-
ADVANCES IN DIAGNOSIS ANDDETECTION OF ORAL DISEASES
BJ. BAUM1, CJ. BURSTONE2, R. DUBNER1, P. GOLDHABER3, M.J.
LEVINE4,WJ. LOESCHE5, and V. TERRANOVA4
"'National Institute of Dental Research, National Institutes of
Health, Bethesda, Maryland; 2Universityof Connecticut, School of
Dental Medicine, Farmington, Connecticut; 3Harvard University
School of
Dental Medicine, Boston, Massachusetts; 4SUNY at Buffalo, School
of Dentistry, Buffalo, New York;and 5University of Michigan, School
of Dentistry, Ann Arbor, Michigan
Adv Dent Res 3(1):7-13, May, 1989
ABSTRACT
Medicine, particularly with respect to diagnostic
decision-making, has seen remarkable advances inthe last ten years.
The art of diagnosis has become much more of a science. Basic
science advanceshave moved from the laboratory into the hospital
and radically changed the way a medical diagnosis is arrivedat or
confirmed. Dentistry, especially oral diagnosis, as yet has not
been a significant part of this general medicaladvance. However,
several examples demonstrate that this situation is starting to
change. Oral conditions arebeginning to be evaluated with greater
precision and sophistication. This report reviews some recent
advancesin oral diagnostic research and suggests where they will
carry dentistry over the next 25 years.
INTRODUCTION
Medicine, particularly with respect to
diagnosticdecision-making, has seen truly remarkable advancesin the
last ten years. The art of diagnosis has becomemuch more of a
science. Technological advances frombiochemistry, immunology,
physics, etc., have movedfrom their laboratories into the hospital
and com-bined to radically change the way a medical diagnosisis
arrived at or confirmed.
Dentistry, especially oral diagnosis, as yet has notbeen a
significant part of this general medical ad-vance. But there are
many examples, some of whichare cited in the sections below, which
demonstratethat this is beginning to change. Oral conditions
arebeginning to be evaluated with considerably
greatersophistication. It is the role of this paper to suggestwhere
these advances in oral diagnostic research andapplication will
carry the diagnostic side of theprofession over the next 25
years.
At the outset, it is worth stating that the authorsrecognize the
precarious task of predicting the future,
A report of the AADR ad hoc Committee on New Frontiers in
OralHealth Research
Please address all correspondence to Dr. Bruce J. Baum,
ClinicalInvestigations and Patient Care Branch, National Institute
of Den-tal Research, National Institutes of Health, Building 10,
Room 1A-05, Bethesda, MD 20892.
particularly as it relates to biomedical science. Forexample,
six years ago it would have been impossibleto predict the profound
and pervasive impact thatAIDS would have on the biomedical research
com-munity. Yet this "epidemic" has markedly influencedthe
directions and nature of biologic research in 1988.Obviously, our
level of confidence decreases with time,but we generally have
accepted the notion that oraldiagnosis as a discipline will change
dramatically overthe time frame considered. This change likely
willreflect a much broader level of stomatological concernby future
dentists than exists at present. In fact, asdiagnostic skills and
methodologies become more so-phisticated, we believe that much
professional oraldiagnosis will be performed outside of the
traditionaldental office setting, occurring rather in a
hospital-type environment, and indeed being performed byan expanded
specialty of more intensively trained oraldiagnosticians. Just as
dental research has contrib-uted, and will continue to contribute,
toward shiftsin the nature of dental practice, research advances
inoral diagnosis will contribute not only to changes inpatient
evaluation and management, but also to shift-ing emphases in dental
education. Future studentswill require greatly expanded training in
many basicand clinical medical science disciplines in order
toutilize the anticipated diagnostic advances. Indeed,for the
transfer to the clinical profession of the "ad-vances" described in
this paper, significant changes
-
BAUM et al. Adv Dent Res May 1989
in dental education and clinical practice behavior willhave to
occur.
For purposes here, we have grouped anticipatedadvances into
short-term (~5 years), intermediate (-10years), and long-term (-25
years) categories. We hopethese provide a convenient time-line for
the reader,but we emphasize that the time course is most
spec-ulative. Also, the number of predictions decreaseswith
increasing time, reflecting what we feel is a greaterconfidence in
our abilities to predict shorter-termtrends.
SHORT-TERM ADVANCES (-5 YEARS)
Research advances here focus on the transfer ofmethods and
ideas, which are currently available inother biomedical areas, to
oral diagnostic problems.In general, these examples were not hard
to choose;in fact, there were many possibilities. However,
alltopics selected have by now brought great benefit toseveral
areas of clinical medical science and, impor-tantly, these topics
have shown themselves to beclearly applicable to problems of the
oral cavity. It isimportant to emphasize that these are diagnostic
toolswhich are capable of being used now, the limitationbeing only
problems in transfer to, or acceptance by,the profession.
(1) Radionuclides in the Diagnosisof Periodontal Disease
Nuclear medicine as a medical specialty has grownenormously in
the last dozen or so years. Manyradionuclides are in common
clinical diagnostic usage,with more sophisticated probes being
developed atan increasingly more rapid pace. The general prin-ciple
involved is quite simple: The diagnostician ad-ministers a
radiolabeled compound which showsparticular affinity for a tissue
and which reflectssomething about the metabolic or functional state
ofthe tissue. Thereafter, some type of detector is usedto
quantitate the relative uptake of tracer in the tissueof interest.
An excellent and common example ofradionuclide diagnostic testing
is the use of 131I or 125Iin evaluations of thyroid gland metabolic
status.
Recently, workers at the Harvard School of DentalMedicine have
suggested the utilization of a radio-nuclide, technetium
99m-tin-diphosphonate (99mTc-Sn-MDP), as an indicator of active
alveolar bone lossin the diagnosis of periodontal disease activity
(Jeff-coat et al., 1985). Commonly used methods of de-tecting
periodontal diseases require repeatedmeasurements over considerable
time to assess rateof attachment loss {i.e., periodontal probing).
Simi-larly, radiographic analyses show only post hoc de-struction
of alveolar bone. Presently, there isconsiderable effort focused on
methods of diagnosingactive periodontal disease (Fine and Mandel,
1986).Jeffcoat and her colleagues recognized that 99mTc-Sn-MDP was
in routine medical use to detect bony
metastases, stress fractures, infections, etc., prior tothe
presence of radiographic evidence. Accordingly,they reasoned that
uptake of this bone-seeking radio-nuclide might provide a
diagnostic mechanism to as-sess periodontal status in a single
examination. Theirresults, found in the report cited above, and
sum-marized in Fig. 1, offer strong support for the utilityof
99mTc-Sn-MDP in the diagnosis of periodontal dis-ease.
The possibilities for application of nuclear medicaltechnology
to oral problems seem to be limitless, re-quiring only imagination,
a good knowledge of tissuephysiology, and a cooperative chemist who
can de-sign a radiolabeled ligand with appropriate
targetspecificities. There are several radionuclides alreadyin
general medical use which should soon find theirway into oral
diagnosis another good example being99mTcO4~ for evaluating
salivary gland dysfunction.We expect there will be considerable
investigative ef-fort in this area over the next 5-10 years,
resulting ina vastly more sophisticated armamentarium for
oraldiagnosticians.
(2) Direct Imaging MethodsAnother major tool in medical
diagnosis which has
yet to find its way into common oral diagnosis is theutilization
of advanced direct imaging methods. Theclinical specialty of
radiology has been expandedwidely due to the rapid development and
applicationof a new generation of imaging devices. It would beeasy
to devote this entire short-term advances section
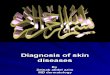
Fig. 1 Schematic representation of detection of active
periodontaldisease with 99m-tin-diphosphonate. A. Normal alveolar
bone ap-pearance observed with little bone-seeking
radiopharmaceuticaluptake (black flecks) associated with the bone
about the teeth. B.Representation of area with evidence of past
periodontal disease.There is horizontal bone loss about the teeth
but no radiophar-maceutical uptake, indicating no active disease.
C. Area similar tothat shown in B, but note that the middle tooth
shows an adjacentarea of bone which has taken up large amounts of
the 99m-tin-diphosphonate tracer, indicating an area of active bone
loss. Thisarea may be detected by means of a small gamma emission
detectorplaced on the patient's gingiva.
-
Vol. 3 No. 1 ADVANCES IN ORAL DIAGNOSIS
to these technologies. Indeed, as further indicatedbelow, we
expect later advances in diagnosis to beparticularly directed at
more sophisticated physicalscience probes.
As with radionuclides, we are best able to showthe value of such
advanced imaging methods to oraldiagnosis through an example of
recent applications.Considerable investigative effort, with an oral
prob-lem area, has come from the use of ultrasound todetect
swallowing disorders (dysphagia) of oral etiol-ogy. In principle,
ultrasonography functions similarlyto sonar on a submarine i.e.,
transmitting a soundwave and, by detecting reflections of sound off
ob-jects in its path, "visualizing" structures. In this
case,ultrasound waves are passed through tissues, andreflections of
these waves are converted to an imageby appropriate hardware.
Ultrasound is an excellentmeans of visualizing soft tissues in
active function{e.g., echocardiography).
Workers at the National Institutes of Health haveutilized this
technology to evaluate and characterizeswallowing disorders in the
oropharyngeal region(Shawker et al., 1983). The dorsum of the
tongue:airinterface offers virtually perfect impedance to an
ul-trasound wave, resulting in a sharp visualization ofthe tongue
during function (Fig. 2). Swallows usingendogenous oral secretions
("dry" swallows) or thosewith a bolus of fluid present {e.g.,
water; "wet" swal-lows) can be followed in real time, recorded on
video
A. B.
Fig. 2 Schematic diagram of midline sagittal views of the
tongueand floor of the mouth as seen on ultrasound scan. The area
en-compassed by the scan is indicated by the somewhat
truncated"V-shape" (-80 sector). The ultrasound transducer is
positionedunder the chin. Dashed lines indicate structures not seen
in scanand are placed here only for reference. A. The tongue at
rest. Thereis a small air space between the tongue and palate. B. A
waterbolus (5 mL) has been placed in the mouth and is held
anteriorly,anticipating a command to swallow. The air space above
the pos-terior tongue is no longer visible. Abbreviations used are
T, tonguetip; H, hyoid bone; E, epiglottis. Swallow analysis can be
per-formed with only endogenous secretions present (i.e., saliva,
asdepicted in A, termed "dry swallow") or with an exogenous
fluidbolus (/.., water, depicted in B, termed "wet swallow").
Tonguemovement is recorded on videotape at a rate of 30 frames/sec
andcan be analyzed by stop-frame analysis.
tape, and analyzed for time kinetics, pattern of mo-tion,
irregular gestures, etc. This is a non-invasive,readily repeatable
technique which allows for imag-ing of oral functions and tissues
heretofore impossi-ble with conventional radiologic tools. In
actuality,little study of oropharyngeal dysphagia has occurred,yet
it appears to be a reasonably common entity(Hughes et al, 1987).
For example, patients with hy-pofunctional salivary glands,
regardless of etiology{e.g., radiation, autoimmune disease,
pharmacologi-cal), routinely display, and complain of,
swallowingdifficulty. Also, many patients, post-treatment for
headand neck tumors, may suffer from a dysphagia oforopharyngeal
etiology.
There are other imaging tools (computer-assistedtomographic
analysis; magnetic resonance) which arein increasingly more common
use in medical diag-nosis and which have also been applied to oral
prob-lems, e.g., temporomandibular joint disorders (Skalericet al.,
1987). They have potentially broad applicationsto oral tissues. We
certainly expect this general fieldto contribute considerably to
advances in oral diag-nosis over the next 5-10 years.
(3) Humoral Markers for Pain and Tissue InjuryRecent advances in
the understanding of the bio-
chemistry and pharmacology of pain pathways haveled to the use
of chemical intermediates as markersof both pain and tissue injury.
Currently used meth-ods to analyze these markers in conjunction
withmanagement decisions for pain patients are an ex-cellent
example of how humoral analyses may be em-ployed or adapted to
problems in oral diagnosis. Forinstance, pain produces
physiological responses in-volving activation of the
hypothalamic-pituitary-ad-renal axis and the consequent secretion
ofneurohumoral agents from these tissues. Thus,
cor-ticotropin-releasing factor is released from the hy-pothalamus;
adrenocorticotrophic hormone, beta-endorphin, and beta-lipotropin
are released from thepituitary; and the adrenal medulla releases
mono-amines and opiate peptides. All of these humoralagents can be
easily measured via standard immu-nochemical methods
(radioimmunoassay) and cor-related with behavioral measures of pain
and stress(Fig. 3). Recent studies have shown that opiate ago-nists
given during surgery suppress beta-endorphinrelease and reduce
pain, while opiate antagonistsstimulate the release of
beta-endorphins and are as-sociated with increased pain (Hargreaves
et al., 1986).Thus, the levels of opioid peptides in plasma seemto
be useful diagnostic markers for quantitating theamount of pain and
stress perceived by patients. Sim-ilar analyses can be performed
for norepinephrineand serotonin.
A comparable monitoring of another area of oraldiagnostic
concern, tissue injury (trauma, post-sur-gery), can be achieved by
following plasma levels ofsubstances such as prostaglandins,
leukotrienes, bra-dykinin, and substance P. All of these analyses
also
-
10 BAUM et at. Adv Dent Res May 1989
Fig. 3 - Schematic representation of the role olf humoral
mediatorsin pain relief. An injury to the tooth sends a nerve
impulse to thebrain causing release of CRF (corticotropin-releasing
factor) fromthe hypothalamus. CRF next signals the pituitary to
secrete B-endorphins (p-End) in response to this pain stress.
(3-Endorphinscirculate through the blood stream and may act to
relieve paineither at the site of injury (the tooth), or in the
brain. (3-Endorphinscan be easily measured in blood samples taken
from patients by aradioimmunoassay procedure and can then be used
as a "physio-logical" measure to compare with behavioral measures
of painmade in parallel.
utilize radioimmunoassays with specific antibodies.These
diagnostic tests allow for accurate staging ofclinical problems and
therefore for accurate, and morespecific, therapeutic
intervention.
Development of other humoral analyses which cor-relate with oral
health status will likely be the subjectof considerable
investigative effort over the next fewyears. The cited, currently
available examples clearlyattest to the increased accuracy,
specificity, and sen-sitivity of such procedures as well as to
their appli-cability and usefulness with respect to problems
facedby the oral diagnostician.
INTERMEDIATE ADVANCES (-10 YEARS)
Research advances here focus on the developmentof new diagnostic
tools/methodologies, which are notuniversally available to clinical
medicine and den-tistry, but which at present exist conceptually,
andpractically, in the laboratory setting. These predic-tions are
derived from advances at the "current edge"of modern biology.
(1) Molecular Probes for Identifying Tumor Cellsand Identifying
Specific Therapies
There has been a veritable explosion of knowledgein the last few
years about how cell growth is con-
trolled. The focus of this development can arguablybe assigned
to cellular oncogenes, eukaryotic cellulargenes which have
considerable homology to onco-genes from transforming viruses.
Several categoriesof cellular oncogenes, and their phenotypic
proteinproducts, have been identified, and nucleotide probesare
available to detect their presence in cells. At pres-ent, many
laboratory studies are directed towardidentifying oncogene
expression or amplification fol-lowing developmental or mitogenic
stimuli. How-ever, a few studies have identified the presence
ofamplified oncogenes in human malignancies. For ex-ample, Aaronson
and his colleagues at the NationalCancer Institute have
demonstrated amplification ofthe mac oncogene in -15% of human
mammary car-cinomas (King et al, 1985). Similarly, a research
groupin Japan has identified oncogene amplification in asalivary
gland carcinoma (Semba et al., 1985). Thesemalignant cells may be
thought to display their un-controlled growth due to this
amplification process.The specific derepression event(s) allowing
for geneamplification is at present not known, but we cananticipate
progress toward its identification within fiveor so years. Thus, we
can predict that in 10 years, forsome malignant tumors, we will
know the gene de-rangement which results in uncontrolled cell
growth,including the actual perturbed, permissive geneticswitch.
Similarly, we will know, and be able to iden-tify
(immunologically), the protein products of theseoncogenes.
Accordingly, we expect that oral diagnostic re-search related to
cancer will in part be directed atidentifying these genetic
signals. This will allow fu-ture diagnosticians to use these types
of probes rou-tinely to identify the specific etiology of a
malignanttumor, both by molecular hybridization studies withbiopsy
samples and by analyses of tissue or serumfor protein products of
malignant transformation. Inprinciple, these techniques are quite
simple (Fig. 4).For example, nucleotide probes can interact
specifi-cally (hybridize) with complementary nucleic acid
se-quences in cells in situ or in extracted DNA. If
theoligonucleotide probe is labeled (e.g., isotopically), itcan be
detected readily, thereby indicating the pres-ence of the gene
sequence of interest. The proteinproducts of these genes can be
easily identified byimmunoassays, as noted earlier. With such
precisediagnostic knowledge, it will also be possible to de-sign
exact therapeutic reagents for specific types oftumors. These can
be targeted only to cells expressingthe malignant aberration a
considerable advanceover current non-specific forms of chemotherapy
whichaffect normal as well as tumor cells. These advances,for
general medicine, are now not far from achievingroutine
practicality. Indeed, the techniques describedin Fig. 4 have been
applied to identify viruses in var-ious tissues and have been
useful in suggesting theviral etiology of a specific oral
AIDS-associated lesion(e.g., Greenspan et al., 1985).
-
Vol. 3 No. 1 ADVANCES IN ORAL DIAGNOSIS U
A.
Biopsy D N A
From ExtractedSuspectedOralTumor
+~ DNA FragmentsTreatWithRestrictionEndonuclease
Electro-phoresisin Agarose
Gel. CanStain withEthidiumBromide for DNA
VisualizationorTransferby CapillaryAction toNitrocellulose
Filter("Southern Blot")
DNALengthinBasePairs
Identifym
Oncogene
Presence with32p-Oligonucleotide Probe andAutoradiography.
Probes forSeveral Oncogenes, Which areSuspected to be Involved, Can
beTested
B.
ImmunocytochemicalStaining ofAcinar Cells
From a SalivaryTumor withAntibody toOncogene
"ProteinProduct"
Fig. 4 Diagnostic methods to identify oncogenes in a biopsy
froma patient's tumor. A. Using molecular biological/biochemical
pro-cedures. B. Using immunocytochemical procedures. In Fig. 4B,
thebiopsy is fixed and incubated with buffer containing antibody
tothe oncogene "protein product". Next, the tissue is washed, anda
second antibody, coupled to peroxidase, is added. After
anotherwash, substrates for peroxidase are added. Deposited
reactionproduct is seen (black dots) where the oncogene "protein
product"is localized (here, in nucleus).
(2) Diagnostic Probes for Assessing FunctionalCapacity of
Salivary Epithelial Cells
In the last two to four years, our knowledge abouthow saliva
formation takes place has expanded enor-mously. We have recognized
several of the ion chan-nels and carrier-mediated transporters
which arenecessary for transepithelial cell water movement.These
include Ca2' -activated K' channels, Ca2 ' -ac-tivated Cl channels,
and the Na'/K'/Cl co-trans-porter. We also know most of the
neurotransmitterreceptor control mechanisms involved in these
fluid-generating events. Current laboratory developmentsin
identifying receptors by experimental imagingmethods and the advent
of isotopic probes for someion transport proteins (particularly the
Na' /K' /Clco-transporter) suggest that research efforts in
-10years hence will be directed at devising methods toallow oral
diagnosticians to ask discrete questionsabout the status of an ion
channel, a transport pro-tein, or a receptor coupling
mechanism.
Salivary gland dysfunction is a reasonably commonoccurrence.
Autoimmune exocrinopathies affect fromtwo to four million
Americans, and iatrogenic causesof gland dysfunction (radiation,
pharmaceuticals) are
frequently seen. In the extreme case (e.g., destructiondue to
autoimmune disease or to radiation damage),gland dysfunction may
be, at present, reasonablystraightforward to diagnose. However,
there are manydisorders of salivary glands for which a definitive
di-agnosis is difficult to reach. Obviously, managementof these
diagnostically elusive situations is also in-adequate. There are
now several examples in medi-cine of diseases which result from
subtle disturbancesin receptors or transduction molecules. The
best-characterized of such deficits is pseudohypoparathy-roidism
(Van Dop and Bourne, 1983). It is highly likelythat there are
salivary (and other oral tissue) disor-ders which result from such
discrete molecular dis-turbances. Future research will take the
currentgeneration of available molecular and immunologicprobes to
more practical levels (e.g., radionuclidescoupled to probes; Drayer
et al., 1982), making rou-tine assessments of the status of key
acinar cell plasmamembrane proteins possible both in situ, during
ac-tual function (Fig. 5), as well as with biopsied mate-rial in
vitro.
Such diagnostic progress, coupled with the presentprogress with
in vitro eukaryotic cell gene transfectionprocedures and the
anticipated success of gene trans-fection techniques in humans,
will pave the way forlong-term future research advances in managing
sal-ivary disorders. For example, we can speculate thatsuch
research will eventually lead to the following,or a similar,
clinical management scenario. After de-termining that a patient is
unable to secrete salivabecause acinar cells possess an apical
membrane Clchannel which is defective and unresponsive to stim-uli,
future clinicians will be able to target the insertionof the gene
coding for a functional Cl channel, or amodifier molecule, via
cell-directed vectors and thusrestore gland function (Wang and
Huang, 1987).
The intermediate period covered here will be onethat will make
commonplace the transfer of today'slaboratory molecular biological
advances into the rou-tine clinical setting. Technically, it is
becoming in-creasingly easier to produce nucleotide, peptide,
orimmunologic probes of exquisite specificity. The
oraldiagnostician of the not-too-distant future will indeedmake
molecular diagnoses. We feel very confidentthat at the period
around the turn of this century,oral diagnostic research will see
such tools in con-ventional use for a variety of oral problems such
asneoplasia and non-neoplastic oral mucosal diseases,viral
infections, autoimmune disorders, and gusta-tory and other sensory
dysfunctions.
LONG-TERM ADVANCES (-25 YEARS)
It would not be surprising that by this time, in theeconomically
advanced countries of the world, tra-ditional oral diseases
(caries, periodontal diseases) willnot be significant clinical
problems. Simple kits, touse at home, will be available for general
monitoring
-
22 BAUM et al. Adv Dent Res May 1989
HealthyControl
Patient with UnknownSalivaryDysfunction
Inject a hypotheticalprobe of interest, in thiscase an iodinated
ligandwhich binds to a Ca 2 + -activated CI" channel in
acinarcells. Visualize planes ofsalivary glands by a
computerizedtomographic analysis.
No liganddetected indicatinga lack of Ca2+-activatedCI" channels
in salivaryglands or the presence ofa defective channel incapableof
interacting with the ligand.
S M / S L
Detectionof ligandpresumablyinteractingwith
"normal"Ca2+-activatedCI" channelsP = area of parotid glandsSM / SL
= area of submandibular /sublingual glands.
Fig. 5 Use of a radionuclide-coupled probe, in conjunction
withphoton emission computed tomography, to assess the
functionalstatus of salivary acinar cell Cl~ channels.
of dental disease, salivary gland function, oral infec-tions,
etc. In addition, it is possible that most formsof cancer will be
easily diagnosed and readily treated.There will still be a place
for biologically oriented di-agnoses within dentistry, although we
speculate thatmany "oral" diagnostic decisions will be in the
handsof a relatively small group of highly trained individ-uals
(-5000) who will practice in sophisticated diag-nostic centers and
concentrate on what now mightbe thought of as subtle glandular,
neural, muscular,and skeletal disorders of the head, neck, and
face.Research emphasis in diagnosis will be substantiallydifferent
from that seen today; physical science willdominate over biological
science. Phenomenal gen-eral technological advances will be made in
the aero-space, communications, and defense industries overthe next
20-30 years, with spin-offs to all facets ofdaily life. This will
lead to revolutionary applicationsin physiology and health
sciences. In many ways, tous now, these belong in the realm of
science fiction.
We expect to see many patients (and patient sam-ples)
interacting with diagnostic instrumentation andcomputers, using
imaging techniques far more ad-vanced than found in today's
biophysics labs {i.e.,electron spin resonance, nuclear magnetic
resonance,x-ray diffraction). There will be little or none of
pres-ent-day physical diagnosis practiced. Clinicians willless
frequently lay hands on patients to assess pa-thology. Diagnosis
will not be done at the first signor symptom of a problem but on a
very routine (be-cause instrumentation will make it easy) and
veryfrequent basis. Patients who at such screening visitsshow
indications of developing pathology will be moreintensively
examined, and disordered molecules thencorrected or excised.
Diagnosis research at this timewill be directed at both
submolecular and supramo-lecular levels. Individuals involved will
have biolog-ical backgrounds but will be heavily trained in
physicsand engineering and will direct their efforts
towardproducing sophisticated molecular clinical-imagingtools.
CONCLUSION
All of medicine will change dramatically over thenext 25 years,
perhaps diagnosis more than most areas.The changes will be fueled
by advances in other, non-related, fields, but also by the
elimination of manymodern diseases. For comparison, take the case
ofthe medical diagnostician who graduated in 1940 be-fore World War
II and only retired last year frompractice. He (she) has witnessed
a dramatic shift inthe diseases he was called upon to detect, the
meanswith which he could detect them, and the tools withwhich he
could treat them. Similarly, the oral diag-nostician will be
shifted in focus dramatically in thenext 10-25 years. By the turn
of this century, ad-vances in oral diagnosis will be a full partner
of main-stream medical advances.
It is, as noted earlier, hard for us to predict withany
reasonable level of accuracy advances beyond a~ 10-year time-point.
We all, however, recognize thatadvances are occurring at
exponential rates. Most im-portantly, we believe that the next 10
years or so area time of almost unrestricted opportunity in oral
di-agnosis research. It is a time of new directions, whichcan be
taken readily from guidelines offered throughcurrent advances in
biology and medicine. We be-lieve that this should give
considerable encourage-ment both to young oral health investigators
concernedabout future clinical research opportunities and to
thedental profession at large, because new practice vis-tas will be
charted. Since many of these advances arein areas which are
non-traditional with respect todental practice, we believe that
substantial attentionmust be paid to transferring advances to the
clinicalarm of the profession. This portends significantchanges in
dental education directed both at the ac-
-
Vol. 3 No. I ADVANCES IN ORAL DIAGNOSIS 13
quisition of the necessary scientific background andthe
alteration of existing "practice behaviors".
REFERENCESDRAYER, B.; JASZCZAK, R.; COLEMAN, E.; STORM, A.;
GREER,
K.; PETRY, N.; LISCHKO, M.; and FLANAGAN, S. (1982):Muscarinic
Cholinergic Receptor Binding: in vivo Depiction UsingSingle Photon
Emission Computed Tomography and Radio-iodinated Quinuclidinyl
Benzilate, / Computer Assist Tomogr 6:536-543.
FINE, D.H. and MANDEL, I.D. (1986): Indicators of
PeriodontalDisease Activity: an Evaluation, / Clin Periodontol 13:
533-546.
GREENSPAN, J.S.; GREENSPAN, D.; LANNETTE, E.T.; ABRAMS,D.J.;
CONANT, M.A.; PETERSEN, V.; and FREESE, U.K. (1985):Replication of
Epstein-Barr Virus within the Epithelial Cells ofOral Hairy
Leukoplakia, an AIDS-associated Lesion, N Engl JMed 313:
1564-1571.
HARGREAVES, K.M.; DIONNE, R.A.; MUELLER, G.P.; GOLD-STEIN, D.S.;
and DUBNER, R. (1986): Naloxone, Fentanyl andDiazepam Modify Plasma
Beta-Endorphin Levels During Sur-gery, Clin Pharmacol Ther 40:
165-171.
HUGHES, C.V.; BAUM, B.J.; FOX, P.C.; MARMARY, Y.; YEH,C.-K.; and
SONIES, B.C. (1987): Oral-Pharyngeal Dysphagia: aCommon Sequela of
Salivary Gland Dysfunction, Dysphagia 1:173-177.
JEFFCOAT, M.K.; WILLIAMS, R.C.; KAPLAN, M.L.; and GOLD-HABER, P.
(1985): Bone-seeking Radiopharmaceutical Uptakeas an Indicator of
Active Alveolar Bone Loss in Untreated andSurgically Treated Teeth
in Beagle Dogs, / Periodont Res 20: 301-306.
KING, C.R.; KRAUS, M.H.; and AARONSON, S.A. (1985):
Am-plification of a Novel v-erb B-related Gene in a Human Mam-mary
Carcinoma, Science 229: 974-976.
SEMBA, K.; KAMATA, N.; TOYOSHIMA, K.; and YAMAMOTO,T. (1985): A
v-erb B-related Protooncogene, c-erb B-2, is Distinctfrom the c-erb
B-1/Epidermal Growth Factor-Receptor Gene andis Amplified in a
Human Salivary Gland Adenocarcinoma, ProcNatl Acad Sci USA 82:
6497-6501.
SHAWKER, T.H.; SONIES, B.; STONE, M.; and BAUM, B J.
(1983):Real-time Ultrasound Visualization of Tongue Movement
Dur-ing Swallowing, / Clin Ultrasound 11: 485-490.
SKALERIC, U.; DOLINSEK, J.; STEPISNIK, J.; CEVC, P.; andSCHARA,
M. (1987): NMR Imaging in Dentistry: Relaxation andDiffusion
Studies, Adv Dent Res 1: 85-87.
VAN DOP, C. and BOURNE, H.R. (1983): Pseudohypoparathy-roidism,
Ann Rev Med 34: 259-266.
WANG, C.-Y. and HUANG, L. (1987): pH Sensitive Immuno-liposomes
Mediate Target-cell-specific Delivery and ControlledExpression of a
Foreign Gene in Mouse, Proc Natl Acad Sci USA84: 7851-7855.