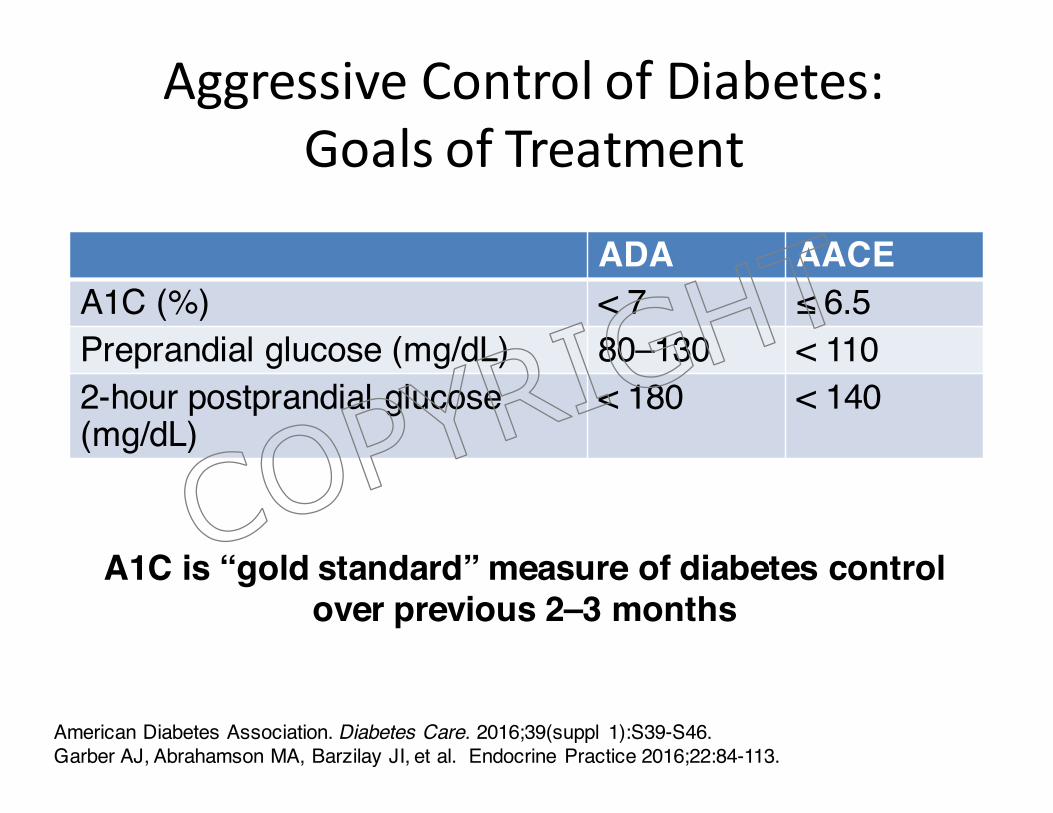
American Diabetes Association. Diabetes Care. 2016;39(suppl 1):S39-S46. Garber AJ, Abrahamson MA, Barzilay JI, et al. Endocrine Practice 2016;22:84-113.
A1C is “gold standard” measure of diabetes control over previous 2–3 months
AggressiveControlofDiabetes:GoalsofTreatment
ADA AACEA1C (%) < 7 ≤ 6.5Preprandial glucose (mg/dL) 80–130 < 1102-hour postprandial glucose (mg/dL)
< 180 < 140
COPYRIG
HT
KeyParametersReflectingGlycemicControl
• A1C
• Preprandialglucoselevels
• Fasting
• Sequentiallythroughtheday
• Postprandialglucoselevels
• Absolutelevel
• Levelrelativetopre-prandial
COPYRIG
HT
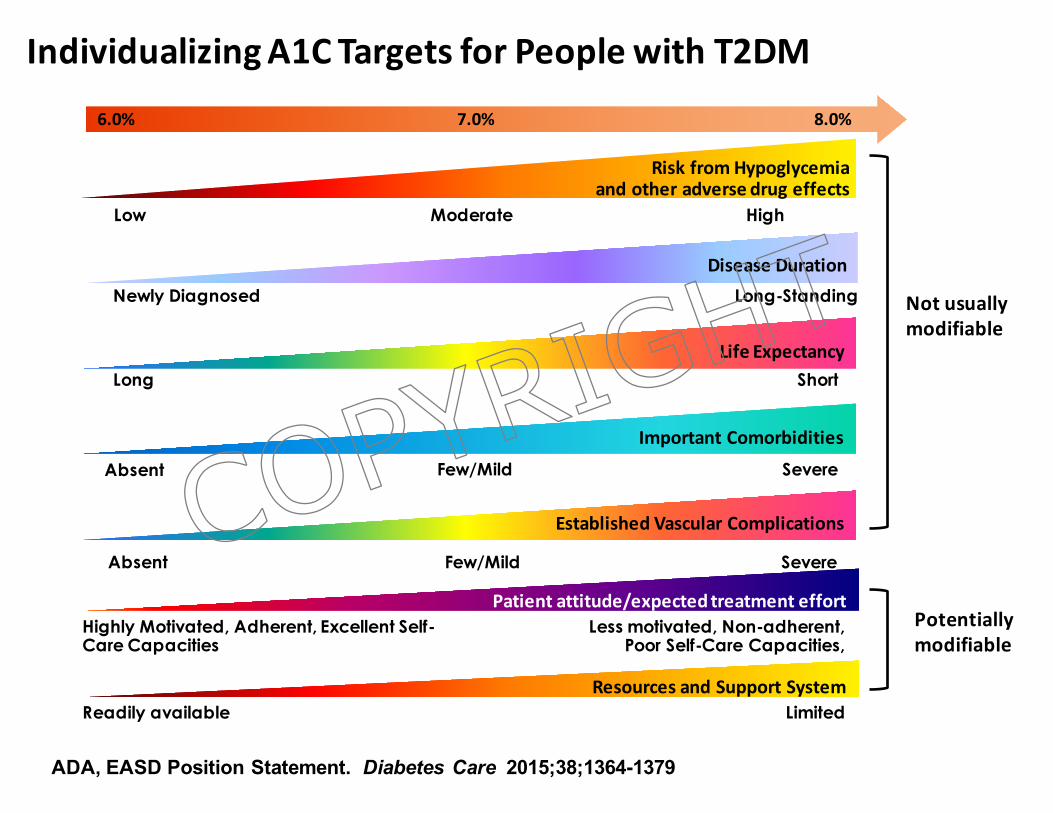
IndividualizingA1CTargetsforPeoplewithT2DM
ADA, EASD Position Statement. Diabetes Care 2015;38;1364-1379
Most Intensive Less Intensive Least Intensive
LifeExpectancy
DiseaseDuration
ImportantComorbiditiesFew/Mild Severe
RiskfromHypoglycemiaandotheradversedrugeffects
Low HighModerate
8.0%6.0% 7.0%
EstablishedVascularComplications
Few/Mild SevereAbsent
Long Short
Absent
Newly Diagnosed Long-Standing Notusuallymodifiable
Patientattitude/expectedtreatmenteffortHighly Motivated, Adherent, Excellent Self-Care Capacities
Less motivated, Non-adherent, Poor Self-Care Capacities,
ResourcesandSupportSystemReadily available Limited
Potentiallymodifiable
COPYRIG
HT
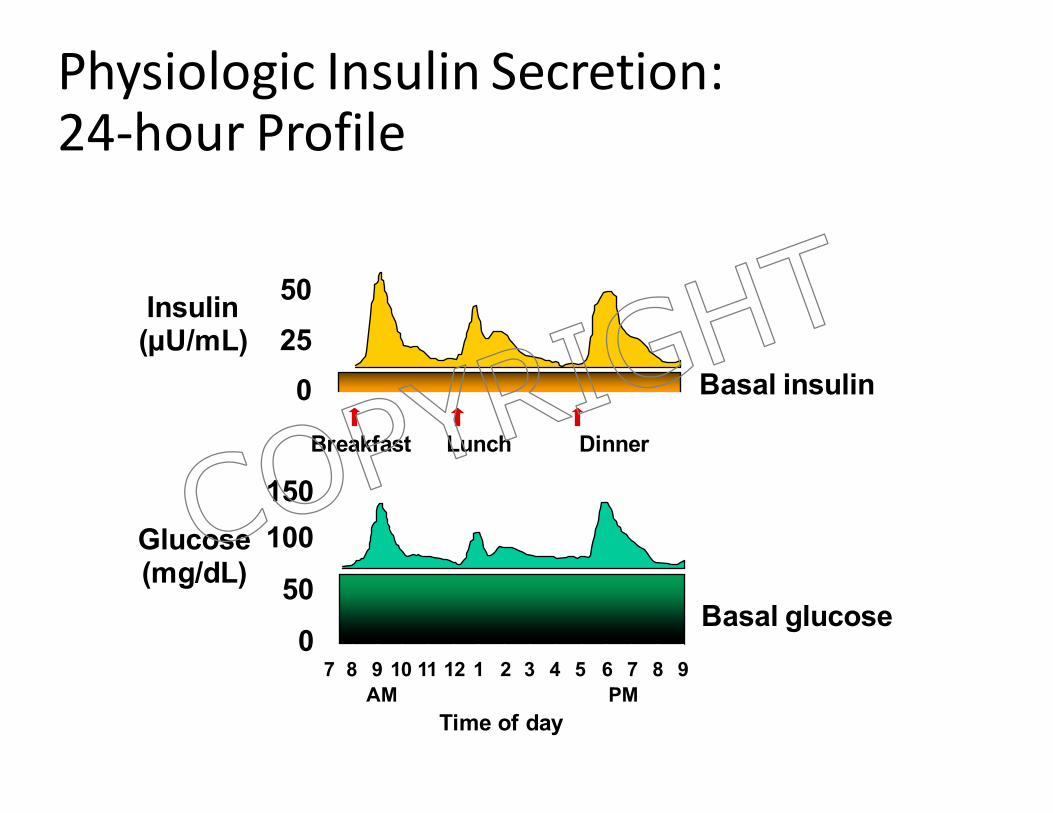
PhysiologicInsulinSecretion:24-hourProfile
Insulin(µU/mL)
50250 Basal insulin
Breakfast Lunch Dinner
150
Time of day
Glucose(mg/dL)
100500
7 8 9 10 11 12 1 2 3 4 5 6 7 8 9AM PM
Basal glucose
COPYRIG
HT
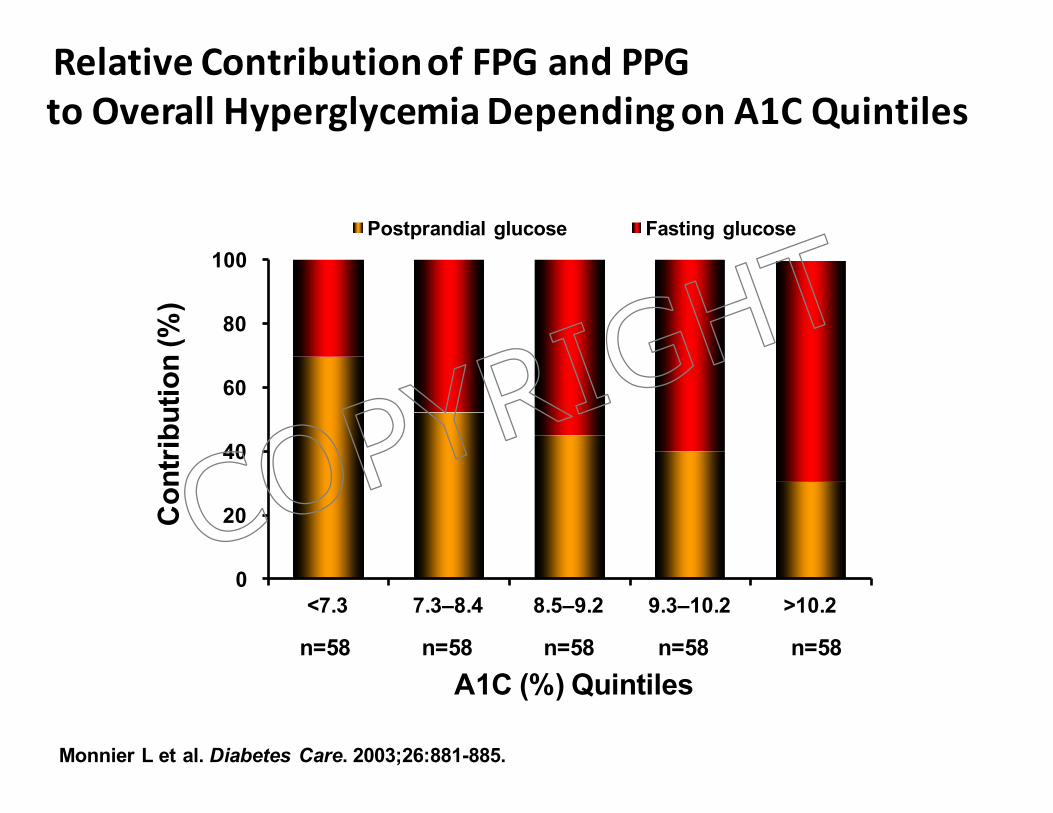
RelativeContributionofFPGandPPGtoOverallHyperglycemiaDependingonA1CQuintiles
Monnier L et al. Diabetes Care. 2003;26:881-885.
n=58 n=58 n=58 n=58n=58
0
20
40
60
80
100
<7.3 7.3–8.4 8.5–9.2 9.3–10.2 >10.2
Postprandial glucose Fasting glucose
Con
trib
utio
n (%
)
A1C (%) Quintiles
COPYRIG
HT
WhentoConsiderInsulininapersonwithType2Diabetes
• Whenacombinationofnon-insulinantidiabetesmedicationsareunabletoachieveA1Ctarget
• Highfastingorpostprandialglycemia
• Unacceptablesideeffectsofothermedications
• Advancedhepaticorrenaldisease
• Specialconsiderations(steroids,infection,pregnancy)
• Hyperglycemiainahospitalizedpatient
• “Severely”uncontrolleddiabetes*
Nathan DM, et al. Diabetes Care. 2009; volume 32,193-203. Inzucchi SE, et al. Diabetes Care.2012;35(6):1364-1379. ADA Diabetes Care. 2015:38(Suppl 1):S41-S48.
* Random Glucose > 300 mg/dL, A1C > 10%, Ketonuria, Symptomatic polyuria/polydipsia, weight loss
COPYRIG
HT
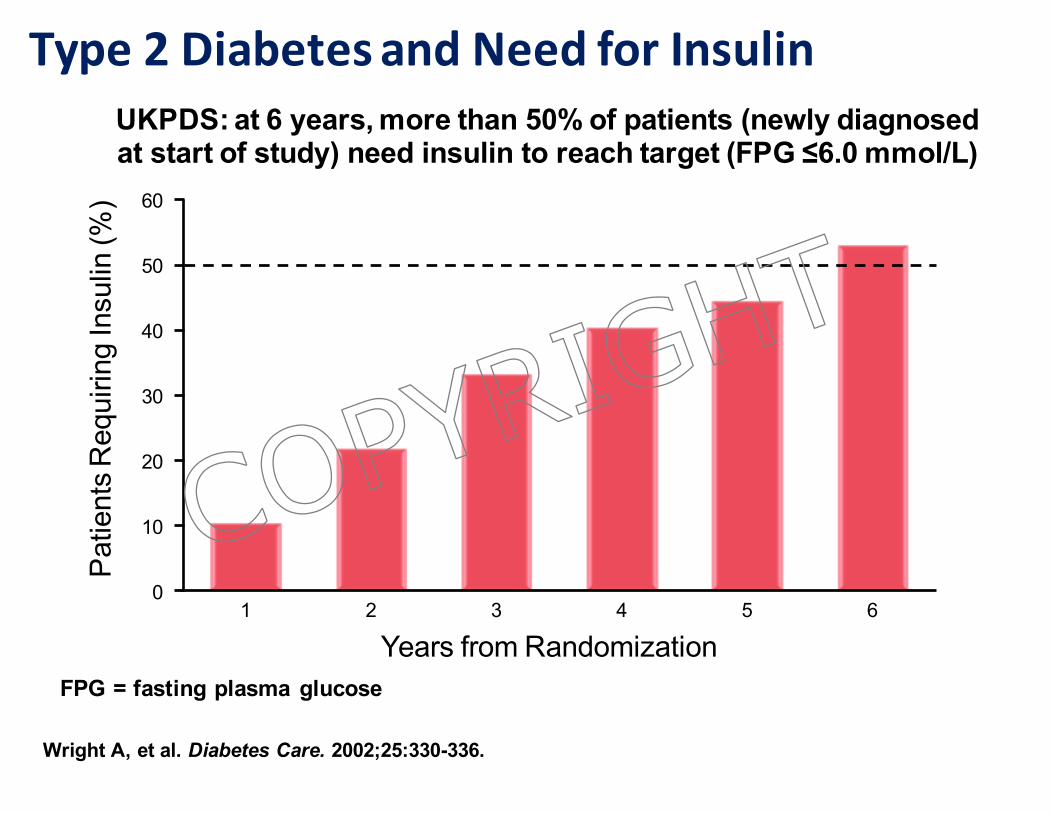
Type2DiabetesandNeedforInsulinP
atie
nts
Req
uirin
g In
sulin
(%)
UKPDS: at 6 years, more than 50% of patients (newly diagnosed at start of study) need insulin to reach target (FPG ≤6.0 mmol/L)
20
40
60
0
10
30
50
1 2 3 4 5 6
Wright A, et al. Diabetes Care. 2002;25:330-336.
FPG = fasting plasma glucoseYears from Randomization
COPYRIG
HT
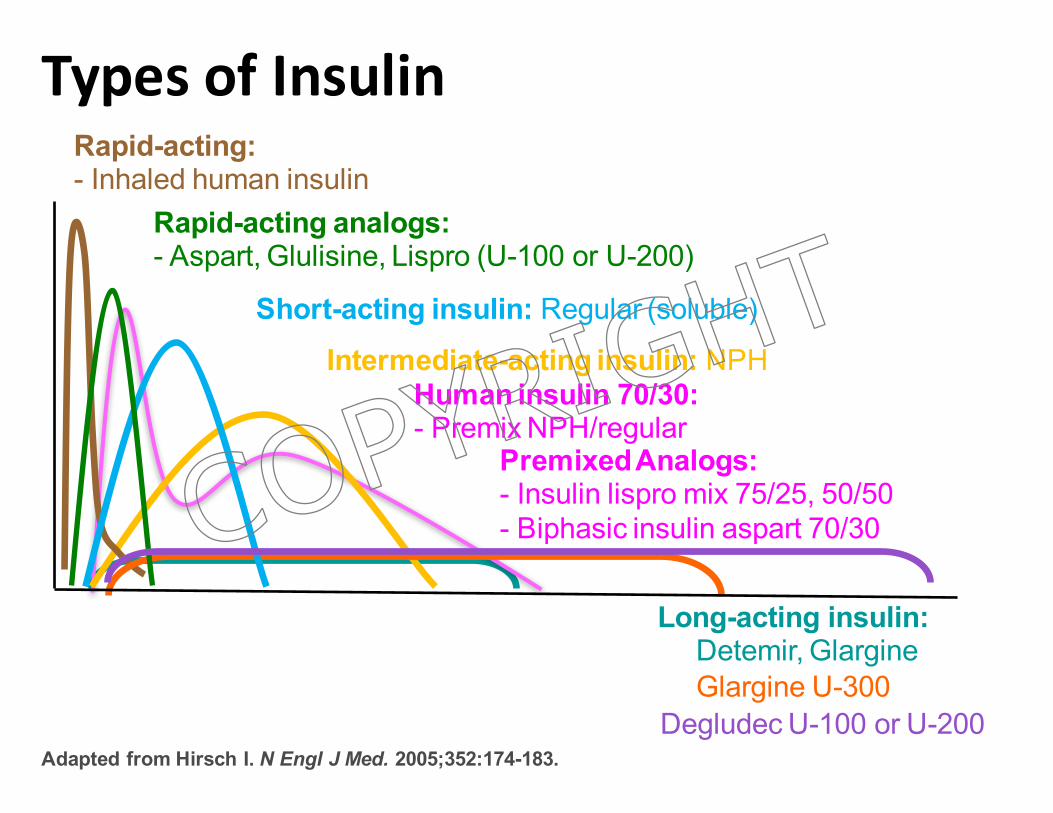
TypesofInsulin
Time (hours)4 8 16 24
Premixed Analogs:- Insulin lispro mix 75/25, 50/50- Biphasic insulin aspart 70/30
Human insulin 70/30: - Premix NPH/regular
Intermediate-acting insulin: NPH
Long-acting insulin:- Detemir, Glargine
Rapid-acting analogs:- Aspart, Glulisine, Lispro (U-100 or U-200)
Short-acting insulin: Regular (soluble)
Rapid-acting:- Inhaled human insulin
Adapted from Hirsch I. N Engl J Med. 2005;352:174-183.
- Glargine U-300- Degludec U-100 or U-200
COPYRIG
HT
Insulin to provide Basal and Bolus Coverage
§ Basal insulin• Replicates normal “basal” insulin secretion in the fasting
and postabsorptive state which regulates hepatic glucose production and limits lipolysis
• Controls fasting and premeal glucose levels• A good basal insulin should have a low risk of
hypoglycemia§ Bolus insulin
• Replicates acute insulin secretion at mealtimes to both suppress liver glucose production and increase uptake of glucose in peripheral tissues
• Blunts rise in glucose after meals
COPYRIG
HT
13
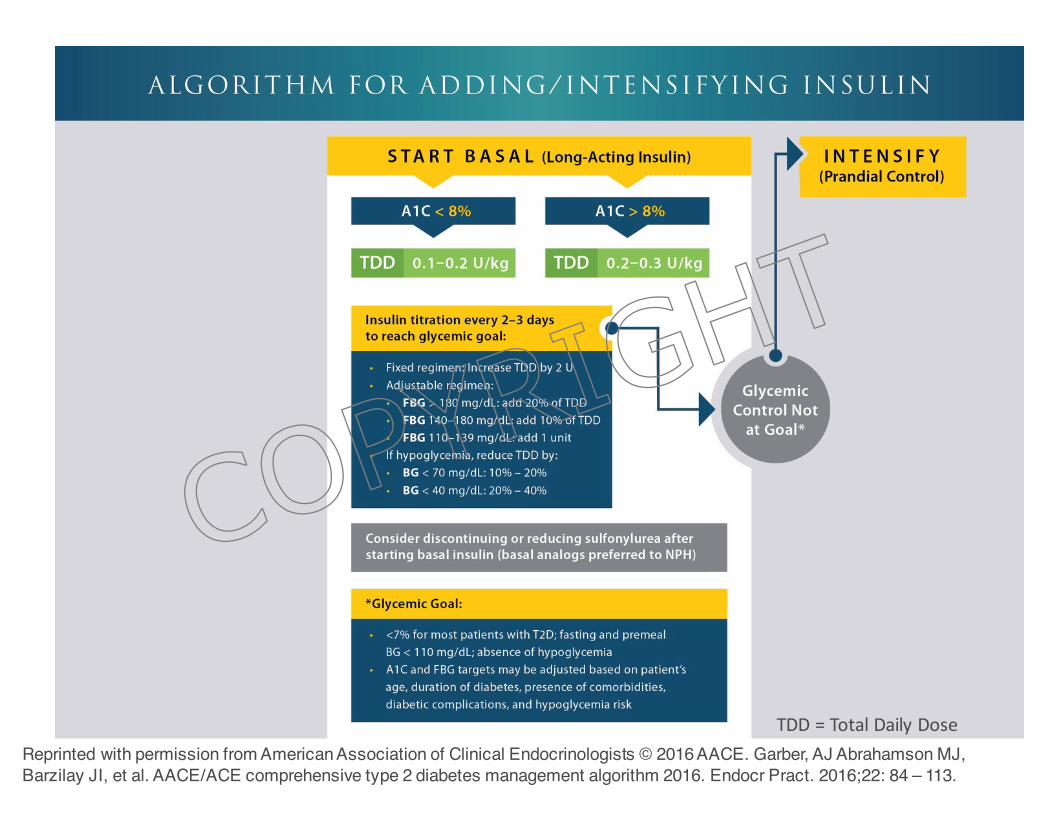
TDD=TotalDailyDose
Reprinted with permission from American Association of Clinical Endocrinologists © 2016 AACE. Garber, AJ Abrahamson MJ, Barzilay JI, et al. AACE/ACE comprehensive type 2 diabetes management algorithm 2016. Endocr Pract. 2016;22: 84 – 113.
COPYRIG
HT
DesiredCharacteristicsofReplacementBasalInsulin
• Mimicsnaturalpancreaticbasalinsulinsecretorypattern
• Nodistinctpeakeffect
• Continuedeffectover24hours
• Minimizesriskofnocturnalhypoglycemia
• Administeredoncedailyforoptimalpatientadherence
• Reliableabsorptionpattern
COPYRIG
HT
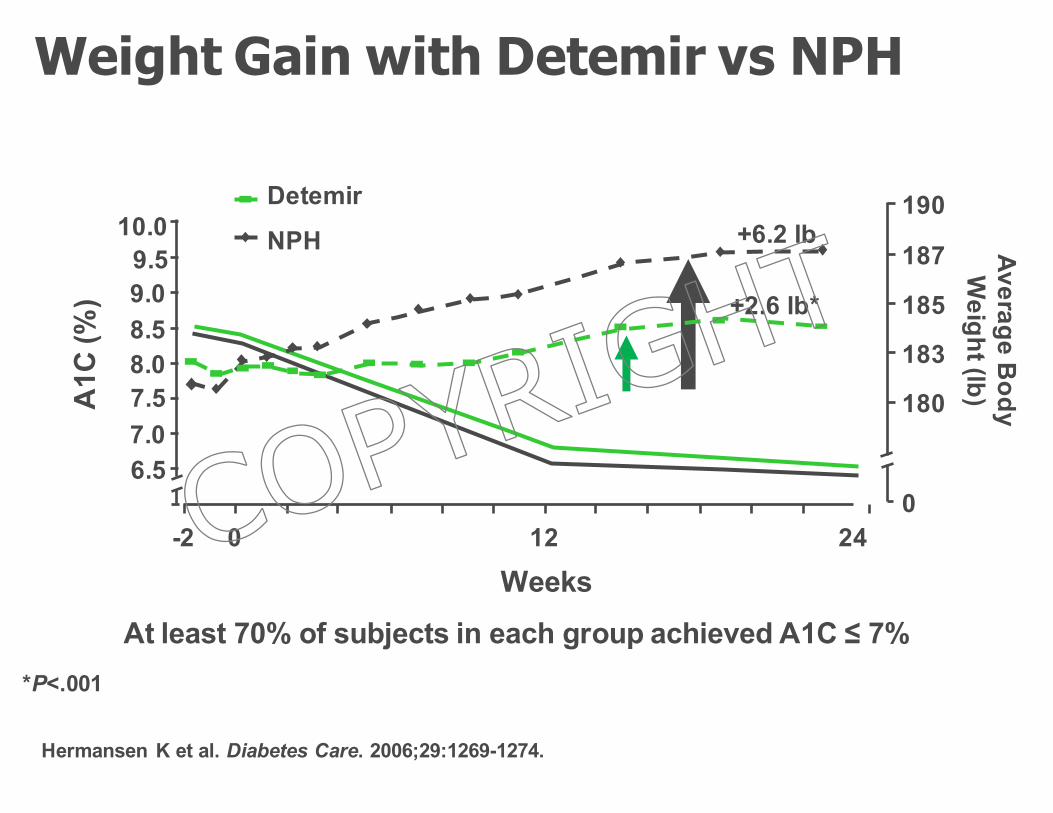
At least 70% of subjects in each group achieved A1C ≤ 7%Weeks
-2 0 12 24
6.57.07.58.08.59.09.5
10.0
A1C
(%)
+6.2 lb
+2.6 lb*
0
180
183
185
187
190
Average Body
Weight (lb)
Detemir NPH
*P<.001
Hermansen K et al. Diabetes Care. 2006;29:1269-1274.
Weight Gain with Detemir vs NPH
COPYRIG
HT
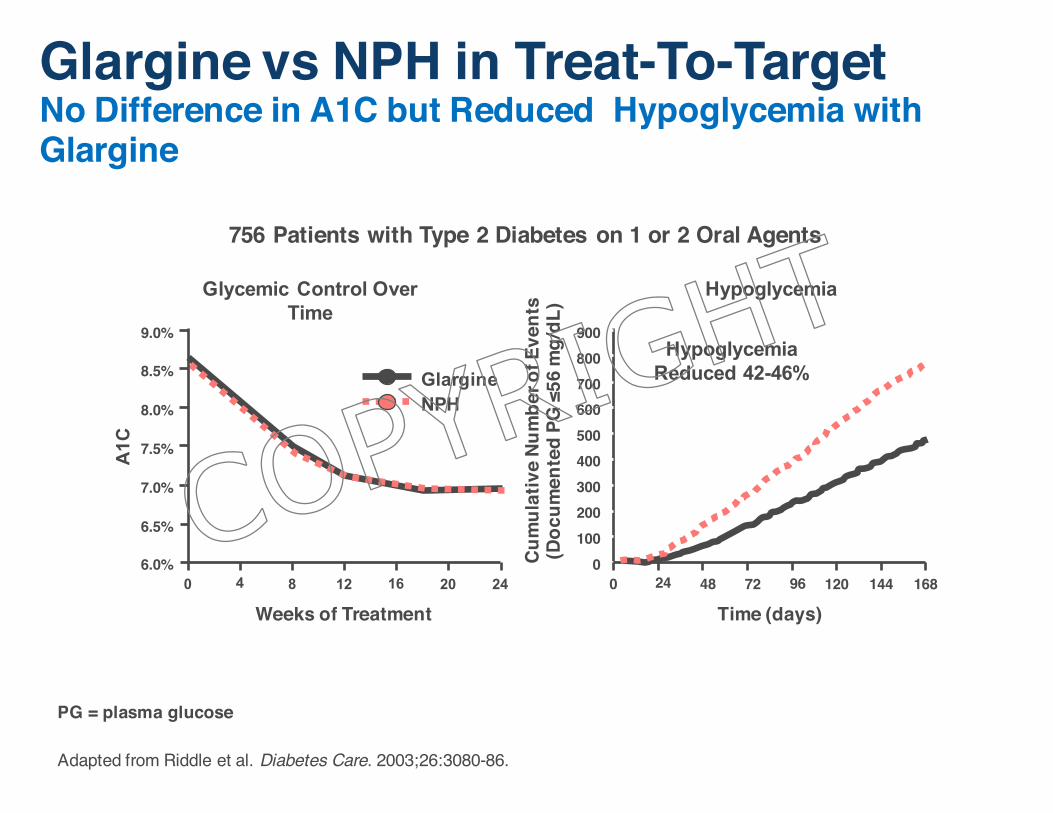
756 Patients with Type 2 Diabetes on 1 or 2 Oral Agents
PG = plasma glucose
Adapted from Riddle et al. Diabetes Care. 2003;26:3080-86.
NPHGlargine
9.0%
8.5%
8.0%
7.5%
7.0%
6.5%
6.0%
A1C
0 4 8 12 16 20 24
Cum
ulat
ive
Num
ber o
f Eve
nts
(Doc
umen
ted
PG ≤
56 m
g/dL
)
Weeks of Treatment Time (days)
900800
600500
300
1000
700
400
200
0 24 48 72 96 120 168144
Glycemic Control Over Time
Hypoglycemia
Glargine vs NPH in Treat-To-TargetNo Difference in A1C but Reduced Hypoglycemia with Glargine
Hypoglycemia Reduced 42-46%
COPYRIG
HT
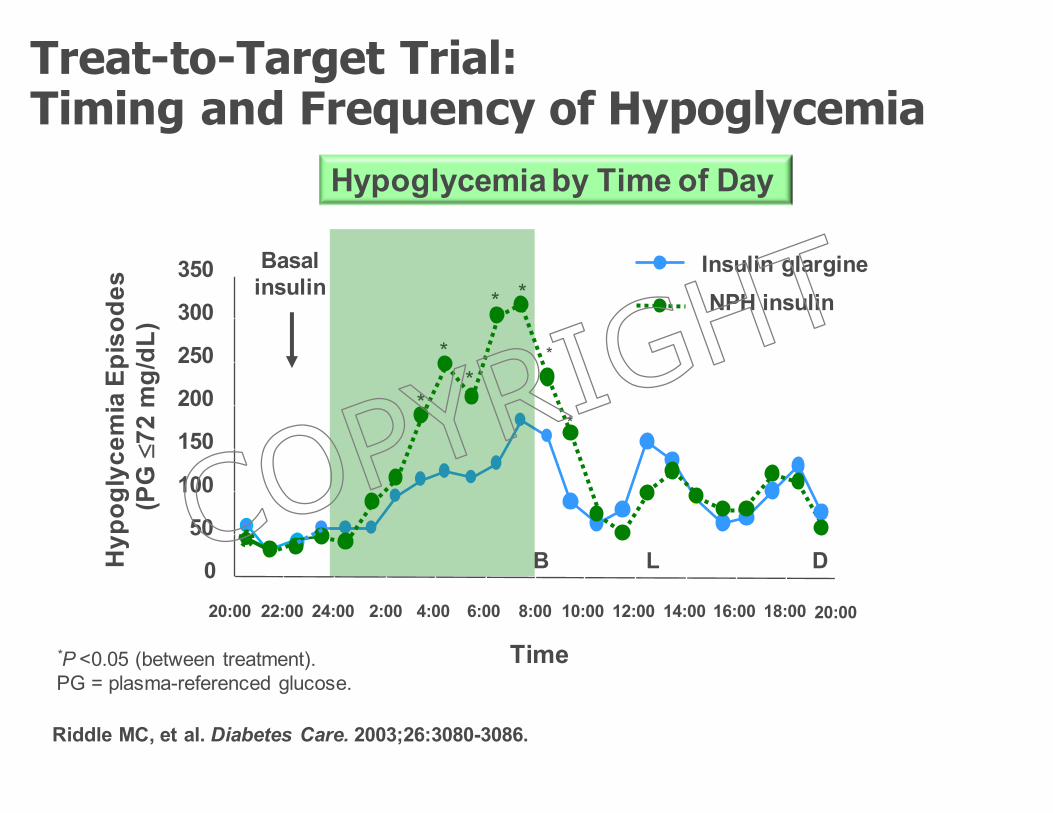
Insulin glargineNPH insulin
0
50
100
150
200
250
300
350
20:00 22:00 24:00 2:00 4:00 6:00 8:00 10:00 12:00 14:00 16:00 18:00
Time
B L D
Basal insulin
20:00
Hypoglycemia by Time of Day
Hyp
ogly
cem
ia E
piso
des
(PG
£72
mg/
dL)
Riddle MC, et al. Diabetes Care. 2003;26:3080-3086.
*P <0.05 (between treatment).PG = plasma-referenced glucose.
*
**
**
*
*
Treat-to-Target Trial: Timing and Frequency of Hypoglycemia
COPYRIG
HT
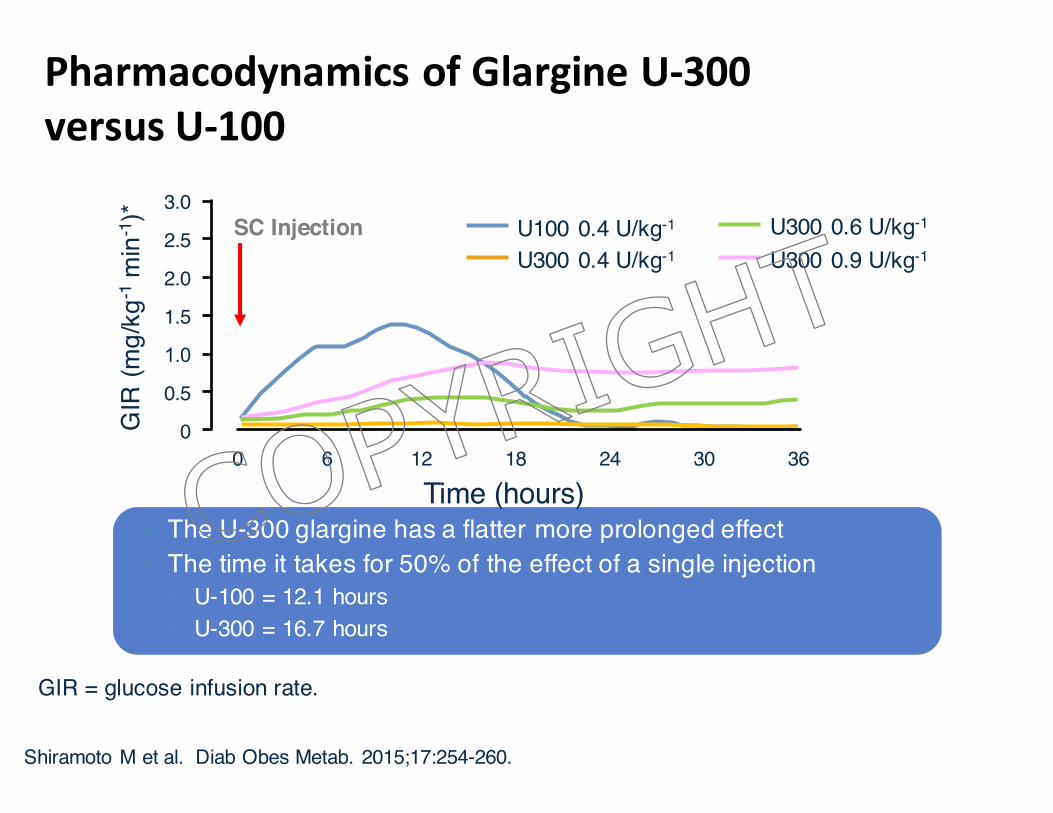
PharmacodynamicsofGlargineU-300versusU-100
GIR
(mg/
kg-1
min
-1)*
1.5
3.0
00 36
Time (hours)3024126 18
0.5
2.5 U100 0.4 U/kg-1
U300 0.4 U/kg-12.0
1.0
U300 0.6 U/kg-1
U300 0.9 U/kg-1SC Injection
• The U-300 glargine has a flatter more prolonged effect • The time it takes for 50% of the effect of a single injection
• U-100 = 12.1 hours• U-300 = 16.7 hours
GIR = glucose infusion rate.
Shiramoto M et al. Diab Obes Metab. 2015;17:254-260.
COPYRIG
HT
U-300InsulinGlargine
• U-300insulinglargineoffersasmallerdepotsurfacearealeadingtoareducedrateofabsorption
• Providesaflatterandprolongedpharmacokineticandpharmacodynamic profilesandmoreconsistency
• Half-lifeis~23hours
• Associatedwithlesshypoglycemiaespeciallynocturnalhypoglycemia
• Onlyavailableinpens– 300U/mL,1.5mL– Maxdosepershotis80unitswithcurrentpen
Garber AJ. Diabetes Obesity Metab 2014;16:483-491. Owens DR, et al. Diabetes Metab Res Rev. 2014;30(2):104-19. Steinstraesser A, et al. Diabetes Obes Metab. 2014;16:873-876. http://www.australianprescriber.com/magazine/19/3/76/8. Accessed September 4, 2015
COPYRIG
HT
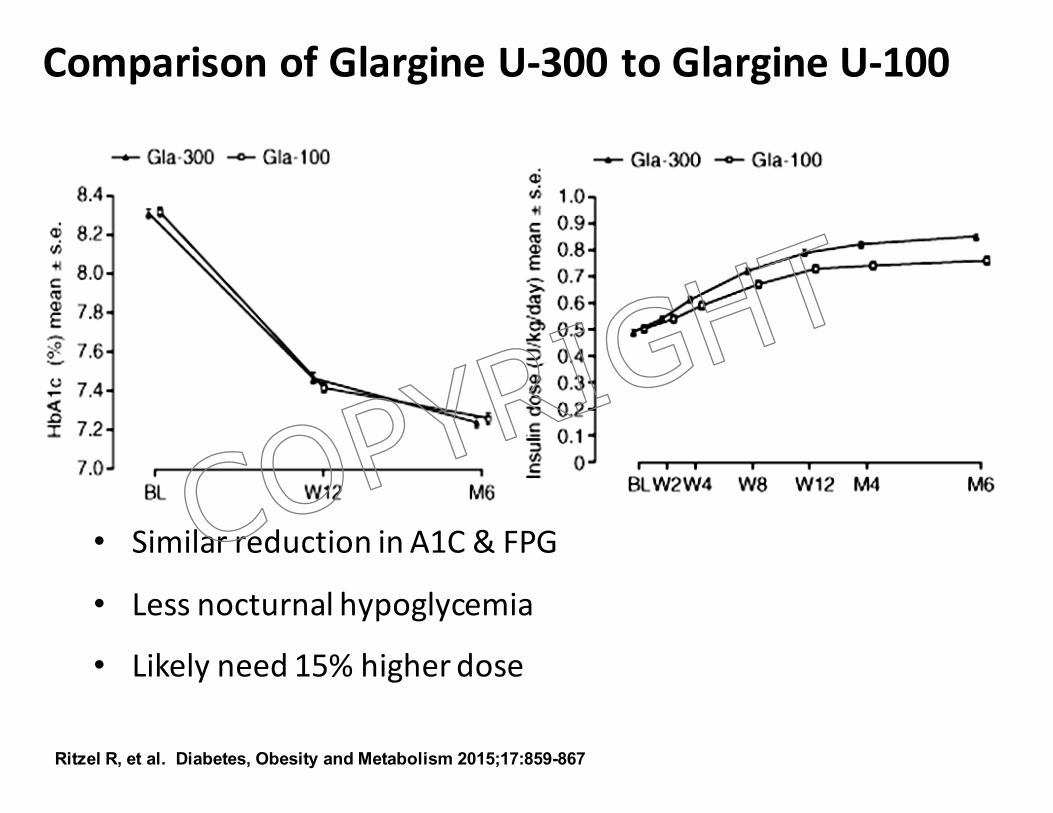
ComparisonofGlargineU-300toGlargineU-100
• SimilarreductioninA1C&FPG
• Lessnocturnalhypoglycemia
• Likelyneed15%higherdose
Ritzel R, et al. Diabetes, Obesity and Metabolism 2015;17:859-867
COPYRIG
HT
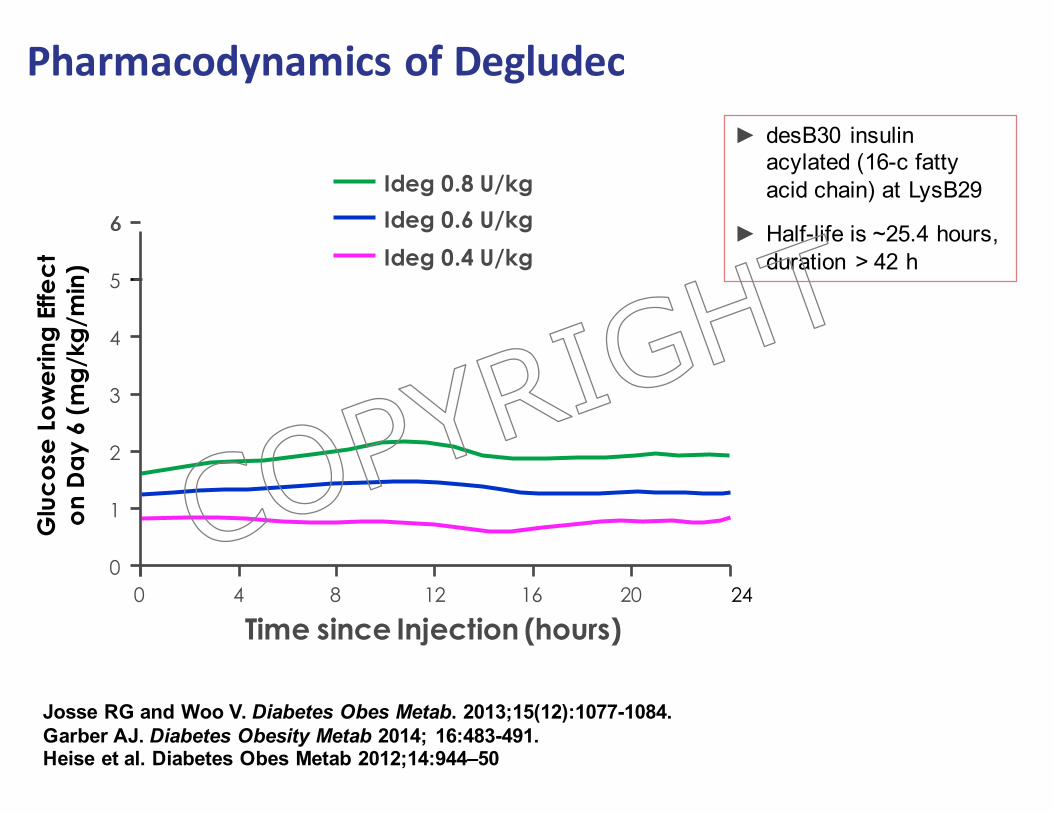
PharmacodynamicsofDegludec
Josse RG and Woo V. Diabetes Obes Metab. 2013;15(12):1077-1084. Garber AJ. Diabetes Obesity Metab 2014; 16:483-491. Heise et al. Diabetes Obes Metab 2012;14:944–50
Glu
cose
Low
erin
g Ef
fect
on D
ay 6
(mg/
kg/m
in)
2
6
00 24
Time since Injection (hours)201684 12
4
1
3
5Ideg 0.4 U/kg
Ideg 0.8 U/kgIdeg 0.6 U/kg6
► desB30 insulin acylated (16-c fatty acid chain) at LysB29
► Half-life is ~25.4 hours, duration > 42 h
COPYRIG
HT

VariabilityofEffectVariabilityineffectsofaninsulincancauseunexplainablevariationsinglucosecontrol
fromdaytoday
Insulin Within Subject Variability(CV% of AUC GIR)
NPH 68Glargine U-100 48 – 99Detemir 27Glargine U-300 34.8Degludec 20
Adapted from: Rossetti P, et al. Diabetes Obes Metab, 2014;16:695-706; Becker RHA, et al. Diabetes ObesMetab, 2015;17:261-7
COPYRIG
HT
§ Basal plus GLP-1 agonistOR
§ Switch to a premixed insulin analog– Divide dose in half and give twice daily (before
breakfast and dinner)§ OR§ Basal Plus
– Basal insulin plus a short-acting insulin analogue before the largest meal of the day
OR§ Switch to basal-bolus regimen
InsulinTitration:Optionswhencontrolisnotadequateusingonedailyinjectionofbasalinsulin
23
COPYRIG
HT
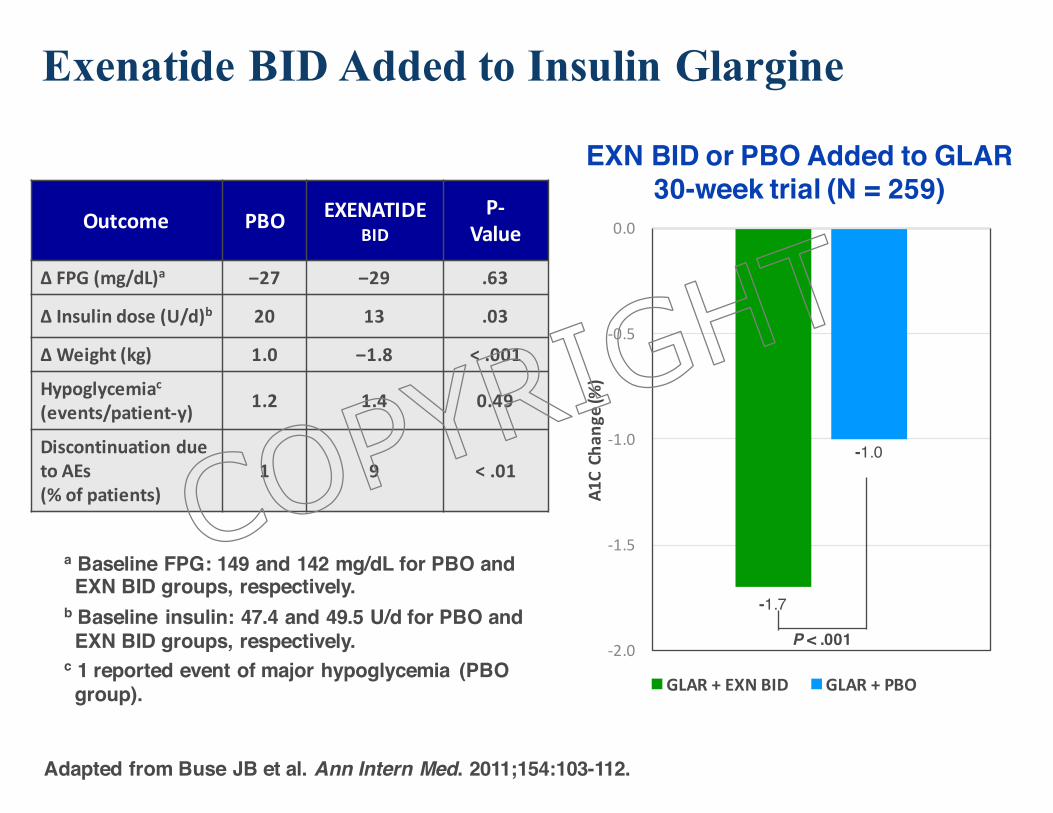
‒1.7
‒1.0
-2.0
-1.5
-1.0
-0.5
0.0
A1CCh
ange(%
)
GLAR+EXNBID GLAR+PBO
Outcome PBO EXENATIDEBID
P-Value
Δ FPG(mg/dL)a ‒27 ‒29 .63
Δ Insulindose(U/d)b 20 13 .03
Δ Weight (kg) 1.0 ‒1.8 <.001
Hypoglycemiac(events/patient-y) 1.2 1.4 0.49
DiscontinuationduetoAEs(%ofpatients)
1 9 <.01
Adapted from Buse JB et al. Ann Intern Med. 2011;154:103-112.
P < .001
EXN BID or PBO Added to GLAR30-week trial (N = 259)
Exenatide BID Added to Insulin Glargine
24
a Baseline FPG: 149 and 142 mg/dL for PBO and EXN BID groups, respectively.
b Baseline insulin: 47.4 and 49.5 U/d for PBO and EXN BID groups, respectively.
c 1 reported event of major hypoglycemia (PBO group).
COPYRIG
HT
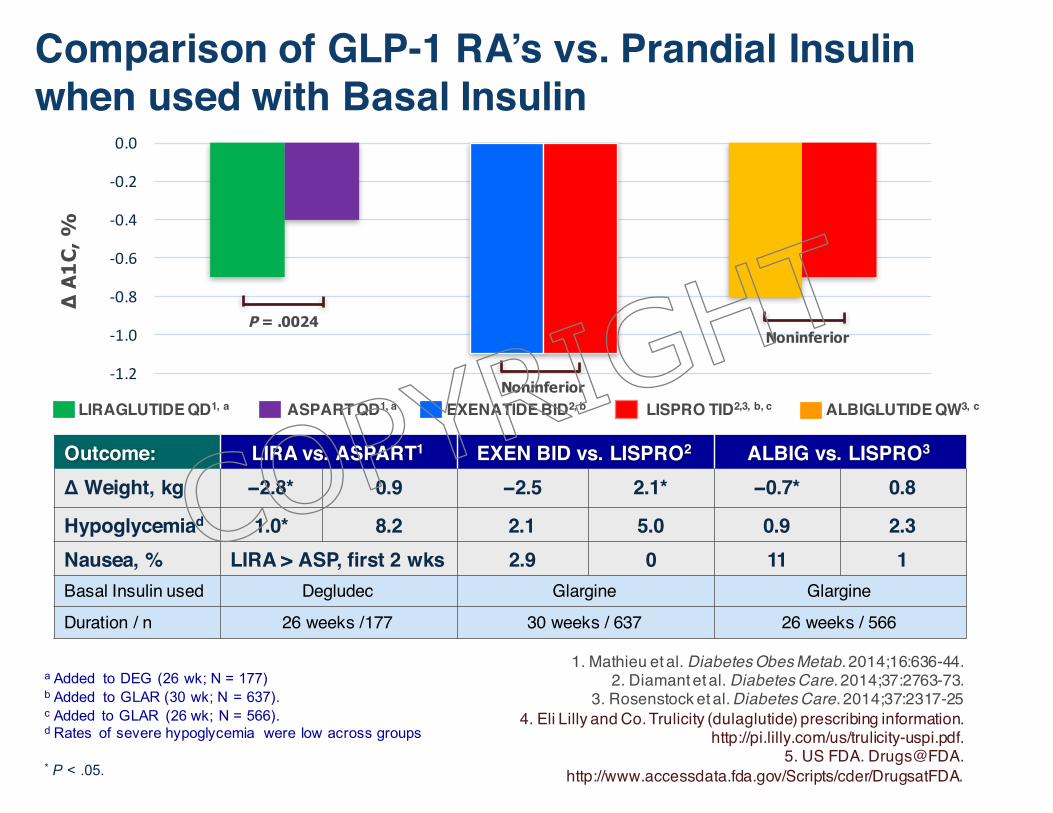
Comparison of GLP-1 RA’s vs. Prandial Insulin when used with Basal Insulin
1. Mathieu et al. Diabetes Obes Metab. 2014;16:636-44.2. Diamant et al. Diabetes Care. 2014;37:2763-73.
3. Rosenstock et al. Diabetes Care. 2014;37:2317-254. Eli Lilly and Co. Trulicity (dulaglutide) prescribing information.
http://pi.lilly.com/us/trulicity-uspi.pdf.5. US FDA. Drugs@FDA.
http://www.accessdata.fda.gov/Scripts/cder/DrugsatFDA.
Outcome: LIRA vs. ASPART1 EXEN BID vs. LISPRO2 ALBIG vs. LISPRO3
Δ Weight, kg −2.8* 0.9 −2.5 2.1* −0.7* 0.8
Hypoglycemiad 1.0* 8.2 2.1 5.0 0.9 2.3Nausea, % LIRA > ASP, first 2 wks 2.9 0 11 1Basal Insulin used Degludec Glargine GlargineDuration / n 26 weeks /177 30 weeks / 637 26 weeks / 566
-1.2
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
EXENATIDE BID2, bLIRAGLUTIDE QD1, a ALBIGLUTIDE QW3, cASPART QD1, a LISPRO TID2,3, b, c
∆ A
1C, %
P = .0024
Noninferior
Noninferior
a Added to DEG (26 wk; N = 177)b Added to GLAR (30 wk; N = 637). c Added to GLAR (26 wk; N = 566).d Rates of severe hypoglycemia were low across groups
* P < .05.
COPYRIG
HT
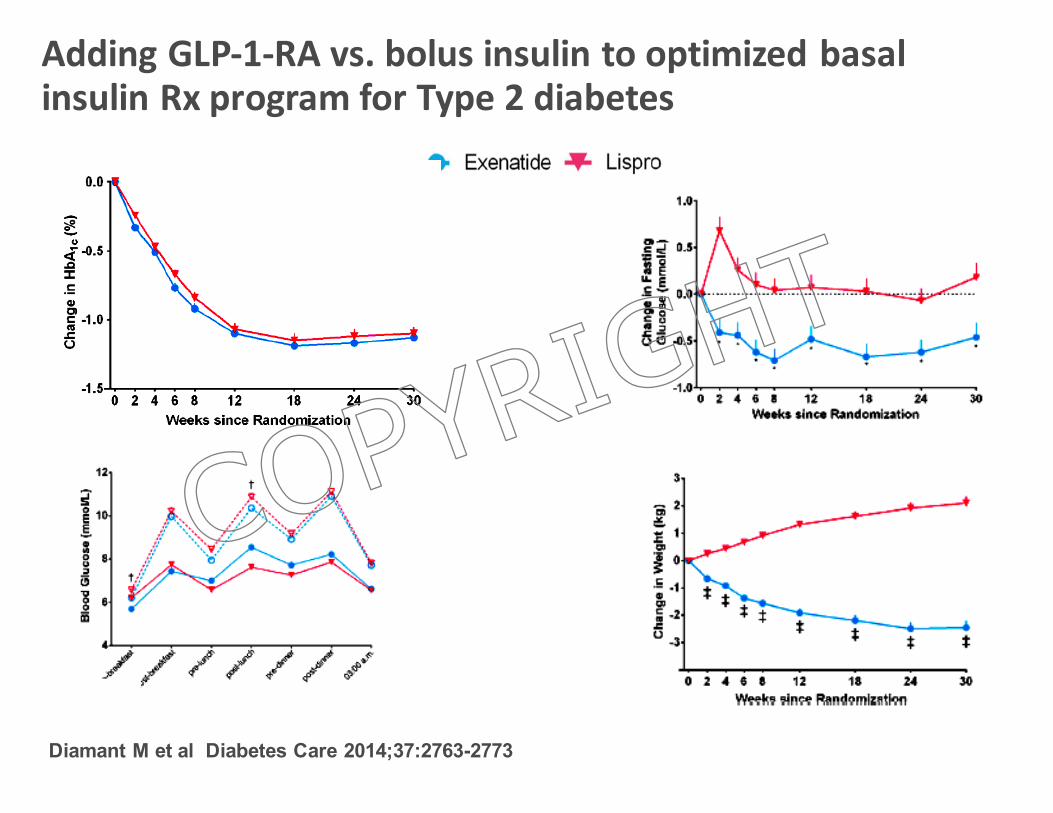
AddingGLP-1-RAvs.bolusinsulintooptimizedbasalinsulinRxprogramforType2diabetes
Diamant M et al Diabetes Care 2014;37:2763-2773
COPYRIG
HT
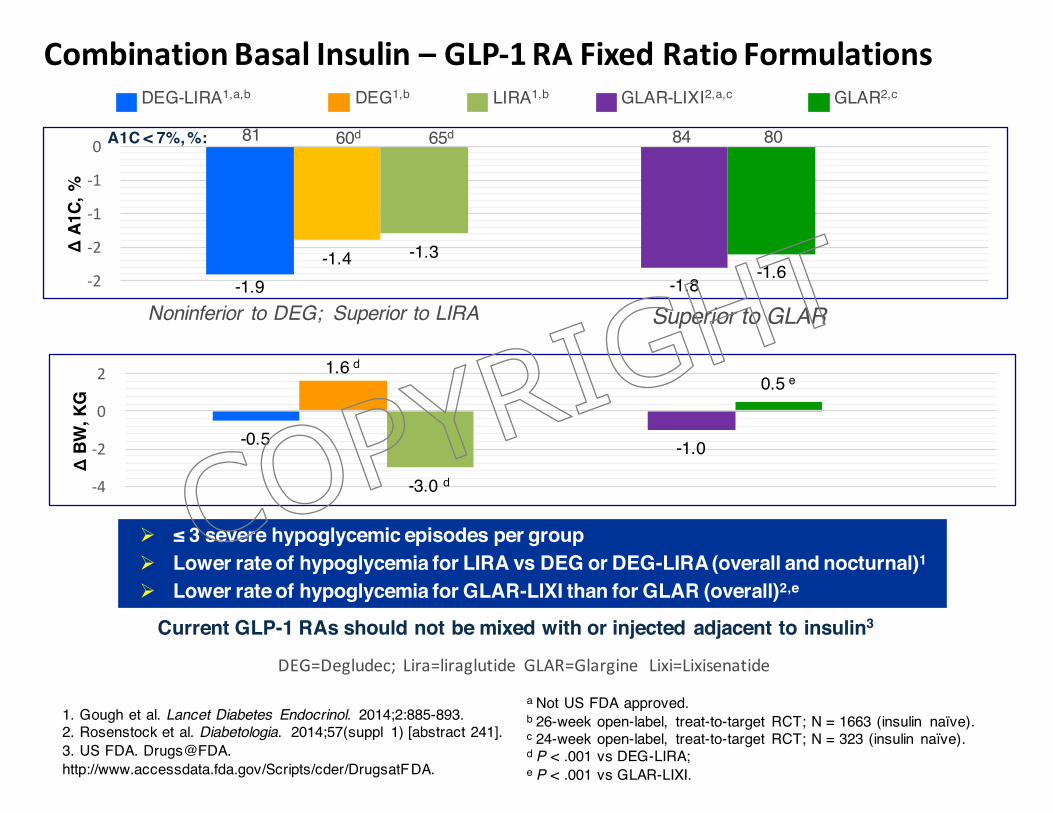
CombinationBasalInsulin– GLP-1RAFixedRatioFormulations
-1.9 -1.8-1.4
-1.6-1.3
-2
-2
-1
-1
0
Δ A
1C, %
-0.5 -1.0
1.6 d0.5 e
-3.0 d-4
-2
0
2
Δ B
W, K
G
a Not US FDA approved.b 26-week open-label, treat-to-target RCT; N = 1663 (insulin naïve). c 24-week open-label, treat-to-target RCT; N = 323 (insulin naïve). d P < .001 vs DEG-LIRA;e P < .001 vs GLAR-LIXI.
1. Gough et al. Lancet Diabetes Endocrinol. 2014;2:885-893.2. Rosenstock et al. Diabetologia. 2014;57(suppl 1) [abstract 241].3. US FDA. Drugs@FDA. http://www.accessdata.fda.gov/Scripts/cder/DrugsatFDA.
Current GLP-1 RAs should not be mixed with or injected adjacent to insulin3
LIRA1,bDEG-LIRA1,a,b GLAR2,cDEG1,b GLAR-LIXI2,a,c
Ø ≤ 3 severe hypoglycemic episodes per groupØ Lower rate of hypoglycemia for LIRA vs DEG or DEG-LIRA (overall and nocturnal)1
Ø Lower rate of hypoglycemia for GLAR-LIXI than for GLAR (overall)2,e
Noninferior to DEG; Superior to LIRA
d
Superior to GLAR
A1C < 7%, %: 81 60d 65d 84 80
DEG=Degludec;Lira=liraglutideGLAR=GlargineLixi=Lixisenatide
COPYRIG
HT
RoleforPremixedInsulin• Advantages
– Easy(nomixing,singleproduct,pensavail.)– Coversinsulinrequirementsthroughmostofday
• Disadvantages– Notphysiologic
– LessFlexible:requiresconsistentmeal/exercisepattern,andcannottitrateindividualinsulinsunlesscustommixedinsulinisused
– ↑Nocturnalhypoglycemia(presupperNPH)
– ↑Fastinghyperglycemia(presupperNPHwearsoff)
– HigherA1C(realisticgoalof≤8%)
Janka HU et al. Diabetes Care. 2005;28:254-259. Fritsche et al. Diab Obes Metab. 2010;12(2):115-123. ADA, EASD Position Statement. Diabetes Care 2012;35;1364-1379.
COPYRIG
HT
29
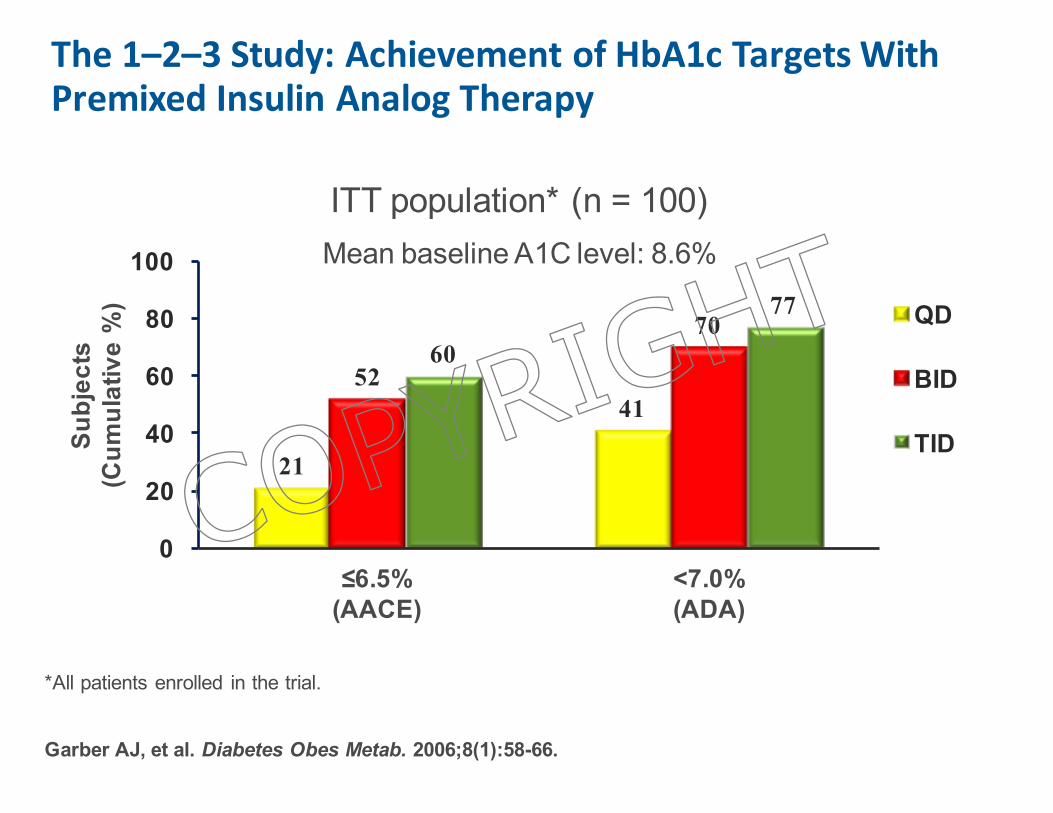
The1–2–3Study:AchievementofHbA1cTargetsWithPremixedInsulinAnalogTherapy
Garber AJ, et al. Diabetes Obes Metab. 2006;8(1):58-66.
Subj
ects
(C
umul
ativ
e %
)
ITT population* (n = 100)Mean baseline A1C level: 8.6%
≤6.5%(AACE)
<7.0%(ADA)
*All patients enrolled in the trial.
21
4152
7060
77
0
20
40
60
80
100
QD
BID
TID
COPYRIG
HT
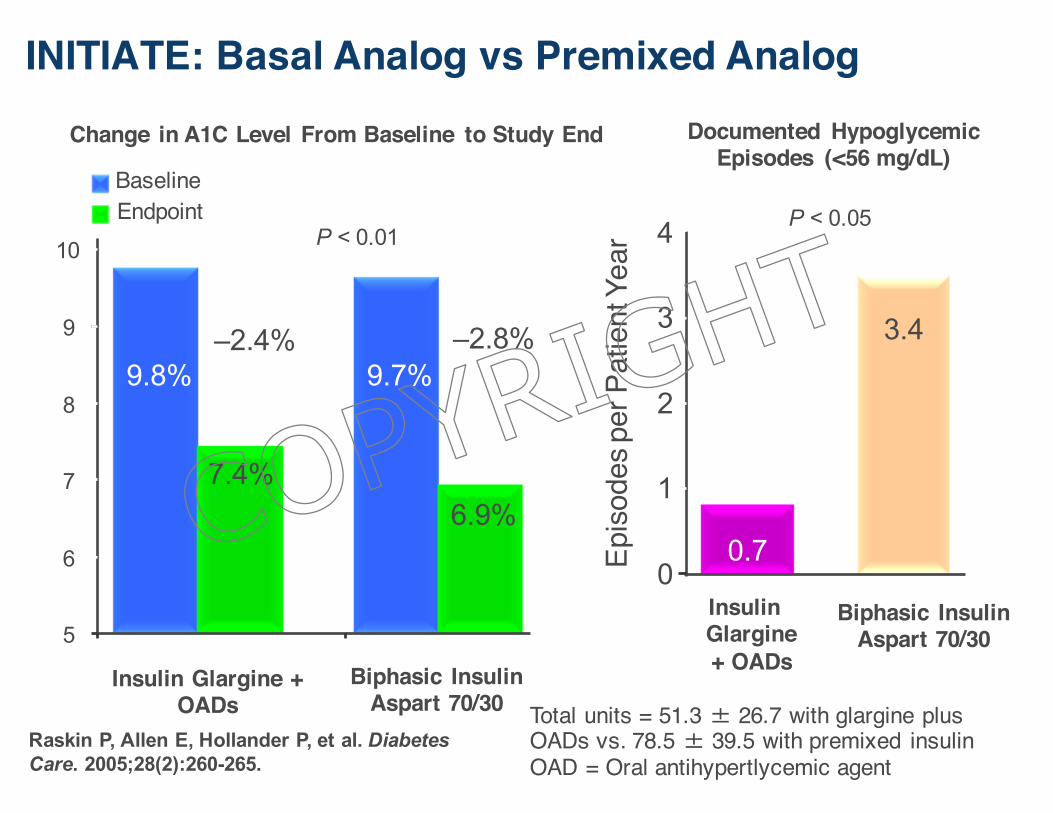
30Raskin P, Allen E, Hollander P, et al. Diabetes Care. 2005;28(2):260-265.
Change in A1C Level From Baseline to Study End
9.8%
6.9%7.4%
5
6
7
8
9
Insulin Glargine + OADs
Biphasic Insulin Aspart 70/30
P < 0.01
A1C
Lev
el (
%)
–2.4% –2.8%
10
9.7%
BaselineEndpoint
0.7
3.4
0
1
2
3
4
Episo
des p
er P
atie
nt Y
ear
P < 0.05
Insulin Glargine + OADs
Biphasic Insulin Aspart 70/30
Total units = 51.3 � 26.7 with glargine plus OADs vs. 78.5 � 39.5 with premixed insulinOAD = Oral antihypertlycemic agent
Documented Hypoglycemic Episodes (<56 mg/dL)
INITIATE: Basal Analog vs Premixed Analog
COPYRIG
HT
31
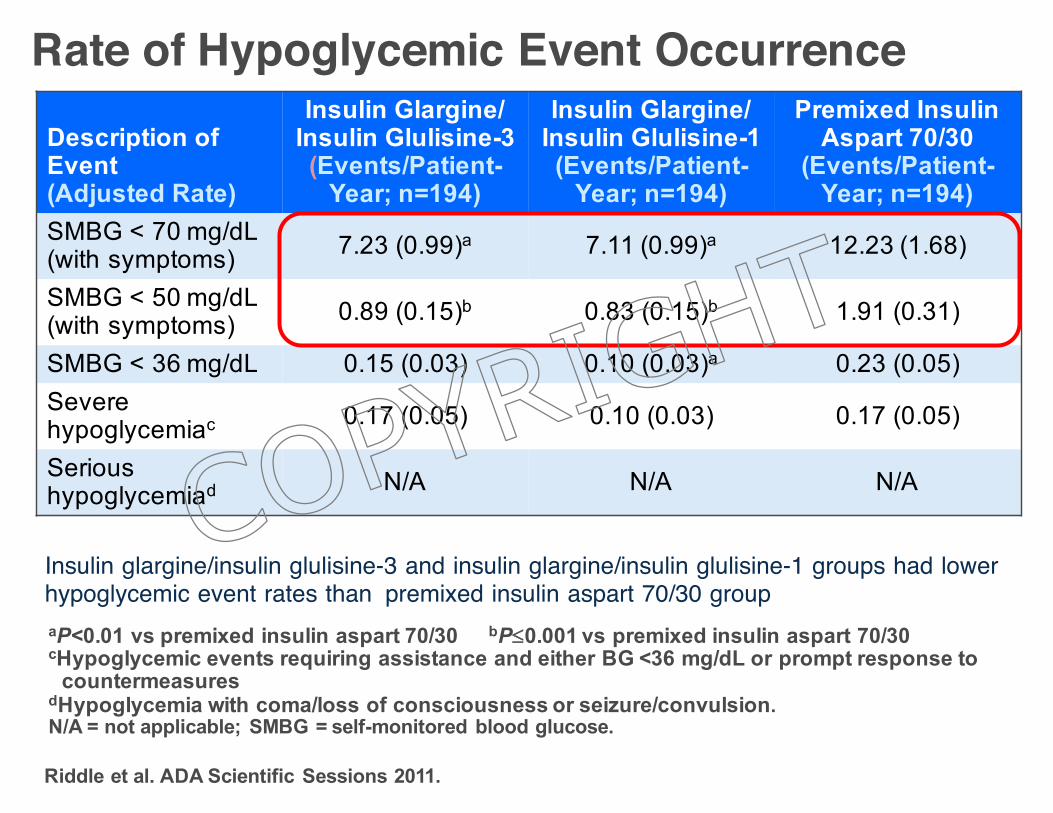
Description of Event (Adjusted Rate)
Insulin Glargine/Insulin Glulisine-3(Events/Patient-
Year; n=194)
Insulin Glargine/Insulin Glulisine-1 (Events/Patient-
Year; n=194)
Premixed Insulin Aspart 70/30
(Events/Patient-Year; n=194)
SMBG < 70 mg/dL (with symptoms) 7.23 (0.99)a 7.11 (0.99)a 12.23 (1.68)
SMBG < 50 mg/dL (with symptoms) 0.89 (0.15)b 0.83 (0.15)b 1.91 (0.31)
SMBG < 36 mg/dL 0.15 (0.03) 0.10 (0.03)a 0.23 (0.05)Severe hypoglycemiac 0.17 (0.05) 0.10 (0.03) 0.17 (0.05)
Serious hypoglycemiad N/A N/A N/A
Rate of Hypoglycemic Event Occurrence
Insulin glargine/insulin glulisine-3 and insulin glargine/insulin glulisine-1 groups had lower hypoglycemic event rates than premixed insulin aspart 70/30 groupaP<0.01 vs premixed insulin aspart 70/30 bP£0.001 vs premixed insulin aspart 70/30cHypoglycemic events requiring assistance and either BG <36 mg/dL or prompt response to
countermeasuresdHypoglycemia with coma/loss of consciousness or seizure/convulsion.N/A = not applicable; SMBG = self-monitored blood glucose.
Riddle et al. ADA Scientific Sessions 2011.
COPYRIG
HT
32
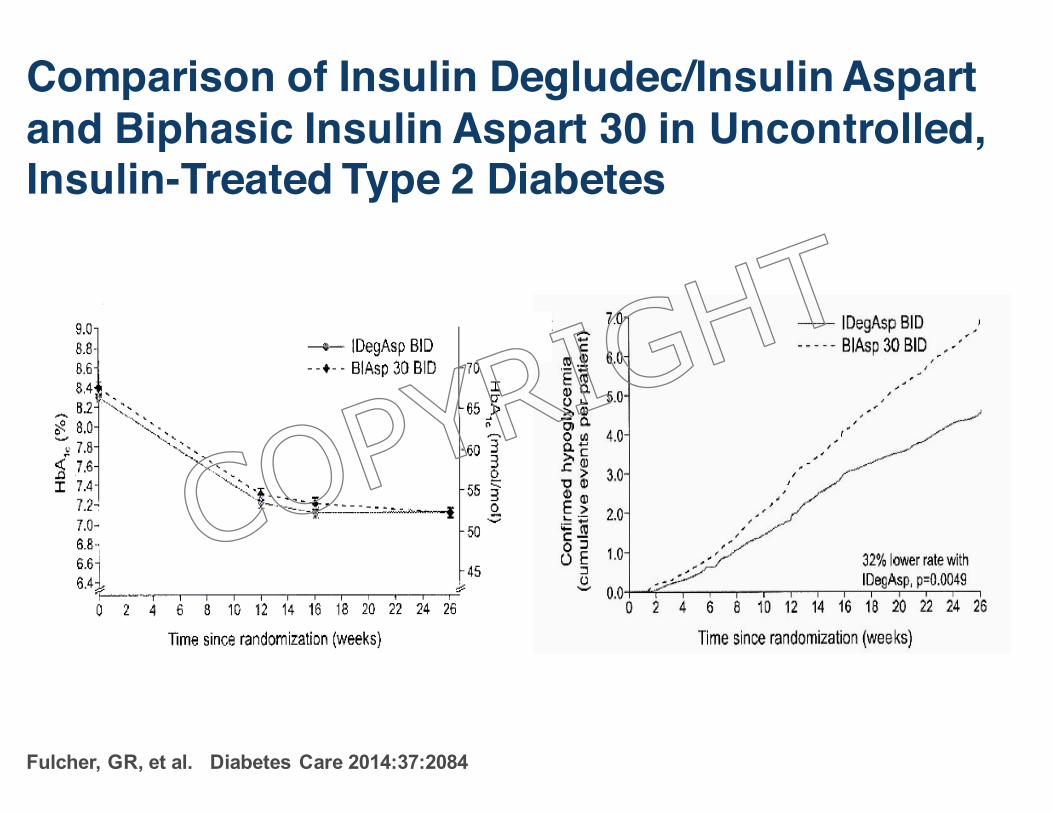
Comparison of Insulin Degludec/Insulin Aspartand Biphasic Insulin Aspart 30 in Uncontrolled, Insulin-Treated Type 2 Diabetes
Fulcher, GR, et al. Diabetes Care 2014:37:2084
COPYRIG
HT
33
Clinical Features of Rapid-Acting Analogues: Aspart, Glulisine, and Lispro
§ Administration immediately prior to meals§ Faster onset of action matches timing of
carbohydrate absorption § Limits postprandial hyperglycemic peaks§ Shorter duration of activity
• Reduced risk of late postprandial hypoglycemia• Frequently can have late postprandial hyperglycemia
§ Glulisine can be given after meals if needed *
6-27
* Garg S et al. American Diabetes Association 64th Scientific Sessions; June 4-8, 2004; Orlando, FL; Abstract 530-P.
COPYRIG
HT
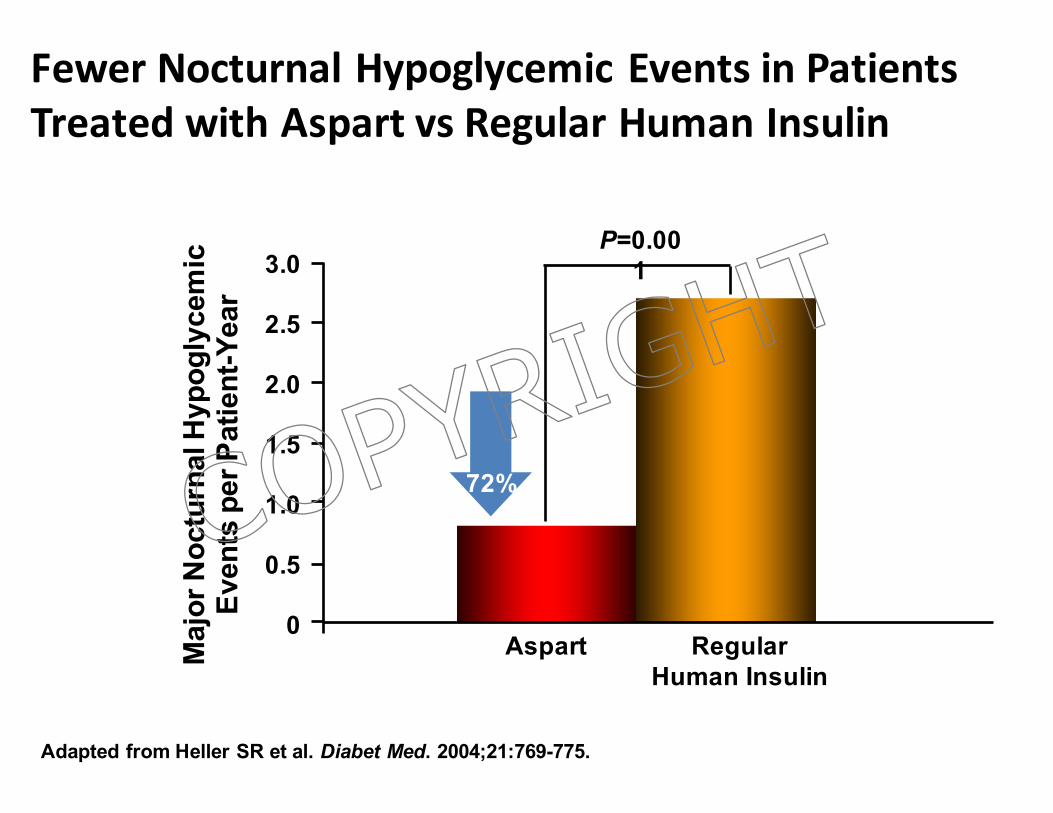
FewerNocturnalHypoglycemicEventsinPatientsTreatedwithAspart vsRegularHumanInsulin
Aspart0
Regular Human Insulin
0.5
1.0
1.5
2.0
2.5
3.0
72%
P=0.001
Maj
or N
octu
rnal
Hyp
ogly
cem
ic
Even
ts p
er P
atie
nt-Y
ear
Adapted from Heller SR et al. Diabet Med. 2004;21:769-775.
COPYRIG
HT
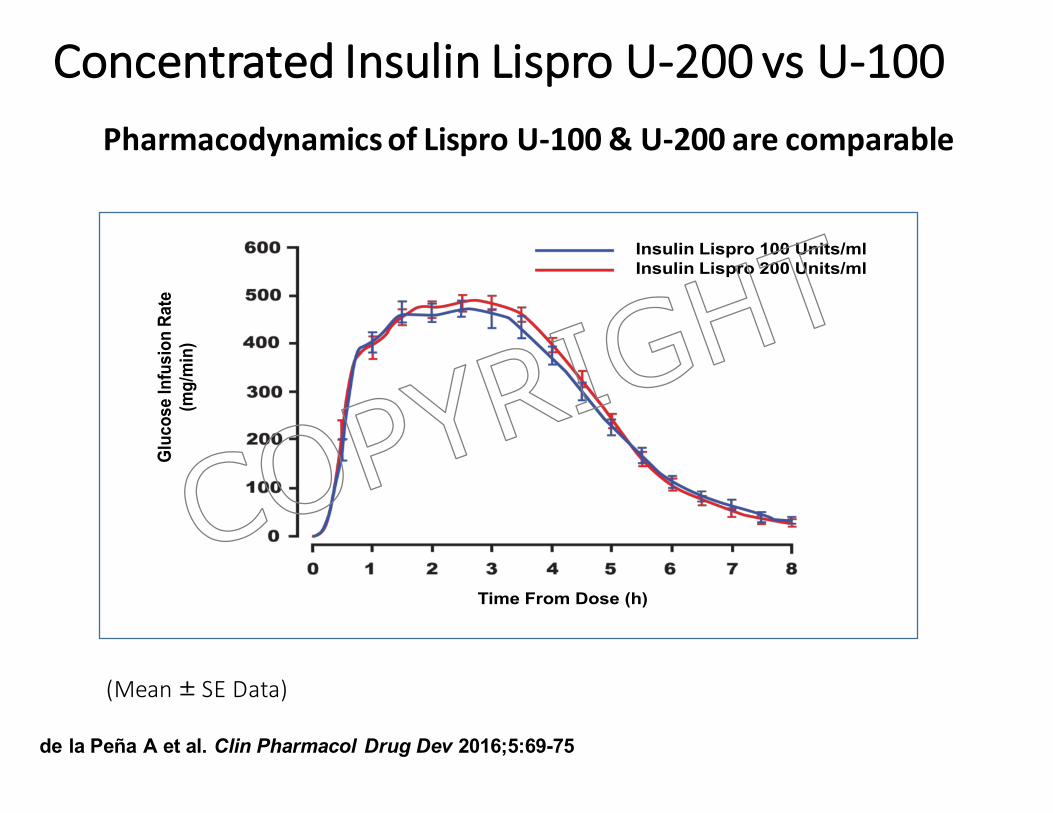
de la Peña A et al. Clin Pharmacol Drug Dev 2016;5:69-75
ConcentratedInsulinLispro U-200vsU-100
Time From Dose (h)
Insulin Lispro 100 Units/mlInsulin Lispro 200 Units/ml
Gluc
ose
Infu
sion
Rat
e (m
g/m
in)
(Mean± SEData)
PharmacodynamicsofLispro U-100&U-200arecomparable
COPYRIG
HT
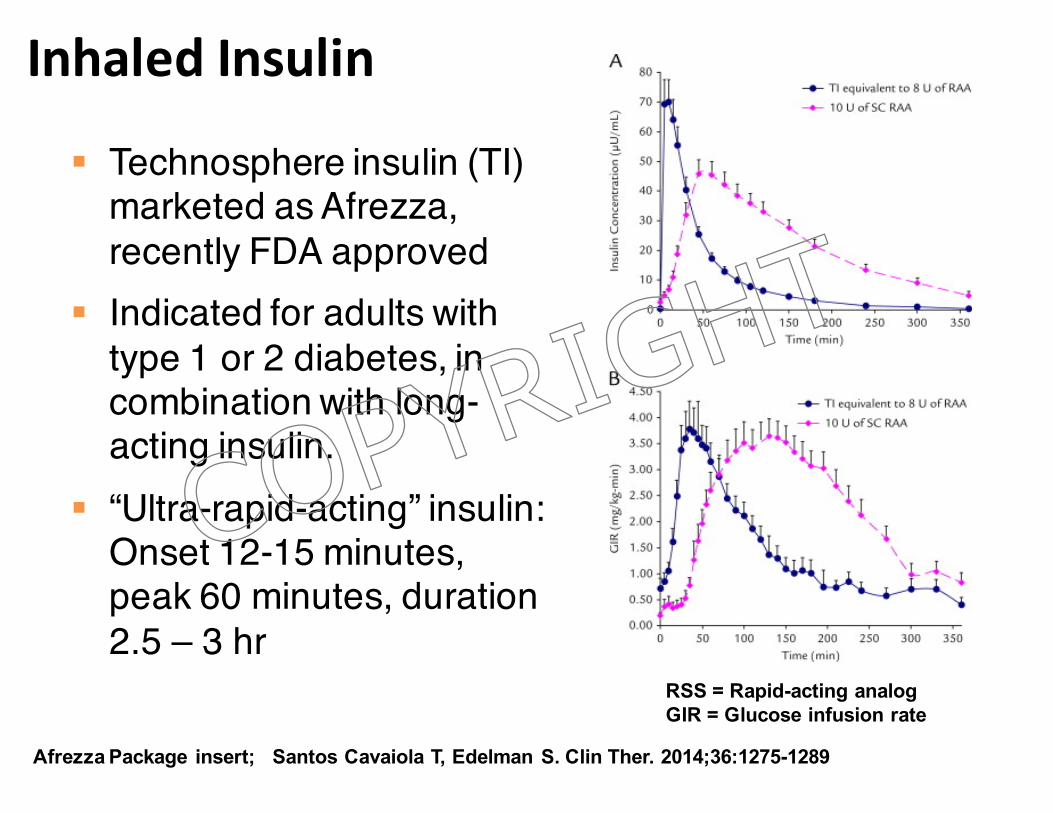
Afrezza Package insert; Santos Cavaiola T, Edelman S. Clin Ther. 2014;36:1275-1289
RSS = Rapid-acting analogGIR = Glucose infusion rate
InhaledInsulin
§ Technosphere insulin (TI) marketed as Afrezza, recently FDA approved
§ Indicated for adults with type 1 or 2 diabetes, in combination with long-acting insulin.
§ “Ultra-rapid-acting” insulin: Onset 12-15 minutes, peak 60 minutes, duration 2.5 – 3 hr
COPYRIG
HT
InhaledInsulin:LimitationsandContraindicationsLimitations:
§ Inhaledinsulinisnotasubstituteforlong-actinginsulin.
§ Notrecommendedforthetreatmentofdiabeticketoacidosis
§ Notrecommendedinpatientswhosmokeorwhohavestoppedsmokinginlast6months.
Contraindications:§ Duringepisodesofhypoglycemia
§ InpatientswhohavechroniclungdiseasesuchasCOPDorasthma
www.fda.gov/downloads/advisorycommittees/committeesmeetingmaterials/drugs/endocrinologicandmetabolicdrugsadvisorycommittee/ucm390865.pdf
COPYRIG
HT
• Consideraddingprandial(mealtime)insulininabout3–6monthsif:– A1Ciselevated– Significantpostprandialglucoseexcursionsoccur(>180mg/dL)
– Therearesignificantdropsinglucosebetweenmealsorovernightasthebasalinsulindoseisincreased
– Likelyneededifthetotaldailyinsulindoseexceeds0.5Units/kg/day.
ADA, EASD Position Statement. Diabetes Care 2015;38;1364-1379
AddingBolusInsulin
COPYRIG
HT
Based on: Nathan DM, et al. Diabetes Care. 2009;32:193-203. ADA, EASD Position Statement. Diabetes Care 2015;38;140-149.AACE/ACE Comprehensive Diabetes Management Algorithm, Endocr Pract. 2015;21(No. 4)
AddingBolusInsulin§ Add prandial insulin before meal with largest
glucose excursion (>180 mg/dl) or the meal with the largest CHO content.
§ Other meals can be covered subsequently. § Alternatively start with coverage of all three meals
at once.§ TDD: 0.3 – 0.5 U/kg; 50/50 basal/prandial§ Antihyperglycemic medications:
§ Generally, stop insulin secretagogues (SU, DPP-4 inhibitors, glinides)
§ Reduce or stop TZD’sTDD=TotaldailydoseSU=Sulfonlyurea
COPYRIG
HT
Do you add injection at the largest meal or the one with the highest postprandial elevation?• Overall reduction in HbA1C of 1.2% was achieved with
the addition of prandial insulin.• Greatest HbA1C reductions were achieved with the first
and second bolus injections.• Glycemic improvement comparable in both groups.• Number of hypoglycemic episodes increased with
increasing number of prandial injections.• Basal-bolus treatment can be introduced in a more
patient-friendly approach, using simple stepwise addition of prandial insulin.
STEPwise Study
Meneghini, et al. Endocr Pract. 2011;17:727-736
COPYRIG
HT
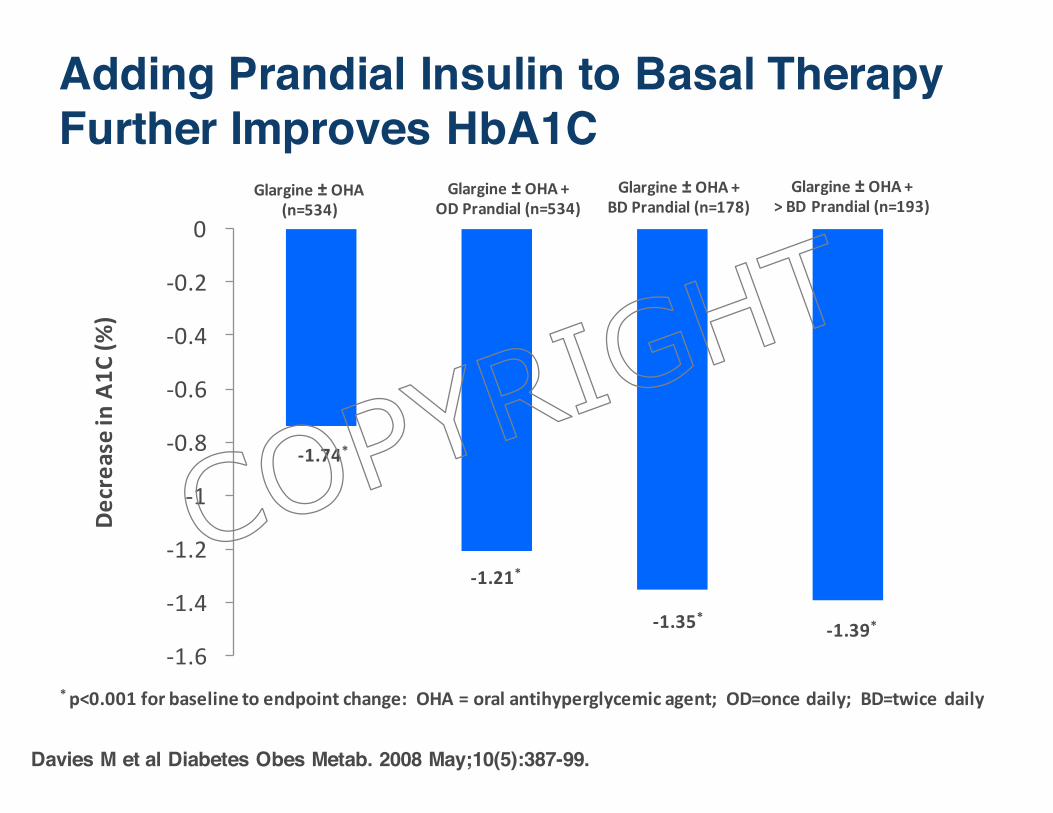
Adding Prandial Insulin to Basal Therapy Further Improves HbA1C
Davies M et al Diabetes Obes Metab. 2008 May;10(5):387-99.
-1.6
-1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
DecreaseinA1C
(%)
Glargine± OHA(n=534)
Glargine± OHA+ODPrandial(n=534)
Glargine± OHA+BDPrandial(n=178)
Glargine± OHA+>BDPrandial(n=193)
*p<0.001forbaselinetoendpointchange:OHA=oralantihyperglycemic agent;OD=oncedaily;BD=twicedaily
-1.74*
-1.35*
-1.21*
-1.39*
COPYRIG
HT
PhysiologicInsulinRegimenswithbasalinsulinplusrapid-actinginsulindosingbeforeeachmeal§ Checking blood glucose 4 to 6 times a day § CHO counting or consistent CHO Intake§ Premeal insulin dosing by algorithmic scale
or, preferably, carbohydrate counting § Surveillance and risk for hypoglycemia § Record keeping: “Monitoring” rather than
just “checking”
COPYRIG
HT
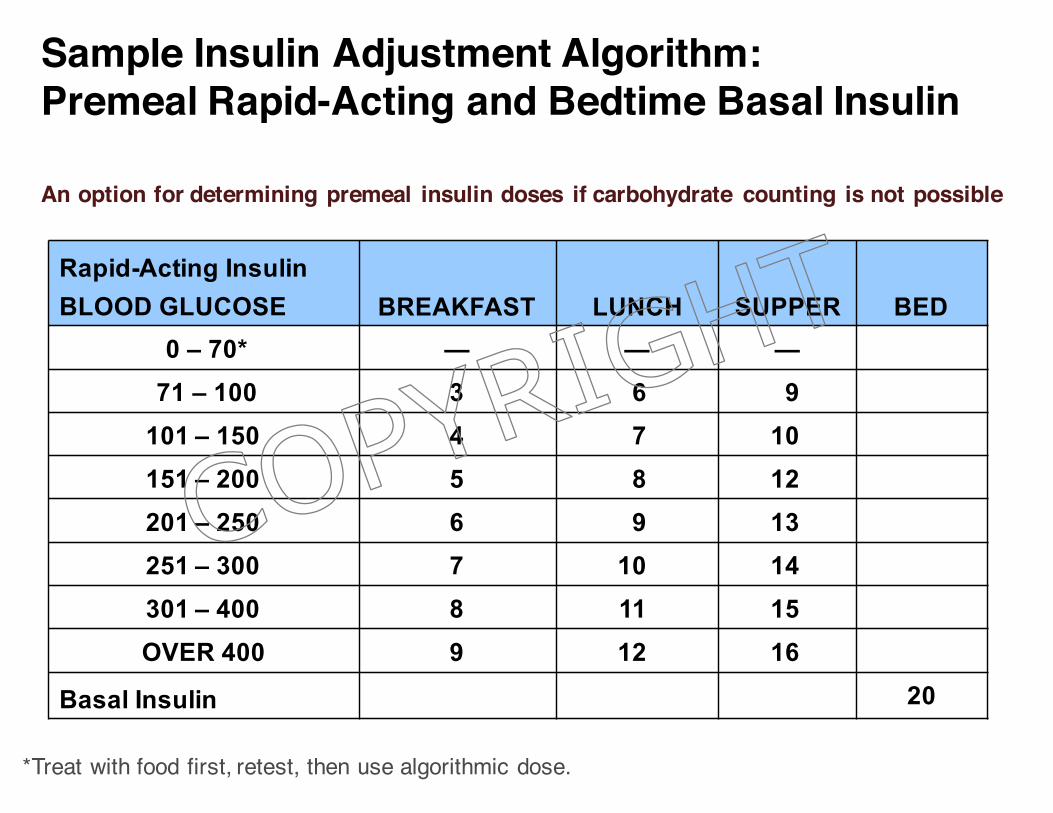
*Treat with food first, retest, then use algorithmic dose.
Rapid-Acting InsulinBLOOD GLUCOSE BREAKFAST LUNCH SUPPER BED
0 – 70* — — —71 – 100 3 6 9
101 – 150 4 7 10151 – 200 5 8 12201 – 250 6 9 13251 – 300 7 10 14301 – 400 8 11 15OVER 400 9 12 16
Basal Insulin 20
An option for determining premeal insulin doses if carbohydrate counting is not possible
*Treat with food first, retest, then use algorithmic dose.
Sample Insulin Adjustment Algorithm: Premeal Rapid-Acting and Bedtime Basal Insulin
COPYRIG
HT
CarbohydrateCounting,MatchingandPostprandialControl
• Twofactorsprimarilygovernthedoseofpremealinsulin:– Gramsofcarbohydrate– Correctiondosesifpremealhyperglycemiaispresent
• Twocalculationsareusefulforinitialdosing:– Carbohydratecoverage:Totaldailyinsulindose(TDD)dividedinto500givestheapproximatenumberofcarbgramsthat1unitofrapidactinginsulinwill“cover.”
– Correctiondose:DividetheTDDinto1500.Usuallyinitiallytargetaglucoseof120mg/dL
COPYRIG
HT
CarbohydrateCounting,MatchingandPostprandialControl:Example
Ø Calculatingacarbohydrate(CHO)countinginsulindosingprogramforatotaldailyinsulindoseof50units:
– Basalinsulin:25unitsdailyatbedtime– PremealcoveragebasedonCHOintake:
§ Totaldailyinsulindose(TDD)=50units§ 500/50=10§ Give1unitofpremealrapid-actinginsulinforevery10gramsofcarbohydratetobeconsumed.
– Correctiondose:§ 1500/50=30§ Giveanextraunitofrapid-actingpremealinsulinforevery30pointsabove120mg/dL
COPYRIG
HT
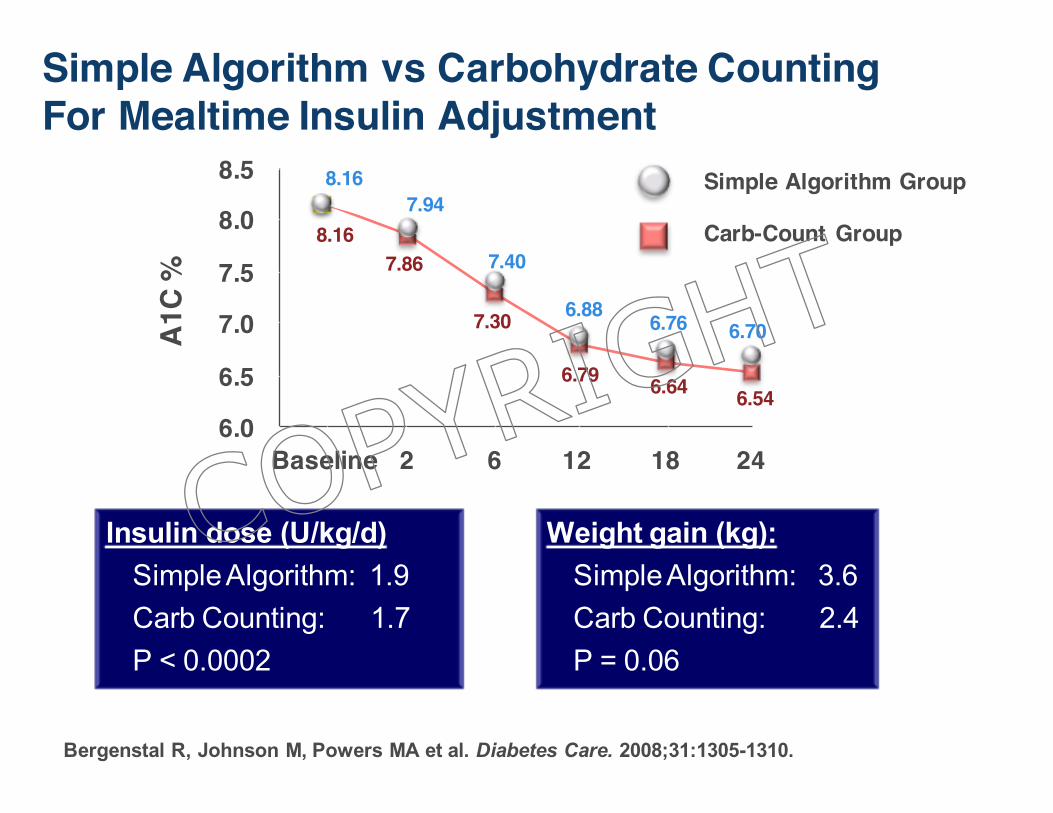
Simple Algorithm vs Carbohydrate Counting For Mealtime Insulin Adjustment
Insulin dose (U/kg/d) Simple Algorithm: 1.9 Carb Counting: 1.7 P < 0.0002
A1C
%8.5
8.0
7.5
7.0
6.5
6.0Baseline 2 6 12 18 24
8.167.94
7.40
6.88 6.76 6.70
6.546.646.79
7.30
7.868.16
Simple Algorithm Group
Carb-Count Group
Bergenstal R, Johnson M, Powers MA et al. Diabetes Care. 2008;31:1305-1310.
Weight gain (kg): Simple Algorithm: 3.6 Carb Counting: 2.4 P = 0.06
COPYRIG
HT
GlucoseMonitoring• Nooneshouldperformasingleglucosetestunlessheorsheknowswhattodowiththeresult!
• Thereisadifferencebetweenglucosechecking(testing)andglucosemonitoring
• Individualizemonitoringschedule
• Record-keepingisofcrucialimportancetothemonitoringprocess
COPYRIG
HT
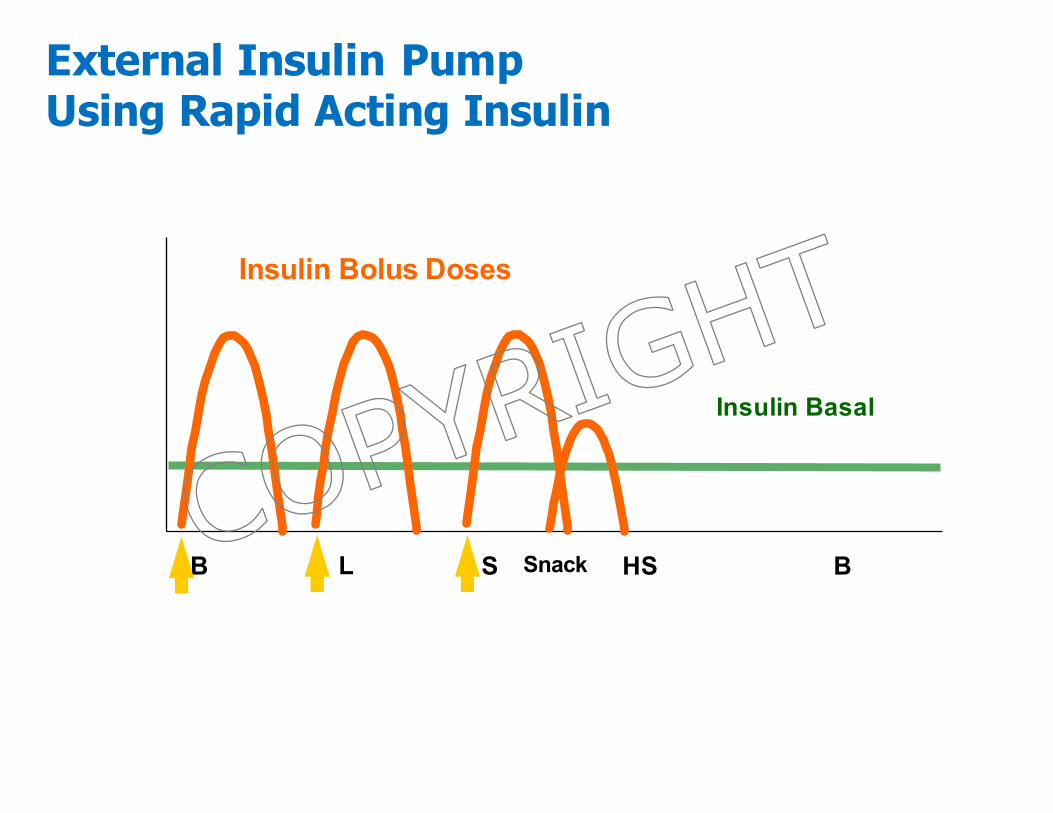
B L S HS B
Insu
lin E
ffect
Meals
External Insulin Pump Using Rapid Acting Insulin
Insulin Bolus Doses
Insulin Basal
SnackCOPYRIG
HT
SuggestedSequenceforAssessmentofGlycemicPatterns
• Fastingvalue• Generalpremeal andbedtimevaluesand
trendsthroughouttheday• Postprandialvalues– absolutelevels• Relativechange,pre- topostprandial
glycemiclevels
à Also,continuallymonitornocturnalglycemia
COPYRIG
HT
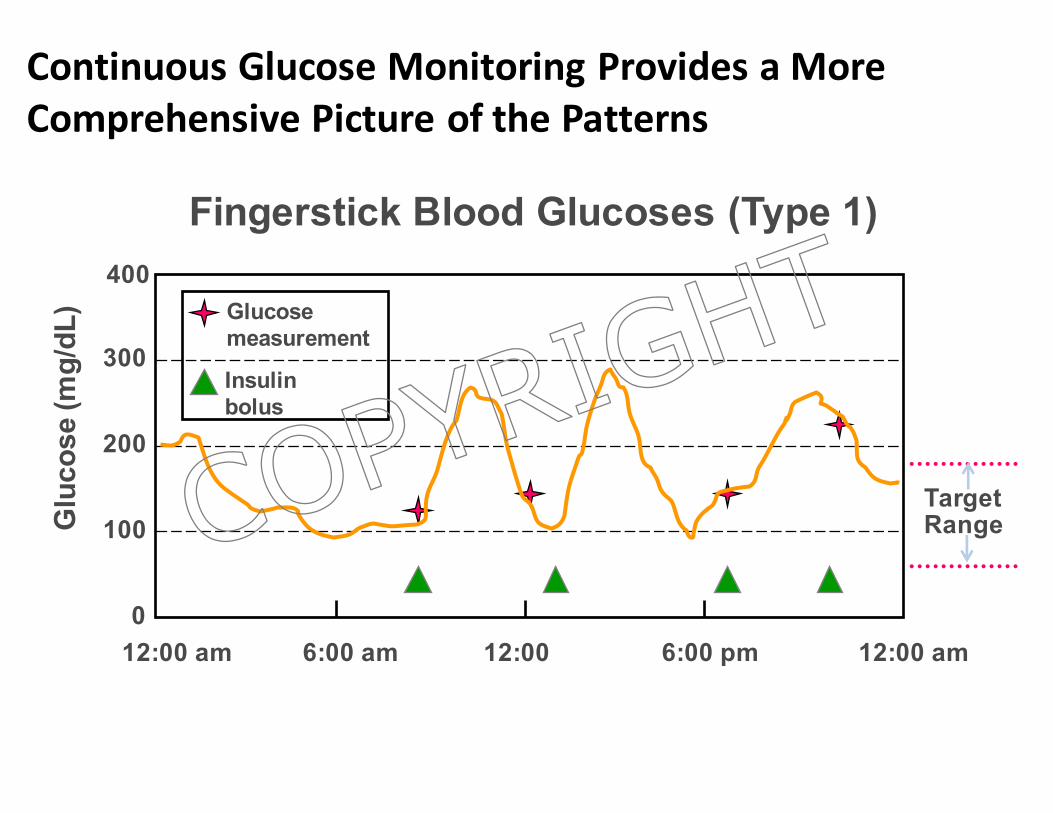
12:00 am 6:00 am 12:00 6:00 pm 12:00 am
Glu
cose
(mg/
dL)
400
300
200
100
0
Glucose measurement
Insulinbolus
TargetRange
Fingerstick Blood Glucoses (Type 1)
ContinuousGlucoseMonitoringProvidesaMoreComprehensivePictureofthePatterns
COPYRIG
HT
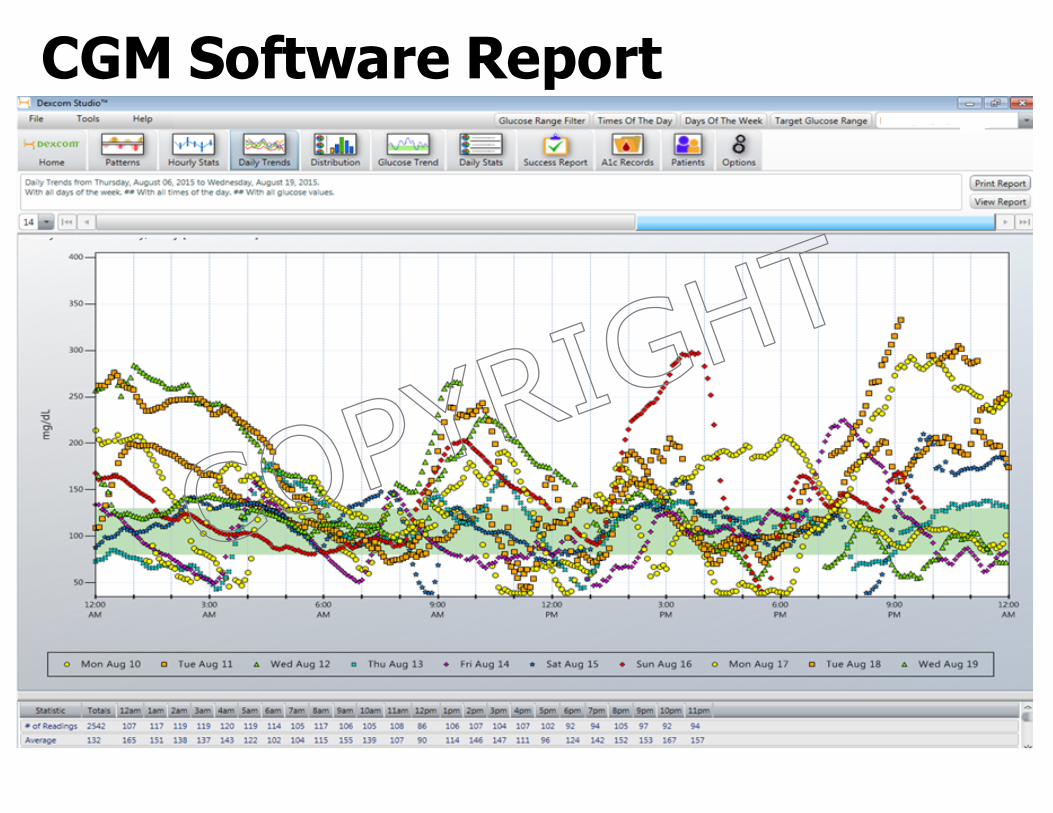
CGM Software Report
COPYRIG
HT
Factors Influencing Therapeutic ChoicesØ Medical needs and treatment goals
• A1C level and distance from target• Postprandial glycemia
Ø SafetyØ Need for flexibility in treatment programØ Patient issues with respect to insulin use
• Intellect and judgment• Psychosocial and cultural considerations• Physical capabilities and limitations• Other medical conditions and issues
relating to use of other non-insulin medications
COPYRIG
HT
Adapted from Funnell MM. Clinical Diabetes. 2007;25(1):36-38.
PatientBarrierstoInsulinInitiationØ Needinginsulinrepresentsapersonalfailure
• Describethenaturalprogressionoftype2diabetesandtheinevitabilityoftheneedforinsulin
• Donotuseinsulinasathreat
Ø Insulinisnoteffective• Manypatientsdonotbelieveinsuliniseffective• Matchinsulinusetogoalsthatpatientscansee:Glycemic
patterns,symptoms
Ø Insulincausescomplications• Manypatientssawrelatives/friendsstartinsulininthe
contextofbadeventshappening• Providesupportiveeducation
Ø Impactonlifestyle• Perceivedcauses:Injectionschedule,hypoglycemia• Providesupportiveeducation• Insulinpens
COPYRIG
HT
Adapted from Funnell MM. Clinical Diabetes. 2007;25(1):36-38.
Ø Injectionsarepainful• Perceivethattheyarethesameasinoculationsorotherpainful
injectionexperiences• Comparetoglucosechecking• Demonstrationinjection• Discussneedlesize;useofpens
Ø Fearofhypoglycemia• Observingproblemsinothers• Educationfocusingonadvantagesofnewerinsulins,hypoglycemia
avoidance,appropriategoalsetting
Ø Insulincausesweightgain• Acknowledgethepossibility• Discussstrategiestoavoid:Dietitian,CHOcounting
Ø Cost• Acknowledge/comparecostforinsulinvs.DMMeds• Explorestrategiestoreducecosts
PatientBarrierstoInsulinInitiation
COPYRIG
HT
PhysicianBarrierstoInsulinInitiation
Adapted from Funnell MM. Clinical Diabetes. 2007;25(1):36-38. Derr RL, et al. Diabetes Spectrum. 2007; 20(3):177-185.
Ø Systemsdeficiencies• Recognizingindications,impactoftreatment:EMRreminders• Educationalsupport:Trainofficestaff;identify/developworking
relationshipwithadditionaleducationalresources
Ø Providereducationaboutinsulin• Optimizeyourownknowledgeandskills
Ø Concernabouthypoglycemia• Similarissuestopatients• SetindividualizedgoalsanddesignappropriateRx• Providesupportiveeducation
Ø Weightgain• Usedietitians,physiologicinsulinprograms
Ø Uneaseindealingwithpatientemotions/barriers• Developstrategiesandpracticethem!
COPYRIG
HT
AStepwisePerspectiveonInsulinTreatment
• Abilitytoidentifypeopleforwhominsulinisindicatedanddiscussthisneedwiththem
• Capabilityoridentifiedreferralresourcestooverseeinsulintreatmentinitiationandsupport
• Abilitytoteachinsulinuse:– Techniques– KnowledgeandSkillsforself-management– Spectrumofprograms,frombasaltopumps
• Abilitytoidentifypeopleforwhomthecurrentprogramisinadequateandadvancementoftherapyisindicated
• Troubleshooting• Referralmanagement
COPYRIG
HT
AStepwisePerspectiveonInsulinTreatment
• Abilitytoidentifypeopleforwhominsulinisindicatedanddiscussthisneedwiththem
• Capabilityoridentifiedreferralresourcestooverseeinsulintreatmentinitiationandsupport
• Abilitytoteachinsulinuse:– Techniques– KnowledgeandSkillsforself-management– Spectrumofprograms,frombasaltopumps
• Abilitytoidentifypeopleforwhomthecurrentprogramisinadequateandadvancementoftherapyisindicated
• Troubleshooting• Referralmanagement
COPYRIG
HT
Take-AwayMessages
• Treatmentgoals,programdesign,andmonitoringrecommendationsmustbeindividualized
• Monitoringofglycemicpatternsisakeytooltoguidetherapeuticdecisions
• Basal-bolusregimensrequiremoreinjectionsbutprovidebetterinsulincoverageandglycemiccontrol
• Patient,provider,andpracticesystemsbarrierstoinsulintherapymustberecognizedandaddressed
• Self-assessofficecapabilitiesinthecontextofinsulintreatmentsupport
COPYRIG
HT
“Insulin is a remedy for the wise and not the foolish, be they patients or doctors. Everyone knows it requires brains to live long with diabetes, but to use insulin successfully requires more brains.”
§ Elliott P. Joslin, MD, ScD§ Diabetic Manual, 1959
COPYRIG
HT





























