Embed Size (px)
Citation preview

- (2013) 1.e1e1.e3 www.onlinecjc.ca
Canadian Journal of CardiologyCase Report
Adherence to Blood PressureeLowering Drugs andResistant Hypertension: Should Trial of Direct ObservationTherapy Be Part of Preassessment for Renal Denervation?
Marcel Ruzicka, MD, PhD, FRCPC,a,b Brendan McCormick, MD, FRCPC,a
Frans HH. Leenen, MD, PhD, FRCPC,b Michael Froeschl, MD, FRCPC, FACC,b and
Swapnil Hiremath, MD, MPHa,c
aDivision of Nephrology, University of Ottawa, Ottawa, Ontario, CanadabDivision of Cardiology, University of Ottawa Heart Institute, Ottawa, Ontario, Canada
cClinical Epidemiology Program, Ottawa Hospital Research Institute, Ottawa, Ontario, Canada
ABSTRACTRenal denervation (RDN) is increasingly used for resistant hyperten-sion. We report here a case of pseudoresistance of hypertensioncaused by nonadherence to prescribed drug therapy (6 medications),which evaded detection by verification of prescription filling. Directobservation therapy (DOT), in which usual antihypertensive medica-tions are given under supervision, produced substantial reductions inblood pressure, which was subsequently controlled chronically with 3antihypertensive agents, confirming pseudoresistant hypertension. Thenovel teaching points are that evaluation of nonadherence to drugtherapy is a crucial component in diagnosing resistant hypertensionbefore RDN and that DOT may be extremely useful in avoiding anunnecessary and costly procedure.
Received for publication May 27, 2013. Accepted July 10, 2013.
Corresponding author: Dr Marcel Ruzicka, MD, PhD, FRCPC, Divisionof Nephrology, The Ottawa Hospital-Riverside Campus, 1967 Riverside,Ottawa, Ontario, Canada, K1H 7W9. Tel.: þ1-613-798-8400 �82535.
E-mail: [email protected]
0828-282X/$ - see front matter � 2013 Canadian Cardiovascular Society. Publishehttp://dx.doi.org/10.1016/j.cjca.2013.07.678
R�ESUM�ELa d�enervation r�enale (DR) est de plus en plus utilis�ee contre l’hy-pertension r�esistante. Nous pr�esentons ici un cas de pseudor�esistancede l’hypertension caus�ee par la non-observance de la pharma-coth�erapie prescrite (6 m�edicaments), qui n’a pas �et�e d�etect�ee par lav�erification avant la pr�eparation de l’ordonnance. Le traitement sousobservation directe (TOD), au cours duquel les m�edicaments anti-hypertenseurs habituels sont donn�es sous supervision, a permis unebaisse substantielle de la pression art�erielle, qui a �et�e par la suitemaîtris�ee en tout temps par 3 agents antihypertenseurs, confirmantainsi l’hypertension pseudor�esistante. Les nouveaux points à retenirsont que l’�evaluation de la non-observance de la pharmacoth�erapie estune composante cruciale au diagnostic d’hypertension r�esistanteavant la DR et que le TOD peut être extrêmement utile pour �eviter uneintervention non n�ecessaire et coûteuse.
Case PresentationIn August 2012, a 53-year-old woman was referred to the
renal hypertension clinic for assessment for RDN. She hadhad hypertension for more than 20 years, but it was never wellcontrolled. Contributing factors to her hypertension weremorbid obesity (body mass index, 50) and treated obstructivesleep apnea. There was no evidence of target organ damage.She admitted to being unable to comply with dietary inter-ventions, but she assured us of adherence to her antihyper-tensive medications. At the time of her referral, she was taking6 blood pressure (BP)-lowering drugs, as shown in Table 1.Her examination was remarkable only for morbid obesity and
bilateral pitting edema up to her knees. Her BP and heart ratereadings at different time points are shown in Table 1. Toexclude pseudoresistance from nonadherence, filling recordsfor her antihypertensive medications were verified with herpharmacy. She was also asked to do 24-hour ambulatory BPmonitoring (ABPM) to rule out “white coat hypertension.”She could only complete 5 hours of readings for 24-hourABPM, however, because the repeated cuff inflationswere reportedly uncomfortable. Nevertheless, average BP was176/100 mm Hg. She had normal serum electrolyte andserum creatinine levels, and urinalysis and screening testresults for secondary hypertension were negative. She under-went uncomplicated RDN. On day 1 after the procedure, herbody weight was lower by 3 kg and she reported “increasedvoiding.” We noticed significant improvement in her systolicBP (Table 1) but made no changes to her antihypertensivemedications because she still had moderate hypertension. Onweekly follow-up visits during the first 2 weeks after RDN,her weight gradually increased to her pre-RDN weight.
d by Elsevier Inc. All rights reserved.
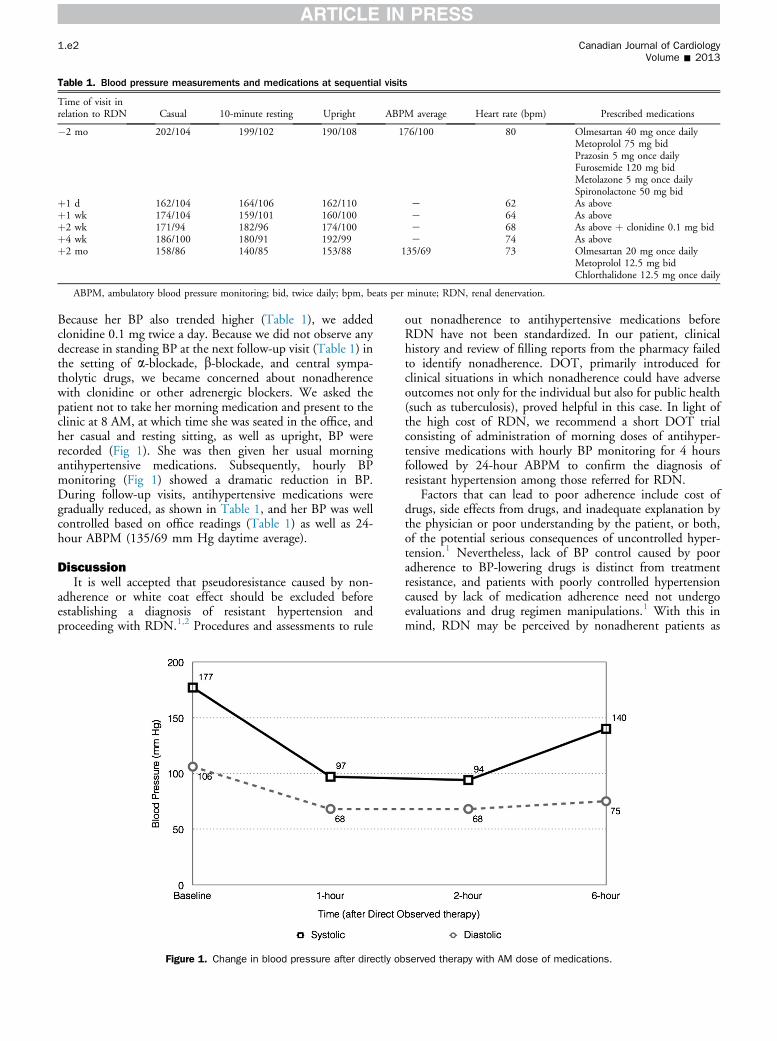
Table 1. Blood pressure measurements and medications at sequential visits
Time of visit inrelation to RDN Casual 10-minute resting Upright ABPM average Heart rate (bpm) Prescribed medications
�2 mo 202/104 199/102 190/108 176/100 80 Olmesartan 40 mg once dailyMetoprolol 75 mg bidPrazosin 5 mg once dailyFurosemide 120 mg bidMetolazone 5 mg once dailySpironolactone 50 mg bid
þ1 d 162/104 164/106 162/110 e 62 As aboveþ1 wk 174/104 159/101 160/100 e 64 As aboveþ2 wk 171/94 182/96 174/100 e 68 As above þ clonidine 0.1 mg bidþ4 wk 186/100 180/91 192/99 e 74 As aboveþ2 mo 158/86 140/85 153/88 135/69 73 Olmesartan 20 mg once daily
Metoprolol 12.5 mg bidChlorthalidone 12.5 mg once daily
ABPM, ambulatory blood pressure monitoring; bid, twice daily; bpm, beats per minute; RDN, renal denervation.
1.e2 Canadian Journal of CardiologyVolume - 2013
Because her BP also trended higher (Table 1), we addedclonidine 0.1 mg twice a day. Because we did not observe anydecrease in standing BP at the next follow-up visit (Table 1) inthe setting of a-blockade, b-blockade, and central sympa-tholytic drugs, we became concerned about nonadherencewith clonidine or other adrenergic blockers. We asked thepatient not to take her morning medication and present to theclinic at 8 AM, at which time she was seated in the office, andher casual and resting sitting, as well as upright, BP wererecorded (Fig 1). She was then given her usual morningantihypertensive medications. Subsequently, hourly BPmonitoring (Fig 1) showed a dramatic reduction in BP.During follow-up visits, antihypertensive medications weregradually reduced, as shown in Table 1, and her BP was wellcontrolled based on office readings (Table 1) as well as 24-hour ABPM (135/69 mm Hg daytime average).
DiscussionIt is well accepted that pseudoresistance caused by non-
adherence or white coat effect should be excluded beforeestablishing a diagnosis of resistant hypertension andproceeding with RDN.1,2 Procedures and assessments to rule
Figure 1. Change in blood pressure after directly ob
out nonadherence to antihypertensive medications beforeRDN have not been standardized. In our patient, clinicalhistory and review of filling reports from the pharmacy failedto identify nonadherence. DOT, primarily introduced forclinical situations in which nonadherence could have adverseoutcomes not only for the individual but also for public health(such as tuberculosis), proved helpful in this case. In light ofthe high cost of RDN, we recommend a short DOT trialconsisting of administration of morning doses of antihyper-tensive medications with hourly BP monitoring for 4 hoursfollowed by 24-hour ABPM to confirm the diagnosis ofresistant hypertension among those referred for RDN.
Factors that can lead to poor adherence include cost ofdrugs, side effects from drugs, and inadequate explanation bythe physician or poor understanding by the patient, or both,of the potential serious consequences of uncontrolled hyper-tension.1 Nevertheless, lack of BP control caused by pooradherence to BP-lowering drugs is distinct from treatmentresistance, and patients with poorly controlled hypertensioncaused by lack of medication adherence need not undergoevaluations and drug regimen manipulations.1 With this inmind, RDN may be perceived by nonadherent patients as
served therapy with AM dose of medications.

Ruzicka et al. 1.e3DOT Test in Diagnosis of Pseudoresistant HTN
a potential “cure” and they may seek the procedure, high-lighting the importance of DOT before RDN. Given thecomplexity of establishing the diagnosis of resistant hyper-tension, the preceding clinical scenario supports the conceptthat a physician with significant clinical expertise in thediagnosis and management of resistant hypertension should bepart of any RDN program.
DisclosuresThe authors have no conflicts of interest to disclose.
References
1. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diag-nosis, evaluation, and treatment: a scientific statement from theAmerican Heart Association Professional Education Committee of theCouncil for High Blood Pressure Research. Circulation 2008;117:510-26.
2. Krum H, Schlaich M, Whitbourn R, et al. Catheter-based renal sympa-thetic denervation for resistant hypertension: a multicentre safety andproof-of-principle cohort study. Lancet 2009;373:1275-81.