Embed Size (px)
DESCRIPTION
Discovery of key biological mechanisms Identify key drug-able molecular targets Develop compound to inhibit target Clinical evaluation of compound
Citation preview

Advanced Clinical Trial Educational Session
Richard Simon, D.Sc.Biometric Research BranchNational Cancer Institute

BRB Websitehttp://brb.nci.nih.gov
• Powerpoint presentations & reprints• BRB-ArrayTools software• Accelerated titration design software• Web based sample size planning
– Optimal 2-stage phase II designs– Phase II/III trials– Clinical Trials with Predictive Biomarkers– Development of prognostic signatures

Discovery of keybiological mechanisms
Identify key drug-ablemolecular targets
Develop compoundto inhibit target
Clinical evaluation of compound

Can the compound be administeredsafely at a dose that inhibits the
target?
Does the drug have sufficient anti-tumor activity in a defined
target population to warrant phase IIITrial?
Does the drug have medical utilityfor a target population?
How should the drug be used inpractice?

Phase III Clinical Trials Should• Test the null hypothesis of no treatment benefit
for the new treatment vs control for the identified target population(s) while preserving the type I error
• Provide physicians with predictive tools and measures of uncertainty to assist in applying the results to individual patients– Method of Freidlin, Jiang, Simon to develop and
internally validate algorithms for individualizing therapy


Objectives of Phase II Trials
• Does the drug inhibit the putative molecular target
• Can a promising predictive biomarker be determined for identifying patients whose tumors are sensitive to the drug
• Does the drug or a regimen containing the drug have sufficient anti-tumor activity in a targeted population to warrant phase III testing?

Success May Require
• Inhibit pathways deregulated by key oncogenic mutations
• Treat the right tumors with the right drugs• Use combinations of molecularly targeted drugs• Treat early
– Before mutational meltdown– Adjuvant studies
• Use sensitive endpoints in phase II to optimize regimens and predictive markers

Endpoints for Phase II
• Objective response rate• Tumor growth delay
– Stable disease– Proportion without progression at 8 weeks– Progression-free survival

Single Arm Optimal Two-Stage Phase II Design=0.10 =0.20
http://brb.nci.nih.gov
Null response probability
Desirable response probabiliity
Stop early if r1 responses in n1 patients
Reject drug if r responses in n patients
Average sample size
Probability of early stopping
p0 p1 r1/n1 r/n EN(p0) PET(p0)
.05 .25 0/6 2/23 10.5 .74
.10 .30 0/7 3/18 12.7 .48
.20 .40 2/12 7/25 17.7 .56
.30 .50 5/15 12/32 20.7 .72

Single Arm Optimal Two-Stage Phase II Design=0.10 =0.20
http://brb.nci.nih.gov
Null response probability
Desirable response probabiliity
Stop early if r1 responses in n1 patients
Reject drug if r responses in n patients
Average sample size
Probability of early stopping
p0 p1 r1/n1 r/n EN(p0) PET(p0)
.05 .20 0/9 2/24 14.5 .63
.10 .25 1/13 5/34 21.0 .62
.20 .35 2/13 12/46 30.0 .50
.30 .45 6/20 20/55 33.7 .62

Single Arm Phase II With Specific Historical Controls
• Patients accrued at the same center or group with same work-up and response evaluation
• Matched for prognostic comparability or post-stratified for comparability

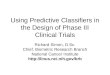
Single arm phase II trial Comparing response rate to specific historical controlsNumber of new patients required to detect 20% absolute difference.
Proportion of Success for Historical Controls Number of Historical Controls
30 50 75 100 inf
0.10
36
30
28
27
18
0.20
68
43
36
33
25
0.30
132
54
41
37
32
0.40
267
59
43
37
37
alpha=0.10, beta=0.20


Progression Delay
• Evaluating progression delay is inherently comparative– Rate of tumor progression untreated is often
highly variable• Stable disease definitions are rarely
documented as being interpretable as a drug effect

Randomized
Specific historical controls or duration documented based
on historical controls
Undocumented duration representing stability withno controls

Rixe and FojoClin Cancer Res 2007;13:7280
• “… agents we now refer to as cytotoxic have for decades been observed to cause cytostasis but were never described in those terms. Indeed, in most cases cytostasis was viewed as ineffective and disregarded. …many if not all of these [molecularly targeted] compounds possess cytotoxic activity that is at least as important if not more so than any cytostatic property…pure cytostatic agents may not exist…when cytostatis occurs it will usually be followed by either cytotoxicity or cellular escape from the stasis.”


Limitations of Randomized Phase II Clinical Trials
• Increased sample size• Reduced accrual rate• Reduced number of new drugs and
regimens that can be screened• Difficulty in accruing to subsequent phase
III trials

Randomized Phase II Trials: What Does Randomization Gain
H. Samuel Wieand JCO 23:1794, 2005
• “Johnson et al presented the results of a randomized phase II design that called for a formal comparison of regimens at the conclusion of the trial. This design is used less frequently because it requires roughly four times as many patients as a single arm trial … the design for the Johnson et al. trial required 33 patients for each of the three arms but was powered for a huge difference in response rates…”

Number of total events to observe in two-arm randomized phase II trial comparing progression-free survival
1-sided significance.
Reduction
in hazard
Ratio of
medians
Equal Randomizat ion 2:1 Randomizat iona
= 0.05 = 0.10 = 0.05 = 0.10
Power=0.8 Power=0.9 Power=0.8 Power=0.9 Power=0.8 Power=0.9 Power=0.8 Power=0.9
25% 1.33 301 417 219 319 339 469 246 358
33% 1.5 155 215 113 164 175 242 127 185
40% 1.67 96 132 70 101 108 149 78 114
50% 2.0 52 72 38 55 59 81 43 62

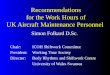
Copyright © American Society of Clinical Oncology
Heymach, J. V. et al. J Clin Oncol; 25:4270-4277 2007
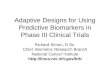
Fig 1. Study design



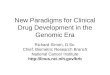
Process and/or flow or approaches for determination of phase II trial design recommendations.
Seymour L et al. Clin Cancer Res 2010;16:1764-1769
©2010 by American Association for Cancer Research

Randomized Phase II Selection Designs
• K experimental arms, no control arm• Select arm with highest response rate or
disease control rate further development
• Simon, Wittes, Ellenberg; Cancer Treatment Reports 69:1375, 1985

Randomized Phase II Selection Designs
• Can use with time to progression endpoint• Can use with early stopping criteria
– e.g. Use optimal 2-stage phase II design separately for each treatment arm; at end of trial select arm with highest observed response rate
• Can be used with cross-over to secondary treatment to obtain additional information
• Can be used within genomically defined strata

K Experimental Arms Optimal Two-Stage Phase II Design
for each arm =0.10 =0.20
Null response probability
Desirable response probabiliity
Stop early if r1 responses in n1 patients
Reject drug if r responses in n patients
Probability of Correct Selection
Probability of Correct Selection
p0 p1 r1/n1 r/n K=2 arms K=3 arms
.05 .25 0/6 2/23 0.81 0.80
.10 .30 0/7 3/18 0.86 0.82
.20 .40 2/12 7/25 0.87 0.83
.30 .50 5/15 12/32 0.83 0.80




Optimizing the Number and Size of Phase II Trials for a Horizon of 1000 patients
Inter-trial
variabilitya
in p0
Size of
treatment
effectb
Optimal single arm trials Optimal randomized 2-arm trials
n patients
per trialc
m trialsc Prob of
successd
n patients
per trialc
m trialsc Prob of
successd
low large 25 40 0.85 50 20 0.79
low moderate 25 40 0.85 50 20 0.79
higha large 20 50 0.64 50 20 0.78
high moderate 20 50 0.58 100 10 0.76

Are There That Many Worthy Candidate Treatment Regimens?
• Combinations of molecularly targeted agents
• Genomic subsets of tumors

Marker Based Phase II DesignPusztai, Anderson, Hess (ClinCancerRes 2007)
• Two stage design, treat all comers of a given primary site
• If the overall number of responders at the end of stage 1 is adequate, then continue and complete trial based on overall analysis
• If the overall number of responders at the end of stage 1 is not adequate, then start separate two stage phase II trials for each marker stratum


Bayesian Adaptive DesignBATTLE Study in NSCLC
• Randomized phase II trial with 4 experimental regimens, no control group– Erlotinib, sorafenib, vandetanib, erlotinib+bexarotene
• Tumor biopsy at entry, assayed for candidate predictive biomarkers– EGFR mutation or amplification– KRAS or BRAF mutation– VEGFr2 over-expression– Cyclin D1 over-expression
• Endpoint is freedom from progression at 8 weeks

Bayesian Adaptive DesignBATTLE Study in NSCLC
• First 97 patients were randomized equally to the 4 arms• Then, the randomization was weighted based on
estimated of effectiveness of each regimen for patients in each biomarker stratum
non suspended treatments i
ˆ ( )( )
ˆ ( )
ˆ ( ) Bayesian estimate of 8 week disease control rate for treatment i of patient in marker stratum k based on using outcome d
jkjk
ik
ik
tw t
t
t
ata available at time t

Bayesian Adaptive DesignBATTLE Study in NSCLC
• As data accumulates, for each treament i and marker stratum k the probability that 8 week disease control is > 0.5 is computed
• If that probability becomes <0.10 for some treatment i and stratum k, then use of that treatment in that stratum is suspended

Bayesian Adaptive DesignBATTLE Study in NSCLC
• Results not yet published• Approximately 255 patients randomized• Erlotinib performed best against EGFR mutant
tumors• Sorafinib performed best against KRAS mutant
tumors• Vandetanib performed best against tumors that
over-expressed VEGFr2• Erlotinib+bexarotene performed best against
tumors that over-expressed cyclin D1

Simpler Approach to Evaluating Treatments Within Pre-specified
Biomarker Strata
• Randomized phase II trial starting with 4 treatment arms
• Evaluate outcome for each treatment in each of 4 biomarker strata separately using an optimal two-stage design– Tumor control at 8 weeks is considered
response

Optimal Two-Stage Phase II Design for Each Regimen in Each Marker Stratum
=0.10 =0.10
Null response
probability
Desirable response
probability
Stop early if r1
responses in n1
patients
Reject drug if r
responses in n
patients
Average sample
size
Probability of early
stopping
Probability of correct selection
p0 P1r1/n1 r/n EN(p0) PET(p0) PCS
K=4 arms
0.30 0.60 2/8 8/20 13.4 0.55 0.89

• Expected sample size with one treatment effective in each of 4 strata– 4*(3*13.4 + 1*20) = 240 patients
• At end of trial, compare treatment arms with regard to disease control at 8 weeks
• Other possible simplifications– Use diagnostic biopsy for assaying candidate
biomarkers

Conclusions
• The purpose of phase II trials is to decide what phase III trials to do and how to do them
• Phase II trials should not serve as the basis for medical practice (except in unusual circumstances)
• The design and analysis of phase II trials can be less restrictive and more exploratory than for phase III trials

Conclusions• If phase II trials were accurate predictors of
phase III results there would be no need for phase III trials
• Phase II trials can be used to exclude clearly unpromising regimens and to screen for large anti-tumor effects in genomically defined sub-populations
• Making phase II trials very large with phase III endpoints is not an effective screening strategy– Such trials might best be designed as seamless
phase II/III designs

Conclusions• Randomized phase II screening trials are useful
for controlling inter-study variation in patient selection and response assessment– Multiple new treatments with or without control arm– One new treatment with control arm– Control may serve as common reference to calibrate
the activity of the new regimen for comparison across trials
– Small randomized trials are often no more effective than small single arm trials for identifying treatments with moderate effects

Conclusions
• Single arm phase II trials are efficient and interpretable for – screening single agents for activity– for identifying genomically characterized
subsets where anti-tumor activity is maximized
– when historical databases are available and inter-study variability in response or disease control is accounted for by known prognostic factors

Conclusions
• Phase II trials should evaluate candidate biomarkers and seek genomically defined subsets of patients whose tumors appear sensitive to the new drug
• Phase II trials of combinations of molecularly targeted agents are essential