Embed Size (px)
Citation preview
Addendum: Pediatrics Review

WHO 2009 Classification
• Dengue without warning signs: Live in/travel to endemic areas Fever and 2 of the ff criteria:1.Nausea, vomiting2.Rash3.Aches & pains4.Tourniquet test positive5.Leukopenia

WHO 2009 Classification
• Dengue with warning signs:1.Abdominal pain or tenderness2.Persistent vomiting3.Clinical fluid accumulation4.Mucosal bleed5.Lethargy, restlessness6.Liver enlargement > 2 cms7. Increase in hct with decrease in platelet

WHO 2009 Classification
• Severe dengue:1.Severe plasma leakage Shock (DSS) Fluid accumulation with respiratory distress
2. Severe bleeding As evaluated by clinician
WHO 2009 Classification
3. Severe organ involvementliver: AST or ALT >1,000CNS: impaired consciousnessHeart and other organs
Dengue Fever
• Dengue NS-1 Ag – Day 1 and Day 4 of the illness
Rickets
• Disease of growing bone which occurs in children only before fusion of the epiphyses
• Due to unmineralized matrix at the growth plates
• Increase in the circumference of the growth plate and the metaphyses --> widening of the wrists & ankles
• General softening of the bones
Rickets
• Craniotabes or softening of the cranial bones
• Widening of the costochondral junctions leads to “rachitic rosary”
• “Harrison groove” is a horizontal depression along the lower anterior chest due to pulling of the softened ribs by the diaphragm during inspiration
La Leche League International
• All milk should be dated before storing. • Preferably, human milk should be refrigerated
or chilled right after it is expressed. • Guidelines for storing human milk:1.At room temperature (19-26 C) for 4 hours
(ideal), up to 6 hours (acceptable)2. In a ref < 4 C for 72 hrs (ideal), up to 8 days
(acceptable)
LLLI
3. In a freezer (-18- -20 C) for 6 months (ideal), up to 12 months (acceptable)
. What type of container should be used?1. Glass or hard-sided plastic containers with
well-fitting tops2. Containers not made with the controversial
chemical bisphenol A (BPA)3. Containers which have been washed in hot,
soapy water, rinsed well, and air-dried

LLLI
4. Containers should not be filled to the top - leave one inch of space to allow for expansion
5. Put only 2-4 ozs of milk in the container to reduce waste.
6. Disposable plastic bags are not recommended as it leads to greater risk of contamination.

How to warm the milk:
1. Do not refreeze thawed milk.2. Previously frozen milk that has been thawed
can be kept in the refrigerator for up to 24 hrs.
3. Frozen milk: thaw in the ref overnight or under cool running water
4. Refrigerated milk: under warm running water for several minutes. Do not heat the milk directly on the stove. Do not use microwave.

Guidelines on Infant & Young Child Feeding
• UNICEF & WHO recommend that infants be exclusively breastfed on demand for the 1st 6 months of life
• Early introduction of food & other liquids?
1.Reduces breast milk intake
2.Decreases full absorption of nutrients from breast milk
3. Increases the risk of diarrhea and URI

Febrile Seizures
Most common seizure disorder in childhoodRare before 9 months and after 5 yrs oldPeak age of onset: 14-18 months oldNormal neurologic examNormal EEG(+) family history

Comparison:
• Simple: Lasts a few secs &
rarely >15 mins. Initially generalized and
tonic-clonic Followed by a brief
period of post-ictal drowsiness
Occurs only once in 24 hrs
• Complex: Duration is >15 mins. Repeated convulsions
occur within 24 hrs Focal seizure activity

Status Epilepticus
• One seizure lasting 30 mins or multiple seizures during 30 mins without regaining consciousness
• Usual cause: breakthrough seizures - missed doses of anti-epileptic drug/s
• May be due to CNS infection
Persistent PulmonaryHypertension of the Newborn
• Failure of the normal circulatory transition that occurs after birth
• Syndrome: marked pulmonary hypertension that causes hypoxemia and right-to-left
extrapulmonary shunting of blood • With inadequate pulmonary perfusion,
neonates are at risk for developing refractory hypoxemia, respiratory distress, and acidosis.

PPHN
• Most common cause is meconium aspiration syndrome
• about 13% of all live births are complicated by meconium-stained fluid but only 5% who had this complication subsequently develop MAS• Coarse streaking granular pattern in both
lung fields• Irregularly aerated lungs
• Flattened diaphragm, increased AP diameter
PPHN
• 2nd most common cause is idiopathic• “black-lung”
• Significant remodeling of pulmonary vasculature with vascular wall thickening and
smooth muscle hyperplasia • Contributory factor: use of NSAIDs during 3rd
trimester leading to constriction of the fetal ductus arteriosus in utero

SMR in BoysSMRStage PUBIC HAIR PENIS TESTES1 None Preadolescent Preadolescent2 Scanty, long, slightly pigmented Slight enlargement Enlarged
scrotum, pink, texture altered
3 Darker, starts to curl, small amount Longer Larger4 Resembles adult type but less in quantity;coarse, curly Larger; glans and breadth increase in size Larger, scrotum
dark5 Adult distribution,spread to medial surface of thighs Adult size Adult size
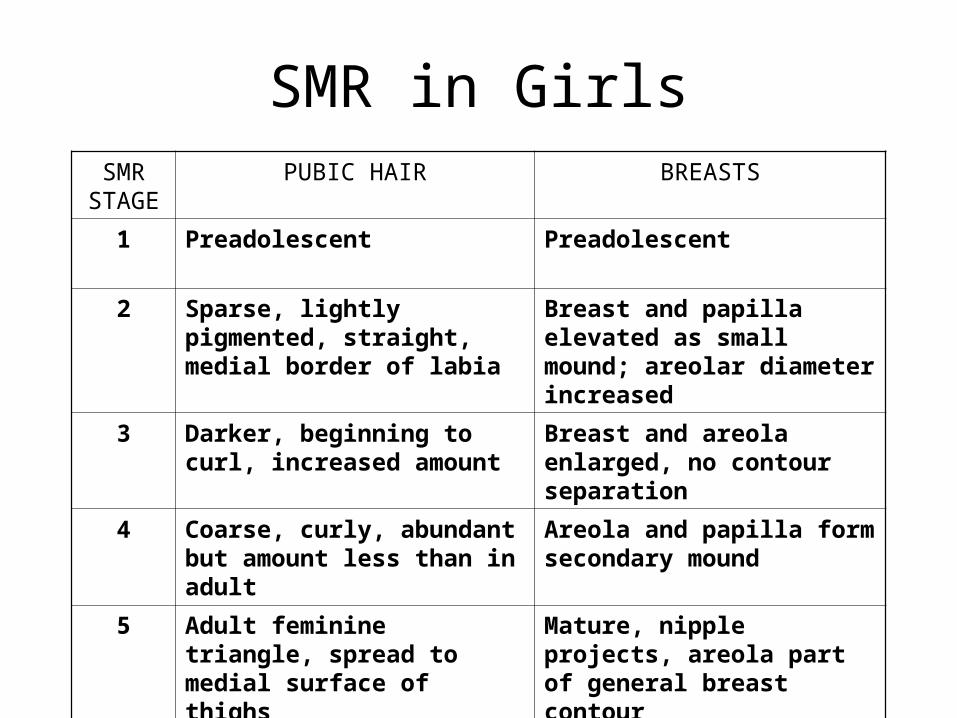
SMR in GirlsSMR
STAGEPUBIC HAIR BREASTS
1 Preadolescent Preadolescent
2 Sparse, lightly pigmented, straight, medial border of labia
Breast and papilla elevated as small mound; areolar diameter increased
3 Darker, beginning to curl, increased amount
Breast and areola enlarged, no contour separation
4 Coarse, curly, abundant but amount less than in adult
Areola and papilla form secondary mound
5 Adult feminine triangle, spread to medial surface of thighs
Mature, nipple projects, areola part of general breast contour
Gross motor skills
• 6 years old – skip
• 8 years old – hop on one foot twice, then the
other
Fine motor skills
• 6 years old- tie shoe laces
• 7 years old- print letters, letter reversal
• 8-10 years old– rapid alternating movement
of the hand, cursive writing
• 10-12 years old – manipulative abilities
similar to adult
Social development
• Expanding social world
• Identification and reliance on peer groups
7 years – attachment to parents decrease
and to peers increase
9 years – tightly knit groups are formed;
group loyalty and commitment to
best friends

Social development 4-5 y/o
• Toilet-trained• Plays imaginary games• Helps in tasks in house• Cooperative group play: takes turns and
shares • Tender and protective• Cooperative most of the time• Chooses own friends
Emotional development4-5 yrs old
Make-believe gamesToy guns are simply an innocent and entertaining way to be competitive and to boost their self-esteem (Shelov, 1994).Interest in basic sexuality May play with their genitals ---- signs of normal curiosity! Do not scold or punish! Be straightforward
Emotional development:4-5 yrs old
• Parents should answer in simple and correct terms.
• Parents should tell their child not to let other person touch the “private parts”.
• Teach your child not to talk to strangers.• Teach child’s name, address, phone if lost.• Normal for a 4 year old to make up stories.• Encourage child to sleep in own bed.





















![Dengue Fever/Severe Dengue Fever/Chikungunya Fever · Dengue fever and severe dengue (dengue hemorrhagic fever [DHF] and dengue shock syndrome [DSS]) are caused by any of four closely](https://img.pdfslide.us/doc/110x75/5e87bf3e7a86e85d3b149cd7/dengue-feversevere-dengue-feverchikungunya-dengue-fever-and-severe-dengue-dengue.jpg)
![European Centre for Disease Prevention and Control - Dengue … · 2019-06-18 · dengue is endemic and who have been infected with DENV before [2]. However, due to an observed increased](https://img.pdfslide.us/doc/110x75/5fae741df617db72355f0f68/european-centre-for-disease-prevention-and-control-dengue-2019-06-18-dengue.jpg)






