Embed Size (px)
Citation preview

ADRENOCORTICAL
HORMONES
DR ASMA JABEEN

Learning Objectives
By the end of lecture, the students should be able to:
• Describe the functional anatomy of adrenal gland• Describe the functions of mineralocorticoids.• Describe the regulation of mineralocorticoids.• Discuss the functions of glucocorticoids• Describe the effects of abnormal secretion of corticosteroids

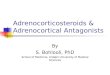
The Adrenal Gland

▪15 % of adrenal cortex
▪ Secretes aldosterone
Zona Fasciculata :
▪Widest layer, 75 %
▪ Secretes glucocorticoids ,
cortisol and corticosterone,
androgens and estrogens
Zona glomerulosa
Zona Reticularis:
▪Adrenal androgens , DHEA and
androstenedione
▪ Small amount of estrogens
and some glucocorticoids

Cortical hormones
➢ Mineralocorticoids
➢ Glucocorticoids
➢ Androgens
Medullary hormones
➢ Epinephrine
➢ Nor epinephrine
Adrenal Hormones

Synthesis of Adrenal steroids
▪ 80% of cholesterol is provided by low
density lipoproteins (LDL) in the plasma
▪ LDL receptors in coated pits on adrenocortical
cell membrane - internalization- release of
cholesterol
▪ ACTH increases the no. of LDH receptors &
enzymes

General features
▪ These are steroids derived from
cholesterol
▪ 90 to 95% 0f cortisol bound to plasma
protein transcortin → long half life of 60 to
90 min
▪ 60% of aldosterone bound to plasma
proteins → half life of 20 min
▪ Adrenocortical hormones are metabolized
in the liver

Mineralocorticoids - Aldosterone

Mechanism of action of aldosterone

Functions of the Mineralocorticoids-
Aldosterone
Increased tubular reabsorption of sodium
and secretion of potassium
▪ Main effect is on PRINCIPAL CELLS of
renal tubules causing sodium
conservation in ECF ,increasing
potassium excretion in the urine

Effects of excess aldosterone
➢ Increased extracellular fluid volume and
arterial pressure
➢ Hypokalemia and muscle weakness
➢ Increased tubular hydrogen ion secretion
leading to mild alkalosis

1. Increased extracellular fluid volume
and arterial pressure
▪ Aldosterone decreases the rate of sodium
excretion by kidneys but conc. of sodium
rises only a few meq.
▪ Aldosterone mediated increase of ECF for
more than 2 days → increased arterial
pressure

▪ The rise in arterial pressure increases
kidney excretion of both salt and water
despite excess aldosterone by pressure
natriuresis and pressure diuresis.
▪ These mechanisms return the renal
output of salt and water to normal despite
excess aldosterone. Mechanism is
called aldosterone escape.


2. Hypokalemia and muscle weakness
Excess aldosterone
Loss of potassium
in urine
Transport of K
from ECF to ICF
Alteration in electrical excitability of
nerve and muscle → muscle weakness

Deficient aldosterone
Potassium in ECF above normal
Cardiac toxicity
Heart failure

3. Tubular secretion of hydrogen and
mild alkalosis
➢ Aldosterone causes secretion of
hydrogen ions in exchange for sodium
in intercalated cells of renal cortical
collecting tubules
➢ Decreased hydrogen ions in ECF →
mild alkalosis

▪ Aldosterone increases the reabsorption
of sodium and secretion of potassium by
the ducts of salivary glands and sweat
glands.
▪ It enhances the sodium reabsorption by
the intestines preventing loss of sodium
in stools.

▪ Total loss of Adrenocortical secretion
causes death within 3 days to 2 weeks
▪ Aldosterone is called the Life saving
portion of adrenocortical hormones. Its
administration can reverse the condition

Regulation of Aldosterone Secretion
The regulation is independent of the
regulation of cortisol and androgen .
❑ Increased potassium ion conc. in ECF
❑ Increased Angiotensin II conc, in ECF
❑ Decreased Sodium ion conc. in ECF
❑ ACTH from anterior pituitary


Glucocorticoids- Cortisol

FUNCTIONS OF GLUCOCORTICOIDS
▪ 95% of glucocorticoid activity is by
cortisol ( hydrocortisone)
▪ Metabolic functions → glucose, fats and
carbohydrates
▪ Role of cortisol in stress and inflammation
▪ Permissive action of cortisol

Effects of cortisol on carbohydrate
metabolism
Stimulation of Gluconeogenesis:
Formation of carbohydrates from proteins
and other substances by the liver.
▪ Increase in enzymes required to convert
amino acids into glucose in the liver cells.
( Activation of DNA transcription)

▪ Mobilization of amino acids from
extra hepatic tissues mainly from muscles.
▪ Increased gluconeogenesis causes marked
increase in glycogen storage in the liver cells .

Decreased glucose utilization by the cells:
▪ Moderate decrease in rate of glucose utilization
by most cells of the body .
▪ Decreased translocation of GLUT 4 to the cell
membrane-Insulin resistance in sk.muscles
▪ Reduced expression of Insulin receptor substrate-1
& phosphatidylinositol
▪ Decreased oxidation of NADH to form NAD,
required to allow glycolysis.
▪ Adrenal diabetes & insulin resistance

Effects of Cortisol on Protein metabolism
Reduction in cellular proteins:
▪ Reduction of protein stores in all body
Cells except liver.
▪ ↓ amino acid transport into extra hepatic
cells ( muscle and lymphoid tissue) →
↓ protein synthesis and ↑ protein
catabolism
▪ Increased blood amino acids

Increase of liver and plasma proteins:
▪ Cortisol increases amino acid transport into liver
cells and enhance the liver enzymes required for
protein synthesis- more plasma proteins
▪


Effects of Cortisol on Fat metabolism
Mobilization of fatty acids:
▪ Promotes fatty acid mobilization from adipose
tissue, increased fatty acids in blood and
increased utilization of fatty acids for energy.
▪ α- glycerophosphate derived from glucose
is required for deposition and maintenance
of TGs in the cells.

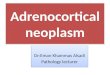
A peculiar type of obesityin peoplewith excess cortisol

Permissive action of Cortisol:
Small amounts of glucocorticoids must
be present for a number of metabolic
reactions to occur, although they do not
produce the reactions themselves. This
effect is called their permissive action.
e.g for glucagon and catecholamines for
their calorigenic, lipolytic and pressor
responses.

Role of cortisol in Stress
➢ Stress causes immediate and marked ↑
in ACTH followed within minutes by
increased cortisol levels.
➢ Glucocorticoids mobilizes fats and amino
acids from their cellular stores and make
them immediately available for energy.


Role of cortisol in inflammation
▪ Cortisol blocks the early stages of
inflammation even before inflammation
begins.
▪ If inflammation has begun, it causes
rapid resolution of inflammation and
cause rapid healing.

Effect of cortisol on blood cells:
• Excess cortisol causes polycythemia
• Eosinopenia
• Atrophy of lymphoid tissue → ↓ T cells
and antibodies → ↓ immunity for all
foreign invaders of the body


Regulation of Cortisol Secretion



Circadian rhythm of glucocorticoid Secretion

Adrenal Androgens
▪ Moderately active male hormones-
Dehydroepiandrosterone
Contribute in:
• Early development of sex organs in males
• Growth of pubic and axillary hair in females

ADDISON’s DISEASE
(Primary adrenal insufficiency)
It results from the failure of adrenal
cortices to produce adrenocortical hormones.
Causes
▪ Primary atrophy of the adrenal cortices
caused by autoimmunity
▪ Tuberculous destruction
▪ Cancer

Secondary adrenal insufficiency
Secondary to impaired function of pituitary gland
which fails to produce sufficient ACTH.

Mineralocorticoid deficiency::
➢ Hyponatremia, hyperkalemia and
mild acidosis
➢ ↓ plasma volume ,↑ RBC conc.
➢ ↓ cardiac output and shock

Glucocorticoid deficiency:
➢ Inability to maintain normal blood glucose
conc. between meals due to ↓ gluconeogenesis
➢ ↓ mobilization of fats and proteins →
sluggishness of energy mobilization
➢ ↑ susceptibility to infection/ stress

Melanin pigmentation:
➢ Blotches of melanin pigmentation
➢ Negative feedback effect → ↑ ACTH
↑ MSH → Stimulation of melanin
pigmentation by melanocytes.
Addisonian crisis:
An acute need of excessive amount of
glucocorticoids in stress, trauma or disease
and associated severe debility is called
addisonian crisis.


Cushing’s Syndrome
A clinical condition produced by prolonged
increase in plasma glucocorticoids
It was described by Harvey Cushing.
❑ ACTH - Independent CS
❑ ACTH – Dependent CS
It can also occur after prolonged treatment with
Glucocorticoids in chronic inflammatory conditions

Causes of ACTH- independent Cushing’s
Syndrome:
▪ 20 to 25% cases
▪ Glucocorticoid secreting adrenal tumors
▪ Adrenal hyperplasia
▪ Prolonged administration of exogenous
glucocorticoids

Causes of ACTH dependant Cushing’s
Syndrome:
▪ ACTH secreting tumors of anterior
pituitary gland (Cushing’s Disease)
▪ Excessive secretion of CRH from hypothalamus
▪ Ectopic ACTH secretion from some carcinomas

Effects on carbohydrate metabolism:
➢ Increased blood glucose levels
(200mg/dl) after meals
➢ Increased gluconeogenesis
➢ Decreased glucose utilization by the
cells

Effects on protein metabolism:
➢ Decreased proteins -with the exception of liver
and plasma proteins.
➢ Loss of proteins from muscles
➢ Loss of protein synthesis from lymphoid
tissues → suppressed immune system
➢ ↓ protein collagen fibers in subcutaneous
tissue → large purplish striae
➢ Osteoporosis

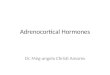
Redistribution of body fat
▪Buffalo torso or buffalo
hump
▪ Moon face
▪ Lemon on match
sticks


Cushing’s syndrome

Dexamethasone Test:
This test is done to distinguish between
ACTH- dependant and ACTH- independent
Cushing’s syndrome.
Treatment of cushing’s syndrome:▪ Surgery for removal of pituitary tumor
▪ Drugs
▪ Partial or total adrenalectomy


Primary Aldosteronism
(Conn’s Syndrome)
Tumor of zona glomerulosa secreting
large amounts of aldosterone results in
primary aldosteronism or conn’s syndrome

Adrenogenital Syndrome
Excessive production of androgens by an
adrenocortical tumor causing:
• Early masculinizing effects in male child
throughout the body.
• Masculinizing effects in female

THANK YOU