Embed Size (px)
Citation preview
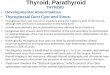
AAdded value of MR and CT to assess Thyroid and parathyroid disease
Surjith Vattoth MD, DNB, FRCR, DABRAssociate Professor of Radiology(Neuroradiology)University of Arkansas for Medical Sciences (UAMS)
Little Rock, AR, USATwitter: @drSurjthVattoth
DDisclosures
• Elsevier Master Author Consultant in Head & Neck Imaging, author Elsevier STATdx, & Imaging Anatomy (IA) and Diagnostic Imaging (DI) books: Royalty
• Many graphics and images used in this presentation from the above-mentioned Elsevier publications
• Acknowledgement: ECHNR course director Dr. Prof. Bernhard Schuknecht for providing many other images used in this presentation
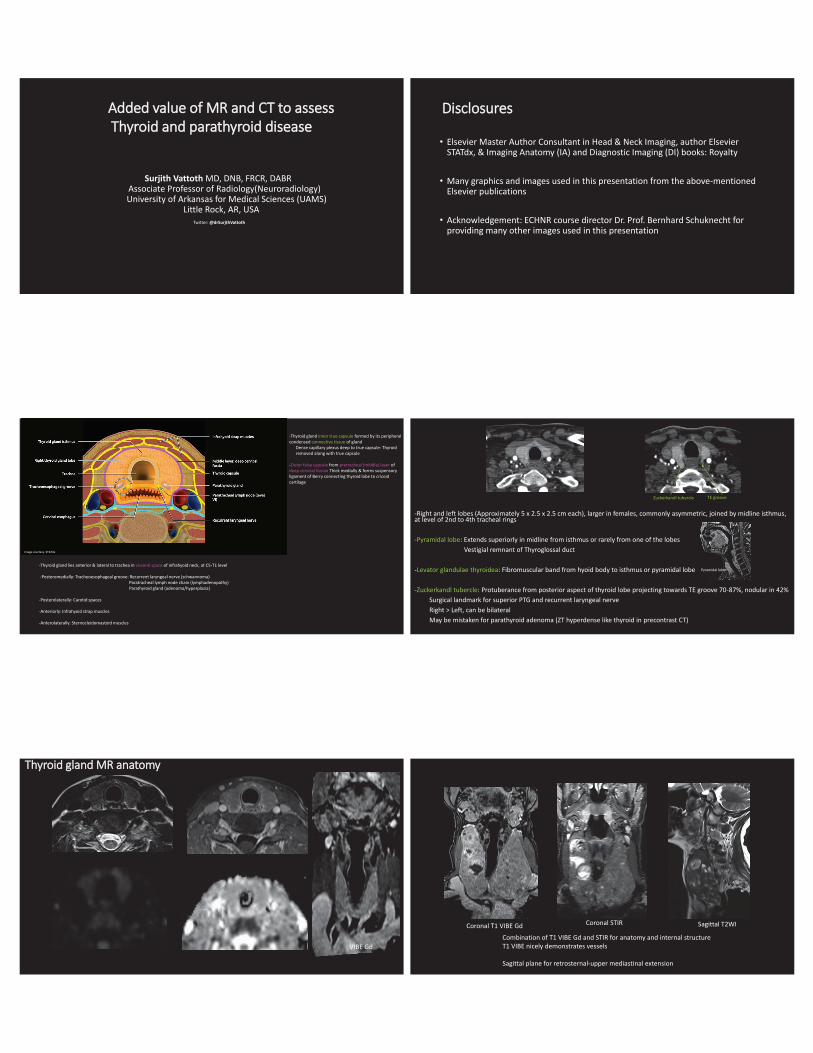
-Thyroid gland lies anterior & lateral to trachea in visceral space of infrahyoid neck, at C5-T1 level
-Posteromedially: Tracheoesophageal groove: Recurrent laryngeal nerve (schwannoma)Paratracheal lymph node chain (lymphadenopathy)Parathyroid gland (adenoma/hyperplasia)
-Posterolaterally: Carotid spaces
-Anteriorly: Infrahyoid strap muscles
-Anterolaterally: Sternocleidomastoid muscles
-Thyroid gland inner true capsule formed by its peripheral condensed connective tissue of gland
Dense capillary plexus deep to true capsule: Thyroid removed along with true capsule
-Outer false capsule from pretracheal (middle) layer of deep cervical fascia: Thick medially & forms suspensory ligament of Berry connecting thyroid lobe to cricoid cartilage
Image courtesy: STATdx
-Right and left lobes (Approximately 5 x 2.5 x 2.5 cm each), larger in females, commonly asymmetric, joined by midline isthmus, at level of 2nd to 4th tracheal rings
-Pyramidal lobe: Extends superiorly in midline from isthmus or rarely from one of the lobesVestigial remnant of Thyroglossal duct
-Levator glandulae thyroidea: Fibromuscular band from hyoid body to isthmus or pyramidal lobe
-Zuckerkandl tubercle: Protuberance from posterior aspect of thyroid lobe projecting towards TE groove 70-87%, nodular in 42%Surgical landmark for superior PTG and recurrent laryngeal nerve Right > Left, can be bilateralMay be mistaken for parathyroid adenoma (ZT hyperdense like thyroid in precontrast CT)
Zuckerkandl tubercle TE groove
Pyramidal lobe
VIBE Gd
TThyroid gland MR anatomy
Combination of T1 VIBE Gd and STIR for anatomy and internal structureT1 VIBE nicely demonstrates vessels
Sagittal plane for retrosternal-upper mediastinal extension
Coronal STIRCoronal T1 VIBE Gd Sagittal T2WI
Retrosternal extension of goiter with right recurrent laryngeal nerve compression/vocal cord palsy
-Superior thyroid arteries: First anterior branch of ECA-Proximal upper part in upper neck closely associated with external (superior) laryngeal nerve
STA ligated CLOSE TO thyroid gland during thyroidectomy to protect external laryngeal nerve
-Anterior branch descends on anterior border of thyroid lobe; sending a branch deep into gland before curving along upper border of isthmus where it anastomoses with contralateral anterior branch
-Posterior branch descends on posterior border of thyroid lobe and anastomose with ascending branch of inferior thyroid artery and supply Parathyroid glands
Anastomosis good guide to Parathyroid glands, usually lie near it
-Inferior thyroid arteries: From Thyrocervical trunk of Subclavian artery
-Ascends vertically, then curves medially to enter TE groove in plane posterior to carotid space
-Most branches penetrate posterior aspect of thyroid lobe; one ascending branch anastomose with superior thyroid artery
-Terminal part near thyroid closely associated with recurrent laryngeal nerve while proximal part in lower neck is away from nerve ITA ligated AWAY FROM thyroid gland during thyroidectomy to protect recurrent laryngeal nerve
-Thyroidea ima artery (3%) – Solitary artery from aortic arch or innominate artery Enters thyroid gland at inferior border of isthmus
3 pairs of veins from venous plexus on thyroid gland surface
Superior & middle thyroid veins drain into internal jugular vein
Inferior thyroid veins end in left brachiocephalic vein
Image courtesy: STATdx Image courtesy: STATdx
-TGD cyst (failure of involution of duct) or thyroid tissue remnants may be found anywhere along its tract from the foramen cecum at tongue base to just anterior to the thyroid lobes
-TGD cysts: 50% at hyoid bone 20%-25% in suprahyoid neck; often in the midline 25% are located in infrahyoid neck; in the midline or paramedian within strap muscles
-Thyroid ectopia-Most common thyroid ectopia: Lingual thyroid at foramen cecum(>90%)
-Defective lateral thyroid component that cannot migrate and fuse with the median thyroid anlage: Submandibular and lateral neck region thyroid ectopia
-Aberrant migration or heterotopic differentiation of uncommitted endodermal cells: Ectopic thyroid tissues in distant locations
-Overdescent of TGD remnants: Mediastinum and subdiaphragmatic locations
-Parthenogenetic development of germ cells into thyroid tissue after failure of these cells to migrate to the genital crest in early embryological development:ectopic thyroid tissue in the genital tract
Image courtesy: STATdx Image courtesy: STATdx
Paramedian thyroglossal duct cysts can mimic second branchial cleft cyst
TGD cyst: Tail “diving” into hyoid
“Claw sign” in strap muscles
TGD cyst has variable T1 and T2 signal depending on thyroglobulin, inflammation, hemorrhage
(Medial anlage: Median endodermal thyroid diverticulum arising from paramedian aspect of 1st & 2nd branchial pouches)
(Lateral anlagen: Lateral thyroid lobes form from 4th branchial pouch)
-Thyroglossal duct carcinoma: 95% papillary thyroid Ca< 5% are squamous cell Ca; more aggressive
- < 2% of TGD cysts harbor carcinoma- Specks of calcification supportive of TGD Ca- Solid components in TGD cyst can be due to prior inflammation- Look for presence/absence of normal thyroid tissue- 65% of TGD cysts have thyroid tissue in the wall microscopically
Lingual thyroid at the base of the tongue/foramen cecum location, with an absent thyroid in the normal thyroid bed in lower neck
-Lingual thyroid is the only functioning thyroid tissue in 75%-Thyroid hormone production can be insufficient with ectopic thyroid gland enlargement-May expand rapidly during puberty-Goiter in ectopic thyroid rarely with obstructive symptoms-Differentiated thyroid carcinoma in lingual thyroid extremely rarely
4th branchial apparatus (pouch) anomaly (4th branchial “cleft” cyst is a misnomer)-Mostly sinus tracts, not cysts, from 4th pharyngeal POUCH remnant-Sinus tract course from apex of pyriform sinus to upper aspect of left thyroid lobe-4th branchial fistula: 2 openings: One in low anterior neck, another into pyriform sinus apex
-Recurrent LEFT thyroiditis/abscess: Embryological asymmetry of 4th branchial arch giving rise to subclavian artery on right and aortic arch on left may be cause of left sidedness-May cause retropharyngeal abscess; vocal cord paralysis if infection extends into TE groove
-CT after Barium/iodinated contrast swallow to look for sinus tract from apex of pyriform sinus to anterior lower neck-Sinus tract may not fill with swallowed contrast if inflamed due to acute infection, or if scarred due to prior infection-Direct iodinated CT contrast injection of fistula best demonstrates its course
-DD: TGD cyst, colloid cyst, 3rd branchial cleft cyst-Note: 3rd branchial cleft cyst can also communicate with pyriform sinus
(Posterior cervical space cyst, can present as a cyst anterior to SCM in the lower neck)
Image courtesy: STATdx

Colloid nodule (cyst): Signal intensity varies: Frequently T1 hyperintense; may be hypo- or isointense
Caution: Hemorrhagic lesion (look for any aggressive features or T2 Low signal- suspect Ca- suggest US)
Image courtesy: STATdx Image courtesy: STATdx
de Quervain Thyroiditis (Subacute granulomatous thyroiditis or Giant cell thyroiditis)
-CECT NOT indicated for diagnosis of thyroiditis: Iodinated contrast may cause falsely decreased iodine uptake on radioiodine scan afterwards
-NECT: Diffusely enlarged edematous thyroid with fuzzy border and low density (around 45 HU) -Normal thyroid gland has a high attenuation (80–100 HU) on NECT because it concentrates iodine around 100x more than serum -In thyroiditis, swollen thyroid has low density, around 45 HU, due to follicular cell destruction and loss of iodine concentration
-CECT shows moderate enhancement indicating inflammatory process-Normal thyroid gland has marked enhancement due to rich vascularity-In thyroiditis, only moderate enhancement of the thyroid gland due to diffuse inflammation
-MR in acute phase shows enlarged thyroid with irregular margins and higher than normal signal intensity on both T1W and T2WI
Image courtesy: Jhaveri K, Shroff MM, Fatterpekar GM, Som PM. CT and MR Imaging Findings Associated with Subacute Thyroiditis. AJNR 2003; 24(1):143-146
T1W MR
T2W MR
NECT CECT
Hashimoto thyroiditis (Chronic lymphocytic thyroiditis)
-CECT: Symmetric enlargement of thyroid unless late stage, atrophic in late stage-Diffusely decreased density typical-No necrosis, cysts, or calcification
-MRI: T1WI: Heterogeneous slightly enlarged glandT2 FS: Increased intensity with lower intensity fibrotic bands may be seen
-Rapid thyroid enlargement with history of Hashimoto thyroiditis: NHL until proven otherwise
NOTE: Low thyroid density in any thyroiditis makes evaluation of Parathyroid adenoma difficult in 4D CT
29-year-old woman after a single gunshot wound to the right lower thorax and upper abdomen
On admission, the thyroid gland demonstrates reduced heterogeneous enhancement with perithyroidal fluid
NECT on day 2 shows normal appearing thyroid with resolution of fluid
CECT on day 7 reveals normal thyroid, with normal enhancement pattern
Brochert A, Rafoth JB. Shock thyroid: A new manifestation of the hypovolemic shock complex in trauma patients. J Comput Assist Tomogr. 2006;30(2):310-2
Shock Thyroid
Thyroid Malignancy
Differentiated thyroid carcinoma • Papillary: 80%, nodal spread
• Follicular: 10%, hematogeneous spread
• Medullary thyroid carcinoma
75-85% sporadic; 15-25% inherited, MEN 2
Anaplastic thyroid carcinomaNecrosis, hemorrhage, 60% calcifications
Non- Hodgkin lymphomaMay follow Hashimoto thyroiditis
CChoice of Imaging Modalities in Thyroid Cancer
• US of thyroid, and neck for lymph node screeningEncapsulated thyroid cancer with no ETE, and no palpable LN
• CE CT/MRILarge thyroid cancer with ETE, clinical symptoms, & palpable lateral LNs
• Post-thyroidectomy/radio-iodine ablation nuclear medicine scanWell differentiated thyroid cancer (papillary/follicular)
• FDG PET-CTPoorly differentiated, or highly aggressive thyroid cancer with suspected distant metastasis
NOTE: With de-differentiation radioiodine scan becomes gradually negative, serum thyroglobulin levels gets elevated, & FDG-PET gets better

TThyroid cancer: What to look for in CT/MRI
• Primary tumor: Look for extrathyroid extension (ETE) violating the thyroid capsule-Tracheoesophageal groove: Direct invasion or lymphadenopathy (secondary vocal cord palsy- recurrent laryngeal nerve)-Hypopharyngeal invasion-Laryngeal invasion-Tracheal invasion-Esophageal invasion-Carotid artery encasement/invasion-IJV invasion
• Lymph nodal metastasis
• Distant metastasis: Lung and Skeleton
(Lung and Renal cell CA are the most common primary cancers metastasizing to thyroid)
Thyroid Lymphatic drainage
-Level VI: Initially to periglandular nodes: Prelaryngeal (Delphian), pretracheal, & paratracheal nodes -Paratracheal nodes drain along recurrent laryngeal nerve into mediastinum
-Regional drainage to Internal jugular chain (levels II-IV) & spinal accessory chain (level V)
-RPLN mets not uncommon in thyroid Ca: Include skull base in evaluation
Image courtesy: STATdx
Papillary thyroid Ca with Tracheoesophageal groove invasion (secondary vocal cord palsy) & Direct laryngeal TVC/FVC invasion
Follicular Ca with Esophagus, Thyroid cartilage & IJV infiltration, and Lung metastasis
AAnaplastic thyroid Ca with Thyroid cartilage and llaryngeal invasion
Windowing 300/100 Soft tissue window width/level
Windowing 1700/600 Cartilage window width/level
-ATC: Stage IV: a-Intrathyroid, b-Extrathyroid, c-Metastases
-50% dedifferentiated from preexisting DTC
- Rapidly enlarging infiltrating mass with necrosis, hemorrhage and lymphadenopathy 50% → distant metastases
AAnaplastic thyroid Ca with Thyroid cartilage and llaryngeal invasion (note wide cricothyroid joint)
Conventional TSE T1Gd FS 3mm
Ax VIBE DIXON Gd MPR 3mm (0.9mm acquisition)

AAnaplastic thyroid Ca with areas of ddiffusion restriction
In Incidental Thyroid Nodules (ITN), we suggest Thyroid Ultrasound if there is low T2 signal or diffusion restriction
-Markers of tumor cellularity
Remember: (Papillary) Thyroid Ca metastatic lymph nodes may be:
-Small (> 1 cm size cut-off criteria may under-call pathological lymph nodes)
-Cystic
-Calcifications
-Retropharyngeal (evaluation should include skull base)
Tuttle RM, Haugen B, Perrier ND. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid. 2017; 27(6):751-756
AJCC 8th edition update has downstaged Thyroid Cancers
Tuttle RM, Haugen B, Perrier ND. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid. 2017; 27(6):751-756
AJCC 8th edition update has downstaged Thyroid Cancers
Radioiodine treatment for hyperthyroidism & thyroid carcinoma: How long to wait after contrast enhanced CT
https://www.acr.org/-/media/ACR/files/clinical-resources/contrast_media.pdf

IIncidental Thyroid Nodules (ITN)-Detected in 16-18% CT/MRI of neck, 1-2% of F18-FDG-PET (20-67% US, 50-60% Autopsy)
-CT chest responsible for the majority of ITNs: Detected in up to 25% CECT chest
-Malignancy: 0-11% of ITN detected on CT/MRI; 33-35% of ITN with FDG-PET uptake; 1.6% of ITNs seen on US (12% in a US biopsy cohort); 36% of ITNs seen at autopsy
-Majority of thyroid cancers in ITN are small PTC, not impacting mortalitySuspicious CT/MRI findings-ACR white paper: Both malignant and benign thyroid nodules can have isointense T1 and hyperintense T2 signals;
Reliable features of benignity or malignancy absent on CT & MRI ?????
The imaging feature that primarily directs further evaluation is nodule size
(-We suggest Thyroid Ultrasound if there is low T2 signal or diffusion restriction
-Markers of tumor cellularity)---------------------------------------------------------------Extrathyroid extension (ETE): Invasion of local tissues by the thyroid nodule--------------------------------------------------------------- When multiple thyroid nodules are present,
size criteria apply to the largest nodule---------------------------------------------------------------Abnormal Lymph Node features: Calcifications, Cystic components, and/or increased Enhancement
- LN enlargement less specific for thyroid cancer metastases
Consider further evaluation if ITN with ipsilateral nodes >1.5 cm in short axis for jugulodigastric LN, and >1 cm for other LNsHoang JK, Langer JE, Middleton WD, et al. Managing Incidental Thyroid Nodules Detected on Imaging: White Paper of the ACR Incidental Thyroid Findings Committee. J Am Coll Radiol 2015;12:143-150
ACR white paper
• ITNs detected on US of extrathyroidal structures• Size criteria according to age < or > 35 yrs, & life expectancy comorbidities same as CT/MR ITNs• Suspicious features: Microcalcifications, marked hypoechogenicity, lobulated or irregular margins, and taller-than-
wide shape on transverse view; refer ACR TI-RADS
• Focal thyroid uptake on FDG-PET• When initial finding is FDG-avid focus on PET, FNA recommended regardless of US findings
• Focal thyroid uptake on other nuclear medicine scans • Like somatostatin analogue evaluation of neuroendocrine tumors: 111 In-octreotide, PET like 68Ga-Dotatate
(medullary Ca thyroid)• Tc-sestamibi
• Both thyroid malignancies and adenomas can have uptake on sestamibi and octreotide scans • 2 small series of selected patients with incidental MIBI-avid thyroid nodules show malignancy rate of 22%- 66% • Do thyroid US for avid nodules on sestamibi and octreotide scans, need for FNA determined by sonographic criteria
PParathyroid imaging
• 4D (triple phase- 4th dimension is time) CT, US, 99m-Tc-Sestamibi scan, 18F-fluorocholine (18F-FCH), 11C-methionine, 18F-FDG, 4D MRI
• Imaging is to localize PT lesions: Anatomical study for patients suitable for surgery like minimally invasive parathyroidectomy (MIP) or uni/bilateral neck exploration (BNE)
• Imaging does not make the hyperparathyroidism diagnosis (serum calcium, PTH, and urine calcium makes the diagnosis)
• Intraoperative PTH monitoring: Success when >50% drop of PTH in anterior or internal jugular vein after 10 minutes-Diseased PT gland dissected free from surrounding tissue, connected only by its blood supply-Selectively cannulate anterior/internal jugular vein with 23G hypodermic needle & collect blood for pre-excision PTH value-Do parathyroidectomy dividing its blood supply connection, wait-After >10 minutes, again selectively cannulate jugular vein, draw blood for post-excision PTH value
• PTH has a very short life span; levels fall by half in less than 5 minutes due to uptake and cleavage in the liver and kidneys
HHyperparathyroidism types
• PT adenoma size/weight and PTH levels dramatically fallen over the years due to correction of Vitamin D deficiency in the population
• Primary hyperparathyroidism: Primary parathyroid gland disease-Majority single adenoma (80%); multigland disease like PT hyperplasia (10%) or multiple adenomas (10%);
rarely PT carcinoma (1%) -High Parathyroid hormone (PTH); & high or high normal serum calcium; high urinary calcium excretion -PT carcinoma has severely elevated PTH, large lesion size, cysts-Beware of Familial hypocalciuric hypercalcemia (FHH): High or high normal serum PTH and calcium;
but low urinary calcium; mutation analysis to confirmMutation inactivates calcium sensitive receptor So PTH less sensitive to calcium
• Secondary hyperparathyroidism: Secondary to disorders like Vit D deficiency or CRF-HighPTH; & low or low normal serum calcium-High PTH is actually appropriate excessive secretion in response to low serum calcium
• Tertiary hyperparathyroidism: When PT glands become autonomous and secrete PTH; in conditions like CRF
• Predictors of Multigland disease (MGD)
-Smaller PT lesion size in 4D CT (size cut-off < 7 mm 85% specific)
- Identification of either multiple PT lesions or no PT lesions on 4D-CT
- Lower Wisconsin Index score (product of serum calcium in mg/dl and parathyroid hormone levels in picog/ml)
Sepahdari AR, Bahl M, Harari A, Kim HJ, Yeh MW, Hoang JK. Predictors of Multigland Disease in Primary Hyperparathyroidism: A Scoring System with 4D-CT Imaging and Biochemical Markers AJNR 2015, 36 (5) 987-992

44D CT Technique
• Mandible to carina (Precontrast: Mandible to clavicular head; OR just the thyroid area)
• 3 phases of scan acquisition: Precontrast, Arterial at 25-30 s, Delayed (venous) at 80-90s
• Time (multiple data points is the 4th dimension)
• May use timing bolus: CRF patient, suboptimal IV access
• IV contrast 4 ml/s, followed by 25-40 ml saline chaser
• 0.625 mm sections sent to PACS, look at up to 2mm thick reconstructions
-Parathyroid glands: 4-6 mm x 3-4 mm x 1-2 mm; 40-50 mg weight
Superior parathyroid glands: Posterior to & close to thyroid, usually within thyroid false capsule or in TE groove -70-75% found on posterior border of middle 1/3 of thyroid gland -20-25% found behind upper or lower 1/3 of thyroid -7% located below inferior thyroid (Dropped Superior PT in TE groove)-Retropharyngeal or retroesophageal (< 2-3% ectopic)-Within scalene fat pad (<1%)-Pyriform sinus (4th branchial pouch gives rise to apex of pyriform sinus)
-Inferior parathyroid glands: More anteriorly and can be more distant-50% located lateral to lower thyroid pole -15% within 1 cm of inferior thyroid poles -25% ectopic along the thyrothymic ligament into superior/lower anterior mediastinum-Within carotid sheath (<1%), intrathyroidal (<1%)-Undescended PT near angle of mandible (near SMG), carotid bifurcation-Embedded in vagus & hypoglossal nerves (3rd branchial pouch contacts the ectodermal structures from which the vagus and hypoglossal nerves arise)
-PTG arterial supply: Inferior thyroid artery and anastomosis between superior & inferior thyroid arteries
-Superior parathyroid glands develop from 4th branchial pouches, along with primordial THYROID; they migrate caudally along the TGD
-Inferior PTG develop from the 3rd branchial pouches along with anlage of THYMUSmigrate caudally along the THYMOPHARYNGEAL DUCT and may descend into anterior mediastinum
Branchial apparatus at end of 4th
week of embryonic life:
-6 arches (mesoderm) interfaced by
-4 clefts (ectoderm) and pouches (endoderm) on each side
[Fifth arch is rudimentary, not contributing to adult structures]
Image courtesy: STATdx Image courtesy: STATdx
Perrier ND, Edeiken B, Nunez R, Gayed I, Jimenez C, Busaidy N, Potylchansky E, Kee S, Vu T. A novel nomenclature to classify parathyroid adenomas. World J Surg. 2009;33(3):412-6
Inferior
Posterior/Lateral
-Superior PT glands consistently lie posterior to the recurrent laryngeal nerve (RLN)
-Inferior PT glands lie anterior to RLN
Bunch PM, Randolph GW, Brooks JA, George V, Cannon J, Kelly H. Parathyroid 4D CT: What the Surgeon Wants to Know. RadioGraphics 2020 40:5, 1383-1394
-4 PT glands usually - 2 Superior, 2 inferior->4 PT glands in 3-5%-<4 PT glands in 3%
-PT adenoma mean weight 1 g
Usually expect Ectopic Parathyroid glands between Hyoid bone and Aortic arch, but may be further up near mandibleCan be retropharyngeal or retroesophageal: Superior PTExtremely rarely near SMG: Inferior PT
A. Superior PT adherent to posterior thyroid parenchyma -A, B, and C glands are posterior & lateral to RLN
-D glands are immediately near RLN
-E and F glands are anterior & medial to RLN
B. Superior PT posterior to thyroid parenchyma in TE groove
B+ gland : Undescended Inferior PT high in neck near mandible or carotid bifurcation
C. Superior PT at level of lower pole of thyroid or further inferior to lower pole of thyroid (closer to the clavicle)in TE groove ; “DROPPED SUPERIOR PT”
D. Can be Superior or Inferior PT based on inferior thyroid artery
-At mid-posterior surface of thyroid parenchyma, near the junction of RLN & inferior thyroid artery or middle thyroidal vein
E. Inferior PT close to lower pole of thyroid parenchyma, lying nearanterior half of the trachea-(Most externally located PT: Easy to resect)-May be around anterior thyroid surface
F. Inferior PT gland has fallen into the thyrothymic ligamentEctopic within or near superior mediastinum, anterior to trachea & posterior to strap muscles
G.-Intrathyroid PT glands: Predictable locations90% in Lower Lateral quadrant7% near RLN & 3% at Superior pole
Bahl M, Sepahdari AR, Sosa JA, Hoang JK. Parathyroid Adenomas and Hyperplasia on Four-dimensional CT Scans: Three Patterns of Enhancement Relative to the Thyroid Gland Justify a Three-Phase Protocol. Radiology. 2015;277(2):454-62
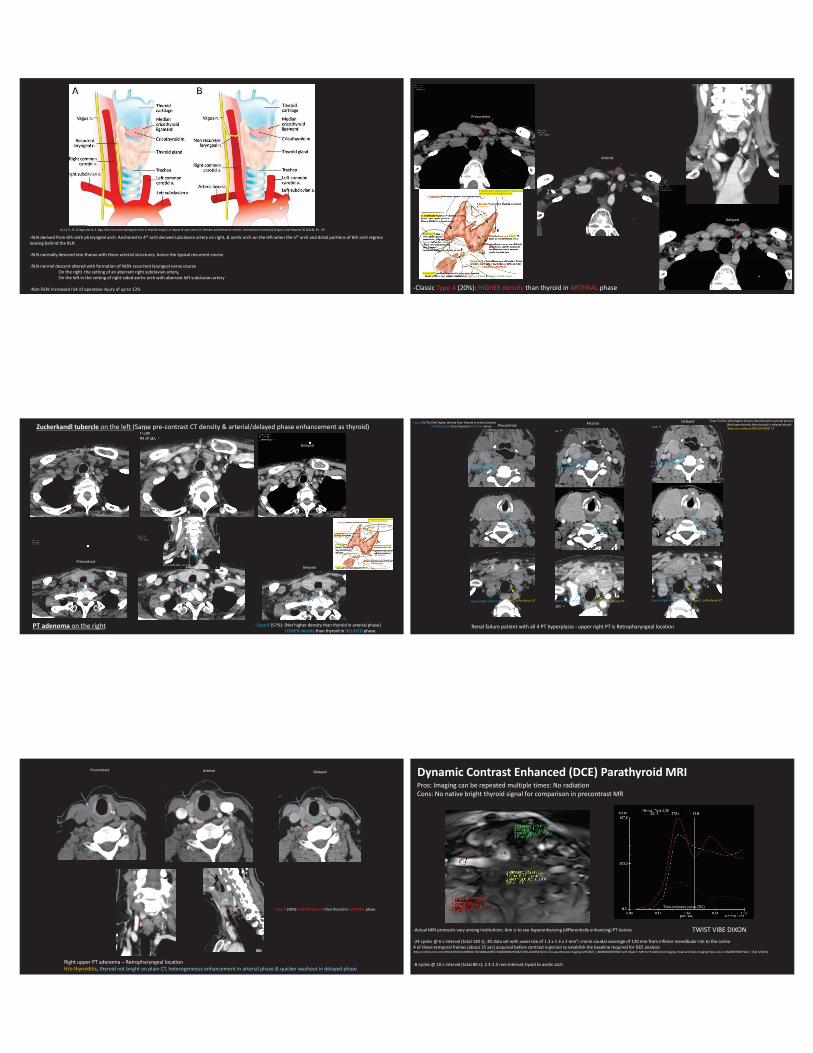
-All types A, B & C: PT lesion has LOWER density than thyroid gland (as thyroid has intrinsic iodine) in PRE-CONTRAST CT
-Classic Type A (20%): HIGHER density than thyroid in ARTERIAL phase
-Type B (57%): (Not higher density than thyroid in arterial phase)LOWER density than thyroid in DELAYED phase
-Type C (22%): (Not higher density than thyroid in arterial phase)(Not lower density than thyroid in delayed phase)May miss without PRECONTRAST CT
Practical Pearl: Look for lesions that is lower in density to thyroid gland in pre-contrast CT, and enhance differently from thyroid gland & lymph nodes
WWhich CT phases and anatomical locations should we focus on?
• First, look at Arterial phase first: Polar artery MAY help (not always there)Polar vessel sign only in 2/3rd of PT adenomas (Lymph nodes have hilar vessel instead)
More common in adenomas with arterial phase hyperenhancement (Type A pattern)Bahl M, Muzaffar M, Vij G, Sosa JA, Choudhury KR, Hoang JK. Prevalence of the polar vessel sign in parathyroid adenomas on the arterial phase of 4D CT. AJNR 2014;35(3):578-81
-Lymph nodes show progressive contrast opacification
• Next, look at Precontrast: Concentrate on subcapsular region (US better for small subcapsular/perithyroid PT adenomas)
• Lastly, look at Delayed (venous) phase
• Look at Eutopic locations firstDo not be satisfied if you find a lesion; keep looking
• Next, look at Ectopic locations
• Practical pearl: Look carefully around the Trachea, Esophagus, TE groove & in lower neck posterior to Strap Muscles
4D CT (or MR)Reporting
• Single or MGD
• Describe precise location: In relation to surgically visible landmarks cricoid, thyroid gland, suprasternal notch, esophagus, AP relation to TE groove (not cervical vertebrae)
• Describe radiologist’s confidence level: When same patient has high & low-confidence lesions surgeon may start with MIP of the highest confidence target, planning to convert to BNE if intraoperative post-excision PTH levels do not come down
• Size: <7mm hyperplasia; >13 mm adenoma
• Describe thyroid lesions: May need further workup & possible concurrent resection of suspicious/malignant nodules
• Describe anatomical variants that may impact surgery-Aberrant right subclavian artery (SCA) arising from descending aorta distal to left SCA crossing to right posterior to esophagus -NON-recurrent laryngeal nerve
Le, Q. V., D. Q. Ngo and Q. X. Ngo. Non-recurrent laryngeal nerve in thyroid surgery: A report of case series in Vietnam and literature review. International Journal of Surgery Case Reports 50 (2018): 56 - 59
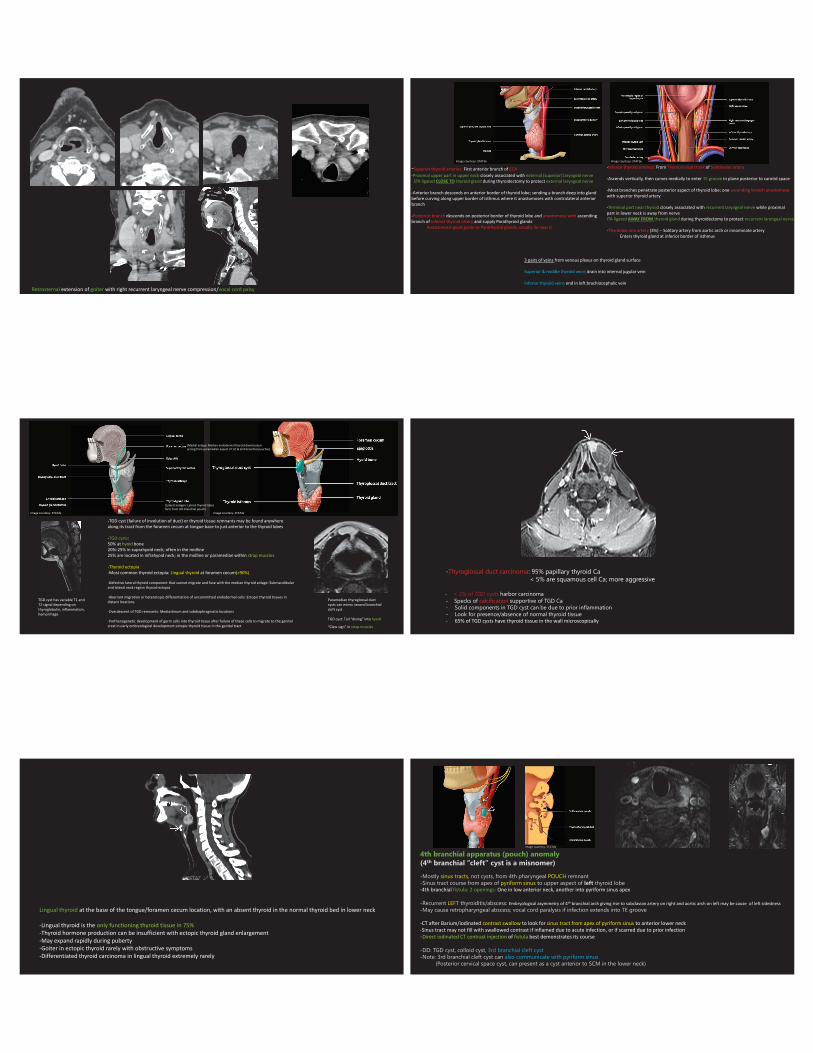
-RLN derived from 6th sixth pharyngeal arch: Anchored to 4th arch derived subclavian artery on right, & aortic arch on the left when the 5th arch and distal portions of 6th arch regress leaving behind the RLN
-RLN normally descend into thorax with these arterial structures, hence the typical recurrent course
-RLN normal descent altered with formation of NON-recurrent laryngeal nerve courseOn the right the setting of an aberrant right subclavian artery, On the left in the setting of right-sided aortic arch with aberrant left subclavian artery
-Non-RLN: Increased risk of operative injury of up to 13%
Delayed
Arterial
Arterial
Precontrast
-Classic Type A (20%): HIGHER density than thyroid in ARTERIAL phase
Zuckerkandl tubercle on the left (Same pre-contrast CT density & arterial/delayed phase enhancement as thyroid)
-Type B (57%): (Not higher density than thyroid in arterial phase)LOWER density than thyroid in DELAYED phase
PT adenoma on the right
Precontrast
Precontrast
Arterial
Arterial
Delayed
Delayed
Renal failure patient with all 4 PT hyperplasia - upper right PT is Retropharyngeal location
Precontrast Arterial Delayed-Type B (57%): (Not higher density than thyroid in arterial phase)LOWER density than thyroid in DELAYED phase
-Type C (22%): (Not higher density than thyroid in arterial phase)(Not lower density than thyroid in delayed phase)May miss without PRECONTRAST CT
Type B: Right Superior PT(Retropharyngeal)
Type B: Right Superior PT(Retropharyngeal)
Type B: Right Superior PT(Retropharyngeal)
Type B: Left Superior PT Type B: Left Superior PTType B: Left Superior PT
Type B: Right Inferior PT Type B: Right Inferior PT Type B: Right Inferior PT Type C: Left Inferior PTType C: Left Inferior PTType C: Left Inferior PT
Right upper PT adenoma – Retropharyngeal locationH/o thyroiditis, thyroid not bright on plain CT, heterogeneous enhancement in arterial phase & quicker washout in delayed phase
Precontrast Arterial Delayed
Type A (20%): HIGHER density than thyroid in ARTERIAL phase
Dynamic Contrast Enhanced (DCE) Parathyroid MRI
TWIST VIBE DIXON -Actual MRI protocols vary among institutions: Aim is to see hyperenhancing (differentially enhancing) PT lesions
-24 cycles @ 6 s interval (total 140 s); 3D data set with voxel size of 1.3 x 1.3 x 2 mm³; cranio-caudal coverage of 120 mm from inferior mandibular rim to the carina 4 of these temporal frames (about 25 sec) acquired before contrast injection to establish the baseline required for DCE analysishttps://cdn0.scrvt.com/39b415fb07de4d9656c7b516d8e2d907/1800000002503827/3d1a5ebf5d3b/mri-for-parathyroid-imaging-02503827_1800000002503827.pdf. (Nael K. MRI for Parathyroid Imaging. Head and Neck Imaging How-I-do-it. MAGNETOM Flash | (63) 3/2015)
-8 cycles @ 10 s interval (total 80 s); 2.3-2.5 mm interval; hyoid to aortic arch
Pros: Imaging can be repeated multiple times: No radiationCons: No native bright thyroid signal for comparison in precontrast MR
Time-intensity curve (TIC)
PParathyromatosis
• Multiple tiny nodules of hyperfunctioning parathyroid tissue form in the neck and mediastinum • Extremely rare cause of recurrent hyperparathyroidism• In patients who have had prior neck surgeries for hyperparathyroidism• May rarely occur primarily
• Histopathology: Real capsule is absent in the nests of the parathyroid tissue in parathyromatosis(in contrast to adenomas & parathyroid carcinomas which have capsule)
2 theories • Result of improper handling of PT glands during surgery
• PT gland left behind during ontogenesis that develops under physiological pressure into hyperfunctioning nests of tissue
Aksoy-Altinboga A, Akder Sari A, Rezanko T, Haciyanli M, Orgen Calli A. Parathyromatosis: critical diagnosis regarding surgery and pathologic evaluation. Korean J Pathol. 2012;46(2):197-200
Thank you@drSurjthVattoth