Embed Size (px)
Citation preview
Advanced MRI methods in diagnostics of spinal cord
pathology
Stanisław KwiecińskiDepartment of Magnetic Resonance
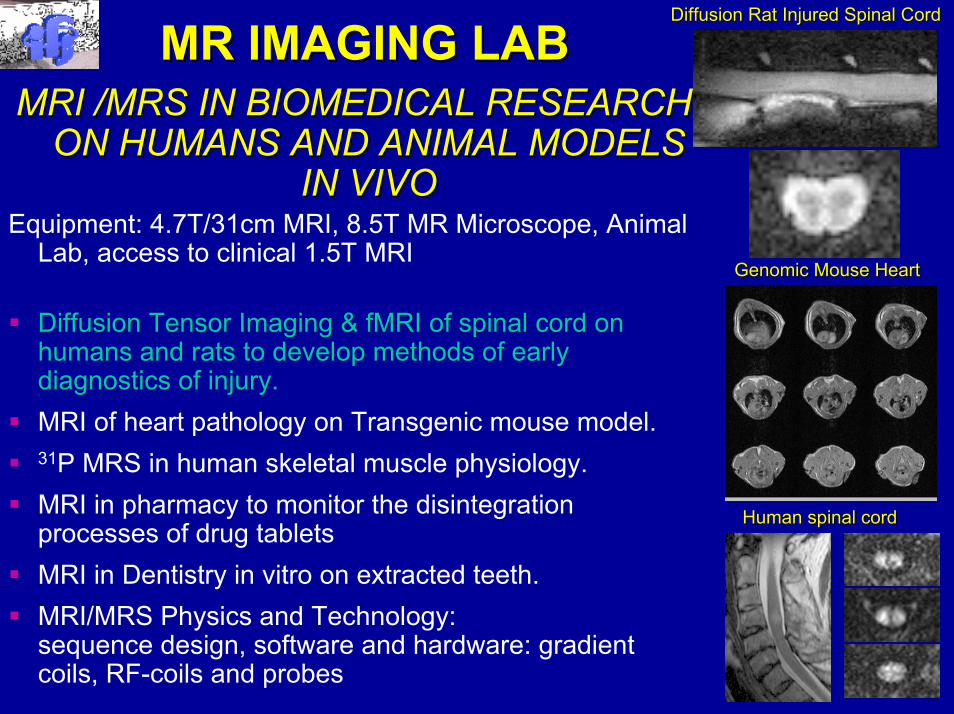
MR IMAGING LABMR IMAGING LABMRI /MRS IN BIOMEDICAL RESEARCH MRI /MRS IN BIOMEDICAL RESEARCH
ON HUMANS AND ANIMAL MODELS ON HUMANS AND ANIMAL MODELS IN VIVOIN VIVO
Equipment: 4.7T/31cm MRI, 8.5T MR Microscope, AnimalLab, access to clinical 1.5T MRI
Diffusion Tensor Imaging & fMRI of spinal cord on humans and rats to develop methods of earlydiagnostics of injury.MRI of heart pathology on Transgenic mouse model.31P MRS in human skeletal muscle physiology.MRI in pharmacy to monitor the disintegration processes of drug tabletsMRI in Dentistry in vitro on extracted teeth.MRI/MRS Physics and Technology:sequence design, software and hardware: gradient coils, RF-coils and probes
GenomicGenomic Mouse HeartMouse Heart
HumanHuman spinal cordspinal cord
DiffusionDiffusion Rat Rat Injured Spinal CordInjured Spinal Cord
Spinal Cord Imaging – why so important ?
• Spinal cord injuries are main factor of permanentdisability affecting population as a result of communication, work or sport accidents.
• Outgrowth and regeneration of injured nerve fibersis possible
• Early diagnosis of pathologies such asAlzheimer, Sclerosis Multiplex, tumors,venous malformations ...
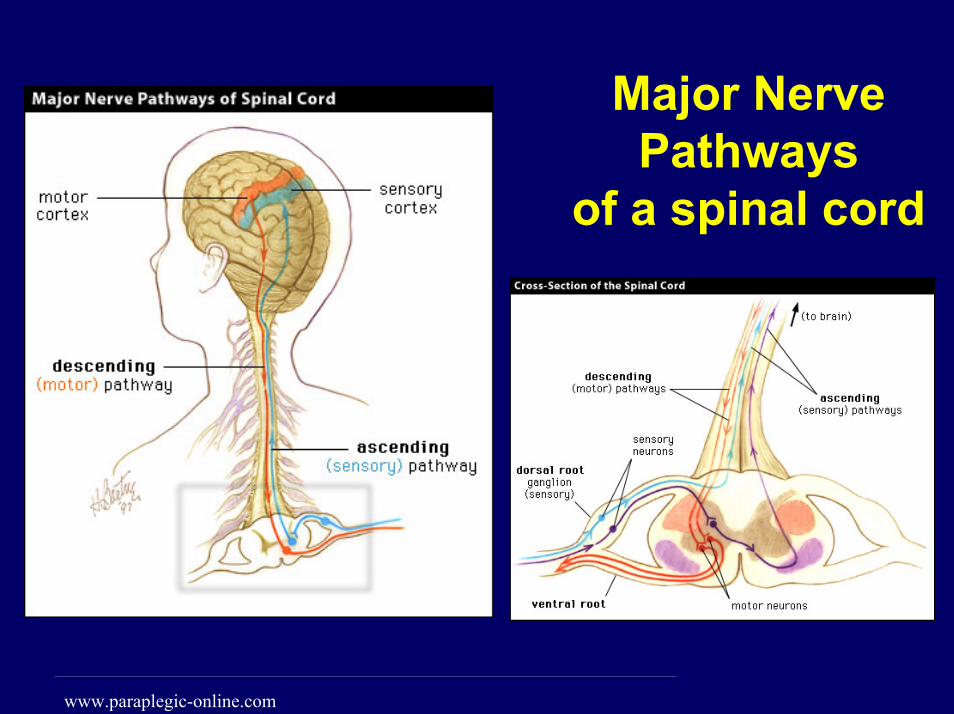
Major Nerve Pathways
of a spinal cord
www.paraplegic-online.com
What MRI Physicist can offer ?
To develop a non-invasive, quantitative method of EARLY COMPLETE DIAGNOSTICS of the spinal cord injuries , white matter diseases and other spinal cord pathologies in humans in vivo based on
MR diffusion tensor imaging (DTI)
and
functional MRI (fMRI)
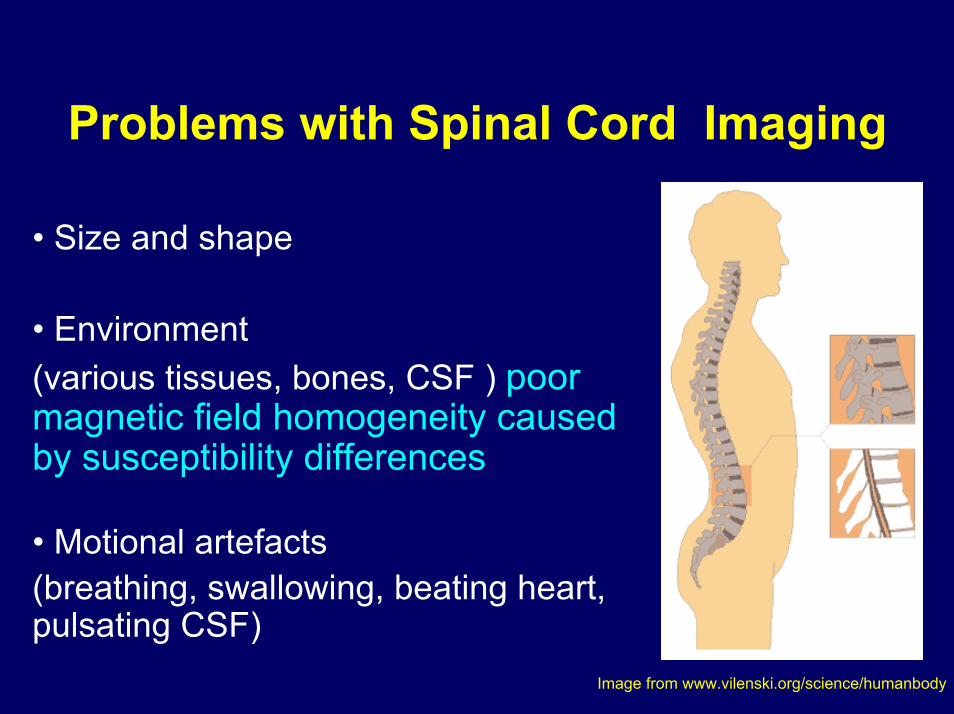
Problems with Spinal Cord Imaging
• Size and shape
• Environment (various tissues, bones, CSF ) poor magnetic field homogeneity caused by susceptibility differences
• Motional artefacts (breathing, swallowing, beating heart, pulsating CSF)
Image from www.vilenski.org/science/humanbody
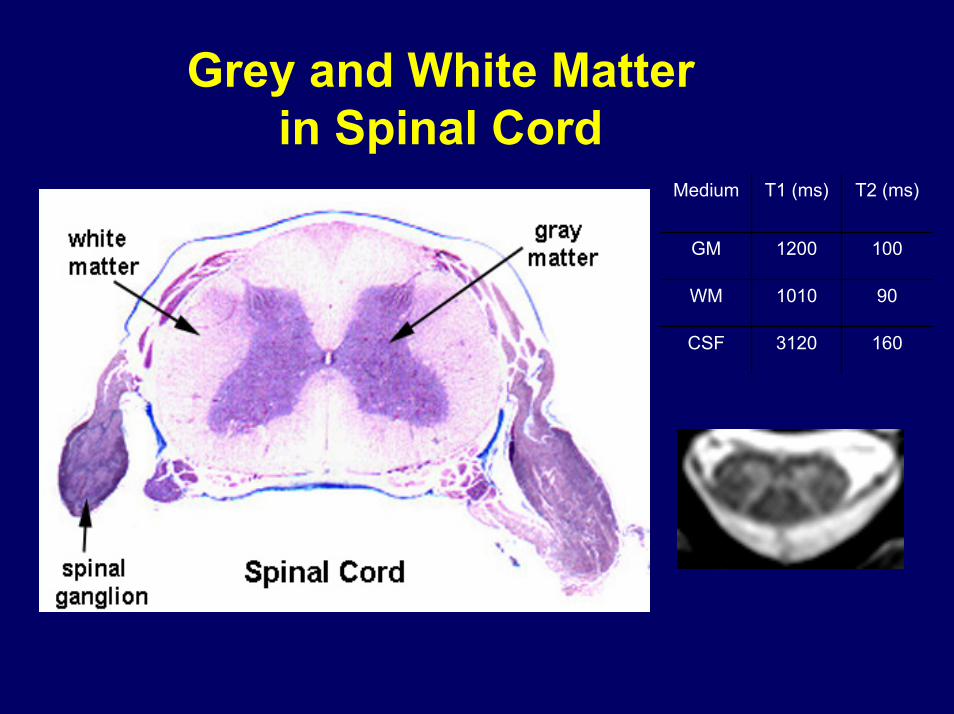
Grey and White Matter in Spinal Cord
1603120CSF
901010WM
1001200GM
T2 (ms)T1 (ms)Medium
Why Diffusion Imaging ?• Diffusion provides unique indicator of tissue
microstructure (natural contrast !!!)
• Diffusional parameters change immediately after injury
• Diffusion attributes allow „fiber tracking“
Extracting information from Diffusion Imaging:
• Images
• Vector Maps
• Quantitative Analysis (FA – Fractional AnisotropyADC – Apparent Diffusion Coeficient...)
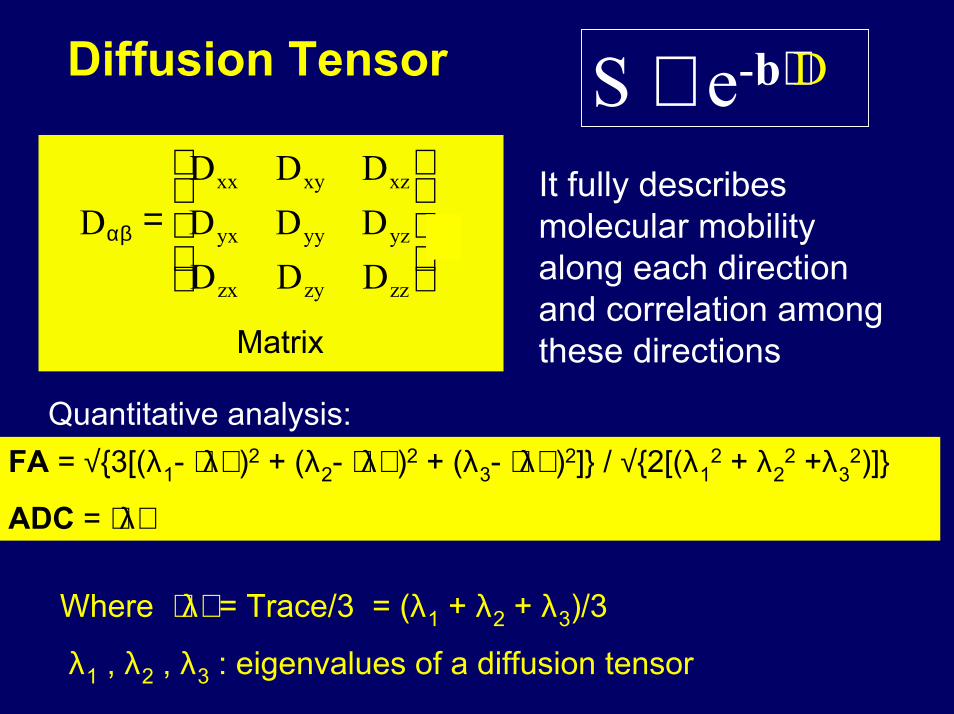
Diffusion Tensor S ∼ e-b⋅D
DD D DD D DD D D
xx xy xz
yx yy yz
zx zy zz
αβ =
,
Matrix
It fully describes molecular mobility along each direction and correlation among these directions
Quantitative analysis:FA = √{3[(λ1- ⟨λ⟩ )2 + (λ2- ⟨λ⟩ )2 + (λ3- ⟨λ⟩ )2]} / √{2[(λ1
2 + λ22 +λ3
2)]}
ADC = ⟨λ⟩
Where ⟨λ⟩ = Trace/3 = (λ1 + λ2 + λ3)/3
λ1 , λ2 , λ3 : eigenvalues of a diffusion tensor
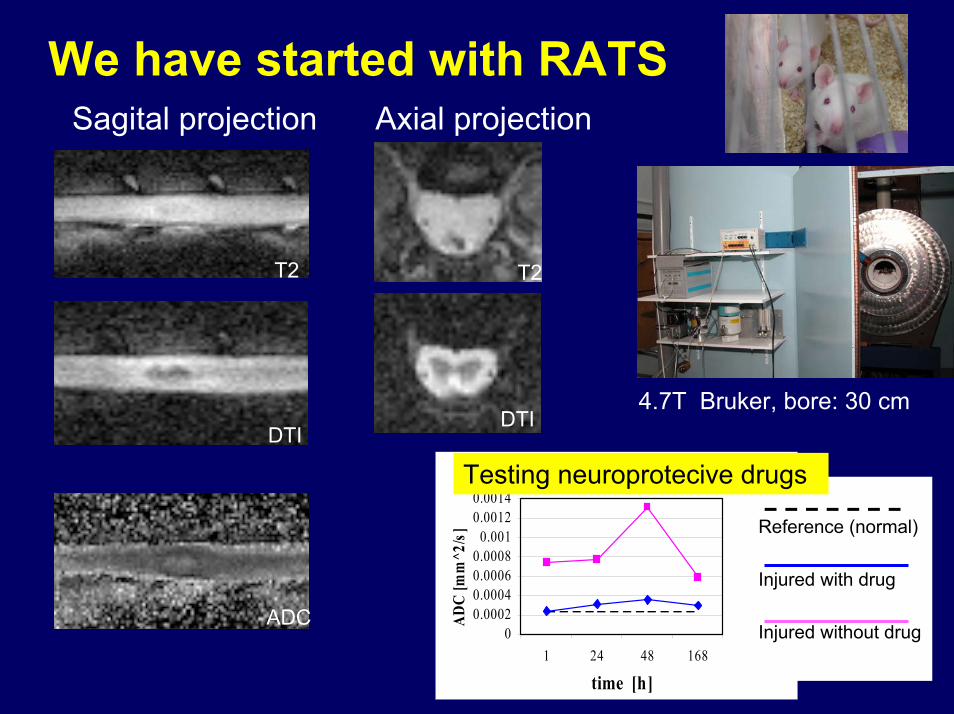
We have started with RATSSagital projection Axial projection
T2T2
DTIDTI
4.7T Bruker, bore: 30 cm
tADC Slice 1 WM
00.00020.00040.00060.0008
0.0010.00120.0014
1 24 48 168
time [h]
ADC
[mm
^2/s
] Reference (normal)
Injured with drug
Injured without drug
Testing neuroprotecive drugs
ADC
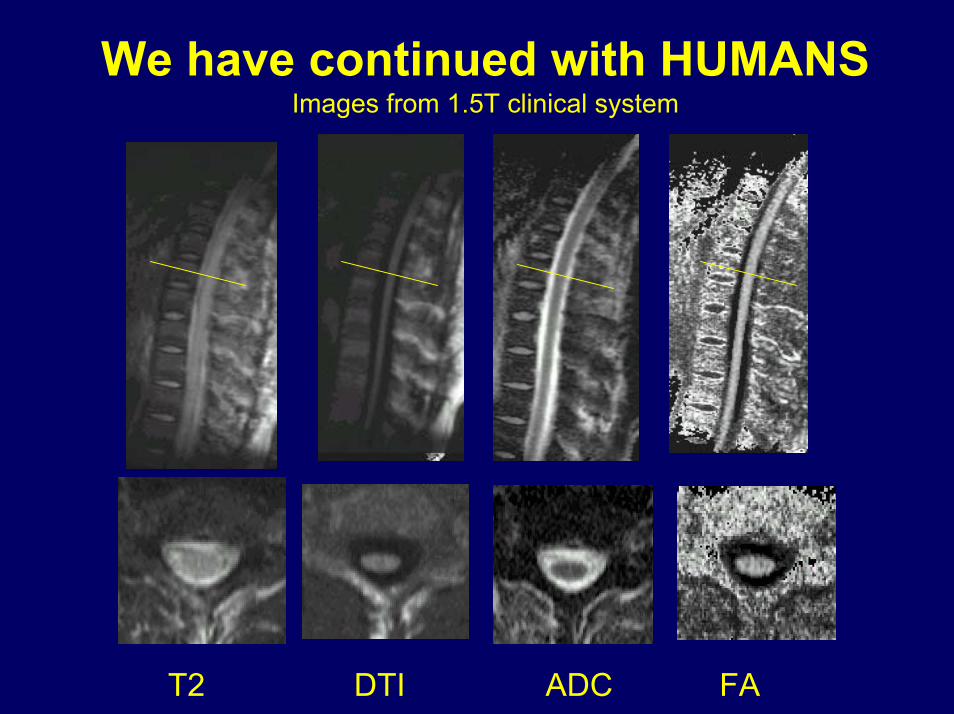
We have continued with HUMANS Images from 1.5T clinical system
T2 DTI ADC FA
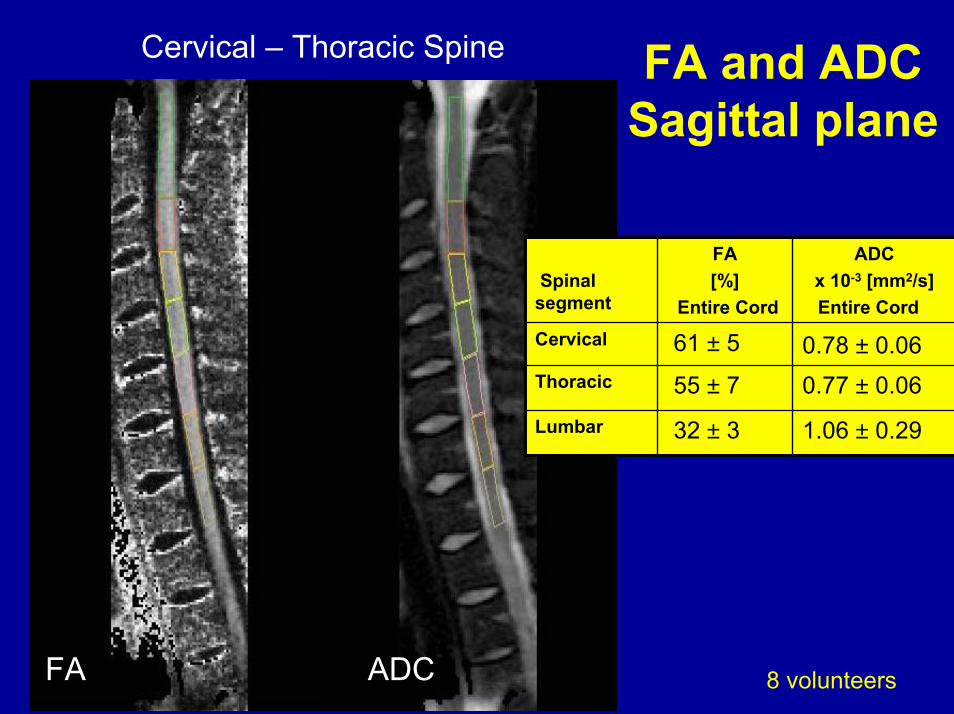
Cervical – Thoracic Spine FA and ADC Sagittal plane
8 volunteersFA ADC
1.06 ± 0.2932 ± 3Lumbar
0.77 ± 0.0655 ± 7Thoracic
0.78 ± 0.0661 ± 5Cervical
ADC x 10-3 [mm2/s] Entire Cord
FA [%]
Entire CordSpinal
segment
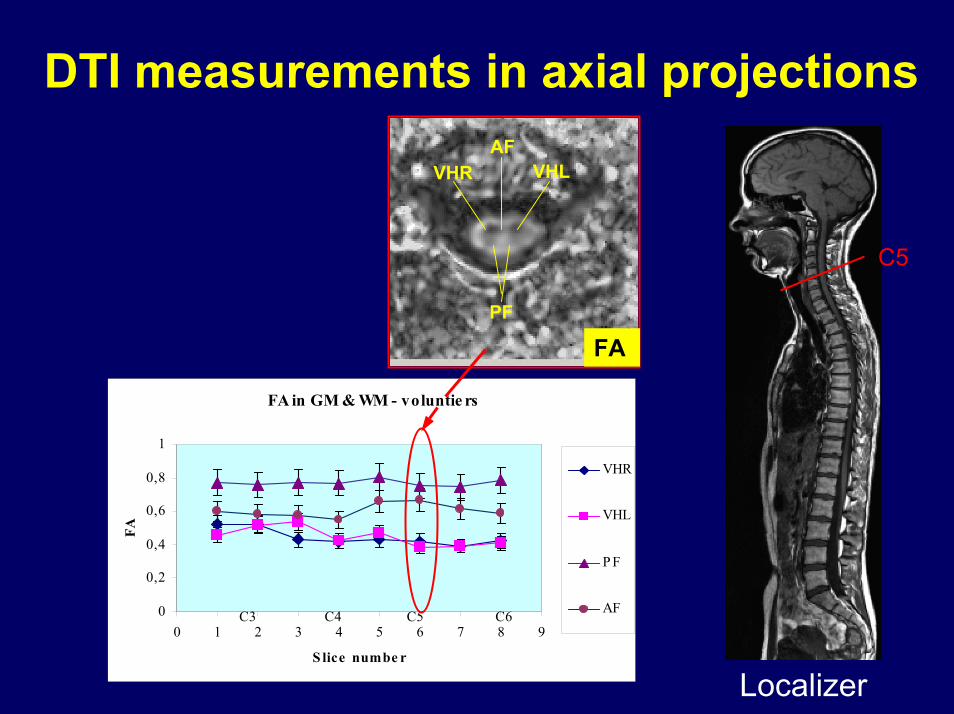
DTI measurements in axial projections
FA in GM & WM - voluntie rs
0
0,2
0,4
0,6
0,8
1
0 1 2 3 4 5 6 7 8 9
S lice numbe r
FA
VHR
VHL
P F
AFC3 C4 C5 C6
Localizer
FA
C5
VHR VHLAF
PF
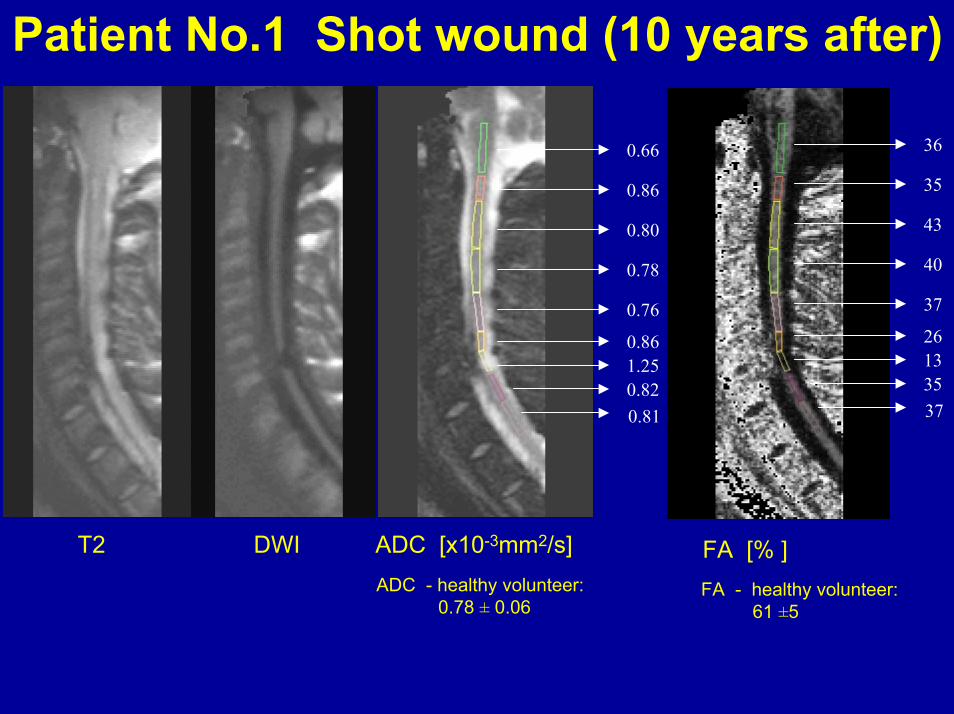
Patient No.1 Shot wound (10 years after)
0.66
0.86
0.80
0.78
0.76
0.861.250.820.81
36
35
43
40
37
26133537
T2 DWI ADC [x10-3mm2/s]ADC - healthy volunteer:
0.78 ± 0.06
FA [% ]FA - healthy volunteer:
61 ±5
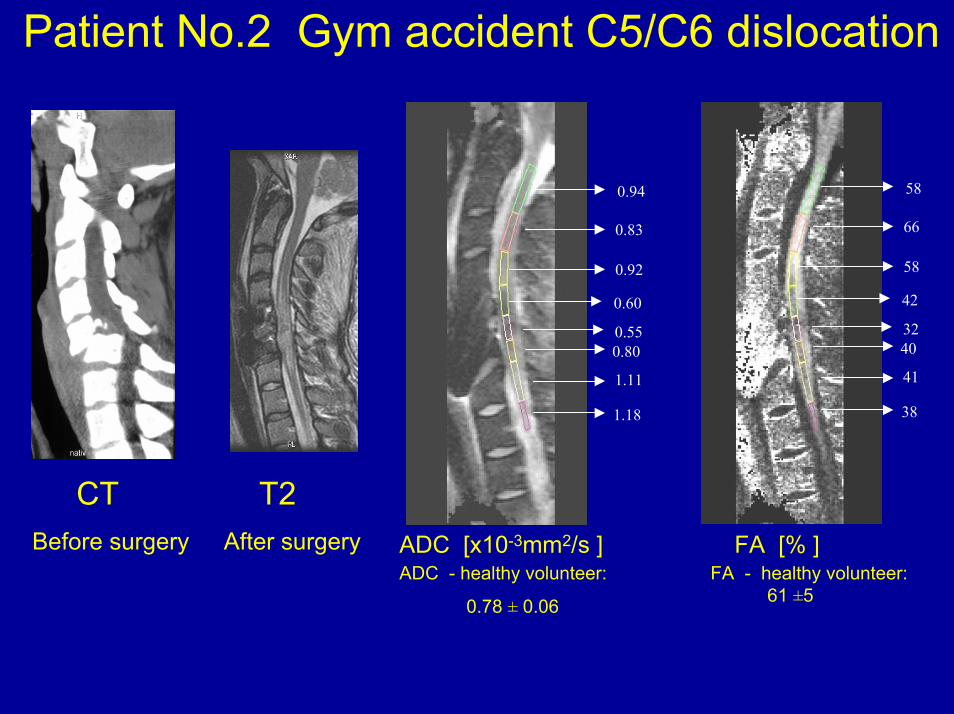
Patient No.2 Gym accident C5/C6 dislocation
ADC [x10-3mm2/s ]ADC - healthy volunteer:
0.78 ± 0.06
FA [% ]FA - healthy volunteer:
61 ±5
0.94
0.83
0.92
0.60
0.550.80
1.11
1.18
58
66
58
42
3240
41
38
CTBefore surgery
T2After surgery
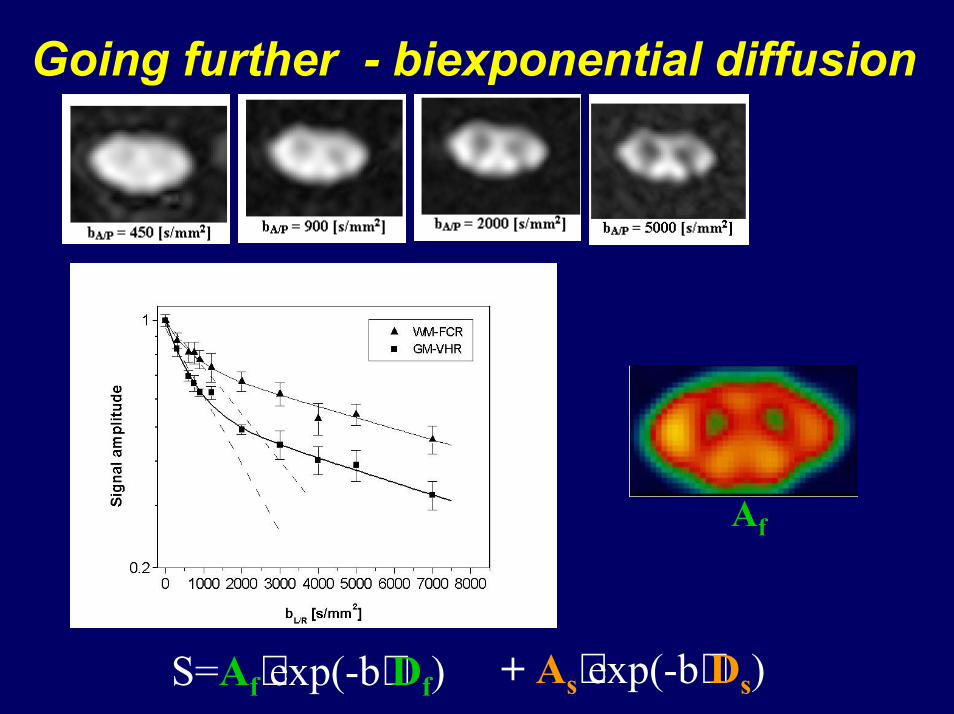
Going further - biexponential diffusion
Af
+ As⋅exp(-b⋅Ds) S=Af⋅exp(-b⋅Df)
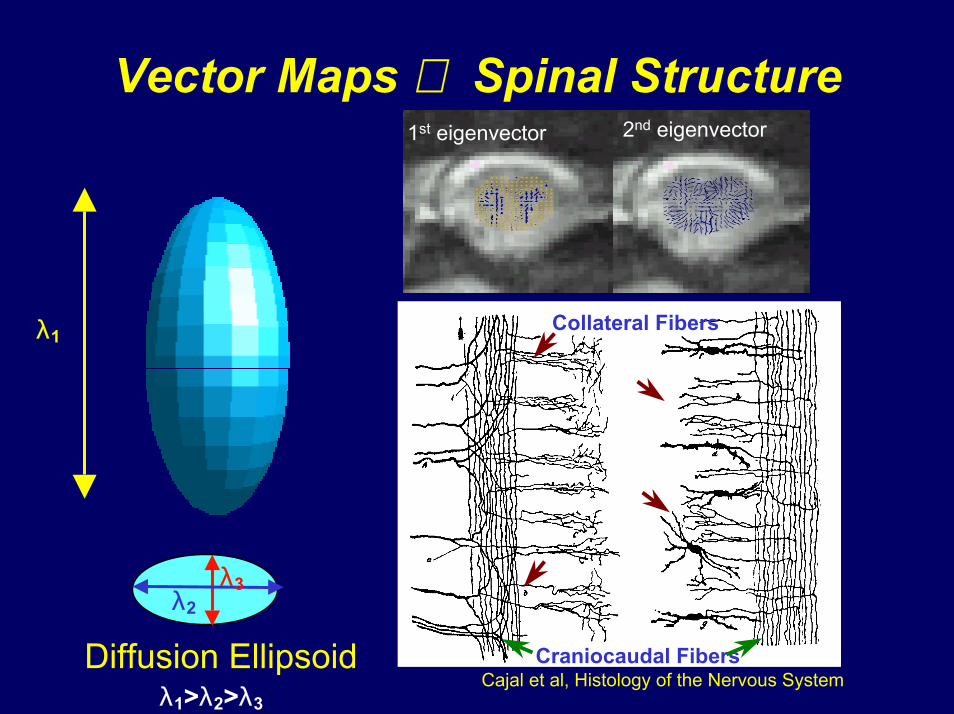
Vector Maps ⇒ Spinal Structure1st eigenvector 2nd eigenvector
Diffusion Ellipsoid
λ1
λ3λ2
λ1>λ2>λ3Cajal et al, Histology of the Nervous System
Craniocaudal Fibers
Collateral Fibers
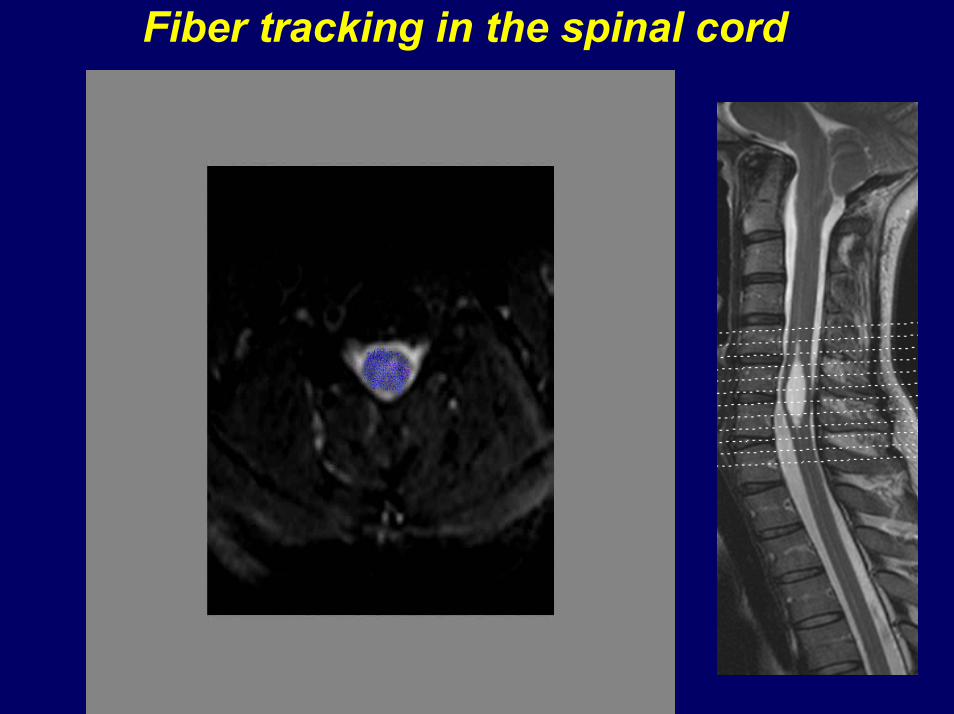
Fiber tracking in the spinal cord
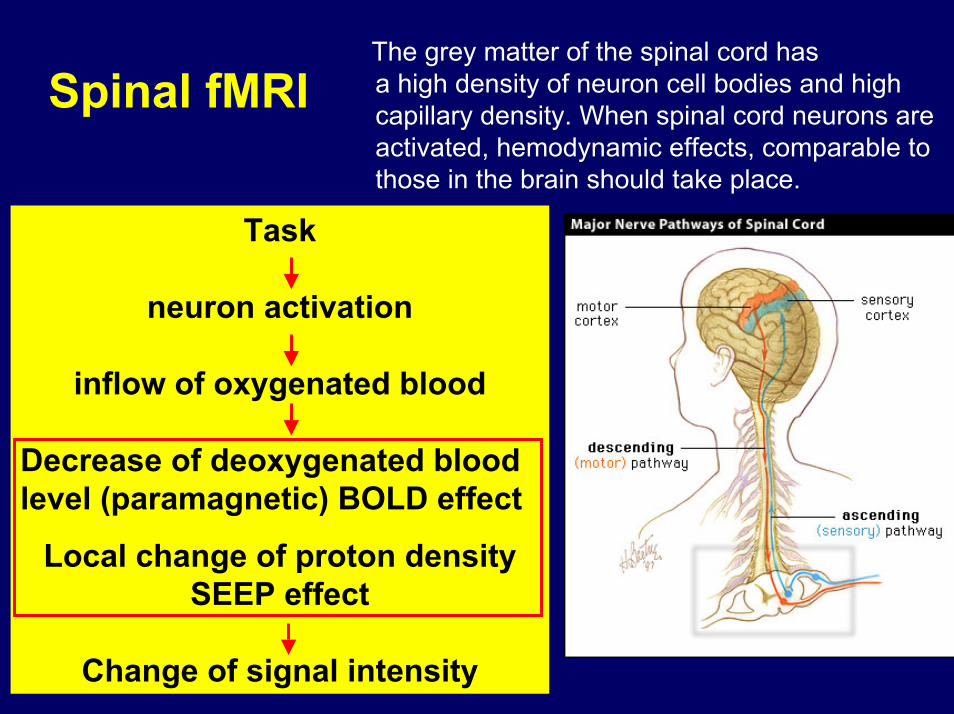
The grey matter of the spinal cord has a high density of neuron cell bodies and high capillary density. When spinal cord neurons are activated, hemodynamic effects, comparable to those in the brain should take place.
Spinal fMRI
Task
neuron activation
inflow of oxygenated blood
Decrease of deoxygenated blood level (paramagnetic) BOLD effect
Local change of proton density SEEP effect
Change of signal intensity
Spinal cord fMRI study: aims
• Determine whether fMRI signal can be measured on a 1.5T / 3T clinical MR systems and on 9T research system
• Determine whether the fMRI signal can be spatially localized to particular anatomical locations
• To verify intra-subject reproducibility
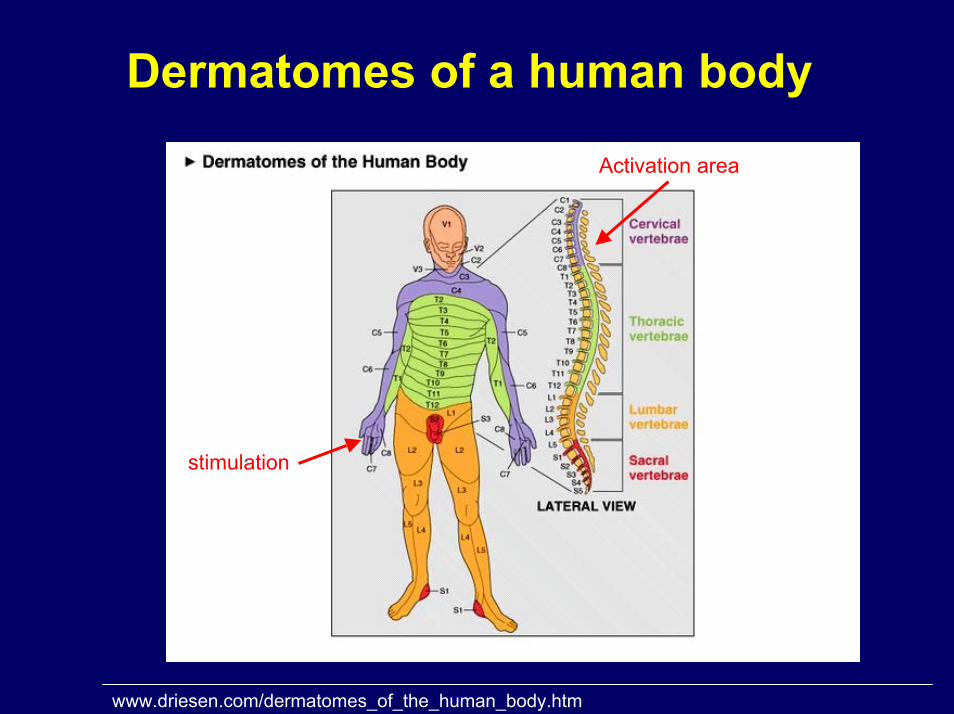
Dermatomes of a human body
stimulation
Activation area
www.driesen.com/dermatomes_of_the_human_body.htm
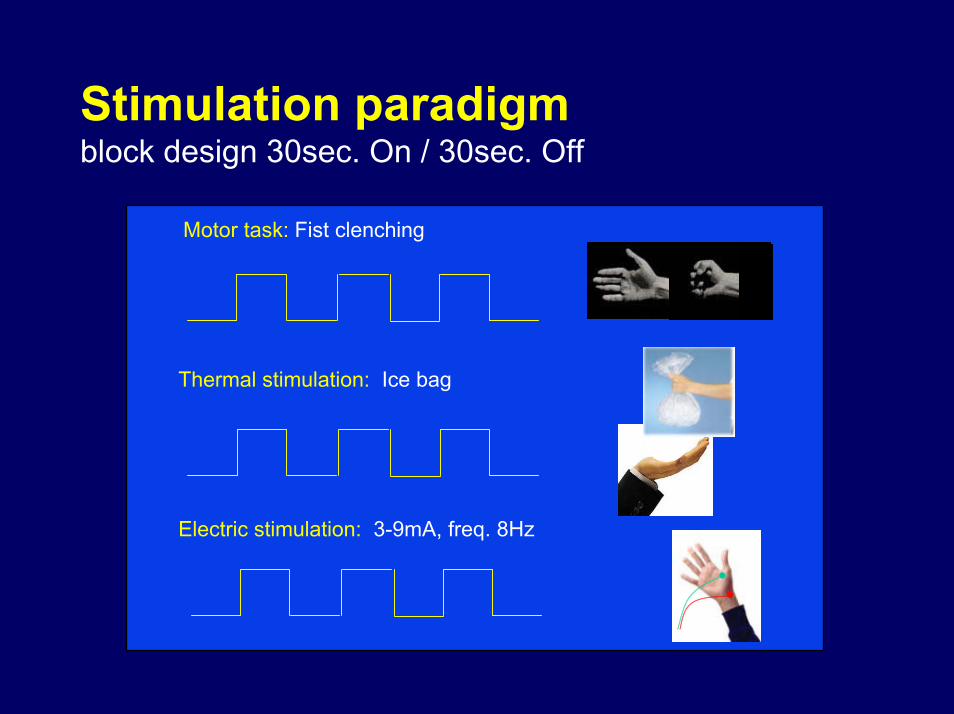
Stimulation paradigmblock design 30sec. On / 30sec. Off
Motor task: Fist clenching
Thermal stimulation: Ice bag
Electric stimulation: 3-9mA, freq. 8Hz
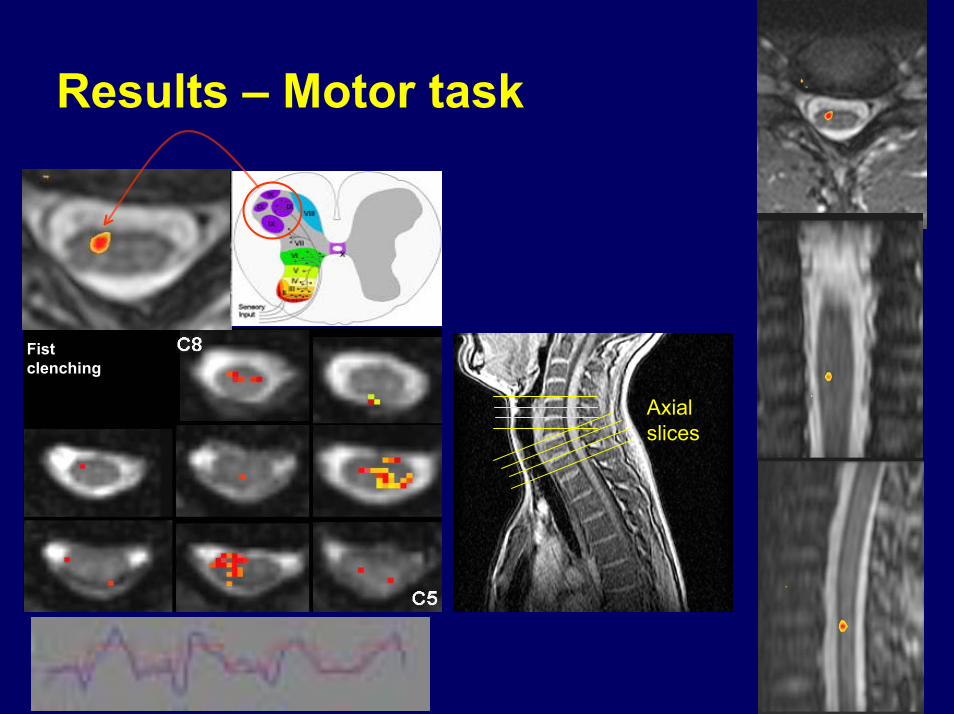
Results – Motor task
Fist clenching
Axialslices
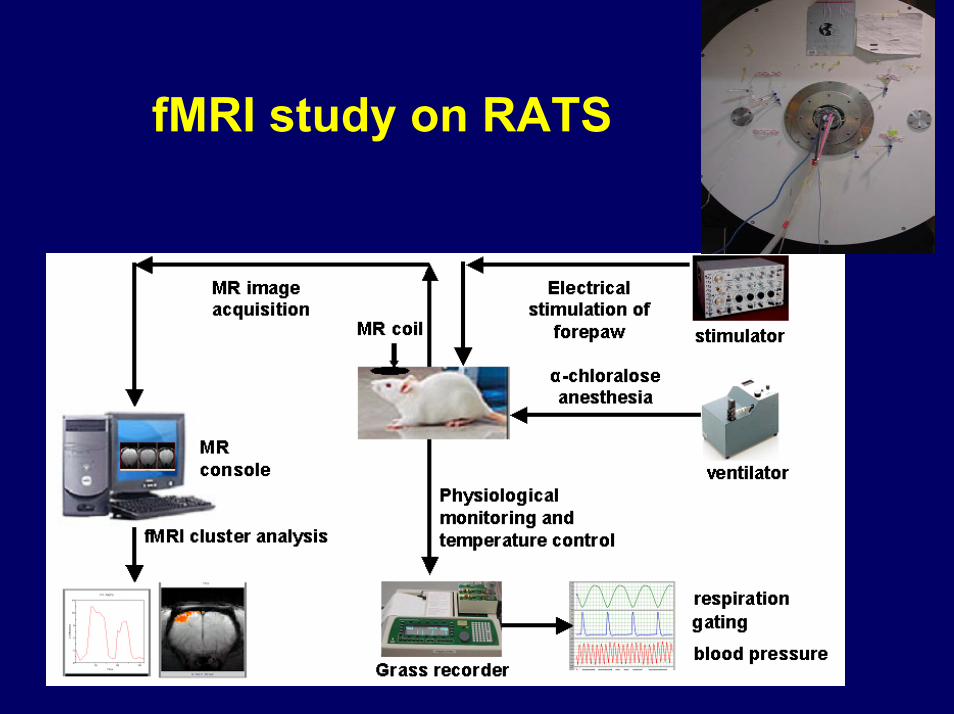
fMRI study on RATS
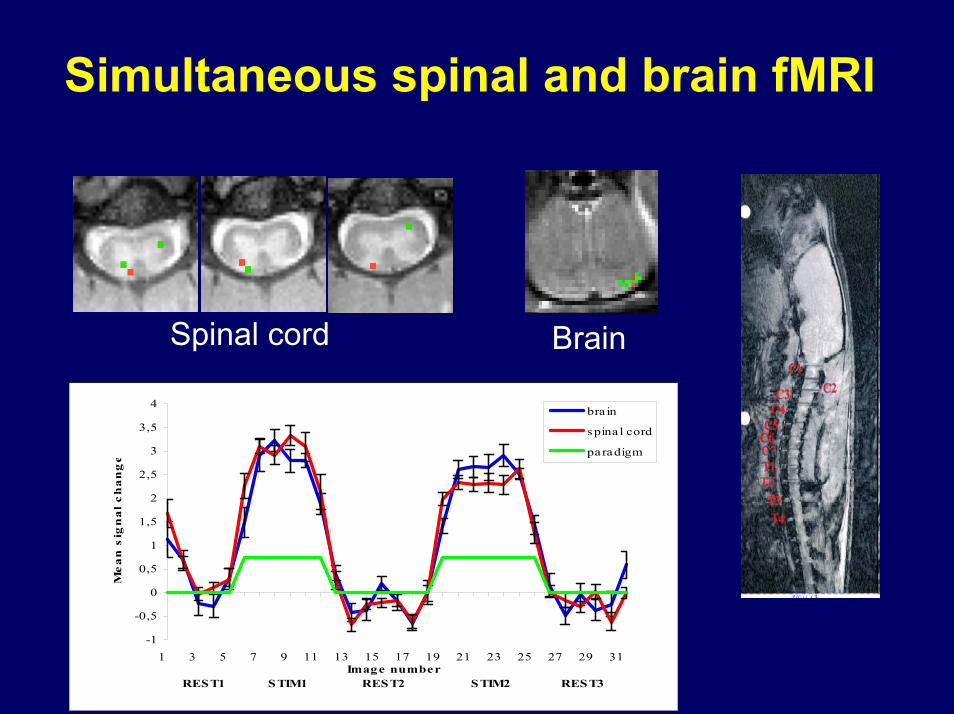
Simultaneous spinal and brain fMRI
Spinal cord Brain
-1
-0,5
0
0,5
1
1,5
2
2,5
3
3,5
4
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31Image number
REST1 STIM1 REST2 STIM2 REST3
Me
an
sig
na
l c
ha
ng
e
bra in
spina l cord
paradigm
Conclusions
DTI and fMRIare powerful tools enabling
complete diagnosis of spinal cord injury and pathology
in the near future

Thank you for your attention
Acknowledgment to our scientific collaborators in the field of spinal MRI
M.Konopka, M.Hartel, Diagnostic Imaging Centre „HELIMED”, Katowice, Poland
B.Tomanek, P.Stroman, Institute for Biodiagnostics, Calgary, Alberta, Canada
S.Kollias, P.Summers, Institute of Neuroradiology, University Hospital Zurich, Switzerland







![Multimodal MRI evaluation of acute mild-contusive injury ...neuroanatomy.org/2008/083_092.pdf · Radiology and Radiological Science, ... Key words [spinal cord] [spinal cord injury]](https://img.pdfslide.us/doc/110x75/5ab771ad7f8b9ad5338b8e6e/multimodal-mri-evaluation-of-acute-mild-contusive-injury-and-radiological-science.jpg)





















