Embed Size (px)
DESCRIPTION
ADCO 2012 Learning From Incidents- HSE
Citation preview
منع وقوع الحوادث من خ�ل الدروس والعبر المستفادة منھا
Incident Prevention Through
Learning from Incidents
January - December, 2012
قسم الصحة والس�مة والبيئة
Health, Safety & Environment Division
1
For further information, comments and suggestions please contact:
Dr. Muhammad. R. Tayab ([email protected])
Health, Safety & Environment Division Tel: 02-6041217; Mobile – 00971 (0) 50 324-3996
للمزيد من المعلومات وإبداء الم�حظات واقتراحات يرجى اتصال بـ:
[email protected]على البريد الكتروني التالي : محمد ريحان طيب الدكتور قسم الصحة والس�مة والبيئة
6041217رقم الھاتف :
This Booklet is circulated within ADCO organization within the framework of HSEMS. It should only serve as guidance and ADCO shall in no event accept any liability for either the fact described, nor for any reliance on the contents by any third party.
2
ADCO regards safety of both ADCO & Contractor staff as well as protection of the environment and integrity of its assets high and I reiterate ADCO commitment to create a safe working environmental for every member of ADCO Community. We have achieved very challenging production and operations targets during 2012 with high focus on personnel and process safety. During the 2012, ADCO has recorded over 160 Million Manhours worked by 52,000 ADCO & Contractor staff; and we have driven approximately 200 Million Kilometers. Regrettably, we have had 2 work related fatalities, 20 Non Accidental Deaths (NAD) and over 75 serious injuries. In addition we had 24 vehicle crashes and 8 oil spills events. Incident investigations highlighted deficiencies in work planning, supervision and behaviour. Key gaps included:
• Task related risks were not adequately identified
• Workers were not made aware of risks and were not effectively supervised.
• Lessons from prior incidents not embedded
• Tasks were not planned adequately (due to lack of competent human resources and non-availability of right tools) ADCO safe system of work (e.g. Task Risk Assessment (TRA), Permit to Work (PTW), Tool Box Talks (TBT) etc.) is designed to save lives and should be respected. It is not mere a paper exercise, it is workers’ life line. I request all ADCO team members to take diligent review of work planning at grass root levels and effectively address these deficiencies. I am sure it will create a positive change and enhance safety at work. I would like every member of ADCO community to review this collection of incidents and what lessons can be learned and then their work activities so that these incidents are not repeated. You are requested never to compromise on the safety of staff & worker, protection of the environment and integrity of our assets. I am fully committed to provide you all the support and resources that you may require to create a safer working environment to all.
Abdul Munim Saif Al Kindy
Chief Executive Officer (CEO)
3
Table of Contents
Finger Injury Resulting from Using Hand Tools 9
33-Kv Underground Cable Damage During Sand Clearance 10
Damage to Underground Fiber Optic Cable During Excavation 11
Crane Mounted Truck (Hiab) Rollover on Gatch Road 12
Crane Mounted Truck Rollover on Gatch Road 13
Loss of Containment 18
Rollover of Truck Carrying Gatch 19
Fire at Wooden Electrical Pole 20
Vehicle Drop in Low Lying Area/Depression 21
Breakage of Hook of Wire Rope 22
Injury from Falling Cap of Circulating Head 27
Struck by Swinging Mud Pump During Lifting 28
Fall of Travelling Block with Full String Weight 29
Gas Release From Coil Tubing 30
Vehicle Collision Near A Rig Site 31
Low Bed Trailer Rollover 32
Finger Injury During Entanglement of Wire from Wireline Reel 33
Release of Oil from Xmas Tree 34
Fall of Foreman from Stand Pipe 35
Dropped Object During Lifting 36
Uncontrolled Descend of Travelling Block 37
Power Generator/Engine Fire 38
Trailer Fire at Rig Camp 39
Water Tanker Rollover 40
Hand Entrapment Inside Tong 41
Electrical Shock 42
Arm Injury Due to Fall of Jumbo Bag 43
Falling Object 44
Fire Due to Poor Grounding During Welding 49
Fiber Optic Cable Cut During Excavation 50
Vehicle Collision & Rollover 51
Asphyxiation of Welder Inside A Pipe 52
Man Lift Drove Over Flagman’s Foot 53
Vehicle Rollover 54
Vehicle Collision on a Sand Track 55
4
Vehicle Drove Over a Berm 56
Cement Mixer Rollover 57
Damage to Overhead Line 58
Ankle Injury During Cable Pulling 59
Vehicles Collision on Gatch Road 60
Arm Injury Due to Explosion During CAD Welding 61
Fire at Scaffolding Platform Around Stripper Column 62
Foreign Object Entering Eye of a Worker 63
Vehicle Rollover on Gatch Road 64
Crane Mounted Truck (Hiab) Rollover on Gatch Road 65
Vehicles Collision 66
Crane Rollover During Move on Gatch Road 67
Vehicle Collision 68
Fatal Fall of Worker from a Moving Vehicle 69
Fall of Mobile Scaffold Platform on a Worker 70
Arm Amputation Inside Foam Concrete Mixer 71
Vehicle Crash During OHL Visual Survey 76
Transformer Fire 77
Fire in UPS Unit of Substation 78
Electrical Flashover Inside Transformer Terminal Box 83
Foreign Object (Metal Particle in Eye) 84
Worker’s Finger Entrapment Between Pipe Flange and Valve Flange 85
Heat Stress 90
HSE Performance, 2012 91
Incident Types - 2012 92
Asset Wise Event Type Distribution - 2012 94
Incident Immediate & Root Cause Categories 2012 95
Incident Immediate Cause Analysis -2012 96
Incident Root Cause Analysis -2012 97
5
BAB & Gas Asset
6
7
Past Incidents
Wireline Truck Rollover
(04-0-7-10)
Loss of Containment near RDS5
(20-11-2010)
Fatal Vehicle Rollover
(01-08-2010)
Fire at Disposal Water Pump
(09-03-2011)
H2S Release from Common Drain
Header (09-06-2010)
Eye Injury Due to Acid Splash (06-
02-2010)
Production Header Leak
(24-04-2011)
Finger Injury Due to Slippage of Cylinder (16-06-2011)
Finger Injury During Bolting of Flange
(29-01-2010)
Gas Release From X-Mas Tree
(16-01-2010)
H2S Release from Water Supply Well (16-05-2010)
H2S Release from Oil Well
(20-11-2012)

8
9
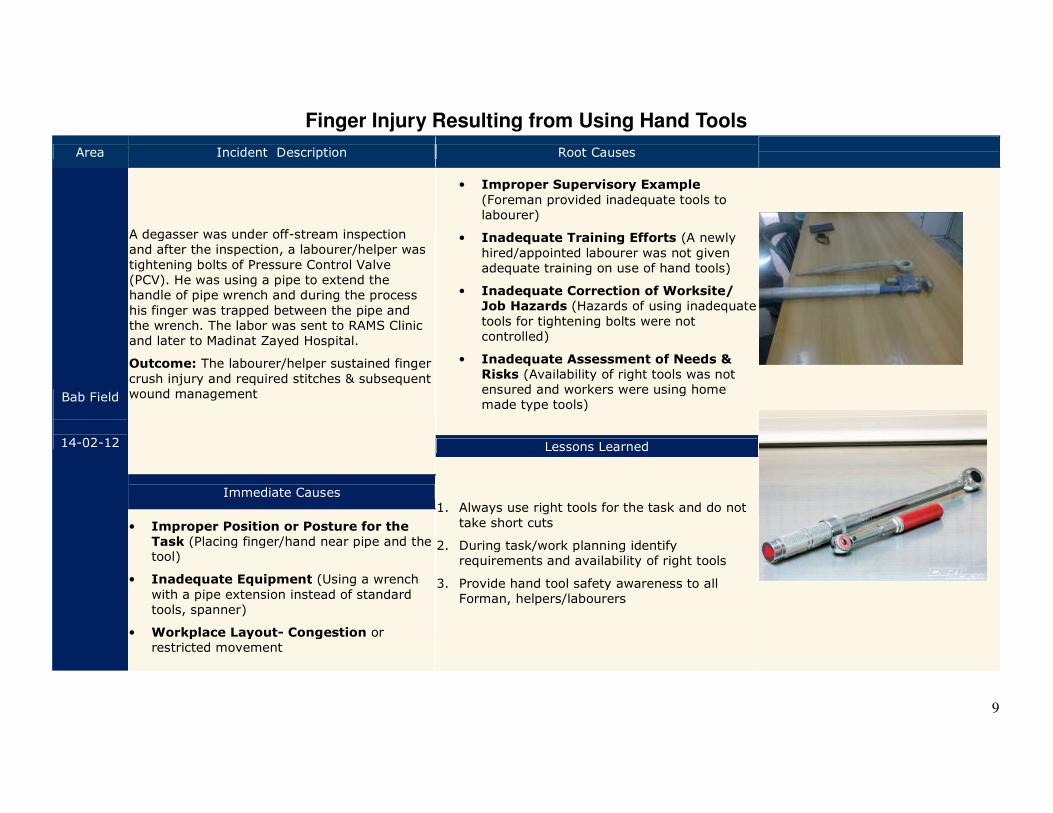
Finger Injury Resulting from Using Hand Tools
Area Incident Description Root Causes
Bab Field
14-02-12
A degasser was under off-stream inspection and after the inspection, a labourer/helper was
tightening bolts of Pressure Control Valve (PCV). He was using a pipe to extend the handle of pipe wrench and during the process
his finger was trapped between the pipe and the wrench. The labor was sent to RAMS Clinic and later to Madinat Zayed Hospital.
Outcome: The labourer/helper sustained finger
crush injury and required stitches & subsequent wound management
• Improper Supervisory Example
(Foreman provided inadequate tools to labourer)
• Inadequate Training Efforts (A newly
hired/appointed labourer was not given adequate training on use of hand tools)
• Inadequate Correction of Worksite/
Job Hazards (Hazards of using inadequate
tools for tightening bolts were not controlled)
• Inadequate Assessment of Needs &
Risks (Availability of right tools was not ensured and workers were using home made type tools)
Lessons Learned
1. Always use right tools for the task and do not
take short cuts
2. During task/work planning identify requirements and availability of right tools
3. Provide hand tool safety awareness to all Forman, helpers/labourers
Immediate Causes
• Improper Position or Posture for the
Task (Placing finger/hand near pipe and the tool)
• Inadequate Equipment (Using a wrench
with a pipe extension instead of standard tools, spanner)
• Workplace Layout- Congestion or restricted movement
10
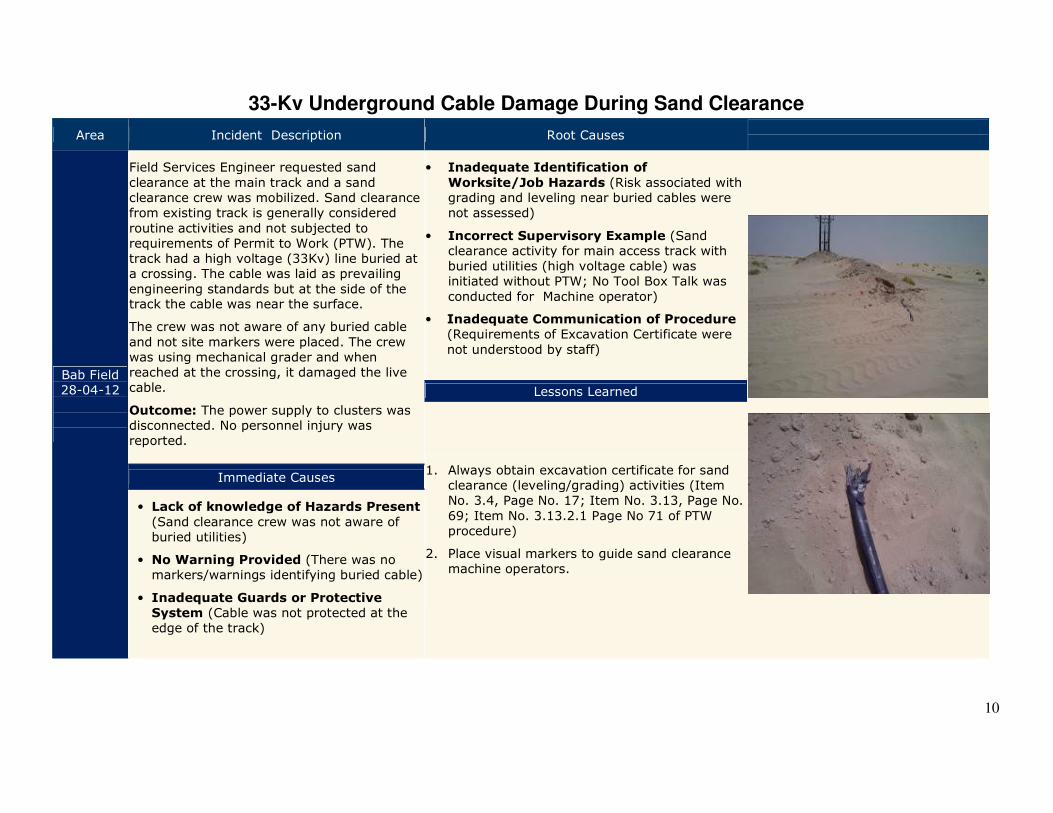
33-Kv Underground Cable Damage During Sand Clearance
Area Incident Description Root Causes
Bab Field 28-04-12
Field Services Engineer requested sand
clearance at the main track and a sand clearance crew was mobilized. Sand clearance from existing track is generally considered
routine activities and not subjected to requirements of Permit to Work (PTW). The track had a high voltage (33Kv) line buried at a crossing. The cable was laid as prevailing
engineering standards but at the side of the track the cable was near the surface.
The crew was not aware of any buried cable
and not site markers were placed. The crew was using mechanical grader and when reached at the crossing, it damaged the live cable.
Outcome: The power supply to clusters was disconnected. No personnel injury was reported.
• Inadequate Identification of
Worksite/Job Hazards (Risk associated with grading and leveling near buried cables were not assessed)
• Incorrect Supervisory Example (Sand clearance activity for main access track with buried utilities (high voltage cable) was initiated without PTW; No Tool Box Talk was
conducted for Machine operator)
• Inadequate Communication of Procedure (Requirements of Excavation Certificate were
not understood by staff)
Lessons Learned
1. Always obtain excavation certificate for sand clearance (leveling/grading) activities (Item No. 3.4, Page No. 17; Item No. 3.13, Page No.
69; Item No. 3.13.2.1 Page No 71 of PTW procedure)
2. Place visual markers to guide sand clearance machine operators.
Immediate Causes
• Lack of knowledge of Hazards Present
(Sand clearance crew was not aware of buried utilities)
• No Warning Provided (There was no markers/warnings identifying buried cable)
• Inadequate Guards or Protective
System (Cable was not protected at the edge of the track)
11
Damage to Underground Fiber Optic Cable During Excavation
Area Incident Description Causes
BAB Field
08-08-12
A 3rd party contractor was working on a project to lay a new potable water pipeline to supply GASCO and ADCO with potable water and the majority of the work was completed in BAB. The work was performed under ADCO Permit to Work (PTW) system and an excavation certificate was issued. As built drawing did not show location of buried fiber optic cables
(which were running parallel to a transfer line) and there were no physical markers on the ground.
The task was intended for manual excavation and the use of machine was limited to removal of excavated material/debris.
The crew did not have adequate resources (i.e. number of laborers for manual excavation) to complete the task on schedule and these resources were not adjusted for work during the fasting month of Ramadan.
The job performer had started to use mechanical excavator, after exposing buried line. During the excavation a fiber optic communication cable was cut and that has resulted in tripping of Remote Degassing Station (RDS-1) and alarm was sounded in the control room of Bab Central Degassing Station (BCDS).
• Inadequate Work Planning (The
number of labourers in the crew were not adequate to manually excavate the site on time and shorter working
hours in Ramadan were not considered during work planning)
• Inadequate Implementation of
Procedure (JP was not a member of Task Risk Assessment (TRA) team and did not endorse the TRA)
• Inadequate Leadership (Job
Originator was not involved in TRA and did not ensure availability of adequate resources for task execution; As built drawings did not
show location of buried cables)
Lessons Learned
1. Do not use mechanical excavator in restricted areas.
2. Ensure availability of adequate
resources prior to execution of tasks
3. Provide updated as built drawings
to support excavation certificate
4. Ensure Job Originator & Job Performer/s are part of Task Risk Assessment (TRA) Team
Immediate Causes
• Violation by Supervisor (The job performer (JP) used a
mechanical excavator in area where manual excavation was authorized)
• Lack of knowledge of Hazards Present (Location of buried cable was not known to Job Performer and there
were no surface makers on the ground; Job Performer was not aware of risks associated with the task)
• Inadequate Guard or Protective Devices (Cable were
buried without any physical protection)
12
Crane Mounted Truck (Hiab) Rollover on Gatch Road
Area Incident Description Root Causes
BAB Field
22-08-12
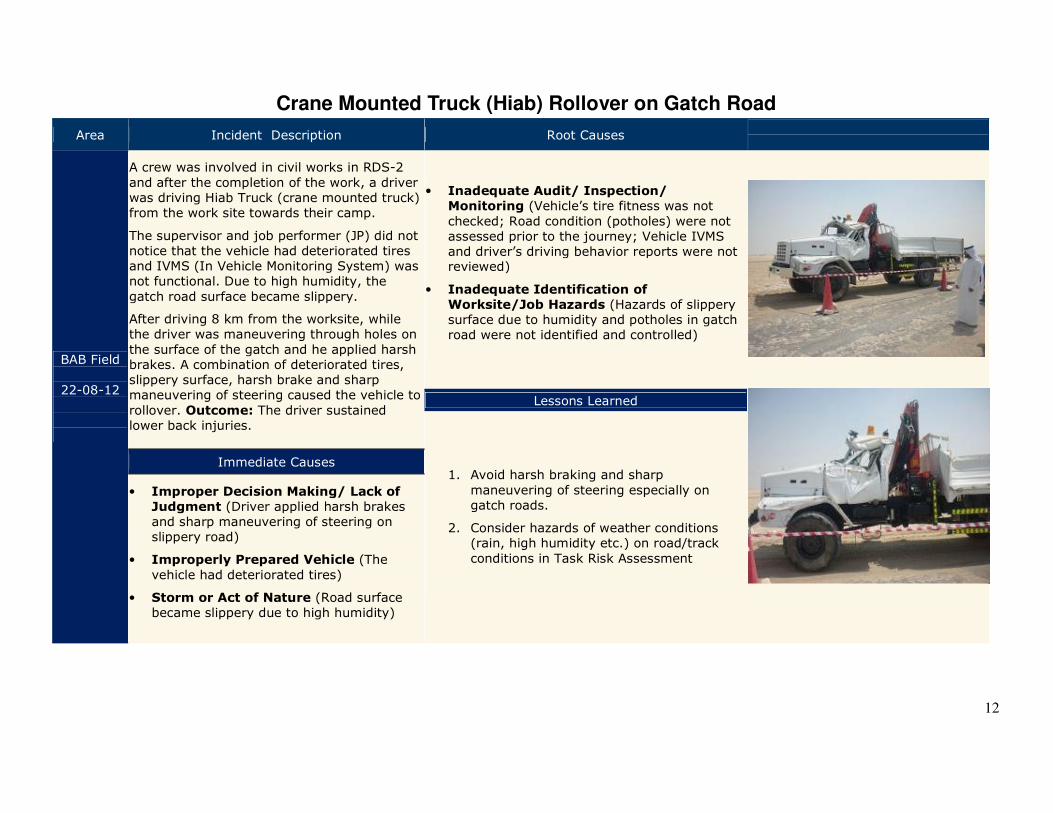
A crew was involved in civil works in RDS-2
and after the completion of the work, a driver was driving Hiab Truck (crane mounted truck) from the work site towards their camp.
The supervisor and job performer (JP) did not notice that the vehicle had deteriorated tires and IVMS (In Vehicle Monitoring System) was not functional. Due to high humidity, the
gatch road surface became slippery.
After driving 8 km from the worksite, while the driver was maneuvering through holes on
the surface of the gatch and he applied harsh brakes. A combination of deteriorated tires, slippery surface, harsh brake and sharp maneuvering of steering caused the vehicle to
rollover. Outcome: The driver sustained lower back injuries.
• Inadequate Audit/ Inspection/
Monitoring (Vehicle’s tire fitness was not
checked; Road condition (potholes) were not assessed prior to the journey; Vehicle IVMS and driver’s driving behavior reports were not reviewed)
• Inadequate Identification of
Worksite/Job Hazards (Hazards of slippery surface due to humidity and potholes in gatch road were not identified and controlled)
Lessons Learned
1. Avoid harsh braking and sharp
maneuvering of steering especially on gatch roads.
2. Consider hazards of weather conditions (rain, high humidity etc.) on road/track
conditions in Task Risk Assessment
Immediate Causes
• Improper Decision Making/ Lack of
Judgment (Driver applied harsh brakes and sharp maneuvering of steering on slippery road)
• Improperly Prepared Vehicle (The
vehicle had deteriorated tires)
• Storm or Act of Nature (Road surface became slippery due to high humidity)
13
Crane Mounted Truck Rollover on Gatch Road
Area Incident Description Root Causes
BAB Field
22-08-12
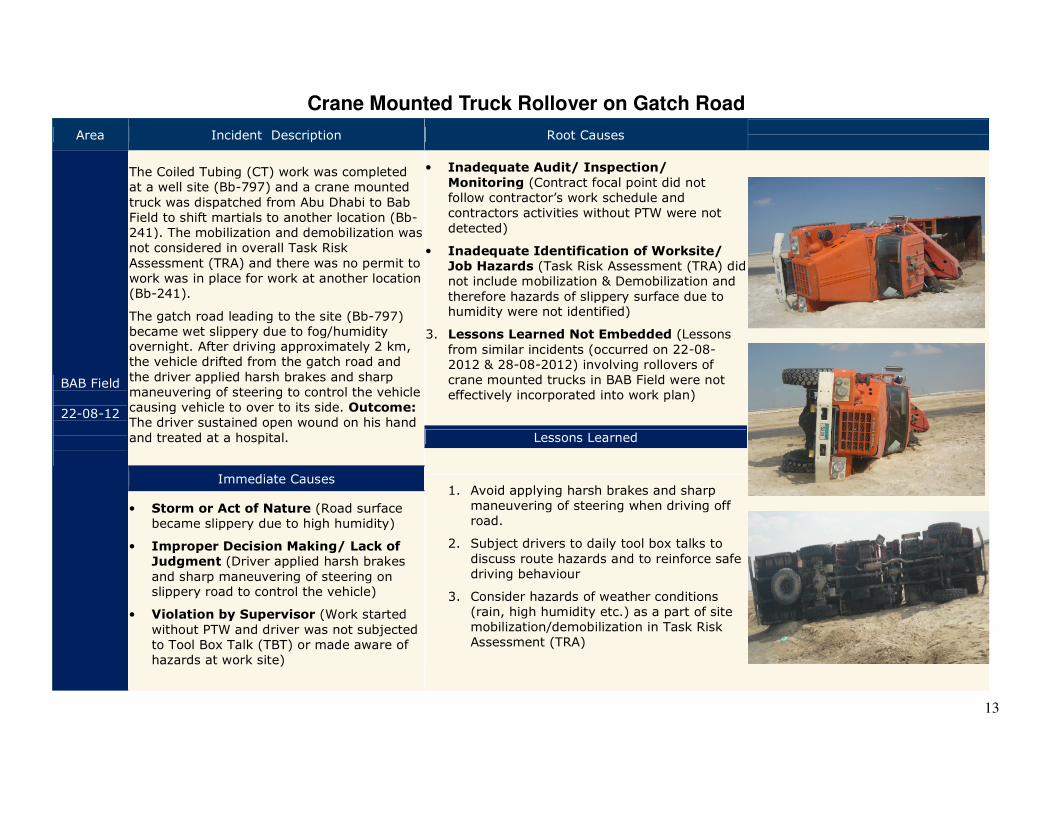
The Coiled Tubing (CT) work was completed at a well site (Bb-797) and a crane mounted
truck was dispatched from Abu Dhabi to Bab Field to shift martials to another location (Bb-241). The mobilization and demobilization was not considered in overall Task Risk
Assessment (TRA) and there was no permit to work was in place for work at another location (Bb-241).
The gatch road leading to the site (Bb-797) became wet slippery due to fog/humidity overnight. After driving approximately 2 km, the vehicle drifted from the gatch road and
the driver applied harsh brakes and sharp maneuvering of steering to control the vehicle causing vehicle to over to its side. Outcome: The driver sustained open wound on his hand
and treated at a hospital.
• Inadequate Audit/ Inspection/
Monitoring (Contract focal point did not follow contractor’s work schedule and contractors activities without PTW were not
detected)
• Inadequate Identification of Worksite/
Job Hazards (Task Risk Assessment (TRA) did not include mobilization & Demobilization and
therefore hazards of slippery surface due to humidity were not identified)
3. Lessons Learned Not Embedded (Lessons
from similar incidents (occurred on 22-08-2012 & 28-08-2012) involving rollovers of crane mounted trucks in BAB Field were not effectively incorporated into work plan)
Lessons Learned
1. Avoid applying harsh brakes and sharp maneuvering of steering when driving off road.
2. Subject drivers to daily tool box talks to
discuss route hazards and to reinforce safe driving behaviour
3. Consider hazards of weather conditions (rain, high humidity etc.) as a part of site mobilization/demobilization in Task Risk Assessment (TRA)
Immediate Causes
• Storm or Act of Nature (Road surface became slippery due to high humidity)
• Improper Decision Making/ Lack of
Judgment (Driver applied harsh brakes
and sharp maneuvering of steering on slippery road to control the vehicle)
• Violation by Supervisor (Work started
without PTW and driver was not subjected to Tool Box Talk (TBT) or made aware of hazards at work site)
14
Buhasa/Huwaila/Bida Qamzan Asset

15
16
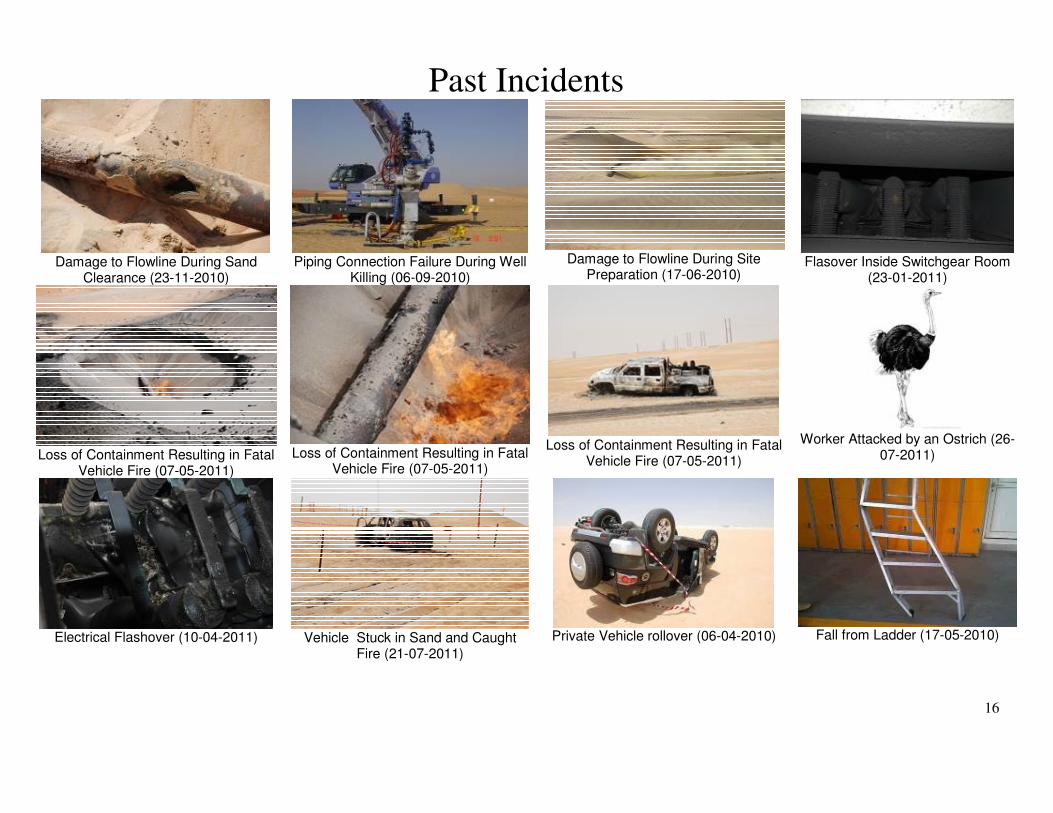
Past Incidents
Damage to Flowline During Sand
Clearance (23-11-2010)
Piping Connection Failure During Well
Killing (06-09-2010)
Damage to Flowline During Site
Preparation (17-06-2010)
Flasover Inside Switchgear Room
(23-01-2011)
Loss of Containment Resulting in Fatal
Vehicle Fire (07-05-2011)
Loss of Containment Resulting in Fatal
Vehicle Fire (07-05-2011)
Loss of Containment Resulting in Fatal
Vehicle Fire (07-05-2011)
Worker Attacked by an Ostrich (26-
07-2011)
Electrical Flashover (10-04-2011)
Vehicle Stuck in Sand and Caught
Fire (21-07-2011)
Private Vehicle rollover (06-04-2010)
Fall from Ladder (17-05-2010)

17
18
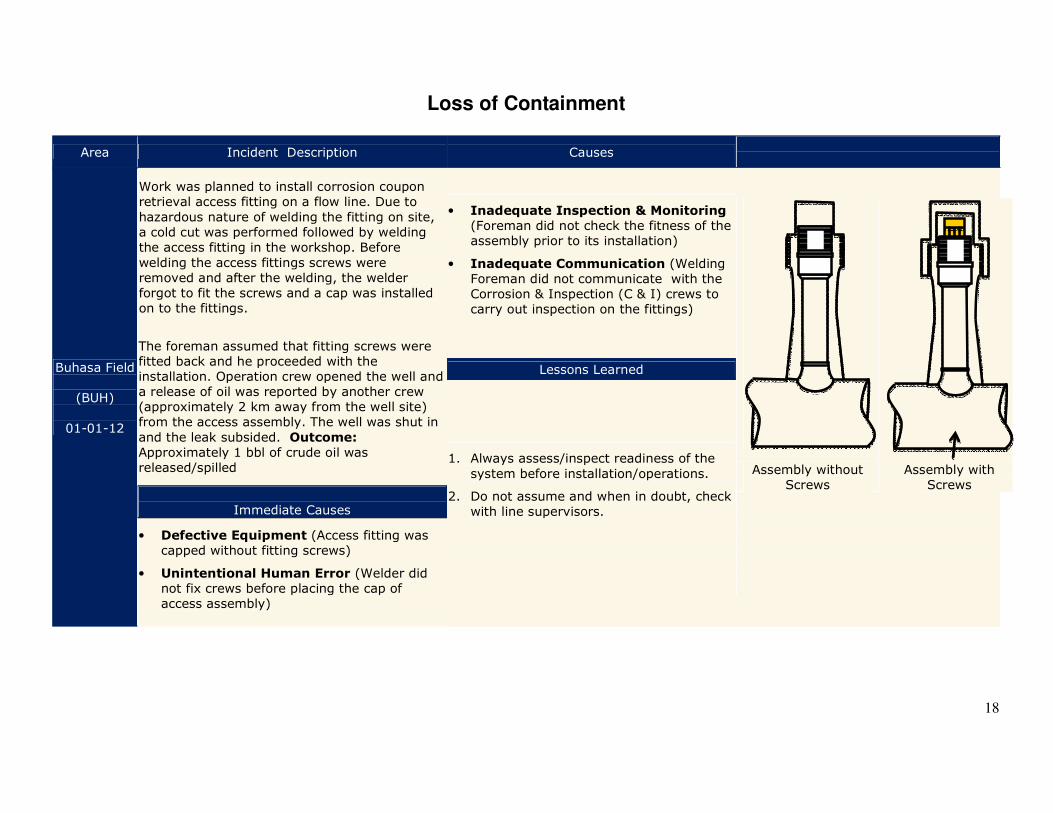
Loss of Containment
Area Incident Description Causes
Buhasa Field
(BUH)
01-01-12
Work was planned to install corrosion coupon retrieval access fitting on a flow line. Due to
hazardous nature of welding the fitting on site, a cold cut was performed followed by welding the access fitting in the workshop. Before
welding the access fittings screws were removed and after the welding, the welder forgot to fit the screws and a cap was installed on to the fittings.
The foreman assumed that fitting screws were fitted back and he proceeded with the installation. Operation crew opened the well and a release of oil was reported by another crew (approximately 2 km away from the well site) from the access assembly. The well was shut in
and the leak subsided. Outcome: Approximately 1 bbl of crude oil was released/spilled
• Inadequate Inspection & Monitoring (Foreman did not check the fitness of the assembly prior to its installation)
• Inadequate Communication (Welding Foreman did not communicate with the Corrosion & Inspection (C & I) crews to carry out inspection on the fittings)
Assembly without Screws
Assembly with Screws
Lessons Learned
1. Always assess/inspect readiness of the
system before installation/operations.
2. Do not assume and when in doubt, check with line supervisors.
Immediate Causes
• Defective Equipment (Access fitting was capped without fitting screws)
• Unintentional Human Error (Welder did not fix crews before placing the cap of access assembly)
19
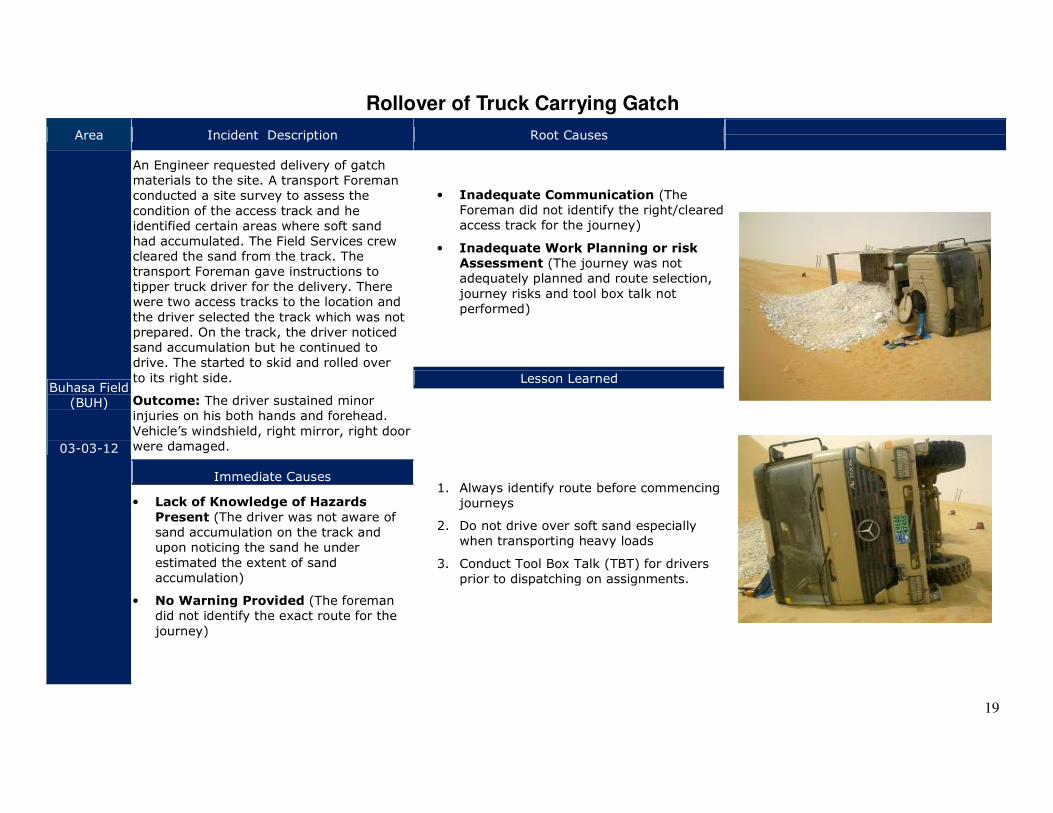
Rollover of Truck Carrying Gatch
Area Incident Description Root Causes
Buhasa Field (BUH)
03-03-12
An Engineer requested delivery of gatch materials to the site. A transport Foreman conducted a site survey to assess the
condition of the access track and he identified certain areas where soft sand had accumulated. The Field Services crew cleared the sand from the track. The transport Foreman gave instructions to tipper truck driver for the delivery. There were two access tracks to the location and
the driver selected the track which was not prepared. On the track, the driver noticed sand accumulation but he continued to drive. The started to skid and rolled over
to its right side.
Outcome: The driver sustained minor injuries on his both hands and forehead.
Vehicle’s windshield, right mirror, right door were damaged.
• Inadequate Communication (The Foreman did not identify the right/cleared access track for the journey)
• Inadequate Work Planning or risk
Assessment (The journey was not adequately planned and route selection,
journey risks and tool box talk not performed)
Lesson Learned
1. Always identify route before commencing journeys
2. Do not drive over soft sand especially when transporting heavy loads
3. Conduct Tool Box Talk (TBT) for drivers prior to dispatching on assignments.
Immediate Causes
• Lack of Knowledge of Hazards
Present (The driver was not aware of sand accumulation on the track and upon noticing the sand he under
estimated the extent of sand accumulation)
• No Warning Provided (The foreman did not identify the exact route for the
journey)
20
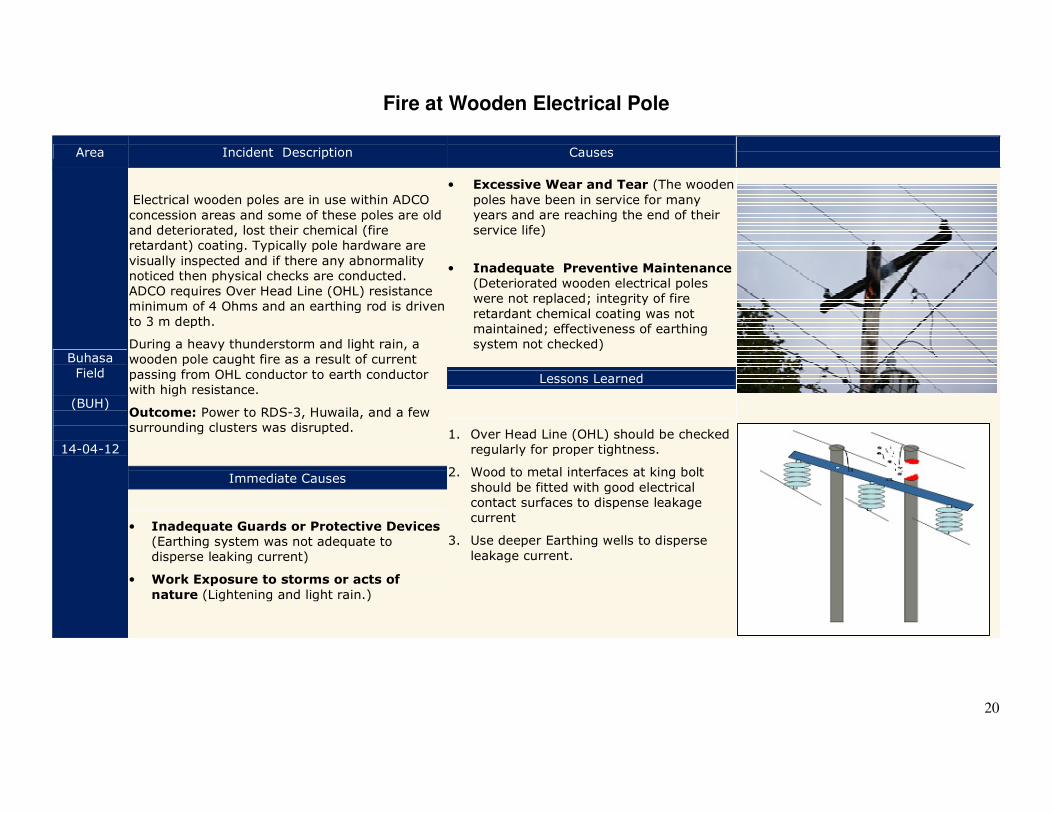
Fire at Wooden Electrical Pole
Area Incident Description Causes
Buhasa Field
(BUH)
14-04-12
Electrical wooden poles are in use within ADCO concession areas and some of these poles are old and deteriorated, lost their chemical (fire retardant) coating. Typically pole hardware are
visually inspected and if there any abnormality noticed then physical checks are conducted. ADCO requires Over Head Line (OHL) resistance minimum of 4 Ohms and an earthing rod is driven
to 3 m depth.
During a heavy thunderstorm and light rain, a wooden pole caught fire as a result of current
passing from OHL conductor to earth conductor with high resistance.
Outcome: Power to RDS-3, Huwaila, and a few surrounding clusters was disrupted.
• Excessive Wear and Tear (The wooden
poles have been in service for many years and are reaching the end of their service life)
• Inadequate Preventive Maintenance
(Deteriorated wooden electrical poles were not replaced; integrity of fire
retardant chemical coating was not maintained; effectiveness of earthing system not checked)
Lessons Learned
1. Over Head Line (OHL) should be checked regularly for proper tightness.
2. Wood to metal interfaces at king bolt
should be fitted with good electrical contact surfaces to dispense leakage current
3. Use deeper Earthing wells to disperse
leakage current.
Immediate Causes
• Inadequate Guards or Protective Devices (Earthing system was not adequate to disperse leaking current)
• Work Exposure to storms or acts of
nature (Lightening and light rain.)
21
Vehicle Drop in Low Lying Area/Depression
Area Incident Description Root Causes
Buhasa Field
(BUH)
22-08-12
A mechanical foreman was returning to the workshop from a wellsite (CL-29) and he was heading the wrong way. His colleagues
(passengers) in the vehicle advised him to proceed in the opposite direction. He turned the vehicle and started to drive in the desrt to get on the designated track. There was a
low lying area /depression in the sand and the vehicle slid down and made contact with the bottom of the dune.
Outcome: The vehicle sustained minor damage on the front-end bumper.
• Inadequate Practice of Skill
(Driver took a u-turn and
entered into non-designated route instead of remaining on track)
Immediate Causes
• Improper decision making/lack of
judgment (The driver did not return back to original track but tried to go another way to merge with the main
track)
• Inattention to surroundings (He did not pay attention to surface conditions
and was focusing to get on the designated track)
Lesson Learned
1. Always take the designated
route to avoid hazards of unstable ground conditions.
22
Breakage of Hook of Wire Rope
Area Incident Description Root Causes
Buhasa Field
(BUH)
10-08-12
A Foreman was driving to a well site (BU-559) and his vehicle got stuck on a sand dune. He requested assistance from the transport pool.
Transport Pool Driver reached the site and tried to pull the stuck vehicle using a wire rope with his own vehicle.
While pulling the vehicle from the rear side, the
wire rope's hook broke and struck against the foreman-vehicle’s rear window. Outcome: Rear window of the vehicle was completely
smashed.
• In adequate removal/replacement of
tools & equipment (The slings in the older
desert safety boxes were not checked/ replaced)
Lesson Learned
1. Check adequacy of tools available for in vehicle tool box.
2. Always check if the slings are certified/checked, and suitable for pulling the vehicle prior to use.
Immediate Causes
• Inadequate Tools or Equipment (The sling used was not suitable for the job)
23
Technical Services – Drilling
24
25
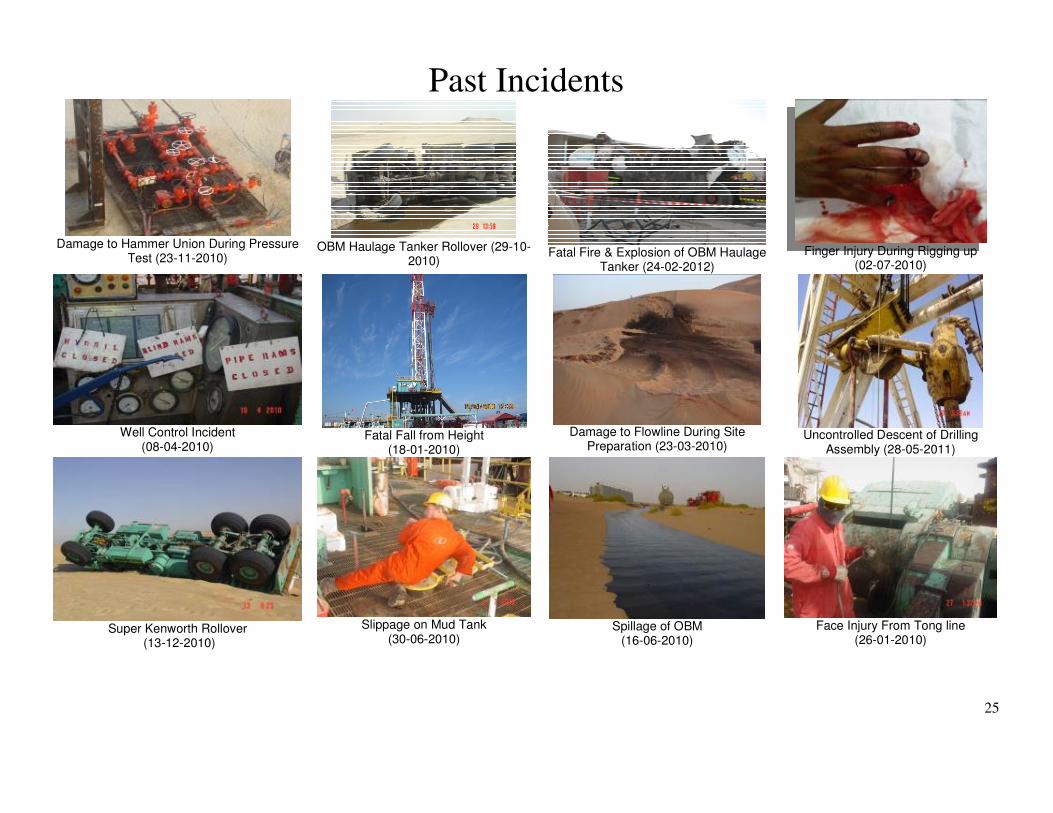
Past Incidents
Damage to Hammer Union During Pressure
Test (23-11-2010)
OBM Haulage Tanker Rollover (29-10-
2010)
Fatal Fire & Explosion of OBM Haulage
Tanker (24-02-2012)
Finger Injury During Rigging up
(02-07-2010)
Well Control Incident
(08-04-2010)
Fatal Fall from Height
(18-01-2010)
Damage to Flowline During Site
Preparation (23-03-2010)
Uncontrolled Descent of Drilling
Assembly (28-05-2011)
Super Kenworth Rollover
(13-12-2010)
Slippage on Mud Tank
(30-06-2010)
Spillage of OBM
(16-06-2010)
Face Injury From Tong line
(26-01-2010)

26
27
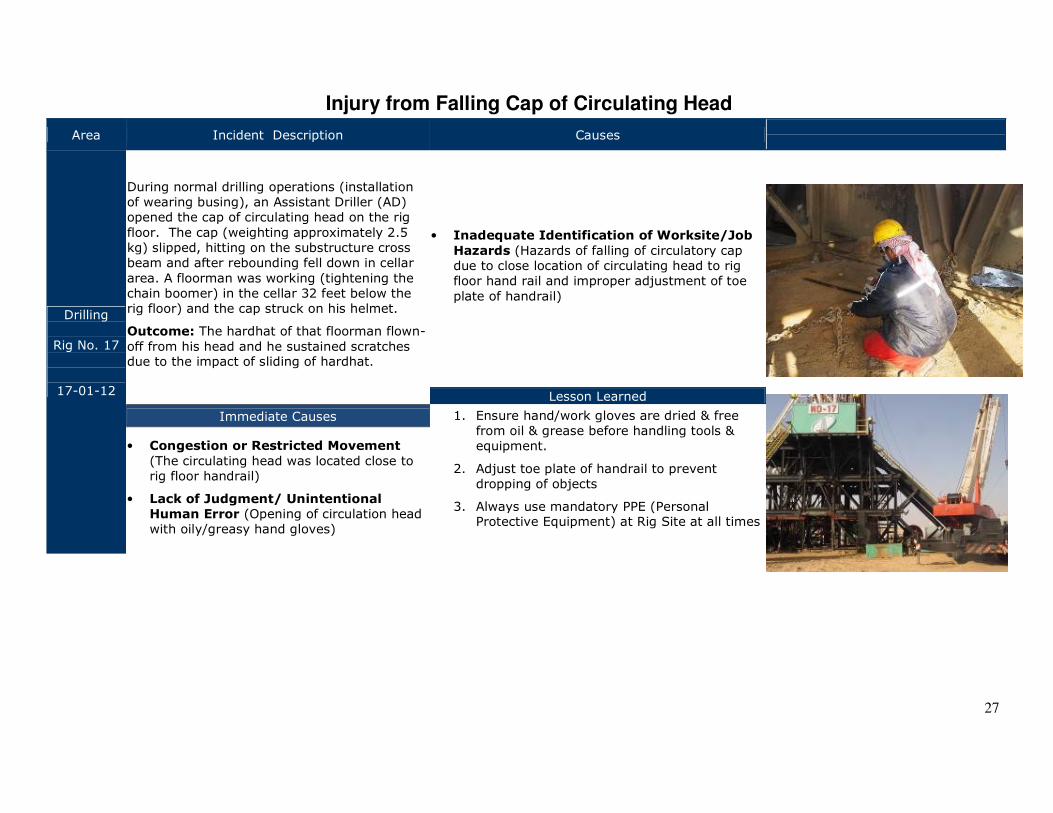
Injury from Falling Cap of Circulating Head
Area Incident Description Causes
Drilling
Rig No. 17
17-01-12
During normal drilling operations (installation of wearing busing), an Assistant Driller (AD) opened the cap of circulating head on the rig
floor. The cap (weighting approximately 2.5 kg) slipped, hitting on the substructure cross beam and after rebounding fell down in cellar
area. A floorman was working (tightening the chain boomer) in the cellar 32 feet below the rig floor) and the cap struck on his helmet.
Outcome: The hardhat of that floorman flown-
off from his head and he sustained scratches due to the impact of sliding of hardhat.
• Inadequate Identification of Worksite/Job
Hazards (Hazards of falling of circulatory cap due to close location of circulating head to rig floor hand rail and improper adjustment of toe
plate of handrail)
Lesson Learned
Immediate Causes 1. Ensure hand/work gloves are dried & free from oil & grease before handling tools & equipment.
2. Adjust toe plate of handrail to prevent dropping of objects
3. Always use mandatory PPE (Personal Protective Equipment) at Rig Site at all times
• Congestion or Restricted Movement
(The circulating head was located close to rig floor handrail)
• Lack of Judgment/ Unintentional
Human Error (Opening of circulation head with oily/greasy hand gloves)
28
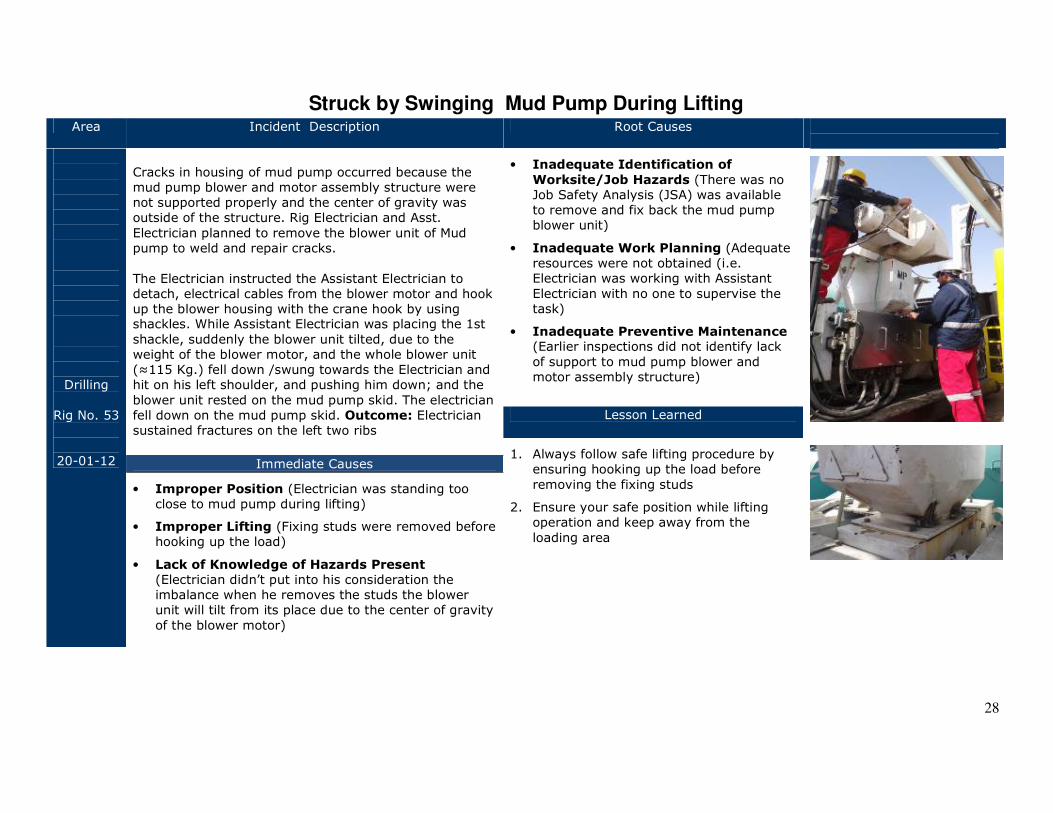
Struck by Swinging Mud Pump During Lifting Area Incident Description Root Causes
Drilling
Rig No. 53
20-01-12
Cracks in housing of mud pump occurred because the mud pump blower and motor assembly structure were not supported properly and the center of gravity was outside of the structure. Rig Electrician and Asst.
Electrician planned to remove the blower unit of Mud pump to weld and repair cracks.
The Electrician instructed the Assistant Electrician to detach, electrical cables from the blower motor and hook up the blower housing with the crane hook by using shackles. While Assistant Electrician was placing the 1st
shackle, suddenly the blower unit tilted, due to the weight of the blower motor, and the whole blower unit (≈115 Kg.) fell down /swung towards the Electrician and hit on his left shoulder, and pushing him down; and the
blower unit rested on the mud pump skid. The electrician fell down on the mud pump skid. Outcome: Electrician sustained fractures on the left two ribs
• Inadequate Identification of
Worksite/Job Hazards (There was no Job Safety Analysis (JSA) was available to remove and fix back the mud pump blower unit)
• Inadequate Work Planning (Adequate resources were not obtained (i.e. Electrician was working with Assistant
Electrician with no one to supervise the task)
• Inadequate Preventive Maintenance (Earlier inspections did not identify lack
of support to mud pump blower and motor assembly structure)
Lesson Learned
1. Always follow safe lifting procedure by ensuring hooking up the load before
removing the fixing studs
2. Ensure your safe position while lifting operation and keep away from the
loading area
Immediate Causes
• Improper Position (Electrician was standing too close to mud pump during lifting)
• Improper Lifting (Fixing studs were removed before hooking up the load)
• Lack of Knowledge of Hazards Present
(Electrician didn’t put into his consideration the imbalance when he removes the studs the blower unit will tilt from its place due to the center of gravity
of the blower motor)
29
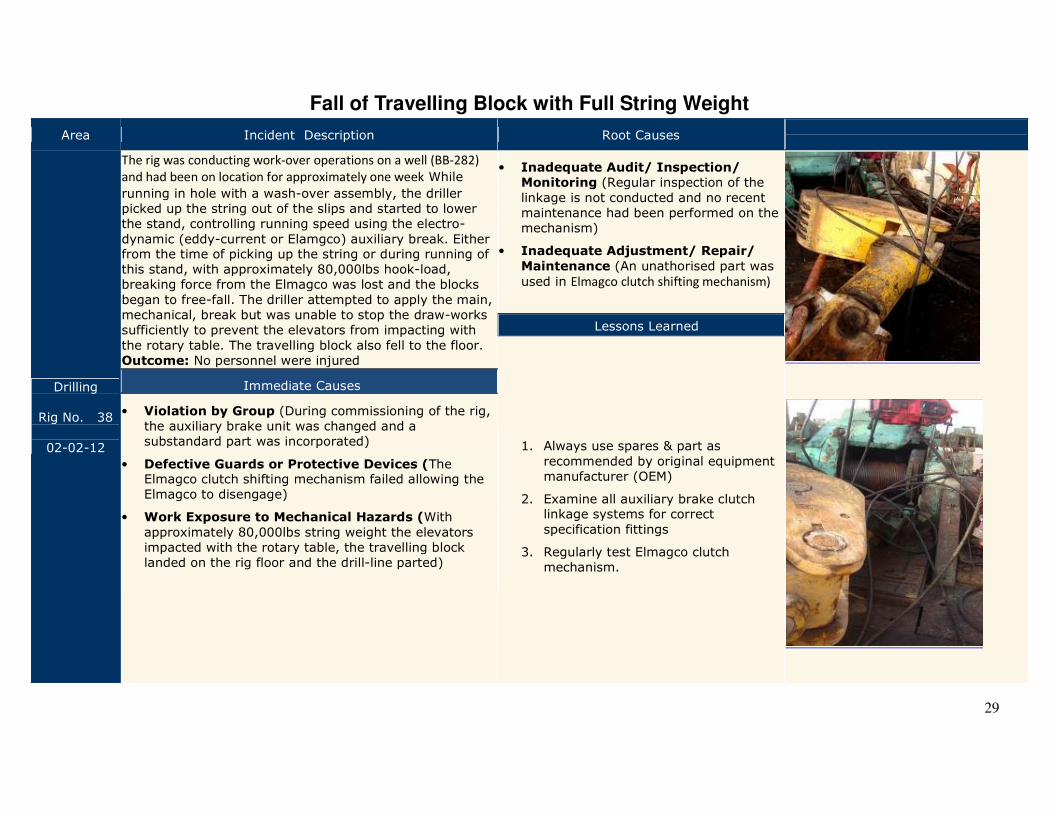
Fall of Travelling Block with Full String Weight
Area Incident Description Root Causes
Drilling
Rig No. 38
02-02-12
The rig was conducting work-over operations on a well (BB-282)
and had been on location for approximately one week While
running in hole with a wash-over assembly, the driller picked up the string out of the slips and started to lower the stand, controlling running speed using the electro-
dynamic (eddy-current or Elamgco) auxiliary break. Either from the time of picking up the string or during running of this stand, with approximately 80,000lbs hook-load, breaking force from the Elmagco was lost and the blocks
began to free-fall. The driller attempted to apply the main, mechanical, break but was unable to stop the draw-works sufficiently to prevent the elevators from impacting with
the rotary table. The travelling block also fell to the floor. Outcome: No personnel were injured
• Inadequate Audit/ Inspection/
Monitoring (Regular inspection of the
linkage is not conducted and no recent maintenance had been performed on the mechanism)
• Inadequate Adjustment/ Repair/
Maintenance (An unathorised part was
used in Elmagco clutch shifting mechanism)
Lessons Learned
1. Always use spares & part as
recommended by original equipment manufacturer (OEM)
2. Examine all auxiliary brake clutch linkage systems for correct
specification fittings
3. Regularly test Elmagco clutch mechanism.
Immediate Causes
• Violation by Group (During commissioning of the rig, the auxiliary brake unit was changed and a substandard part was incorporated)
• Defective Guards or Protective Devices (The Elmagco clutch shifting mechanism failed allowing the Elmagco to disengage)
• Work Exposure to Mechanical Hazards (With
approximately 80,000lbs string weight the elevators impacted with the rotary table, the travelling block landed on the rig floor and the drill-line parted)
30
Gas Release From Coil Tubing
Area Incident Description Root Causes
Drilling
Rig No. 22
21-03-12
The well was drilled as exploratory well and after the production test, it was scheduled for work
over to perforate and test Hith Formation and horizontalization.
During run in hole with coil tubing and lifting the well with nitrogen at depth 370ft from surface,
the coil tubing partially parted (almost 75% from its circle) just 1.5ft before the mechanical depth indicator of the coil causing big sound, nitrogen &
gas with H2S (Hydrogen Sulphide) release to the atmosphere due to failure of dual check valve in the Bottom Hole Assembly (BHA). N2 (Nitrogen) and gas with H2S (1400PMM) was released into
the atmosphere. All the personnel were evacuated and the well was killed by bull-heading with 100bbls of brine water (75pcf). Gas leak was stopped after pumping 15bbls of the brine into
tubing. Outcome: Release of N2 (Nitrogen) and gas with H2S from coil tubing to the atmosphere.
• Inadequate Inspection/Monitoring (Rigless
Supervisor and Drilling Supervisor did not monitor the exposure time; Dual check valve installed with coil tubing BHA and coil tubing reel was not inspected or
tested after acid job and prior lifting job)
• Inadequate Assessment of Required Skills or
competency/Inadequate Job Placement (The assigned Drilling Supervisor lacked experience in acid
treatment job and it was the first time to attend gas production test; Rigless supervisor was shifted to this job just before acid job without adequate handover)
• Inadequate Work Planning (There was no detailed acid program from town and no formal job order for the execution of job from Rigless & Drilling Supervisors to Service Providers on site)
Lessons Learned
1. Do not exceed recipe exposure time during acid job test.
2. Always inspect & test coil tubing & double check valve after acid job
3. Assign competent staff on high risk jobs
Immediate Causes
• Violation by Supervisor (Rigless crew exceeded acid recipe time duration)
• Defective Equipment (Coil tubing lost 70% from its material thickness and partially parted; Double check valve was severely
damaged due to long exposure time for acid 28% during acid treatment).
• Work Exposure to Energized System (Exposure to high pressure sour gas in gas
well)
31
Vehicle Collision Near A Rig Site
Area Incident Description Root Causes
Drilling
NDC Rig 25
24-05-12
Unspool drilling line operation was ongoing and the Drilling Supervisor (DS) decided to go to camp after finishing his tasks at the rig site. He called for his driver and he was on the way to the rig camp using the designated rig road. Rig Crew change vehicle
was approaching the rig site from rig camp at the same time. Both vehicle approached from opposite directions and collided at a
slope.
Outcome: Both vehicle sustained minor damaged on their front right sides.
• Inadequate Identification of
Worksite/Job Hazards (Rig access track design did not mitigate risks of driving on slopes in low visibilities (e.g night driving).
• Inadequate Monitoring (Access track was adequately maintained resulting in sand accumulation at places)
Lesson Learned
1. Avoid driving at night time/low visibility conditions between rig site and rig camp.
2. Regularly maintain access tracks to avoid
accumulation of sand on tracks causing drivers to move towards middle of the track or on the wrong side of the track.
Immediate Causes
• Violation by Individual (Driver of Rig
Crew Move vehicle was driving on the wrong side of the track)
• Lack of Knowledge of Hazards
Present (Drivers were not aware of approaching vehicles due to low visibility and road layout- Slopes)
32
Low Bed Trailer Rollover
Area Incident Description Causes
Drilling
NDC Rig 9
02-06-12
Shifting of a crane from one location to another (Well site No. Sa-220 to Sa231) and was loaded on a low bed trailer. The trailer operator was not aware of the access route to the new location and was travelling in wrong direction. When he realized the error he tried to take a U Turn to return back. Due to sand
accumulation/soft humps and lack of space for turning, the trailer with the crane rolled over. Outcome: The trailed 5th Wheel was damaged and the crane was moved by another crew.
• Improper Supervisory Example (A new & inexperience operator was assigned to transfer the load and the route was not defined/identified)
• Inadequate Assessment of the required
Skill or Competency The driver had only one week experience on low bed trailer and his
competency to operate the trailer with heavy load in field conditions was not assessed and was inadequate)
• Inadequate Communication (The supervisor did not properly identify the route)
Lesson Learned
Immediate Causes
1. Always inspect and identify access route for the
movement of equipment
2. Familiarize new drivers/operators with roads and access routes prior to their assignments
• Improper Decision making/Lack of
Judgment (The operator of low bed trailer
attempted to take a U turn on sand bars/humps)
• Lack of Knowledge of Hazards Present
(The operator of the trailer was not
familiarized with road/access route conditions and hazards associated with the journey)
33
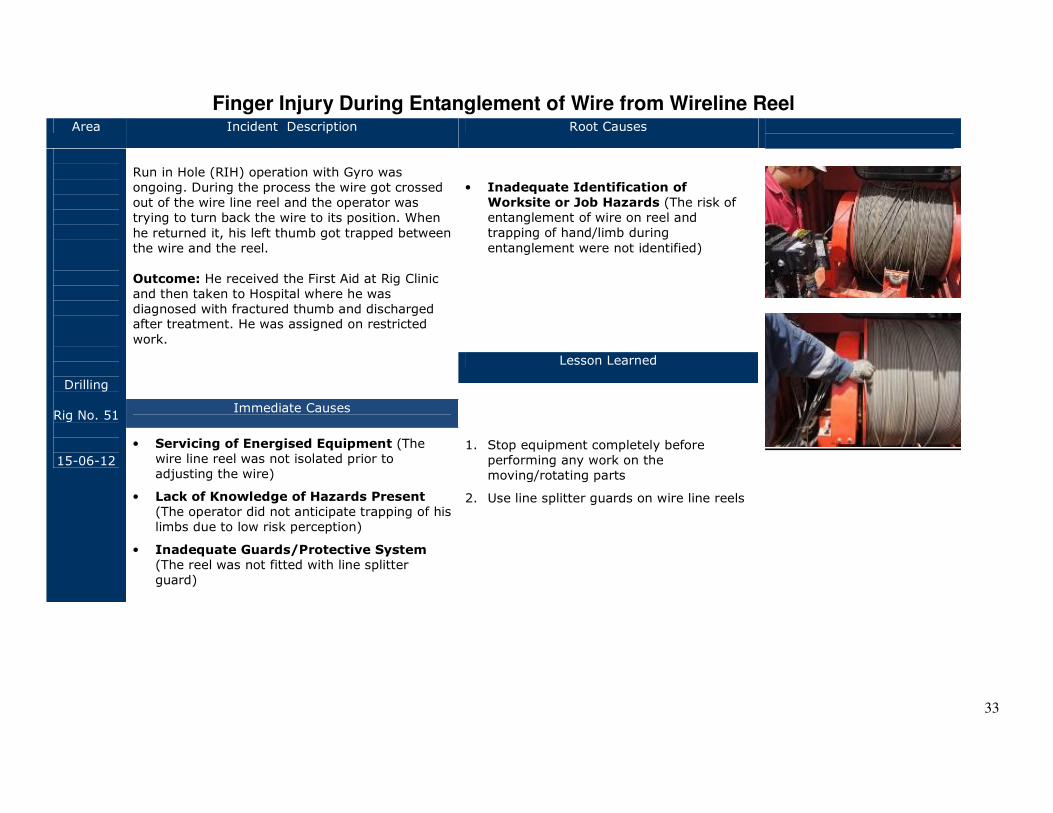
Finger Injury During Entanglement of Wire from Wireline Reel Area Incident Description Root Causes
Drilling
Rig No. 51
15-06-12
Run in Hole (RIH) operation with Gyro was ongoing. During the process the wire got crossed out of the wire line reel and the operator was trying to turn back the wire to its position. When
he returned it, his left thumb got trapped between the wire and the reel.
Outcome: He received the First Aid at Rig Clinic and then taken to Hospital where he was diagnosed with fractured thumb and discharged after treatment. He was assigned on restricted
work.
• Inadequate Identification of
Worksite or Job Hazards (The risk of entanglement of wire on reel and trapping of hand/limb during
entanglement were not identified)
Lesson Learned
1. Stop equipment completely before performing any work on the moving/rotating parts
2. Use line splitter guards on wire line reels
Immediate Causes
• Servicing of Energised Equipment (The wire line reel was not isolated prior to adjusting the wire)
• Lack of Knowledge of Hazards Present (The operator did not anticipate trapping of his limbs due to low risk perception)
• Inadequate Guards/Protective System
(The reel was not fitted with line splitter guard)
34
Release of Oil from Xmas Tree Area Incident Description Root Causes
Drilling
Rig No. 1
05-06-12
A Water Alternating Gas (WAG) well was drilled, and after the rig move X- mas tree was installed by a Wellhead Engineer & set Non Return Valve (NRV- in place but NRV was passing and all X-mas
tree valves were in open position. X-mass tree installation job was not witnessed by Drilling Supervisor or the Rig Manager and the Wellhead
Engineer was not on the list of approved wellhead Engineers. The well location was under preparation prior to well handover for operations. During the location preparation the well was
found flowing from X-mas tree top needle valve. The DS reported the incident and closed all X-Tree valves to secure the well. Outcome: It had resulted in release of well fluid and gases.
Contaminated soil/sand was removed and sent to treatment facility.
• Inadequate Leadership (Unapproved Wellhead Engineer was assigned to install X-mass Tree and the installation was not witnessed by Rig Management)
• Inadequate Planning or Risk
Assessment Performed (Wellhead
Engineer’s competency was not assured and high risk activity was not supervised)
• Lack of Procedure for the Task (There
was no formal well securing procedure in place)
Lesson Learned
1. Drilling Supervisor should witness installation of X-mas Tree and securing
well.
2. Assure Wellhead Engineers’ competency prior to their assignment on high risk
activities
Immediate Causes
• Violation by Individual (The wellhead Engineer did not close Xmas Tree Valves and NRV installation procedure was not followed)
• Violation by Supervisor (Drilling Supervisor did not witness the installation & securing of X-mas Tree)
• Defective Guards or Protective Devices
(NRV was passing)
35
Fall of Foreman from Stand Pipe
Area Incident Description Root Causes
Drilling
NDC Rig 54
18-06-12
Work was planned to connect 2” High Pressure Hose between reverse line and chock manifold and an
Assistant Driller with three roustabouts was moving the hose. A labor foreman, who was not involved in the task (but he was the supervisor of these newly assigned roustabouts – green hats), stepped over the
horizontal section of the stand pipe to observe and assist in pulling the hose.
The Assistant Driller asked him not to stand on the stand pipe but he stayed there for a moment and then he lost his balance resulting in his fall back with his full weight on his left elbow on the compacted sand ground. Outcome: The Labor Foreman
sustained fractured elbow.
• Improper Supervisory Example (The Assistant Driller did not effectively stop the Labor Foreman from standing on standpipe).
• Inadequate Identification of
Worksite/ Job Hazards (The Foreman did not realize of risks of standing on
standpipe and assisting the crew).
Lessons Learned
1. Do not stand on stand pipe or other
similar structures without fall protection equipment.
2. Stop all unsafe actions effectively
3. Supervisor should supervise crew and should not participate in execution of tasks.
Immediate Causes
• Improper Position or Posture for the Task (The Foreman was standing on the standpipe).
• Improper Decision Making/Lack of Judgment
(Forman intended to observe his newly assigned crews and assist them in pulling the hose while standing on the stand pipe).
36
Dropped Object During Lifting
Area Incident Description Root Causes
Drilling
NDC Rig 56
24-06-12
During normal drilling operations at the rig site, a task of removing lifting-sub and crossover
(weighting approximately 250 kg) from rig floor to the ground (33 feet down).
An inexperienced rigger without effective supervision was assigned the task of rigging the
load. Prior to the task, no tool box talk (TBT) or pre job safety meeting was conducted. The rigger used the wire rope sling to attach it to the load by single wrap only and then load was lifted by crane from the rig floor, at height 33ft, to cross over box on the ground. A floor-man noticed that the load was unstable and he requested the rigger to
stop the lifting and advised to secure it through double wrap slinging method. The rigger ignored the advised and continued to lift the load and later, the lifting sub slipped and fell down on the
V-door causing damage to steps of the V-door stair then it is slipped down to the ground. Outcome: No injury to personnel and damage to
three steps of V door stairs.
• Improper Supervisory Example (An inexperienced rigger, without supervision was assigned the rigging task)
• Inadequate Coaching on the Skill (New Rigger was not effectively coached/ mentored by experienced rigger or supervisors prior to the assignment of the task)
• Inadequate /Lack of Safety Meetings (Prior to
the task, no tool box talk (TBT) or pre job safety meeting was conducted)
Lessons Learned
1. Ensure adequate supervision during lifting operations.
2. Attach new riggers with experienced riggers prior to assigning them task independently
3. Conduct Tool Box Talk/ Pre Job Safety prior to all tasks especially high risk activities
Immediate Causes
• Violation by Individual (The rigger did not follow the requirements for safe lifting/rigging
and the load was not secured)
• Improper Lifting (The rigger used one wrap of sling around the load instead of two wraps)
37
Uncontrolled Descend of Travelling Block
Area Incident Description Root Causes
Drilling
NDC Rig 31
28-06-12
During Run In Hole (RIH) operations with fishing assembly, the block with top drive started
descending. Assistant Rig Manager, who was running the operations, attempted to stop but failed when applied brakes with joy stick neutral (Auto Park) position. He then applied the parking
brake, meanwhile the Top Drive (T/D) saver sub pin engaged in Drill Pipe (D/P) box which was stab in and avoided further lowering of Top Drive (T/D), but the block continue descending towards off driller side resulting in drilling lines became loose in mast hoisting system.
Outcome: It resulted in minor damage to
equipment.
• Inadequate adjustment/ repair/
maintenance (Integrity of Draw Work (D/W) & anti-collision system was not assured through
regular maintenance regime)
• Inadequate Practice of Skill (When joy stick controlled brake failed, ARM did not use EDS/VFD)
• Inadequate Procedure for the Task (No
written D/W safe work practices/ guidelines were available in driller cabin
Lessons Learned
1. After each rig move, verify the integrity of Draw Work (D/W) & anti-collision system.
2. Use Disconnect System/ Variable Frequency Drive
(EDS/VFD) to stop any free fall of blocks.
3. Post D/W safe work practices/ guidelines in driller cabin for quick reference
Immediate Causes
• Defective Equipment (Joy Stick controlling the brake malfunctioned)
• Improper Decision Making/Unintentional
Human Error (ARM did not use/activate Emergency Disconnect System (EDS))
38
Power Generator/Engine Fire
Area Incident Description Root Causes
Drilling
NDC Rig 11
02-06-12
During normal drilling operations, two labourers noticed fire at a diesel driven generator and they informed the night shift Assistant Mechanic. The
Mechanic closed the diesel supply line and shut down the engine then labourers used fire extinguishers to extinguish the fire.
Outcome: Minor damage to the engine fuel supply line
• Inadequate Correction of Worksite/Job
Hazards (Similar incident had occurred on 21st
October, 2007, 25th of August, 2009 & 17th May, 2010 at NDC Rig 25, NDC Rig No.2 & NDC Rig No. 17 respectively)
• Inadequate Preventive Maintenance
(Daily/weekly visual checks and Preventive Maintenance programme was not robust enough to identify deteriorated fuel line)
Lessons Learned
1. Develop and implement rigorous testing/replacement of fuel lines after each
Rig move.
2. Maintain fire watch during the operations of generators.
Immediate Causes
• Defective Equipment (Diesel hose line was leaking due to material fatigue/deterioration
and vibration)
• Work Exposure to Extreme Temperature (High temperature at diesel engine surface)
39
Trailer Fire at Rig Camp
Area Incident Description Root Causes
Drilling
NDC Rig 51
06-06-12
After the completion of Rigless operation, equipment (high pressure pump, air compressor,
transfer pump and pipe basket) were loaded on a trailer and the trailer departed from the rig location (Mandar Field) for Abu Dhabi. The driver stopped at Rig Camp (5 km from the Rig for lunch
break), parked the vehicle and went to Mess Hall.
Shortly after, the camp staff observed fire of trailers tires and raised the alarm. The driver separated the truck from the trailer and moved the truck. The camp crew responded and extinguished the fire using 3 water tankers and 10 fire extinguishers.
Outcome: No personnel injury occurred and the trailer and loaded equipment were damaged.
Inadequate Communication Between
Work Groups (Hazards of smoking near parked vehicles were not effectively communicated)
Lessons Learned
1. Provide and mark location of
designated smoking areas
2. Do not smoke near parked vehicles.
Immediate Causes
Violation by Individual (Smoking cigarette in non-smoking areas)
Lack of knowledge of Hazards Present
(Smoker was not aware of hazards of smoking near truck)
40
Water Tanker Rollover
Area Incident Description Root Causes
Drilling
21-07-12
For a cementing job, 500 barrels (bbls) of freshwater delivery was required at the rig site
and an urgent delivery request was sent to water supply contractor. The contractor assigned tankers & drivers were not available and therefore a new driver and a tanker was sent from Musafah
Base to make this delivery. The driver did not have ADCO Safe Driving Document (ADSD) and the vehicle was not fitted with In Vehicle Monitoring System (IVMS).
It was the first day of Ramadan and the driver missed his Dinner & Sahur and made a delivery of water. After the delivery he went back to his
camp to refill tanker and then again proceeded to the rig site for another delivery. The air conditioning system in driver’s cabin was not working and it was a hot day and the driver was
working in excess of six hours. During the trip the driver felt dizzy and lost control of the tanker. It resulted in tanker to rollover. Outcome: The
driver escaped unhurt and the tanker sustained minor damage.
• Inadequate Leadership (Knowingly an untrained driver was assigned on the task)
• Inadequate Work Planning (Request for supply large quantity of water was made
without ensuring availability of contractor’s resources)
• Inadequate Audit/ Inspection/
Monitoring (There was no monitoring
system in place to check contractor compliance with contractual requirements for the safety of driver and vehicles)
Lessons Learned
1. Assess availability of contractors’ resources prior to issuing task order.
2. Monitor contractor compliance with
contractual requirements for the safety of driver and vehicles.
Immediate Causes
• Violation by Supervisor (A new driver, without ADSD was assigned to the task; Unauthorized vehicle was used)
• Defective Vehicle (Air conditioning unit in driver’s cabin was not working)
• Work Exposure to Temperature Extreme (The driver was fasting, working over 6 hours
during peak summer hours in hot cabin of the water tanker)
41
Hand Entrapment Inside Tong
Area Incident Description Root Causes
Drilling
NDC Rig 21
03-08-12
While an inexperienced tubular services operator was working as a tong operator, he
had his left hand at the top of the tong rotary while the other hand was on the lever adjusting the tong rotary.
His supervisor left the Rig Floor leaving the
operator alone before completing the job. When he started to operate the tong, the tong jumped resulted in slippage of his left hand which got trapped inside the tong.
Outcome: Tong Operator sustained an open displaced fracture on his left hand.
• Inadequate Leadership (Senior Operator left the inexperienced operator at the rig floor before completing the job; Rig crew did not
stop “Green Hat” – (New or Inexperienced Worker) from working alone)
• Inadequate Identification of Required
Skill or Competency (Inexperienced
operator was not adequately coached on required skills to work independently)
Lessons Learned
1. Do not leave in experienced staff (Green Hat) workers unsupervised at hazardous locations such as Rig Floor
2. Include all sequence of works (such as operations as well as any repair/ troubleshooting) in Job Safety Analysis (JSA)
Immediate Causes
• Improper Posture/Position for the
Task (The operator had placed his hand on the top of tong rotary while adjusting the rotary)
• Lack of Knowledge of Hazards Present (The Supervisor left the operator working alone on the rig floor; the operator was not adequately trained to recognize pinch
points on power tongs)
• Work Exposure to Mechanical Hazards
(Power Tong at Rig Floor)
42
Electrical Shock
Area Incident Description Root Causes
Drilling
NDC Rig 55
06-09-12
The electrical panel door of the fire unit fall down due to broken hinges (caused by the deterioration of pin in the hinges) resulting in cables
cut/damage inside the panel.
An isolation certificate and permit to work was issued. The damaged/cut cables were fixed/replaced by an electrician. After electrical cables were fixed, the electrician restored the power supply and started to check cables voltage using a portable voltmeter. During the process an
electrical spark occurred.
Outcome: It has resulted in a second degree burn on electrician’s right hand thumb.
• Inadequate Practice of Skills (The electrician did not systematically check the electrical system and did not ensure physical protection from coming in contact with live conductor)
• Excessive Wear & Tear (Due to harsh climatic conditions and rig move, hinge pins were deteriorated)
Lessons Learned
1. Always follow systematic way of checking
electrical circuit
2. Stay clear of live conductors when servicing energized electrical system
3. After each rig move visually check the integrity of hinge pins
4. Conduct trade relate workshops for experience electricians to share their knowledge and incident
lessons learned.
Immediate Causes
• Servicing of Energized System (The Electrician was checking cables voltage using a portable voltmeter on a live system)
• Improper Decision Making/Lack of
judgement (The Electrician made a physical contact with a live conductor)
43
Arm Injury Due to Fall of Jumbo Bag
Area Incident Description Root Causes
Drilling
NDC Rig 11
29-10-12
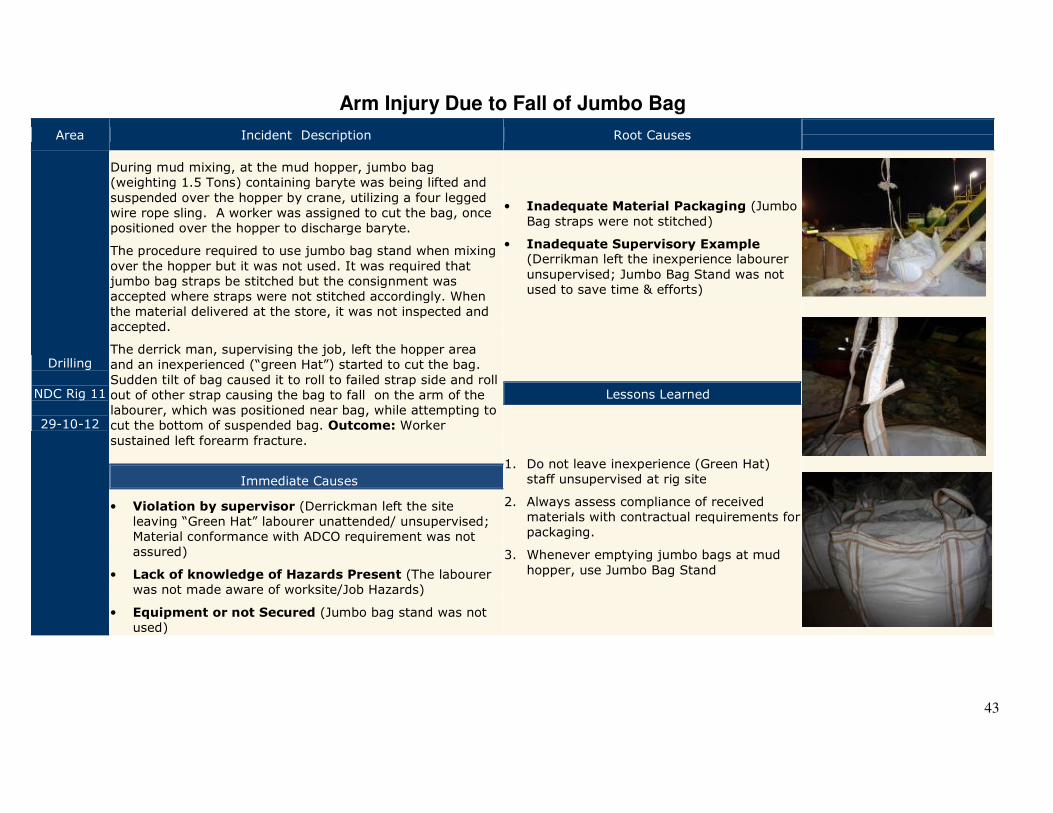
During mud mixing, at the mud hopper, jumbo bag (weighting 1.5 Tons) containing baryte was being lifted and
suspended over the hopper by crane, utilizing a four legged wire rope sling. A worker was assigned to cut the bag, once positioned over the hopper to discharge baryte.
The procedure required to use jumbo bag stand when mixing
over the hopper but it was not used. It was required that jumbo bag straps be stitched but the consignment was accepted where straps were not stitched accordingly. When the material delivered at the store, it was not inspected and accepted.
The derrick man, supervising the job, left the hopper area and an inexperienced (“green Hat”) started to cut the bag.
Sudden tilt of bag caused it to roll to failed strap side and roll out of other strap causing the bag to fall on the arm of the labourer, which was positioned near bag, while attempting to cut the bottom of suspended bag. Outcome: Worker
sustained left forearm fracture.
• Inadequate Material Packaging (Jumbo
Bag straps were not stitched)
• Inadequate Supervisory Example (Derrikman left the inexperience labourer
unsupervised; Jumbo Bag Stand was not used to save time & efforts)
Lessons Learned
1. Do not leave inexperience (Green Hat) staff unsupervised at rig site
2. Always assess compliance of received materials with contractual requirements for packaging.
3. Whenever emptying jumbo bags at mud
hopper, use Jumbo Bag Stand
Immediate Causes
• Violation by supervisor (Derrickman left the site leaving “Green Hat” labourer unattended/ unsupervised; Material conformance with ADCO requirement was not assured)
• Lack of knowledge of Hazards Present (The labourer was not made aware of worksite/Job Hazards)
• Equipment or not Secured (Jumbo bag stand was not used)
44
Falling Object
Area Incident Description Root Causes
Drilling
NDC Rig 57
28-10-12
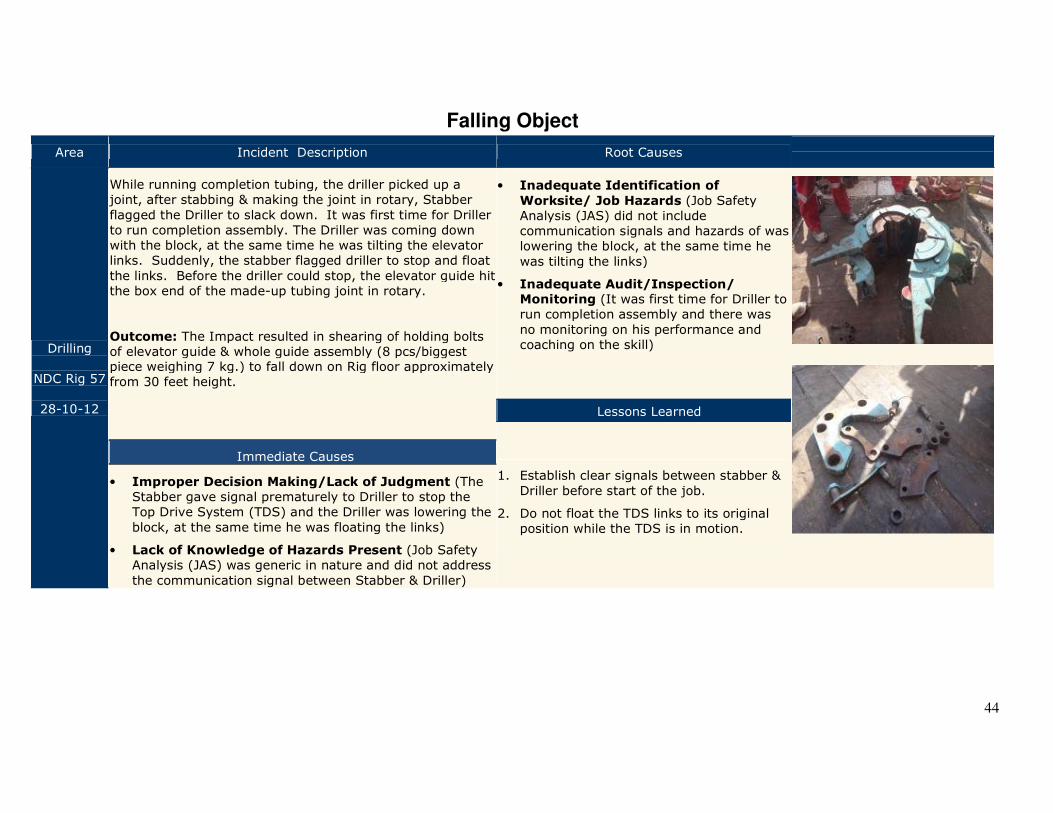
While running completion tubing, the driller picked up a joint, after stabbing & making the joint in rotary, Stabber
flagged the Driller to slack down. It was first time for Driller to run completion assembly. The Driller was coming down with the block, at the same time he was tilting the elevator links. Suddenly, the stabber flagged driller to stop and float
the links. Before the driller could stop, the elevator guide hit the box end of the made-up tubing joint in rotary.
Outcome: The Impact resulted in shearing of holding bolts of elevator guide & whole guide assembly (8 pcs/biggest piece weighing 7 kg.) to fall down on Rig floor approximately from 30 feet height.
• Inadequate Identification of
Worksite/ Job Hazards (Job Safety Analysis (JAS) did not include communication signals and hazards of was lowering the block, at the same time he
was tilting the links)
• Inadequate Audit/Inspection/ Monitoring (It was first time for Driller to run completion assembly and there was
no monitoring on his performance and coaching on the skill)
Lessons Learned
1. Establish clear signals between stabber &
Driller before start of the job.
2. Do not float the TDS links to its original position while the TDS is in motion.
Immediate Causes
• Improper Decision Making/Lack of Judgment (The Stabber gave signal prematurely to Driller to stop the Top Drive System (TDS) and the Driller was lowering the
block, at the same time he was floating the links)
• Lack of Knowledge of Hazards Present (Job Safety Analysis (JAS) was generic in nature and did not address
the communication signal between Stabber & Driller)
45
Engineering & Projects

46
47
Past Incidents
Cement Mixer Truck Rollover (12-06-
2010)
Head on Collision (03-03-2010)
Tipper Truck Rollover 28-04-2010)
Leg Trap in Potable Cement Mixer
(17-07-2011)
Worker Ran Over by Water Tanker
02-08-2011)
Flagman Ran Over by Wheel dozer
(17-08-2011)
Fall of Worker from Height (10-09-
2011)
Hand Injury During Cable Pulling
(17-04-2010)
Vehicle Rollover (18-01-2011)
Fatal Injuries to Rigger (22-01-2011)
Tipper Truck rollover (14-02-2011)
Death of a Worker from Heat Stress (24-08-2010)
48
49
Fire Due to Poor Grounding During Welding
Area Incident Description Root Causes
Engineering & Projects
Sahil Field
03-01-12
Welding job at a pipe rack was planned and Permit to Work (PTW) issued. The task risk assessment (TRA) identified the risk and need for proper grounding was identified. The
work was in progress and the welder assigned a helper to set up the welding station and during the set up, the helper connected the grounding clamp to an incorrect spool. The helper placed the grounding clamp on another
spool because there was no place available to place grounding clamp of the spool the welding job was being carried. The clamp was in contact with a scaffolding (wooden) plank.
Outcome: During the welding job, current passed through
the grounding clamp, warming it up causing smoldering in adjacent scaffolding plank. The crew stopped the operation and extinguished the fire.
• Inadequate Audit/Inspection
/Monitoring (Job Performer as well as the welder did not inspect the set up of
welding station (as highlighted in Task Risk Assessment) prior to start of welding)
• Inadequate Leadership (Permit issuing
authority did not ensure adequate grounding prior to issuing the permit; (Job Performer did not discuss task related hazards with his crew)
• Lack of Procedure for the Task (There was no formal work procedure or checklist available)
Lessons Learned
1. Check and ensure proper Grounding /
Earthing of welding stations prior to commence welding
2. Conduct task specific Tool Box Talk (TBT) discussion hazards and control
3. Permit Issuing Authority (IA) & Job Performers (JP) must assess/check system, readiness prior to issuance of
permit and start of work
Immediate Causes
• Violation by Supervisor (Welder did not check the
adequacy of grounding prior to starting welding; Job Performer (JP) did not supervise welding operations and did not conduct specific tool box talk; PTW Issuing
Authority (IA) issued the permit without confirming grounding and confirmed adequacy of grounding on the permit)
• Improper Placement of Tools/ Equipment
(Grounding clamp was placed on wrong spool which was contacting a wooden plank)
• Congestion or Restricted Movement (The work location did not provide clear location for grounding)
50
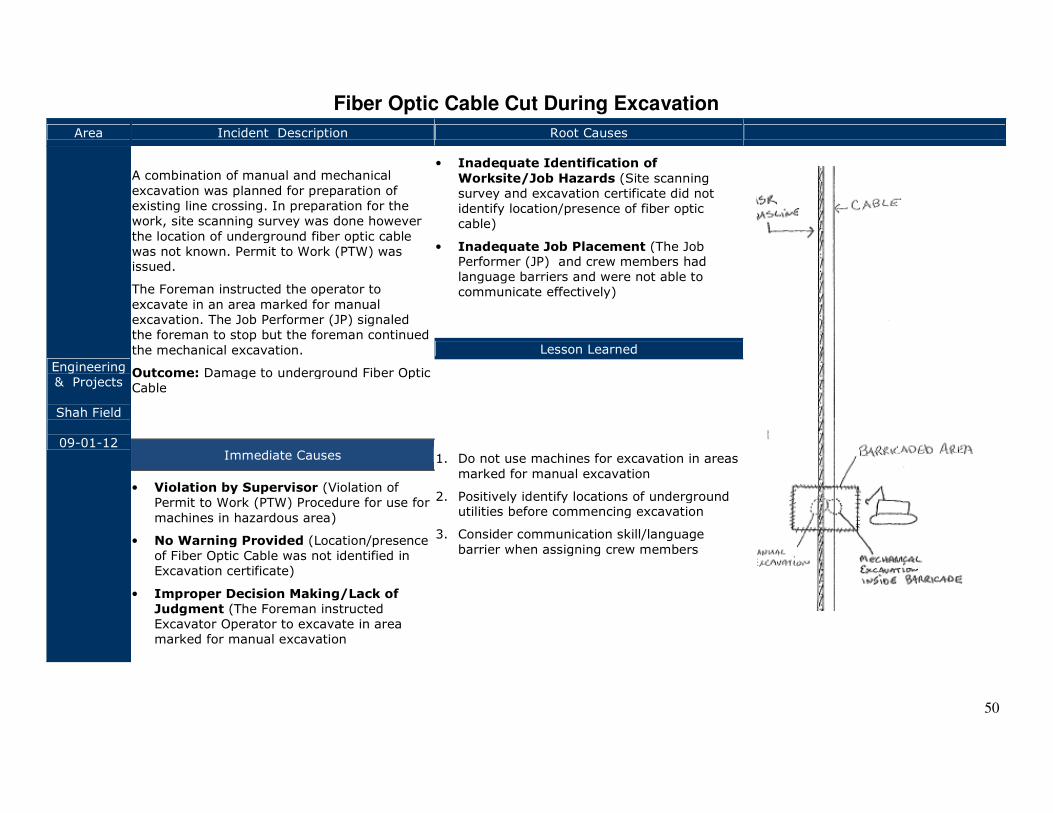
Fiber Optic Cable Cut During Excavation
Area Incident Description Root Causes
Engineering & Projects
Shah Field
09-01-12
A combination of manual and mechanical
excavation was planned for preparation of existing line crossing. In preparation for the work, site scanning survey was done however
the location of underground fiber optic cable was not known. Permit to Work (PTW) was issued.
The Foreman instructed the operator to
excavate in an area marked for manual excavation. The Job Performer (JP) signaled the foreman to stop but the foreman continued
the mechanical excavation.
Outcome: Damage to underground Fiber Optic Cable
• Inadequate Identification of
Worksite/Job Hazards (Site scanning survey and excavation certificate did not identify location/presence of fiber optic cable)
• Inadequate Job Placement (The Job Performer (JP) and crew members had language barriers and were not able to communicate effectively)
Lesson Learned
1. Do not use machines for excavation in areas
marked for manual excavation
2. Positively identify locations of underground utilities before commencing excavation
3. Consider communication skill/language
barrier when assigning crew members
Immediate Causes
• Violation by Supervisor (Violation of Permit to Work (PTW) Procedure for use for
machines in hazardous area)
• No Warning Provided (Location/presence of Fiber Optic Cable was not identified in Excavation certificate)
• Improper Decision Making/Lack of
Judgment (The Foreman instructed Excavator Operator to excavate in area marked for manual excavation
51
Vehicle Collision & Rollover
Area Incident Description Root Causes
Engineering & Projects
Bab Field
30-01-12
Due to pre commissioning of Gas Compression Station No. 2, there were increased activities and working hours were extended to meet the schedule. A project driver pick up driver was supporting crew and staff movement
between offices and work sites and over the last one week the driver was working between upto 15 Hrs a day with irregular breaks/rest.
The driver was proceeding to Gas Compressor Station to collect staff. When he entered Habshan –Buhasa Road, his
pickup vehicle was hit by an oncoming bus. It resulted in pickup vehicle to rollover. Outcome: The driver sustained minor injuries on his hands and the vehicle
was badly damaged
• Inadequate Inspection & Monitoring (There was no monitoring system in
place to monitor drivers working conditions)
• Inadequate Implementation of PSP
(Procedure/ Standards/Policy)
(Drivers RAG (Driving Behaviour) Reports were not adequately reviewed)
• Inadequate Work Planning (Due to pre commissioning activities working hours were increased without sourcing additional manpower; Night time driving request form did not include assessment
of risks)
Lesson Learned
1. Monitor drivers working conditions and review RAG (deriving behaviour) reports regularly
2. Conduct Risk Assessment prior to approving night time driving request.
Immediate Causes
• Inattention to Footing &
Surroundings (Driver misjudge the speed of approaching vehicle and
started to cross the road)
• Overexertion of Physical
Capabilities (The driver was working
upto 15 Hrs a day with irregular breaks/rest resulting in loss of concentration and fatigue)
• Violation by Supervisor (Night time
driving approval was not subjected to risk assessment)
52
Asphyxiation of Welder Inside A Pipe
Area Incident Description Root Causes
Engineering & Projects
Sahil Field
06-02-12
Piping erection work was in progress and a welding crew was engaged in welding of 30 Inch diameter pipe joint. Due to leakage of Argon gas from argon dam foam pads, welding could not proceed further as it
could have oxidized welds and compromised the quality of welding.
To fix the problem, pipe joint needed to be cut and then Argon Purge Dam Pads adjusted. This process
could have resulted in 1-2 days delay. The crew resolved the issue in about an hour (Foremen sent a welder inside the pipe (without confined space entry certificate) to adjust foam pads) and welders
proceeded with the rest of the welding. The next day, after completing welding, the same welder went inside the pipe and he collapsed inside the pipe and asphyxiated. Outcome: Crew members tried to recover and evacuate the welder to site Clinic and he was pronounced dead by the Physician upon arrival.
• Inadequate Assessment of Needs & Risks (Home-made type Argon Gas Dam foam pads were used resulting in leakage instead of using inflatable or other type of dam pads)
• Inadequate Supervisory Example (Conflicting roles & responsibilities of JPs and foremen created
an environment where no one felt accountable/responsible, Supervisor exposed workers to risks for the sake of meeting time line)
• Inadequate Audit/Inspection/ Monitoring (For this welding crew audit/ inspection/ monitoring of PTW & TBT and safe work flow was inadequate for welders, there was no monitoring system to assess
quality of TRA prepared)
• Inadequate Training (Contractor Job Performer and Foreman were not trained in conducting Tool
Box Talk (TBT; Welders were subjected to intensive HSE training without effective feed-back to assess their knowledge; Confined space training was inadequate to all members of the welding crew)
Immediate Causes
• Violation by Individual (The welder made unauthorized confined space entry in pipe; Co-welder did not stop welder entering the pipe; Job Performer (JP) and welding supervisor were not supervising welders after welding task was
completed and left them at the site unattended)
• Lack of Knowledge of Hazards Present (Welders were not aware of asphyxiation hazards
due to Argon gas escaping from leaking foam pads ; over confidence due to earlier entry into the pipe, Lessons learned from incidents were not shared with welders; No specific Tool Box Talk (TBT) for
welders was conducted
Lesson Learned
1. Do not use any sub-standard or home-made type
tool/equipment at work site
2. Do not enter pipes or other confined spaces unless confined space entry permits are obtained
3. Do not leave workers unsupervised at work site
especially during high risk activities
4. We all are authorized (by ADCO Chief Executive Officer) to stop any unsafe action in ADCO work
areas.
5. Educate yourself with risks associated with your job
53
Man Lift Drove Over Flagman’s Foot
Area Incident Description Root Causes
Engineering & Projects
Bab Field
15-03-12
A crew (Man Lift Operator & Banksman/ Flagman) was relocating man-lift from one location to another for a paint touch-up work. On the way, a forklift was approaching from the opposite
direction and Flagman signaled to the man-lift operator to stop, allowing the forklift to pass.
The Flagman stepped towards the man-lift to get out of the way of the passing forklift. When the forklift had passed, the man-lift Operator started to move the man-lift without any signal from the flagman or confirming his location. The operator
drove the man lift over Flagman’s right foot. The Flagman was taken to the site clinic and then referred to hospital for further assessment.
Outcome: Flagman sustained minor foot injury
• Inadequate Practice of Skill (Man-lift operator started moving the man-lift without
taking a signal from the Banksman/ Flagman)
• Inadequate Safety Meetings (No specific TBT was conducted for machinery/ equipments
operators & Banksmen/ Flagmen)
• Inadequate Communication Between Work
Groups (Simultaneous operations were taking place at the same area without any
coordination within Job Performers (JPs))
Lesson Learned
1. Do not move heavy machines/ equipment
unless directed by Banksmen/Flagmen.
2. Machine/equipment operators must maintain clear sight of Banksmen/ Flagmen.
3. Conduct task specific Tool Box Talk (TBT) for
each crew.
Immediate Causes
• Violation by Individual (Man-lift operator started moving the man-lift without signal from Banksman/ Flagman and did not maintain clear sight of Banksman/ Flagman)
• Improper Position for the Task (Banksman/
Flagman was standing close to the man-lift)
54
Vehicle Rollover
Area Incident Description Root Causes
Engineering & Projects
Buhasa Field
19-02-12
An instrument commissioning Engineer was involved in integration communication system in Central Degassing Station (CDS). The engineer was based in Mussafah and travelled
to Bu Hasa in a private vehicle and he did not have ADCO Safe Driving Document (ADSD). After finishing his tasks (approximately at 17:30 Hrs) he was on his way back to Abu
Dhabi. Earlier, there was a sand storm resulting in sand accumulation (sand bars) on the road and when he drove over sand bars,
he lost control of the vehicle, resulting in the vehicle to roll over. Outcome: The driver sustained shoulder injury and the vehicle was badly damaged.
• Inadequate Communication of Policies,
Standards and Procedures (ADCO Road
Safety requirements were not adequately communicated to the subcontractor/vendor)
• Inadequate Supervisory Example (Supervisors did not arrange for company
vehicle and/or trained driver for the journey)
• Inadequate Work Planning (Supervisor did not monitor the commissioning engineer’s work schedule)
• Inadequate Inspection & Monitoring (Contractor did not adequately monitor compliance with ADCO Road Safety
requirements.)
Lesson Learned
1. Do not drive private vehicle on ADCO business.
2. Only assign trained drivers to drive or provide drivers for staff transit.
3. Supervisors should monitor compliance of their contractor staff with ADCO Road Safety Requirements.
Immediate Causes
• Violation by Supervisors (Allowed the use of private vehicle to travel to fields.)
• Inattention to footing & Surroundings
(Staff was working for the last 11 hours including the 2.5 hrs journey to site and did not pay attention to road conditions
(sand accumulation) due to fatigue)
55
Vehicle Collision on a Sand Track
Area Incident Description Root Causes
Engineering & Projects
Qw
28-02-12
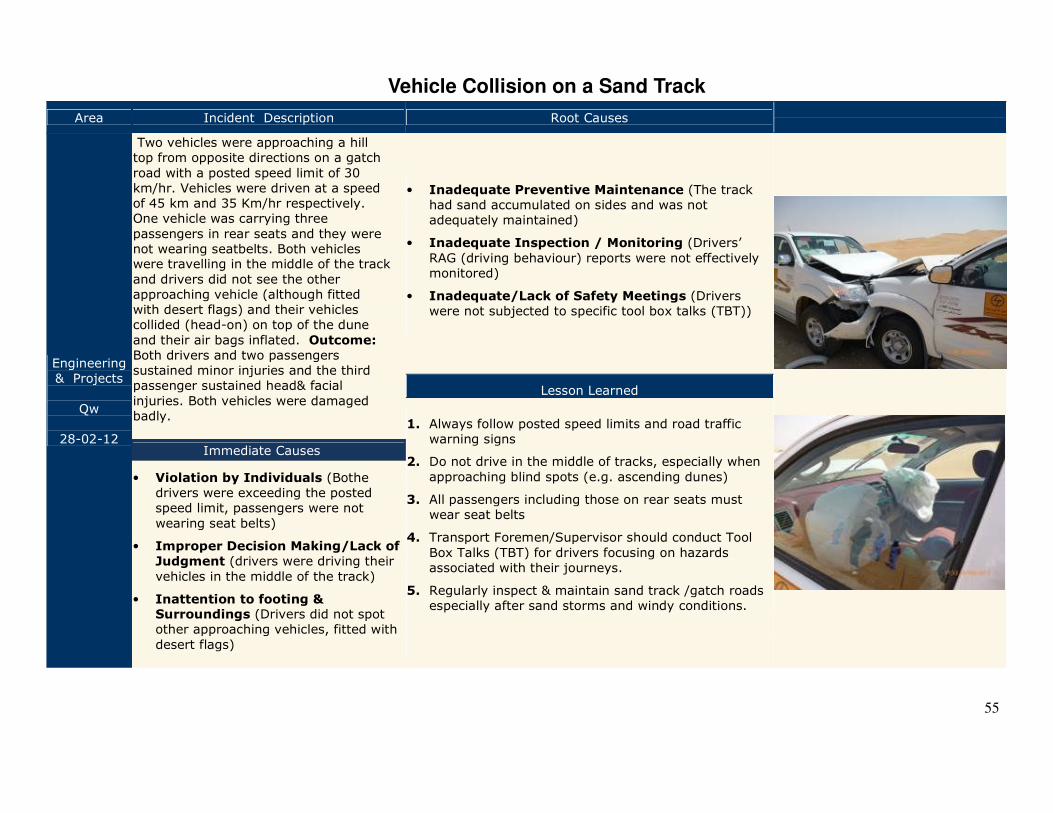
Two vehicles were approaching a hill top from opposite directions on a gatch
road with a posted speed limit of 30 km/hr. Vehicles were driven at a speed of 45 km and 35 Km/hr respectively. One vehicle was carrying three
passengers in rear seats and they were not wearing seatbelts. Both vehicles were travelling in the middle of the track
and drivers did not see the other approaching vehicle (although fitted with desert flags) and their vehicles collided (head-on) on top of the dune
and their air bags inflated. Outcome: Both drivers and two passengers sustained minor injuries and the third passenger sustained head& facial
injuries. Both vehicles were damaged badly.
• Inadequate Preventive Maintenance (The track had sand accumulated on sides and was not adequately maintained)
• Inadequate Inspection / Monitoring (Drivers’
RAG (driving behaviour) reports were not effectively monitored)
• Inadequate/Lack of Safety Meetings (Drivers were not subjected to specific tool box talks (TBT))
Lesson Learned
1. Always follow posted speed limits and road traffic warning signs
2. Do not drive in the middle of tracks, especially when
approaching blind spots (e.g. ascending dunes)
3. All passengers including those on rear seats must wear seat belts
4. Transport Foremen/Supervisor should conduct Tool
Box Talks (TBT) for drivers focusing on hazards associated with their journeys.
5. Regularly inspect & maintain sand track /gatch roads especially after sand storms and windy conditions.
Immediate Causes
• Violation by Individuals (Bothe drivers were exceeding the posted speed limit, passengers were not
wearing seat belts)
• Improper Decision Making/Lack of
Judgment (drivers were driving their
vehicles in the middle of the track)
• Inattention to footing & Surroundings (Drivers did not spot other approaching vehicles, fitted with
desert flags)
56
Vehicle Drove Over a Berm
Area Incident Description Root Causes
Engineering & Projects
Asab Field
01-03-12
A crew consisting of a driver, Foreman and three labourers were proceeding to MOL MP-24 location in a double cabin
pickup. The purpose of the trip was to retrieve Permit to Work (PTW) papers from a bus which was stuck in sand and was immobilized a day before. The driver was using the blue key of the Foreman (sitting next him). The driver
did not engage vehicle into 4x4 mode and driving at a speed of 105 km/hr. There was low visibility due to early hours and hazy conditions. One of the labourers, sitting in the rear middle seat did not fasten his seatbelt.
The driver was not familiar with the access track and he did not notice the pipe line crossing ahead of them. He drove over pipe line berm. As an impact; the vehicle hit
the berm, jumped over the berm and landed on the front bumper.
Outcome: Three occupant sustained injuries and two were discharged after the treatment from the hospital. The
third labourer was admitted for three days in the hospital and then discharged.
• Inadequate Supervisory Example
(Supervisor reinforced incorrect behaviour of the driver)
• Inadequate/Lack of Safety Meetings (Drivers were not subjected to specific tool box talks (TBT))
• Inadequate Inspection / Monitoring (Drivers’ RAG (driving behaviour) reports were not effectively monitored)
• Inadequate Implementation of
Policies/ Standards/ Procedures (PSP) (ADCO road safety requirements and Life Protection Rules (LPRs) were not effectively implemented.
Lesson Learned
1. Always follow posted speed limits and road traffic warning signs
2. All passengers including those on rear seats must wear seat belts
3. Transport Foremen/Supervisor should
conduct Tool Box Talks (TBT) for drivers focusing on hazards associated with their journeys.
4. Supervisors should review drivers’ RAG
(driving behaviour) reports regularly and provide counseling to drivers to reinforce correct driving behaviour.
Immediate Causes
• Violation by Individual (The driver was over speeding, did not engage vehicle in 4x4 mode)
• Violation by Supervisor (He gave his blue key to the driver and did not stop driver from over speeding)
• Improper Decision Making/Lack of Judgment
(Driver continued driving during low visibility on an unknown track)
57
Cement Mixer Rollover
Area Incident Description Root Causes
Engineering & Projects
Shah Field
18-04-12
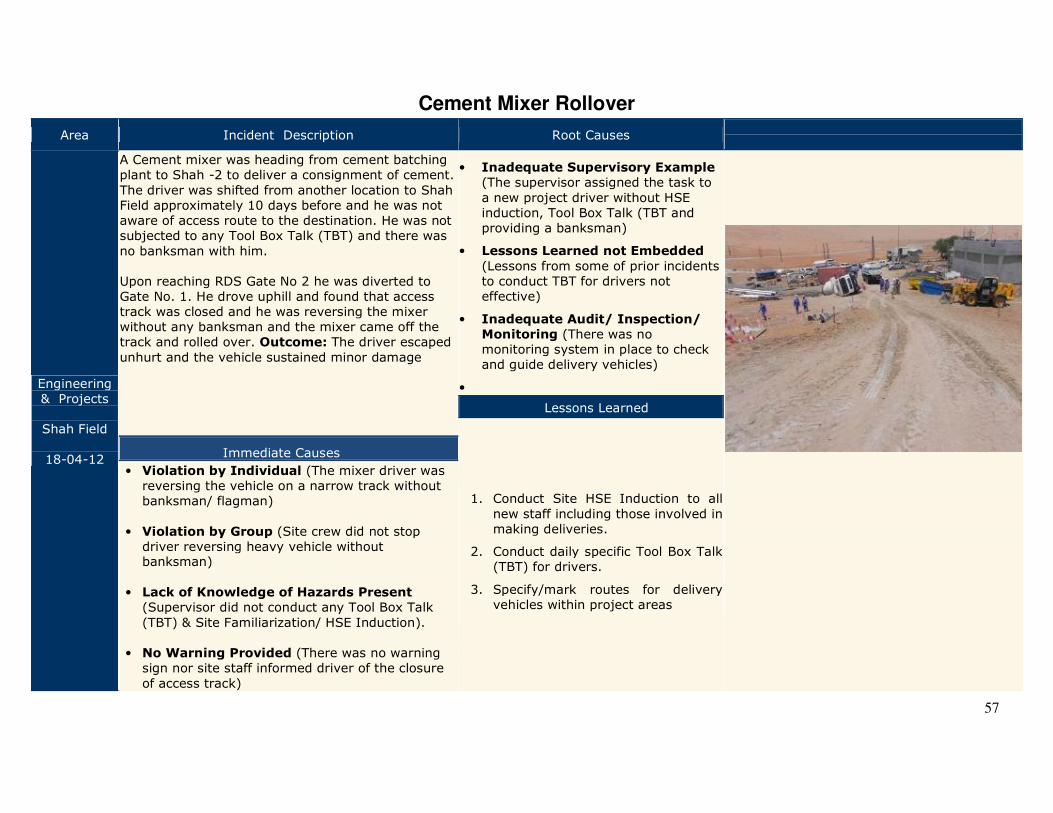
A Cement mixer was heading from cement batching plant to Shah -2 to deliver a consignment of cement.
The driver was shifted from another location to Shah Field approximately 10 days before and he was not aware of access route to the destination. He was not subjected to any Tool Box Talk (TBT) and there was
no banksman with him. Upon reaching RDS Gate No 2 he was diverted to Gate No. 1. He drove uphill and found that access track was closed and he was reversing the mixer without any banksman and the mixer came off the track and rolled over. Outcome: The driver escaped
unhurt and the vehicle sustained minor damage
• Inadequate Supervisory Example (The supervisor assigned the task to
a new project driver without HSE induction, Tool Box Talk (TBT and providing a banksman)
• Lessons Learned not Embedded
(Lessons from some of prior incidents to conduct TBT for drivers not effective)
• Inadequate Audit/ Inspection/
Monitoring (There was no monitoring system in place to check and guide delivery vehicles)
•
Lessons Learned
1. Conduct Site HSE Induction to all
new staff including those involved in making deliveries.
2. Conduct daily specific Tool Box Talk (TBT) for drivers.
3. Specify/mark routes for delivery vehicles within project areas
Immediate Causes
• Violation by Individual (The mixer driver was reversing the vehicle on a narrow track without banksman/ flagman)
• Violation by Group (Site crew did not stop driver reversing heavy vehicle without banksman)
• Lack of Knowledge of Hazards Present (Supervisor did not conduct any Tool Box Talk
(TBT) & Site Familiarization/ HSE Induction). • No Warning Provided (There was no warning sign nor site staff informed driver of the closure
of access track)
58
Damage to Overhead Line
Area Incident Description Root Causes
Engineering
& Projects
BAB Field
24-04-12
A contractor crew was involved in stringing, welding and support installation of a new flowline and an excavator operator was hired
from a sub-contractor. The operator was mobilized to the site without any HSE Induction and he was not included in Tool Box Talk
(TBT). Piping Foreman was preparing the site and requested Excavator Operator to move the excavator closer to the work site. The
excavator driver mover the excavator with his boom in extended position and struck against 33KV overhead line conductors.
Outcome: The overhead line tripped on earth fault. The operator came out of the excavator safely
• Inadequate Identification of Worksite/
Job Hazards (The Task Risk Assessment (TRA) did not identify the hazard)
• Inadequate Training Efforts (TRA team was not adequately trained in conducting
TRAs; Excavator operator was not subjected to site HSE induction and was not included in Tool Box Talk (TBT))
• Inadequate Monitoring (Foreman or Job
Performer did not monitor excavator operator’s movement)
(For Illustration Purpose)
Lesson Learned
1. Install goal posts at crossing under over head line conductors prior to initiating site works involving movement of equipment.
2. Include vehicle/equipment operators in Tool Box Talks (TBT)
3. Do not operate equipment/machinery when
emotionally disturbed or stressed
Immediate Causes
• Unintentional Human Error (Excavator
Operator moved the equipment with the boom in elevated position)
• Distracted by Other Concerns (The operator was emotionally stressed due to
personal issues)
• Inadequate Guards or Protective
Devices (There no goal post/height level markers was installed at overhead line crossing)
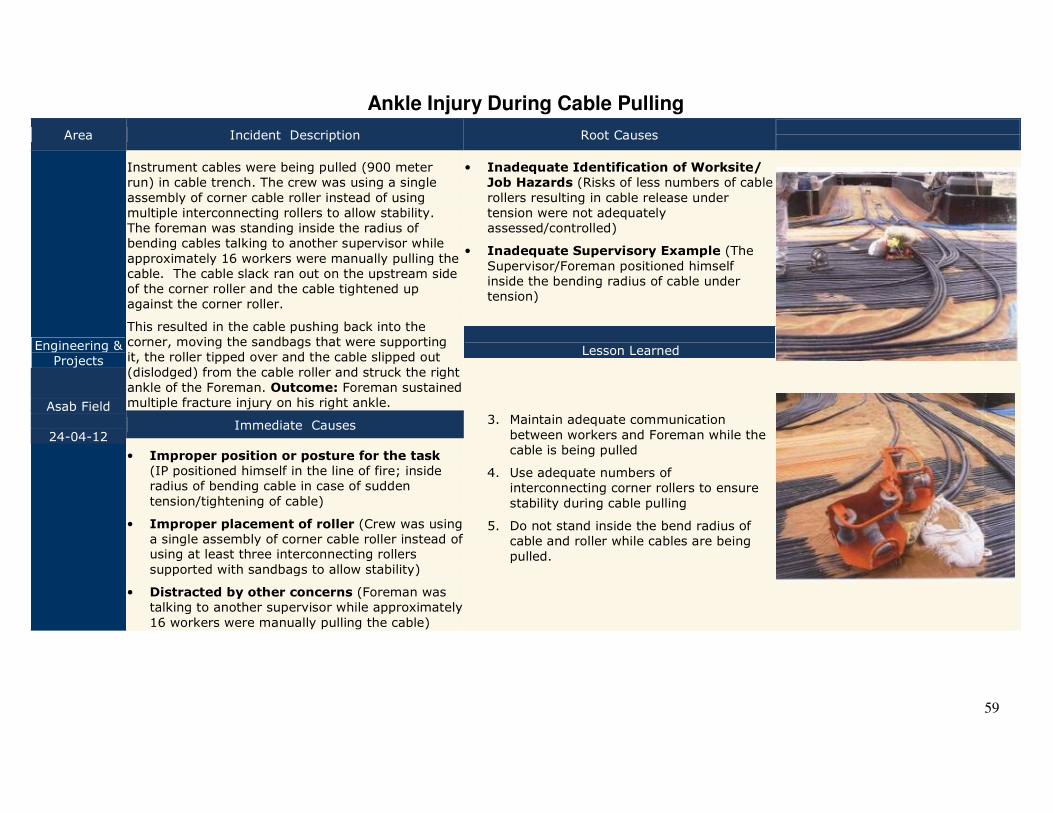
59
Ankle Injury During Cable Pulling
Area Incident Description Root Causes
Engineering & Projects
Asab Field
24-04-12
Instrument cables were being pulled (900 meter run) in cable trench. The crew was using a single
assembly of corner cable roller instead of using multiple interconnecting rollers to allow stability. The foreman was standing inside the radius of bending cables talking to another supervisor while
approximately 16 workers were manually pulling the cable. The cable slack ran out on the upstream side of the corner roller and the cable tightened up against the corner roller.
This resulted in the cable pushing back into the corner, moving the sandbags that were supporting it, the roller tipped over and the cable slipped out
(dislodged) from the cable roller and struck the right ankle of the Foreman. Outcome: Foreman sustained multiple fracture injury on his right ankle.
• Inadequate Identification of Worksite/
Job Hazards (Risks of less numbers of cable
rollers resulting in cable release under tension were not adequately assessed/controlled)
• Inadequate Supervisory Example (The
Supervisor/Foreman positioned himself inside the bending radius of cable under tension)
Lesson Learned
3. Maintain adequate communication
between workers and Foreman while the cable is being pulled
4. Use adequate numbers of interconnecting corner rollers to ensure
stability during cable pulling
5. Do not stand inside the bend radius of cable and roller while cables are being
pulled.
Immediate Causes
• Improper position or posture for the task
(IP positioned himself in the line of fire; inside radius of bending cable in case of sudden
tension/tightening of cable)
• Improper placement of roller (Crew was using a single assembly of corner cable roller instead of using at least three interconnecting rollers
supported with sandbags to allow stability)
• Distracted by other concerns (Foreman was talking to another supervisor while approximately
16 workers were manually pulling the cable)
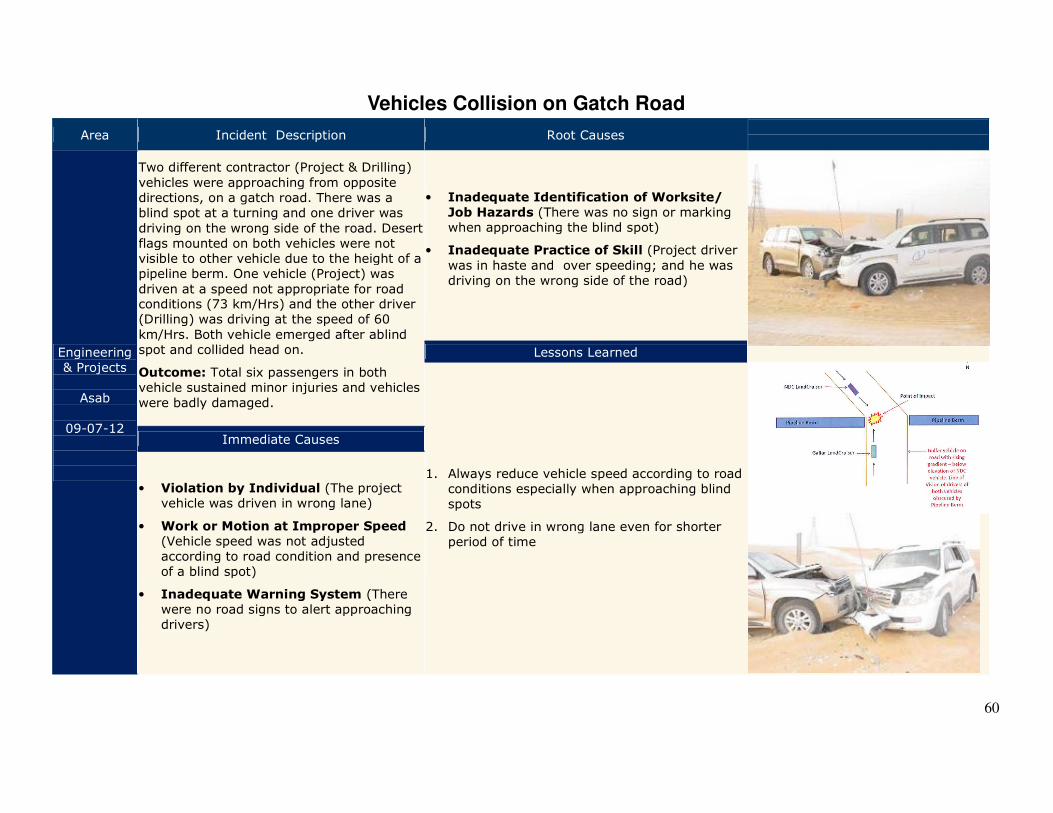
60
Vehicles Collision on Gatch Road
Area Incident Description Root Causes
Engineering & Projects
Asab
09-07-12
Two different contractor (Project & Drilling)
vehicles were approaching from opposite directions, on a gatch road. There was a blind spot at a turning and one driver was
driving on the wrong side of the road. Desert flags mounted on both vehicles were not visible to other vehicle due to the height of a pipeline berm. One vehicle (Project) was
driven at a speed not appropriate for road conditions (73 km/Hrs) and the other driver (Drilling) was driving at the speed of 60
km/Hrs. Both vehicle emerged after ablind spot and collided head on.
Outcome: Total six passengers in both vehicle sustained minor injuries and vehicles
were badly damaged.
• Inadequate Identification of Worksite/
Job Hazards (There was no sign or marking when approaching the blind spot)
• Inadequate Practice of Skill (Project driver
was in haste and over speeding; and he was driving on the wrong side of the road)
Lessons Learned
1. Always reduce vehicle speed according to road conditions especially when approaching blind spots
2. Do not drive in wrong lane even for shorter period of time
Immediate Causes
• Violation by Individual (The project vehicle was driven in wrong lane)
• Work or Motion at Improper Speed (Vehicle speed was not adjusted according to road condition and presence of a blind spot)
• Inadequate Warning System (There were no road signs to alert approaching drivers)
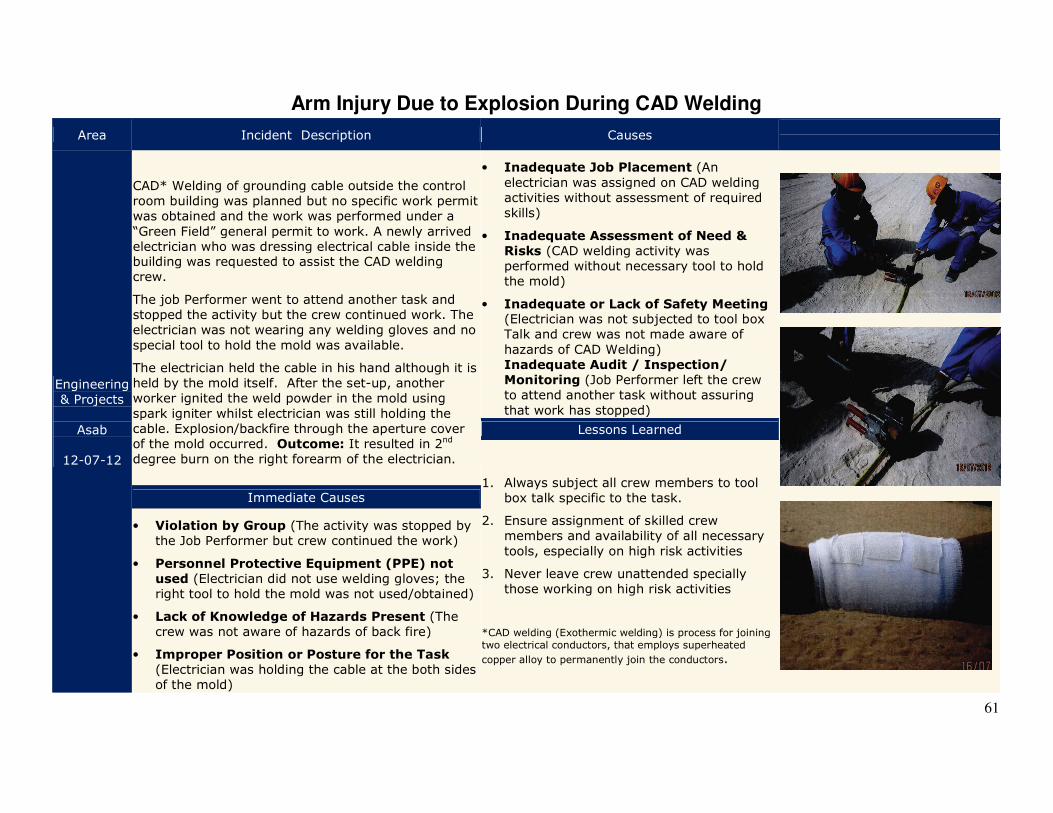
61
Arm Injury Due to Explosion During CAD Welding
Area Incident Description Causes
Engineering & Projects
Asab
12-07-12
CAD* Welding of grounding cable outside the control room building was planned but no specific work permit was obtained and the work was performed under a
“Green Field” general permit to work. A newly arrived electrician who was dressing electrical cable inside the building was requested to assist the CAD welding crew.
The job Performer went to attend another task and stopped the activity but the crew continued work. The electrician was not wearing any welding gloves and no
special tool to hold the mold was available.
The electrician held the cable in his hand although it is held by the mold itself. After the set-up, another worker ignited the weld powder in the mold using
spark igniter whilst electrician was still holding the cable. Explosion/backfire through the aperture cover of the mold occurred. Outcome: It resulted in 2nd degree burn on the right forearm of the electrician.
• Inadequate Job Placement (An
electrician was assigned on CAD welding activities without assessment of required skills)
• Inadequate Assessment of Need &
Risks (CAD welding activity was performed without necessary tool to hold the mold)
• Inadequate or Lack of Safety Meeting (Electrician was not subjected to tool box Talk and crew was not made aware of
hazards of CAD Welding) Inadequate Audit / Inspection/
Monitoring (Job Performer left the crew to attend another task without assuring
that work has stopped)
Lessons Learned
1. Always subject all crew members to tool box talk specific to the task.
2. Ensure assignment of skilled crew members and availability of all necessary
tools, especially on high risk activities
3. Never leave crew unattended specially those working on high risk activities
*CAD welding (Exothermic welding) is process for joining
two electrical conductors, that employs superheated
copper alloy to permanently join the conductors.
Immediate Causes
• Violation by Group (The activity was stopped by the Job Performer but crew continued the work)
• Personnel Protective Equipment (PPE) not
used (Electrician did not use welding gloves; the right tool to hold the mold was not used/obtained)
• Lack of Knowledge of Hazards Present (The crew was not aware of hazards of back fire)
• Improper Position or Posture for the Task (Electrician was holding the cable at the both sides of the mold)
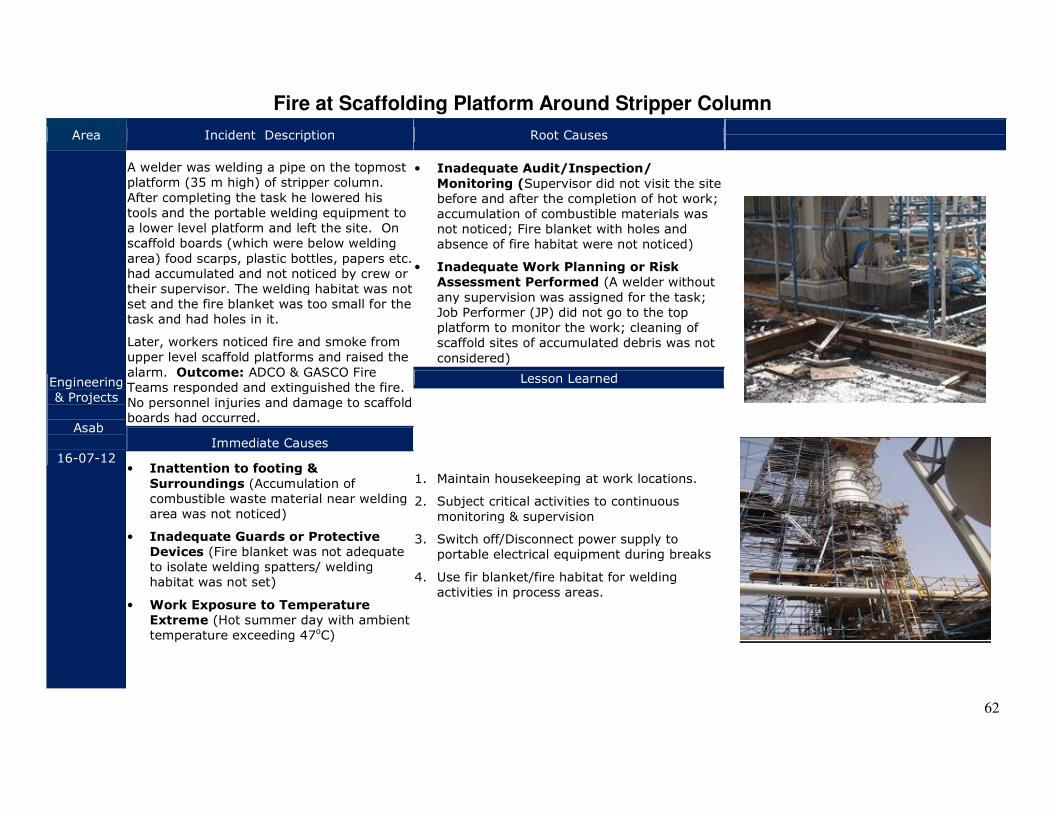
62
Fire at Scaffolding Platform Around Stripper Column
Area Incident Description Root Causes
Engineering & Projects
Asab
16-07-12
A welder was welding a pipe on the topmost platform (35 m high) of stripper column.
After completing the task he lowered his tools and the portable welding equipment to a lower level platform and left the site. On scaffold boards (which were below welding
area) food scarps, plastic bottles, papers etc. had accumulated and not noticed by crew or their supervisor. The welding habitat was not set and the fire blanket was too small for the task and had holes in it.
Later, workers noticed fire and smoke from upper level scaffold platforms and raised the
alarm. Outcome: ADCO & GASCO Fire Teams responded and extinguished the fire. No personnel injuries and damage to scaffold boards had occurred.
• Inadequate Audit/Inspection/
Monitoring (Supervisor did not visit the site before and after the completion of hot work; accumulation of combustible materials was not noticed; Fire blanket with holes and absence of fire habitat were not noticed)
• Inadequate Work Planning or Risk
Assessment Performed (A welder without
any supervision was assigned for the task; Job Performer (JP) did not go to the top platform to monitor the work; cleaning of scaffold sites of accumulated debris was not
considered)
Lesson Learned
1. Maintain housekeeping at work locations.
2. Subject critical activities to continuous
monitoring & supervision
3. Switch off/Disconnect power supply to portable electrical equipment during breaks
4. Use fir blanket/fire habitat for welding activities in process areas.
Immediate Causes
• Inattention to footing &
Surroundings (Accumulation of combustible waste material near welding area was not noticed)
• Inadequate Guards or Protective
Devices (Fire blanket was not adequate to isolate welding spatters/ welding habitat was not set)
• Work Exposure to Temperature
Extreme (Hot summer day with ambient temperature exceeding 47oC)
63
Foreign Object Entering Eye of a Worker
Area Incident Description Root Causes
Engineering & Projects
Sahil
26-07-12
A welder was assigned to perform welding task for the installation of pipe support. After
completing the welding task, while he was removing welding face shield, he felt a sand particle had entered his left eye.
He washed his eye with water and felt relieved
and continued his job. Later, at night he felt pain and irritation in his eye and he visited the camp clinic the next morning and he was attended by the Physician and then referred to a Hospital for the removal of foreign object from his eye.
Outcome: The foreign object (sand particle)
was removed from his eye.
• Inadequate Identification of
Worksite/Job Hazards (Workers were not adequately made aware of hazards of working
on a windy day; risks of rubbing eyes when a foreign body enters eye were not known)
• Inadequate Communication (Lessons from prior similar incident occurred on 04-05-2012
were not effectively communicated)
Lessons Learned
1. If a foreign object enters eye, do not rub eyes and seek medical attention
2. Report all incidents (including minor incidents/injuries) to your supervisor
3. Always use eye wears for protection in working sites, especially in sandy areas.
Immediate Causes
• Storm or Act of Nature (Blowing wind carrying particles/dust/light objects)
• Personal Protective Equipment (PPE)
Not Used (Welder removed his welding face shied after the task and due to blowing
winds sand particle entered his eye)
64
Vehicle Rollover on Gatch Road
Area Incident Description Causes
Engineering & Projects
BAB
23-08-12
A vendor crew was involved in installing gauges on multi flow meters and after the completion
of the task, transport was arranged to transfer them back to Abu Dhabi. The plan was to collect passengers from Accommodation Camp and proceed to Abu Dhabi via Madinat Zayed
Road.
An Engineer decided to go to Abu Dhabi with vendor crew and boarded the vehicle. The Engineer advised the driver to go through Bab-Tarif Road and to avoid going through security check post, the engineer identified a gatch road. The driver was driving fast (80-90
Km/Hrs) for the road condition and at a bend he lost control of the vehicle and the vehicle rolled over. Outcome: No serious injuries to passengers and the vehicle sustained minor
damage.
• Improper Supervisory Example (The Engineer changed the journey plan and advised the driver to take short cuts/gatch road and did not stop him from over
speeding)
• Inadequate Audit/ Inspection/
Monitoring (Driver’s RAG reports were not used to coach the driver with history of over
speeding)
• Inadequate Correction of Worksite/ Job
Hazards (Lessons from prior Road Traffic
Accidents were not effectively communicated; No tool Box Talk was conducted for drivers)
Lesson Learned
Immediate Causes
1. Always drive within posted speed limits and reduce speed according to rad conditions
2. Conduct Tool Box Talks for drivers and empower them to not let any passenger to change journey plan
3. Passenger/s should stop driver from over speeding, taking short cuts and from driving recklessly.
• Violation by Individual (The driver was driving fast in excess of posted speed limit)
• Violation by Supervisor (The Engineer
did not stop driver from overspending)
65
Crane Mounted Truck (Hiab) Rollover on Gatch Road Area Incident Description Root Causes
Engineering
& Projects
BAB
28-08-12
A crew consisting of a Rigger & Operator of
Crane Mounted Truck (Hiab) were instructed by their Engineer drive the truck to work site and lift pre-cast materials. The crew left their camp and was proceeding to the location.
They were travelling on a gatch road parallel to an existing pipeline. This road contained many pot holes and the surface was wet/ slippery
due to high humidity. The driver was attempting to drive around potholes and made a sharp maneuvering of steering followed by harsh brakes.
It resulted in vehicle to get out of control. The rear end of the vehicle spun around in the opposite direction and then rolled over on passenger side against the pipeline berm.
Outcome: The vehicle rolled over to its side on the berm of the pipeline. Driver and passenger sustained minor injuries as they were wearing
seat belts.
• Inadequate Audit/ Inspection/
Monitoring (Driver had history of applying harsh brakes and harsh acceleration and his driving behavior reports were not effectively reviewed to
initiate counseling/ coaching on the skill)
• Inadequate Identification of
Worksite/Job Hazards (Hazards
associated with the journey (i.e. gatch road condition and high humidity) were not identified)
Lesson Learned
1. Avoid applying harsh brakes and sharp maneuvering of steering when driving off road.
2. Review drivers’ driving behavior reports and provide coaching and counseling to risky drivers
3. Subject drivers to daily tool box talks to discuss route hazards and to reinforce safe driving behaviour
Immediate Causes
• Improper Decision Making/Lack of
Judgment (The driver applied harsh brake and sharp maneuvering of steering to avoid pot hole on the gatch road)
• Work or Motion at Improper Speed (The
vehicle was driven on gatch road at a speed between 20 to 45 kph with a sudden acceleration to approx. 58 kph followed by
a harsh breaks immediately prior to the incident)
66
Vehicles Collision
Area Incident Description Root Causes
Engineering &
Projects
BAB
04-09-12
A 3rd Party mechanic was working on a broken down vehicle near the road side a replacement tire was
requested from their base camp in Mussafah. A truck carrying the replacement tire arrived and stopped on the road side. The mechanic requested the driver to move the truck on the opposite side.
A project driver involved was transferring staff to and from difference locations since morning and was making a trip to collect three passengers from Bab Central Degassing Station (BCDS) to their Camp. The driver was driving 128 km/Hr on a road with a speed limit of 80 km/Hr.
The project driver was over taking the truck whilst
the truck started to turn left. Outcome: The project vehicle collided with the front tire of the truck. Two passenger sustained minor injuries and the vehicle sustained moderate damage.
• Inadequate Audit / Inspection
/Monitoring (Drivers driving behavior
and driving assignments were not adequately monitored)
• Improper Performance to save time (The driver was involved in transferring
passengers to & from different locations since early morning and was rushing to the camp for mid-day break)
• Inadequate Identification of
Worksite/Job Hazards (In Vehicle Monitoring System (IVMS) was reconfigured so that speeding event
below 130 km/Hr were not recorded as system violation)
Lessons Learned
1. Always follow the posted speed limits
and do not over speed.
2. Use vehicle signal before maneuvering vehicles even on a short journey
3. Monitor the driving behavior of new/inexperience driver more frequently
Immediate Causes
• Violation by individual (The driver was overspending (128 km/Hr on a road with a speed limit of 80 km/Hr)
• Improper Decision Making (The truck driver started to turn left without using indicators/ signal)
67
Crane Rollover During Move on Gatch Road
Area Incident Description Root Causes
Engineering & Projects
BAB
26-09-12
A 25 Tone Grove Crane, was mobilized on site to load /
offload piping materials from various locations within the vicinity of RDS-8 Transfer Line area. The crane reached the site at around 06:30am and started off-loading pipe supports from the trailer truck. The crane being moved
between locations (approximately 100 meters apart) to lift excess pipe supports. The crane operator was following the pick-up vehicle (boarded by the Rigging Foreman) and the trailer truck on gatch road, parallel to
the transfer line.
There was slope between the two gatch roads and the pick-up and trailer truck managed to drive across the
bank and reached the elevated gatch road.
As the crane tried to ascend on slope (with crane boom not fully folded), the crane lost the balance causing it to roll over to its right side. Outcome: The operator
managed to exit the crane cabin safely through the cabin door and the crane sustained minor damage.
• Inadequate Supervisory Example (Rigging Forman did not ensure the
suitability of the track)
• Inadequate Audit / Inspection/
Monitoring (Job Performer (JP) was away supervising another crew and the crew moved without his knowledge)
Lesson Learned
4. Do not move heavy equipment from one location to another location unless track conditions are inspected
and are found suitable.
5. Ensure Crane boom is fully folded and hook block secured when moving crane, to maintain stability of the equipment
Immediate Causes
• Violation by Individual (The operator did not fully fold the boom of the crane and did not lock the hook
block while moving the crane)
• Violation by Supervisor (Rigging Foreman did not assess the road conditions and asked the crane operator to follow the vehicle)
68
Vehicle Collision
Area Incident Description Root Causes
Engineering
& Projects
BAB
01-10-12
A project vehicle (Double Cabin Pickup) was returning back from their project site (RDS
8) to their camp store for the collection of materials. He was in mostly in Red and Yellow categories as per his driving behavior report (RAG Report) over the last one month
and there was no effective review of RAG reports in place to provide coaching/ counseling to the driver. An ADCO staff was coming from Ghayathi to BAB in his private vehicle (Land Cruiser) after his rest period and he stopped by a shop in Al Dhafra camp and then proceeded to BAB Accommodation
Camp. There was a long trailer on the hard shoulder, restricting the direct view. The project vehicle was driver at a speed of 121 km/hr on the road with posted speed limit of
80 km/Hr. ADCO staff vehicle entered the T Junction and crossed the road and the project vehicle collided on the side of the
land cruiser. Outcome: Minor injuries (Bruises) to passengers as they were wearing seatbelts and serious damage to both vehicles.
• Inadequate Audit/ Inspection/
Monitoring (Drivers driving behavior reports were not effectively reviewed and the driver did not receive any coaching or counseling to develop safe driving skills)
• Inadequate Identification of Critical
Safe Behaviour (The project driver drove
considerable long distances with BAB (250-300 km/day) and his work assignment, journey management and time pressure were not effectively addressed)
Lesson Learned
1. Regularly review drivers’ driving behavior(RAG) reports and provide counseling to risky drivers
2. Review drivers’ driving hours and work assignments to reduce time pressure.
Immediate Causes
• Violation by Individual (The project vehicle (Pickup) was over speeding)
• Improper Decision Making/Lack of
Judgment (ADCO Staff entered the
junction without ensuring clearance)
69
Fatal Fall of Worker from a Moving Vehicle
Area Incident Description Causes
Engineering & Projects
Qw
17-11-12
While two Workers were involved in manually offloading of fence gates from a pickup truck, the site Foreman instructed
the driver to move the vehicle to another location nearby (while two workers were still in the back of pickup). Workers sat down on stacked fence gates which were unsecured. At a sharp turn, the load slipped and workers fell down from the moving vehicle. Outcome: One worker escaped
unhurt whilst the other sustained head injuries and later he died in the hospital
• Inadequate Leadership (HSE site inspections/visits to sites for less than 20 workers were suspended; effective inspection/monitoring system was not in place to identify
this change)
• Inadequate Identification of Worksite or Job
Hazards (Risk associated with transfer & loading/offloading of fencing material were not identified
and there was no Task Risk Assessment (TRA) available for fencing work)
• Improper Supervisory Example (Foreman sent workers to another location to load fence gates into the pickup,
unsupervised and transfer the load; Job Performer did not effectively conduct tool box talk (TBT); After offloading a few gates, Foreman instructed the driver to move the
vehicle while two workers were on the back of the pickup)
• Inadequate Work Planning (Crane mounted truck was not made available for the transfer of wide fence gates therefore the crew used a smaller vehicle for the task)
• Inadequate Enforcement of Policy/ Procedure/Plan
(Contractor staff did not feel empowered to stop unsafe actions due to fear of losing job)
Immediate Causes
• Violation by Supervisor (Foreman
advised the driver to move the vehicle while two workers were in the cargo area of the vehicle; The Foreman & the driver did not ensure that the load was
secured)
• Equipment or Materials not Secured
(Fence gates were not secured before
moving the vehicle)
• Inadequate Vehicle for the Purpose
(Vehicle was not suitable for transferring oversized fence gates)
• Congestion or Restricted movement
(Narrow access track for the movement of vehicle)
Lessons Learned
1. Provide coaching to Job Performers (JP) on conducting
effective tool box talks (TBT) 2. Develop and publicize an incentive scheme both for
workers and their JPs/Foremen to stop & report unsafe actions and set a target for each worker.
3. Ensure contractor JPs & Foreman have supervisory skills prior to their assignment and subject them to regular motivational training to enhance their supervisory skills
70
Fall of Mobile Scaffold Platform on a Worker
Area Incident Description Causes
Engineering & Projects
Asab
28-11-12
An electrical crew was assigned to cable pulling, dressing and installation of cable tray cover. The crew was using a mobile
scaffold platform. The platform was not subjected to any checks/inspections and its caster wheels were not secured. During the
work, while crew was pushing the platform, over a wooden plant (used as a bridge to cross over a gap), the platform fell down, hitting on the right leg of a worker.
Outcome: The worker sustained compound fracture on his right leg and he underwent constructive surgery
• Inadequate Supervisory Example (The work was started without PTW; JP was not on site and workers were working unsupervised)
• Inadequate Audit/ Inspection/ Monitoring (The mobile platform was not checked/ inspected prior to its use)
• Inadequate Identification of Worksite/Job Hazards (Use of mobile scaffold platform in the area was not risk assessed and workers created inadequate crossing over a gap).
Immediate Causes
• Violation by Supervisor (The work was not subjected to Permit to Work (PTW) and the Job Performer was not supervising the crew at the location)
• Lack of knowledge of Hazards
Present (A narrow wooden plank was used as a bridge for crossing of the
mobile platform)
• Defective Equipment (The mobile platform wheels had no locking mechanism)
Lessons Learned
1. Always inspect mobile equipment and tools to assess
fitness prior to their use.
2. Identify worksite hazards and do not take short cuts.
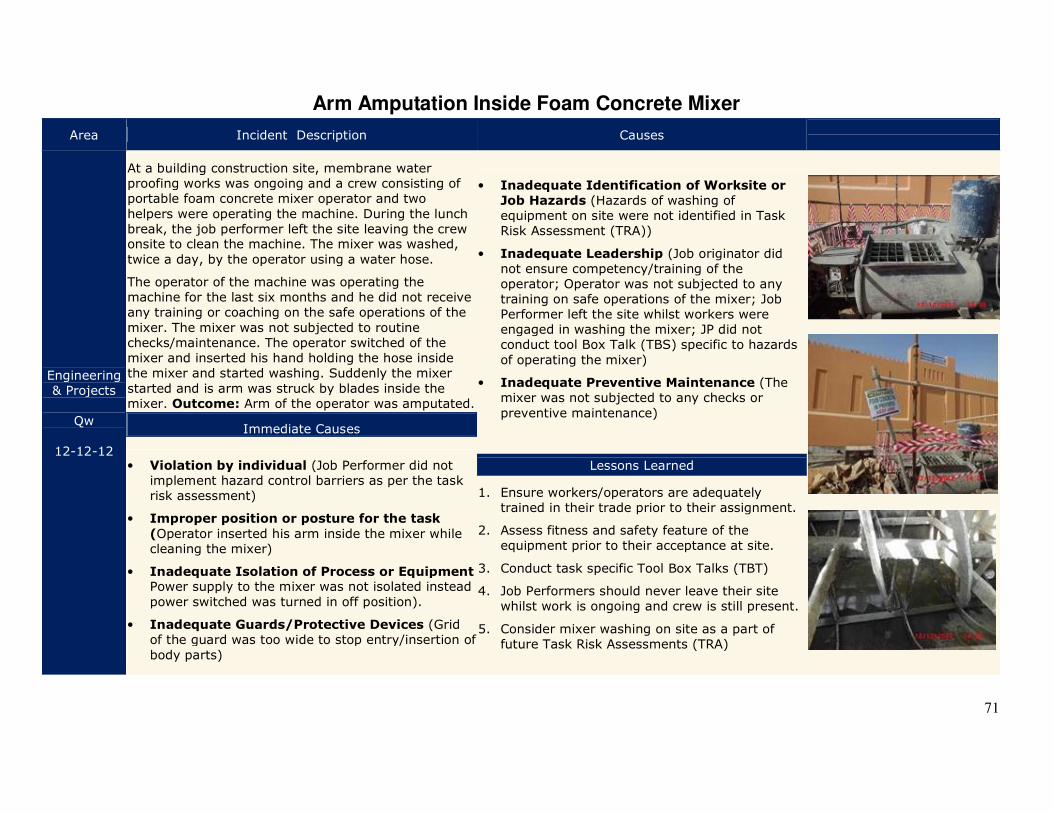
71
Arm Amputation Inside Foam Concrete Mixer
Area Incident Description Causes
Engineering & Projects
Qw
12-12-12
At a building construction site, membrane water proofing works was ongoing and a crew consisting of portable foam concrete mixer operator and two
helpers were operating the machine. During the lunch break, the job performer left the site leaving the crew onsite to clean the machine. The mixer was washed,
twice a day, by the operator using a water hose.
The operator of the machine was operating the machine for the last six months and he did not receive any training or coaching on the safe operations of the
mixer. The mixer was not subjected to routine checks/maintenance. The operator switched of the mixer and inserted his hand holding the hose inside the mixer and started washing. Suddenly the mixer
started and is arm was struck by blades inside the mixer. Outcome: Arm of the operator was amputated.
• Inadequate Identification of Worksite or
Job Hazards (Hazards of washing of equipment on site were not identified in Task Risk Assessment (TRA))
• Inadequate Leadership (Job originator did not ensure competency/training of the operator; Operator was not subjected to any training on safe operations of the mixer; Job Performer left the site whilst workers were engaged in washing the mixer; JP did not conduct tool Box Talk (TBS) specific to hazards
of operating the mixer)
• Inadequate Preventive Maintenance (The mixer was not subjected to any checks or
preventive maintenance)
Immediate Causes
• Violation by individual (Job Performer did not implement hazard control barriers as per the task risk assessment)
• Improper position or posture for the task
(Operator inserted his arm inside the mixer while cleaning the mixer)
• Inadequate Isolation of Process or Equipment Power supply to the mixer was not isolated instead
power switched was turned in off position).
• Inadequate Guards/Protective Devices (Grid of the guard was too wide to stop entry/insertion of
body parts)
Lessons Learned
1. Ensure workers/operators are adequately trained in their trade prior to their assignment.
2. Assess fitness and safety feature of the equipment prior to their acceptance at site.
3. Conduct task specific Tool Box Talks (TBT)
4. Job Performers should never leave their site whilst work is ongoing and crew is still present.
5. Consider mixer washing on site as a part of future Task Risk Assessments (TRA)
72
North East Bab (NEB) Asset

73
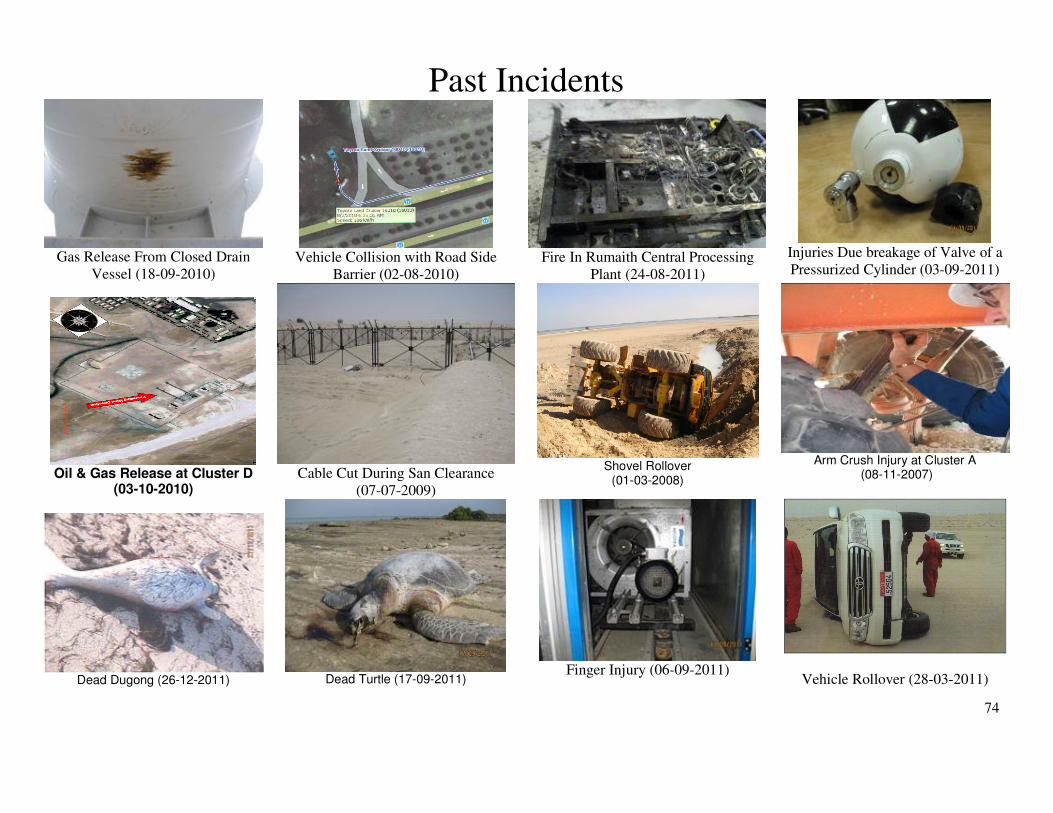
74
Past Incidents
Gas Release From Closed Drain
Vessel (18-09-2010)
Vehicle Collision with Road Side
Barrier (02-08-2010)
Fire In Rumaith Central Processing
Plant (24-08-2011)
Injuries Due breakage of Valve of a
Pressurized Cylinder (03-09-2011)
Oil & Gas Release at Cluster D
(03-10-2010)
Cable Cut During San Clearance
(07-07-2009)
Shovel Rollover
(01-03-2008)
Arm Crush Injury at Cluster A
(08-11-2007)
Dead Dugong (26-12-2011)
Dead Turtle (17-09-2011)
Finger Injury (06-09-2011)
Vehicle Rollover (28-03-2011)
75
76
Vehicle Crash During OHL Visual Survey
Area Incident Description Root Causes
North East Bab (NEB)
30-04-12
As a part of routine inspection of over head line (OHL, visual inspections was ongoing.
There is no access track along the overhead line network. A foreman and a driver were travelling in a vehicle and the Foreman
decided to drive the vehicle himself and the driver was seating in passenger seat. The Foreman inspected one pole and was driving towards the next one to do the same
inspection. Suddenly the vehicle fell down as there was a sharp slop formed by sand dune. Outcome: The foreman and the
driver felt back pain and the car front bumper was damaged (estimated to be $1500). The Foreman was assigned on light duties for one week.
• Inadequate Preventive Maintenance (The right of way was not maintained and resulting in formation of sand dunes beside over-head lines)
• Improper Supervisory Example (The
Foreman decided to drive himself and carry our visual inspection at the same time; and a professional driver was not used for driving)
Immediate Causes
• Improper decision making/lack of judgment (The Foreman decided to drive and visually inspect over head lines
at the same time whilst a professional driver was seating as a passenger))
• Inattention to surroundings (While focusing on overhead lines the
depression was overlooked)
Lesson Learned
6. Do not drive and get distracted by other activities 7. Maintain right of way (ROW) near overhead line
poles and check adequacy of the track prior to commence work
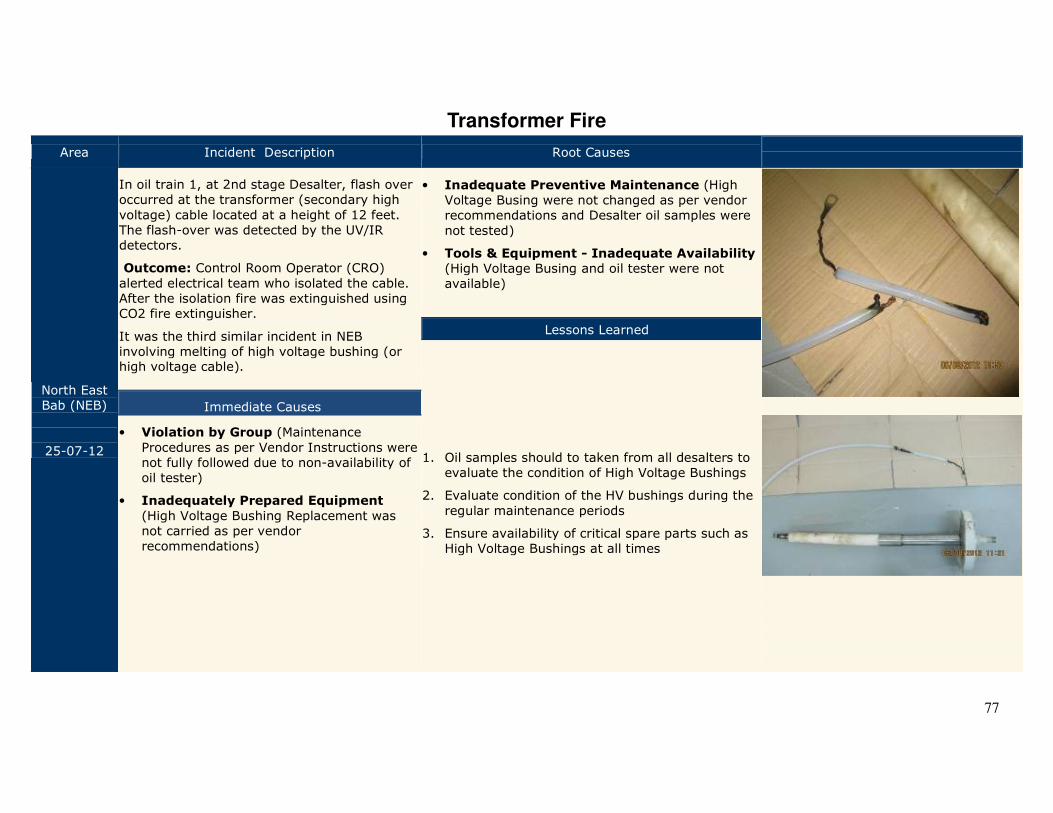
77
Transformer Fire
Area Incident Description Root Causes
North East Bab (NEB)
25-07-12
In oil train 1, at 2nd stage Desalter, flash over occurred at the transformer (secondary high
voltage) cable located at a height of 12 feet. The flash-over was detected by the UV/IR detectors.
Outcome: Control Room Operator (CRO)
alerted electrical team who isolated the cable. After the isolation fire was extinguished using CO2 fire extinguisher.
It was the third similar incident in NEB involving melting of high voltage bushing (or high voltage cable).
• Inadequate Preventive Maintenance (High Voltage Busing were not changed as per vendor recommendations and Desalter oil samples were
not tested)
• Tools & Equipment - Inadequate Availability (High Voltage Busing and oil tester were not available)
Lessons Learned
1. Oil samples should to taken from all desalters to evaluate the condition of High Voltage Bushings
2. Evaluate condition of the HV bushings during the
regular maintenance periods
3. Ensure availability of critical spare parts such as High Voltage Bushings at all times
Immediate Causes
• Violation by Group (Maintenance
Procedures as per Vendor Instructions were not fully followed due to non-availability of oil tester)
• Inadequately Prepared Equipment
(High Voltage Bushing Replacement was not carried as per vendor recommendations)
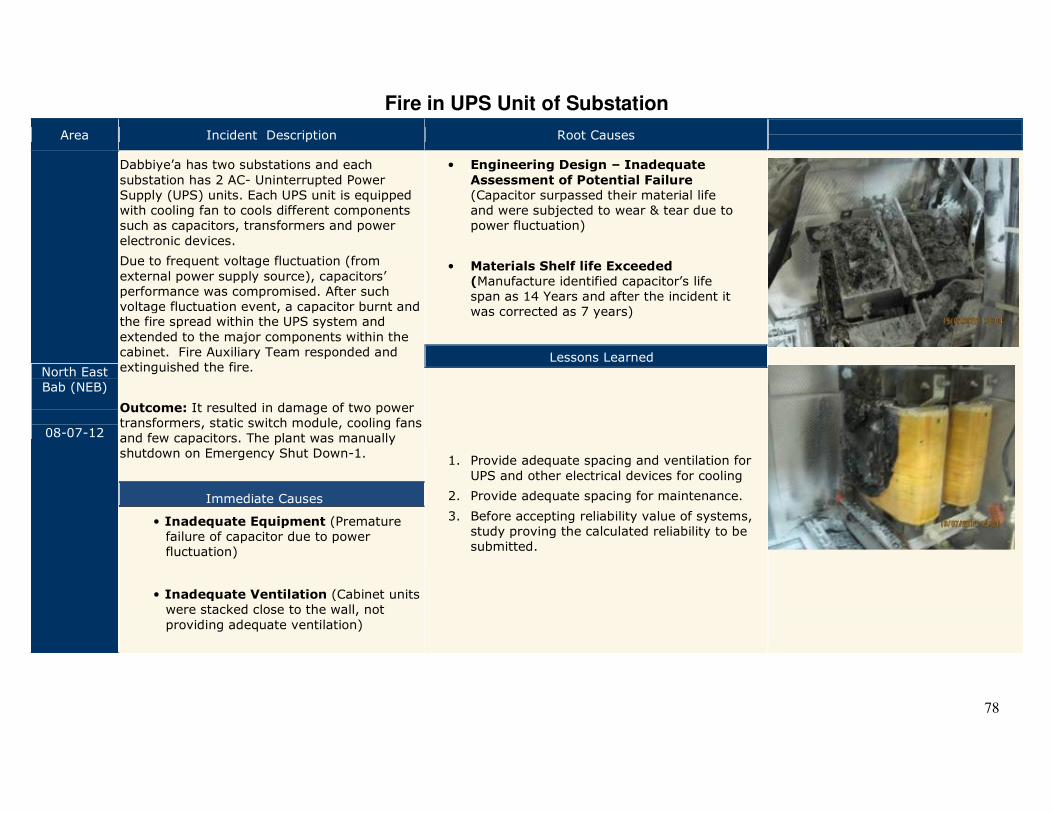
78
Fire in UPS Unit of Substation
Area Incident Description Root Causes
North East Bab (NEB)
08-07-12
Dabbiye’a has two substations and each
substation has 2 AC- Uninterrupted Power Supply (UPS) units. Each UPS unit is equipped with cooling fan to cools different components such as capacitors, transformers and power
electronic devices.
Due to frequent voltage fluctuation (from
external power supply source), capacitors’ performance was compromised. After such voltage fluctuation event, a capacitor burnt and the fire spread within the UPS system and
extended to the major components within the cabinet. Fire Auxiliary Team responded and extinguished the fire.
Outcome: It resulted in damage of two power transformers, static switch module, cooling fans and few capacitors. The plant was manually shutdown on Emergency Shut Down-1.
• Engineering Design – Inadequate
Assessment of Potential Failure
(Capacitor surpassed their material life and were subjected to wear & tear due to power fluctuation)
• Materials Shelf life Exceeded
(Manufacture identified capacitor’s life span as 14 Years and after the incident it was corrected as 7 years)
Lessons Learned
1. Provide adequate spacing and ventilation for
UPS and other electrical devices for cooling
2. Provide adequate spacing for maintenance.
3. Before accepting reliability value of systems, study proving the calculated reliability to be submitted.
Immediate Causes
• Inadequate Equipment (Premature failure of capacitor due to power fluctuation)
• Inadequate Ventilation (Cabinet units were stacked close to the wall, not
providing adequate ventilation)
79
South East (SE) Asset

80
81
Past Incidents
Multiple Fatalities Due to H2S Release in Shah (03-02-2009)
Multiple Fatalities Due to Vehicle
Collision –Sahil (07-09-2009)
Loss of Containment During
Replacement of Corrosion Coupon (23-10-2010)
Buried Cable Cut During Site
Preparation (16-04-2010)
Carpenter’s Finger Injury
(10-02-2011)
Fall of Worker in Wellhead Celler
(24-03-2011)
Wireline Crew Vehicle Rollover
(03-08-2011)
Vehicle Tire Disengagement
(03-08-2011)
Finger Injury during Unplugging of
Drain (14-08-2010)
Scorpion Sting During Sand
Clearance (25-05-2010)
Wrong Flow Line Tie in
(07-04-2011)
Vehicle Rollover
(24-03-2011)
82
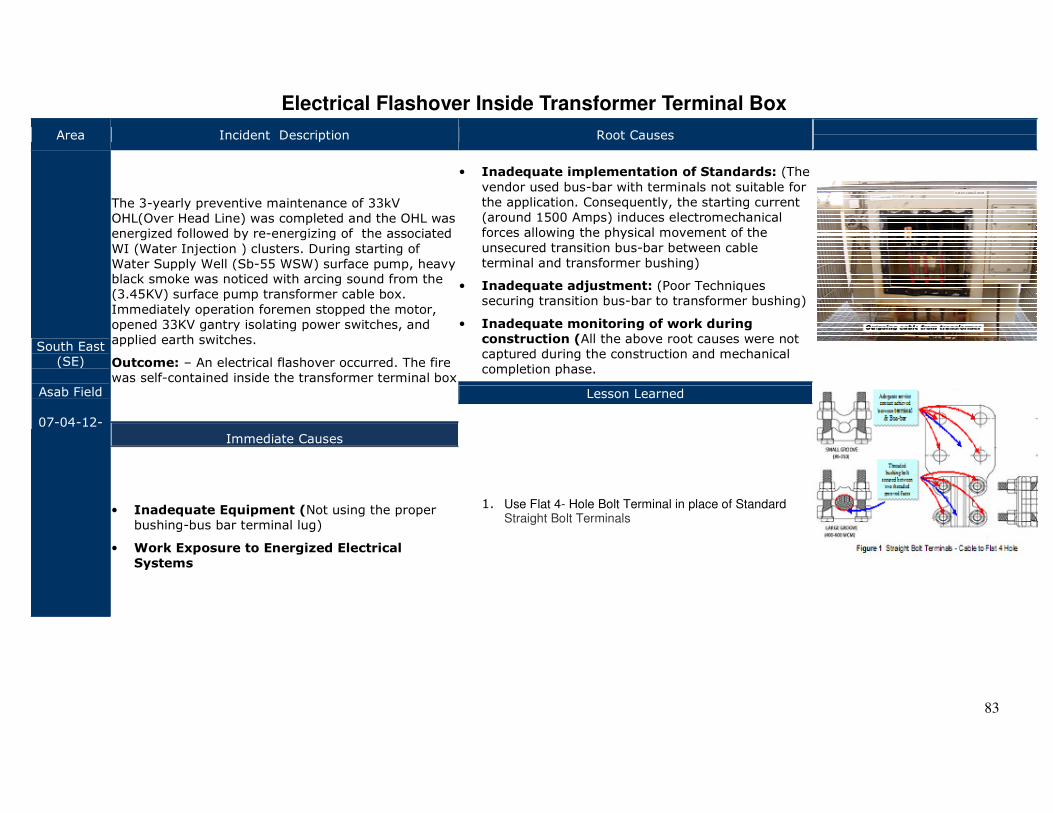
83
Electrical Flashover Inside Transformer Terminal Box
Area Incident Description Root Causes
South East (SE)
Asab Field
07-04-12-
The 3-yearly preventive maintenance of 33kV OHL(Over Head Line) was completed and the OHL was energized followed by re-energizing of the associated
WI (Water Injection ) clusters. During starting of Water Supply Well (Sb-55 WSW) surface pump, heavy black smoke was noticed with arcing sound from the (3.45KV) surface pump transformer cable box.
Immediately operation foremen stopped the motor, opened 33KV gantry isolating power switches, and applied earth switches.
Outcome: – An electrical flashover occurred. The fire was self-contained inside the transformer terminal box
• Inadequate implementation of Standards: (The
vendor used bus-bar with terminals not suitable for the application. Consequently, the starting current (around 1500 Amps) induces electromechanical forces allowing the physical movement of the
unsecured transition bus-bar between cable terminal and transformer bushing)
• Inadequate adjustment: (Poor Techniques securing transition bus-bar to transformer bushing)
• Inadequate monitoring of work during
construction (All the above root causes were not captured during the construction and mechanical completion phase.
Lesson Learned
1. Use Flat 4- Hole Bolt Terminal in place of Standard Straight Bolt Terminals
Immediate Causes
• Inadequate Equipment (Not using the proper bushing-bus bar terminal lug)
• Work Exposure to Energized Electrical
Systems
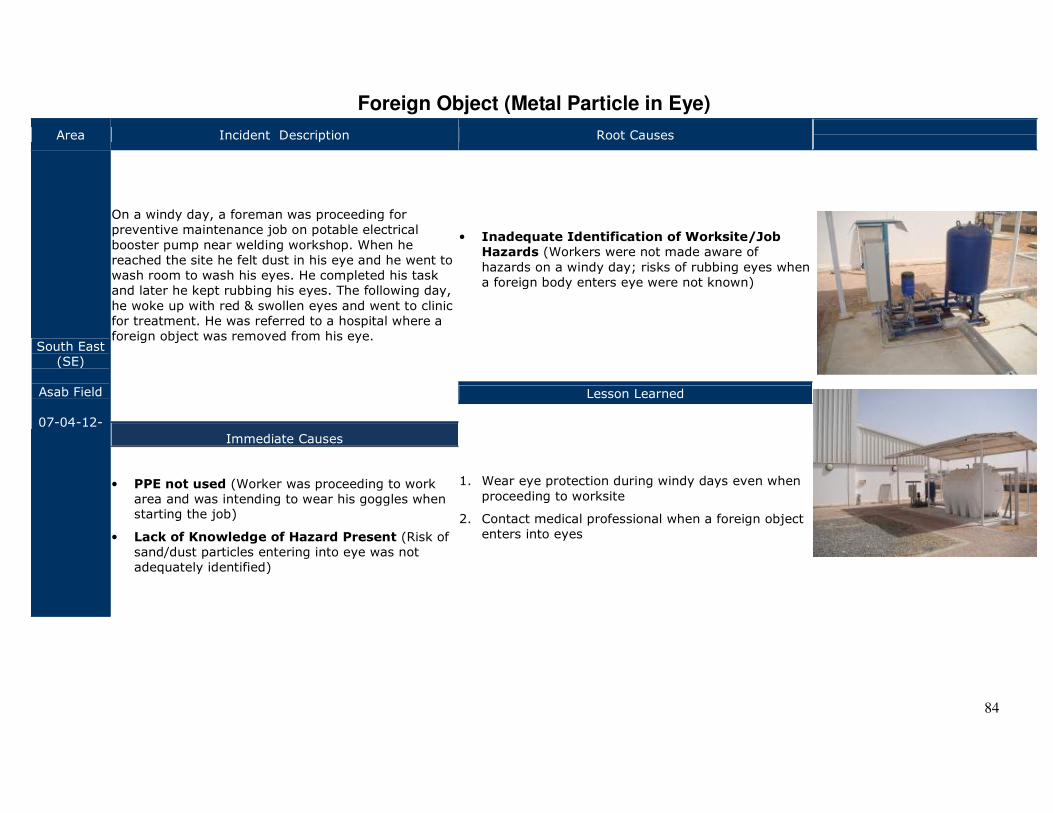
84
Foreign Object (Metal Particle in Eye)
Area Incident Description Root Causes
South East (SE)
Asab Field
07-04-12-
On a windy day, a foreman was proceeding for preventive maintenance job on potable electrical
booster pump near welding workshop. When he reached the site he felt dust in his eye and he went to wash room to wash his eyes. He completed his task and later he kept rubbing his eyes. The following day,
he woke up with red & swollen eyes and went to clinic for treatment. He was referred to a hospital where a foreign object was removed from his eye.
• Inadequate Identification of Worksite/Job
Hazards (Workers were not made aware of
hazards on a windy day; risks of rubbing eyes when a foreign body enters eye were not known)
Lesson Learned
1. Wear eye protection during windy days even when
proceeding to worksite
2. Contact medical professional when a foreign object enters into eyes
Immediate Causes
• PPE not used (Worker was proceeding to work area and was intending to wear his goggles when starting the job)
• Lack of Knowledge of Hazard Present (Risk of sand/dust particles entering into eye was not adequately identified)
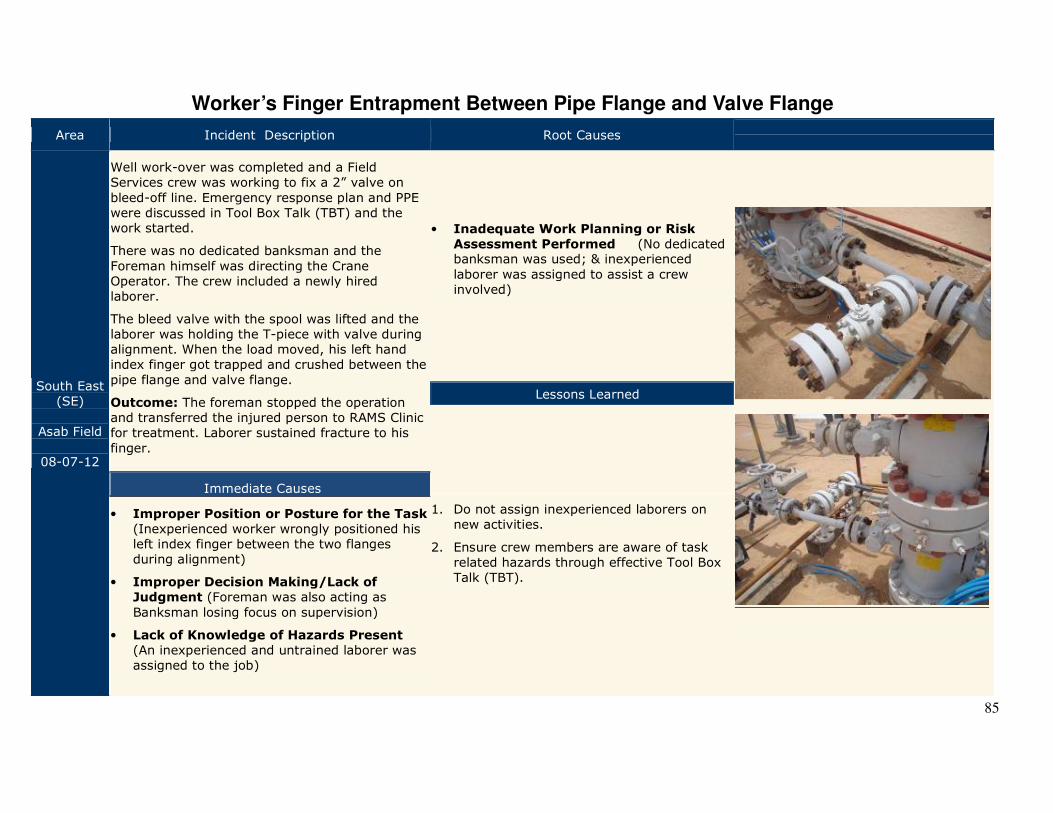
85
Worker’s Finger Entrapment Between Pipe Flange and Valve Flange
Area Incident Description Root Causes
South East (SE)
Asab Field
08-07-12
Well work-over was completed and a Field Services crew was working to fix a 2” valve on
bleed-off line. Emergency response plan and PPE were discussed in Tool Box Talk (TBT) and the work started.
There was no dedicated banksman and the
Foreman himself was directing the Crane Operator. The crew included a newly hired laborer.
The bleed valve with the spool was lifted and the laborer was holding the T-piece with valve during alignment. When the load moved, his left hand index finger got trapped and crushed between the
pipe flange and valve flange.
Outcome: The foreman stopped the operation and transferred the injured person to RAMS Clinic for treatment. Laborer sustained fracture to his
finger.
• Inadequate Work Planning or Risk
Assessment Performed (No dedicated banksman was used; & inexperienced
laborer was assigned to assist a crew involved)
Lessons Learned
1. Do not assign inexperienced laborers on new activities.
2. Ensure crew members are aware of task related hazards through effective Tool Box Talk (TBT).
Immediate Causes
• Improper Position or Posture for the Task (Inexperienced worker wrongly positioned his left index finger between the two flanges during alignment)
• Improper Decision Making/Lack of
Judgment (Foreman was also acting as
Banksman losing focus on supervision)
• Lack of Knowledge of Hazards Present (An inexperienced and untrained laborer was assigned to the job)
86
Terminal & Pipelines Operations (TPO) Asset

87
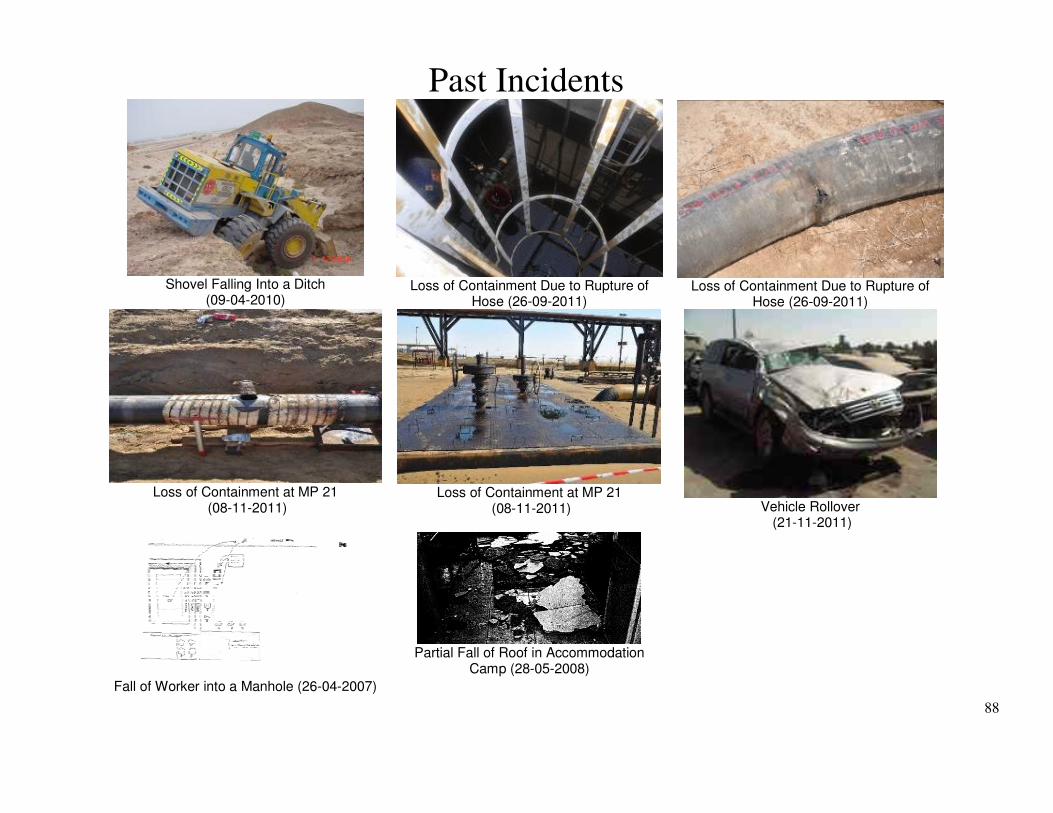
88
Past Incidents
Shovel Falling Into a Ditch
(09-04-2010)
Loss of Containment Due to Rupture of
Hose (26-09-2011)
Loss of Containment Due to Rupture of
Hose (26-09-2011)
Loss of Containment at MP 21
(08-11-2011)
Loss of Containment at MP 21
(08-11-2011)
Vehicle Rollover
(21-11-2011)
Fall of Worker into a Manhole (26-04-2007)
Partial Fall of Roof in Accommodation
Camp (28-05-2008)

89
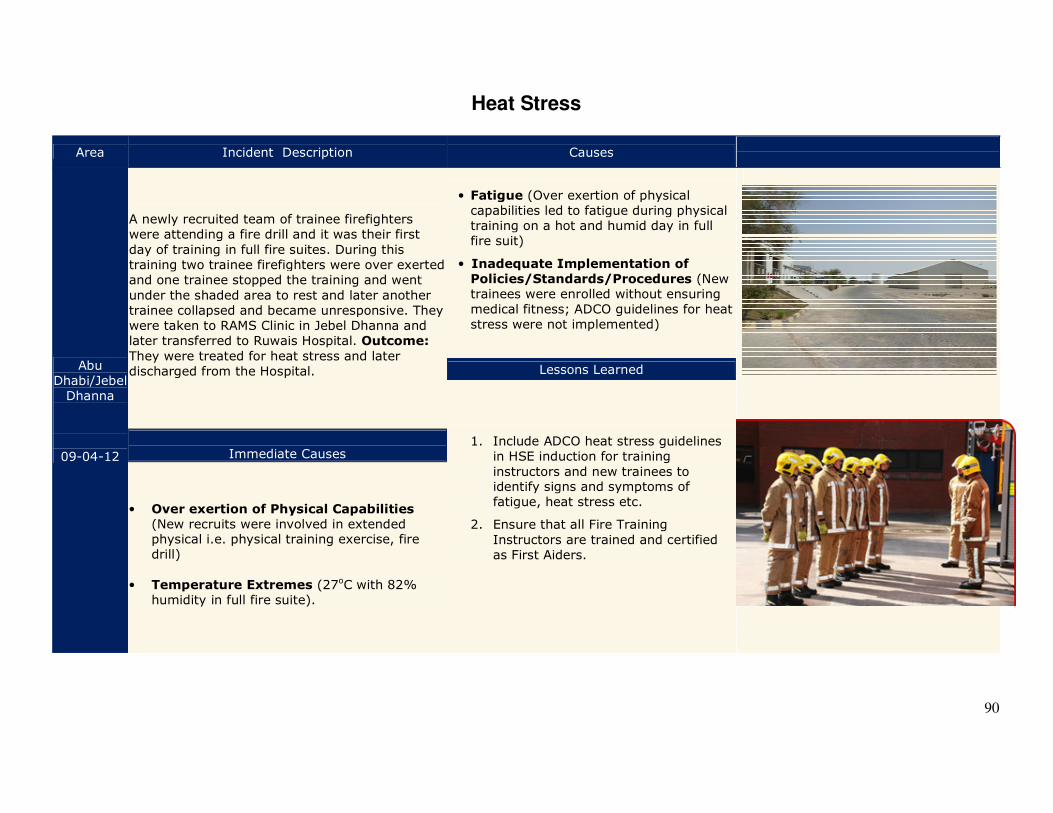
90
Heat Stress
Area Incident Description Causes
Abu Dhabi/Jebel Dhanna
09-04-12
A newly recruited team of trainee firefighters were attending a fire drill and it was their first
day of training in full fire suites. During this training two trainee firefighters were over exerted and one trainee stopped the training and went
under the shaded area to rest and later another trainee collapsed and became unresponsive. They were taken to RAMS Clinic in Jebel Dhanna and later transferred to Ruwais Hospital. Outcome:
They were treated for heat stress and later discharged from the Hospital.
• Fatigue (Over exertion of physical capabilities led to fatigue during physical training on a hot and humid day in full fire suit)
• Inadequate Implementation of
Policies/Standards/Procedures (New trainees were enrolled without ensuring medical fitness; ADCO guidelines for heat stress were not implemented)
Lessons Learned
1. Include ADCO heat stress guidelines in HSE induction for training
instructors and new trainees to identify signs and symptoms of fatigue, heat stress etc.
2. Ensure that all Fire Training
Instructors are trained and certified as First Aiders.
Immediate Causes
• Over exertion of Physical Capabilities (New recruits were involved in extended physical i.e. physical training exercise, fire drill)
• Temperature Extremes (27oC with 82%
humidity in full fire suite).
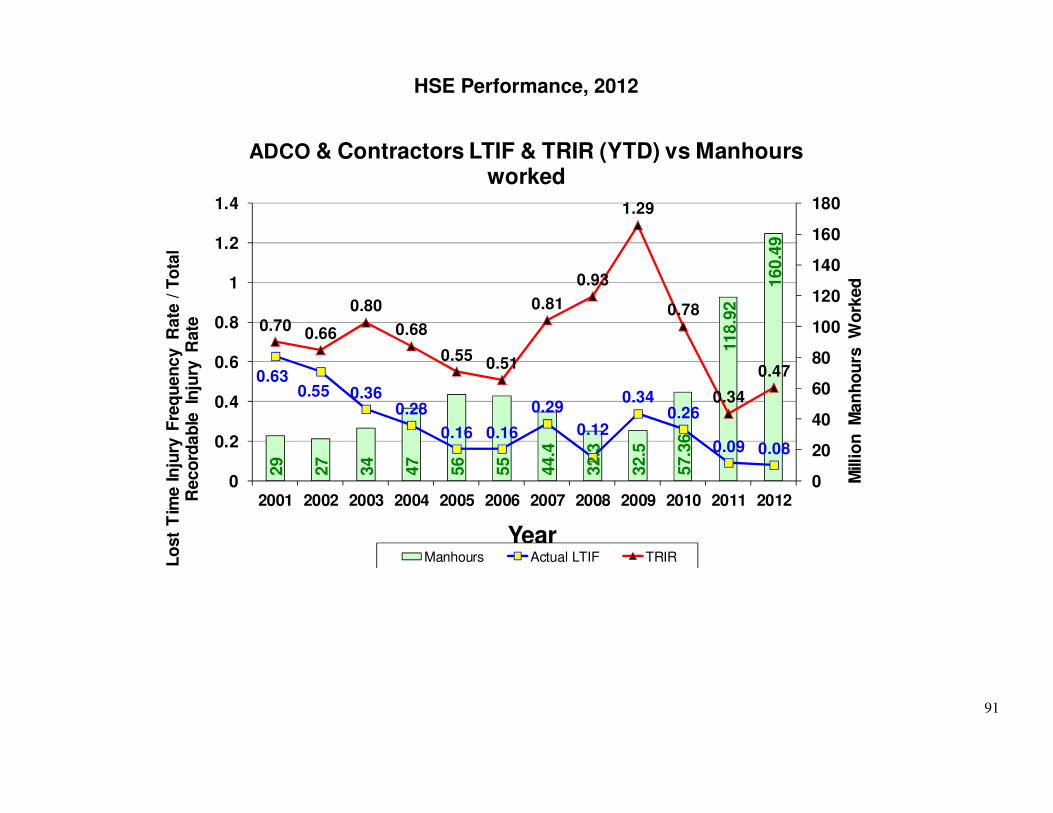
91
HSE Performance, 2012
29
27
34
47
56
55
44.4
32.3
32.5
57.3
6
118.9
2
160.4
9
0.630.55 0.36
0.28
0.16 0.16
0.29
0.12
0.340.26
0.09 0.08
0.700.66
0.80
0.68
0.550.51
0.81
0.93
1.29
0.78
0.34
0.47
0
20
40
60
80
100
120
140
160
180
0
0.2
0.4
0.6
0.8
1
1.2
1.4
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Mill
ion
M
an
ho
urs
W
ork
ed
Lo
st
Tim
e In
jury
Fre
qu
en
cy R
ate
/ T
ota
l R
eco
rdab
le In
jury
R
ate
Year
ADCO & Contractors LTIF & TRIR (YTD) vs Manhours worked
Manhours Actual LTIF TRIR
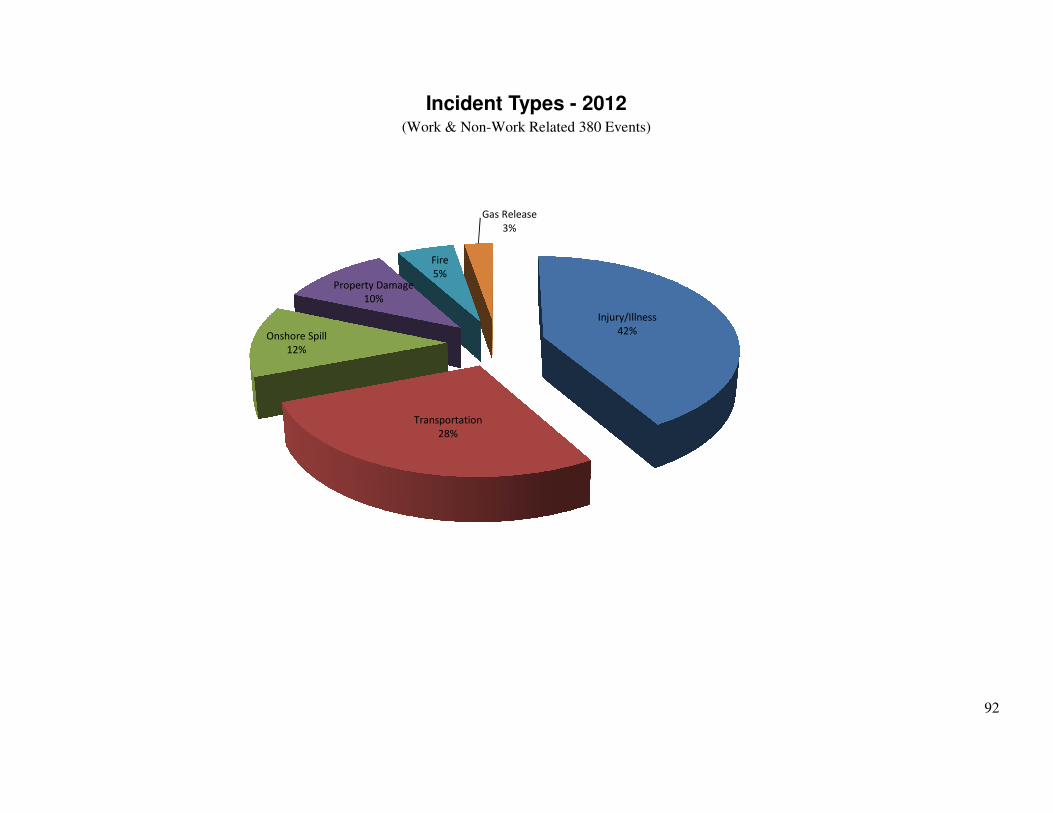
92
Incident Types - 2012 (Work & Non-Work Related 380 Events)
Injury/Illness
42%
Transportation
28%
Onshore Spill
12%
Property Damage
10%
Fire
5%
Gas Release
3%
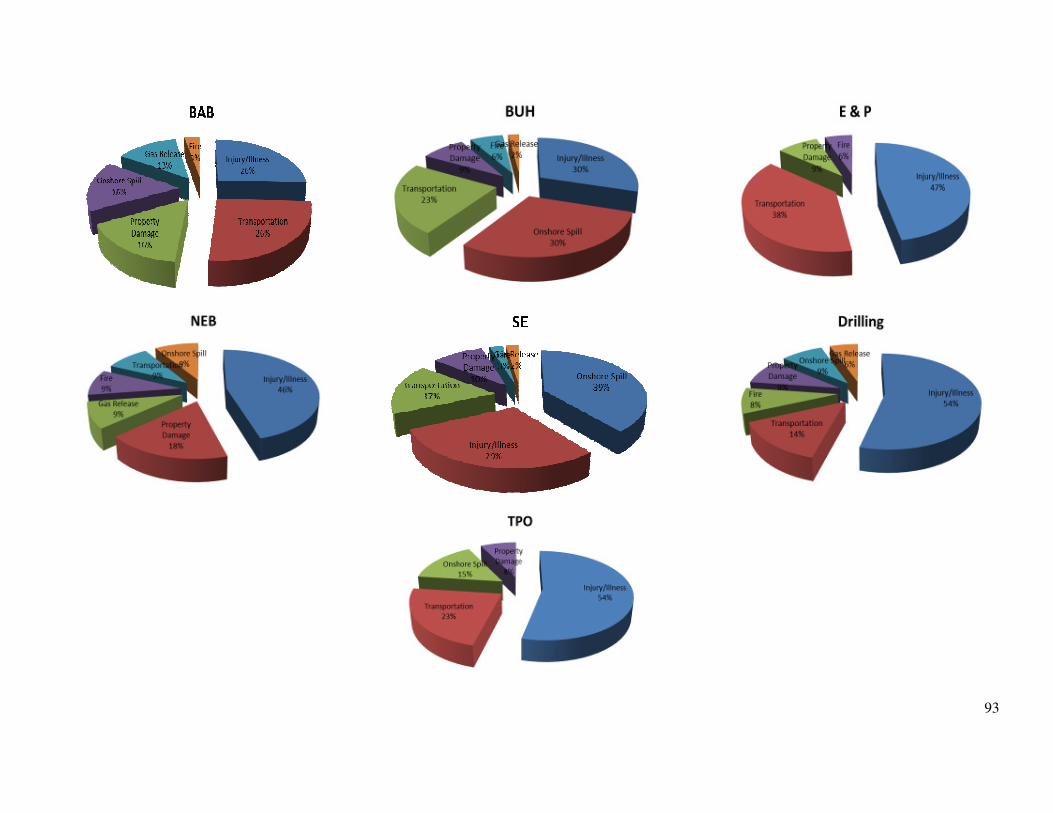
93
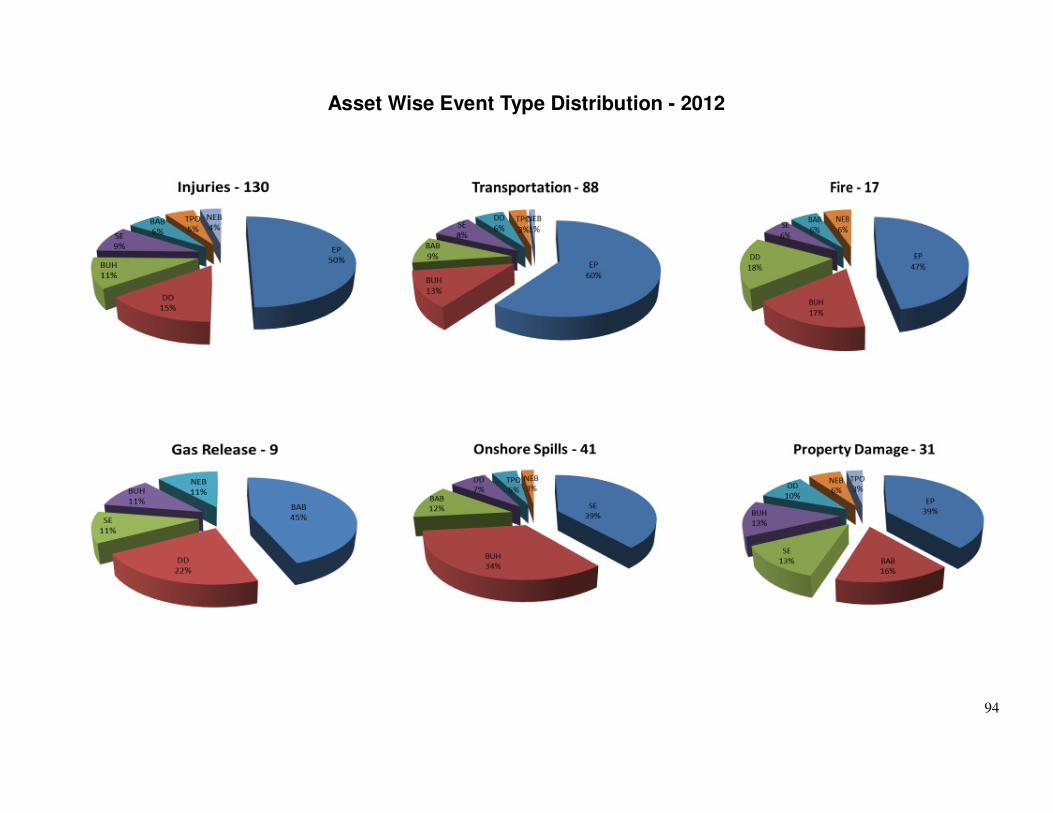
94
Asset Wise Event Type Distribution - 2012
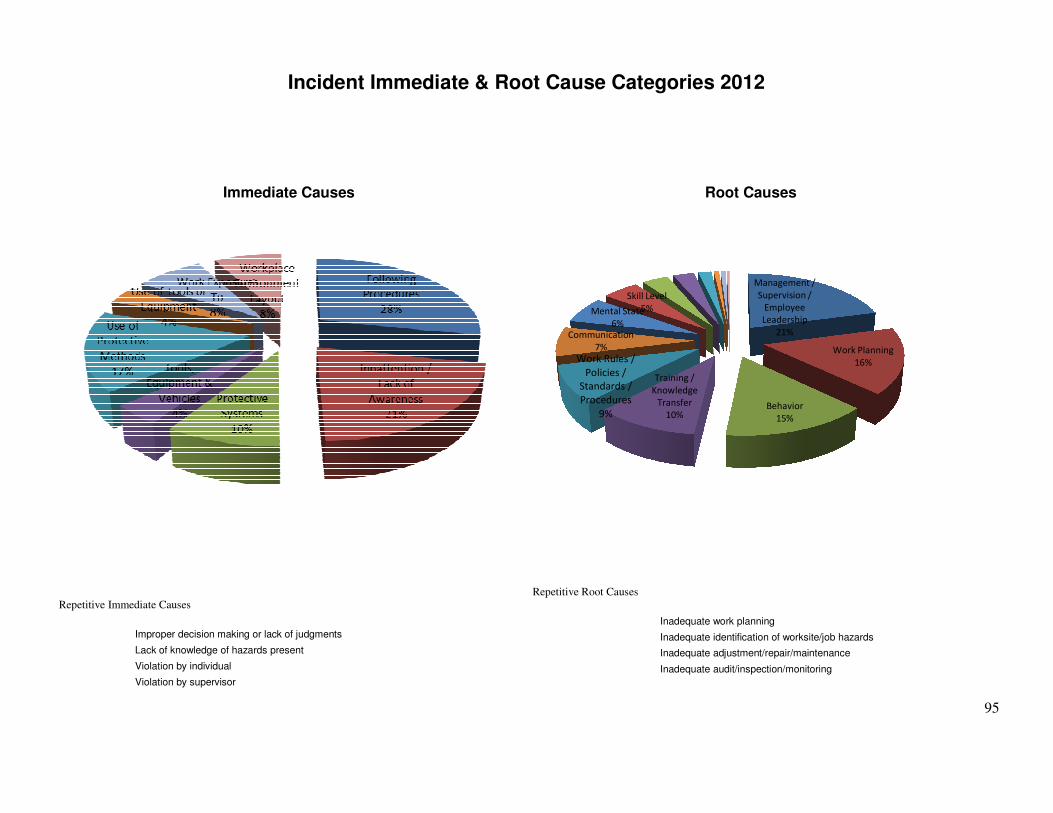
95
Incident Immediate & Root Cause Categories 2012
Immediate Causes
Root Causes
Management /
Supervision /
Employee
Leadership
21%
Work Planning
16%
Behavior
15%
Training /
Knowledge
Transfer
10%
Work Rules /
Policies /
Standards /
Procedures
9%
Communication
7%
Mental State
6%
Skill Level
5%
Repetitive Immediate Causes
Improper decision making or lack of judgments
Lack of knowledge of hazards present
Violation by individual
Violation by supervisor
Repetitive Root Causes
Inadequate work planning
Inadequate identification of worksite/job hazards
Inadequate adjustment/repair/maintenance
Inadequate audit/inspection/monitoring
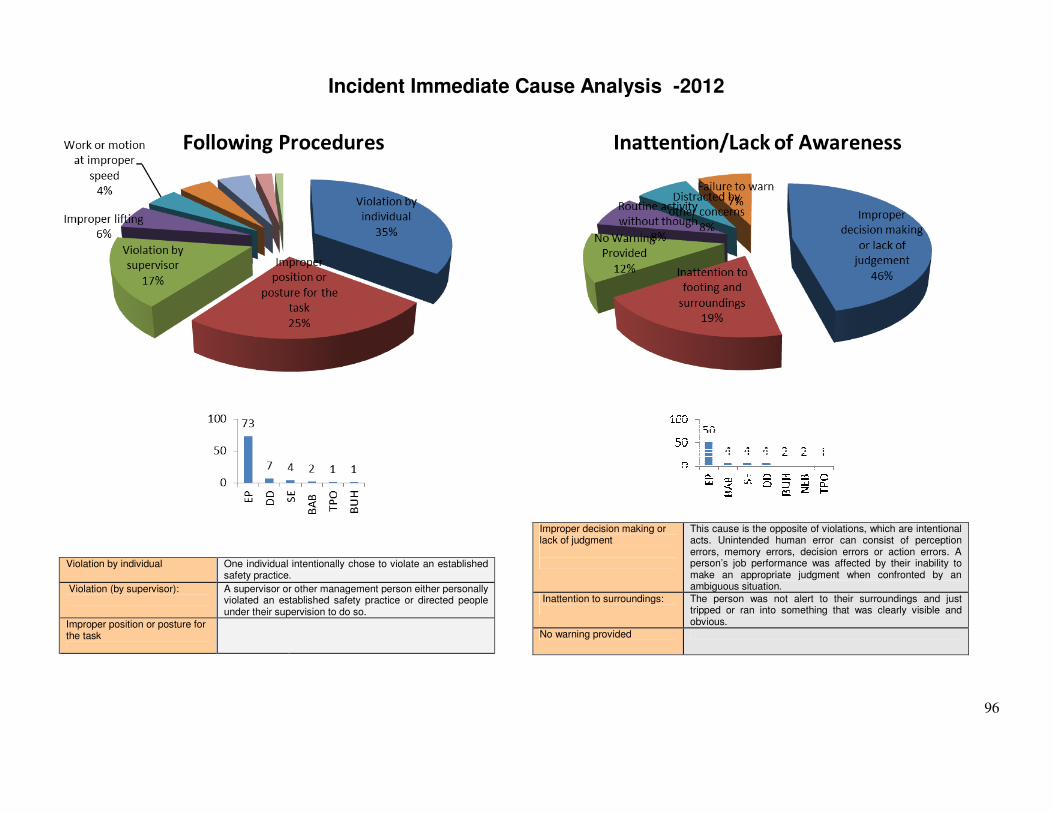
96
Incident Immediate Cause Analysis -2012
Violation by individual One individual intentionally chose to violate an established
safety practice.
Violation (by supervisor):
A supervisor or other management person either personally violated an established safety practice or directed people under their supervision to do so.
Improper position or posture for the task
Improper decision making or lack of judgment
This cause is the opposite of violations, which are intentional acts. Unintended human error can consist of perception errors, memory errors, decision errors or action errors. A person’s job performance was affected by their inability to make an appropriate judgment when confronted by an ambiguous situation.
Inattention to surroundings:
The person was not alert to their surroundings and just tripped or ran into something that was clearly visible and obvious.
No warning provided
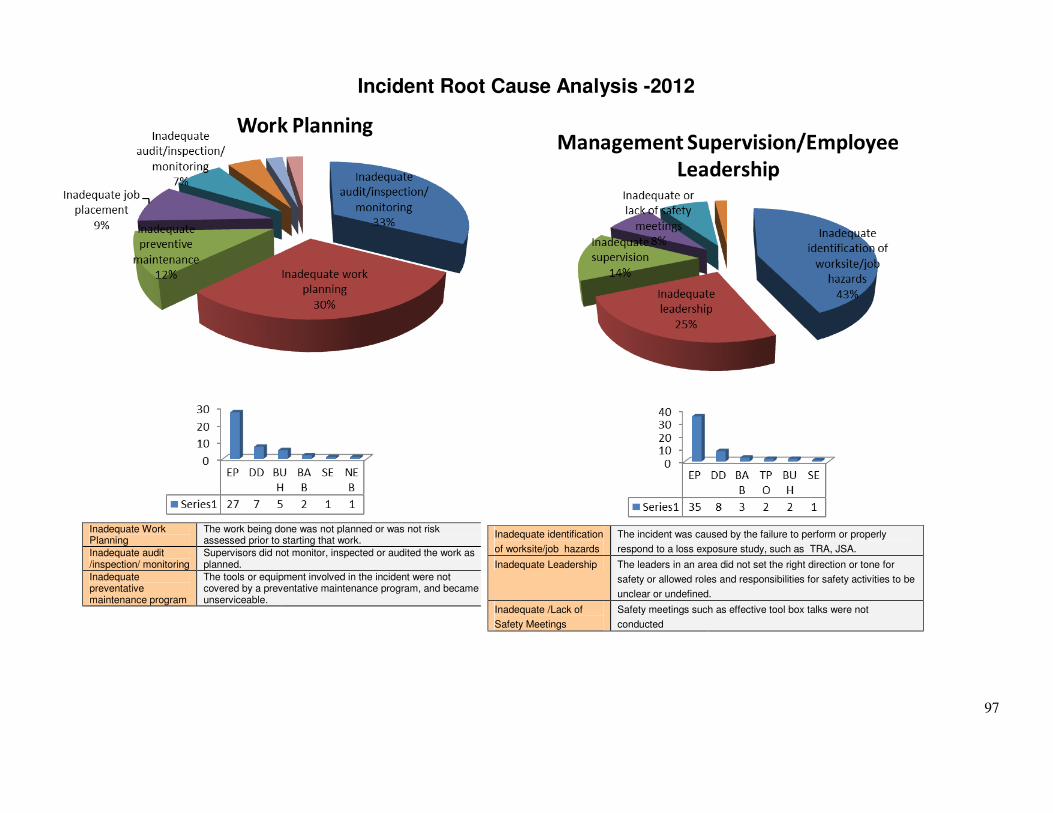
97
Incident Root Cause Analysis -2012
Inadequate Work Planning
The work being done was not planned or was not risk assessed prior to starting that work.
Inadequate audit /inspection/ monitoring
Supervisors did not monitor, inspected or audited the work as planned.
Inadequate preventative maintenance program
The tools or equipment involved in the incident were not covered by a preventative maintenance program, and became unserviceable.
Inadequate identification
of worksite/job hazards
The incident was caused by the failure to perform or properly
respond to a loss exposure study, such as TRA, JSA.
Inadequate Leadership The leaders in an area did not set the right direction or tone for
safety or allowed roles and responsibilities for safety activities to be
unclear or undefined.
Inadequate /Lack of
Safety Meetings
Safety meetings such as effective tool box talks were not
conducted
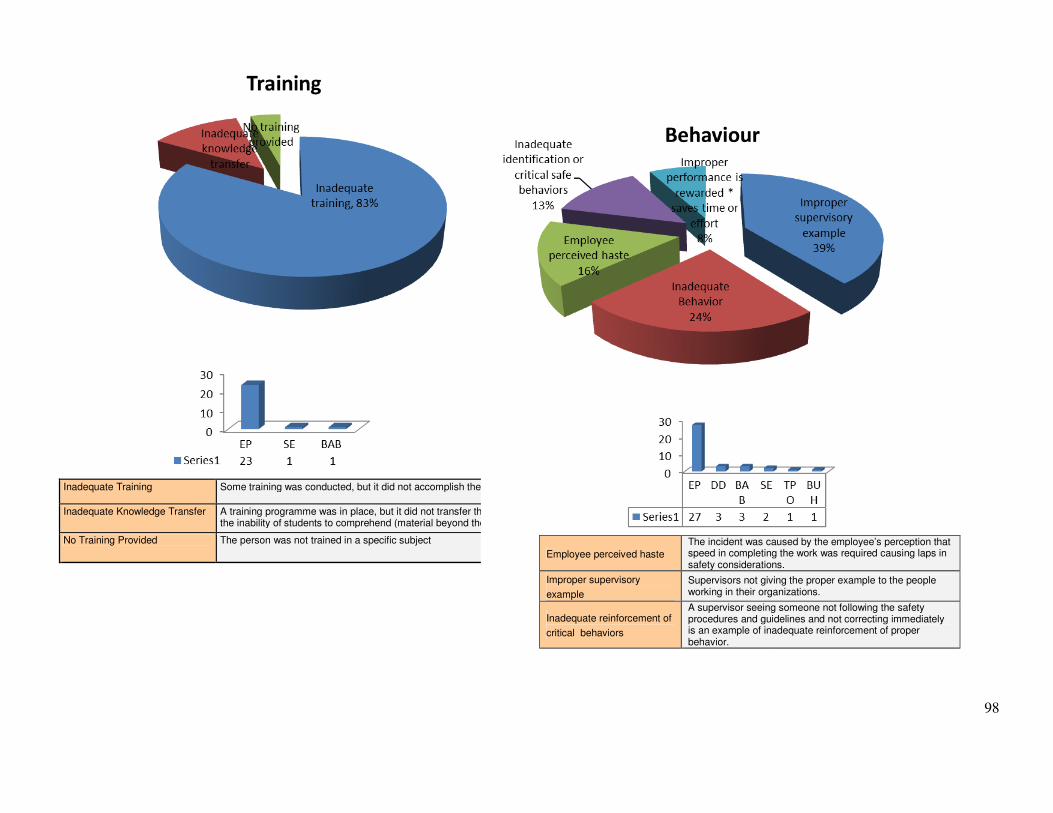
98
Inadequate Training Some training was conducted, but it did not accomplish the objectives of the training
Inadequate Knowledge Transfer A training programme was in place, but it did not transfer the necessarythe inability of students to comprehend (material beyond their level, language difficulties),
No Training Provided The person was not trained in a specific subject
Employee perceived haste
The incident was caused by the employee’s perception that speed in completing the work was required causing laps in safety considerations.
Improper supervisory
example
Supervisors not giving the proper example to the people working in their organizations.
Inadequate reinforcement of
critical behaviors
A supervisor seeing someone not following the safety procedures and guidelines and not correcting immediately is an example of inadequate reinforcement of proper behavior.

99
Do Not Compromise on the Safety of Staff & Workers, Protection of the Environment and Integrity of our assets
ABU DHABI COMPANY FOR ONSHORE OIL OPERATIONS
(ADCO)