Embed Size (px)
Citation preview
Advancing Health in South Texas Engagement Series: Engaging the
Community Voice/Building the Patient- Centered Partnership
Summary Report February 2017
TABLEOFCONTENTS
Introduction and Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Overview of Approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 RecruitmentStrategy...................................................................................................................................3FactorsInfluencingHealth...........................................................................................................................4IntegrationofPerspectivesandApproaches...............................................................................................5
Engaging the Community Voice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 Overview......................................................................................................................................................6Methods.......................................................................................................................................................6SessionFindingsandKeyThemes................................................................................................................7SessionConclusions.....................................................................................................................................9
Building the Patient-Centered Partnership . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 Overview....................................................................................................................................................10Methods.....................................................................................................................................................10SessionFindingsandKeyThemes..............................................................................................................10SessionConclusions...................................................................................................................................13
List of Appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 Appendix1:EngagingtheCommunityVoiceAgenda................................................................................15Appendix2:EngagingtheCommunityVoiceParticipants.........................................................................16Appendix3:BuildingthePatient-CenteredPartnershipAgenda..............................................................20Appendix4:BuildingthePatient-CenteredPartnershipParticipants........................................................21Appendix4:KeyDifferencesandCommonalitiesAmongConvenedSessions..........................................24Appendix5:DefinitionofTerms................................................................................................................25
3
INTRODUCTIONANDBACKGROUNDInthefallof2015,MethodistHealthcareMinistrieswasawardedtheEugeneWashingtonPCORI(Patient-CenteredOutcomesResearchInstitute)EngagementAwardtoimplementaprojecttitledAdvancingHealthinSouthTexasEngagementSeries.ThroughthisawardMethodistHealthcareMinistriesconvenedpatientsandkeystakeholdersacrossa20-countyareatodevelopacoordinatedregionalapproachforpatient-centeredresearchandevaluationamonguniversitysystems,academicinstitutions,managedcareorganizations(MCOs),andpublichealthsystems.Tothisendofdevelopingacoordinatedregionalapproach,theAdvancingHealthinSouthTexasEngagementSeriesaimedtocreateasafespacetofacilitatemeaningfuldialoguebetweenpeopleandinstitutionalsystemstoensuretrustedrelationshipsareformed,informationisshared,andallvoicesareengagedintheplanningandco-creatingofsolutions.Theseriesalsoaimedtoidentifyandadoptmulti-sectorstrategiesbasedondifferentiatedbutalignedactivitiesandacommonframework.MethodistHealthcareMinistriespartneredwithHealthResourcesinAction(HRiA),anon-profitpublichealthorganization,toserveastheseriesfacilitatorstoidentifyappropriatepatientengagementmodelsfortheregion.Thefourthsessionintheseries,EngagingtheCommunityVoiceaimedtoreengageend-usersthroughfacilitated“town-hall”discussionsinordertosharebackfindingsfromtheconvenedsessions,askforadditionalsuggestionsorclarifications,anddiscussnextstepsintheprocess.Participantsincluded:consumers,stakeholders,academicinstitutions,healthadvocacygroups,andhealthcareproviders.Here,findingsfromthethreeprecedingengagementsessions,WhatMatterstoYou?KnowledgeSharingChampions,andEngagingHealthPayerswerepresentedtothegroup,followedbyfacilitateddiscussionstoelicitfeedbackandsuggestionsforfutureplanningprocesses.Followingthecommunitytown-hallmeetinginMcAllen,participantsbeganthefoundationalplanningprocessdescribedasBuildingthePatient-CenteredPartnership.Thisplanningsessionengagedparticipantsinadiscussiontoidentifypotentialareasofcollaborativeresearchmovingforward,aswellasthespecificstrategiesfordevelopingandsustainingthecollaborativepartnershipandeffectivelydisseminatingtheresearchtokeygroupsinthecommunity.Thefollowingreportsprovidesasynthesisofthesetown-hallstylediscussionsthatwereheldinCorpusChristi,Laredo,andMcAllen,TX,aswellasthefoundationalplanningprocess,highlightingcommonalitiesanddifferencesbygeographiclocationwhereappropriate.
OVERVIEWOFAPPROACH
RecruitmentStrategyThefocusonthoughtfulpartnershipshasbeenacornerstoneofMethodistHealthcareMinistries’strategytoencourageauthenticengagementthroughouttheEngagementSeries.Similartotherecruitmentstrategyusedinthefirstthreesessions,MethodistHealthcareMinistriesreachedouttotrustedinstitutionalpartnerstoassistwiththerecruitmentprocess.Theeffortfordeliberatepartnershipsensuredthattheappropriatestakeholderswereengagedthroughoutthisprocess.
4
Fromtheseconversations,MethodistHealthcareMinistriesidentifiedinternalandexternalparticipantswhoattendedpreviousEngagementSeriessessions.ParticipantswereinvitedtoattendtheEngagingtheCommunityVoicesessionsintheCoastalBend,Laredo,ortheRioGrandeValleyregion,wheretheWhatMatterstoYou?focusgroupswereheld.Acombinedtotalof122participantsfromthefollowingcountiesattended:Cameron,Hidalgo,JimHogg,JimWells,Nueces,SanPatricioandWebb.Theywereselectedbecausetheyrepresentedactiveresearchers,patients/clients,communitystakeholders,healthcareprovidesystemandpublicpolicymakersintheregionwithaspecialtyoncommunityengagementandpatient-centeredfocusthatinfluenceoutcomesofcare.Individualswerepersonallycontactedbyhigh-touchphonecallsfacilitatedbyMethodistHealthcareMinistries.
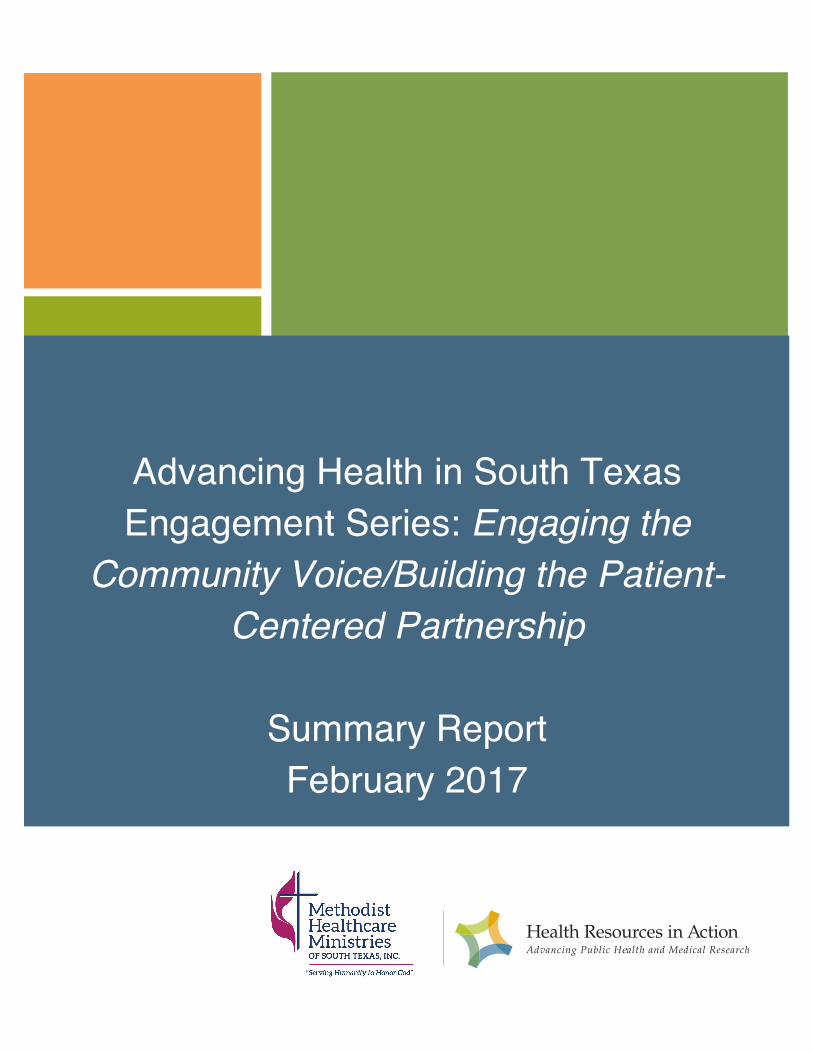
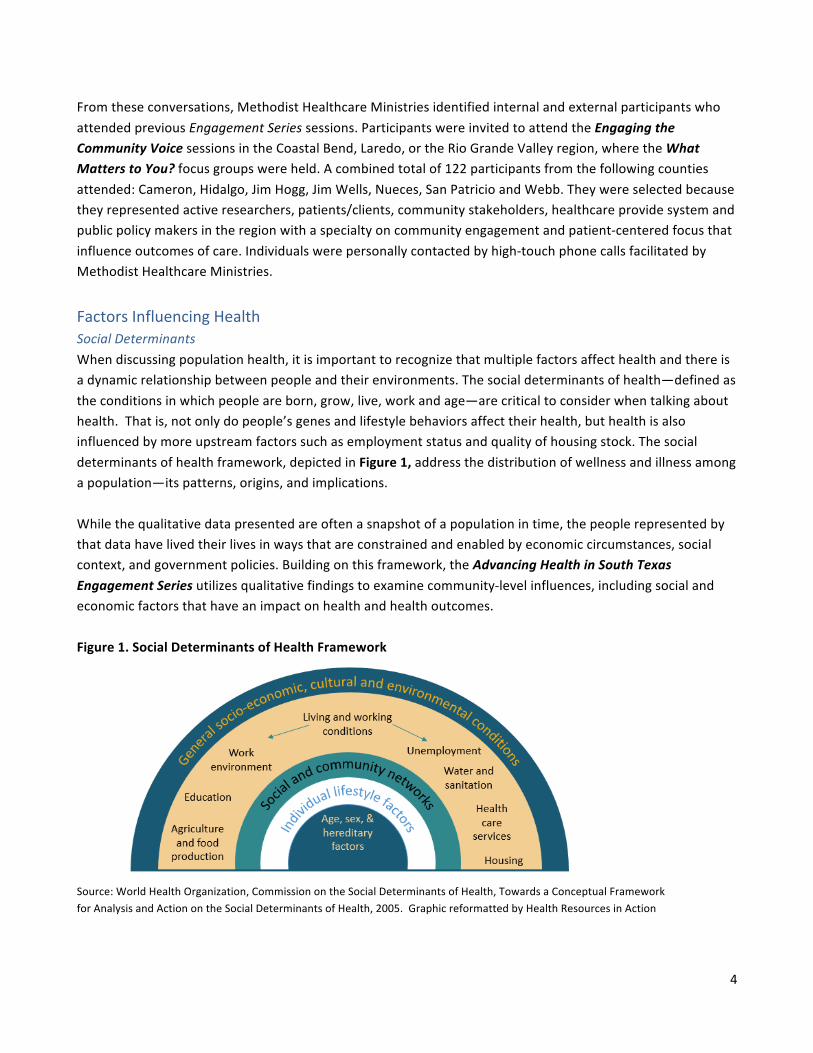
FactorsInfluencingHealthSocialDeterminantsWhendiscussingpopulationhealth,itisimportanttorecognizethatmultiplefactorsaffecthealthandthereisadynamicrelationshipbetweenpeopleandtheirenvironments.Thesocialdeterminantsofhealth—definedastheconditionsinwhichpeopleareborn,grow,live,workandage—arecriticaltoconsiderwhentalkingabouthealth.Thatis,notonlydopeople’sgenesandlifestylebehaviorsaffecttheirhealth,buthealthisalsoinfluencedbymoreupstreamfactorssuchasemploymentstatusandqualityofhousingstock.Thesocialdeterminantsofhealthframework,depictedinFigure1,addressthedistributionofwellnessandillnessamongapopulation—itspatterns,origins,andimplications.Whilethequalitativedatapresentedareoftenasnapshotofapopulationintime,thepeoplerepresentedbythatdatahavelivedtheirlivesinwaysthatareconstrainedandenabledbyeconomiccircumstances,socialcontext,andgovernmentpolicies.Buildingonthisframework,theAdvancingHealthinSouthTexasEngagementSeriesutilizesqualitativefindingstoexaminecommunity-levelinfluences,includingsocialandeconomicfactorsthathaveanimpactonhealthandhealthoutcomes.Figure1.SocialDeterminantsofHealthFramework
Source:WorldHealthOrganization,CommissionontheSocialDeterminantsofHealth,TowardsaConceptualFrameworkforAnalysisandActionontheSocialDeterminantsofHealth,2005.GraphicreformattedbyHealthResourcesinAction

5
HealthEquityInadditiontoconsideringthesocialdeterminantsofhealth,itiscriticaltounderstandhowthesecharacteristicsdisproportionatelyaffectvulnerablepopulations.Healthequityisdefinedasallpeoplehavingtheopportunityto“attaintheirfullhealthpotential”andentailsfocusedsocietaleffortstoaddressavoidableinequalitiesbyequalizingconditionsforhealthforallgroups,especiallyforthosewhohaveexperiencedsocioeconomicdisadvantagesorhistoricalinjustices.Whenexaminingthelargersocialandeconomiccontextofthepopulation(e.g.,upstreamfactorssuchashousing,employmentstatus,racialorethnicdiscrimination,thebuiltenvironment,andneighborhood-levelresources),arobustassessmentshouldcapturethedisparitiesandinequitiesthatexistfortraditionallyunderservedgroups.Thus,ahealthequitylensguidedtheAdvancingHealthinSouthTexasEngagementSeriestoensurequalitativedatacomprisedarangeofsocialandeconomicindicatorsandwerepresentedforspecificpopulationgroups.Understandingfactorsthatcontributetohealthpatternsforthesepopulationscanfacilitatetheidentificationofdata-informedandevidence-basedstrategiestoprovideallresidentswiththeopportunitytoliveahealthylife.
IntegrationofPerspectivesandApproachesThestrategybehindtheEngagementSerieswastoidentifytheareasofsynergyamonguniquebutequallyimportantstakeholdersinregardstopatient-centeredresearchinthePCORIservicearea.ThecenteroftheVenndiagramconcept,depictedinFigure2,wouldbeusedtoidentifypriorityareastoleverageinfutureeffortsamongvaryingsectors,stakeholders,and/orareasofalignment.Figure2.EngagementSeriesVennDiagram:AreasofAlignmentBetweenVaryingStakeholderGroups
6
ENGAGINGTHECOMMUNITYVOICE
OverviewThefourthconvenedsessionoftheSeries,EngagingtheCommunityVoice(ECV)aimedtoreengageend-usersofMethodistHealthcareMinistries-sponsoredinitiativesandprograms—includingconsumers,stakeholders,academicinstitutions,healthadvocacygroups,healthcareproviders,andpayers--throughfacilitated“town-hall”discussionsinordertoaskforadditionalsuggestionsorclarifications,anddiscussnextstepsintheprocess.Duringthe90-minutesessionsheldinCorpusChristi,Laredo,andMcAlleninFebruary2017,findingsfromthethreeprecedingengagementsessionswerepresentedtothegroup,followedbyfacilitateddiscussionstoelicitfeedbackandsuggestionsforfutureplanningguidingbythefollowingquestions:
1. Whatismissingthatyouwouldwantaddedandwhy?2. Whatdoyoulikeabouttheinformationpresentedthusfar?3. Whatwouldyouchangeorclarifyaboutwhathasbeenpresented?
MethodsAspartofthisprocess,everyparticipantwasalsogivenanindexcardtosolicitadditionalwrittenfeedbackthatmayhavenotbeendiscussed.Intotal,122participantswereinvolvedinthetown-hallstylediscussions.Theobjectivesforthedayincludedthefollowing:
• ProvideahighlevelsummaryofthePatientCenteredOutcomesResearchInstituteaward-short-term,mid-termandlong-termobjectives.TheoverallgoalofPOCRIistoimprovepopulationhealthforthecommunitiesserved.
• Sharethekeythemesfromthecommunityfocusgroups,academicandpayersessions,andtheirimplicationsfortheresultingresearch,care,andeducationprogramsaswellastheeffectivedisseminationoftheinformation
• Engageendusers,suchasconsumers,caregivers,policymakers,andhealthadvocacygroups,todiscussbest-in-classstrategiesforresearchdissemination.
Thefollowingsectionsummarizesthethemesthatemergedfromthisconversation—manyofwhichstronglyresonatewithkeythemesfromtheWhatMatterstoYou?KnowledgeSharingChampions,andEngagingHealthPayerssessions.Thetablethatprecedesthenarrativerepresentsavisualofcrosscuttingthemesamongtown-halldiscussions.Aspreviouslydiscussed,thevaryinglevelsofreadinesstodiscusspatient-centeredresearchamongstakeholdergroupslimitedthediscussionregardingspecificresearchdisseminationstrategiesthanoriginallyintended.Nonetheless,findingsfromthesesessionsprovidevaluableinsighttotheopportunitiesforeachofthesegroupstoaddresspatient-centeredresearchmovingforward.
7
SessionFindingsandKeyThemesPromoteAuthenticEngagementandReframeResearchAgendaValidatingfindingsfromtheprevioussessions,participantsacknowledgedthecomplexitiesandchallengesofauthenticcommunityengagement;onechallengewasbeingperceivedas“elitist”bycommunitymembers.Alsonotedwastheimportanceofclarifyingthedifferentneedsofruralandurbanareas.Asoneparticipantshared,“Whatweneedin[ruralareas]isnothinglikewhattheyneedinLaredo[urban].Our[rural]needsareverydifferentandsadly,overlooked.”ThissentimentalsocameupinMcAllen,TX,whereoneindexcardsubmissionread,“Iwonderwhattheoutcomeswould’vebeenifsmallercoloniasoutsideofthe[RioGrande]Valleywereinterviewed;Ibettheyneverare.”AparticipantinCorpusChristi,TXalsoexplainedtheimportanceofconsideringculturalnuanceswhenframingdiscussionsbyavoidinglanguagethatovergeneralizesantiquatedculturalnorms--forexample,notassumingthatallmenoperatefroma“machismo”perspective,theconceptassociatedwith"astrongsenseofmasculinepride”.Further,participantsstressedtheneedforusinglanguageandterminologythatwasaccessible,clear,andfreeofnegativeconnotations(e.g.,“patient”couldconnoteonewhoisapassiverecipientofinformationratherthananactiveparticipantinhis/herownhealth).Intermsofengagingwithresearch,participantsemphasizedtheimportanceoffollow-upandrapportbuildingamongprovidersandresearchers;theneedforface-to-facecommunicationwasseenascrucialforthisprocess.Apartfromface-to-facecontact,town-hallparticipantssuggestedhighlightingqualitativestoriesinmarketingeffortsinorderto“understandthepersonvs.aggregatedata.”
ConsideraMixed-methodsCommunicationStrategyforFutureEndeavorsParticipantsacrossgeographiespreferredamixed-methodcommunicationstrategyforhealth-relatedinformation.Focusgroupandtownhallparticipantsalikecitedthatin-personandface-to-faceinteractionswerethepreferredmethodsofdisseminatingresearch-relatedinformation—withthecaveatthatthisinformationshouldcomefromtrustedsources.Modesofpreferredwrittenororalcommunicationalsodifferedbymunicipalities,butword-of-mouthandtheInternetwerereportedasthemosttrustedsourcestoreceivehealth-relatedinformation.Thenextmostfrequentlycitedincludedlocalradio,communityevents,andflyers.Lastly,participantsstressedtheimportanceofunderstandingtheuniquecommunitiesbeingengagedbeforedisseminatinghealth-informationandresearchopportunities.
AFocusonPreventionandWellnessSimilartokeyfindingsintheprevioussessions,EngagingtheCommunityVoicetown-hallparticipantsoverwhelmingagreedthattherearenotenoughresourcesallocatedforprimarypreventioneffortsonasystems-widebasisforinitiativessuchassmokingcessation,physicaleducationinschools,andhealthliteracy.Asoneintervieweeobserved,“AllofusshouldagreethatP.E.needstobearequirementinschoolstomakesureourkidsareexercising.”Participantssuggestedmoreparks,walkablecommunities,andexpandedgrocerystoresinlow-incomeorruralareas;theysuggestedbuildingonexistinghealthylivinginitiativesinthecommunity,butemphasizedtheneedforcontinuityandconsistencyamongwellnessprograms,which,duetofundingcycles,manyreportedaslackinginthepast.Enhancedinformationaboutpreventionwasalsoseenas
8
aneed:asonecommunityparticipantshared,“gettinginformationaboutresourcesshouldbeeasierthanitisnow.”Further,findingnewwaystodeliverhealthcareinunderservedcommunitieswasalsoacommonthemeinconversations,especiallyinruralcommunitiesthatreportedchallengesrecruitingandretainingspecialists.InLaredo,TX,forexample,telemedicinewassuggestedasapossiblestrategytobridgethegapinspecialtycareinprovider-shortageareasthataremorerural.
AddressingtheSocialDeterminantsofHealthAnoverarchingthemeamongthetown-hallmeetingswastheimportanceofaddressingkeybarriers—poverty,accesstocare,transportation,andemployment—alsoknownasthesocialdeterminantsofhealth—thatpreventSouthTexasresidentsfromachievingoptimalhealth.Thisthemeisconsistentwithfindingsfromthethreeprecedingconvenedsessions.Oftheenvironmentalfactorsmentioned,povertyandincreasingaccesstocareweremostfrequentlycitedastopbarrierstoimprovedhealthforlow-incomeresidents.Participantsacknowledgedtheimportanceofconsideringenvironmentalfactorswhenthinkingaboutpopulationhealthacrosstheregion,yettherewasoverwhelmingagreementthatthiswasnotcurrentlythestate’sapproach.Thisgapcreatedfutureresearchopportunitiestostudytheimpactsofthesesocialdeterminantsonpopulationhealth,sharedacademicians,whichcouldbuildthecaseforamoreupstreamapproachtohealthonastatewidebasis.
ImprovedHealthCareAccessAccesstocarewasidentifiedasaconcerninalltown-hallmeetings.Similartothefirstthreesessions,thefollowingbarrierswereidentified:lackofspecialtyproviders—especiallybehavioralhealth—,challengeswithhealthinsurancecoverage,navigatingacomplexhealthsystem,lackofcoordinatedcare,andtransportation.Helpingindividualsobtainandunderstandhealthinsurance,accessingbehavioralhealthservices,andparticipantsidentifiedincreasingservicesforlow-incomeindividualsashighpriorities.Further,manyagreedthatimprovedalignmentandcoordinationwasneededamongthecommunity,hospitals,localinstitutions,andhealthcenters,citingthatitwasdifficulttoknowwhatresourceswereavailable.
MoreEmphasisonPolicyandAdvocacyAnotherthemethatwasprominentamonggroupswasthatmoreeffortsareneededforcollaborationonsystems-levelandpolicychangesatthestateandlocallevels.Moreimportantly,thereisaneedtocontextualizetheworkbeingdoneatthestateandfederallevelthatimpactshealthpayers’,researchers,andproviders’abilitytothinklongitudinallyinregardstopopulationhealth.Participantsnotedthatpolicychangescomeinvaryingshapesandsizes.Someusetheideaof“BigPandLittleppolicy”;aBigPpolicymightbeonethatisatthestatelevelthroughlegislation,regulations,andtaxes,whileLittleppolicyaresmallerinitiatives—possiblyatthelocalgovernment,worksitepolicies/investments,andnormsandstandardsthatdriveotheraction.Acommondiscussionamongparticipantswastheneedtoleverage“Littlep”initiativesandmobilizelocalorganizationsthroughgrassrootsefforts.Asoneparticipantshared,“Thereisnopolicychangewithoutadvocacy;weshouldalsobetalkingabouthowtomobilizethecommunitymovingforward.”Theseeffortsshouldalsoengagelocalofficialsandhealthpayers,sharedparticipants.Thetablebelowsynthesizesthecrosscuttingtown-hallthemesbygeographiclocation(Table1).
9
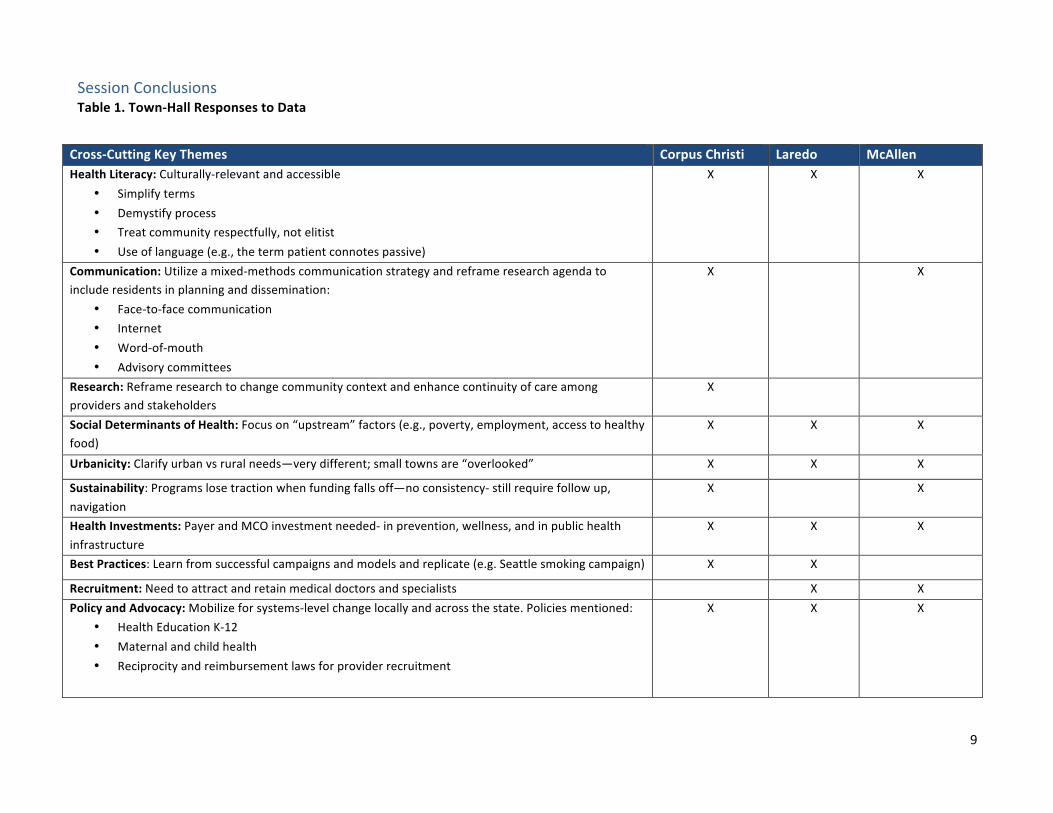
SessionConclusionsTable1.Town-HallResponsestoData
Cross-CuttingKeyThemes CorpusChristi Laredo McAllenHealthLiteracy:Culturally-relevantandaccessible
• Simplifyterms• Demystifyprocess• Treatcommunityrespectfully,notelitist• Useoflanguage(e.g.,thetermpatientconnotespassive)
X X X
Communication:Utilizeamixed-methodscommunicationstrategyandreframeresearchagendatoincluderesidentsinplanninganddissemination:
• Face-to-facecommunication• Internet• Word-of-mouth• Advisorycommittees
X X
Research:Reframeresearchtochangecommunitycontextandenhancecontinuityofcareamongprovidersandstakeholders
X
SocialDeterminantsofHealth:Focuson“upstream”factors(e.g.,poverty,employment,accesstohealthyfood)
X X X
Urbanicity:Clarifyurbanvsruralneeds—verydifferent;smalltownsare“overlooked” X X X
Sustainability:Programslosetractionwhenfundingfallsoff—noconsistency-stillrequirefollowup,navigation
X X
HealthInvestments:PayerandMCOinvestmentneeded-inprevention,wellness,andinpublichealthinfrastructure
X X X
BestPractices:Learnfromsuccessfulcampaignsandmodelsandreplicate(e.g.Seattlesmokingcampaign) X X
Recruitment:Needtoattractandretainmedicaldoctorsandspecialists X XPolicyandAdvocacy:Mobilizeforsystems-levelchangelocallyandacrossthestate.Policiesmentioned:
• HealthEducationK-12• Maternalandchildhealth• Reciprocityandreimbursementlawsforproviderrecruitment
X X X
10
BUILDINGTHEPATIENT-CENTEREDPARTNERSHIP
OverviewInthefinalafternoonplanningsessioninMcAllenfollowingthecommunitytown-hallmeeting,participantsbegantheprocessofidentifyingthekeyelementsoftheCollaborativeResearchFramework,describedasBuildingthePatient-CenteredPartnership,whichincludesboththefocusoftheresearch,aswellasthespecificstrategiesfordevelopingandsustainingthecollaborativepartnershipandeffectivelydisseminatingtheresearchtokeygroupsinthecommunity.
MethodsDuringthissession,participantsbrokeintodifferentconfigurationsofsmallworkgroupstoanswerquestionsaboutthecontentandsharedmetricsfortheresearch;thecomponentsthatwouldsupportcollaboration,withastrongfocusonauthenticengagement;keycriteriaforselectingpartnersinthecollaborativeeffort;potential“quickwins”thatcouldbedevelopedandachievedintheneartermtosustainenthusiasmandmomentum;andcriticalgroups/individualswhoshouldbeatthetableforthenextstageofplanning.Thefollowingsectionsummarizesthesekeythemesbytopicarea.
SessionFindingsandKeyThemesKeyThemes:ContentandMetrics
• Chronicdiseasesandtheirriskfactors—especiallydiabetes,obesity,heartdisease,andcancer—werereportedasprioritycontentareastoconsiderforafuturecollaborativeresearchagenda.Participantswereespeciallyconcernedabouttheperceivedincreaseinchildhoodobesity.Asoneresidentshared,“moreandmoreofourkidsareoverweighttoo;weshouldbefocusingonwhatkidsareeatingatschoolsandathome.”Competingtimecommitments,theavailabilityofaccessibleandaffordablehealthyfood,andculturalnormswereattributedaschallengestomaintainingahealthyweight.Again,participantsstressedaneedforresearch-informedsystems-levelstrategiestopromotehealthyeatingandphysicalactivitytoreducechronicillnessinthecommunity;examplesofstrategiesincludedrequirementsforphysicaleducationinschools,healthyschoollunchprograms,andworksitewellnessinitiatives.
• Inadditiontolookingatchronicdiseasesandtheirriskfactors,participantsalsosharedtheimportanceofaccesstohealthyfoodasatopconcern.Manyparticipantsdescribedmultiplepocketsoffooddesertsintheregionthatmadeaccesstohealthyfoodsdifficult.Thisproblem,sharedparticipants,wasexacerbatedbylimitedtransportationoptions.Participantssuggestedthatfutureresearchtopicareascouldexploresuccessfulmodelsofruralmobilefoodoutreach,andtheimpactoflocalfarmssupplyinglocalmarketswithhealthyfood.
• Mentalhealth–whichoftenco-occurswithsubstanceabuse,wasidentifiedasatophealthissueinthecommunity;especiallynotedwasthelackofservicestoaddressthesegrowingbehavioralhealthissues.Participantsdescribedissuesofanxiety,stressandsubstanceabuseforadults—largelyattributedtopoverty—asthemostcommonconcerns.SessionparticipantsinbothLaredoandMcAllenexplainedthechallengesofbehavioralhealthservicesbecauseoflimitedproviders,reimbursementmodelsforbehavioralhealth,andstigma.Futureresearchtopicsdiscussedincludedtheintersectionofpovertyandmentalhealthdiagnoses,anti-povertyinitiatives,andaccesstosubstanceabusetreatmentservicesthatwereculturallyrelevant.
11
• Thebuiltenvironment—especiallytransportation,safe,walkablecommunities,andfoodaccess—werereportedasareastoexploremovingforward.Thesekeydeterminantsofhealthwereseenasimpedingimprovedhealth,especiallyforlow-incomeresidentswholiveinareaswithlimitedinfrastructure.Whileindividualchallengessuchastimeconstraintswerementionedasbarrierstoahealthylifestyle,structuralchallengessuchaslivinginafooddesertandhavinglimitedaccesstosidewalksaroseasaprominentthemeamongdiscussionsforfutureresearchtopicareastoexplore.
Participantswereaskedtosuggestpossibleindicatorstoincludeinfutureresearchendeavors.Thetablebelowshowstopicareaandindicatorsthatwerediscussedduringthissession.Topics IndicatorsChronicDiseasesandRiskFactors • HbA1c,BMI
• Ratesofmedicationadherence• UtilizationofEmergencyMedicalServices• Diseaseincidenceandmortality
AccesstoHealthyFoods • SupermarketspercapitaMentalHealth • NonediscussedBuiltEnvironment • Publictransportationroutes
KeyThemes:Components/StrategiesthatSupportCollaboration,Communication,andEngagementGroupsalsodiscussedwhatcomponentsorstrategieswouldbeessentialtoconsiderwhencraftingthecollaborativeframework.Amongthemostfrequentlycited,ensuringthatpartnershadsharedvisionsandgoals,clearexpectationsregardingrolesandresponsibilities,andaplanforsustainabilityweremostprominent.Inlinewithfindingsfromtheprevioussessionsandtownhalls,participantsalsostressedtheimportanceofaneutralconvenertobringinstitutionstogether.Intermsofcommunication,sessionparticipantssuggestedmonthlymeetingsorquarterlymeetingswherestakeholderscouldidentifyareasofcollaborationanddiscussneedsandopportunitiesonanon-goingbasis.Communityengagementwouldalsobeessentialthroughoutthisprocess,anddeliberateopportunitiesforengagementshouldbecreatedtosupportinclusion.Participantsstressedtheimportanceofnotmakingcommunitymembersfeel“actedupon”or“experimentedwith”butrathermeaningfullyandsubstantivelyengagedinprocessesthatareimportanttothem.Specificsuggestionsincluded:bilingualmeetings,minimaluseofacronymsandjargon,transportationsupporttoandfrommeetings,childcaresupport,andcommunitypanels.Similartothetown-hallfindings,participantsstressedtheneedforamixed-methodscommunicationstrategytoengageresidentswhowerenotinvolvedinongoingdiscussionsofpatient-centeredresearch.Specifically,in-personinteractions,localradio,andcommunityeventswerethemostfrequentlysuggestedwaystodisseminateinformationandinvitefeedback.Participantsexpressedfrustrationovercomplicatedjargonandacronymsandstressedtheimportanceofconsideringliteracylevelsandterminologywhendisseminatinghealth-relatedandresearchinformation.ProvidingalaysummaryofstudyfindingsinbothEnglishandSpanishwerestrategiesmentionedbyfocusgroupparticipants.Lastly,theimportanceoffollow-upandfollow-
12
throughwasdiscussedasacriticalfactorforbuildingtrustandmaintainingeffectiverelationships;thosewhoareaskedtoprovideinformationorinput,ortoparticipateinsomewayinaresearchstudy,shouldbeinformedoftheresultsoftheirinvolvement.Finally,itshouldbereiteratedthatthroughouttheseconversations,theimportanceofkeepingsystems-levelstrategiestop-of-mindwasseenascritical.Specificsuggestionsincludedlookingatcurrentpolicyproposalsandaddingvoice/weightatthelocallevelthroughadvocacydays;buildingadvocacycapacityintheregionthroughawarenessandtraining;andusingreturnoninvestment-basedargumentsforstakeholderssuchashealthpayersandacademicians.Participantsexplainedthatthefoundationforthisworkhasalreadybegunthroughvariousorganizationsthroughouttheregion,andsuggestedcollaboratingandsupportingthoseeffortssoastonot“reinventthewheel.”Specificstrategieswerediscussedamongparticipantsthroughoutthissession.Thefollowingtablesummarizesthecomponentsandstrategiesreferenced.Components StrategyCommunicationandDissemination
• Createacommunicationanddisseminationstrategythroughtrustedcommunityorganizations
• Decreaseacronymsandresearch-specificjargon;accommodatelanguagepreference
• RegularmeetingswithstakeholdersPolicyandAdvocacy • Buildadvocacycapacityatthelocallevel
• Continuouslyreiteratethehistoryoftheresearchprocess(i.e.,wherehavetheybeenandwherearetheynow?)
• Increaseknowledgeofhealthcarepolicies• Plantore-alignincentivestofocusonpreventionandwellness
Collaboration • Plantoreducecompetitionamongprovidersandinstitutions• Sharedtemplatesforpartnershipagreements• Regularconveningbothwithinsectorsandacrosssectors• Sustainabilityplanning
KeyThemes:PartnershipInclusionCriteria(andwhoshouldbeatthetable)Alsodiscussedwerepartnershipcriteriatoconsiderwhenmovingforwardwithplanningprocesses.Participantssharedthathavingsimilartargetpopulations,alignedvisionsandgoals,andstrongcredibilityinthecommunitywereamongthemostimportantwhenselectingpotentialpartnersforthecollaborativeresearchprocess.Theneedforaneutralconvenertoensurethatpartnerswereheldaccountablewasdescribedasacritical,butcurrentlyunidentified,componenttosuccess.Lastly,therewasdiscussionaroundtheneedtohavediversesectorsrepresentedinfuturepartnerships.Forexample,participantsdiscussedthebenefitsofhavingamixoflocalinstitutionswithestablishedrapport,andcorporateinstitutionswithawiderreach,atthesametable.Asanote,therewasastrongefforttorecruitdiversesectorsintheseconversations,however,morecanbedonetoengageentitiesthathavenothistoricallybeeninvolvedinhealthandphilanthropicinitiatives.Specificstakeholdersidentifiedinthissessionincluded:
13
• Policymakers-local,regional,state• UniversitiesandCommunityColleges• CountyHealthDepartments• CommunityProviders
• Legalcounselfororganizations• Promotorasandcommunityhealth
workers• Medicalschoolsandmedicalresidents
KeyThemes:QuickWinsTheBuildingthePatient-CenteredPartnershipsessionconcludedwithadiscussionaroundpossible“quickwins”tofocusonwhencreatingasharedresearchframework.Strengtheningandleveragingestablishedpartnershipsthroughfrequentconvenedsessionsandsummitswouldbeaquick-wintoincreasecollaborationandcommunication.Intermsofaccesstocare,participantssuggestedleveragingmobileclinicstoincreasethereachofvulnerablepopulationsorpatientswithoutestablished“medical-homes”.Lastly,thereareavarietyofdefinitionsandtermsusedwhendiscussingcommunityengagement,andsharedlanguage—includingdefinitionsanddefinedprocessesandexpectations—wouldbehelpfulmovingforward.
SessionConclusionsInordertostrengthenthefoundationalworkthathasbeenestablishedthroughthePCORIproject,apotentialnextstepistore-engageacademiciansandresearcherswhoparticipatedintheKnowledgeSharingChampionssessioninordertofurtherreflectontheoutcomesofthisreportandtocontinuetheprocessofoutliningaCollaborativeResearchFrameworkandplanthatwouldincludealloftheelementsabove,aswellasmorespecificstrategiesarounddecisionmakingstructureandaccountability,financialstructureandincentives,sustainabilityandscalability,datasharing,anddissemination.
14
LISTOFAPPENDICES
Appendix1 EngagingtheCommunityVoiceAgenda
Appendix2 EngagingtheCommunityVoiceParticipantList
Appendix3 BuildingthePatient-CenteredPartnershipAgenda
Appendix4 BuildingthePatient-CenteredPartnershipParticipantList
Appendix5 DefinitionsofTerms
15
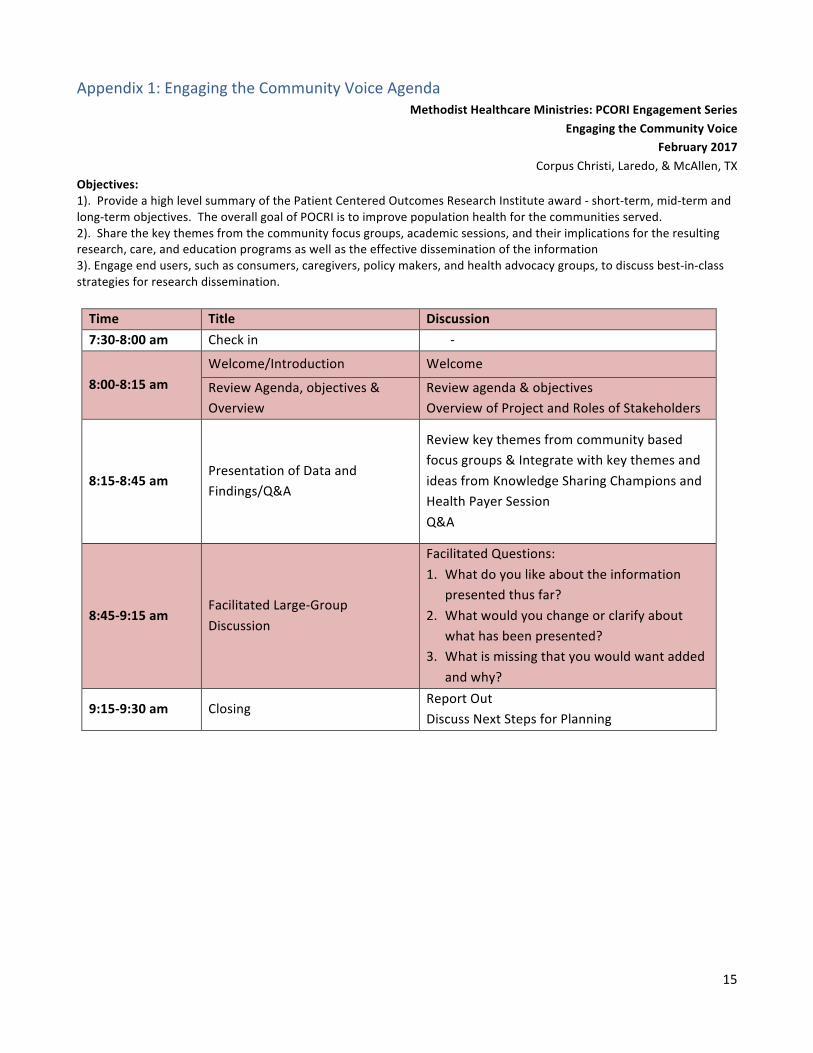
Appendix1:EngagingtheCommunityVoiceAgendaMethodistHealthcareMinistries:PCORIEngagementSeries
EngagingtheCommunityVoiceFebruary2017
CorpusChristi,Laredo,&McAllen,TXObjectives:1).ProvideahighlevelsummaryofthePatientCenteredOutcomesResearchInstituteaward-short-term,mid-termandlong-termobjectives.TheoverallgoalofPOCRIistoimprovepopulationhealthforthecommunitiesserved.2).Sharethekeythemesfromthecommunityfocusgroups,academicsessions,andtheirimplicationsfortheresultingresearch,care,andeducationprogramsaswellastheeffectivedisseminationoftheinformation3).Engageendusers,suchasconsumers,caregivers,policymakers,andhealthadvocacygroups,todiscussbest-in-classstrategiesforresearchdissemination.
Time Title Discussion7:30-8:00am Checkin -
8:00-8:15amWelcome/Introduction Welcome
ReviewAgenda,objectives&Overview
Reviewagenda&objectivesOverviewofProjectandRolesofStakeholders
8:15-8:45amPresentationofDataandFindings/Q&A
Reviewkeythemesfromcommunitybasedfocusgroups&IntegratewithkeythemesandideasfromKnowledgeSharingChampionsandHealthPayerSessionQ&A
8:45-9:15amFacilitatedLarge-GroupDiscussion
FacilitatedQuestions:1. Whatdoyoulikeabouttheinformation
presentedthusfar?2. Whatwouldyouchangeorclarifyabout
whathasbeenpresented?3. Whatismissingthatyouwouldwantadded
andwhy?
9:15-9:30am ClosingReportOutDiscussNextStepsforPlanning
16
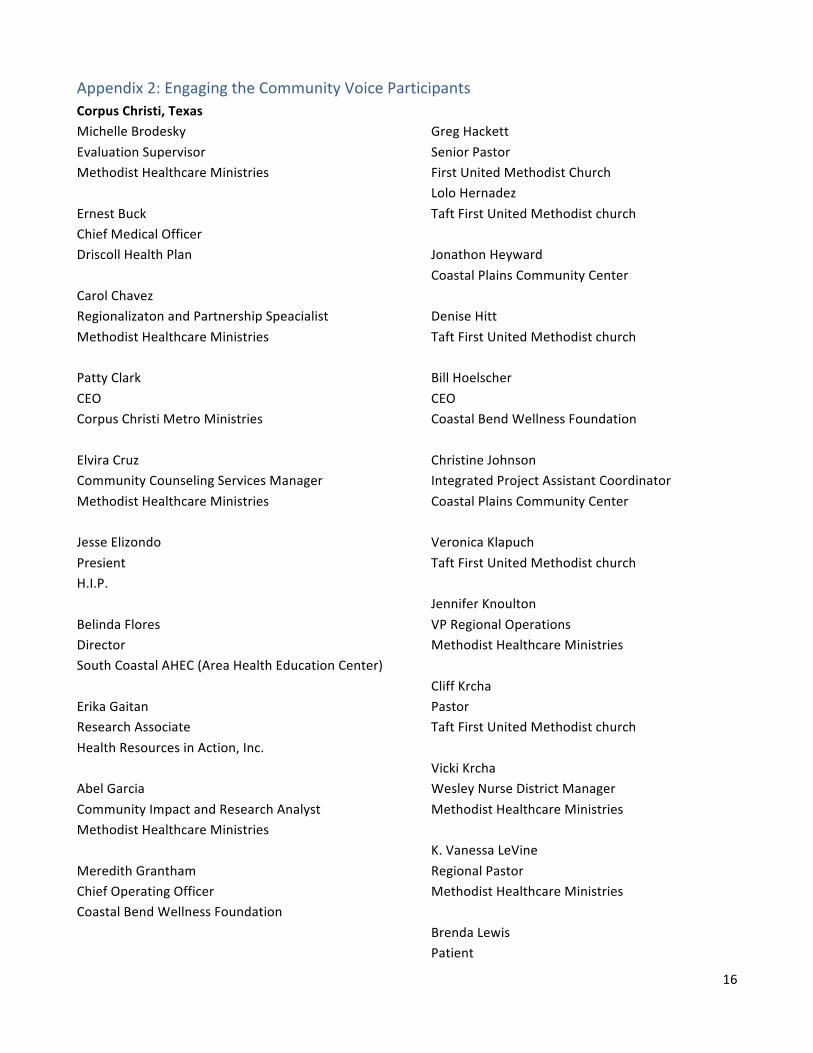
Appendix2:EngagingtheCommunityVoiceParticipantsCorpusChristi,TexasMichelleBrodeskyEvaluationSupervisorMethodistHealthcareMinistriesErnestBuckChiefMedicalOfficerDriscollHealthPlanCarolChavezRegionalizatonandPartnershipSpeacialistMethodistHealthcareMinistriesPattyClarkCEOCorpusChristiMetroMinistriesElviraCruzCommunityCounselingServicesManagerMethodistHealthcareMinistriesJesseElizondoPresientH.I.P.BelindaFloresDirectorSouthCoastalAHEC(AreaHealthEducationCenter)ErikaGaitanResearchAssociateHealthResourcesinAction,Inc.AbelGarciaCommunityImpactandResearchAnalystMethodistHealthcareMinistriesMeredithGranthamChiefOperatingOfficerCoastalBendWellnessFoundation
GregHackettSeniorPastorFirstUnitedMethodistChurchLoloHernadezTaftFirstUnitedMethodistchurchJonathonHeywardCoastalPlainsCommunityCenterDeniseHittTaftFirstUnitedMethodistchurchBillHoelscherCEOCoastalBendWellnessFoundationChristineJohnsonIntegratedProjectAssistantCoordinatorCoastalPlainsCommunityCenterVeronicaKlapuchTaftFirstUnitedMethodistchurchJenniferKnoultonVPRegionalOperationsMethodistHealthcareMinistriesCliffKrchaPastorTaftFirstUnitedMethodistchurchVickiKrchaWesleyNurseDistrictManagerMethodistHealthcareMinistriesK.VanessaLeVineRegionalPastorMethodistHealthcareMinistriesBrendaLewisPatient
17
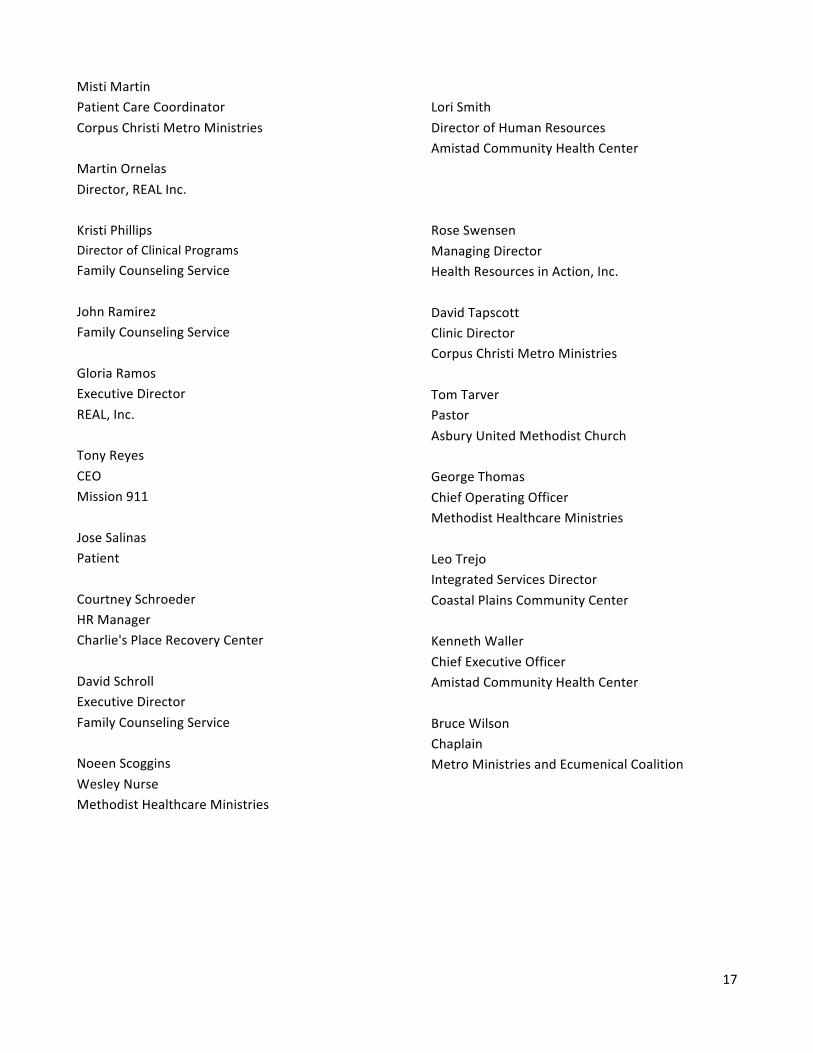
MistiMartinPatientCareCoordinatorCorpusChristiMetroMinistriesMartinOrnelasDirector,REALInc.KristiPhillipsDirectorofClinicalProgramsFamilyCounselingServiceJohnRamirezFamilyCounselingServiceGloriaRamosExecutiveDirectorREAL,Inc.TonyReyesCEOMission911JoseSalinasPatientCourtneySchroederHRManagerCharlie'sPlaceRecoveryCenterDavidSchrollExecutiveDirectorFamilyCounselingServiceNoeenScogginsWesleyNurseMethodistHealthcareMinistries
LoriSmithDirectorofHumanResourcesAmistadCommunityHealthCenterRoseSwensenManagingDirectorHealthResourcesinAction,Inc.DavidTapscottClinicDirectorCorpusChristiMetroMinistriesTomTarverPastorAsburyUnitedMethodistChurchGeorgeThomasChiefOperatingOfficerMethodistHealthcareMinistriesLeoTrejoIntegratedServicesDirectorCoastalPlainsCommunityCenterKennethWallerChiefExecutiveOfficerAmistadCommunityHealthCenterBruceWilsonChaplainMetroMinistriesandEcumenicalCoalition
18
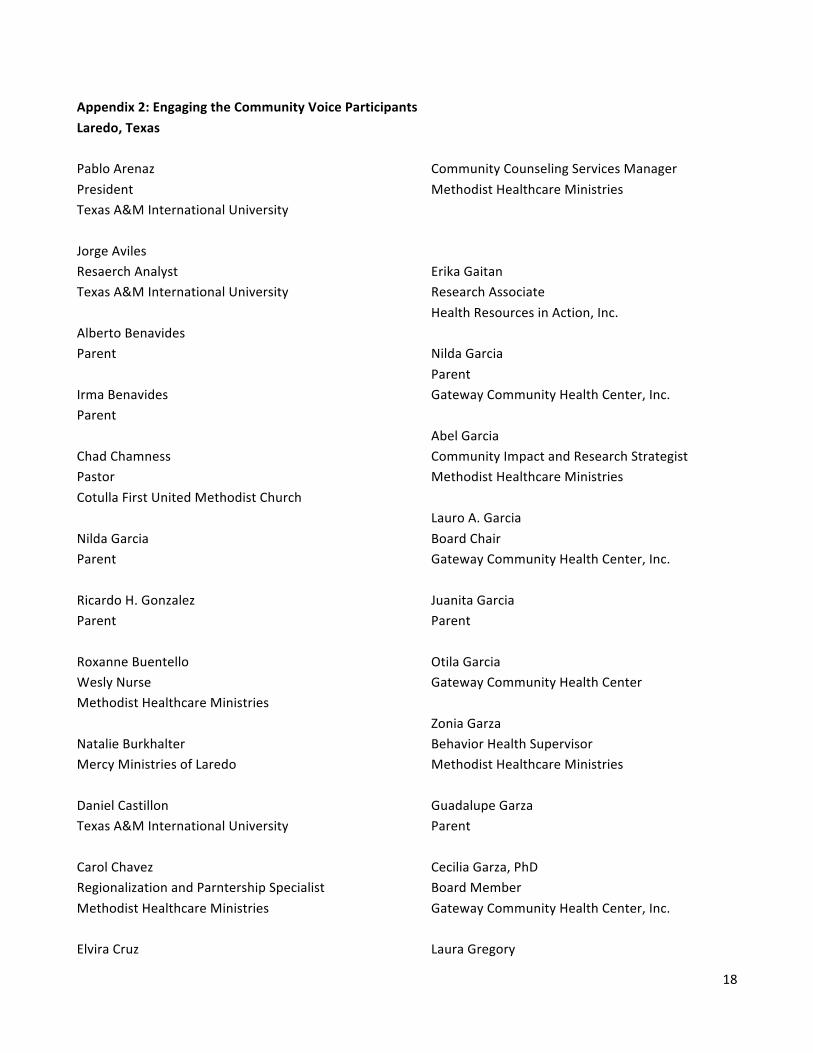
Appendix2:EngagingtheCommunityVoiceParticipantsLaredo,TexasPabloArenazPresidentTexasA&MInternationalUniversityJorgeAvilesResaerchAnalystTexasA&MInternationalUniversityAlbertoBenavidesParentIrmaBenavidesParentChadChamnessPastorCotullaFirstUnitedMethodistChurchNildaGarciaParentRicardoH.GonzalezParentRoxanneBuentelloWeslyNurseMethodistHealthcareMinistriesNatalieBurkhalterMercyMinistriesofLaredoDanielCastillonTexasA&MInternationalUniversityCarolChavezRegionalizationandParntershipSpecialistMethodistHealthcareMinistriesElviraCruz
CommunityCounselingServicesManagerMethodistHealthcareMinistriesErikaGaitanResearchAssociateHealthResourcesinAction,Inc.NildaGarciaParentGatewayCommunityHealthCenter,Inc.AbelGarciaCommunityImpactandResearchStrategistMethodistHealthcareMinistriesLauroA.GarciaBoardChairGatewayCommunityHealthCenter,Inc.JuanitaGarciaParentOtilaGarciaGatewayCommunityHealthCenterZoniaGarzaBehaviorHealthSupervisorMethodistHealthcareMinistriesGuadalupeGarzaParentCeciliaGarza,PhDBoardMemberGatewayCommunityHealthCenter,Inc.LauraGregory
19
ParentMariaHerreraParentJenniferKnoultonVPofRegionalOperationsMethodistHealthcareMinistriesElmoLopezCEOGatewayCommunityHealthCenterMaraLopez-MaldonadoDirectorofMarketingMargaritaG.MendozaParentLourdesRangelGatewayCommunityHealthCenterMarioA.RenteriaJr.ParentMariaTeresaSifuentesParent
RoseSwensenManagingDirectorHealthResourcesinAction,Inc.GeorgeThomasChiefOperatingOfficierMethodistHealthcareMinistriesClaraluzVelascoParentSisterMariaLuisaVeraCEOMercyMinistriesofLaredoParticiaVillarrealWesleyNurseDistrictManagerMethodistHealthcareMinistriesSusanWalkerEvaluationconsultantMercyMinistriesofLaredoElenaWeatherholtParentAlfredoZamoraCEOSouthTexasRuralHealthServices
20
Appendix 3: Building the Patient-Centered Partnership Agenda
MethodistHealthcareMinistries:PCORIEngagementSeriesBuildingthePatient-CenteredPartnership
February2017 McAllen,TX
Time Title Discussion
9:00-9:15amWelcome/Introduction Welcome
ReviewAgenda,objectives&Overview Reviewagenda&objectivesOverviewofProjectandRolesofStakeholders
9:15-9:45am PresentationofDataandFindings/Q&A
Reviewkeythemesfromcommunitybasedfocusgroups&IntegratewithkeythemesandideasfromKnowledgeSharingChampionsandHealthPayerSessionQ&A
9:45-10:30am FacilitatedLarge-GroupDiscussion
Asklarge-groupthreequestionsandbringtogethertoreportout.1. Whatdoyoulikeabouttheinformation
presentedthusfar?2. Whatwouldyouchangeorclarifyabout
whathasbeenpresented?3. Whatismissingthatyouwouldwant
addedandwhy?11:15-11:45am Networkinglunch
11:45-12:30pm Synthesisonallthetown-hallsinformation
Recapinformationgatheredthroughoutthe3town-halls
12:30-1:30pm1:30-1:45
ContentAreaandMetricsDiscussion1) Whichcontentareasandmetricsshouldwefocusonforcollaborativepatient
centeredresearchmodel?2) Whatcomponentsareessentialtosupportcollaborativepatient-centeredresearch3) Whatistheinclusioncriterianeededtomoveforwardwithpartnerships?
Break
1:45-2:15
BuildingConsensus1. Whatisthecurrentstateofpatientcenteredresearch,includingchallenges,
enablersandopportunities?2. Whatarepossiblestrategiestoaddressthese?
2:15-3:00pm
Large-GroupPlanning1. Whatarequickwinstoworktowards?2. Whatisourlong-termstrategytomoveagendaforward?3. Whoneedstobeatthetable?
3:00-3:15pm Reportout
21
Appendix 4: Building the Patient-Centered Partnership Participants McAllen,TXBeatrizAlanizBehavioralHealthCounselorMethodistHealthcareMinistriesConradoAlvaradoExecutiveDirectorTexasHealthPlanUnitedHealthcareCommunity&StateCiaraAyalaCommunityOutreachSpecialistLaUniondelPuebloEnteroKendallBandaProgramCoordinatorTexasA&MUniversityTimBarrCollectiveImpactStrategyManagerMethodistHealthcareMinistriesAthenaBournakisProgramAssistantValleyBaptistLegacyFoundationLuisCaloMedicalDirectorUnitedHealthcareRobertChapaCommunityCounselingServicesSupervisorMethodistHealthcareMinistriesTaniaChavezFundDevelopmentStrategistLaUniondelPuebloEnteroCarolChavez
RegionalizationandPartnershipSpecialistMethodistHealthcareMinistriesMariaDillMedicalDirectorRioGrandeStateCenterMonikaFloresProgramManagerTropicalTexasBehaviorHealthErikaGaitanResearchAssociateHealthResourcesinAction,Inc.AbelGarciaCommunityImpactandResearchStrategistMethodistHealthcareMinistriesEvelynGarzaProgramsAssoicateValleyBaptistLegacyFoundationRobertoGonzalezSiTexas-JuntosCommunityOutreachCoordinatorTexasA&MInternationalUniversityJenniferKnoultonVPRegionalOperationsMethodistHealthcareMinistriesGraceLawsonExecutiveDirectorLowerRioGrandeValleyCommunityHealthManagementKVanessaLeVine
22
RegonalPatorMethodistHealthcareMinistriesStephanieMandujanoGrantsSpecialistMethodistHealthcareMinistriesSandraMartinezCommunityImpact&AdvocacyStrategistManagerMethodistHealthcareMinistriesAmiraMaya-MartinezCommunityBasedCounselorMethodistHealthcareMinistriesVivianaMartinezSiTexas-JuntosforBetterHealthProgramDirectTexasA&MInternationalUniversityStephanieMcClainProjectManagerSiTexasMethodistHealthcareMinistriesYajairaNavaPublicRelationsAdvocateHopeFamilyHealthCenterMichaelPerezDirectorofPlanningandCommunicationsBehavioralHealthSolutionsofSouthTexasJudyQuisenberryGrantsDirectorValleyBaptistLegacyFoundationMarisolResendezAdministrativeAssistantElMilagroClinic
IreliaRiosWesleyNurseMethodistHealthcareMinistriesPerlaRiveraWesleyNurseMethodistHealthcareMinistriesJohnP.RonnauSeniorAssociateDeanforInterprofessionalEducationUTRGVSchoolofMedicinePedroSanchezCommunityBasedCounselorMethodistHealthcareMinistriesRuthanneSharrowCommunityBasedCounselorMethodistHealthcareMinistriesRoseSwensenManagingDirectorHealthResourcesinAction,Inc.LauraTrevinoAssociateRegionalDirector,LowerRioGrandeRegionTexasA&MInternationalUniversityJuanitaValdez-CoxDirectorLaUniondelPuebloEntero(LUPE)MaryValenciaClinicDirectorRioGrandeStateCenterCandyWileyWesleyNurseMethodistHealthcareMinistries

23
24
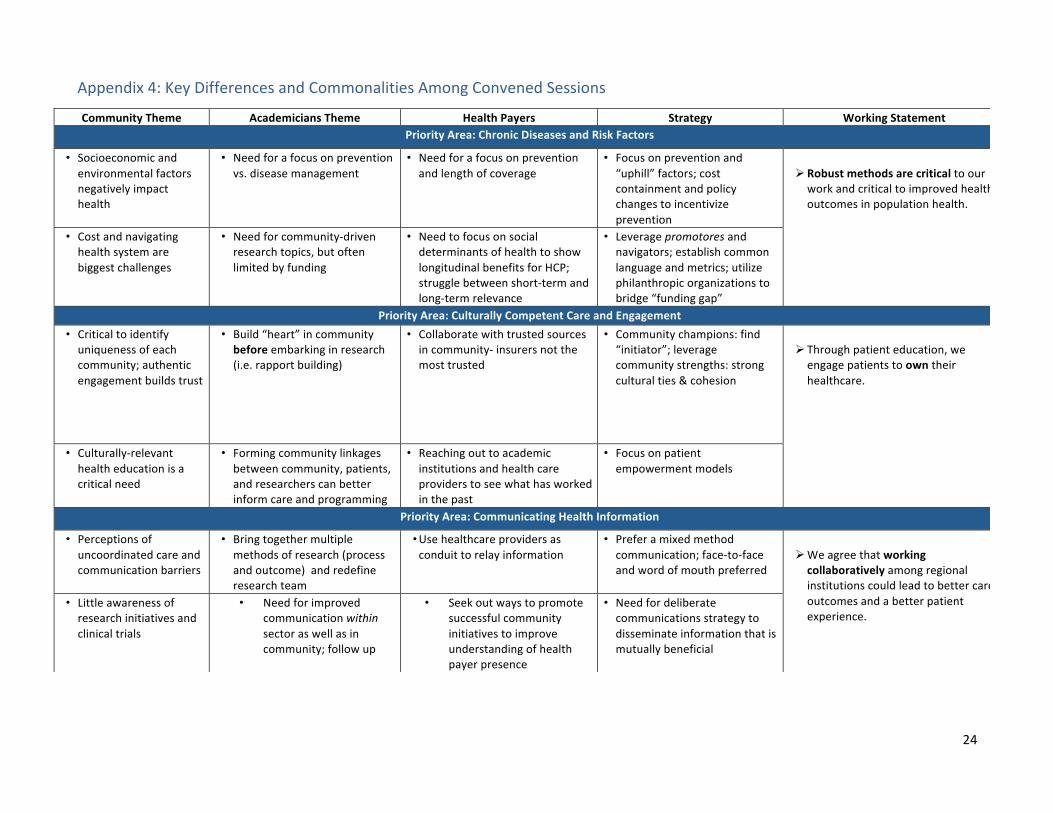
Appendix4:KeyDifferencesandCommonalitiesAmongConvenedSessions
CommunityTheme AcademiciansTheme HealthPayers Strategy WorkingStatementPriorityArea:ChronicDiseasesandRiskFactors
• Socioeconomicandenvironmentalfactorsnegativelyimpacthealth
• Needforafocusonpreventionvs.diseasemanagement
• Needforafocusonpreventionandlengthofcoverage
• Focusonpreventionand“uphill”factors;costcontainmentandpolicychangestoincentivizeprevention
Ø Robustmethodsarecriticaltoourworkandcriticaltoimprovedhealthoutcomesinpopulationhealth.
• Costandnavigatinghealthsystemarebiggestchallenges
• Needforcommunity-drivenresearchtopics,butoftenlimitedbyfunding
• NeedtofocusonsocialdeterminantsofhealthtoshowlongitudinalbenefitsforHCP;strugglebetweenshort-termandlong-termrelevance
• Leveragepromotoresandnavigators;establishcommonlanguageandmetrics;utilizephilanthropicorganizationstobridge“fundinggap”
PriorityArea:CulturallyCompetentCareandEngagement• Criticaltoidentifyuniquenessofeachcommunity;authenticengagementbuildstrust
• Build“heart”incommunitybeforeembarkinginresearch(i.e.rapportbuilding)
• Collaboratewithtrustedsourcesincommunity-insurersnotthemosttrusted
• Communitychampions:find“initiator”;leveragecommunitystrengths:strongculturalties&cohesion
Ø Throughpatienteducation,weengagepatientstoowntheirhealthcare.
• Culturally-relevanthealtheducationisacriticalneed
• Formingcommunitylinkagesbetweencommunity,patients,andresearcherscanbetterinformcareandprogramming
• Reachingouttoacademicinstitutionsandhealthcareproviderstoseewhathasworkedinthepast
• Focusonpatientempowermentmodels
PriorityArea:CommunicatingHealthInformation
• Perceptionsofuncoordinatedcareandcommunicationbarriers
• Bringtogethermultiplemethodsofresearch(processandoutcome)andredefineresearchteam
• Usehealthcareprovidersasconduittorelayinformation
• Preferamixedmethodcommunication;face-to-faceandwordofmouthpreferred
Ø Weagreethatworkingcollaborativelyamongregionalinstitutionscouldleadtobettercareoutcomesandabetterpatientexperience.
• Littleawarenessofresearchinitiativesandclinicaltrials
• Needforimprovedcommunicationwithinsectoraswellasincommunity;followup
• Seekoutwaystopromotesuccessfulcommunityinitiativestoimproveunderstandingofhealthpayerpresence
• Needfordeliberatecommunicationsstrategytodisseminateinformationthatismutuallybeneficial
25
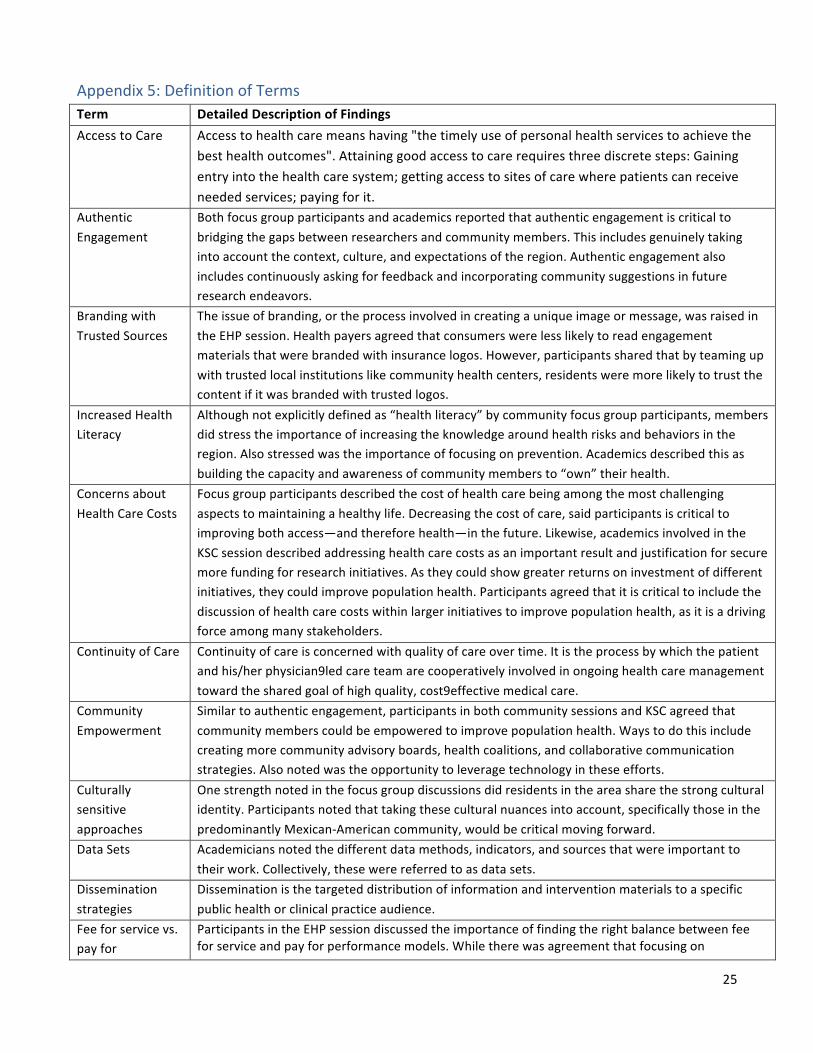
Appendix5:DefinitionofTermsTerm DetailedDescriptionofFindingsAccesstoCare Accesstohealthcaremeanshaving"thetimelyuseofpersonalhealthservicestoachievethe
besthealthoutcomes".Attaininggoodaccesstocarerequiresthreediscretesteps:Gainingentryintothehealthcaresystem;gettingaccesstositesofcarewherepatientscanreceiveneededservices;payingforit.
AuthenticEngagement
Bothfocusgroupparticipantsandacademicsreportedthatauthenticengagementiscriticaltobridgingthegapsbetweenresearchersandcommunitymembers.Thisincludesgenuinelytakingintoaccountthecontext,culture,andexpectationsoftheregion.Authenticengagementalsoincludescontinuouslyaskingforfeedbackandincorporatingcommunitysuggestionsinfutureresearchendeavors.
BrandingwithTrustedSources
Theissueofbranding,ortheprocessinvolvedincreatingauniqueimageormessage,wasraisedintheEHPsession.Healthpayersagreedthatconsumerswerelesslikelytoreadengagementmaterialsthatwerebrandedwithinsurancelogos.However,participantssharedthatbyteamingupwithtrustedlocalinstitutionslikecommunityhealthcenters,residentsweremorelikelytotrustthecontentifitwasbrandedwithtrustedlogos.
IncreasedHealthLiteracy
Althoughnotexplicitlydefinedas“healthliteracy”bycommunityfocusgroupparticipants,membersdidstresstheimportanceofincreasingtheknowledgearoundhealthrisksandbehaviorsintheregion.Alsostressedwastheimportanceoffocusingonprevention.Academicsdescribedthisasbuildingthecapacityandawarenessofcommunitymembersto“own”theirhealth.
ConcernsaboutHealthCareCosts
Focusgroupparticipantsdescribedthecostofhealthcarebeingamongthemostchallengingaspectstomaintainingahealthylife.Decreasingthecostofcare,saidparticipantsiscriticaltoimprovingbothaccess—andthereforehealth—inthefuture.Likewise,academicsinvolvedintheKSCsessiondescribedaddressinghealthcarecostsasanimportantresultandjustificationforsecuremorefundingforresearchinitiatives.Astheycouldshowgreaterreturnsoninvestmentofdifferentinitiatives,theycouldimprovepopulationhealth.Participantsagreedthatitiscriticaltoincludethediscussionofhealthcarecostswithinlargerinitiativestoimprovepopulationhealth,asitisadrivingforceamongmanystakeholders.
ContinuityofCare Continuityofcareisconcernedwithqualityofcareovertime.Itistheprocessbywhichthepatientandhis/herphysician9ledcareteamarecooperativelyinvolvedinongoinghealthcaremanagementtowardthesharedgoalofhighquality,cost9effectivemedicalcare.
CommunityEmpowerment
Similartoauthenticengagement,participantsinbothcommunitysessionsandKSCagreedthatcommunitymemberscouldbeempoweredtoimprovepopulationhealth.Waystodothisincludecreatingmorecommunityadvisoryboards,healthcoalitions,andcollaborativecommunicationstrategies.Alsonotedwastheopportunitytoleveragetechnologyintheseefforts.
Culturallysensitiveapproaches
Onestrengthnotedinthefocusgroupdiscussionsdidresidentsintheareasharethestrongculturalidentity.Participantsnotedthattakingtheseculturalnuancesintoaccount,specificallythoseinthepredominantlyMexican-Americancommunity,wouldbecriticalmovingforward.
DataSets Academiciansnotedthedifferentdatamethods,indicators,andsourcesthatwereimportanttotheirwork.Collectively,thesewerereferredtoasdatasets.
Disseminationstrategies
Disseminationisthetargeteddistributionofinformationandinterventionmaterialstoaspecificpublichealthorclinicalpracticeaudience.
Feeforservicevs.payfor
ParticipantsintheEHPsessiondiscussedtheimportanceoffindingtherightbalancebetweenfeeforserviceandpayforperformancemodels.Whiletherewasagreementthatfocusingon
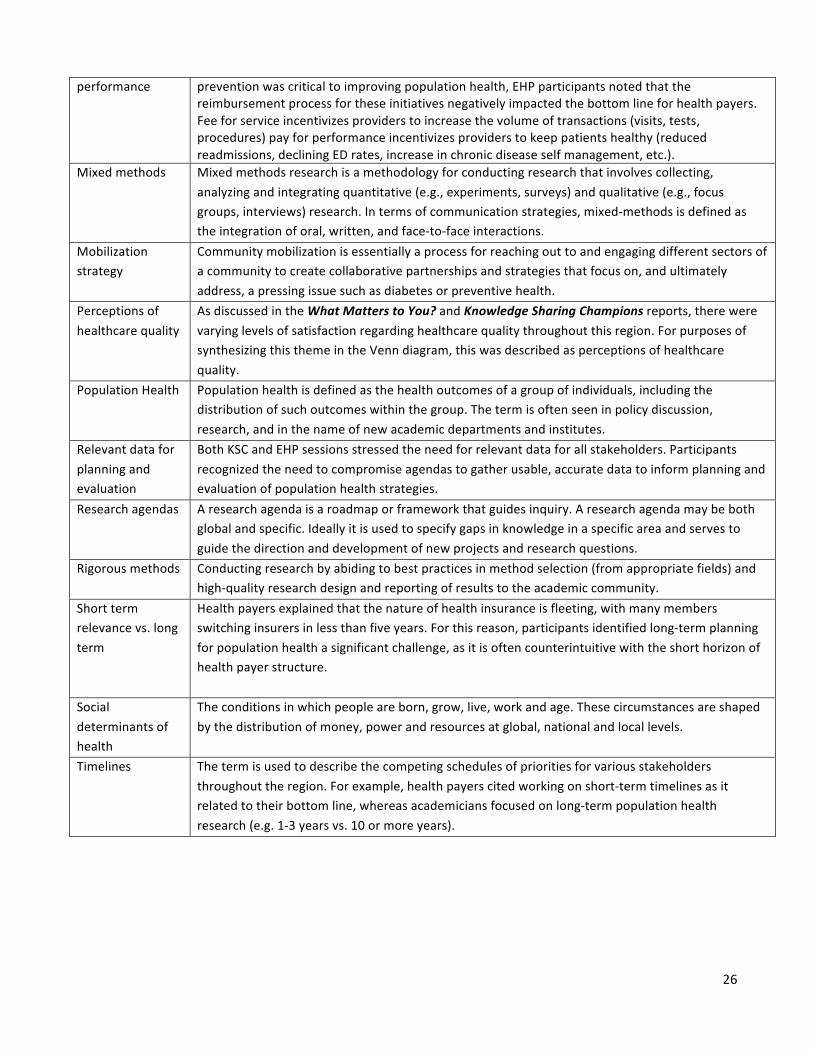
26
performance preventionwascriticaltoimprovingpopulationhealth,EHPparticipantsnotedthatthereimbursementprocessfortheseinitiativesnegativelyimpactedthebottomlineforhealthpayers.Feeforserviceincentivizesproviderstoincreasethevolumeoftransactions(visits,tests,procedures)payforperformanceincentivizesproviderstokeeppatientshealthy(reducedreadmissions,decliningEDrates,increaseinchronicdiseaseselfmanagement,etc.).
Mixedmethods Mixedmethodsresearchisamethodologyforconductingresearchthatinvolvescollecting,analyzingandintegratingquantitative(e.g.,experiments,surveys)andqualitative(e.g.,focusgroups,interviews)research.Intermsofcommunicationstrategies,mixed-methodsisdefinedastheintegrationoforal,written,andface-to-faceinteractions.
Mobilizationstrategy
Communitymobilizationisessentiallyaprocessforreachingouttoandengagingdifferentsectorsofacommunitytocreatecollaborativepartnershipsandstrategiesthatfocuson,andultimatelyaddress,apressingissuesuchasdiabetesorpreventivehealth.
Perceptionsofhealthcarequality
AsdiscussedintheWhatMatterstoYou?andKnowledgeSharingChampionsreports,therewerevaryinglevelsofsatisfactionregardinghealthcarequalitythroughoutthisregion.ForpurposesofsynthesizingthisthemeintheVenndiagram,thiswasdescribedasperceptionsofhealthcarequality.
PopulationHealth Populationhealthisdefinedasthehealthoutcomesofagroupofindividuals,includingthedistributionofsuchoutcomeswithinthegroup.Thetermisoftenseeninpolicydiscussion,research,andinthenameofnewacademicdepartmentsandinstitutes.
Relevantdataforplanningandevaluation
BothKSCandEHPsessionsstressedtheneedforrelevantdataforallstakeholders.Participantsrecognizedtheneedtocompromiseagendastogatherusable,accuratedatatoinformplanningandevaluationofpopulationhealthstrategies.
Researchagendas Aresearchagendaisaroadmaporframeworkthatguidesinquiry.Aresearchagendamaybebothglobalandspecific.Ideallyitisusedtospecifygapsinknowledgeinaspecificareaandservestoguidethedirectionanddevelopmentofnewprojectsandresearchquestions.
Rigorousmethods Conductingresearchbyabidingtobestpracticesinmethodselection(fromappropriatefields)andhigh-qualityresearchdesignandreportingofresultstotheacademiccommunity.
Shorttermrelevancevs.longterm
Healthpayersexplainedthatthenatureofhealthinsuranceisfleeting,withmanymembersswitchinginsurersinlessthanfiveyears.Forthisreason,participantsidentifiedlong-termplanningforpopulationhealthasignificantchallenge,asitisoftencounterintuitivewiththeshorthorizonofhealthpayerstructure.
Socialdeterminantsofhealth
Theconditionsinwhichpeopleareborn,grow,live,workandage.Thesecircumstancesareshapedbythedistributionofmoney,powerandresourcesatglobal,nationalandlocallevels.
Timelines Thetermisusedtodescribethecompetingschedulesofprioritiesforvariousstakeholdersthroughouttheregion.Forexample,healthpayerscitedworkingonshort-termtimelinesasitrelatedtotheirbottomline,whereasacademiciansfocusedonlong-termpopulationhealthresearch(e.g.1-3yearsvs.10ormoreyears).