Embed Size (px)
Citation preview
Adjustments in Hepatitis C Infection
Adjustments in Hepatitis C Infection
Roger A Wong BSc MRCPsychBrownlee Centre, Glasgow
Roger A Wong BSc MRCPsychBrownlee Centre, Glasgow
Psychiatric symptoms among clients seeking treatment for drug dependence. Intake data from the National
Treatment Outcome Research Study
J Marsden et al. National Addiction Centre, London
Psychiatric symptoms among clients seeking treatment for drug dependence. Intake data from the National
Treatment Outcome Research Study
J Marsden et al. National Addiction Centre, London
Marsden J British Journal of Psychiatry 2000Marsden J British Journal of Psychiatry 2000
• 1075 drug users in UK
• Heroin use 87%
• Brief Symptom Inventory
• 1075 drug users in UK
• Heroin use 87%
• Brief Symptom Inventory

• Anxiety 32.3%
• Depression 29.7%
• Psychiatric treatment in last 2 years 20%
• Suicidal thoughts in last 3 months 29%
• Anxiety 32.3%
• Depression 29.7%
• Psychiatric treatment in last 2 years 20%
• Suicidal thoughts in last 3 months 29%
National Veterans Affairs Database
1.9 million veterans admitted to hospital in USA between 1992 - 1999
Hepatitis C infection 33,824 (1.8%)
National Veterans Affairs Database
1.9 million veterans admitted to hospital in USA between 1992 - 1999
Hepatitis C infection 33,824 (1.8%)
El-Serag, Gastroenterology 2002;123El-Serag, Gastroenterology 2002;123
• Psychiatric or substance misuse 86%
• Opiate use 48%
• Inpatient care for psychiatric or drug misuse disorder 31%
• Psychiatric or substance misuse 86%
• Opiate use 48%
• Inpatient care for psychiatric or drug misuse disorder 31%
• Substance use with other psychiatric co-morbidity 16,828 50%
• Depression 14,210 42%
• Anxiety 11,946 35%
• Substance use without other psychiatric comorbidity 10,286 30%
• Substance use with other psychiatric co-morbidity 16,828 50%
• Depression 14,210 42%
• Anxiety 11,946 35%
• Substance use without other psychiatric comorbidity 10,286 30%
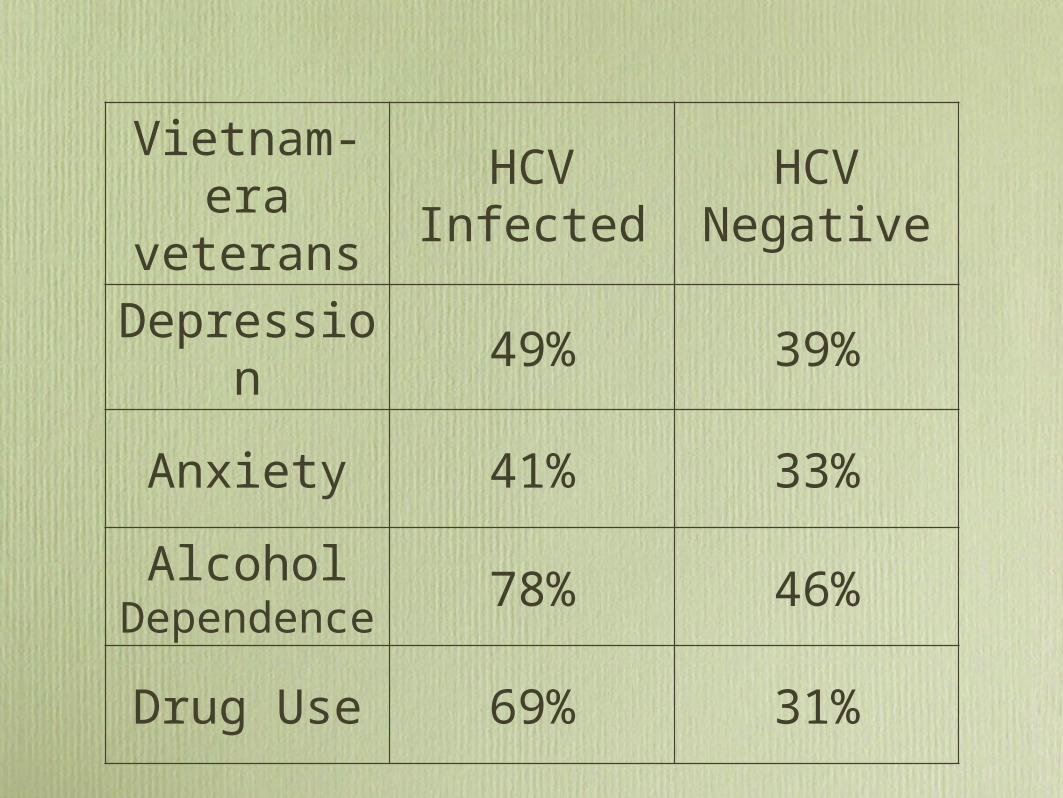
Vietnam-era
veterans
HCV Infected
HCV Negative
Depression
49% 39%
Anxiety 41% 33%Alcohol
Dependence
78% 46%
Drug Use 69% 31%

“A study to determine the extent of psychological morbidity occurring in persons with a diagnosis of Hepatitis C virus infection, attending a specialist
outpatient clinic.”
“A study to determine the extent of psychological morbidity occurring in persons with a diagnosis of Hepatitis C virus infection, attending a specialist
outpatient clinic.”
J. Fraser, Master of Public Health Degree, University of Glasgow 1998J. Fraser, Master of Public Health Degree, University of Glasgow 1998

• Psychological Morbidity 60%
• Depression 27%
• Previous psychiatric history 50%
• Psychiatric treatment within last year 41%
• Psychological Morbidity 60%
• Depression 27%
• Previous psychiatric history 50%
• Psychiatric treatment within last year 41%
Because of the potential implications of a positive diagnosis of hepatitis C virus infection (including the knowledge that it can cause a chronic disease from which the person can develop long term symptoms, with the risk of death in a minority), all tests should be preceded by careful information and advice so that the implications of the testing are clearly understood. It is very important to recognise the anxiety this subject can create for the drug user. Those drug users who seek testing should be offered well-informed advice, and be made aware of the implications of both a positive result and of a negative result, to provide a basis for giving informed consent.
Because of the potential implications of a positive diagnosis of hepatitis C virus infection (including the knowledge that it can cause a chronic disease from which the person can develop long term symptoms, with the risk of death in a minority), all tests should be preceded by careful information and advice so that the implications of the testing are clearly understood. It is very important to recognise the anxiety this subject can create for the drug user. Those drug users who seek testing should be offered well-informed advice, and be made aware of the implications of both a positive result and of a negative result, to provide a basis for giving informed consent.
Those drug users who seek testing should be offered well-informed advice, and be made aware of the implications of both a positive result and of a negative result, to provide a basis for giving informed consent. A wide range of health professionals in both primary and specialist substance misuse services are appropriate to deliver hepatitis C antibody pre- and post-test information, advice and discussion, as well as arranging onward assessment and care for those with positive results.
Those drug users who seek testing should be offered well-informed advice, and be made aware of the implications of both a positive result and of a negative result, to provide a basis for giving informed consent. A wide range of health professionals in both primary and specialist substance misuse services are appropriate to deliver hepatitis C antibody pre- and post-test information, advice and discussion, as well as arranging onward assessment and care for those with positive results.

“You must obtain consent from patients before testing for a serious communicable disease,...”
“The information you provide when seeking consent should be appropriate to the circumstances and to the nature of the condition or conditions being tested for.”...”you must make sure that the patient is given appropriate information about the implications of the test, and appropriate time to consider and discuss them.”
“You must obtain consent from patients before testing for a serious communicable disease,...”
“The information you provide when seeking consent should be appropriate to the circumstances and to the nature of the condition or conditions being tested for.”...”you must make sure that the patient is given appropriate information about the implications of the test, and appropriate time to consider and discuss them.”
Pre-Test Discussion in Hepatitis C Screening
Pre-Test Discussion in Hepatitis C Screening
• Obtain informed consent
• Explain possible test results
• Prepare for possible positive result
• Advise on reducing risks of transmission
• Obtain informed consent
• Explain possible test results
• Prepare for possible positive result
• Advise on reducing risks of transmission
Post-Test Discussion in Hepatitis C Screening
Post-Test Discussion in Hepatitis C Screening
• Communicate result clearly
• Explain implications of result
• Identify relevant issues for follow-up/referral
• Advise on reducing risks of transmission
• Communicate result clearly
• Explain implications of result
• Identify relevant issues for follow-up/referral
• Advise on reducing risks of transmission

Identified Psychological and Social Problems in Hepatitis C Antibody
Positive Clients
Identified Psychological and Social Problems in Hepatitis C Antibody
Positive Clients
• Poor self-image/confidence 58%
• Information on Hepatitis C 52%
• “Coming to terms with the condition” 47.5%
• Transmission 46.5%
• Family/relationship difficulties 43.75%
• Poor self-image/confidence 58%
• Information on Hepatitis C 52%
• “Coming to terms with the condition” 47.5%
• Transmission 46.5%
• Family/relationship difficulties 43.75%
Audit of referrals to V. Lynch, Hep C Counsellor, Brownlee Centre 1999 unpublishedAudit of referrals to V. Lynch, Hep C Counsellor, Brownlee Centre 1999 unpublished
Identified Psychological and Social Problems in Hepatitis C Antibody
Positive Clients
Identified Psychological and Social Problems in Hepatitis C Antibody
Positive Clients
• Substance misuse alcohol/drugs 40%
• Mood swings 33.75%
• Bouts of depression/depressed 30%
• Former IVDU 27.5%
• General fatigue/apathy 27%
• Substance misuse alcohol/drugs 40%
• Mood swings 33.75%
• Bouts of depression/depressed 30%
• Former IVDU 27.5%
• General fatigue/apathy 27%

Identified Psychological and Social Problems in Hepatitis C Antibody
Positive Clients
Identified Psychological and Social Problems in Hepatitis C Antibody
Positive Clients
• Suicidal thoughts 22.5%
• Social isolation 22%
• Housing problems 16.5%
• Attempted suicide/self-harm 9.5%
• Coping with treatment 6.25%
• Suicidal thoughts 22.5%
• Social isolation 22%
• Housing problems 16.5%
• Attempted suicide/self-harm 9.5%
• Coping with treatment 6.25%
Neuropsychiatric Side Effects of Interferon-α
Therapy
Neuropsychiatric Side Effects of Interferon-α
Therapy
• Irritability
• Depression
• Insomnia
• Mania
• Suicide
• Irritability
• Depression
• Insomnia
• Mania
• Suicide
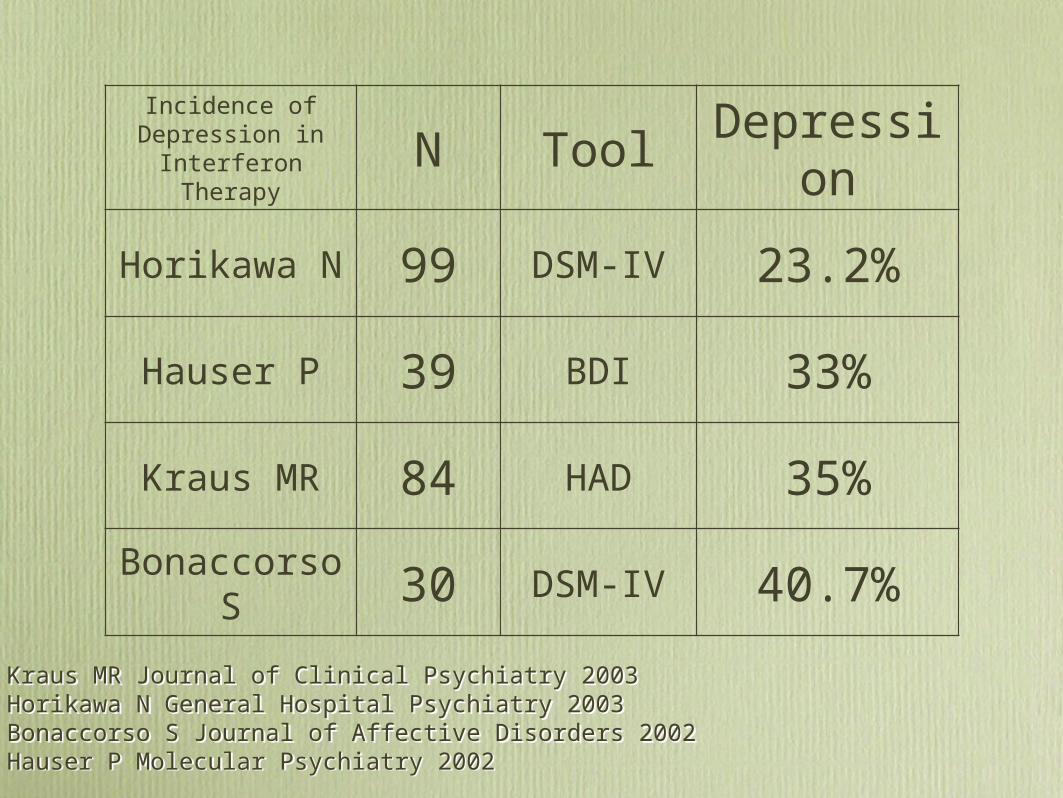
Incidence of Depression in
Interferon TherapyN Tool
Depression
Horikawa N 99 DSM-IV 23.2%
Hauser P 39 BDI 33%
Kraus MR 84 HAD 35%
Bonaccorso S 30 DSM-IV 40.7%
Kraus MR Journal of Clinical Psychiatry 2003Horikawa N General Hospital Psychiatry 2003Bonaccorso S Journal of Affective Disorders 2002Hauser P Molecular Psychiatry 2002
Kraus MR Journal of Clinical Psychiatry 2003Horikawa N General Hospital Psychiatry 2003Bonaccorso S Journal of Affective Disorders 2002Hauser P Molecular Psychiatry 2002

Commonest Cause of Drop Out from Interferon Treatment for Hepatitis C
Neuropsychiatric Side Effects
Commonest Cause of Drop Out from Interferon Treatment for Hepatitis C
Neuropsychiatric Side Effects

• Baseline psychiatric assessment
• Pre-treatment information, advice and support
• On-treatment monitoring and support
• Managing neuropsychiatric side effects
• Baseline psychiatric assessment
• Pre-treatment information, advice and support
• On-treatment monitoring and support
• Managing neuropsychiatric side effects
DieteticsBBV Specialist NursingOccupational Therapy
PharmacyPsychiatry & Counselling
PhysiotherapySexual HealthSocial Work
DieteticsBBV Specialist NursingOccupational Therapy
PharmacyPsychiatry & Counselling
PhysiotherapySexual HealthSocial Work
• Nurse-led Interferon Clinic
• Routine mood screening
• Clinical psychiatric assessment
• Nurse-led Interferon Clinic
• Routine mood screening
• Clinical psychiatric assessment

A Systematic Guide for the Management of Depression in Primary Care
DSM-IV criteria
Major depression is:
Over the last 2 weeks five of the following features should be present of which one or more should be:
1. depressed mood most of the day nearly every day 2. loss of interest or pleasure in almost all activities most of the day nearly every day
and the remaining (the total to make at least five) from any of the following:
3. significant weight loss or gain (more than 5% change in 1 month) or an increase or decrease in appetite nearly every day 4. insomnia or hypersomnia nearly every day 5. psychomotor agitation or retardation nearly every day (observable by others, not merely subjective feelings of restlessness or being slowed down) 6. fatigue or loss of energy nearly every day 7. feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day (not merely self reproach about being sick) 8. diminished ability to think or concentrate, or indecisiveness, nearly every day (either by subjective account or observation of others) 9. recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan or a suicide attempt or a specific plan for committing suicide.
And the symptoms cause clinically significant distress or impairment in occupational or other "important areas of functioning.
BUT
It cannot be established that an organic factor initiated and maintained the disturbance . The disturbance is not a normal reaction to the death of a loved one (morbid preoccupation with worthlessness, suicidal ideation, marked functional impairment or psychomotor retardation, or prolonged duration suggest bereavement complicated by major depression)At no time during the disturbance have there been delusions or hallucinations for as long as two weeks in the absence of prominent mood symptoms (i.e. before the mood symptoms developed or after they have remitted).Not super imposed on schizophrenia, schizophreniform disorder, delusional disorder or psychotic disorder not superimposed on schizophrenia.
A Systematic Guide for the Management of Depression in Primary Care
DSM-IV criteria
Major depression is:
Over the last 2 weeks five of the following features should be present of which one or more should be:
1. depressed mood most of the day nearly every day 2. loss of interest or pleasure in almost all activities most of the day nearly every day
and the remaining (the total to make at least five) from any of the following:
3. significant weight loss or gain (more than 5% change in 1 month) or an increase or decrease in appetite nearly every day 4. insomnia or hypersomnia nearly every day 5. psychomotor agitation or retardation nearly every day (observable by others, not merely subjective feelings of restlessness or being slowed down) 6. fatigue or loss of energy nearly every day 7. feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day (not merely self reproach about being sick) 8. diminished ability to think or concentrate, or indecisiveness, nearly every day (either by subjective account or observation of others) 9. recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan or a suicide attempt or a specific plan for committing suicide.
And the symptoms cause clinically significant distress or impairment in occupational or other "important areas of functioning.
BUT
It cannot be established that an organic factor initiated and maintained the disturbance . The disturbance is not a normal reaction to the death of a loved one (morbid preoccupation with worthlessness, suicidal ideation, marked functional impairment or psychomotor retardation, or prolonged duration suggest bereavement complicated by major depression)At no time during the disturbance have there been delusions or hallucinations for as long as two weeks in the absence of prominent mood symptoms (i.e. before the mood symptoms developed or after they have remitted).Not super imposed on schizophrenia, schizophreniform disorder, delusional disorder or psychotic disorder not superimposed on schizophrenia.
Management of the Neuropsychiatric Side Effects of
Interferon Therapy
Management of the Neuropsychiatric Side Effects of
Interferon Therapy
• Support
• Antidepressant medication
• Hypnotics
• Discontinuation of treatment
• Support
• Antidepressant medication
• Hypnotics
• Discontinuation of treatment
Living with Hepatitis C InfectionLiving with Hepatitis C Infection
• Make informed decisions
• Identify relevant psychosocial and medical issues
• Access appropriate services
• Utilise appropriate help and support
• Make informed decisions
• Identify relevant psychosocial and medical issues
• Access appropriate services
• Utilise appropriate help and support
Managing Hepatitis C InfectionManaging Hepatitis C Infection
• Make informed decisions
• Identify relevant psychosocial and medical issues
• Access appropriate services
• Utilise appropriate help and support
• Make informed decisions
• Identify relevant psychosocial and medical issues
• Access appropriate services
• Utilise appropriate help and support
Enable the individual to:Enable the individual to: