Embed Size (px)
Citation preview

Advances in FetalCardiac Imaging
Margaret M. Vernon, MD*, Mark B. Lewin, MDKEYWORDS
� Fetal � Echocardiogram � Prenatal � Ultrasound � Cardiac
Imaging the fetal heart has evolved considerablysince the first report of ultrasonographic visualiza-tion of the fetal heart in the early 1970s. From thatdescription of ventricular output inferred fromm-mode tracings,1 one can trace the roots of fetalechocardiography. This article reviews the currentstate of the art in ultrasonographic evaluation ofthe fetal cardiovascular system.
Ultrasound remains the primary imaging modal-ity for evaluating the fetal heart and cardiovascularsystem. Beginning in the 1980s, commonly usedtransthoracic cross-sectional views of the hearthad been reproduced in utero,2 and the possibilityof prenatal detection of major congenital heartdisease was realized. As in utero ultrasonographicevaluations became mainstream, the goal of inutero identification of congenital heart diseasewas established.
Today, fetal cardiac imaging has moved froma novel, reportable technique to a component ofthe nearly universal mid-trimester fetal anatomicsurvey. In addition, a comprehensive ultrasono-graphic evaluation of the fetal cardiovascularsystem, the fetal echocardiogram, has emerged.As part of the mid-trimester screening ultrasound,a 4-chamber view of the heart is obtained, and ifpossible, views of both outflow tracts. Abnormalor unsatisfactory (the inability to establish normal)cardiac views obtained as part of this surveyaccount for more than 20% of all referrals for fetalechocardiography and lead to over half of allprenatal diagnoses of congenital heart disease.The role of routine obstetric ultrasound screeningis critical in the prenatal identification of congenitalheart disease.
The authors have nothing to disclose.Division of Cardiology, Seattle Children’s Hospital, M/S G* Corresponding author.E-mail address: [email protected]
Ultrasound Clin 6 (2011) 47–56doi:10.1016/j.cult.2011.01.0071556-858X/11/$ – see front matter � 2011 Published by E
Alternatively, it is well established that a varietyof maternal or fetal disorders may place a fetusat increased risk for congenital heart disease(Table 1). In these circumstances, a fetal echocar-diogram is recommended as well. Of these indica-tions, a positive family history accounts for anothernearly 20% of referrals for fetal echocardiography,though leading to the identification of fewer than5% of all prenatal diagnoses. All combined, inabout 5% of all pregnancies a fetal echocardio-gram is obtained.
TECHNICAL IMPROVEMENTSImprovements in Image Resolution
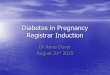
Historically the goal of fetal echocardiographywas simply to detect congenital heart disease.While this goal remains lofty, as recently as theearly 1990s the rate of prenatal diagnosis ofcongenital heart disease was fewer than 10% ofinfants undergoing cardiac surgery in the firstmonth of life,3 hence an emerging goal is toestablish an accurate diagnosis. Today detailedanatomic diagnoses can successfully be estab-lished with excellent correlation with postnatalechocardiograms. Arriving at an accurate diag-nosis depends first, on the ability to obtaina complete set of images and second, on thecorrect interpretation of those images. Thedevelopment of high-frequency transducers(6–10 MHz) with variable focus has been instru-mental in establishing this goal. Today’s ultra-sound transducers provide a markedly improvedlevel of image quality compared with that of the1990s (Fig. 1).
-0035, PO Box 5371, Seattle, WA 98145, USA
lsevier Inc. ultrasound.th
eclinics.com

Table 1Indications for fetal echocardiography
Maternal Indications Fetal Indications
Family history of congenital heart diseaseincluding prior child or pregnancy withcongenital heart disease
Abnormal obstetric screening ultrasonography
Metabolic disorders (eg, diabetes) Extracardiac abnormality
Exposure to teratogens Chromosomal abnormality
Exposure to prostaglandin synthetase inhibitors(ibuprofen)
Arrhythmia
Infection (rubella, Coxsackie, parvovirus B19) Hydrops
Autoimmune diagnosis (eg, Sjogren, systemiclupus erythematosus)
Increased first-trimester nuchal translucency
Familial inherited disorder (Marfan, Noonan) Multiple gestation and suspicion for twin-twintransfusion syndrome
In vitro fertilization
Vernon & Lewin48
Today the identification of arch branchingpatterns and systemic and pulmonary venousdrainage patterns is frequently possible. The entryof the superior and inferior vena cava into the rightatrium can be documented in an image identical tothe transthoracic bicaval view. The pulmonaryveins are often best evaluated in the 4-chamberview. By 2-dimensional (2-D) imaging pulmonaryveins can be seen entering the left atrium, whichcan be confirmed by color Doppler (Fig. 2).Unfortunately, fetal lie and position, maternal
body habitus and placental position, oligohydram-nios, and the relatively fixed fetal position associ-ated with advanced gestational age or a multiplegestation will always limit the acoustic windowsavailable.
Fig. 1. Four-chamber view from the late 1990s (A) comparof 2010 (B).
EXAMINATION STANDARDIZATION
Successful fetal cardiac imaging requires theability to obtain and properly interpret standardviews as well as the ability to approach the heartfrom multiple different orientations given the avail-able acoustic windows.
Screening Cardiac Views
Depending on the population, more than one-thirdof all cases of congenital heart disease occur inpregnancies not identified as high risk. For thisreason, the prenatal detection of congenital heartdisease relies most heavily on the images obtainedduring the nearly universal mid-trimester anatomicscan. In the mid 1990s, the American Institute of
ed with one obtained at 20 weeks during the summer

Fig. 2. Pulmonary venous return is seen entering theleft atrium from both lung fields.
Advances in Fetal Cardiac Imaging 49
Ultrasound in Medicine (1994) and the AmericanCollege of Radiology (1995) incorporated the4-chamber view into their formal guidelines forthe screening fetal ultrasound. This single view isabnormal in up to 60% of fetuses with majorcongenital heart disease if it is interpretedcorrectly.4
The 4-chamber view is the most important ina comprehensive examination of the fetal heart(Fig. 3 and MMC 1). The 4-chamber view illus-trates the pulmonary venous connections, theatrioventricular valves and cardiac crux, the atrialseptum, and the inlet and portions of the muscularventricular septum. It is important to assess forsymmetry in size of atria and ventricles. Late in
Fig. 3. Four-chamber view of the heart with the atrio-ventricular valves closed. The moderator band isclearly seen in the right ventricle and the normalvery slight apical displacement of the tricuspid valveannulus is noted.
gestation the right ventricle may be slightly largerthan the left ventricle. The right ventricle, in itsnormal position, is posterior to the sternum andidentified by the presence of the moderatorband. The image is obtained in a transverse scan-ning plane (cross section). In comparison to trans-thoracic imaging, the view can be obtained byrotating 90� from a long-axis view of the fetusdue to the large size of the fetal liver and moretransverse orientation of the fetal heart. The valveleaflets should open fully and should appear thin.Leaflets should show complete coaptation. Pres-ence of the foramenal flap in the left atrium aswell as the coronary sinus (Fig. 4) should beapparent.
The 4-chamber view may fail to detect a signi-ficant percentage of major, frequently ductal-dependent congenital heart disease (ie, pulmonaryatresia, tetralogy of Fallot, double-outlet rightventricle, transposition of the great arteries, andtruncus arteriosus).
Many investigators have demonstrated an incre-mental value of adding outflow tracts to the routinescreening fetal ultrasound. In 2007, The AmericanCollege of Radiology (ACR) Practice Guideline forthe Performance of Obstetrical Ultrasound,5 whichhas been adopted by the American College ofObstetricians and Gynecologists (ACOG),6
included a 4-chamber view and, if technicallyfeasible, visualization of both the right and leftventricular the outflow tracts. It is estimated thatby combining the 4-chamber and outflow tractviews, 75% of all congenital heart lesions couldbe detected prenatally.
The left ventricular outflow tract (LVOT) can beobtained by rotating the transducer from the
Fig. 4. Four-chamber view of the heart with a dilatedcoronary sinus noted in the left atrium. Furtherimaging confirmed the presence of a left-sided supe-rior vena cava.

Fig. 6. The right ventricular outflow tract is seen orig-inating from the right ventricle.
Vernon & Lewin50
4-chamber view and angling very slightly towardthe fetal right shoulder, a similar movement tothe transthoracic imaging in a pediatric patient(Fig. 5). Once the LVOT is opened up, rockingthe transducer slightly anteriorly (and cranially)will allow visualization of the main pulmonaryartery arising from the right ventricle (Fig. 6) in nor-mally related great arteries. The main pulmonaryartery and ascending aorta should criss-cross(MMC 2). In transposed great arteries, the aortaand pulmonary artery are oriented parallel toeach other as the pulmonary artery arises fromthe left ventricle and courses posteriorly beforebifurcating (MMC 3). If the great arteries are notclearly seen crossing, the possibility of a conotrun-cal malformation, specifically transposition of thegreat arteries, should be investigated. The outflowtracts can also be evaluated in a short-axis imagesimilar to the pediatric parasternal short axis. Inthis image, the pulmonary artery is seen wrappingaround the aorta, which is visible en face.Since the addition of the outflow tracts, consid-
erable debate has remained about the inclusion ofthe words “if possible.” This author shares theopinion that establishing the origin of the mainpulmonary artery from the right ventricle and theaorta from the left ventricle is mandatory. Thisbeing said, the formal incorporation of the4-chamber view with an attempt at viewing bothoutflow tracts into the routine screening fetal ultra-sound represents an important advance in fetalcardiac imaging.
Components of a Fetal Echocardiogram
The demand for and number of fetal echocardio-grams performed has increased drastically overthe past decade. Similar to transthoracic imaging,fetal echocardiography depends on the ability to
Fig. 5. The left ventricular outflow tract is seen origi-nating from the left ventricle.
obtain standard views and evaluate structures inorthogonal views. In the ideal situation, the echo-cardiogram is approached in a systematic fashionsimilar to a postnatal transthoracic examination.This being said, the fetus may be very active,changing position many times during the ultra-sound procedure, and the examiner may need tobe piece together many partial images to forma composite picture, particularly in the presenceof complex congenital heart disease. Frequentlythese examinations can take well over an hour tocomplete. In addition, fetal echocardiograms areinterpreted by obstetricians, cardiologists, andradiologists and are performed by sonographersworking closely with these varied practitioners.Because of this variety, and recognizing thegrowth in the field, the need to standardize thecomponents of the fetal echocardiogram hasbeen recognized.Both the American Society of Echocardiography
(ASE) (2004)7 and the American Institute of Ultra-sound in Medicine (AIUM) (2010)8 have publishedpractice guidelines for the performance of the fetalechocardiogram. The AIUM guideline was pub-lished in conjunction with the ACOG and theSociety for Maternal Fetal Medicine (SMFM), andis endorsed by the ACR. The essential compo-nents of a comprehensive evaluation followingthe ASE Guidelines are listed in Table 2. All agreethat the performance and interpretation of a fetalechocardiogram requires a unique set ofadvanced skills because the fetal heart is smalland dynamic, and its pathology is limitless.Whereas the ASE Practice Guideline is quitedetailed and lists sweeps, a Doppler examination,and measurement data as essential componentsof the fetal echocardiogram, the AIUM guidelinerecommends spectral and color Doppler, andmeasurement of anatomic structures only if there

Table 2Components of the fetal echocardiogram
Overview Fetal number and positionStomach position andabdominal situs
Cardiac position
Biometricexamination
Cardiothoracic ratioBiparietal diameter andhead circumference
Femur lengthAbdominal circumference
Cardiac imaging Four-chamber viewLeft ventricularoutflow tract
Right ventricularoutflow tract
Great arteriesThree-vessel viewBicaval viewDuctal archAortic arch
Dopplerexamination
Inferior and superiorvena cava
Pulmonary veinsDuctus venosusForamen ovaleAtrioventricular valvesSemilunar valvesDuctus arteriosusTransverse aortic archUmbilical arteryUmbilical vein
Measurementdata
Atrioventricular valvediameter
Semilunar valve diameterMain pulmonary arteryAscending aortaBranch pulmonary arteriesTransverse aortic archVentricular lengthVentricular short-axisdimensions
Examination ofrate and rhythm
M-mode of atrial andventricular wall motion
Doppler examination ofatrial and ventricularflow patterns
Fig. 7. Four-chamber view with normal color Doppleracross the tricuspid and mitral valves during diastolicfilling.
Advances in Fetal Cardiac Imaging 51
is a suspected abnormality. Color Doppler isextremely useful in fetal cardiac assessment. Itcan be used to quickly confirm normal flow(Fig. 7) or alternatively abnormal flow. ColorDoppler evaluation of the aortic and ductal archesshowing normal antegrade flow is essential, asflow reversal is consistent with severe congenitalheart disease such as semilunar valve hypoplasiaor atresia. It is particularly useful in identifyinga structure as vascular or during the search for
very small structures, either because the structureis abnormally small (hypoplastic ascending aorta)or the evaluation is being undertaken early in fetallife (pulmonary venous return).
EARLIER IMAGING
Pregnancy is routinely split into trimesters:conception to 13 weeks, 14 to 26 weeks, and27 weeks to full term (40 weeks). Historically theadvocated optimal timing for performance ofa comprehensive transabdominal fetal echocardi-ography is between 18 and 22 weeks’ gestation.At this gestational age, the fetus has grown suchthat it is out of the maternal pelvis, there are stilllarge pockets of amniotic fluid to be used, andfetal position is still variable. These characteristicscombined lead to a complete study in mostpatients. This procedure has not changed;however, we are moving into an era of early riskassessment and recognition of fetal anomalies.With this has come an interest in earlier evaluationof the fetal heart. Fortunately, technologicaladvances in sonographic instrumentation, specifi-cally the availability of high-resolution probes,have led to earlier attempts at evaluation of thefetal heart.
The first-trimester screen performed between11 and 13 weeks’ gestation combines maternalhuman chorionic gonadotropin (hCG) andpregnancy-associated plasma protein A (PAPP-A) blood levels as well as fetal nuchal translucency(NT) with maternal age, to come up with acomposite risk of a chromosomal abnormality.The NT, the measurement of the thickness of thefluid collection observed beneath the fetal skinalong the posterior neck, is increased in fetuseswith Down syndrome and other chromosomal

Vernon & Lewin52
abnormalities. Initially introduced as a noninvasiveassessment of increased risk for a chromosomalabnormality, an increased NT has now been iden-tified as a risk factor for congenital heart disease.This increased risk holds in chromosomally normalfetuses.9,10 Not surprisingly, there has beena surge of interest in earlier diagnosis of congenitalheart disease since this was discovered, as itprovides invaluable reassurance to the motherwith a fetus at high risk for heart disease whohas a normal study or, alternatively, providesmore time for further testing if heart disease is de-tected. In addition, earlier diagnosis allows for anearlier, safer, and less traumatic termination ifchosen.Today, transabdominal fetal echocardiography
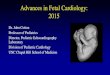
is feasible in the late first and early second trimes-ters (Fig. 8; MMC 4 and 5). In experienced centers,a complete transabdominal evaluation of the fetalheart can reliably be obtained in all patients by15 weeks’ gestation.11 A limited number of reportsdescribe the utility of transvaginal imagingbetween 10 and 13 weeks.12
As there are some lesions that tend to progressor evolve in utero, primarily outflow tract obstruc-tion, it is strongly recommended that all early fetalechocardiograms be followed by evaluation atmid-gestation. Some defects cannot, however,develop from a normal-looking heart, includingtransposition of the great arteries, atrioventricularcanal defects, double-outlet right ventricle, trun-cus arteriosus, total anomalous pulmonary venousreturn, and Ebstein anomaly, and early reassur-ance is beneficial.
QUANTITATIVE ASSESSMENT
The goal of fetal echocardiography has been toprovide a primarily structural, cardiac diagnosis
Fig. 8. (A) Four-chamber view at 14 weeks’ gestation. (Bgestation. There is severe left ventricular dysfunction, theminimal flow detectable across the aortic valve consistent
for prenatal counseling. A quantitative assessmentof fetal cardiovascular structure and functionis increasingly becoming a part of fetalechocardiography.
Normal Data Sets
Serial observation of in utero heart disease hasprovided critical insight into the evolution ofcongenital heart disease and potential for in uteroprogression.13 Though not all structures requiremeasuring, especially if visually there are noconcerns, structures can be measured andcompared with established normal subjects forvarying gestational ages. Serial assessment hasbeen aided by the compilation of normative datasets. Similar to the normative data sets availablefor transthoracic echocardiography, the com-pilation of normative data allows comparison ofobtained measurements with establishednormals.14,15 The creation of z-scores,16,17 whichquantify the degree to which a given measurementlies above or below the mean value for a givenpopulation, have been instrumental to fetal echo-cardiography and the ability to longitudinally trackpathology. Assessment of in utero disease severityis challenging, as many of the well-understoodpostnatal hemodynamic findings are altered orabsent in the presence of the placental circulation.In particular, equalization of pressures betweenthe left and right ventricles and aorta and pulmo-nary arteries makes evaluation of semilunar valvepathology, known to progress in utero, chal-lenging. Fetal echocardiography relies on thesecondary findings for indirect measurement ofseverity. Critical to the applicability of these datasets is an understanding of how a measurementis obtained and to what it is indexed. In uteromeasurement sets have been created, which
) Abnormal early fetal echocardiogram at 16 weeks’left ventricular myocardium is bright, and there waswith severe aortic stenosis.

Advances in Fetal Cardiac Imaging 53
index measurements for gestational age as well asbiometric measurements (biparietal diameter,head circumference, and femur length).
Access to in utero serial observatory data setsas well as normal data sets has aided the evolvingfield of in utero cardiac intervention. A relativelylimited number of centers have cautiouslyexplored this field in hopes of altering outcomefor a few of the most severe and devastatingforms of congenital heart disease, includingcritical aortic18 and pulmonary stenosis. Early inutero interventional data are encouraging, withnormalization of growth and tolerance ofbiventricular circulation postnatally in somepatients uniformly destined for single ventricularpalliation.19
Composite Comparative Scores
Semiquantitative scoring systems have beencreated to estimate severity, facilitate serialassessment, and predict outcome. Increasinglythese models of standardization of assessmentwill become important as in utero interventionsare introduced in hopes of altering the naturalcourse of a disease state. To date, cardiovascularscores have been developed for fetal heartfailure,20 twin-twin transfusion syndrome, and crit-ical aortic stenosis.
For fetal congestive heart failure, the cardiovas-cular profile score (CVP)21 comprises a 10-pointscoring system that combines data collectedduring a fetal echocardiogram known to be asso-ciated with perinatal mortality: hydrops, cardiacsize, abnormal myocardial function, redistributionof cardiac output, and abnormal venous Dopplerpatterns. The maximum CVP score is 10 and theminimum is 0. Deductions from the maximum of1 or 2 points for each of the 5 categories aremade for abnormal findings.
Ventricular Function
The evaluation of fetal cardiac function was limitedhistorically to an eyeballed qualitative globalassessment of systolic function (good, poor,depressed) with no defined criteria to assure inter-observer reproducibility. As perinatology hasmoved from quiet observation of high-risk fetusesto in utero management, early induced delivery,and even in utero intervention, an interest ina reproducible quantitative assessment ofmyocardial function has developed. Evaluation ofheart size, heart rate, and the presence or absenceof hydrops can provide clues to cardiac function,and indices of systolic and diastolic function arebeing investigated.
Systolic functionFetuses with lesions known to effect cardiacfunction such as volume overload (in the recipientin twin-twin transfusion syndrome), a hyperdy-namic circulation (arterio-venous malformation),cardiac compression (diaphragmatic hernia orlung lesions), and increased placental resistance(intrauterine growth restriction and placentalinsufficiency) have been studied and reported.Systolic function is estimated qualitatively andcan also be quantified by calculating theshortening fraction from either 2-D images orM-mode tracings. The simplest calculation isthe M-mode derived estimated shortening frac-tion, calculated as the end-diastolic dimensionminus the end-systolic dimension divided by theend-diastolic dimension. One of the greatestchallenges to estimating both the shorteningfraction and an ejection fraction is the smallsize of the fetal heart and the reproducibility ofmeasurements. In addition, all measurementsrequire definition of end-diastole and systole,which without an electrocardiogram can be diffi-cult to define.
Diastolic functionOnce recognized as the precursor to clinicallyapparent systolic dysfunction, diastolic dysfunc-tion and its assessment has be at the forefront offetal imaging today. At present, diastolic perfor-mance is assessed by measuring the forwardpulsed Doppler tracings of velocities across themitral valve. Early passive diastolic filling producesthe E-wave and active filling during atrial systoleproduces the A-wave. During fetal life, the majorityof diastolic ventricular filling occurs during atrialsystole, thus the A-wave is of greater velocitythan the E-wave. When diastolic ventricular fillingpredominantly relies on atrial systole, the magni-tude of the A-wave will increase and accordingly,the E/A ratio will decline. A decrease in the E/Aratio and fusion of the two peaks producinga monophasic waveform are considered evidenceof decreased cardiac diastolic function. Withincreasing gestation, the Doppler pattern changessuch that by term the tracing mimics that of thepostnatal.
Tissue Doppler imaging (TDI) is a relatively newechocardiographic technique that uses traditionalDoppler principles to measure the velocity ofmyocardial motion. Doppler echocardiographyrelies on the detection of the shift in frequency ofultrasound signals reflected from moving objects.Conventional Doppler assesses the velocity ofblood flow by measuring signals from blood cells.In TDI, the same principles are used to quantifymyocardial tissue motion.

Vernon & Lewin54
Global cardiac functionThe early recognition of subtle changes inmyocardial function is critical. The myocardialperformance or Tei index (TI) was introduced in1995.22 The TI is calculated from the Dopplerwaveform obtained by placing the pulsed Dopplersample in the left ventricle at the junction of theanterior leaflet of the mitral valve and the LVOT.It is the sum of the isovolumic contraction time(ICT), defined as the time interval from the endof the A-wave to the onset of the aortic pulsedDoppler tracing, and the isovolumic relaxationtime (IRT), defined as the time interval from theend of the aortic pulsed Doppler to the onset ofthe E-wave, divided by the ejection time (ET),the onset to the end of the aortic pulsed Dopplertracing.
TI5 ðICT1IRTÞ=ETThe use of the TI in the assessment of fetal func-
tion was first reported in 1999 by Tsutsumi andcolleagues.23
Since its introduction, the utility of the TI in theassessment of global fetal cardiac function hasbeen investigated and normal values have beenestablished.24 It is an easily obtained, Doppler-derived index that appears to be independent ofboth gestational age and heart rate.8,9 It is madeup of both systolic (ICT and ET) and diastolic(IRT) components. By incorporating only timeintervals, the TI is less dependent on anatomy orprecise imaging. There is some variability in re-ported left ventricular values, with reported normalTI values between 0.35 � 0.0325 and 0.53 �0.13.24 If the functional properties of the ventriclesdecline, an increasing amount of time is spenteither building up enough ejection force to openthe semilunar valve or relaxing after ejection ofblood has been achieved. Either of these develop-ments will produce a shortened ET interval, andlonger isovolumetric contraction and relaxationtimes. Accordingly, an increase in the TI indicatesa decrease in global myocardial performance.
APPLICATION OF NEW ULTRASONOGRAPHICTECHNOLOGY TO FETALECHOCARDIOGRAPHYCine Loop Capture
Considerable discussion continues as to the utilityof cine loop capture rather than solely still framecapture. A comprehensive cardiac evaluationshould include sweeps rather than solely a seriesof still frame captures. Sweeps allow for mentalreconstruction and are essential to the under-standing of complex cardiac lesions. With theadvent of 3-dimensional (3-D) sample volume
capture, this may become a moot point in thefuture.
Three-Dimensional Imaging
Arguably the next ultrasonographic advance togain widespread acceptance will be 3-D fetalechocardiography. 3-D echocardiography offerspotential advantages over conventional 2-Dimaging. By acquiring volumetric data sets withina few seconds, 3-D imaging promises to signifi-cantly reduce scan time. Compared with 2-Dimaging, which may require 30 minutes or moreof imaging time in the presence of a complexcongenital lesion, 3-D echocardiography withpractice may offer a significantly reduced scan-acquisition time of as little as 5 to 10 minutes.3-D imaging does pose some challenges. Thefetus must remain still for 15 to 30 seconds duringacquisition and as many as 5 scan sequences mayroutinely be necessary as part of a completestudy. In addition, off-line computer processingremains complicated and time consuming. Finally,fetal 3-D has limitations similar to those encoun-tered with 2-D studies: fetal lie, plane of imageacquisition, and late-gestation shadowing fromfetal bones and extremities all directly affect thequality of 3-D images.For screening of low-risk pregnancy, 3-D
imaging may allow visualization of the 4-chamberview and outflow tracts from one data set froma single acoustic window. Such a volume dataset could then be manipulated, allowing for imageplane alignment errors and sonographer inexperi-ence. This potential likely offers the next step insignificantly increasing the rate of prenataldiagnosis.
Telemedicine
As expertise in fetal echocardiography may not beavailable in all communities, unique strategieshave been proposed using the rapidly expandingfield of telemedicine. Reports of using spatio-temporal image correlation volumes obtained bya nonexpert (general obstetrician) and transmit-ted electronically via the Internet for remoteanalysis and interpretation by an expert haveemerged.26–28 As this technology is used moreand more, its utility in fetal echocardiography willundoubtedly be realized.In summary, imaging the fetal heart has evolved
significantly since the first reports. Today nearly allwomen have a screening ultrasound, includingcardiac views, during the second trimester andnearly 5% of all women are referred for compre-hensive fetal echocardiogram. These detail-oriented examinations can detect and accurately

Advances in Fetal Cardiac Imaging 55
diagnose nearly all forms of congenital heartdisease. Serial in utero evaluations combinedwith postnatal images have provided a naturalhistory of nearly all lesions and have set the stagefor fetal intervention, which hopes to alter theobserved natural history of the most devastatinglesions.
Progress in fetal echocardiography is due in partto gained experience, but also has benefitedgreatly from technological advances in ultraso-nography. In the future, it is likely that 3-D and4-D fetal echocardiography will further revolu-tionize the field.
SUPPLEMENTARY DATA
Supplementary data related to this article can befound online at doi:10.1016/j.cult.2011.01.007.
REFERENCES
1. Winsberg F. Echocardiography of the fetal and
newborn heart. Invest Radiol 1972;3:152.
2. Sahn DJ, Lange LW, Allen HD, et al. Qualitative real-
time cross-sectional echocardiography in the devel-
oping human fetus and newborn. Circulation 1980;
62:588.
3. Montana E, Khoury MJ, Cragan JD, et al. Trends and
outcomes after prenatal diagnosis of congenital
cardiac malformations by fetal echocardiography
in a well defined birth population, Atlanta, Georgia,
1990-1994. J Am Coll Cardiol 1996;28:1805–9.
4. Allan LD, Crawford DC, Chita SK, et al. Prenatal
screening for congenital heart disease. Br Med J
(Clin Res Ed) 1986;292:1717–9.
5. American College of Radiology. ACR practice
guidelines for the performance of antepartum
obstetrical ultrasound. In Practice Guidelines and
Technical Standards. Reston (VA): ACR; 2007.
6. Ultrasonography in Pregnancy. ACOG Practice
Bulletin, # 101. Obstet Gynecol 2009;113(2 Pt 1):
451–61.
7. Rychik J, Ayres N, Cuneo B, et al. American Society
of Echocardiography guidelines and standards for
performance of the fetal echocardiogram. J Am
Soc Echocardiogr 2004;17:803–10.
8. Lee W, Drose J, Wax J, et al. AIUM practice guide-
line for the performance of fetal echocardiography.
J Ultrasound Med 2011;30:127–36.
9. Mavrides E, Cobian-Sanchez F, Tekay A, et al. Limi-
tations of using first-trimester nuchal translucency
measurement in routine screening for major congen-
ital heart defects. Ultrasound Obstet Gynecol 2001;
17:106–10.
10. Ghi T, Huggon IC, Zosmer N, et al. Incidence of
major structural heart defects associated with
increased nuchal translucency but normal karyo-
type. Ultrasound Obstet Gynecol 2001;18:610–4.
11. Smrcek JM, Berg C, Geipel A, et al. Early fetal
echocardiography. J Ultrasound Med 2006;25:
173–82.
12. Carvalho JS,MoscosoG, TekayA, et al. Impact of first
and early second trimester fetal echocardiography
on high-risk pregnancies. Heart 2004;90:921–6.
13. Trines J, Hornberger LK. Evolution of heart disease
in utero. Pediatr Cardiol 2004;25:287–98.
14. Tan J, Silverman NH, Hoffman JI, et al. Cardiac
dimensions determined by cross-sectional echocar-
diography in the normal human fetus from 18 weeks
to term. Am J Cardiol 1992;70:1459–67.
15. Sharland GK, Allan LD. Normal fetal cardiac
measurements derived by cross-sectional echo-
cardiography. Ultrasound Obstet Gynecol 1992;2:
175–81.
16. Schneider C, McCrindle BW, Carvalho JS, et al.
Development of z scores for fetal cardiac dimen-
sions from echocardiography. Ultrasound Obstet
Gynecol 2005;26:599–605.
17. Lee W, Riggs T, Amula V, et al. Fetal echocardiog-
raphy: z-score reference ranges for a large patient
population. Ultrasound Obstet Gynecol 2010;35:
28–34.
18. Makikallio K, McElhinney DB, Levine JC, et al. Fetal
aortic valve stenosis and the evolution of hypo-
plastic left heart syndrome: patient selection for fetal
intervention. Circulation 2006;113:1401–5.
19. McElhinney DB, Marshall AC, Wilkins-Haug LE, et al.
Predictors of technical success and postnatal biven-
tricular outcome after in utero aortic valvuloplasty for
aortic stenosis with evolving hypoplastic left heart
syndrome. Circulation 2009;120:1482–90.
20. Huhta JC. Guidelines for the evaluation of heart
failure in the fetus with or without hydrops. Pediatr
Cardiol 2004;25:274–86.
21. Falkensammer CB, Paul J, Huhta JC. Fetal conges-
tive heart failure: correlation of Tei-index and cardio-
vascular score. J Perinat Med 2001;29:390–8.
22. Tei C, Ling L, Hodge D, et al. New index of
combined systolic and diastolic myocardial perfor-
mance: a simple and reproducible measure of
cardiac function—a study in normal and dilated
cardiomyopathy. J Cardiol 1995;26:357–66.
23. Tsutsumi T, Ishii M, Eto G, et al. Serial evaluation for
myocardial performance in fetuses and neonates
usinganewDoppler index.Pediatr Int 1999;41:722–7.
24. Friedman D, Buyon J, Kim M, et al. Fetal cardiac
function assessed by Doppler myocardial perfor-
mance index (Tei index). Ultrasound Obstet Gynecol
2003;21:33–6.
25. Eidem BW, Edwards JM, Cetta F. Quantitative
assessment of fetal ventricular function: establishing
normal values of the myocardial performance index
in the fetus. Echocardiography 2001;18:9–13.

Vernon & Lewin56
26. Vinals F, Mandujano L, Vargas G, et al. Prenatal
diagnosis of congenital heart disease using four-
dimensional spatiotemporal image correlation
(STIC) telemedicine via an Internet link: a pilot study.
Ultrasound Obstet Gynecol 2005;25:25–31.
27. Vanals F, Ascenzo R, Naveas R, et al. Fetal Echo-
cardiography at 11 1 0 to 13 1 6 weeks using
four-dimensional spatiotemporal image correlation
telemedicine via an Internet link: a pilot study. Ultra-
sound Obstet Gynecol 2008;31:633–8.
28. Michailidis G, Simpson J, Karidas C, et al. Detailed
three-dimensional fetal echocardiography facilitated
by an Internet link. Ultrasound Obstet Gynecol 2001;
18:325–8.