Embed Size (px)
Citation preview

Advances in VA Advances in VA Utilization and Cost DataUtilization and Cost Data
VA HSR&D National MeetingVA HSR&D National Meeting
February 16, 2005February 16, 2005
Mark W. SmithMark W. Smith
Paul BarnettPaul Barnett
Todd WagnerTodd Wagner

Health Economics Resource CenterHealth Economics Resource Center 22
OutlineOutline
1.1. OverviewOverview
2.2. DSS NDEs vs. HERC average cost dataDSS NDEs vs. HERC average cost data
3.3. DSS intermediate product dataDSS intermediate product data
3.3. NPPD prosthetics dataNPPD prosthetics data
4. Fee Basis data4. Fee Basis data

Health Economics Resource CenterHealth Economics Resource Center 33
Study objectives and data needs
VA Utilization
Non-VA Utilization
Patient costs

Health Economics Resource CenterHealth Economics Resource Center 44
VA Utilization
HERC AnnualPerson-level costs
EncounterLevel
DSS IntermediateProduct
Specialty care:e.g., prosthetics

Health Economics Resource CenterHealth Economics Resource Center 55
VA Utilization
HERC AnnualPerson-level costs
EncounterLevel
DSS IntermediateProduct
HERC
DSS
Bedsecn
Discharge
TRT
Discharge
Opat
Opat
Specialty care:e.g., prosthetics
Pharmacy
Med/surg
Rehab, MH,LTC

Health Economics Resource CenterHealth Economics Resource Center 66
VA Utilization
HERC AnnualPerson-level costs
EncounterLevel
DSS IntermediateProduct
HERC
DSS
Bedsecn
Discharge
TRT
Discharge
Opat
Opat
Specialty care:e.g., prosthetics
Pharmacy
Med/surg
Rehab, MH,LTC

Health Economics Resource CenterHealth Economics Resource Center 77
HERC
DSS
Discharge
TRT
Discharge
Opat
Outpatient
Med/surg
Rehab, MH, LTC PTF Bedsection files
PTF Main files
NPCD
PTF Bedsection files
PTF Main files
NPCD
easy
hard
easy
easy
very hard
easy
moderate

Health Economics Resource CenterHealth Economics Resource Center 88
Non -VA Utilization
Paid by VA
Not paid byVA
Fee Basis
Contract Care
Out of pocket
Private Insurance
Medicare/Medicaid

HERC vs DSSHERC vs DSS
Todd WagnerTodd Wagner

Health Economics Resource CenterHealth Economics Resource Center 1010
HERC or DSSHERC or DSS
Strategies for choosing datasetStrategies for choosing dataset– Cost determination methodCost determination method
– VA versus non-VA Relative value unitsVA versus non-VA Relative value units
– Ease of useEase of use

Health Economics Resource CenterHealth Economics Resource Center 1111
Cost Determination MethodCost Determination Method
DSS costs are created using an activity-DSS costs are created using an activity-based costing allocation methodbased costing allocation method
HERC is created using a mixture of HERC is created using a mixture of methodsmethods
Advantage: Advantage: – Inpatient: DSSInpatient: DSS
– Outpatient: TieOutpatient: Tie

Health Economics Resource CenterHealth Economics Resource Center 1212
RVU-based decisionRVU-based decision
DSS is based on VA relative value units DSS is based on VA relative value units (RVUs); hospitals can modify RVUs(RVUs); hospitals can modify RVUs
HERC is based on non-VA RVUs HERC is based on non-VA RVUs (mostly Medicare)(mostly Medicare)
Advantage: depends on audience (slight Advantage: depends on audience (slight advantage to HERC)advantage to HERC)

Health Economics Resource CenterHealth Economics Resource Center 1313
Ease of UseEase of Use
HERC annual person level is easy to useHERC annual person level is easy to use HERC discharge dataset merges to PTF HERC discharge dataset merges to PTF
mainmain– Has subtotal costs and LOS for HERC Has subtotal costs and LOS for HERC
categoriescategories Advantage HERCAdvantage HERC Caveat: HERC may not exist foreverCaveat: HERC may not exist forever

Health Economics Resource CenterHealth Economics Resource Center 1414
AccuracyAccuracy
Is one more accurate?Is one more accurate?
Don’t confuse Don’t confuse precision and precision and accuracyaccuracy

Health Economics Resource CenterHealth Economics Resource Center 1515
AccuracyAccuracy
Hard to quantify accuracy of cost dataHard to quantify accuracy of cost data– Quality changes over timeQuality changes over time
– Varies by medical center and type of careVaries by medical center and type of care
– True costs are unknownTrue costs are unknown Comparisons to other VA or non-VA Comparisons to other VA or non-VA
costs (construct validity)costs (construct validity) Understand the production costsUnderstand the production costs

Health Economics Resource CenterHealth Economics Resource Center 1616
OutliersOutliers
DSS is more subject to outliers than DSS is more subject to outliers than HERCHERC
DSS tries to weed out high cost outliers DSS tries to weed out high cost outliers in production datain production data

Health Economics Resource CenterHealth Economics Resource Center 1717
Identifying Inpatient OutliersIdentifying Inpatient Outliers
Decompose the discharge dataDecompose the discharge data Rehab, MH, LTC:Rehab, MH, LTC:
– Calculate a per diem costCalculate a per diem cost– Multiply per diem by LOSMultiply per diem by LOS– Compare estimated cost to costCompare estimated cost to cost
Med/surgMed/surg– Calculate cost per DRGwt per day; flag records Calculate cost per DRGwt per day; flag records
with >$50000with >$50000

Health Economics Resource CenterHealth Economics Resource Center 1818
SummarySummary Choice of data should be based on:Choice of data should be based on:
– The precision you needThe precision you need
– Level of detailLevel of detail
– Your audienceYour audience Choose a primary database (HERC or DSS)Choose a primary database (HERC or DSS)
– Don’t mix and match DSS and HERCDon’t mix and match DSS and HERC
– Except for HERC with DSS pharmacyExcept for HERC with DSS pharmacy

Health Economics Resource CenterHealth Economics Resource Center 1919
Accuracy and OutliersAccuracy and Outliers
No easy solutionNo easy solution
Consider:Consider:– Comparing costs to other another cost Comparing costs to other another cost
datasetdataset
– Investigate DSS production dataInvestigate DSS production data
– Check accuracy of outliersCheck accuracy of outliers

Health Economics Resource CenterHealth Economics Resource Center 2020
Remainder of WorkshopRemainder of Workshop
DSS Intermediate Product data: DSS Intermediate Product data:
- - Greater granularity on procedures Greater granularity on procedures
National Prosthetics Patient Database (NPPD):National Prosthetics Patient Database (NPPD):- Only source of prosthetics information: cost, type, patients- Only source of prosthetics information: cost, type, patients- Essential for rehab studies, polytrauma patients - Essential for rehab studies, polytrauma patients
Fee Basis data:Fee Basis data:- Non-VA costs excluded from HERC average cost data- Non-VA costs excluded from HERC average cost data- Most non-VA costs excluded from DSS- Most non-VA costs excluded from DSS- Useful for studying outsourcing of care, home-based care- Useful for studying outsourcing of care, home-based care

Health Economics Resource CenterHealth Economics Resource Center 2121
DSS Intermediate Product Detail: DSS Intermediate Product Detail: Looking Inside the Black BoxLooking Inside the Black Box
Paul G. Barnett PhDPaul G. Barnett PhD
Shuo Chen PhDShuo Chen PhD

Health Economics Resource CenterHealth Economics Resource Center 2222
DSS National Data ExtractsDSS National Data Extracts
National files available at VA national National files available at VA national computing center in Austin, TXcomputing center in Austin, TX– Hospital staysHospital stays
– Bed section segment of a stayBed section segment of a stay
– Days in outpatient clinicDays in outpatient clinic
– Day of outpatient pharmacy Day of outpatient pharmacy
– Dispensed prescriptionsDispensed prescriptions

Health Economics Resource CenterHealth Economics Resource Center 2323
Data in DSS National Data ExtractsData in DSS National Data Extracts
Total cost of an encounterTotal cost of an encounter
Some subtotalsSome subtotals

Health Economics Resource CenterHealth Economics Resource Center 2424
Study questionsStudy questions
Where to DSS cost estimates come from?Where to DSS cost estimates come from?
Are they accurate?Are they accurate?– What is importance of previously identified What is importance of previously identified
limitations?limitations?

Health Economics Resource CenterHealth Economics Resource Center 2525
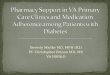
Where do DSS data come from?Where do DSS data come from?
Extracts of DSS- SAS Files at Austin
Cost of stays and visits
DSS VISN Level Production Databases
(a “Black Box” to most researchers)
Cost of intermediate products, stays, visits

Health Economics Resource CenterHealth Economics Resource Center 2626
Where do DSS data come from? Where do DSS data come from?
DSS allocates cost to departments DSS allocates cost to departments
DSS finds quantity of services and products DSS finds quantity of services and products from VISTA (VA electronic medical from VISTA (VA electronic medical records)records)
DSS assigns set of Relative Value Units DSS assigns set of Relative Value Units (RVUs) to each service and product(RVUs) to each service and product

Health Economics Resource CenterHealth Economics Resource Center 2727
Intermediate productIntermediate product
The products (and services) used during a The products (and services) used during a hospital stay or an outpatient encounter, hospital stay or an outpatient encounter, e.g.:e.g.:– Days in wardDays in ward
– Number of chest x-raysNumber of chest x-rays
– Minutes in operating room Minutes in operating room

Health Economics Resource CenterHealth Economics Resource Center 2828
Where do DSS data come from? Where do DSS data come from?
DSS combines department costs with count DSS combines department costs with count of products and RVUs of products and RVUs
DSS determines the cost of each DSS determines the cost of each intermediate productintermediate product
DSS sums the costs of all intermediate DSS sums the costs of all intermediate products used in a stay or visitproducts used in a stay or visit

Health Economics Resource CenterHealth Economics Resource Center 2929
Previously identified problems with Previously identified problems with DSS cost estimatesDSS cost estimates
““Million dollar” products.Million dollar” products.– Unit costs errorsUnit costs errors
– Encounters assigned extremely high costs Encounters assigned extremely high costs

Health Economics Resource CenterHealth Economics Resource Center 3030
Previously identified problems (cont.) Previously identified problems (cont.)
Missing medical proceduresMissing medical procedures– At some sites inpatient medical procedures not At some sites inpatient medical procedures not
recorded in a way that can be extracted by DSSrecorded in a way that can be extracted by DSS– Medical procedures: endoscopy, cardiac Medical procedures: endoscopy, cardiac
catheterization (expensive procedures not recorded catheterization (expensive procedures not recorded in surgical software package)in surgical software package)
– May result in an May result in an underestimateunderestimate of costs of some of costs of some hospital stays and outpatient visitshospital stays and outpatient visits

Health Economics Resource CenterHealth Economics Resource Center 3131
Looking inside the “black box”Looking inside the “black box”
Goals: Goals: – Evaluate if unit cost outliers affect cost Evaluate if unit cost outliers affect cost
estimatesestimates
– Identify if DSS used information on Identify if DSS used information on inpatient medical procedures to assign costinpatient medical procedures to assign cost
– Where procedure data are missing, find the Where procedure data are missing, find the effect on cost estimateseffect on cost estimates

Health Economics Resource CenterHealth Economics Resource Center 3232
Evaluation of DSS cost estimates of Evaluation of DSS cost estimates of stays involving medical proceduresstays involving medical procedures
Study population: Study population: – Clinical trial participants who had cardiac Clinical trial participants who had cardiac
angioplasty angioplasty
Method:Method:– Obtained detailed data on cost of each product Obtained detailed data on cost of each product
used in inpatient stays (2001-2002)used in inpatient stays (2001-2002)– Compared to corresponding record in DSS NDECompared to corresponding record in DSS NDE– Studied stays with angioplasty according to PTFStudied stays with angioplasty according to PTF
Evaluated intermediate products of these staysEvaluated intermediate products of these stays

Health Economics Resource CenterHealth Economics Resource Center 3333
Access to DSS Intermediate Product Access to DSS Intermediate Product DetailDetail
In In production levelproduction level data (in the black box) data (in the black box)– No national level extract of intermediate No national level extract of intermediate
products (data set would be too large) products (data set would be too large)
– Access granted by each medical centerAccess granted by each medical center
– Alternative: DSS national program office Alternative: DSS national program office can extract detailcan extract detail

Health Economics Resource CenterHealth Economics Resource Center 3434
Access to DSS Intermediate Product Access to DSS Intermediate Product DetailDetail
Requested data from DSS national program Requested data from DSS national program officeoffice– Hoped to pilot test method for future use by other Hoped to pilot test method for future use by other
researchers researchers – 2 year wait to obtain these data 2 year wait to obtain these data – Probably not a viable strategy for other researchersProbably not a viable strategy for other researchers
DSS office not funded to do this workDSS office not funded to do this work System not designed to extract data on a cohortSystem not designed to extract data on a cohort

Health Economics Resource CenterHealth Economics Resource Center 3535
Comparison of intermediate product Comparison of intermediate product detail to national data extractdetail to national data extract
– Costs in intermediate product data nearly Costs in intermediate product data nearly matched national data extracts (NDE)matched national data extracts (NDE) A very few records for products with costs A very few records for products with costs
greater than $30,000 had been excluded in greater than $30,000 had been excluded in tabulating costs to prepare NDE tabulating costs to prepare NDE
Evidently “high cost outliers” are filtered out in Evidently “high cost outliers” are filtered out in preparing NDEpreparing NDE
Appropriate to exclude these valuesAppropriate to exclude these values

Health Economics Resource CenterHealth Economics Resource Center 3636
Evaluation of intermediate products on Evaluation of intermediate products on cost estimatescost estimates
Study of inpatient stays with cardiac angioplastyStudy of inpatient stays with cardiac angioplasty– Identified 158 inpatient stays in which angioplasty Identified 158 inpatient stays in which angioplasty
took place according to Patient Treatment File took place according to Patient Treatment File (PTF)(PTF)
– Identified whether stay had intermediate products Identified whether stay had intermediate products for “angioplasty”, “PTCA”, or “catheterization”, for “angioplasty”, “PTCA”, or “catheterization”, etc.etc.
– Matched stay to “wage index” assigned to Matched stay to “wage index” assigned to geographic area by Medicaregeographic area by Medicare

Health Economics Resource CenterHealth Economics Resource Center 3737
Evaluation of inpatient costs using Evaluation of inpatient costs using intermediate products on cost estimates intermediate products on cost estimates
– Mean cost of a stay was $11,941Mean cost of a stay was $11,941– 55/158 stays (35%) had at least one angioplasty 55/158 stays (35%) had at least one angioplasty
productproduct– Regression Regression
Dependent variable: DSS cost Dependent variable: DSS cost Independent variables: length of stay, wage, days in Independent variables: length of stay, wage, days in
ICU, and whether DSS included an angioplasty ICU, and whether DSS included an angioplasty intermediate product intermediate product
– Stay with at least one angioplasty product were Stay with at least one angioplasty product were assigned $7,404 greater cost assigned $7,404 greater cost

Health Economics Resource CenterHealth Economics Resource Center 3838
Study limitationsStudy limitations
Hard to evaluate cost or quantity of an Hard to evaluate cost or quantity of an intermediate productintermediate product– products may be characterized differently at each products may be characterized differently at each
site, according to work processes and organizationsite, according to work processes and organization
Uncertain if we identified all angioplasty Uncertain if we identified all angioplasty products products – e.g., generic names: minutes in ambulatory surgerye.g., generic names: minutes in ambulatory surgery
VA continues to improve methods since study VA continues to improve methods since study time frame (2001-2002)time frame (2001-2002)

Health Economics Resource CenterHealth Economics Resource Center 3939
Improved inpatient procedure reportingImproved inpatient procedure reporting
New VA mandate that cardiac procedures New VA mandate that cardiac procedures be recorded as data (not just text)be recorded as data (not just text)

Health Economics Resource CenterHealth Economics Resource Center 4040
A new way to look into the black boxA new way to look into the black boxIntermediate Product Intermediate Product Department (IPD) Department (IPD) DetailDetail
– One record with costs incurred in each IPD One record with costs incurred in each IPD (Production Unit) during the stay/visit(Production Unit) during the stay/visit Gives sum of cost of all products from the departmentGives sum of cost of all products from the department Does not give quantity or cost of intermediate Does not give quantity or cost of intermediate productsproducts
– Both inpatient and outpatient filesBoth inpatient and outpatient files– Located at AustinLocated at Austin– Not yet documentedNot yet documented– Will allow researchers to estimate cost subtotals Will allow researchers to estimate cost subtotals

Health Economics Resource CenterHealth Economics Resource Center 4141
ConclusionsConclusions
DSS is excluding “million dollar products” DSS is excluding “million dollar products” in building the NDEin building the NDE
Incomplete data on inpatient procedures Incomplete data on inpatient procedures may result in significant underestimate of may result in significant underestimate of the cost of some hospital staysthe cost of some hospital stays

Health Economics Resource CenterHealth Economics Resource Center 4242
Recommendations Recommendations
Is accurate estimate of cost of stays Is accurate estimate of cost of stays involving inpatient procedures important involving inpatient procedures important to study? to study? – See DSS IPD extract to see if costs assigned See DSS IPD extract to see if costs assigned
to appropriate intermediate product to appropriate intermediate product department department

Health Economics Resource CenterHealth Economics Resource Center 4343
RecommendationsRecommendations
Alternatives Alternatives – Use HERC cost estimates as primary, Use HERC cost estimates as primary,
especially if data are several years old.especially if data are several years old.
– Conduct sensitivity analysis using HERC Conduct sensitivity analysis using HERC estimates estimates
– Estimate a cost function with DSS data and Estimate a cost function with DSS data and use it to simulate missing cost datause it to simulate missing cost data

Health Economics Resource CenterHealth Economics Resource Center 4444
Alternatives (cont.)Alternatives (cont.)
Estimate costs using DSS cost functionEstimate costs using DSS cost function– Estimate cost function Estimate cost function
Data: stays that have costs based on appropriate IPD Data: stays that have costs based on appropriate IPD Independent variables: Use clinical characteristics, Independent variables: Use clinical characteristics,
LOS, days in ICU, wage index, etc. LOS, days in ICU, wage index, etc.
– Predict costs based on clinical characteristicsPredict costs based on clinical characteristics– In our example, we would have added about In our example, we would have added about
$7,400 to cost estimates$7,400 to cost estimates

The Fee Basis (FEE) filesThe Fee Basis (FEE) files
Mark W. Smith, PhDMark W. Smith, PhDAdam Chow, B.A.Adam Chow, B.A.

Health Economics Resource CenterHealth Economics Resource Center 4646
Overview of Fee Basis ProgramOverview of Fee Basis Program
Pays for care at Pays for care at non-VA facilitiesnon-VA facilities in three in three situations:situations:– VA cannot provide the care locallyVA cannot provide the care locally– It is economical to do soIt is economical to do so– Travel to a VA facility is medically infeasibleTravel to a VA facility is medically infeasible

Health Economics Resource CenterHealth Economics Resource Center 4747
Overview of Fee Basis ProgramOverview of Fee Basis Program
Limited emergent care:Limited emergent care:
- no more than 10-day supply of Rx- no more than 10-day supply of Rx
- inpatient only until transfer is medically - inpatient only until transfer is medically feasible, typically 3 days or lessfeasible, typically 3 days or less
Full range of services coveredFull range of services covered

Health Economics Resource CenterHealth Economics Resource Center 4848
Overview of Fee Basis ProgramOverview of Fee Basis Program
Some common uses:Some common uses:
Community nursing home careCommunity nursing home care
Home-based care Home-based care – E.g.: long-term oxygen therapyE.g.: long-term oxygen therapy
Compensation & pension examsCompensation & pension exams

Health Economics Resource CenterHealth Economics Resource Center
Fee Basis files Fee Basis files
Subset of all VA contract careSubset of all VA contract care– Most “sharing agreement” care from Most “sharing agreement” care from
affiliate universities is affiliate universities is notnot included included– Substantial non-VA utilization unaccounted Substantial non-VA utilization unaccounted
forfor

Health Economics Resource CenterHealth Economics Resource Center 5050
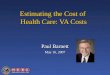
Fee Basis Payments FY2003Fee Basis Payments FY2003
Service typeService type Fee Basis Fee Basis PaymentsPayments FrequencyFrequency
Inpatient 116,000 stays $ 545 mNon-Rx Outpatient 5,418,000 visits $ 477 mRx 15,000 scripts $ 0.6 m
TOTAL $ 1,023 m

Health Economics Resource CenterHealth Economics Resource Center
Names of Fee Basis Files - INames of Fee Basis Files - I
Hospital stayHospital stayMDPPRD.MDP.SAS.FEN.FYyy.INPTMDPPRD.MDP.SAS.FEN.FYyy.INPT
Ancillary services provided to inpatientsAncillary services provided to inpatientsMDPPRD.MDP.SAS.FEN.FYyy.INPT.ANCILMDPPRD.MDP.SAS.FEN.FYyy.INPT.ANCIL
Outpatient servicesOutpatient servicesMDPPRD.MDP.SAS.FEN.FYyy.MEDMDPPRD.MDP.SAS.FEN.FYyy.MED
Payments to pharmaciesPayments to pharmaciesMDPPRD.MDP.SAS.FEN.FYyy.PHRMDPPRD.MDP.SAS.FEN.FYyy.PHR

Health Economics Resource CenterHealth Economics Resource Center
Names of Fee Basis Files - IINames of Fee Basis Files - IITravel expensesTravel expenses MDPPRD.MDP.SAS.FEN.FYyy.TVLMDPPRD.MDP.SAS.FEN.FYyy.TVL
Pharmacy vendor file Pharmacy vendor file MDPPRD.MDP.SAS.FEN.FYyy.PHARVENMDPPRD.MDP.SAS.FEN.FYyy.PHARVEN
Other vendors file Other vendors file MDPPRD.MDP.SAS.FEN.FYyy.VENMDPPRD.MDP.SAS.FEN.FYyy.VEN
Veterans with FEE cards (long-term users)Veterans with FEE cards (long-term users)
MDPPRD.MDP.SAS.FEN.FYyy.VETMDPPRD.MDP.SAS.FEN.FYyy.VET

Health Economics Resource CenterHealth Economics Resource Center 5353
Highlights of Patient DataHighlights of Patient Data
Scrambled SSN Scrambled SSN
Primary Service Area (PSA)Primary Service Area (PSA)– 3-digit station number3-digit station number
County, state, zip County, state, zip

Health Economics Resource CenterHealth Economics Resource Center 5454
Highlights of Clinical DataHighlights of Clinical Data
Outpatient: Outpatient: – Date of serviceDate of service– 1 CPT procedure code1 CPT procedure code
Inpatient:Inpatient:– Start and end dates of invoice period Start and end dates of invoice period – Up to 5 surgery codesUp to 5 surgery codes– Up to 5 ICD-9 diagnosis codes (*no decimal*)Up to 5 ICD-9 diagnosis codes (*no decimal*)

Health Economics Resource CenterHealth Economics Resource Center 5555
Highlights of Financial DataHighlights of Financial Data
Amount claimedAmount claimed
Amount paidAmount paid
Medicare prospective payment amount (inpatient) Medicare prospective payment amount (inpatient)
Many variable relating to FMS record-keeping: Many variable relating to FMS record-keeping: invoice date, processing date, check number, etc.invoice date, processing date, check number, etc.

Health Economics Resource CenterHealth Economics Resource Center 5656
What Data Rows RepresentWhat Data Rows Represent
Each row of data represents a service Each row of data represents a service provided for a particular date provided for a particular date (outpatient) or time period (inpatient)(outpatient) or time period (inpatient)
TREATDT: Outpatient date of service TREATDT: Outpatient date of service
TREATDTF: Inpatient start of invoice periodTREATDTF: Inpatient start of invoice period
TREATDTO: Inpatient end of invoice periodTREATDTO: Inpatient end of invoice period

Health Economics Resource CenterHealth Economics Resource Center 5757
Highlights of Vendor DataHighlights of Vendor Data
Vendor IDVendor ID
Address (city, state, zip)Address (city, state, zip)
Related VA station numberRelated VA station number
Payment totals by month, not by patient or servicePayment totals by month, not by patient or service

Health Economics Resource CenterHealth Economics Resource Center 5858
Finding CasesFinding Cases
Search all relevant variables:Search all relevant variables:
– Place of service (PLSER) Place of service (PLSER) – Treatment code (TRETYPE) Treatment code (TRETYPE) – Purpose of visit (FPOV)Purpose of visit (FPOV)
Cautions:Cautions: – Variable values can change year to yearVariable values can change year to year– Missing valuesMissing values

Health Economics Resource CenterHealth Economics Resource Center 5959
Creating Discharge Records (1)Creating Discharge Records (1)
Goal: Create a single discharge record Goal: Create a single discharge record from multiple inpatient service (INPT) from multiple inpatient service (INPT) recordsrecords
Method: Concatenate by SCRSSN using Method: Concatenate by SCRSSN using TREATDTF and TREATDTO.TREATDTF and TREATDTO.

Health Economics Resource CenterHealth Economics Resource Center 6060
Creating Discharge Records (2)Creating Discharge Records (2)
Records are typically processed within 30 days of Records are typically processed within 30 days of invoicing.invoicing.
BUTBUT
Invoices may be sent LONG after services are Invoices may be sent LONG after services are rendered.rendered.
THEREFORETHEREFORE
To find all services in a fiscal year, look in the Fee To find all services in a fiscal year, look in the Fee Basis files in that year Basis files in that year andand the 2 following years. the 2 following years.

Health Economics Resource CenterHealth Economics Resource Center 6161
Creating Discharge Records (3)Creating Discharge Records (3)
Searching for records:Searching for records:Outpatient: TREATDT Outpatient: TREATDT
Inpatient: TREATDTF, TREATDTOInpatient: TREATDTF, TREATDTO
Use vendor ID (VENDID) to track particular Use vendor ID (VENDID) to track particular facilitiesfacilities

Health Economics Resource CenterHealth Economics Resource Center 6262
Creating Discharge Records (4)Creating Discharge Records (4)
CautionsCautions– Watch for outliers: extremely long staysWatch for outliers: extremely long stays
– If a stay appears to end on September 30, check If a stay appears to end on September 30, check the October recordsthe October records
– Stays may end with a transfer to VA – look for Stays may end with a transfer to VA – look for VA recordVA record

Health Economics Resource CenterHealth Economics Resource Center 6363
Other NotesOther Notes
There is repetition across variables: state There is repetition across variables: state appears twice, some dates appear in both appears twice, some dates appear in both Julian and SAS formatsJulian and SAS formats
Blank fields are common. They could Blank fields are common. They could mean “not applicable” as well as mean “not applicable” as well as “missing.”“missing.”

Health Economics Resource CenterHealth Economics Resource Center 6464
Overlap with Other VA FilesOverlap with Other VA Files
Community nursing home care also inCommunity nursing home care also in– DSS outpatient filesDSS outpatient files– PTF Extended Care filesPTF Extended Care files
Most completed hospital stays also in PTF Most completed hospital stays also in PTF Non-VA Hospitalization filesNon-VA Hospitalization files

Health Economics Resource CenterHealth Economics Resource Center 6565
HERC Technical ReportHERC Technical Report
A HERC technical report on Fee Basis data A HERC technical report on Fee Basis data can be found on the HERC web site atcan be found on the HERC web site at
http://www.herc.research.med.va.gov/publications/ http://www.herc.research.med.va.gov/publications/ technical_reports.asptechnical_reports.asp

Health Economics Resource CenterHealth Economics Resource Center 6666
Questions on Fee Basis files?Questions on Fee Basis files?

National Prosthetics Patient National Prosthetics Patient Database (NPPD)Database (NPPD)
Ciaran Phibbs, PhDCiaran Phibbs, PhDMark W. Smith, PhDMark W. Smith, PhD
Pon Su, MAPon Su, MA

Health Economics Resource CenterHealth Economics Resource Center 6868
NPPD DescriptionNPPD Description
Contains records of prosthetics dispensed in VAContains records of prosthetics dispensed in VA– e.g. glasses, hearing aids, artificial limbs, e.g. glasses, hearing aids, artificial limbs,
stents, metal fixturesstents, metal fixtures
Data drawn from VISTA and Denver Data drawn from VISTA and Denver Distribution Center recordsDistribution Center records
Available FY1998 – presentAvailable FY1998 – present

Health Economics Resource CenterHealth Economics Resource Center 6969
Selected VariablesSelected Variables
Patient ID (links to SSN)Patient ID (links to SSN)
Location of serviceLocation of service
HCPCS code & item description HCPCS code & item description
Quantity dispensedQuantity dispensed
Cost estimateCost estimate

Health Economics Resource CenterHealth Economics Resource Center 7070
Additional Notes on NPPDAdditional Notes on NPPD
NPPD date refers to the day the record was NPPD date refers to the day the record was entered, NOT to date of service! There is no entered, NOT to date of service! There is no service date.service date.
Costs may vary by site due to local contracts.Costs may vary by site due to local contracts.
Used items automatically assigned 50% of new Used items automatically assigned 50% of new cost. cost.

Health Economics Resource CenterHealth Economics Resource Center 7171
NPPD vs. Utilization Files (1)NPPD vs. Utilization Files (1)
HERC compared NPPD records to major HERC compared NPPD records to major utilization databases:utilization databases:– Outpatient: OPC, DSS NDEOutpatient: OPC, DSS NDE– Inpatient: PTF, DSS NDEInpatient: PTF, DSS NDE
Purpose: To determine validity of NPPDPurpose: To determine validity of NPPD

Health Economics Resource CenterHealth Economics Resource Center 7272
NPPD vs. Utilization Files (2)NPPD vs. Utilization Files (2)
Idea: Prosthetics should be dispensed in an Idea: Prosthetics should be dispensed in an encounter that is recorded in a utilization encounter that is recorded in a utilization record.record.

Health Economics Resource CenterHealth Economics Resource Center 7373
NPPD vs. Utilization Files (2)NPPD vs. Utilization Files (2)
MethodMethod– Use date of outpatient NPPD record Use date of outpatient NPPD record – Look –30 to +30 days around outpatient Look –30 to +30 days around outpatient
visit in NPCD (OPC) for a related clinic visit in NPCD (OPC) for a related clinic stop stop
ResultResult– Only about 50% of records matchOnly about 50% of records match– Poor correspondence for inpatient recordsPoor correspondence for inpatient records

Health Economics Resource CenterHealth Economics Resource Center 7474
NPPD vs. Utilization Files (3)NPPD vs. Utilization Files (3)
ResultResult– Only about 50% of records match!Only about 50% of records match!
– Poor correspondence for inpatient recordsPoor correspondence for inpatient records
Potential CausesPotential Causes– Need to use longer window: -30 to +90 days ?Need to use longer window: -30 to +90 days ?
– Blind rehab units report using ward stock – not Blind rehab units report using ward stock – not
tied to individual patients.tied to individual patients.
– Weak incentive for accurate data entryWeak incentive for accurate data entry

Health Economics Resource CenterHealth Economics Resource Center 7575
RecommendationsRecommendations
NPPD is a work in progressNPPD is a work in progress– It does not list every prostheticIt does not list every prosthetic– It does not have a service dateIt does not have a service date
Potential use: estimating purchase cost of new Potential use: estimating purchase cost of new prosthetic items, locally or nationallyprosthetic items, locally or nationally

Health Economics Resource CenterHealth Economics Resource Center 7676
ReferencesReferences
Contents: Contents: VIReC InsightsVIReC Insights 2001;2(3)) 2001;2(3))
Comparison to utilization files: Comparison to utilization files: HERC technical report (in progress)HERC technical report (in progress)

Health Economics Resource CenterHealth Economics Resource Center 7777
Access to NPPDAccess to NPPD
ContactsContactsFrederick Downs, MD (VACO)Frederick Downs, MD (VACO)Liz Kiley, NPPD data manager (Hines)Liz Kiley, NPPD data manager (Hines)
ProcessProcessSubmit request to Frederick Downs with project Submit request to Frederick Downs with project
description, IRB approval, list of variables description, IRB approval, list of variables neededneeded

Health Economics Resource CenterHealth Economics Resource Center 7878
Questions on NPPD files?Questions on NPPD files?