Embed Size (px)
Citation preview

ADVANCED PRACTICE PROVIDER INITIATED ADVANCE CARE PLANNING
DISCUSSIONS TO ENHANCE PATIENT- CENTERED END OF LIFE CARE
A SCHOLARLY CLINICAL PROJECT SUBMITTED IN PARTIAL FULFILLMENT OF THE
REQUIREMENTS FOR THE
DEGREE OF DOCTOR OF NURSING PRACTICE
IN THE GRADUATE SCHOOL OF THE
TEXAS WOMAN’S UNIVERSITY
COLLEGE OF NURSING
BY
POONAM GOSWAMI MS, BSN, FNP-C
DENTON, TEXAS
March, 16 2019

iii
ACKNOWLEDGEMENT
The completion of this degree program is dedicated to my late father Vijay Prakash
Sharma, and my mother Raj Rani Sharma, without them I would not be the person I am today.
My sons Akshay and Chirag have been my motivation for studying at this age. I want to thank
my husband Navneet, for his patience and support throughout my educational journey.
Dr. Michael Mistric, the chair of the Doctor of Nursing Practice (DNP) committee has
been a guiding light. Thank you for all your warm encouragement and knowledge. To my
committee member, Dr. Sabrenda Littles, thank you for reviewing my final project paper writing.
I must acknowledge Dr. Sandra Cesario my advisor, thank you for your encouragement
throughout my DNP journey, especially being an advocate for End of Life conversations. I not
only learned through elective End of Life class but also developed passion towards this critical
topic.
I want to thank Dr. Diane Barber, my manager and my mentor for selecting me as part of
the Advance Practice Provider team in the department of Investigational Cancer Therapeutics
(ICT) at MD Anderson Cancer Center, and her step by step guidance for my success in the
department as well as on my project. I also would like to acknowledge Dr. Sabrina Mikan,
Director of Palliative and Supportive care, who advised and enhanced my understanding on
Advance Care Planning through her initiation of My Choice My Wishes program at Texas
Oncology.
Finally, I would like to thank GOD for the one and only one responsible for everything in
my life.
Poonam Goswami

iv
ABSTRACT
Advance Care Planning (ACP) is the process by which patients, with their healthcare provider
and family establish values, goals, and preferences for future care, and include discussions on
End of Life (EOL) care options. Advance Directives (AD) provide written documentation of
patient’s wishes for future care and comprise of a Medical Power of attorney, living will
document, and an Out-of-Hospital Do Not Resuscitate (OOHDNR) order. Institute of Medicine
(IOM) in their 2014 report, Dying in America, identified an urgent need for improvement in
health care at the end of life. The IOM also called for patient-centered EOL care that honors
individual preferences and promotes quality of life. Cancer patients experience the high cost of
care, may also receive unwanted treatment towards the EOL, and additional suffering, which
may not reflect their values and goals. The problem exists that only 20% of the patients have
completed AD documents in the Department of Investigational Cancer Therapeutics (ICT), and
admitted patients’ resuscitation status remains a full code, which includes a cardiopulmonary
resuscitation, and endotracheal intubation with mechanical ventilation. This Doctoral of Nursing
Practice project consists of designing, implementing, and evaluating the effect of ACP
discussions initiated by an Advanced Practice Provider with advanced cancer patients and their
family members in the ICT department. The project aims to enhance patient-centered EOL care
with a goal to increase the AD completion and /or a change in code status of the patients referred
to ICT department.
Keywords: advanced cancer patients, advance care planning discussions, advance
directives, end-of-life (EOL), code status

v
TABLE OF CONTENTS
ACKNOWLEDGEMENT……………………………………………………………….....iii ABSTRACT………………………………………………………………………………...iv Chapter
I. INTRODUCTION…………………………………………………………………...1
Problem Statement...........................................................................................1 Theoretical Framework....................................................................................4
II. LITERATURE REVIEW.............................................................................................7
III. METHODOLOGY......................................................................................................15
IV. RESULTS....................................................................................................................26
V. DISCUSSION..............................................................................................................31
REFERENCES........................................................................................................................36 APPENDICES..........................................................................................................................45
A. Level of Evidence
B. Synthesis of Literature
C. Project Timeline
D. Email from Patient education director
E. Proposal Application to MD Anderson

vi
F. Power Point Presentation at PFAC
G. Feedback from PFAC
H. Proposal Approval from MD Anderson
I. Approval from TWU IRB
J. ACP Certification
K. ACP Slogan and letter for ACP folder
L. Rosswurn and Larrabee change model
M. Plan-Do-Study-Act model
N. Cost Benefit and Potential cost avoidance

1
CHAPTER I
INTRODUCTION
Problem and Significance
National guidelines from the American Society of Clinical Oncology (ASCO) and the
National Comprehensive Cancer Network (NCCN) recommend that Advance Care Planning
(ACP) discussions take place within three months of a diagnosis of incurable cancer (Bestvina &
Polite, 2017). ASCO's Quality Oncology Practice Initiatives emphasizes documentation of
patients' advance directives by the third office visit as a metric for quality care (Bestvina &
Polite, 2017). Institute of Medicine [IOM] (2014) specifies that lack of ACP conversations is the
result of lack of initiation from patients, family members, and providers, which results in a wait
for each other on these important discussions
Studies have shown that ACP results in completion of the Advance Directives (AD) or
related clinician orders such as do-not-resuscitate (DNR) orders (Billings & Bernacki, 2014;
Houben, Spruit, Groenen, Wouters, & Janssen, 2014; Luckett et al., 2014). The AD enable the
patients to articulate and convey their treatment preferences while their cognitive status is intact,
and comprises of a durable power of attorney for healthcare designation, a living will that
articulates a person’s wishes regarding treatment, resuscitation with CPR including mechanical
ventilation, and tube feeding at the end of life (Carr & Luth, 2016). ACP discussions also
provide better outcomes for family members, including reduced decision making burden,
reduced anxiety and depressive symptoms (Stein et al., 2013).
Problem Statement and Significance with Economic, Policy, and Health System The cost of end of life (EOL) care in the U.S. in the year 2011 was approximately $205
billion or 13% of the total healthcare cost. This cost was among 80 % of the population who fall

2
in the high health care cost due to their disease (Aldridge & Kelly, 2015, p. 517). Cancer is
considered a high health care cost disease, and according to American Cancer Society, direct
medical costs (total of all health care costs) for cancer was $80.2 billion in the U.S. in the year
2015. The cost noted was increased to $147. 3 billion in 2017 (cancer.gov, 2018). Effective
January 1, 2016, Medicare started covering ACP as a separate service by providers using the
physician fee schedule and the Current Procedural Terminology [CPT] code 99497. There is also
an add-on code 99498 for each additional 30 minutes for a face to face ACP discussion (Centers
for Medicare & Medicaid Services [CMS], 2016). At MD Anderson Cancer Center, patients are
referred to the department of Investigation Cancer Therapeutics (ICT) for clinical trial options
after all standard treatment options for the metastatic cancers are exhausted. Patients with
metastatic and progressive disease on admission remain a full code. Due to this, any deterioration
in the clinical status places an extra burden on the family and providers. The Institution had an
initiative to encourage the ACP discussions and help patients complete the AD documents.
Unfortunately, according to Alma Rodriguez (personal communication, December 20, 2017),
only 20 % of the patients in the ICT had completed the AD.
Stakeholders. According to Hughes (2008), the Quality Improvement (QI) process
should involve all stakeholders and gain their understanding that the investment of proposed
resources will be regained with efficiency and reduction of adverse events. The primary
stakeholders for this project includes the clinical administrative director (CAD), nurse manager,
social workers, Advance Practice Provider [APP] (DNP student), APP manager, physicians,
patients and their family. Hughes (2008) recommends stakeholders to prioritize the process
which needs an improvement, and develop strategies and process improve the identified
problem, and finally assist with data collection and implementation of proposed changes

3
(Hughes, 2008).
Purpose of the Study. This quality improvement (QI) project aimed to increase the
awareness among the advance practice providers (APPs), and physicians on the importance of
initiating the ACP and end of life (EOL) discussions for all patients with advanced cancer
referred to the department. The ACP discussions are a part of institutional initiative, and hence
having the ACP discussions, documenting them in patients’ electronic medical record (EMR)
will ensure the compliance with the institutional initiative. This QI project proposed to determine
if the ACP discussions initiated by the APP with - 20 clinic patients, as well as 20 patients
admitted to the ICT department, would enhance patient-centered EOL care reflected by an
increase in the completion of advance directives (AD) and /or change in the code status of
patients with advanced cancer.
The project aimed to promote APPs’ initiation of ACP and EOL discussions with
advanced cancer patients by implementing and evaluating an educational intervention and a
folder provided to the patients and families. The goal was to enhance shared decision making
care in line with patients’ wishes, strengthen patient autonomy, change in the code status of the
patients when they are admitted to the hospital.
The intervention aims were (a) to increase the ACP discussions conducted with advanced
cancer patients of ICT department, (b) to increase the AD completion rate in the department, and
(c) to increase APP and physicians’ intention to change practice regarding ACP discussions with
advanced cancer patients referred to the Department of Investigational Cancer Therapeutics
(ICT).
The PICOT Question. It is critical that the ACP discussions with patients and family be
initiated at diagnosis of advanced cancer and should not delay until the patient is incapacitated.

4
The hypothesis is, “Does initiation of advance care planning discussions by an advance practice
provider with advanced cancer patients enhances patient-centered end of life care and result in an
increase completion of advance directives and /or change in code status?”
Theoretical Framework The theoretical framework selected for guiding the ACP discussions was Roy’s
Adaptation Model (RAM). The use of models in nursing allows nurses to focus on the role of
nursing and its application, and helps patient care to be systematic, purposeful, controlled and
effective. RAM was developed by Sister Callista Roy in the late 1960s, and it defines nursing as
a scientific and humanistic profession, and emphasizes the importance of nurses’ specialized
knowledge in contributing health needs and well-being of the community (Roy, 2009).
The metaparadigm concepts of RAM are person, environment, health, and nursing. RAM
sees a person in constant interaction with the environment, uses innate or acquired mechanisms
to adapt, includes people as individuals or groups, and utilizes health-illness continuum
(Ursavas, Karayurt, & Iseri, 2014). This model was important in guiding me in this DNP project
because, ACP discussions with advanced cancer patients is a service that helps to maintain
patient autonomy, enhances the shared decision making with knowledge sharing between patient
and providers. As mentioned by Eldridge (2017), this model allows the providers to understand
patients’ adaptation process, help the patients to cope and adapt towards changing state of health,
and can also assist the family to find ways to enhance their coping skills. RAM advocates that
the nursing purpose is to ensure adaptation. RAM encourages advanced cancer patients to adapt
to their changing environment secondary to their deteriorating health condition related to
advanced cancer disease, thus ultimately changing their focus on quality of life based on their
values, and goals of care. Increasing adaptation during health and disease improves the

5
interaction between the environment and health systems, and promotes health, therefore, it
contributes to health, quality of life and end of life care (Ursavas, Karayurt, & Iseri, 2014).
Significance of the Study. Uhler et al. (2015) emphasizes the importance of shared
decision making among patients and their physicians. Advance care planning (ACP) and AD
completion helps to ensure patients receive healthcare that they prefer toward the EOL
(Bernacki, Block, & American College of Physicians High-Value Care Task Force, 2014). When
patients lack ACP or have not completed an AD, there can be unnecessary and unwanted
interventions, and increased cost of care the patient and family incurs (Bernacki & Block, 2014;
IOM, 2014); this scenario is a significant facilitator of this pilot project. ACP and ADs are
helpful for patients and their healthcare providers because they guide care based on the patient's
wishes and preferences even when the patient is unable to speak on their behalf (McCusker et al.,
2013; Schrijvers, Cherny, & ESMO Guidelines Working Group, 2014). Nurse practitioners have
the opportunity to discuss ACP and ADs during their initial contact with patients. According to
Dube, McCarron, and Nannini (2015), those who received education and training on EOL topics
are more likely to engage patients in ACP. The DNP student who conducted this study is an
advanced practice registered nurse (APRN) and attended the ACP certification to enhance ACP
conversation skills. Studies have shown that health care providers benefit from education and
training in ACP. Findings from a study by Chung, Oczlowski, Hanvey, Mbuagbaw, and You
(2016) on interventions for physicians increased knowledge, self-efficacy, and communication
skills in ACP. The results of the project will provide guidance and preparation of physicians and
other APPs in the department thereby developing confidence in the ACP discussions. Alleviating
obstacles to EOL care begins with reforming policies to promote ACP discussions and helping

6
the AD document completion (Sonenberg & Sepulveda-Pacsi, 2018). The strategies will be used
to facilitate ACP discussions with every patient in the ICT department.
This quality improvement (QI) project finding provides APPs and physicians with
additional training to enhance ACP discussions. Implementation of the ACP discussions with
every patient of the ICT department will streamline the process encouraging the patients on
completion of AD, reflecting the care in line with their wishes.

7
CHAPTER II
LITERATURE REVIEW A comprehensive search for evidence was conducted via the Texas Woman's University's
online library database collections as well as MD Anderson Cancer Center’s medical research
library. The search engines included PubMed, CINHAL, Medline, Cochrane, and TWU
Universal. The search terms included the following keywords: advance care planning, ACP
conversation or communication and/or discussion, advance care planning in cancer, advance care
planning, and advance practice providers, advance care planning barriers, and interventions, End
of Life (EOL) decision making, EOL discussion, advanced directive, living will, and durable
power of attorney.
Inclusion criteria for articles included (a) published within the last ten years, (b) English
language, and (c) human subjects. These searches yielded a total of 150 articles. The exclusion
criteria of the article included (a) absence of advance care planning discussions and (b)
interventions more than ten years old. Preferences included studies related to the oncology
settings, and conducted within five years, 2013 or after. However, two articles of 2012 and one
2010 were included due to their significant contributions for this project. A total of 50 relevant
articles were selected for this paper, and there were four major themes extracted for synthesis of
25 articles.
Result from the synthesis of the 25 studies included various study designs: one evidence-
based guideline, four systematic reviews of quantitative studies, one Meta-analysis, six
quantitative randomized control trials, three cohort studies, one QI project, one feasibility study,
and eight qualitative studies. The levels of evidence indicated by Melnyk Levels of Evidence
included six articles for levels of evidence I, seven articles of levels of evidence II, none for

8
levels of evidence III, three articles level of evidence IV, two articles for level of evidence V and
seven articles for levels of evidence VI (Melnyk & Fineout-Overholt, 2015; see Appendix-A).
Major Themes of ACP & EOL
Four themes emerged from the synthesis of literature to support the need for this DNP
pilot project on the importance of ACP and AD completion. The themes included six relevant
studies for benefits of ACP, eight studies include barriers to ACP, nine studies for ACP timings,
and finally, a total of nine studies shows various interventions used to enhance the ACP and EOL
care. Seven studies were conducted in the oncology setting, of which six studies were
randomized control trials (RCT) studies for interventions for ACP (Appendix-B).
Benefits of ACP. Many articles included in the literature search highlighted the benefits
of ACP for patients and their families.
Increased patient autonomy, decrease family/surrogate anxiety, and decision making
burden. According to Klingler, Schmitten, and Marckmann (2015), facilitated ACP strengthens
patient autonomy and lowers the net cost of care by reducing unwanted and unnecessary
treatment towards the EOL, and can reduce family burden. Chiarchiaro, Buddadhumaruk,
Arnold, and White (2015) described the association of ACP discussions with less decisional
conflict among the surrogates of patients critically ill with acute respiratory distress syndrome.
Improved quality of care near the end of life. According to Bestvina and Polite (2014),
ACP lowers the rates of ventilation, resuscitation, intensive care unit admission, early hospice
enrollment with a decreased cost of care at the end of life, and an improved quality of care near
the end of life (Klingler et al., 2015). A systematic review without meta-analysis by Brinkman-
Stoppelenburg, Rietjens, & Heide, 2014) found a positive impact of ACP on AD completion

9
rates and compliance with end-of-life wishes. This review demonstrated increased use of
palliative care by shifting the goal of care from curative to palliative care and shifting on
symptom management with improving quality of life. Houben et al. (2014) suggest that ACP
reduces the number and length of hospital admissions, whether for life-sustaining treatments or
EOL care.
Place of death based on the patient's preference. ACP provides an opportunity for
patients with a life-limiting illness to verbalize preferences of dying at home - a location of their
choice- which increases the likelihood of it happening. It allows health care professional and care
providers to make arrangements so people nearing the end of life can spend more time at home
in home hospice rather than the hospital (Khan et al., 2014).
Barrier to ACP. Various barriers for ACP discussions include lack of time, patient and
family reluctance, oncologists’ discomfort, lack of experience, lack of education in ACP
conversations, lack of system support/resources, lack of understanding of ACP, the lack of active
collaboration, communication between specialties, and poor timings of the ACP discussions
(Chander et al., 2017; Granek, Krzyzanowska, Tozer, & Mazzotta, 2013; Nedjat-Haiem et al.,
2016; O’Hare et al., 2016; Zhou, stoltzfus, Houldin, Parks, & Swan, 2010).
Lack of time. A study with a cross-sectional online survey by Chander et al. (2017) on
oncologists, oncology support staff, cardiologists and PCP reported lack of time as the main
barrier to ACP discussions. Zhou et al. (2010) findings are similar to the findings of Chander et
al. (2017) showing that time restraint is a significant factor in avoiding discussion of ACP with
patients.
Discomfort (patients, family, and provider). Granek, Krzyzanowska, Tozer, and
Mazzotta (2013) reported patient and family reluctance, oncologists' discomfort, lack of

10
experience, lack of education in ACP conversations, and lack of system support/resources as
barriers to ACP discussions. IOM (2014) and Odejide et al. (2016) describe the reluctance of
some providers due to fear of affecting patients’ hope and emotional coping or patients’ view of
provider giving up. Zhou et al. (2010), in their study on oncology patients, found that the
physicians were reluctant to address ACP due to the feeling of being rushed thus delaying ACP
and focused on treatment options (Zhou et al., 2010).
Lack of experience, understanding, and Collaboration. Studies on perspectives and
perceptions of multidisciplinary providers of patients with chronic illness reveal that lack of
knowledge of ACP, lack of experience in ACP conversations, and lack of collaboration and
communication between specialties were barriers to ACP (O’Hare et al., 2016; Nedjat-Haeim et
al., 2016).
Timing of ACP. IOM, in their 2014 report, Dying in America, identified an urgent need
for improvement in health care at the end of life. IOM (2014) emphasized that all patients should
have the opportunity to participate in ACP and receive care based on their goals, values, and
preferences (IOM, 2014). National guidelines from the American Society of Clinical Oncology
(ASCO) and the National Comprehensive Cancer Network (NCCN) recommend that ACP
discussions take place within three months of a diagnosis of incurable cancer (Bestvina & Polite,
2017; Levy et al., 2009). ASCO's Quality Oncology Practice Initiatives emphasizes
documentation of patients' advance directives by the third office visit as a metric for quality care
(Bestvina & Polite (2017), Bernacki et al., (2014), IOM (2014), and Mack et al. (2012)
recommend ACP discussions before patients’ becoming ill or early in the chronic disease process
with patients.

11
A need for earlier ACP conversations. Early ACP and EOL discussions were noted to
provide less aggressive care, and care in line with patient wishes, (e.g., acute care hospitalization,
chemotherapy, ICU admission, and associated ICU procedures and treatments), and greater
hospice utilization (Epstein, Shuk, O’Reilly, Gary, & Volandes, 2015). A qualitative study by
Pollock & Wilson (2015) suggests that if the ACP process is launched too late in the disease
trajectory, it is less likely to be effective. ACP discussions later in the disease trajectory impede
patients to plan and preserve their autonomy at the end of life (Pollock & Wilson, 2015). A study
by Odejide et al. (2016) suggested that there is minimum or no benefit of ACP discussions if the
timings were not appropriate, as 56% of the study respondents reported that EOL discussion
occurred too late to be most beneficial. According to Mack et al. (2012), patients with terminal
cancer had their first EOL conversation an average of 33 days before death, and 55% occurred
while hospitalized (Mack et al., 2012).
Routine and regular ACP discussions. While many studies emphasize early ACP
discussions, IOM (2014) also recommended frequent evaluation and updates to the ACP to
ensure goals, values, and preferences in response to the changing circumstances of the patient
and family. Bestvina and Polite (2017), place emphasis on the expectation for high-quality
patient care and suggests that ACP occur regularly in outpatient oncology clinics. According to
McCusker et al. (2013), one-third of the patients alter their AD because of progression of
disease, hospitalization, health status changes, social issues, and functional ability and hence
providers need to improve on the assessment and reassessment of patient’s goals of care and
documentation of this on-going conversation (McCusker et al., 2013).
Interventions to enhance ACP. ACP may help patients receive treatments that align
with their goals of care through shared decision making (Uhler et al., 2015). Spoelhof and Elliott

12
(2012) advocated for simplifying the terminology used in the AD forms for patients, use of
interactive interventions, such as face-to-face conversations and repeated conversations about
completion of ADs over time, providing the opportunity for the patient and their family to ask
questions and receive assistance (Spoelhof & Elliott, 2012).
The literature search revealed various interventions used to enhance the ACP discussions.
The interventions include using values and goals and educating of patient, family through (a)
vignette technique, (b) educational pamphlets, (c) website training, and (d) video education on
CPR with or without narratives. Another intervention consisted of preparing the staff and
providers through (a) face-to-face education, (b) vignette technique, and (c) support through the
electronic medical records/communication support program.
Use of Values and goals of care questionnaire. Hoverman et al. (2017) provide
information on a quality improvement study in a community oncology setting, where the use of
value assessment tool stimulated the ACP discussions. This study showed a positive outcome
with 58% of the patients completing the AD over a period of 27 months. Menon et al. (2016)
conducted a pilot RCT and used values inventory to enhance the ACP and EOL discussions.
Use of CPR video with and without narration. Volandes et al. (2013) and Epstein et al.
(2015) demonstrated that use of a CPR video with narration could enhance patients'
understanding of the resuscitation. Following this, the family, as well as patients, chose DNR as
a desired option instead of aggressive treatment options towards the end of life.
Use of educational pamphlets. An RCT by Stein et al. (2013) demonstrated that an
intervention to enhance the understanding of ACP through educational brochures before the ACP
discussion can increase DNR as an option towards EOL.
Use of online website and tools. Sudore et al. (2017) conducted an RCT to evaluate the

13
efficacy of an interactive, patient-centered website (PREPARE) with an easy- to- read AD to
increase ACP discussions in older veterans with chronic illness. This study reported higher ACP
documentation compared to AD alone (35% vs. 25%).
Staff education. Michael and colleagues (2016) described the analysis of data from three
studies to place the importance of Vignettes and conducted a staff training through role-playing
or case discussions as part of face-to-face interventions to improve knowledge and information
to facilitate the initiation of ACP discussions.
Improvement of the workflow. Obel et al. (2014) provide information on the feasibility
of conducting ACP early in the patients with Stage IV cancer with the help of systematic
improvement in workflow through training seminars for the providers; improving electronic
medical records, and preparing the patients and family with the help of an educational
guidebook. Walczak et al. (2017) conducted RCT to evaluate the efficacy of nurse-facilitated
communication support program for advanced cancer patients to assist in discussing prognosis
and EOL care. The findings showed that communication support program was effective and
well received solution to encourage early information on EOL.
Lessons learned from the literature search There is a need for ACP discussions with patient and families. Inadequate ACP results in
more aggressive treatment than what the patient desires (Bernacki et al., 2014; IOM, 2014).
Improving patient education and awareness of ACP is beneficial in helping patients consider and
communicate their preferences to providers who then document their wishes as part of the
medical record (Butler et al., 2014). The findings from several studies showed a positive
correlation with the use of AD and decreased rate of hospitalization, reduced chances of dying in
hospital and dying at the patient's place of choice-home, reduced use of life-sustaining

14
treatments, and an increased use of hospice or palliative care towards EOL (Brinkman-
Stoppelenburg, Rietjens, &Van der Heide, 2014; Khan et al., 2014). The literature search
provided various interventions that could be used to promote ACP discussions and enhance
patient-centered EOL care. There is a need to develop standards which are evidence-based,
measurable, actionable, and be reported publicly (Bernacki et al., 2014; IOM, 2014).

15
CHAPTER III
METHODOLOGY
Advance Care Planning discussion results in completion of the AD or related clinician
orders such as do-not-resuscitate (DNR) orders (Billings & Bernacki, 2014; Houben et al., 2014;
Luckett et al., 2014). An AD enables the patient to articulate and convey his/her treatment
preferences while their cognitive status is intact (Carr & Luth, 2016), and provides better
outcomes for family members, including reduced decision making burden, reduced anxiety, and
depressive symptoms (Stein et al., 2013). The presence of AD has been shown to decrease the
rate of hospitalization, decrease the use of life-sustaining treatments, and increased the use of
hospice or palliative care services. ACP helps patients spend more time at home towards the
EOL in a home hospice, resulting in dying at home - a place of death, based on patients'
preference ( Brinkman-Stoppelenburg, Rietjens, & van der Heide, 2014; Khan et al., 2014)
Project Objective This quality improvement project was proposed to determine if the ACP discussions
initiated by the APP (DNP student) with a total of 40 patients (20 hospitalized and 20
ambulatories) of ICT department, would enhance patient-centered EOL care reflected by an
increase in the completion of Advance Directives (AD) and /or change in the code status of
patients with advanced cancer. A meta-analysis of 25 articles extracted four major themes on
ACP and EOL including various interventions to enhance the ACP discussions. Bernacki et al.
(2014) and Mack et al. (2012) advocates on one-on-one provider-patient counseling. Spoelhof
and Elliott (2012) recommends face-to-face conversations, and simplifying the terminology used
in the AD forms for patients, repeated conversations about the completion of ADs over time, and
providing the opportunity for the patients and their family to ask questions and receive assistance

16
(Spoelhof & Elliott, 2012).
Study Design This quality improvement project used a descriptive study design in two phases, a
retrospective data collection and an ACP intervention. Phase 1 involved a retrospective data
collection with a chart review of the patients without a scanned AD in the EMR at the time of
admission/clinic visit. Baseline data was obtained for September 2018 on first 20 admitted
patients who were noted to have no scanned AD in EMR and 5 patients of each four physicians
of ICT on one clinic day in September 2018. Phase 2 consisted of a post ACP intervention data
eight weeks following the ACP discussion by APP (DNP student) on 20 admitted and 20
ambulatory visit (clinic) patients. The data collection included ACP documentation and AD
completion for 20 admitted patients and 20 patients of four physicians on one clinic day.
Theoretical/Conceptual Framework According to Stevens (2013), Evidence-Based Practice (EBP) is a process which
combines research evidence with clinical expertise and encourages to individualize the care
which includes patient preferences (Stevens, 2013). EBP can facilitate ongoing Quality
Improvement (QI) measures by standardizing care process that is more efficient and effective for
improving organizational and patient outcomes (Hughes, 2008). Theoretical and conceptual
models can be used to provide structure and guidance to a QI project. QI measures aimed at
making positive changes in healthcare processes can often lead to more favorable outcomes for
an organization (Hughes, 2008).
Evidence-Based Change Model. Russwurm and Larrabee's Evidence-Based Practice &
Change Model is frequently used in healthcare organizations for QI projects. This model
provided excellent guidelines for this quality improvement project. Rosswurn and Larrabee
17
(1999) developed a six-step model for change in Evidence-Based Practice (EBP) that aims for
the integration of EBP into a care delivery system (White, Dudley-Brown, & Terhaar, 2016).
Plan Do Study Act model uses a cyclical method for impacting and assessing change for quick
implementation before the system-wide change (Hughes, 2008).
The six steps of Rosswurn and Larrabee's model include:
Step 1 - An assessment of the need for change with the comparison of internal and
external data. This step includes the initial assessment for the need for ACP due to low (20%)
AD completion rate in the ICT department;
Step 2 - Once problem identification, link it with interventions and outcomes (standard
interventions if possible). Following step two of the model, the ACP discussions were initiated
with 20 clinics' as well as 20 admitted patients of ICT department by the APP (DNP student);
Step 3 - Synthesize the best evidence (research and contextual evidence). This step
includes meta-analysis of 25 articles which provided information on various interventions to
enhance the ACP discussions. Best intervention selected for intervention includes face-to-face
conversation and reviewing of the AD forms with the patients;
Step 4 - Change how the practice is designed. The results of the study were presented at
the monthly APP meeting as well as to the faculty and department leadership;
Step 5 - Implementing and evaluating the change in practice including process outcomes.
The department APPs were presented the findings of the project, and the plan is to work with
leadership to hire additional APP and incorporate ACP discussions with every patient presenting
at the Fast Track clinic; and finally,
Step 6 - Integrating and change to everyday practice. Following the last two steps of the
model, the DNP student is working closely with department leadership as well Institutional ACP

18
initiative task force to provide guidance on strategic planning for integrating ACP discussions in
our daily practice starting with ICT department, and plan to expand it to other departments. The
DNP student is selected as a core member for the EOL task force for strategic planning for the
Institution.
PDSA Model. The Plan-Do-Study-Act (PDSA) model is also frequently used in
healthcare organizations for QI projects. The PDSA model establishes a functional or causal
relationship between changes in processes and expected outcomes of a QI project (Hughes,
2008). The PDSA cycle begins with assessing the scope of the problem, what changes should
occur, development of a plan for proposed change, identification of stakeholders, identify
outcome measures, and place of targeted QI strategy (Hughes, 2008). PDSA involves the four
steps consisting of plan, do, study, and act (See Appendix M).
Project Timeline The pilot project was estimated be conducted over 6 months from October 2018- March
2019, or until the total number of proposed patients was completed (Appendix C). The Plan
phase was based on observation of the clinical deterioration and lack of AD on the admitted
patients of the ICT department. The project planning was initiated at the beginning of the Fall
semester; hence a meeting with ICT leadership was arranged by DNP student on August 29,
2018. The members invited were ACP physician champion, clinic administrator, nurse manager,
APP manager, MD Anderson's ACP initiative project manager, and myself APP (DNP student).
This meeting validated the need for the quality improvement project in the department. A
meeting was then arranged with DNP Project Chair for approval on the DNP project topic of
interest. The project objectives and instruments which included survey questions were developed
by the DNP student and edited by Patient Education department for readability (Appendix D).

19
The proposal for the QI project was submitted at MD Anderson's Quality Improvement
Assessment Board (QIAB) on October 23, 2018 (Appendix E), and was approved on November
13, 2018 (Appendix H). Finally, the application was submitted for expedited review was
submitted to and reviewed by the Texas Woman University's IRB on November 21, 2018
(Appendix I).
The Do phase involved another meeting on December 4, 2018, with the ACP team and
included department social workers and finally the implementation of established interventions
from December 5, 2018, with baseline data collection and completed on January 23, 2019 (a
break from December 25, 2018, to January 8, 2019, as the DNP student was on vacation).
The Study phase began on February 5, 2019 after collecting the data from the EMR of the
study population on ACP discussions and AD completion. The data were analyzed and
interpreted in February by Statistician assigned for nursing research.
The Act phase completed in March 2019 after the project outcome and recommendations
were given to the ICT leadership. (Appendix C).
Ethical Considerations The DNP student, an APRN, followed the Code of Ethics for Nurses with Interpretive
Statements. The provision 1.4 Right to self-determination specifies that nurse should educate and
advocate the patient’s legal right to self-determination. Hence promoting advance care planning
conversations, discussing benefits and limitations of various AD documents enables the patients
to maintain their right to self-determination (ANA, 2015, p. 4). ANA (2015) code of nursing
emphasizes the importance of applying research into practice as an essential aspect of nurses'
role. This QI project integrated findings from the literature on various ACP interventions to
enhance patients’ understanding regarding the AD documents. The Quality Improvement

20
Assessment Board (QIAB) at the MD Anderson Cancer Center approved the project as a QI
project. The Institutional Review Board (IRB) at Texas Woman’s University concurred with MD
Anderson’s QIAB and determined that IRB review was not needed (Appendix H & I).
Population and Sample The population of this project included advanced cancer patients in the ICT department.
The study was conducted in a dual setting (outpatient and inpatient) on patients managed through
the ICT service in a cohort of 40 total patients [ambulatories (20) and hospitalized (20)] enrolled
in the clinical trial. A convenient sample of a total of 40 patients assigned to the APP (DNP
student) was selected based on the lack of AD scanned in patients' electronic medical record
(EMR). Medical decision-making capacity was also a part of the inclusion criteria.
Preparation for the EBP Intervention Preparation for the intervention included a literature review and attendance at the ACP
certification course (September 24, 2018 - November 16, 2018) by the DNP student to obtain
ACP certification (Appendix J). The certification course included extensive teaching on phrasing
and conversational techniques, which were similar to the conversational approaches described by
Wasylynuk and Davison (2016) and Lum, Sudore, and Bekelman (2015). The DNP student
prepared for the patients' feedback through the survey questions. The survey questions were
reviewed by the director of patient education for readability and by the director of nursing
research for an expert opinion (Appendix D). Lastly, before initiating the interventions, the DNP
student presented a power point presentation about the ACP project to the patient and family
advisory committee (PFAC) at MD Anderson, which is part of the patient experience
department. The purpose of this presentation was to understand the patient and family's
perspectives on ACP and review of the survey questions (Appendices F & G).

21
EBP Intervention The literature search provided various interventions to enhance ACP discussions.
Spoelhof and Elliott (2012) advocates for face-to-face conversations, simple terminology on the
AD forms for patients, repeated conversations about the completion of ADs over time, and the
opportunity for the patient and their family to ask questions and receive assistance. Additionally,
the ACP certification improved the ACP communication skills of the DNP student. This project
intervention consisted of a face-to-face ACP discussion, and review of the AD documents with
patients.
Prior to face-to-face ACP discussions with the advanced cancer patients of the ICT
department, a folder was prepared which comprised of a letter to the patients from the ICT
department mentioning the ACP discussions with APP, blank AD documents (MPOA and a
living will document), and the survey questionnaire. The television in the clinic lobby displayed
the slogan: “Advance Care Planning: It’s all about you! Your decisions, Your plans”. Please
make your wishes known and let us help you! (Appendix K).
The assignment of DNP student to the clinic included four days when she worked with
four different physicians and selected five patients per each physician per day. The patients for
ACP discussion were selected based on the absence of a scanned AD in the Electronic Medical
Record (EMR), and willingness of the patients to participate in the ACP discussions. Following
an initial introduction, the APP (DNP student) conducted the physical exam and proceeded with
ACP discussions with the selected patients. After the ACP discussion, the DNP student reviewed
the blank AD documents with the patients. The patients had an option to complete the AD
document at the same visit, or review again and complete at the next visit. The clinic social
assisted with document completion for the patients who were interested in completing the AD

22
documents at the same visit. Two patients wished to change the resuscitation status, the
physician was informed of changing the code status in EMR to DNR and signing the Out-of-
Hospital Do Not Resuscitate (OOHDNR) form. The survey questions were reviewed and
clarified with the patients and once completed, collected by the DNP student before leaving the
patient's room.
Follow UP Follow up phone calls were made by the DNP student for a total of seven patients whom
ACP discussions were conducted but did not get the AD documents completed the same day.
These patients were encouraged to bring in their completed forms to their next appointment.
Factors that influenced the need for the telephone to follow up included those patients who were
unable to complete AD's in office due to lack of witnesses required for signing, patients who
wanted to have an additional conversation with family members, and for patients who stated that
they had a completed AD at home. Patients who had an AD at home were also encouraged to
bring the completed form to their appointment or send via email to the clinic social worker.
Similarly, for the assigned hospitalized patients, ACP discussion proceeded after
developing the relationship with patient, assessment, and discussion of the plan of care for the
admission, managing any symptoms like pain, nausea, vomiting, shortness of breath etc. Once
the patient and family verbalized readiness for the ACP discussion, the DNP student proceeded
with ACP discussions along with the review of AD documents in the ACP folder. For the
patients who were interested in AD completion, the inpatient social worker was consulted and
called. Patients who demonstrated clear understanding related to goals of care, disease status, and
personal values as reflected in willingness for a change in resuscitation status, were referred to
the inpatient physician, who placed a DNR order in EMR. Patients who were DNR, and were

23
able to be discharged from the hospital received an OOHDNR form signed by the physician and
two witnesses. The DNP student also reviewed the goals of the care survey reflecting feedback
on ACP discussions with patients, and after completion collected by DNP student.
Limitations and Barriers Evaluation of the effectiveness of the intervention in the clinic setting was limited by the
following: (a) Lack of Prioritization, for some of the stakeholders it was not a priority to assist
patients in completion of documents because of their other responsibilities, hence patients were
advised to bring completed forms at the next visit, this also include a patient who was interested
in an OOHDNR form completion same day; (b) Time limit secondary to other scheduled
appointment of patients like infusion, appointment with other specialties postponed the
completion of documents for next visit; and (c) Lack of follow up, since the DNP student was an
inpatient APP, the clinic-assigned days depend on many factors like inpatient census, presence of
all three inpatient APPs so the DNP student can go to clinic. Due to this intervention with ACP
discussions was on 4 clinic days only. The patients who received the ACP discussion were not
followed by the same APP (DNP student), and hence were lost to follow up.
Measurement Instrument and Data Collection A total of 40 patients was the targeted number for this project to obtain adequate data for
analysis. A survey developed by the DNP student, received an expert opinion from the project
chair, project mentor, as well as the patient education director. The reliability and validity of the
survey were not checked as the data from the survey was not a part of the project outcome. The
survey questions were created to reflect the feedback from the patients on the ACP discussions.
A folder was provided with a cover letter, explaining the importance of ACP and department
initiative on ACP (Appendix K). The folder included the blank AD documents (MPOA and

24
living will document), which were reviewed with the patients. The data on the AD completion
(MPOA and/or living will, DNR, OOHDNR), and ACP discussion documentation was the
desired outcome of this project; the data was collected retrospectively through the chart review.
The survey questions included a total of 18 questions: (a) six Likert scale questions: one
question to reflect patients’ goals and; four questions reflecting their understanding and
importance of an AD; one pre and post ACP discussion reflecting understanding of ACP, (b)
Five questions on demographic information, (c) six yes/no questions, and (d) one willingness to
complete an AD (Table 2). The DNP student provided the survey to the patients before starting
the discussion and collected after the completion. A total of 17 inpatients and 19 outpatient
surveys were collected (except three inpatients and one outpatient).The survey did not include
the patients' name and were separated according to the patient settings (inpatient versus
outpatient). The data collection template on the excel sheet included responses to the questions
from both settings, entered manually, without any protected health information.
The intervention included promotion of ACP through face-to-face discussions with a
review of AD with patients; this intervention was chosen based on evidence and
recommendations from the literature review (Spoelhof & Elliott, 2012; Bernacki et al., 2014;
Mack et al., 2012). The data integrity remained intact as access to EMR was password protected.
The data was collected by a senior social worker who was not a part of this study team and hence
there was no bias. Patients' willingness to ACP and AD completion could have influenced
internal validity. A threat to validity could be the patient's previous knowledge and perceptions
of ACP and AD (IOM, 2014).
Data Analysis and Statistical Analysis Procedures

25
The measurable outcome of this EBP project was to increase the ACP, AD completion
rate and/or change in code status. After 8 weeks of project implementation, the number of
completed AD improved from 20% to 40% or above for the sample population. The goal was
met for the improvement of completed AD.
Statistical Analysis. Summary statistics such as frequencies and percentages were used
to describe AD completion rates pre and post ACP intervention implementation. A Fishers’
exact test was used to compare pre and post frequencies. Summary statistics were also used to
describe the demographic characteristics and survey results by inpatient and outpatients and
compared using a Fisthers’ exact test. All statistical analysis was performed using Stata/MP
v15.0 (College Station, TX).

26
CHAPTER IV
RESULTS
After eight weeks of project initiation, the data was retrospectively collected by chart
review of the patients who had ACP discussion by the APP (DNP student). The baseline data, as
well as the post ACP intervention data was collected by a senior social worker, who was not
involved in this QI project, thereby lessening the chance of bias. The data was collected on the
patients who were noted to have no scanned AD in their EMR. This included ACP discussion
and documentation, AD completion, change in code status, Out of Hospital DNR (OOHDNR)
form. Additional data was collected on hospice enrollment of the admitted patients (pre and post
intervention) as well number of deceased patients, death during hospitalization, death post
discharge, and place of death information was also collected. Table 1a and 1b contain the
summary statistics of AD completion pre and post intervention with ACP discussions.
The findings showed a significant difference in ACP during admission 15% vs. 100% (p
< 0.001), Total AD completed 5% vs. 65% (p < 0.001), either AD or code status change 20% vs.
85% (p < 0.001), and MPOA 5% vs. 65% (p < 0.001). There was a significant difference noted
in ACP done in the outpatient setting as well 0% vs. 100% (p <0.001), total AD completed 0%
vs. 40% (p <0.001), MPOA 0% vs. 35% (p = 0.002), and OOHDNR 0% vs. 10% (0.192).
Summary statistics of the survey are located in Table 2. Inpatient and outpatients tended to
answer the survey the same (p>0.05). Demographics are located in Table 3. There was a positive
association between race and inpatient vs. outpatient status (p = 0.023). Patients in the inpatient
setting had a significant difference in total AD completion (20% vs 85%) as compared to
outpatient setting (0% vs 40%).

27
Table 2 includes results from the post survey. No significant differences were seen
between inpatient and outpatient answers. The patients’ feedback survey completion post ACP
intervention was 85% from hospitalized and 95% ambulatory patients. The survey results
revealed a positive impact of ACP discussion on patients’ understanding of ACP and AD
documents as reflected by 100% of the patients in both the settings expressing the importance of
ACP discussion. The result of post ACP discussion understanding, 82% of hospitalized, and
89% of ambulatory patients noted complete understanding while 18% hospitalized, and11%
ambulatory patients felt somewhat understanding. Patients willingness to complete the AD same
day was significant (65% hospitalized and 35 % ambulatory). The result of goals of care survey
questions were noted to be similar in both the settings, spending quality time with friends and
family was extremely important as reflected by 100% of outpatient setting patients and 82% in
the inpatient setting; 76% of the inpatients felt pain control as extremely important as compared
to 53% of outpatient setting patients. Similarly, resuscitation with CPR was extremely important
for 53% of inpatient setting patients and 47% of outpatient; breathing better was indicated as
extremely important for 41% of inpatients as compared to 26% of outpatient setting patients.
Table 1A Summary statistics of AD completion pre and post intervention (Inpatient)
Pre
(n = 20) Post
(n = 20) Complete N % N % p-value ACP During admission No 17 85% 0 0% <0.001
Yes 3 15% 20 100% Total AD Completed No 19 95% 7 35% <0.001
Yes 1 5% 13 65% Total Code Status Change No 17 85% 15 75% 0.695
Yes 3 15% 5 25% Either AD or code status change No 16 80% 3 15% <0.001 Yes 4 20% 17 85% MPOA No 19 95% 7 35% <0.001

28
Table 1B
Summary statistics of AD completion pre and post intervention (Outpatient)
Pre
(n = 20) Post
(n = 20) Complete N % N % p-value ACP done No 20 100% 0 0% <0.001
Yes 0 0% 20 100% Total AD Completed No 20 100% 12 60% <0.001
Yes 0 0% 8 40% MPOA No 20 100% 13 65% 0.002
Yes 0 0% 7 35% Living Will No 20 100% 13 65% Yes 0 100% 7 35% OOHDNR No 20 100% 18 90 0.192 Yes 0 0% 2 10%
Table 2 Summary statistics of survey by Inpatient and Outpatients
Inpatient
Outpatient
Question Level N % N % p-value
How much did you know and understand about ACP (before discussion)
None 3 18% 4 21% 0.410 Poor 3 18% 2 11% A little 7 41% 4 21% Somewhat 4 24% 6 32% Complete 0 0% 3 16%
How much did you know and understand about ACP (after discussion)
None 0 0% 0 0% 0.650 Poor 0 0% 0 0% A little 0 0% 0 0% Somewhat 3 18% 2 11% Complete 14 82% 17 89%
Spending quality time with family and friends
Not Very 0 0% 0 0% 0.095 Somewhat 2 12% 0 0%
Yes 1 5% 13 65% Living Will No 0 0% 9 45%
Yes 0 0% 11 55% DNR No 17 85% 15 75% 0.695
Yes 3 15% 5 25% OOHDNR No 19 95% 17 85% 0.605 Yes 1 5% 3 15%

29
Important 1 6% 0 0% Extremely 14 82% 19 100%
Pain Control Not Very 0 0% 1 5% 0.322 Somewhat 2 12% 2 11% Important 2 12% 6 32% Extremely 13 76% 10 53%
Breathing Better Not Very 2 12% 4 21% 0.468 Somewhat 3 18% 1 5% Important 5 29% 9 47% Extremely 7 41% 5 26%
Nutrition Not Very 5 29% 2 11% 0.267 Somewhat 3 18% 3 16% Important 2 12% 7 37% Extremely 7 41% 7 37%
CPR Not Very 3 18% 4 21% >0.999 Somewhat 0 0% 1 5% Important 5 29% 5 26% Extremely 9 53% 9 47%
Do you feel ACP discussion was important (Explain)
Yes 17 100% 19 100% >0.999
No 0 0% 0 0% When would you like to complete AD documents
Today 11 65% 7 35% 0.015 This admission 3 18% 0 0% Next visit 3 18% 12 65% Not yet 0 0% 0 0%
Table 3 Summary statistics of demographic characteristics Inpatient Outpatient Characteristic Level N % N % p-value Gender Male 3 15% 8 40% Female 17 85% 12 60% Age Greatest Generation 1 6% 2 11% >0.999
Baby Boomers 10 59% 11 58% Generation X 6 35% 6 32% Millennial 0 0% 0 0%
Race Black 7 41% 1 5% 0.024 White 9 53% 16 84% Asian 1 6% 1 5% Other 0 0% 1 5%
Ethnicity Hispanic 1 6% 1 5% >0.999 Non-Hispanic 16 94% 18 95%
Time since diagnosis Less than 1 year 2 12% 5 26% 0.162

30
1-2 years 6 35% 3 16% 3-5 years 3 18% 7 37% 6-10 years 3 18% 4 21% greater than 10 years 3 18% 0 0%
Do you have AD Yes 2 12% 4 21% 0.662 No 15 88% 15 79%

31
CHAPTER V
DISCUSSION AND RECOMMENDATION
The results of this project reveal success as demonstrated by achievement of the expected
outcomes and an additional outcome.
Interpretation, Expected and Actual Outcomes
The expected outcomes included an increase in ACP discussions and AD completion
with a change in code status of patients (admitted and ambulatory) seen in the ICT department.
The results demonstrate that ACP discussions by the APP were associated with an increased AD
completion and also a change in the code status of the advanced cancer patients, as shown in
Table 1A, 1B. There was a significant difference in ACP during admission 15% vs. 100% (p <
0.001), Total AD completed 5% vs. 65% (p < 0.001), either AD or code status change 20% vs.
85% (p < 0.001), and MPOA 5% vs. 65% (p < 0.001). There was a difference noted in outpatient
setting as well in ACP 0% vs 100% (p <0.001), Total AD completed 0% vs 40% (p <0.001), and
OOHDNR 0% vs 10% (0.192). The additional positive outcome was an increase in hospice
enrollment of admitted patients (15% (3/20) vs. 40% (8/20). Total deceased patients 40% (8/20)
vs. 20% (4/20). While only 12.5% (1/8) patient died in an inpatient hospice pre intervention, post
intervention it was noted that 50% (2/4) patients died at home in the home hospice and the other
2/4 (50%) died during hospitalization (one patient was DNR and died at MD Anderson, while
other died due to extensive Myocardial Infarction at another acute care hospital). This fact likely
reflect the wishes of the patients post ACP discussion.
Limitations During the project intervention, it was essential to encourage the patients to review the
AD documents and complete the AD documents same day or same admission. In the inpatient

32
setting, it was possible to follow up on the patient during the hospitalization, however in the
outpatient setting, it was less likely to follow up on intervention patient on AD documents
completion as the APP (DNP student) was an inpatient APP and clinic assignment dependent on
various variables addressed before. Although a total of seven patients were interested in
completing the AD same day, only four of them could complete due to the factors discussed in
limitation and barriers. This lack of AD completion also included one patient who wished to
complete and OOHDNR which did not occur as it was not a priority for some of the
stakeholders. There were seven follow up phone calls made; however, only three patients could
provide the completed AD post follow up call, the reason is lost to follow up as the APP (DNP
student) was not in the clinic on the day of patient’s follow up. Hence in the clinic setting, it
might have been feasible to measure implementation of ACP post-intervention follow up of the
patients by the clinic team. Practice recommendation include increasing awareness among the
stakeholders of the ACP and AD completion.
Recommendations, Intervention Revision and Plans to Maintain Effects Recommendations from the results of this project includes improving the ACP
discussions in the ICT department as well as in the institution. ACP discussions are essential for
patients as reflected by the project outcomes. The DNP student is actively involved with
department leadership in making strategic plans to incorporate the ACP discussions into daily
practice. Some of the plans include educating and encouraging the participation of ICT staff
(nurses, medical assistants, study coordinator, social workers) in assisting patients to discuss
ACP with APP and physicians. There is a plan to include systems alert through EMR to notify on
AD completion, this will show an alert/reminder for ACP until an AD is scanned in EMR.
Finally, the plan is to schedule an additional visit for patients without a scanned AD for an ACP

33
discussion at their regular follow up appointment with an APP. The CMS encourages providers
for ACP discussion by reimbursing for the total face-to-face time spent on these discussions. The
revenue generated from the ACP discussions might result in hiring additional APPs for the
department. Intervention review includes adding the ACP video which can be watched by the
patients in the waiting area of clinic and for the admitted patients.
Cost Benefit Analysis and Cost Avoidance Analysis As of January 1, 2016, Medicare provides reimbursement for ACP, which may be billed
as a distinct service, and completion of AD is not a criteria for reimbursement (CMS, 2016).
According to CMS, 2016, ACP must be conducted face-to-face by a provider with the patient or
proxy decision-maker. Reimbursement for ACP with Medicare patients is $86 for the initial 30
minutes during a visit and $75 for each subsequent 30-minute period of time. An APP who bills
incident to a physician for one 30-minute ACP encounter can reimburse for $86. According to
Khandelwal et al. (2016), for patients with severe lung disease, avoidance of a single intensive
care unit (ICU) admission for an average duration could save $38,000 in hospital costs. A
reduction in length of stay by 1.7 days in an intensive care unit as the result of a palliative care
consultation was calculated to save $6,100 in costs of care (Khandelwal et al., 2016).

34
Calculation of cost benefit and cost avoidance analysis of this project. It is essential
to understand that the goal of this QI project was not to reduce cost of care or increase revenue.
The global aim was to increase the awareness among the APPs and physicians on the importance
of initiating the ACP and EOL discussions for all advanced cancer patients who were referred to
the department. The project aimed to enhance shared decision making, ensure care in line with
patients’ wishes, strengthen patient autonomy, encourage for a change in the code status of the
patients when they get admitted to the hospital. There were additional benefits noted with ACP
discussions as reflected by a gain of $1,491 through reimbursement, and probable health care
savings of $48,000 as a total of 8 patients opted for hospice enrolment and hence avoided
hospital/ICU admission (Appendix N).
Conclusions Advance Care Planning can allow patients to make more personalized decisions
regarding their AD, and they can increase the number of patients taken care of outside of a
hospital or intensive care unit (Johnson et al., 2016). The results of this project show that
additional help and support are needed for the patients and family to make wise decisions when it
comes to ACP/EOL decisions. There is a need for ACP discussions with advanced cancer
patients. The patient’s feedback survey showed that 100% of the patients acknowledged the
importance of ACP discussions. Every patient who had the ACP discussions replied that they
strongly agree on the importance of having an AD. ACP discussion requires subsequently
revisiting based on any change in clinical status of the patient and /or a change of the MPOA.
It was noted that patients undergoing complex situations related to the metastatic disease
would not like to listen to the ACP until they were made comfortable with symptom
management. ACP was not given importance by patients and family who discovered bad news or

35
new metastasis of their cancer. Overall impact of this project for patients was positive as
reflected in the patients’ feedback survey. According to Bernacki and Block (2014), ACP is
about conversations with patients and their family, and shared decision-making to ensure a care
plan is in place that outlines clearly the patient’s health-care wishes and end-of-life care
preferences should they be unable to direct their own care. ACP conversations, when done early
and throughout the patient’s illness, not only improve end-of-life outcomes, but also help
patients adjust to their ill-ness, hence ACP is seen as a critical component of patient-centered
care.
The ACP discussions were successful and enhanced patients’ understanding of their
values and goals of care. Additionally, these discussions helped the patients in completion of the
AD documents, a change in the code status to DNR, and acceptance to the palliative care with
hospice services. In summation, the project was able to show that ACP discussions initiated by
APP can enhance patient - centered EOL care. It would be appropriate to continue the ACP
discussions with patients with advanced cancer.

36
REFERENCES
Aldridge, M.D., & Kelly, A.S. (2015). Epidemiology of serious illness and high utilization of
Health care. Dying in America: Improving quality and honoring individual preferences.
Near the end of life (pp. 487-532). Doi: 10. 17226/18748
American Cancer Society. Cancer Facts and Figures 2018. Retrieved from https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and- statistics/annual-cancer-facts-and-figures/2018/cancer-facts-and-figures-2018.pdf American Cancer Society. Cancer basics: The economic impact of cancer. Retrieved from https://www.cancer.org/cancer/cancer-basics/economic-impact-of-cancer.html American Nurses Association. (2015). Code of ethics with interpretive statements. Silver Spring, MD: ANA. ASCO Institute for Quality: QCDR measures. Retrieved from
http://www.instituteforquality. org/sites/instituteforquality.org/files/QOPI 2015 QCDR
Measures - Narrative_0.pdf
Bernacki, R. E., Block, S. D., & American College of Physicians High-Value Care Task Force.
(2014). Communication about serious illness care goals: A review and synthesis of best
practices. JAMA Internal Medicine, 174(12), 1994-2003.
doi:10.1001/jamainternmed.2014.5271
Bestvina, C. M., & Polite, B. N. (2017). Implementation of Advance Care Planning in Oncology: A Review of literature. Journal of Oncology Practice, 13(10), 657-662. doi:10.1200/JOP. 2017.021246 Butler, M., Ratner, E., Mccreedy, E., Shippee, N., & Kane, R. L. (2014). Decision aids
for advance care planning: An overview of the state of the science. Annals of

37
Internal Medicine, 161(6), 408. Doi: 10.7326/m14-0644 Billings, J.A., & Bernacki, R. (2014). Strategic targeting of Advance Care Planning Interventions: The Goldilocks phenomenon. JAMA Internal Medicine, 174(4), 620-624. doi: 10.10001/jamainternmed.2013.14384 Brinkman-Stoppelenburg, A., Rietjens, J. AC., & Heide, A. VD. (2014). The effects of advance
care planning on end-of-life care: A systematic review. Palliative Medicine, 28(8), 1000-
1025. doi: 10.1177/026921631452672
Carr, D., & Luth, E. (2016). End of life planning and health care. Handbook of aging and social sciences. (pp 375-394, 8th ed). L.K. George & K. Ferraro (Eds.). New York: Academic Press. doi: 10.1016/B978-012-417235-7.00018-4 Centers for Medicare & Medicaid Services. (2015) Federal Register, 80 (220),70943. Retrieved from https://www.gpo.gov/fdsys/pkg/FR-2015-11-16/pdf/2015-28005.pdf Centers for Medicare and Medicaid Services, (2018). Physician fee for schedule search. Retrieved from https://www.cms.gov/apps/physician-fee-schedule/search/search-criteria.aspx Chander, M., Brockstein, B., Zunamon, A., Silverman, I., Dlouhy, S., Ashlevitz,
K.,…Obe, J. (2017). American Journal of Hospice & Palliative Medicine, 34(5), 423- 429. doi:10.1177/1049909116636614
Chiarchiaro, J., Buddadhumaruk, P., Arnold, R. M., & White, D. B. (2015). Prior advance care
planning is associated with less decisional conflict among surrogates for critically ill
patients. Annals of the American Thoracic Society, 12(10), 1528.
Chung, H.O., Oczkowski, S. J. W., Hanvey, L., Mbuagbaw, L., & Yu, J. J. (2016). Educational

38
interventions to train healthcare professionals in end-of-life communication: A systematic
review and meta-analysis. BMC Medical Education, 16(130), 1-13.
Dube, M., McCarron, A., & Nannini, A. (2015). Advance care planning complexities for nurse
practitioners. The Journal for Nurse Practitioners,11(8), 766-773.
Eldridge, C. R. (2017). Nursing science and theory: scientific underpinnings for practice. In M.
E. Zaccagnini & K. W. White (Eds.), The doctor of nursing practice essentials: a new
model for advanced practice learning, (3rd ed.) (pp. 3-38). Burlington, MA: Jones &
Bartlett Learning.
Epstein, A. S., Shuk, E., O’Reilly, E. M., Gary, K. A., & Volandes (2015). ‘We have to discuss
it’: cancer patients’ advance care planning impressions following educational information
About cardiopulmonary resuscitation. Psycho-Oncology, 24(12), 1767-1773. doi:
10.1002/pon.4786
Financial Burden of Cancer Care. Retrieved from
https://progressreport.cancer.gov/after/economic_burden
Granek, L., Krzyzanowska, M.K., Tozer, R., & Mazzotta, P. (2013). Oncologists’ strategies and
barriers to effective communication about end of life. Journal of Oncology Practice, 9(4),
e129-1e35. Doi: 10.1200/JOP.2012.000800
Hughes, R., & United States Agency for Healthcare Research and Quality. (2008). Patient safety
and quality: An evidence-based handbook for nurses. Rockville, MD: Agency for
Healthcare Research and Quality, U.S. Dept. of Health and Human Services. Retrieved from
http://purl.access.gpo.gov/GPO/LPS93676; http://www.ahrq.gov/qual/nurseshdbk/
Houben, C.H.M., Spruit, M. A., Groenen, M.T.J., Wouters, E.F.M., & Janseen, D.J.A. (2014). Efficacy of Advance Care Planning: A systemic review and meta-analysis. Journal of the

39
American Medical Directors Association, 15(7), 477-489. Doi: 10.1016/j.jamda.2014.01.008 Hoverman, J. R., Taniguchi, C., Eagye, K., Mikan, S., Kalisak, A., Ash-Lee, S., & Henchel, R. (2017). If we don’t ask, our patients might never tell: The impact of routine use of a patient values assessment. Journal of Oncology Practice, 13(10), e831- e837. Doi: 10.1200/jop.2017.022020 Institute of Medicine (IOM). (2014). Dying in America: Improving quality and honoring Individual preferences near the end of life. Washington, DC: The National Academies. Johnson, S., Clayton, J., Butow, P.N., Silvester, W., Detering, K., Hall, J., ...Tattersall, M.H.N.
(2016). Advance care planning in patients with incurable cancer: study protocol for a
randomized controlled trial. BMJ Open, 6(12), 1-11. doi: 10.1136/bmjopen-2016- 012387
Johnson, C. E., Chong, J.C., Wilkinson, A., Hayes, B., Tait, S., & Waldron, N. (2017). Goals of patient care system changes with video-based education increases rates of advance cardiopulmonary resuscitation decision- making and discussions in hospitalized rehabilitation patients. Internal Medicine Journal, 47 (7), 798-806. Doi:10.1111/imj.13454
Kermel-Schiffman, I., & Werner, P. (2017). Knowledge regarding advance care planning: a
systematic review. Archives of Gerontology and Geriatrics, 73, 133-142. Doi:
10.1016/j.archger.2017.07.012
Khan, S. A., Gomes, B., & Higginson. (2014). End-of-life care-What do cancer patients want?
Nature Reviews Clinical Oncology, 11(2), 100-108. doi: 10.1038/nrclinonc.2013.217
Khandelwal, N., Benkeser, D., Coe, N. B., Engelberg, R. A., Curtis, J. R., & Teno, J. M. (2016).
Patterns of cost for patients dying in the intensive care unit and implications for cost

40
savings of palliative care interventions. Journal of Palliative Medicine, 19(11), 1171-
1178. doi:10.1089/jpm.2016.0133
Klingler, C., Schmitten, J. I., & Marckmann, G. (2015). Does facilitated advance care planning
reduces the costs of care near the end of life? Systematic review and ethical
considerations. Palliative Medicine. Doi: 10.1177/0269216315601346
Luckett, T., Sellars, M., Tieman, J., Pollock, C. A., Silvester, W., Butow, P. N.,…Clayton, J. M.
(2014). Advance Care Planning for adults with CKD: A Systematic Integrative Review.
American Journal of Kidney Disease, 63(5), 761-770. Doi:10.1053/j.ajkd.2013.12.007
Lum, H.D., Sudore, R. L., & Bekelman, D. B. (2015). Advance care planning in the elderly.
Medical Clinics of North America, 99(2), 391-403. Doi: 10.1016/j.mcna.2014.11.010
Mack, J. W., Cronin, A., Taback, N., Huskamp, H. A., Keating, N. L., Malin, J. L.. . Weeks, J.
C. (2012). End-of-life care discussions among patients with advanced cancer: A cohort
study. Annals of Internal Medicine, 156(3), 204.
McCusker, M., Ceronsky, L., Crone, C., Epstein, H., Greene, B., Halvorson, J., Kephart, K.,
Mallen, E., Nosan, B., Rohr, M., Rosenberg, E., Ruff, R., Schlecht, K., & Setterlund, L.
(2013). Palliative care for adults. Bloomington, MN: Institute for Clinical Systems
Improvement (ICSI). Retrieved from Agency for Healthcare Research and Quality
National Guideline Clearinghouse https://www.icsi.org/_asset/k056ab/PalliativeCare.pdf
Menon, S., Mccullough, L.B., Beyth, R. J., Ford, M.E., Espadas, D., & Braun, U. K. (2016). Use
of a values inventory as a discussion aid about end-of-life care: A pilot randomized
controlled trial. Palliative and Supportive Care, 14, 330-340.
Doi:10.1017/S1478951515001091
41
Michael, N., O’Callaghan, C., Baird, A., Gough, K., Krishnasamy, M., Hiscock, N., & Clayton,
J. (2015). A mixed method feasibility study of a patient-and-family-centered advance
care Planning intervention for cancer patients. BMC Palliative Care, 14(27), 1-12. Doi:
10.1186/s12904-015-0023-1
Michael, N., O’Callaghan, C., & Clayton, J. M. (2016). Exploring the effect of utilizing the
vignette technique in promoting advance care planning discussions with cancer patients
and caregivers. Patient Education and Counseling, 99(8), 1406-1412. Doi:
10.1016/j.pec.2016.03.021
Nedjat-Haiem, F. R., Carrion, I. V., Gonzales, K., EII, K., Thompson, B., & Mishra, S. I.
(2017), Exploring health care providers’ views about initiating End-of-Life care
communication. American Journal of Hospice & Palliative Medicine, 34(4), 308-317.
Doi:10.1177/1049909115627773
Obel, J., Brockstein, B., Marschke, M., Robicsek, A., Konchak, C., Sefa, M.,…Hensing, T.
(2014). Outpatient Advance Care Planning for metastatic cancer: A pilot quality
improvement initiative. Journal of Palliative Medicine, 17(11),1231-1237.
Doi:10.1089/jpm.2014.0085
Odejide, O. O., Cronin, A. M., Condron, N., Earle, C. C., Wolfe, J., & Abel, G. A. (2016).
Timeliness of end-of-life discussions for blood cancers: A national survey of
hematologic oncologists. JAMA, 176(2), 263. Doi:10.1001/jamainternmed.2015.6599
O'Hare, A. M., Szarka, J., McFarland, L. V., Taylor, J. S., Sudore, R. L., Trivedi, R.,... Vig, E.
K. (2016). Provider perspectives on advance care planning for patients with kidney
disease: Whose job is it anyway? Clinical Journal of the American Society of
Nephrology, 11(5), 855-866. doi:10.2215/CJN.11351015

42
Plan-Do-Study-Act (PDSA). (2008) Retrieved from
https://innovations.ahrq.gov/qualitytools/plan-do-study-act-pdsa-cycle
Pollock, K., & Wilson, E. (2015). Care and communication between health professional and
patients affected by severe or chronic illness in community care settings: a qualitative
study of care at the end of life. Health Service and Delivery Research, 3(31),
doi:10.3310/hsdr03310
Roy C. The Roy adaptation model. 3 edition. Upper Saddle River New Jersey: Pearson
Education; 2009.
Russwurm, M.A., & Larrabee, J. H. (2007). A Model for change to Evidence-Based
Practice. Journal of Nursing Scholarship, 31(4), 317-322. Doi: 10.1111/j.1547-5069.
1999.tb00510.x
Schrijvers, D., Cherny, N. I., & ESMO Guidelines Working Group. (2014). ESMO clinical
practice guidelines on palliative care: Advanced care planning. Annals of Oncology:
25(Suppl 3), iii138-iii142. Doi:10.1093/annonc/mdu241
Sonenberg, A., & Sepulveda-Pacsi, A.L. (2018). Medicare Payment: Advanced Care Planning.
The Journal for Nurse Practitioners, 14(2), 112-116. Doi: 10.1016/j.nurpra.2017.11.23
Spoelhof, G. D., & Elliott, B. (2012). Implementing advance directives in office practice. American Family Physician, 85(5), 461-466. Stein, R. A., Sharpe, L, Bell, M. L., Boyle, F.M., Dunn, S. M., &Clarke, S. J. (2013).
Randomized Controlled Trial of a structured intervention to facilitate End-Of-Life
decision making in patients with advanced cancer. Journal of Clinical Oncology, 31(27),
3403- 3410. Doi: 10.1200/JCO.2011.40.8872

43
Stevens, K. R. (2013). The impact of evidence-based practice in nursing and the next big ideas.
Online Journal of Issues in Nursing, 18(2), 4. doi: Vol-18-2013/No2-May-2013/Impact-of-
Evidence-Based-Practice. html [pii]
Sudore, R. L., Boscardin, J., Feuz, M. A., McMahan, R.D., Katen, M.T., & Barnes, D. E. (2017). Effect of the PREPARE website vs. an easy-to-read advance directive on advance care Planning documentation and engagement among veterans. A randomized control trial. JAMA internal medicine, 177(8), 1102-1109. Doi: 10.1001/jamainternmed.2017.1607 Uhler, L. M., Fifueroa, R. E. P., Dickson, M., McCullah, L., Kushniruk, A., Monkman,
H.,…Hajizadeh, N. (2015). Informed together: Usability evaluation of a Web-Based decision aid to facilitate shared advance care planning for severe chronic obstructive pulmonary disease. JMIR Human Factors, 2(11), e2-.
doi: 10.2196/humanfactors.3842 Ursavaş FE, Karayurt Ö, İşeri Ö. (2014). Nursing Approach Based on Roy Adaptation Model in a patient undergoing Breast Conserving Surgery for Breast Cancer. J Breast Health. 10(3),134-140. doi:10.5152/tjbh.2014.1910 Volandes, A. E., Paasche-Orlow, M. K., Mitchell, S. L., El-Jawahri, A., Davis, A. D., Barry, M.
J.,…Temel, J. S. (2013). Randomized Controlled Trial of a video decision support tool
for cardiopulmonary resuscitation decision making in advanced cancer. Journal of
Clinical Oncology, 31(3), 380-386. Doi: 10.1200/JCO.2012.43.9570
Wasylynuk, B. & Davison, S. N. (2016). Advance care planning in advanced chronic kidney
disease: Practical communication tips for clinicians. The Canadian Association of
Nephrology Nurses and Technologists Journal, 26(3), 20-25.
Walczak, A., Butow, P. N., Tattersall, M.H.N., Davidson, P.M., Young, J., Epstein, M.

44
R.,…Clayton, J.M. (2017). Encouraging early discussion of life expectancy and end- of-
life care: A randomized controlled trial of a nurse-led communication support program
for patients and caregivers. International Journal of Nursing Studies, 67, 31-40. Doi:
10.1016/j.ijnurstu.2016.10.008
White, K. M. & Dudley-Brown, S. & Terhaar, M. F. (2016). Translation of evidence into nursing
and health care practice. New York: Springer Publishing Company
Zhou, G., Stoltzfus, J. C., Houldin, A. D., Parks, S. M., & Swan, B. A. (2010). Knowledge,
attitudes, and practice behaviors of oncology advanced practice nurses regarding advance
care planning for patients with cancer. Oncology Nursing Forum, 37(6), e400-e410.

45
APPENDIX A HIERACHY OF EVIDENCE

46
APPENDIX B SYNTHESIS OF LITERATURE Theme Author (s) Title and
Publisher
Aim/purpose of the study Study Design and Level of Evidence
Setting and Study Participants
Results/Findings
Benefits of ACP
Increase Patient autonomy
Klinger, Schmitten, & Marckmann
2015 Does facilitated advance care planning reduces the costs of care near the end of life? Systematic review and ethical considerations. Palliative Medicine.
To describe the cost of implications of Advance Care Planning programs and discusses ethical conflicts arising in this context.
A systematic review based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.
Level I
A Total of 7 studies were used for this Systematic Review. Four- RCT, One - before-after design Two -observational studies
The Findings suggest that Advance Care Planning has the potential to strengthen patient autonomy and to improve quality of care at or near the end of life and besides has implication on reductions in costs of care which ranges from USD1041 to USD64,827 per patient
Decrease Family
Chiarchiaro, J., Buddadhumaruk,
2015 Prior advance care planning is associated with
To Examine if ACP results in less surrogate decisional conflict for
A total of 471 Surrogates of 257 patients with
Findings suggest prior ACP discussions

47
/surrogate decision burden
P., Arnold, R. M., & White, D. B.
less decisional conflict among surrogates for critically ill patients.
Annals of the American Thoracic Society
critically ill patient families
Prospective Cohort study
Level IV
ARDS at five US Academy Medical Canter completed questionnaires regarding any prior ACP conversations with their loved ones
reduces the decision conflict of the surrogates of critically ill patients
Improved quality of care near end of life
Bestvina, C.M., & Polite, B.N.
2017 Implementation of Advance Care Planning in Oncology: A Review of the Literature. Journal of Oncology Practice
To evaluate and summarize the interventions to increase ACP in the oncology setting, knowledge of healthcare providers and training in ACP conversations Systematic Review Level I
A total of 26 prospective interventions, including one secondary analysis of ACP in outpatient oncology clinics, were included in this review.
Several components of a successful implementation of ACP. -Patients with an oncologic diagnosis should receive ACP early in their disease course, and this should be readdressed often. -Educational tools to prepare patients for ACP discussions include - pamphlet or a guidebook - use of video decision aids
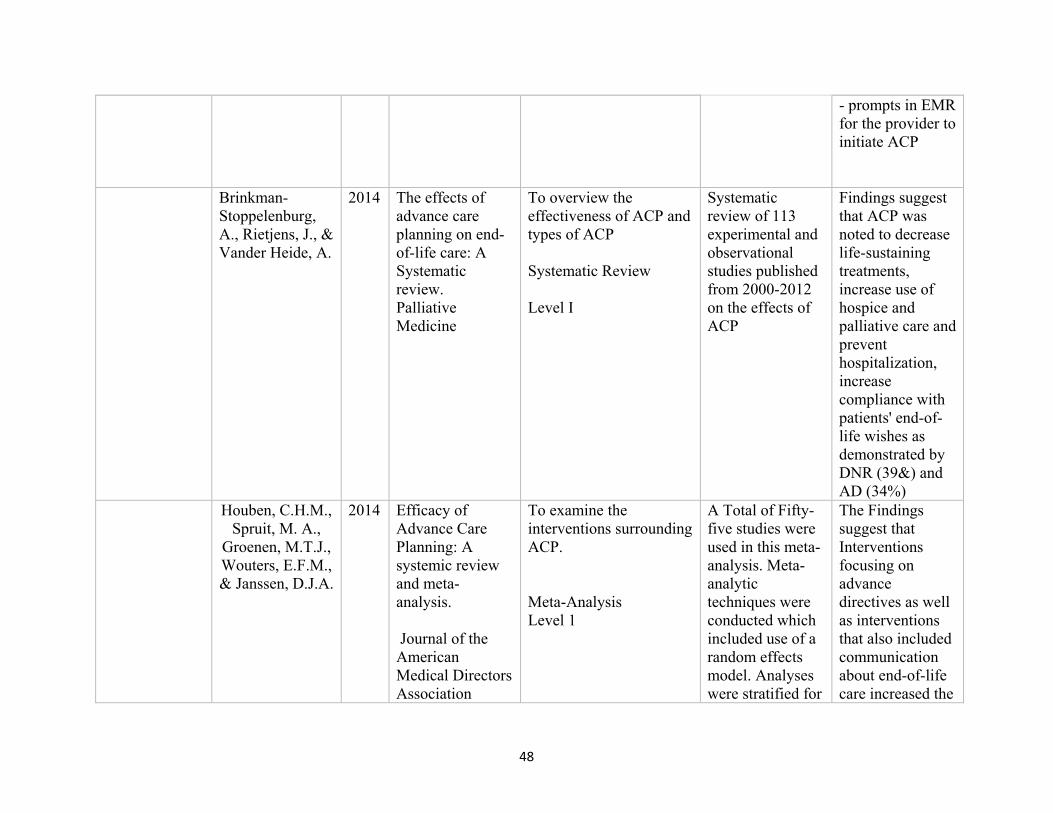
48
- prompts in EMR for the provider to initiate ACP
Brinkman-Stoppelenburg, A., Rietjens, J., & Vander Heide, A.
2014 The effects of advance care planning on end-of-life care: A Systematic review. Palliative Medicine
To overview the effectiveness of ACP and types of ACP Systematic Review Level I
Systematic review of 113 experimental and observational studies published from 2000-2012 on the effects of ACP
Findings suggest that ACP was noted to decrease life-sustaining treatments, increase use of hospice and palliative care and prevent hospitalization, increase compliance with patients' end-of-life wishes as demonstrated by DNR (39&) and AD (34%)
Houben, C.H.M., Spruit, M. A.,
Groenen, M.T.J., Wouters, E.F.M., & Janssen, D.J.A.
2014 Efficacy of Advance Care Planning: A systemic review and meta-analysis. Journal of the American Medical Directors Association
To examine the interventions surrounding ACP. Meta-Analysis Level 1
A Total of Fifty-five studies were used in this meta-analysis. Meta-analytic techniques were conducted which included use of a random effects model. Analyses were stratified for
The Findings suggest that Interventions focusing on advance directives as well as interventions that also included communication about end-of-life care increased the

49
type of intervention: advance directives and communication
completion of advance directives and the occurrence of end-of-life care discussions between patients and healthcare professionals.
Klinger, Schmitten, & Marckmann
2015 Does facilitated advance care planning reduces the costs of care near the end of life? Systematic review and ethical considerations. Palliative Medicine.
To describe the cost related to implications of Advance Care Planning programs and to discuss ethical conflicts arising in this context. A systematic review was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. Level I
A Total of 7 studies were used for this Systematic Review Four- RCT, One - before-after design Two -observational studies
The Findings suggest that Advance Care Planning has the potential to strengthen patient autonomy and improve quality of care at end of life, and besides has implication on reductions in costs of care which ranged from $ 1041 to USD64,827 per patient
Place of death based on patient’s choice
Khan, S. A., Gomes, B., &
Higginson.
2014 End-of-life Care-What do cancer patients want? Nature Reviews Clinical Oncology
To discuss the preferences of patients with cancer regarding their end of life care, including the importance of the early provision of palliative care, and the
Various Factors that contribute to the place of death, including environmental factors, disease-specific issues,
Findings from the study suggest that ACP provides an opportunity to verbalize the preferences of dying at home,

50
central role of advance care planning in meeting patients' preferences. A Qualitative Study Level VI
and the availability of resources were discussed with the cancer patients
which increases the likelihood of it happening. It allows health care professional and care providers to make arrangements, so people nearing the end of life can spend more time at home in a home hospice rather than the hospital.
Barriers to ACP
Lack of Time Chander, M., Brockstein, B., Zunamon, A., Silverman, I., Dlouhy, S., Ashlevitz,
K.,...Obel, J.
2017 Perspectives of health-care providers toward advance care planning in patients with advanced cancer and congestive heart failure.
American Journal of Hospice & Palliative Medicine
A quality improvement initiative to clarify attitudes of oncologists, cardiologists, and primary care physicians (PCPs) toward ACP and to identify persistent barriers related to ACP discussion A Qualitative Study Level VI
A 20-question included in a cross-sectional online survey to cardiologists, oncologists, PCPs, and cardiology and oncology support staff at the North Shore University Health System (North Shore) from February to March 2015. A total of 117
Findings from this study suggest that attitudes towards ACP vary among medical specialty and medical conditions as compared to Oncologists and Primary Care Providers. Implying that there is a great need for collaboration

51
individuals (46% of distributed) completed the surveys.
between office-based PCPs and specialists in both the inpatient and the ambulatory settings.
Zhou, G., Stoltzfus, J. C., Houldin, A. D., Parks, S. M., & Swan, B. A.
2010 Knowledge, attitudes, and practice behaviors of oncology advanced practice nurses regarding advance care planning for patients with cancer.
Oncology Nursing Forum
A Web-based survey was obtained to evaluate preliminary understanding of APNs' knowledge, attitudes, and practice behaviors and perceived barriers to advanced care planning. This survey was mainly focused on oncology advanced practice nurses' (APNs') knowledge, attitudes, and to understand their practice behaviors regarding advanced care planning. A Qualitative Study Level VI
The survey was distributed to 300 APN of the Eastern U.S. The survey was sent via e-mail which was resend to 89 APNs who responded to the initial survey.
The attitudinal and practice behaviors portion of the survey demonstrated that respondents were moderately knowledgeable, but their advanced care planning practice was not routine. Lack of time was one of the reason
Discomfort Granek, L., Krzyanowska,
2013 Oncologists’ strategies and barriers to
To evaluate barriers of ACP and EOL conversations and to
Interviews of twenty oncologists from
Findings suggest that a multipronged

52
(patient, family, and provider)
M.K., Tozer, R., & Mazzotta, P.
effective communication about end of life. Journal of Oncology Practice
assess the best approach to resolve the obstacles to ACP and EOL conversations A Qualitative study Level VI
three Oncology Centers in Canada
approach which provides support for the providers, patient education, and Institutional support is necessary to remove barriers for ACP and EOL conversations
Institute of Medicine (IOM)
2014 Dying in America: Improving Quality and Honoring individual preferences near the end of life. The National Academic Press Report on current state, studies, and improvements to ACP
Systematic Review of over 1500 studies Level 1
It was a review by a committee of 21 members to review ACO and Evidence-Based Practice
This review resulted in education and development for ACP
Odejide, O.O., Cronin, A.M., Condron, N., Earle, C.C., Wolfe, J., & Abel, G.A..
2015 Timeline of End-of-Life Discussions for Blood Cancers. JAMA
To evaluate the timing of ACP discussion with patients with blood cancer.
Postal Survey send to US hematologists ( total of 349 participants)
Suggest that there is a need for provider intervention to improve the timing of ACP

53
Quantitative non-intervention/experimental qualitative study Level IV
Zhou, G., Stoltzfus, J. C., Houldin, A. D., Parks, S. M., & Swan, B. A.
2010 Knowledge, attitudes, and practice behaviors of oncology advanced practice nurses regarding advance care planning for patients with cancer.
Oncology Nursing Forum
A Qualitative Study Level VI
The survey was distributed to 300 APN of the Eastern U.S. The survey was sent via e-mail and was resend to the 89 APNs who responded to the initial study.
The attitudinal and practice behaviors portion of the survey demonstrated that respondents were moderately knowledgeable, but their advanced care planning practice was noted to be deficient in daily practice
Lack of Experience, Understanding, and Collaboration
Nedjat-Haiem, F. R., Carrion, I. V.,
Gonzales, K., EII, K.,
Thompson, B., & Mishra, S. I.
2017
Exploring health care providers’ views about initiating End-of-Life care communication.
To explore the perspectives of physicians, nurses, social workers, and chaplains on engaging seriously ill patients and families in
Qualitative data were collected from 79 (medical and nonmedical) providers practicing at 2
Findings suggest that ACP Discussions should be started early -Physicians to lead the

54
American Journal of Hospice & Palliative Medicine
EOL care communication. A Qualitative Study Level VI
medical centers in Central Los Angeles.
discussions specifically due to their medical training and need to clarify medical information regarding patients' prognosis. -An interdisciplinary approach with nurses, social workers, and chaplains could significantly improve patient care.
O'Hare, A. M., Szarka, J., McFarland, L. V., Taylor, J. S., Sudore, R. L., Trivedi, R., ... Vig, E. K.
2016 Provider perspectives on advance care planning for patients with kidney disease: Whose job is it anyway?
Clinical Journal of the American Society of Nephrology
to evaluate the perspectives related to advance care planning of multidisciplinary providers caring for patients with advanced kidney disease. A Qualitative Study Level VI
Semi-structured interviews conducted on 26 providers from multispecialty at VA Puget Sound Health Care System between April-December 2014. The participants interviewed on their perspectives and experience related to ACP
The study reports various barriers to ACP -lack of shared understanding -lack of active collaboration &communication among providers caring for the same patient regarding the ACP -Complex medical care of the patients

55
Timing of ACP
Need for earlier ACP Conversations
Epstein, A. S., Shuk, E.,
O’Reilly, E. M., Gary, K. A., &
Volandes
2015 ‘We have to discuss it’: cancer patients’ advance care planning impressions following educational information about cardiopulmonary resuscitation. Psycho-Oncology
To evaluate the effectiveness of the educational method on advance care planning and to understand the gap in knowledge Randomized Trial Level II
A total of 54 study participants were Randomized to either the Video Arm or the Narrative arm of the Intervention.
The Findings suggest that Patients with advanced cancer noted to be apprehensive about ACP but wanted to discuss ACP. 26 total (41% of V arm, 56% of N arm) articulated questions. There were seven themes resulted from the questions.

56
Pollock & Wilson
2015 Care and communication between health professional and patients affected by severe or chronic illness in community care settings: a qualitative study of care at the end of life. Health Service and Delivery Research
To investigate how patients, their relatives, and health care professionals engage in the initiation of ACP discussions and relate the outcomes of advance care planning discussions in shaping care at the end of life. Qualitative Study Level VI
Qualitative study with two work streams: (1) interviews with 37 health professionals (general practitioners, specialist nurses and community nurses) about their experiences on ACP (2) longitudinal case studies of 21 patients who had a 6-month follow-up.
The study found ACP to be absent and providers were noted to be focused primarily on specific documented tasks involving decisions about patients' preferred place of death and cardiopulmonary resuscitation. There was no evidence of ACP among (9 of 21) patient cases. Professionals reported ACP discussions to be challenging.
Odejide, O.O., Cronin, A.M., Condron, N., Earle, C.C., Wolfe, J., & Abel, G.A.
2015 Timeline of End-of-Life Discussions for Blood Cancers. JAMA
To evaluate the timing of ACP discussion with patients with blood cancer Quantitative non-intervention/experimental qualitative study Level IV
Postal Survey send to US hematologists (total of 349 participants
The findings from this study suggested a need for provider intervention to improve the timing of ACP

57
Mack, J. W., Cronin, A., Taback, N., Huskamp, H.A., Keating, N.L., Malin, J. L.,….Weeks, J.C.
2012 End-of-life care discussions among patients with advanced cancer: A cohort study. Annals of Medicine
To evaluate the effect of ACP discussions with patients with lung or colon cancer based on Evidence-Based Practice Group recommendations. Prospective cohort study Level IV
Review of documentation of ACP discussions within 15 months in EMR on 2155 patients cared at HMO or the VA of California/North Carolina/Iowa/ or Alabama
Findings show that 73% of the patients had ACP discussions. On patients who died-87% had ACP versus 41 % of Alive patients. Study findings report only 27% of 55% ACP were documented and of those patients who died the ACP occurred 33 days before death
Routine and regular ACP discussions
Bestvina & Polite 2017
Implementation of Advance Care Planning in Oncology: A Review of the Literature. Journal of Oncology Practice
To evaluate and summarize the interventions to increase ACP in the oncology setting, knowledge of healthcare providers and training in ACP conversations Systematic Review Level I
A total of 26 prospective interventions were included in this review along with a secondary analysis of ACP in outpatient oncology clinics.
Several components of a successful implementation of ACP were noted. - Oncology patients should receive ACP early in their disease course, and this should be readdressed at various visits. -Educational tools to prepare

58
patients for ACP can include - a pamphlet or a guidebook - use of video decision aids- prompts in EMR for the provider to initiate ACP
McCusker, M., Ceronsky, L., Crone, C., Epstein, H., Greene, B., Halvorson, J.,…Setterlund, L.
2013 Palliative Care for adults National Guideline Clearinghouse-AHRQ
To improve provider understanding of palliative care, increase identification of patients who would benefit from palliative care, improve provider comfort with discussions and assessment, and increase ACP and AD. Evidence-Based Practice Guidelines Level I
Adult patients with a life-limiting illness were may benefit from palliative care
N/A These are the evidence-based practice guidelines
Institute of Medicine (IOM)
2014 Dying in America: Improving Quality and Honoring individual
Systematic Review of over 1500 studies Level 1
This was a review by a committee of 21 members to review ACO and Evidence-Based Practice
This review resulted in education and development for ACP

59
preferences near the end of life. The National Academic Press Report on current state, studies, and improvements to ACP
Interventions to Enhance ACP
Use of Values and goals of care questionnaire
Hoverman, J. R., Taniguchi, C.,
Eagye, K., Mikan, S.,
Kalisak, A., Ash-Lee, S., &
Henchel, R.
2017 If we don't ask, our patients might never tell The impact of routine use of a patient values assessment. Journal of Oncology Practice
To evaluate the effect of good communication and its association with better end-of-life outcomes. Test of Values Assessment (VA) for facilitating advance care planning (ACP). Quality Improvement Project Level V
A total of 1,268 patients completed the VA (56.7% were ≥ 65 years of age, 57.8% completed advance directives.
The findings of the study suggested using a Value Assessment to stimulate ACP discussions over 27 months resulted in (58%) completion of AD. The study also demonstrated that the cancer patients who completed the AD were more likely to die at home and less likely to die in the hospital.
Menon, S., Mccullough,
2016 Use of a values inventory as a
To evaluate the use of a Value Inventory to aid in
Participants were seriously ill male
Findings suggest that allowing

60
L.B., Beyth, R. J., Ford, M.E., Espadas, D., & Braun, U. K.
discussion aid about end-of-life care: A pilot randomized controlled trial. Palliative and Supportive Care
discussion to elicit patients' values and goals for EOL care. A Pilot Randomized Control Trial Level II
outpatients (n = 120) at a large urban Veterans Affairs medical center. The pilot randomized controlled trial, randomizing 60 patients to either the intervention (with the values inventory) or usual care
extra time with an additional visit for EOL discussions might increase the efficacy of ACP
Use of CPR video with and without narration
Epstein, A. S., Shuk, E., O’Reilly, E. M., Gary, K. A., & Volandes
2015 We have to discuss it’: cancer patients’ advance care planning impressions following educational information about cardiopulmonary resuscitation. Psycho-Oncology
To evaluate the effectiveness of the educational method on advance care planning and to understand the gap in knowledge Randomized trial Level II
A total of 54 study participants were Randomized to either the Video Arm or the Narrative arm of the Intervention.
The Findings suggest that Patients with advanced cancer noted to be apprehensive about ACP but wanted to discuss ACP. 26 total (41% of V arm, 56% of N arm) articulated questions. There were seven themes resulted from the questions.

61
Volandes, A. E., Paasche-Orlow, M. K., Mitchell, S. L., El-Jawahri, A., Davis, A. D., Barry, M. J.,…Temel, J. S.
2013 Randomized Controlled Trial of a video decision support tool for cardiopulmonary resuscitation decision making in patients with advanced cancer. Journal of Clinical Oncology
To evaluate the patients and family member understanding of the CPR and resuscitation to make a wise decision on the Resuscitation status Randomized Control Trial Level II
Randomized Control Trial conducted on the patient with advanced cancer who viewed the video of CPR (even just on the mannequin) along with verbal narrative were less likely to opt for CPR as compared to the patient who received the only oral description of CPR and resuscitation
Findings suggest that Education aid with Video along with verbal narration can enhance patient and their family’s understanding of resuscitation
Use of educational pamphlets
Stein, R. A., Sharpe, L, Bell, M. L., Boyle, F.M., Dunn, S. M., &Clarke, S. J.
2013 Randomized Controlled Trial of a structured intervention to facilitate End-Of-Life decision making in patients with advanced cancer. Journal of Clinical Oncology
Evaluation of intervention on end-of-life decision making for patients with advanced cancer who had no additional curative treatment options Randomized Control Trial Level II
Randomized Control Trial at the University of Sydney
Findings of the study demonstrate that the intervention consisting of informational pamphlet and discussion aid earlier placement of DNR orders and patients to choose death at home

62
Use of online website and tools
Sudore, R. L., Boscardin, J., Feuz, M. A., McMahan, R.D., Katen, M.T., & Barnes, D. E.
2017 Effect of the PREPARE website vs. an easy-to-read advance directive on advance care planning documentation and engagement among veterans: a randomized clinical trial. JAMA Internal Med
To evaluate the efficacy of an interactive, patient-centered ACP website (PREPARE) with an easy-to-read advance directive to increase planning documentation in older veterans with chronic illness. Randomized Control Trial Level II
A total of 414 participants were randomized to review PREPARE plus an easy-to-read AD or the AD alone. There were no clinician and system-level interventions or education at multiple primary care clinics at the San Francisco VA Medical Center
The study showed that combining PREPARE and an easy-to-read advance directive resulted in statistically significant higher advance care planning documentation compared to advance directive alone (35% vs. 25%).
Staff education through Vignette techniques
Michael, N., O’Callaghan, C., & Clayton, J. M.
2016 Exploring the utility of the vignette technique in promoting advance care planning discussions with cancer patients and caregivers. Patient Education and Counseling
Evaluation of the intervention with vignette technique along with clinical scenarios to facilitate ACP discussions with patients and caregivers Qualitative descriptive design Level II
Qualitative descriptive design to analyze the data from 3 studies that incorporated Vignette Technique
Research demonstrates that Vignettes may be used in staff training through role play or case discussions as part of the face -to -face interventions to improve knowledge/information processing and facilitate end-of-life conversations

63
Improvement in workflow
Obel, J., Brockstein, B., Marschke, M., Robicsek, A., Konchak, C., Sefa, M.,…Hensing, T.
2014 Outpatient Advance Care Planning for metastatic cancer: A pilot quality improvement initiative. Journal of Palliative Medicine
To evaluate the Timing of ACP and relationship between the improvement in workflow, education, and preparation of guidebook to help in ACP A Feasibility Study Level V
A Feasibility Study in patients with stage IV cancer
Findings from this study suggest that the Timing for ACP was noted to be feasible immediately after a stage IV diagnosis. Systematic improvement in workflow including education on ACP with educational guidebook improved the ACP initiation which was followed by the physician discussing the goals and completing ACP notes in the EMR.
Walczak, A., Butow, P. N., Tattersall, M.H.N., Davidson, P.M., Young, J., Epstein, M.
2017 Encouraging early discussion of life expectancy and end-of-life care: A randomized controlled trial of a nurse-led
To establish and evaluate a nurse facilitated communication support program for patients with advanced cancer assisted in discussing prognosis and end-of-life care.
Randomized control trial conducted at six cancer treatment centers in Sydney, Australia
Findings of the study suggest that the communication support program was the effective and well-received solution to

64
R.,…Clayton, J.M.
communication support program for patients and caregivers. International Journal of Nursing Studies
Randomized Control Trial Level II
encourage early information on end-of-life

65
APPENDIX C PROJECT TIMELINE
August 2018
September 2018
October 2018
November 2018
December 2018
January 2019
February 2019
March 2019
Initial Meeting with ICT
Leadership
Meeting with Project chair
Approval from Project chair
Baseline Data Collection
Proposal initiation ACP Certification Course
Proposal Submission
QIAB and TWU IRB Approval
PFAC Presentation
Meeting with ICT CAD, APP manager, Nurse manager Social Workers
Project Intervention
Data Collection and
Analysis
Presentation of
Project Findings

66
APPENDIX D E-MAIL FROM PATIENT EDUCATION DIRECTOR

67
APPENDIX E PROPOSAL APPLICATION TO MD ANDERSON CANCER CENTER Advance Practice Provider-initiated Advance Care Planning discussions to enhance patient-centered end of life care Poonam Goswami, MS, APRN, FNP
1. Background National guidelines from the American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network (NCCN) recommend that Advance Care Planning (ACP) discussions take place within three months of a diagnosis of incurable cancer. ASCO's Quality Oncology Practice Initiative includes documentation of patients' advance directives by the third office visit as a metric for quality care. Institute of Medicine (IOM) (2014), relates the lack of ACP conversations to patients, family members, and providers expect and wait for the other to initiate them. Results from various studies demonstrated that ACP results in completion of the Advance Directives (AD) or related clinician orders such as a do-not-resuscitate (DNR) order (Billings & Bernacki, 2014; Houben et al., 2014; Luckett et al., 2014). ACP discussion also provides better outcomes for family members, including reduced decision making burden and a few anxieties or depressive symptoms (Stein et al., 2013).
In the Department of Investigational Clinical Trials (ICT), patients referred for clinical trial options after all standard treatment options for the metastatic cancers are exhausted. These patients with metastatic and progressive disease on admission often remain a full code. The Resuscitation status as full code can result in decisions about life-sustaining measures being made in urgency if a patient's condition rapidly deteriorates, resulting in potential burden and distress for family members.
According to Alma Rodriguez (personal communication, December 2017), only 20 % of the patients in the Department of Investigational Clinical Trials (ICT) had completed the Advance Directives. This quality improvement initiative seeks to build on existing interventions to further enhance compliance with ACP discussions and ultimately completion of ADs by patients in the Department of ICT.
2. What are you trying to accomplish? This quality improvement initiative aims to increase communication between advanced practice nurses and patients about ACP and to increase the completion of ADs by patients managed through the ICT service in a pilot cohort of patients. This pilot cohort will include 40 total ambulatory (20) and hospitalized (20) patients for whom Dr. Subbiah is the attending. The pilot project is planned over 6 months from October 2018- March 2019, or until the total number of proposed patients is complete.

68
Increased communication will be measured by the documentation of an ACP discussion in the patients’ electronic medical records with the goal to increase this documentation from 20% of patients to 100% of patients in the pilot cohort. Increased completion of ADs by this patient population will be measured by the presence of the AD documents in the electronic medical records of these patients with the goal to increase the presence of ADs from 20% to 50%.
3. What data will you collect to measure your Improvement? Baseline data collection will include the following:
1. Data, including the presence of documentation of an advanced directive discussion by the APN or physician, and the existence of an AD document, collected from the electronic health record of all new consults seen by Dr. Subbiah in October 2018. This data will provide a baseline completion rate for patients in the pilot cohort compared with the overall department rate of 20% completion. A report will be created in EPIC to generate advanced directive documentation for new patients consulting with Dr. Subbiah.
Outcome data collection will include the following:
1. Data, including the presence of documentation of an advanced directive discussion by the APN or physician, and the presence of an AD document, collected from the electronic health record of up to 40 new consults seen by Dr. Subbiah (20 inpatients and 20 outpatient) in November 2018-March 2018.
2. Patients receiving the ACP education will also be asked to complete a five-question survey (attached) to assess their understanding and how the discussions with the APP on their goals of treatment and wishes influenced their knowledge and helped in the completion of AD and /or change of the code status.
While the data will be collected from individual patient records, it will be reported in aggregate and is consistent with current tracking of advanced directive completion conducted throughout the organization. Survey data responses will be collected without patient identifiers in Qualtrics.
4. Are these data currently being collected?
Currently, the AD completion can be accessed through the Electronic Health Record (EHR) as documented and scanned by the social worker. This project will require the creation of a report from the EHR specific to the selected physician as well as from the list of admitted patients.
5. Are you using patient information? Yes, the patient’s information will be gathered
a. The completion of ACP note and the AD completion will be collected on the new patients consulted by the selected physician in the ICT outpatient clinic.
b. The Completion of ACP note and Code status information will be gathered on the admitted patients in the ICT inpatient.

69
However, patients will be de-identified, and a report will be generated as an aggregate. Besides, the collected data will be explored to identify any variable(s) associated with the AD completion rate and/or code status change, such as ethnicity, race, sex, age, disease type/stage. For the admitted patients, the data will be de-identified to explore the reason for the change in code status as related to stage at EOL versus ACP discussions and/or demographics variables to correlate. We will also collect a data on the patients who will be noted more interested in the Advance Care Planning discussions and willing for AD completions and/or code status change and compare the setting as inpatient versus outpatient.
6. How will data be analyzed? The data will be analyzed using descriptive statistics in collaboration with an MD Anderson Cancer Center’s statistician to evaluate improvement in the AD completion, code status change and also general correlation with the variables as discussed. Also, we will take the qualitative data from the question number three of the survey for analysis for themes generated with various responses.
7. Do you plan to survey patients as part of your project? Yes, we plan to administer a brief five questions survey to assess the impact of ACP discussions by the APP and the patient and family's understanding regarding AD and code status discussions which reflect patient's goals and wishes.
8. What is the intervention you will use to achieve the Aim?
The intervention to be used as part of this project will include a folder prepared with the help of department social worker, guided by the APP (myself) in collaboration with the department administrator and nurse manager. The folder will contain the letter about the ACP initiatives, AD documents and goals of care questionnaire. Currently, these documents are emailed to the patients who were noted to be interested in AD. However, as patients and family get overwhelmed with information and emails, we believe this more personalized approach to the discussion of that information may yield a greater completion of ADs. As part of this project, a team will be formed which will consist of one physician, medical assistant (MA), Registered Nurse (RN), department administrator, APP manager. The meeting will be held before the initiation of the pilot project. The MA and RN will be educated on the need for ACP and AD completion in the clinic. Before the scheduled consult, the EMR will be checked for any scanned AD documents. Patients without the AD documents will be noted on the list for ACP discussions. The MA who will room the patient will check with the patient and family if they have completed the AD at another department or institution the patients without AD will be introduced to the Pilot Project by the RN to get their approval for the discussion.

70
The interested patient would be allowed to choose to watch the ACP video developed by MD Anderson. The APP will initiate the ACP discussions and the importance of completing the AD reflecting the patient's wishes. The APP will go over the AD documents in the folder, and once patient's willingness to complete the documents at the same visit is determined, the social worker will be notified to help with completion of AD documents. Similarly, for the admitted patients, the ACP documents folder will be ready and provided by the APP. After discussing the goals of care and the importance of AD completion, code status will be addressed. For the patients willing to complete the documents same day, the social worker will be notified, and order will be placed in EMR for the social worker to assist in the completion of AD documents. The discussion of code status and wishes will enable the patients to select the code status as either to remain Full Code or to change to Do Not Resuscitate (DNR). For the patient requesting the change of code status to DNR the inpatient attending/primary ICT physician will be notified. The physician will then confirm with the patient and witnesses and would officially place the DNR order in the EMR of the patient. As needed an Out of Hospital Do Not Resuscitate (OOHDNR) form will also be made available for signature by the physician.
9. Which Institute of Medicine Quality Dimension(s) of Patient Care is/are addressed?
The following Institute of Medicine Quality Dimensions of patient care are addressed.
1. Safe 2. Efficient, 3. Patient-Centered 4. Effective

71
Goals of Care and Advance Care Planning Survey This brief survey is a way for you to show which goals of care are important to you. It also measures how much you have been told about advanced care planning. Please put an X in each row to show your answers to the questions below. 1. How much did you know and understand about Advance Care Planning?
1 None
2 Poor
3 A Little
4 Somewhat
5 Complete
Before our discussion
After our discussion
2. Rate how much each of the following goals of care means to you. 1
Not very Important
2 Somewhat Important
3 Important
4 Extremely Important
Spending quality time with family and friends
Pain control (even if the medicine makes me sleepy)
Breathing better (even if I have to be on a machine)
Nutrition (even if I have to have a feeding tube)
CPR (if I am not breathing or my heart stops)
3. Do you feel the Advance Care Planning discussion was important and helped you understand
more about it? Choose Yes or No and Explain
Explain Yes
NO
4. When would you like to complete the Advance Directive documents? Today Next Visit Not Yet

72
Suggested questions (Items 1-6 Pre education; items 7-14 post-intervention)
1. Gender a. Male b. Female
2. Age a. Date of birth up to an including 1944 (Greatest Generation) b. Date of birth 1945-1964, inclusive (Baby Boomers) c. Date of birth 1965- 1984 inclusive (Generation X) d. Date of birth 1985-2004 inclusive (Millennials)
3. Race a. Black b. White c. Asian d. Other
4. Ethnicity a. Hispanic b. Non-Hispanic
5. Time since diagnosis a. Less than 1 year b. 1-2 years c. 3-5 years d. 6-10 years e. Greater than 10 years
6. Do you have an advanced directive? a. Yes b. No
7. I am aware of what an advanced directive is a. Strongly Agree b. Agree c. Disagree d. Strongly Disagree
8. I believe completing an advanced directive is important a. Strongly Agree b. Agree c. Disagree d. Strongly Disagree
9. I believe an advance directive will help to improve the quality of my care a. Strongly Agree b. Agree c. Disagree d. Strongly Disagree

73
10. I believe an advanced directive will help my healthcare providers understand my care decisions
a. Strongly Agree b. Agree c. Disagree d. Strongly Disagree
11. Did you find the ACP educational materials understandable?
a. Yes b. No
i. Please explain: 12. Did reviewing the ACP education with the Advanced Practice Nurse encourage you to
complete an advanced directive? a. Yes b. No
13. Did reviewing the ACP education with the Advanced Practice Nurse encourage you to make any changes to your advanced directive?
a. Yes b. No
14. Did reviewing the ACP education with the Advanced Practice Nurse prompt you to provide a copy of your AD to MD Anderson?
a. Yes

74
APPENDIX F POWERPOINT PRESENTATION AT PFAC

75
APPENDIX G FEEDBACK FROM PFAC
76
APPENDIX H PROPOSAL APPROVAL LETTER FROM MD ANDERSON

77
APPENDIX I APPROVAL LETTER FROM TWU IRB

78
APPENDIX J ACP CERTIFICATION

79
APPENDIX K ACP SLOGAN AND LETTER FOR ACP FOLDER Advance Care Planning It is all about You! Your Decisions Your Plans Please Make your wishes known and let us help you!

80
APPENDIX L ROSSWURN AND LARRABEE’S CHANGE MODEL

81
APPENDIX M PLAN-DO-STUDY-ACT MODEL

82
APPENDIX N COST BENEFIT ANALYSIS AND POTENTIAL COST AVOIDANCE
Project Cost Expenses
Direct Cost
Total
APP salary approx. $75/hr
40 (patients) X 30 minutes $1500
Cost of ACP Certification course $189 Cost of folders and printed documents provided by ICT
Approximately $ 4 per folder X40 folders
$160
Indirect Cost Other costs Building maintenance
( approximately) $200
Total Expenses $1999 Potential Revenue
Reimbursement Total visits billed Billing code
40 99497 $86x40= $3,440 Total Cost Benefit $1,491
Potential Cost Avoidance One day ICU length of stay reduced x1 patient $6,100 (per Khandelwal et al.,
2016) Total length of stay avoided x1 patient $38,000
Total patients enrolled in hospice and hence avoided the hospital stay
8
Total Likely cost avoidance 8 x 6,100= $48, 800





















![Home [] · 2021. 2. 24. · samsung samsung samsung samsung samsung advance advance advance advance advance advance advance advance advance advance 223sw 2233sw 2233sw 2233sw 933sn](https://img.pdfslide.us/doc/110x75/613cd1974c23507cb6359ff0/home-2021-2-24-samsung-samsung-samsung-samsung-samsung-advance-advance.jpg)







