Embed Size (px)
Citation preview

ADAD Substance Use Disorder Reform WebEx11:30-12:30
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 1
Presenters Today:
Brytanie Mertes, Charlie Mishek, Tara Holt
Teleconference call information is available in the Event info section of the WebEx.

Welcome Everyone
Presenter audio is muted until the presentation begins
If you are using your computer speakers and have trouble hearing the volume during the presentation, we recommend participating with a telephone line.
Attendee microphones are muted upon entry.
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 2
Teleconference call information is available in the Event info section

Introduction
Overview of SUD System Reform Section 1115
Waiver
Governor Dayton’s Opioid Action Plan
Updates/News
Today’s Agenda
Charlie MishekLegislative and Communications sectionAlcohol and Drug Abuse Division
Tara HoltOpioid Integration Specialist Community Supports Administration
Speakers:

Sign-Up! E-MEMO and Website Resources
• Visit our website to sign up for the E-memo to receive updates from the Alcohol and Drug Abuse Division.
• SUD Resources and presentations are posted on the SUD Reform Page at our website: DHS Website
• We are encouraging participants to review the SUD Reform e-memos and website resources available on the website prior to attending the WebEx's. These materials provide information that is helpful to understand reform and its implications.
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 4
Website Resources
• SUD Treatment Coordination (PDF & Audio)
• Comprehensive Assessment/Direct Access (PDF & Audio)
• Direct Reimbursement (PDF & Audio Recordings)
• Peer Recovery Support (PDF & Audio Recordings)
• Withdrawal Management (PDF & Audio Recordings)
• New Services in 2017 SUD Reform Legislation
• SUD Reform Implementation Timeline
• Rule 31 to 245G Table of Legislative Changes
• http://www.fast-trackermn.org/DHS SUD Site
Licensing Site:
https://mn.gov/dhs/general-public/licensing/#1
DHS Site: https://mn.gov/dhs/
https://mn.gov/dhs/partners-and-providers/news-initiatives-reports-workgroups/alcohol-drug-other-addictions/
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 5

Questions or Comments
Q & A Section:
• For technical difficulties please send your comments to “Brytanie Mertes” by selecting her name from the drop down menu in the Q&A section------->
• [email protected] and put “SUD Reform" in the subject line.
Submit questions or comments following the WebEx
Request a presentation about SUD reform (e.g. regional provider meetings, provider/county meetings, etc.)
Provide suggestions for future WebEx topics
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 6

Questions for today’s WebEx:
• Because this WebEx is happening as part of the 30 day public comment period, we are not able to take questions and answers as part of this WebEx, but
• We are interested in having any questions and comments sent in writing to [email protected] with “1115 Waiver” in the subject line.
• Any questions or comments must be sent by the end of business on March 8, 2018 so they can be part of the application, if appropriate. The public comment period closes on March 13, 2018.
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 7

Introductions
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 8

Overview: SUD System Reform Section 1115 Waiver
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 9
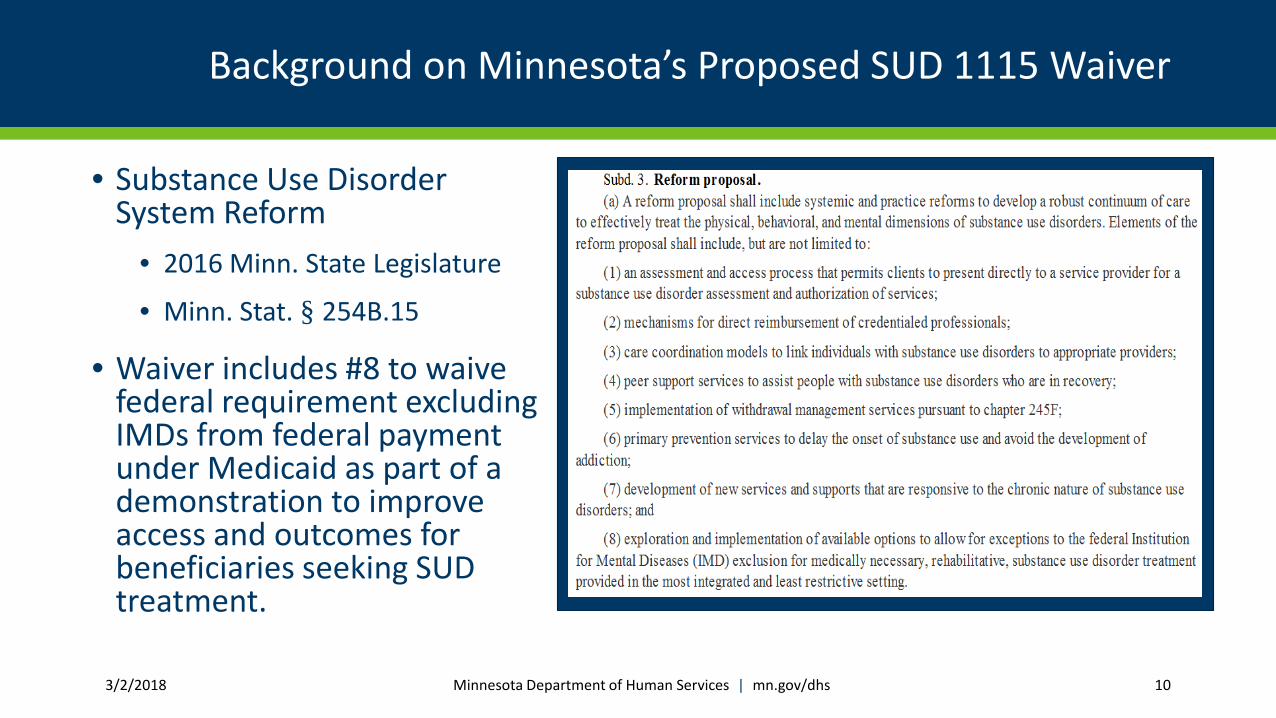
Background on Minnesota’s Proposed SUD 1115 Waiver
• Substance Use Disorder System Reform
• 2016 Minn. State Legislature
• Minn. Stat. § 254B.15
• Waiver includes #8 to waive federal requirement excluding IMDs from federal payment under Medicaid as part of a demonstration to improve access and outcomes for beneficiaries seeking SUD treatment.
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 10
Federal Section 1115 Medicaid Waiver Initiative
• Medicaid Section 1115 Demonstrations to improve access to andquality of treatment for opioid use disorder and other substance usedisorders
• State Medicaid Director Letter #17-003 “Re: Strategies to AccessOpioid Epidemic”
• Overarching Goals and Milestones
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 11
Minnesota’s SUD System Reform Waiver
• Minnesota’s SUD System Reform waiver will establish new provider delivery systems that are modeled after ASAM’s standards and continuum of care
• The state will evaluate the impact of evidence-based provider referral arrangements and practices on access to appropriate treatment, quality of care and health outcomes for Medicaid enrollees with substance use conditions
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 12

Minnesota’s SUD System Reform Waiver
• Provider referral networks that provide access to each of the levels of care recommended by the American Society of Addiction Medicine (ASAM), also known as ‘ASAM Criteria’ for treating addictive, substance-related and co-occurring conditions.
• Use of evidence-based assessment guidelines, the ASAM Six Dimensions of Multidimensional Assessment to assess treatment needs and placement.
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 13

Proposed Project Timelines
Waiver Year One: July 1, 2018 to June 30, 2019• SUD Providers with ASAM Referral Networks Established
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 14

Beginning in Year Two
Waiver Year Two: July 1, 2019 to June 30, 2020
• CCBHC continuation of Six demonstration sites established under section 223 of PAMA
• CCBHC will provide services or have MOAs with a full range of ASAM levels of care, but will not require IMD Status
• CCBHC service and payment model will continue for duration of 1115 waiver
• CCBHC Evaluation Plan will continue for duration of 1115 waiver
• Existing SUD Providers with ASAM Referral Networks Continue
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 15

Basic Requirements for Section 1115 waiver
• State must design a demonstration for afive-year period with goals, a hypothesisand an evaluation proposal that willmeasure impact of the waiver, if approved.
• State must show how its demonstrationwill promote objectives of Medicaid.
• State must submit a proposal that isbudget neutral to the federal governmentover course of waiver.
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 16
CMS, Medicaid Waivers (2017), at https://www.medicaid.gov/medicaid/section-1115-demo/index.html.
Waiver and Expenditure Authorities
State-wideness & Uniformity to permit the State to operate the demonstration on a less than statewide-basis in the geographic areas served by the participating providers in the pilot project.
Comparability to include withdrawal management as a Medicaid-covered benefit for demonstration beneficiaries prior to its approval in the State Medicaid Plan.
IMD Expenditure Authority to provide federal funding to cover services, otherwise ineligible for federal financial participation, when furnished to Medicaid beneficiaries in facilities participating in this demonstration that meet the federal definition of an Institution for Mental Disease.
CCBHC Expenditure Authority to provide federal funding to cover services through a cost-based payment structure, when furnished to Medicaid beneficiaries in clinics participating in the SUD waiver demonstration that meet the federal definition of a CCBHC.
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 17

Waiver Timeline
Timeline if CMS determines application is complete as of submission.
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 18
February March April May
State public comment period and public forums
Submit application by March 15 to CMS
CMS notifies state application is complete (within 15 days of submission)
Federal public comment period (30 days)
June
CMS decision

RFP Timeline
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 19
• RFP Timeline
March April May June July
RFP Issued
Responsesdue by May 1
Selection and
Contracting
Contracting Start of Project
Proposed Waiver Demonstration Project and Requirements
Charlie Mishek | MN Department of Human Services| Community Supports, Alcohol and Drug Abuse Division
Jeff Hunsberger| MN Department of Human Services| Community Supports, Alcohol and Drug Abuse Division3/2/2018 20
Federal requirements for SUD/IMD waivers
CMS State Medicaid Director Letter -- July 27, 2015
- Comprehensive, evidence-based benefit design
- ASAM standards of care
- Strong provider networks and a continuum of care that meets ASAM criteria
- Treatment coordination designs across the care continuum
- Coordinating/integrating SUD with physician and behavioral health care (within 2 years of waiver)
- Rigorous program integrity protocols to safeguard against fraudulent billing
- Regular utilization review to ensure clinically intensive services are medically necessary
- Community integration and settings rule compliance
- Strategies for prescription drug abuse
- SUD for youth/adolescent populations
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 21
New additional requirements from revised CMS letter
• CMS issued a new guidance on November 1, 2017; all projects must meet 6 goals and 6 milestones. The 6 goals are:
1. Increased rates of identification, initiation and engagement in treatment;
2. Increased adherence to and retention in treatment;
3. Reductions in overdose deaths, particularly those due to opioids;
4. Reduced utilization of emergency departments and inpatient hospital settings for treatment where the utilization is preventable or medically inappropriate throughimproved access to other continuum of care services;
5. Fewer readmissions to the same or higher level of care where the readmission ispreventable or medically inappropriate;
6. Improved access to care for physical health conditions among beneficiaries.
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 22

Six Milestones from revised CMS letter
The 6 milestones are:
1. Access to critical levels of care for Opioid Use Disorders (OUD) and other Substance Use Disorders, SUDs;
2. Widespread use of evidence-based, SUD-specific patient placement criteria
3. Use of nationally recognized, evidence-based SUD program standards to set residential treatment provider qualifications;
4. Sufficient provider capacity at each level of care;
5. Implementation of comprehensive treatment and prevention strategies to address opioid abuse and OUD; and
6. Improved treatment coordination and transitions between levels of care.
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 23
MN SUD Waiver Overview
This proposed project and application will test the effectiveness of new provider delivery models for SUD treatment that are modeled after ASAM’s standards and continuum of care.
Goal: To improve access to and quality of care for Medicaid beneficiaries seeking SUD treatment.
• These new models of care delivery will include residential IMDs
• This pilot will also allow for consumer choice of provider for SUD treatment, consistent with the state’s existing reform efforts
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 24

Opt-In Participation
• Each pilot will include one or more provider entities that together comprise the full ASAM level of care continuum
• Providers must either deliver all levels of care directly or have formal arrangements and the ability to facilitate access to other levels of care
• The “hub” provider in each network must use ASAM patient placement criteria to determine initial placement recommendation and facilitate on-going movement between levels of care as needed (treatment coordination)
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 25


The ASAM Dimensions and Process

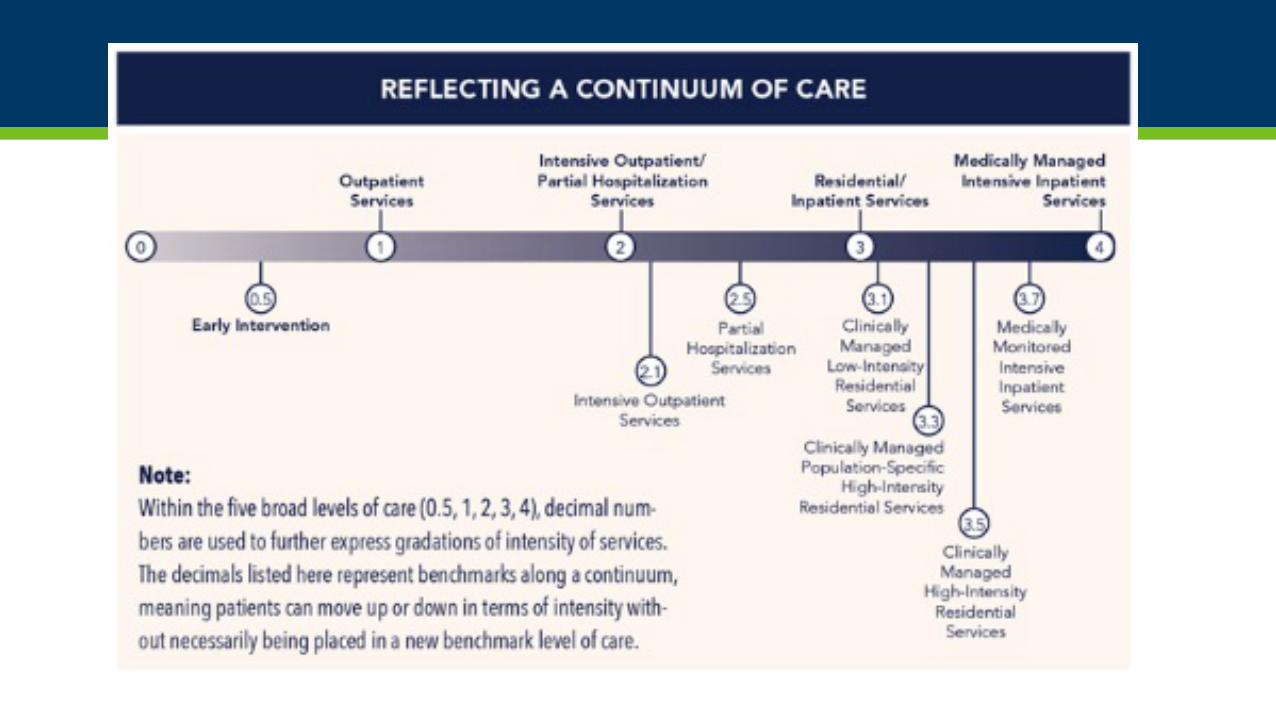
ASAM Levels of Non-Residential Care
• 0.5 Early Intervention: Assessment and intervention for at-risk persons who do not meet the diagnostic criteria for SUD
• 1.0 Outpatient Services: Less than 9 hours of service/weekly for recovery or motivational enhancement therapies/strategies
• 1.0 Opioid Treatment Program: Daily or several times weekly opioid agonist medication and counseling available to maintain multidimensional stability
• 2.1 Intensive Outpatient Services: Nine or more hours of service/weekly to treat multidimensional instability
• 2.5 Partial hospitalization Services: Twenty (20) or more hours of service/weekly for multidimensional instability not requiring 24-hour care
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 29
ASAM Levels of Residential Care
• 3.1 Clinically Managed Low-Intensity Residential Services: 24 hour structure with trained personnel; at least 5 hours of clinical service/week
• 3.3 Clinically Managed Population-Specific High Intensity Residential Services: 24 hour care with trained counselors to stabilize multidimensional imminent danger. Less intensive milieu & group treatment for those with cognitive or other impairments unable to use full active milieu or therapeutic community
• 3.5 Clinically Managed High Intensity Residential Services: 24 hour care with trained counselors to stabilize multidimensional imminent danger and prepare for outpatient treatment. Able to tolerate and use full active milieu or therapeutic community
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 30

ASAM Levels of Inpatient Care
• 3.7 Medically Monitored High Intensity Inpatient Services: 24 hour nursing care with physician availability for significant problems in Dimensions 1, 2, or 3.
• 4.0 Medically Managed Intensive Inpatient Services: 24 hour nursing care and daily physician care for severe, unstable problems in Dimensions 1, 2, or 3. Counseling available to engage patient in treatment with 16 hour/day counselor ability
ASAM Ambulatory Withdrawal Management Levels
• 1-WM Ambulatory Withdrawal Management without Extended On-site Monitoring: Mild Withdrawal with daily or less than daily outpatient supervision; likely to complete withdrawal management and to continue in treatment or recovery
• 2-WM Ambulatory Withdrawal Management with Extended On-site Monitoring: Moderate withdrawal with all day withdrawal management support and supervision; at night, has supportive family or living situation; likely to complete withdrawal management
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 32
ASAM Residential Withdrawal Management Levels
• 3.2-WM Clinically Managed Residential Withdrawal Management: Moderate Withdrawal, but needs 24-hour support to complete withdrawal management and increase likelihood of continuing treatment or recovery
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 33

ASAM Inpatient Withdrawal Management Levels
• 3.7-WM Medically Monitored Inpatient Withdrawal Management: Severe withdrawal and needs 24-hour nursing care and physician visits as necessary; unlikely to complete withdrawal management without medical, nursing monitoring
• 4-WM Medically Managed Intensive Inpatient Withdrawal Management: Severe, unstable withdrawal and needs 24-hour nursing care and daily physician visits to modify withdrawal management regimen and manage medical instability
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 34

Health Effectiveness Data and Information Set (HEDIS)
The Healthcare Effectiveness Data and Information Set (HEDIS) is a tool used by more than 90 percent of America's health plans to measure performance on important dimensions of care and service. Altogether, HEDIS consists of 81 measures across 5 domains of care
Originally, for this project, we were required to collect two HEDIS Measures, while other HEDIS were recommended; the new letter requires four HEDIS Measures, as well as Pharmacy Quality Alliance measures and other additional utilization data
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 35

Example: Required HEDIS Measure 1. NQF 0004-Initiation and Engagement
1. Number of MA patients age 13 or older who were diagnosed with a new episode of AOD between Jan. 1 and Nov 15, excluding those who had a claim with a diagnosis of AOD during the 60 days before the Index Episode Start Date or patients whose initiation of treatment is an inpatient stay with a discharge date after Dec. 1 of the measurement year
2. Number of MA patients age 13 or older who initiated treatment within 14 days of the diagnosis
3. Number of MA patients age 13 or older who had two or more additional services with a diagnosis of AOD within 30 days of the initiation visit
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 36

Required HEDIS 2. NQF 2605—Follow-up after Discharge from Emergency Department for Mental Health/Alcohol/Other Drug Dependence
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 37
Four rates are reported:
1. Percentage of ED visits for MH of patients age 18 or older identified with MH or AOD receiving follow-up within 7 days of discharge
2. Percentage of ED visits for MH of patients age 18 or older identified with MH or AOD receiving follow-up within 30 days of discharge
3. Percentage of ED visits for AOD of patients age 18 or older identified with MH or AOD receiving follow-up within 7 days of discharge
4. Percentage of ED visits for AOD of patients age 18 or older identified with MH or AOD receiving follow-up within 30 days of discharge
In Addition, CMS Requires Data Collection on the Following;
• Continuity of Pharmacotherapy for OUD (NQF #3175)
• Percentage of beneficiaries with a SUD diagnosis who used following services per month:
• Outpatient;
• Intensive Outpatient Services;
• Medication assisted treatment for OUDs and alcohol;
• Residential treatment; and
• Medically supervised withdrawal management
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 38

Additional Required Measures per CMS
• Use of Opioids at High Dosage in Persons Without Cancer- NQF #2940
• Number of overdose deaths specific to opioids
• ED visits for SUD, specifically related to OUD
• Inpatient admissions for SUD specifically related to OUDs
• 30 day readmission rates following hospitalization for SUD-related diagnosis and specifically for OUD
• Percentage of beneficiaries with an SUD diagnosis, and specifically those with OUD, who access physical care
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 39

From this 1115 project and its evaluation and data findings, DHS anticipates that our reform goals will be supplemented by a streamlined assessment process that improves access, reduces wait times and place individuals in need of treatment for Substance Use Disorders (SUD) in the correct level of treatment, at the right time, and in the correct amounts needed in order to achieve treatment outcomes
Outcomes
Questions and Answers
If you have questions and/or input after a session, please email to [email protected] with "1115 Waiver" in the subject line
Staff Contact for Further Questions and/or concerns:
Michele (Mikki) Maruska. 651.431.2178, or
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 41

Governor Dayton’s Opioid Action Plan
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 42
Tara Holt| Opioid Integration Specialist| Community Supports
Opioid Background
• Opiates versus Opioid
• Opioid overdose deaths are greater than traffic deaths, and are the leading cause of accidental death in our state.
• 1 of every 550 patients started on opioid therapy died of opioid-related causes a median of 2.6 years after the first opioid prescription
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 43

Opioid Overdose Deaths
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 44

Rx Drug Misuse: MN Minnesota Student Survey (MSS), 2016
Past 30 day prescription drug misuse higher among:
• American Indian (9.3%), Pacific Islander (9.7%), and Bi-/ Multi-Racial students (7.4%)
• Bisexual (12.2%) and gay/lesbian students (10.1%)
• Students identifying as transgender, gender queer, gender fluid, or unsure of their gender identity (12.4%)
Disparities in Opioid Overdose Deaths
3/1/2018

Department of Human Services Response to the Opioid Crisis
• The State of Minnesota is both a leader and a partner in addressing the opioid epidemic.
• We’re using existing collaborative efforts, and we’re forming new collaborations with partners inside and outside of government.
• Our actions to respond to this epidemic must be well integrated with the work of other organizations and levels of government.
• In 2012, the state established a comprehensive, multi-agency plan, State Substance Abuse Strategy, to tackle substance abuse (including opioid abuse), focusing on prevention, treatment, and recovery services.
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 46

State Substance Abuse Strategy
• The Statewide plan that established an multi-agency, multi-faceted approach to prevent and address the far-reaching impacts of drug and alcohol abuse.
AUTHORITY
• The authority of the Minnesota Department of Human Services to develop this Strategy lies in Minnesota Statutes Chapter 254A.03 which creates an Alcohol and Other Drug Abuse Section in the Department of Human Services that shall, among other things,
• coordinate and review all activities and programs of all the various state departments as they relate to alcohol and other drug dependency and abuse problems [MS 254A.03, subd.1(2)] , and
• establish a state plan which shall set forth goals and priorities for a comprehensive alcohol and other drug dependency and abuse program for Minnesota [MS 254A, subd.1(7)].
• The Strategy is intended to be a living document, revised over time to ensure relevance and currency.
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 47
State Opioid Oversight Project
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 48
• The State Opioid Oversight Project (SOOP) is the organizational structure within Minnesota state government that reports up to the Commissioners of the State Substance Abuse Strategy.
• The goal is to integrate state governmental efforts to reduce the impact of opioid use and dependence in Minnesota
• State partners include the Department of Human Services, Corrections, Education, Health, Labor and Industry, Public Safety, Pollution Control, State Judicial Branch, Board of Pharmacy, Dentistry, Medical Practice, Nursing and Podiatric Medicine.
• SOOP partners meet monthly to tackle opioid use disorder from every angle.
• The State Opioid Oversight Project is currently developing an external communications plan to propose a strategy for the integrated cross agency efforts.

DHS Opioid Initiatives
• NGA Prescription Drug Abuse Academy – 2014
• Pain.Pill.Problem. – August 2014
• State Opioid Oversight Project (SOOP)
• DHS Uniform Prescribing Work Group (UPPW)
• Integrated Care for High Risk Pregnancies (ICHRP)
• Health Services Advisory Council MAT Policy Recommendations
• Opioid Prescribing Improvement Program (OPIP) • Opioid Prescribing Work Group (OPWG)
• New 21stCentury Cures Act $5.3 million to Minnesota for 2 years
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 49

Governor Dayton's Opioid Action Plan
• This Action Plan is an overview of state government’s actions to address the opioid epidemic
• This Action Plan is a joint product of agencies that lead the State of Minnesota’s actions to address the opioid epidemic: Minnesota Department of Health, Minnesota Department of Human Services, Minnesota Department of Corrections, and Minnesota Department of Public Safety.
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 50
Contents of the Opioid Action Plan
The strategic plan includes these elements:
• Primary prevention and public health
• Prescription drug overdose and heroin overdose death prevention
• Emergency response
• Intervention and treatment
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 51

Primary Prevention
Prevention
• Engaging health care providers to improve how opioids are prescribed and used
• Building capacity, coordinating our efforts, and sharing information to maximize our impact
• Getting the right information and resources to the public
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 52
Emergency Response
Emergency Response
• Removing barriers to responding to overdoses
• Increasing access to Naloxone (also known as Narcan)
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 53

Treatment and Recovery
Treatment and recovery
• Streamlining and modernizing the state’s substance use disorder treatment system
• Deploying state efforts and resources where they can have the most impact
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 54
Law Enforcement
Law enforcement
• Integrating our work
• Increasing access to treatment
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 55

Actions Already Taken
• Expanded Access to Life-Saving Opioid Overdose Medication
• Joined National Task Force Focused on Addressing Prescription Drug Abuse
• Established Opioid Prescribing Workgroup to Reduce Abuse
• Provided Additional Support for Pregnant Women Struggling with Addiction
• Convened Tribal-State Opioid Summit to Develop Prevention and Treatment Strategies
• Improved Access to Prescription Drug Drop-Off Sites
• Secured $1.5 Million Federal Grant for Opioid Abuse Prevention
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 56
Actions Taken Continued
• Reformed Minnesota’s Substance Abuse Disorder Treatment System
• Expanded Prescription Monitoring Program to Crack Down on “Doctor Shopping”
• Secured Grant to Expand Access to Naloxone
• Mandated Addiction Risk Warning on Opioid Prescriptions
• Established Grant Programs to Expand Opioid Addiction Treatment Programs
• Expanded Access to Medication-Assisted Treatment for Opioid Addiction
• Secured $6 Million Grant to Expand Access to Medication-Assisted Treatment
• Secured $10 Million Federal Grant to Improve Opioid Prevention and Treatment
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 57

Proposed Legislative Initiatives in the Opioid Action Plan
• An “Penny-a-Pill” Opioid Stewardship Program
• Supporting American Indian, Community, and Culturally-Sensitive Opioid Abuse Prevention Efforts
• Investing in Minnesota’s Prescription Monitoring Program to Reduce Opioid Overprescribing
• Improving Access to High-quality Opioid Use Disorder Treatment
• Integrating Opioid Treatment into Other Medical Care and Community Services
• Expanding access to Life-Saving Overdose Medication
• Supporting the Efforts of Local Law Enforcement to Curb and Respond to Opioid Abuse
• Improving Treatment in Correctional Facilities
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 58
Questions
3/1/2018 Minnesota Department of Human Services | mn.gov/dhs 59
Ways to Stay Informed
• Visit our website to:• Subscribe for email updates (e-Memo)
• Learn more about substance use disorder policies and procedures, initiatives, workgroups, training and conferences, grant announcements, access forms and more
Look for ADAD “Friday’s Digest” E-memo!
• We want to hear from you about YOUR substance use disorder system. Send input to: [email protected]
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 60

Next SUD WebEx:April 5th
11:30am-12:30pm

Thank you for joining usAlcohol and Drug Abuse Division
3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 62

3/2/2018 Minnesota Department of Human Services | mn.gov/dhs 63
“The staff in the Alcohol and Drug Abuse Division are eager to work with our partners and providers to create an efficient and effective system of
prevention, early intervention, treatment and recovery that values a person’s dignity, is accessible, utilizes best practices and optimizes value. It is our hope that collaboration with all entities that are affected by, pay
for, or provide addiction services will result in a redesigned chemical health system that will become a watershed moment for the citizens of
Minnesota.”
− Brian Zirbes, Deputy Director, Alcohol and Drug Abuse Division (Stakeholder Engagement Invitation 2016)





























