Embed Size (px)
Citation preview

1653
SeCtion 14 renal Disease anD Dysfunction
CHAPTER
132Acute Renal injuryrashid alobaidi, rinaldo bElloMo, and sEan M. baGshaW
intRoDUCtion
Acute kidney injury (AKI) remains a major diagnostic and therapeutic challenge for the critical care physician. The term, AKI, describes a syndrome characterized by a rapid decrease—that is, hours to days—in the kidney’s ability to eliminate met-abolic waste and maintain volume homeostasis. Such loss of function is clinically manifested by the accumulation of end products of nitrogen metabolism such as urea and creatinine. Other typical clinical manifestations include decreased urine output (although this is not always present), accumulation of nonvolatile acids, an increased concentration of potassium and phosphate, and extravascular fluid accumulation.
ConSenSUS DeFinitionS oF AKi
There have been longstanding challenges for arriving at a uni-fied definition of AKI. In response, a consensus definition and classification for AKI has been developed and validated in hospitalized and critically ill patients. The RIFLE classifica-tion scheme provides an operational definition for AKI and stratifies it into categories of severity (risk, injury, failure, and end-stage kidney disease) (1–3). Recently, the Kidney Disease: Improving Global Outcomes (KDIGO) AKI group proposed further refinement to this classification scheme. The KDIGO classification defines AKI as the rapid deterioration of kidney function that is associated with (a) an increase in serum creati-nine by at least 0.3 mg/dL (26.5 μmol/L) within 48 hours; (b) an increase in serum creatinine at least 1.5 times above base-line over 7 days; and/or (c) oliguria with urine output below 0.5 mL/kg/hr over 6 hours (Table 132.1) (4). The KDIGO clas-sification utilizes absolute and relative changes in serum creati-nine level and urine output to define and assess the severity of kidney injury. While the KDIGO classification is an important advance in the field of AKI, the use of creatinine and urine out-put have limitations that will be discussed in the next section.
ASSeSSMent oF RenAL FUnCtion
Renal function is complex, involving acid–base balance, water balance, tonicity control, regulation of calcium and phos-phate, erythropoiesis, disposal of selected cytokines, lactate removal, and so forth. In the clinical context, however, moni-toring of renal function is reduced to the indirect assessment of glomerular filtration rate (GFR) by the measurement of serum
creatinine and urea. These waste products are insensitive markers of GFR and are heavily modified by numerous factors such as age, sex, muscle mass, nutritional status, the use of ste-roids, the presence of gastrointestinal blood, or muscle injury. They start becoming abnormal only when GFR is reduced by over 50%, and they fail to reflect dynamic changes in GFR and can be grossly modified by aggressive fluid resuscitation. Moreover, changes to serum creatinine are often delayed, requiring more than 24 hours to reach a new steady state after acute changes to GFR (5,6). The use of creatinine clearance via a 2- or 4-hour urine collection or of calculated clearance by means of formulae might increase the accuracy of GFR estima-tion but rarely changes clinical management. The use of more sophisticated radionuclide-based tests is cumbersome in the ICU and useful only for research purposes.
Urine output is another commonly measured parameter of renal function and is often more sensitive to changes in renal hemodynamics than biochemical markers of solute clearance. However, urine output alone is also of limited value, with patients capable of developing severe AKI, as detected by a markedly elevated serum creatinine, while maintaining normal urine output (so-called nonoliguric AKI). Some data suggest that the use of urine output of 0.5 mL/kg/hr might be too sensi-tive in detecting AKI, and that lower threshold of 0.3 mL/kg/hr may better correlate with outcome (7). While an episode of oli-guria may not always be followed by increments in serum cre-atinine consistent with AKI, oliguria still remains a valuable bedside predictor of early changes on kidney function (8,9). Recent evidence has shown a strong association between the duration and frequency of episodes of oliguria and increased risk for mortality (10,11).
Classic urine biochemistry and derived indices such as mea-surement of urinary sodium, fractional excretion of sodium and urea, have been promoted to help clinicians identify and classify AKI (Table 132.2). Unfortunately, their accuracy and significance are questionable (Fig. 132.1) (12–15). The clinical value of these tests in ICU patients who receive vasopressors, massive fluid resuscitation, and loop diuretics is low. Instead, recent evidence suggests urinary sediment for renal epithelial cells and casts can provide prognostic information about the risk for worsening AKI (Table 132.3). A higher urinary sedi-ment score, defined by a greater quantity of measured cells and casts in the urine, can help discriminate AKI severity and better inform a patients’ risk for worsening AKI (16).
The precise role of novel kidney damage biomarkers (e.g., cystatin C; neutrophil gelatinase-associated lipocalin [NGAL]; insulin-like growth factor-binding protein 7 [IGFBP7] and tis-sue inhibitor of metalloproteinases-2 [TIMP-2]; kidney injury
LWBK1580-CH132_p1651-1665.indd 1653 01/08/17 6:58 PM

1654 SECTion 14 rEnal disEasE and dysFunction
to changes in population demographics, baseline suscepti-bilities, and comorbid diseases, and greater exposure to more complex and technologically advanced procedures and treat-ments (i.e., immune suppression; chemotherapy; organ trans-plantation; cardiac surgery).
Several risk factors for AKI in ICU patients have been identified including baseline (nonmodifiable) susceptibili-ties and potentially modifiable events or factors. These risk factors include older age, male sex, preexisting comorbid ill-ness, a diagnosis of sepsis, cardiogenic shock, major surgery (specifically cardiac surgery), hypovolemia, and exposure to nephrotoxic drugs (18,19). In addition, multiorgan dysfunc-tion, specifically concomitant acute circulatory, pulmonary, and hepatic organ dysfunction, is commonly associated with AKI (Table 132.4) (20–22).
PReSentAtion AnD CLiniCAL CLASSiFiCAtion
The clinical presentation of AKI may vary according to the etiology and the severity. AKI may be clinically silent until there are overt changes to serum creatinine (which is depen-dent on serum creatinine being routinely monitored in “at-risk” patients) and/or urine output. Urine output is often, but not always, decreased. As kidney function worsens, electro-lyte disturbances such as hyperkalemia, hyperphosphatemia, metabolic acidosis due to diminished clearance of acid, and fluid accumulation occur. In those patients not carefully moni-tored or untreated, disruption of metabolic and fluid balance homeostasis can lead to life-threatening complications such as ventricular dysrhythmias and pulmonary edema.
Table 132.2 laboratory Tests to Differentiate Prerenal aKI from established aKI
Test Prerenal aKI established aKI
urine sediment normal Epithelial casts
specific gravity high: >1.020 low: <1.020
urine sodium (mmol/l) low: <10 high: >20
Fractional excretion of sodium
<1% >1%
Fractional excretion of urea <35% >35%
urine osmolality (mosm/kg h2o)
high: >500 near serum: <300
urine/Plasma creatinine ratio high: >40 low: <10
Plasma urea:creatinine ratio high normal
Table 132.1 KDIGO aKI Staging
Stage Serum Creatinine Urine Output
1 1.5–1.9 times baselineorincrease of ≥0.3 mg/dl
(≥26.5 mmol/l)
<0.5 ml/kg/hr for 6–12 hr
2 2.0–2.9 times baseline <0.5 ml/kg/hr for ≥12 hr
3 3.0 times baselineorincrease of ≥4.0 mg/dl
(≥353.6 mmol/l)orinitiation of renal replace-
ment therapyorin patients <18 yr,
decrease in eGFr to <35 ml/min per 1.73 m2
<0.3 ml/kg/hr for ≥24 hroranuria for ≥12 hr
molecule-1 [KIM-1]; interleukin-18 [IL-18]; L-type fatty acid binding protein (L-FABP]) detectable in the blood and urine, while very promising for the earlier detection of patients at risk for developing AKI and for the earlier diagnosis of kidney damage, are still undergoing investigation to optimally under-stand their use to inform bedside clinical decision support (i.e., when to start renal replacement therapy [RRT]).
ePiDeMioLoGy
In a recent systematic review of 312 studies including 49 mil-lion patients, the syndrome of AKI (according to KDIGO defi-nition) was found to affect 1 in 5 adults and 1 in 3 children during hospital admission (17). A degree of acute renal injury (manifested by release of NGAL, albuminuria, loss of small tubular proteins, or inability to excrete a water load, sodium load or an amino acid load, or any combination of the above) can be demonstrated in most ICU patients. Using the RIFLE classification, the incidence of at least some degree of AKI has been reported as high as 67% in a study of more than 5,000 critically ill patients (3). The development of AKI with a maximum RIFLE category Failure has been reported in up to 28% of critically ill patients and is associated with a several fold increased risk of in-hospital death (2,3). Recent trends have suggested that the incidence of AKI may be increasing, in particular in critically ill patients. This may be attributable to improved recognition and reporting with the introduction of consensus definitions; however, this is also likely attributable
1.8
1.6
1.4
1.2
1
0.8
0.6
0.4
0.2
0baseline 12hr 24hr 36hr 48hr
P < 0.01
FeN
a [%
]
Control
Septic
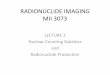
FiGURe 132.1 histogram showing the effect of experimental sep-sis in sheep on the fractional excretion of sodium (Fena). Fena decreased in sepsis as would be expected during decreased perfusion. in fact, all experimental animals had a twofold to threefold increase in renal blood flow, providing proof of the concept that Fena cannot be used to infer renal hypoperfusion.
LWBK1580-CH132_p1651-1665.indd 1654 01/08/17 6:58 PM

CHAPTER 132 acute renal injury 1655
The contributing factors for AKI can largely be categorized into conditions that alter renal hemodynamics, conditions that cause direct kidney injury, or conditions that contribute to the obstruction of urine flow. Often patients will present with multiple concurrent and temporally associated contribut-ing factors for AKI. The early identification of precipitating causes is essential for limiting the extent of ongoing injury and promoting repair and recovery.
Alternation to kidney hemodynamics, due to either or both systemic and regional factors, is likely the most common etiology for AKI in the ICU. These include events that affect systemic hemodynamics by causing decrease of extracellular volume (i.e., hypovolemia, dehydration, hemorrhage, burns), redistribution of that volume (i.e., capillary leak in sepsis, pan-creatitis, or hepatic failure), events associated with decreased cardiac output (i.e., myocardial infarction, heart failure, septic cardiomyopathy), or those associated with low perfusion pres-sure (i.e., anaphylaxis). Kidney function can also be impacted by alterations to regional kidney hemodynamics. Processes that alter afferent (i.e., nonsteroidal anti-inflammatory drugs) and/or efferent arteriolar tone (i.e., ACE inhibitors/ARB) can adversely impact glomerular filtration.
Less commonly, AKI can present where the principal source of damage is within the kidney and where typical structural
changes can be seen on microscopy. Numerous disorders, which affect the glomerulus or the tubule, may be responsible. Among these, nephrotoxins are particularly important, especially in hospitalized patients (23). The most common nephrotoxic drugs affecting ICU patients are listed in Table 132.5. Many cases of drug-induced AKI rapidly improve upon removal of the offending agent. Accordingly, a careful history of drug adminis-tration is essential in all patients with AKI.
More than a third of patients who develop AKI in ICU have chronic kidney disease (CKD) due to factors such as age-related changes in nephron mass, longstanding hypertension, diabetes mellitus, or atheromatous disease of the renal ves-sels. Such CKD may be manifest by a prehospital elevation in serum creatinine or evidence of proteinuria; however, this may not be universally evident or known. Often, what may seem to the clinician as a relatively trivial kidney insult may unmask more significant AKI due to a lack of renal functional reserve related to subclinical pre-existing CKD.
Obstruction to urine outflow is a common cause of func-tional AKI in the community (24), but is uncommon in the ICU. The pathogenesis of obstructive AKI involves several humoral responses as well as mechanical factors. Typical causes of obstructive AKI include bladder neck obstruction from an enlarged prostate, ureteric obstruction from pelvic tumors or retroperitoneal fibrosis, papillary necrosis, or large calculi. The clinical presentation of obstruction may be acute or acute-on-chronic in patients with longstanding renal calculi. It may not always be associated with oliguria. If obstruction is suspected, ultrasonography can be easily performed at the bedside. How-ever, not all cases of acute obstruction have an abnormal ultra-sound and, in many cases, obstruction occurs in conjunction with other renal insults (e.g., staghorn calculi and severe sepsis of renal origin). The use of medications that lead to urinary reten-tion in those without an indwelling urinary catheter may exacer-bate the presentation. Assessment of the role of each factor and overall management should be conducted in conjunction with an urologist. Finally, the sudden and unexpected development of anuria in an ICU patient should always suggest obstruction of the urinary catheter as the cause. Appropriate flushing or chang-ing of the catheter should be implemented in this setting.
Clinical risk prediction tools can be utilized to identify patients at greater risk of AKI. Those at high-risk patients can be monitored closely for development of AKI including frequent assessments of serum creatinine, continuous urine
Table 132.3 Urinary Sediment Scoring System (16)
Score Description
1 rtE cells 0 and granular casts 0
2 rtE cells 0 and granular casts 1–5, orrtE cells 1–5 and granular casts 0
3 rtE cells 1–5 and granular casts 1–5 or rtE cells 0 and granular casts 6–10, or
rtE cells 6–20 and granular casts 0
rtE, renal tubular epithelial.
Table 132.5 list of Medications Known to be associated with Nephrotoxicity (26)
acyclovirambisomeamikacinamphotericin bcaptoprilcarboplatincefotaximeceftazidimecefuroximecidofovircisplatincolistimethatecyclosporinedapsoneEnalapril
EnalaprilatFoscarnetGadopentetateGadoxetate GanciclovirGentamicinibuprofenifosfamideiodixanoiohexoiopamidoioversolketorolaclisinoprillithium
MesalamineMethotrexatenafcillinPiperacillin/tazobactamPiperacillinsirolimussulfasalazinetacrolimusticarcillin/clavulanic acidtobramycintopiramatevalacyclovirvalganciclovirvancomycinzonisamide
Table 132.4 aKI Risk Factors
baseline Susceptibilities•older age•Male sex•black race•Pre-existing chronic kidney disease•Proteinuria•hypertension•diabetes mellitus•heart failure•chronic liver disease•Peripheral vascular disease•Malignancy•obesity
Modifiable Risk Factors•anemia•critical illness•sepsis•trauma•cardiopulmonary bypass•Major noncardiac surgery•rhabdomyolysis•Exposure to radiocontrast agents•nephrotoxic drugs•Fluid accumulation/overload•high-risk emergency procedures• intra-abdominal hypertension
LWBK1580-CH132_p1651-1665.indd 1655 01/08/17 6:58 PM

1656 SECTion 14 rEnal disEasE and dysFunction
output monitoring, and strict avoidance of nephrotoxins. For example, Kheterpal et al. (25) developed and validated a clini-cal risk score for AKI for patients undergoing general surgery. Five classes of risk were created based on the presence of 11 preoperative risk factors. The risk index showed progressively greater AKI risk with higher class, with a 9% risk in those in Class V (at least six risk factors) compared to a 0.2% risk in those with Class I (up to two risk factors).
Modern clinical information systems can be designed to trigger alerts to clinicians for “at-risk” patients who are devel-oping early AKI or who are exposed to unnecessary nephro-toxins. Recently, the use of automated alerting from clinical information systems that can integrate bedside information such as urine output, laboratory information such as abso-lute and relative changes in serum creatinine, and pharmacy information, such as potential nephrotoxin exposure have been shown to improve the recognition of AKI in hospitalized patients. Electronic alerting has been shown to translate into earlier interventions, reduce severity among those developing AKI, and improve outcomes (26,27).
PAthoGeneSiS oF SPeCiFiC SynDRoMeS
septic aKi
Sepsis is a leading predisposing factor to AKI in critically ill patients (19). Epidemiologic studies estimate between 45% and 70% of all AKI encountered in the ICU is associated with sepsis (18,19,28). The distinction between septic and non-septic AKI may have particular clinical relevance considering recent evidence to suggest that septic AKI may be character-ized by a unique pathophysiology (29–32).
The classic teaching is that sepsis brings about hypotension, leading to a reduction in critical organ blood flow including in the kidney, causing ischemic injury and AKI. Furthermore, sepsis would lead to activation of the sympathetic nervous system, stimulating the release of potent vasoconstrictors that induce renal vasoconstriction and aggravate kidney ischemia, thus worsening AKI. However, growing evidence questions this ischemic-induced paradigm of septic AKI (29,30,32). An experimental study in a large mammalian model of hyper-dynamic sepsis found that RBF was marked increased above baseline despite significant reductions in kidney excretory function (Fig. 132.2) (31). These findings are supported by small clinical studies of resuscitated patients with septic AKI that also show increases in RBF (33–35). The implications are that in hyperdynamic sepsis, AKI is hyperemic, rather than ischemic, with global RBF considerably increased. More-over, experimental studies have shown that regional cortical and medullary RBF are preserved in sepsis and can be further augmented by infusion of norepinephrine (Fig. 132.3) (36). This concept of hyperemic AKI in sepsis is consistent with the relative paucity of renal histopathologic evidence of tubular necrosis in patients with septic AKI (37).
Thus, evolving evidence suggests that the pathogenesis of septic AKI predominantly involves toxic and immune- mediated mechanisms. Sepsis is known to release a vast array of pro- and anti-inflammatory mediators such as cytokines (damage-associated molecular proteins [DAMPs] and patho-gen-associated molecular proteins [PAMPs], arachidonic acid metabolites, and thrombogenic agents that all may participate in the development of AKI (38). Similarly, experimental studies have found evidence of renal tubular cell apoptosis in response to inflammatory mediators in endotoxemia (39,40). Renal tubular apoptosis may prove an important mechanism of sep-tic AKI in critically ill patients (37,41,42). No studies exist to
P < 0.01700
600
500
400
300
200
100
0Baseline 12hr 24hr 36hr 48hr
Control
Septic
Ren
al B
lood
Flo
w (
ml/m
in)
1009080706050403020100
p < 0.0001
BSL 1 hour 6 hours
Norepinephrine
Dopamine
Mea
n A
rter
ial P
ress
ure
(mm
Hg)
*Norepinephrine added
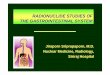
FiGURe 132.2 histogram showing the effect on renal blood flow of experimental sepsis in sheep. renal blood flow increased threefold while creatinine increased from 80 to 400 μmol/l, providing evidence that acute renal failure in sep-sis can occur during renal hyperemia.
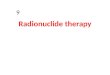
FiGURe 132.3 histogram showing the effect of norepinephrine on mean arterial blood pressure (MaP) compared to high-dose dopamine in a randomized controlled trial in humans. MaP is more reliably restored using norepinephrine when given alone as an alternative to high-dose dopamine or after high-dose dopamine has failed. bsl, baseline.
LWBK1580-CH132_p1651-1665.indd 1656 01/08/17 6:58 PM

CHAPTER 132 acute renal injury 1657
tell us which of the above mechanisms are most important and when they might be active in the course of an episode of sep-tic AKI. However, interventions with antiapoptotic properties, such as with selective caspase inhibitors, may theoretically aid in attenuating kidney injury and promote recovery of function (38). To date, however, no human randomized controlled tri-als have assessed the impact of these interventions on kidney function and their value is unknown.
aKi in association with Major surgery
AKI is a common complication following major surgery (19, 43). The incidence is variable and dependent on the prevalence of pre-existing comorbid illnesses, preoperative kidney func-tion, and the type and urgency of surgery being performed. Numerous intraoperative events can act to negatively affect kidney function, including the following:• Hemodynamic instability (e.g., intravenous or inhaled anes-
thetic agents)• Hypovolemia due to blood loss or third spacing• Details of the operative field (e.g., aortic cross-clamping in
major vascular surgery)• Increases in intra-abdominal pressure (e.g., laparoscopic
insufflation of CO2)• Concomitant sepsis• Use of nephrotoxin drugs
Any of these factors, alone or in combination, may con-tribute to a critical reduction in RBF and ischemia, impaired oxygen delivery, and toxin- or inflammatory-mediated injury. Postoperative AKI is believed to be, in part, mediated by pro-inflammatory mechanisms such as increased endothelial cell adhesion, tubular cell infiltration, generation of reactive oxy-gen species, proinflammatory cytokines, and reperfusion injury (44,45). Cardiac surgery with cardiopulmonary bypass (CPB) commonly induces early postoperative AKI. The mechanisms whereby CPB causes injury are incompletely understood, although there is a suggestion that CPB is proinflammatory, activating components of the nonspecific immune system. In turn, this leads to oxidative stress with the generation of oxygen-free radical species and serum lipid peroxidation prod-ucts (46). In addition, CPB has been shown to deplete serum antioxidative capacity for a prolonged duration after surgery. Such oxidant stress has been shown to directly induce kidney injury in experimental studies (47).
Surgery-specific clinical prediction tools have been devel-oped and validated to assess risk and predict AKI after surgery. Such tools can be utilized to identify patients at greater risk of perioperative AKI prior to planned procedures or among those requiring urgent or emergent procedures. These patients can be triaged to higher levels of perioperative monitoring if indi-cated (i.e., high-dependency units or intensive care; frequent assessments of serum creatinine; continuous urine output monitoring; strict avoidance of nephrotoxins).
Hepatorenal syndrome
This condition is a form of AKI, which typically occurs in the setting of advanced cirrhosis; however, it can occur with severe liver dysfunction due to alcoholic hepatitis or other forms of acute hepatic failure (48). The recent consensus definition of HRS includes any form of kidney disease occurring in patients with cirrhosis regardless of etiology (Table 132.6) (49). The
pathogenesis of hepatorenal syndrome (HRS) is incompletely understood; however, there are several potential mechanisms that may contribute to HRS, including activation of the renin–angiotensin system in response to systemic hypotension, activation of the sympathetic nervous system in response to systemic hypotension and increased intrahepatic sinusoidal pressure, increased release of arginine vasopressin due to sys-temic hypotension, and reduced hepatic clearance of various vascular mediators such as endothelin, prostaglandins, and endotoxin (48,50).
Although HRS can occur spontaneously in patients with advanced cirrhosis, it is important to recognize that other precipitants are much more common. These include sepsis, specifically spontaneous bacterial peritonitis (SBP), raised intra-abdominal pressure due to tense ascites, bile acid nephropathy in those with severe hyperbilirubinemia, gastrointestinal bleed-ing, and hypovolemia due to paracentesis, diuretics and/or lactulose, or any combination of these factors. Likewise, other contributing factors to AKI should be routinely assessed for including cardiomyopathy due to alcoholism, nutritional defi-ciencies or viral infection, and exposure to nephrotoxins.
Typically, HRS develops in patients with advanced cir-rhosis and evidence of portal hypertension with ascites in the absence of other apparent causes of AKI. It generally presents as oligo-anuria with progressive increases in serum creatinine and/or urea and bland urinary sediment. These patients develop profound sodium and water retention with evidence of hyponatremia, a urine osmolality higher than that of plasma, and a very low urinary sodium concentration (<10 mmol/L).
Management of the patient with HRS can be challenging. However, it should include the systematic identification and prompt treatment of potential reversible precipitants (i.e., sep-sis). The avoidance of hypovolemia by albumin administration in patients with SBP has been shown to decrease the incidence
Table 132.6 Summary of the Diagnostic Criteria for Kidney Dysfunction in Chronic liver Disease and Hepatorenal Syndrome (49)
Diagnosis Definition
aki •↑ in scr ≥50% from baseline or ↑ scr >0.3 mg/dl (26.5 µmol/l)
•type-1 hrs is a specific form of aki
ckd •GFr <60 ml/min for >3 mo calculated using Mdrd-6 formula
acute on ckd
•↑ in scr ≥50% from baseline or ↑ scr >0.3 mg/dl (26.5 µmol/l) in a patient with cirrhosis whose GFr is <60 ml/min for >3 mo calculated using Mdrd-6 formula
hepatorenal syndrome
•confirmed diagnosis of cirrhosis with ascites•scr >1.5 mg/dl (132.6 µmol/l)•no improvement in scr (<1.5 mg/dl
[132.6 µmol/l]) after 2 d of diuretic with-drawal and volume expansion
•absence of shock•no current or recent exposure with nephro-
toxin medications•absence of parenchymal kidney disease as
indicated by proteinuria > 0.5 g/d, micro-hematuria (>50 cells/hpf) and/or abnormal ultrasonography
aki, acute kidney injury; ckd, chronic kidney disease; scr, serum creatinine.Mdrd-6: GFr = 170 × scr (mg/dl) – 0.999 × age – 0.176 × 1.180 (if black) × 0.762
(if female) × serum urea nitrogen – 0.170 × albumin 0.138.
LWBK1580-CH132_p1651-1665.indd 1657 01/08/17 6:58 PM

1658 SECTion 14 rEnal disEasE and dysFunction
of AKI in a randomized controlled trial (51). These causes must be looked for and promptly treated. Some studies suggest that vasopressin derivatives (i.e., terlipressin) may improve GFR in this condition (52,53). Other treatment options include oral α-adrenergic agonist midodrine with subcutaneous octreotide or referral for albumin-based extracorporeal therapies. Place-ment of a transjugular intrahepatic portosystemic stent-shunt (TIPS) has been associated with modest improvements in kid-ney function in those with HRS, may improve outcome and represent a measure for those who are not a candidate for or awaiting transplant (54,55). In general, the ideal solution for reversal of AKI in these patients is either improvement in hepatic function by therapy for the underlying primary liver disease and/or referral for and successful liver transplantation.
aKi with rhabdomyolysis
The incidence of rhabdomyolysis-induced AKI is estimated at 1% in hospitalized patients but it may account for close to 5% to 7% of cases of AKI in critically ill patients depending on the setting (23,28). Its pathogenesis involves the interplay of pre-renal, intrarenal, and postrenal factors including concurrent hypovolemia, ischemia, direct tubular toxicity mediated by the heme pigment in myoglobin, and intratubular obstruction (56). The causes of muscle injury that can result in rhabdomyolysis include major trauma, burns, drug overdose (i.e., narcotics, cocaine, or other stimulants), vascular embolism, prolonged seizures, neuroleptic malignant syndrome, various infections (i.e., pyomyositis, necrotizing fasciitis, influenza, HIV), severe exertion, impaired cellular energy production (i.e., hereditary enzyme disorders, toxins), increased calcium influx (i.e., malig-nant hyperthermia), alcoholism, and in response to a variety of agents which can interact to induce major muscle injury (i.e., combination of macrolide antibiotics or cyclosporin and statins). The clinical manifestations of rhabdomyolysis include an elevated serum creatine kinase and evidence of pigmented granular casts and red to brown coloring of the urine. Patients can also have various electrolyte disorders as a result of mus-cle breakdown including hyperphosphatemia, hyperkalemia, hypocalcemia, and hyperuricemia.
The principles of prevention of AKI include identification and elimination of potential causative agents and/or correction of underlying compartment syndromes; prompt and aggres-sive fluid resuscitation and maintenance of polyuria (i.e., ≥1.5 to 2 mL/kg ideal or adjusted body weight per hour, usu-ally more than about 300 mL/hr to restore vascular volume and potentially flush obstructing cellular casts); and urine alkalinization to a goal pH above 6.5 in order to reduce renal toxicity by myoglobin-induced lipid peroxidation and improve the solubility of myoglobin (56). Experimental studies have suggested mannitol may act as a scavenger of free radicals and reduce cellular toxicity; however, the role of forced diure-sis with mannitol remains controversial. Other controversial therapies include allopurinol; deferoxamine; dantrolene, and glutathione, and high volume and/or high cut-off membrane hemofiltration.
aKi due to nephrotoxins
Several mechanisms have been reported to play a role in the development of kidney injury after exposure to nephrotoxins. Particular drugs can often invoke a variety of pathophysiologic
effects on the kidney that collectively contribute to AKI. Alter-ations in intra-renal hemodynamics are an important initial consequence of many nephrotoxins. These changes to regional renal blood flow may occur through increased activity of local vasoconstrictors such as angiotensin II, endothelin, adenos-ine; at the same time, there is diminished activity of impor-tant vasodilators (i.e., nitric oxide and prostaglandins). This imbalance can lead to renal vasoconstriction and ischemia, particularly to susceptible regions such as the outer medulla, for example, in response to radiocontrast media, or can induce humorally mediated vasoconstriction of afferent arterioles as a result of exposure to NSAIDs and cyclosporine. The end result of a reduction in regional blood flow is a critical reduction in oxygen delivery, thus predisposing to tubular hypoxia (57). In addition, nephrotoxins can directly contribute to impaired tubular metabolism and oxygen utilization. They lead to gen-eration of radical oxygen species including superoxide anions, hydrogen peroxide, hydroxyl radicals, reduction in intrinsic antioxidant enzyme activity, accumulation of intracellular cal-cium, mitogen-activated protein kinases, and phospholipase A2, for example, after exposure to aminoglycosides (58–60).
These responses to nephrotoxins can induce tubular cell vacuolization, interstitial inflammation, altered cell membrane properties, and disruption of normal tubular adhesion to base-ment membranes. Failure of these mechanisms contributes to tubular cell apoptosis, necrosis and tubular sloughing into the luminal space, cast formation, and obstruction (58). Raised intraluminal pressures due to obstruction, altered cellular per-meability, and interstitial inflammation can contribute back diffusion of fluid and secondary edema formation.
Radiocontrast media and aminoglycosides are leading agents contributing to nephrotoxin-induced AKI (61,62). Radiocontrast media–induced toxicity is believed to occur from the interplay of alterations in renal hemodynamics due to vaso-constriction, increased intravascular viscosity and erythrocyte aggregation, direct tubular epithelial cell toxicity, and concomi-tant atheroembolic microshowers in the renovasculature. Ami-noglycosides are taken up via organic anion transport systems in the proximal tubules where they accumulate and generate radical oxygen species, increased intracellular calcium, which lead to tubular apoptosis, necrosis, and nonoliguric AKI.
radiocontrast-induced nephropathy
Radiocontrast-induced nephropathy (RCIN) is the leading cause of iatrogenic AKI in hospitalized patients and results in prolonged hospitalization, higher mortality rates, excessive health care costs, and potentially long-term kidney impair-ment (23). RCIN presents with an acute rise in serum creati-nine within 24 to 48 hours following injection of radiocontrast media. The serum creatinine level generally peaks within 3 to 5 days and returns toward baseline within 7 to 10 days; however, in some patients kidney function may not return to baseline and a persistent reduction in function may occur. RCIN is often asso-ciated with pre-existing risk factors, in particular pre-existing CKD (GFR <60 mL/min/1.73 m2), a diagnosis of diabetes mel-litus, and use of large quantities of radiocontrast media.
There are few effective prophylactic or therapeutic inter-ventions with evidence for reducing the occurrence of radio-contrast nephropathy and no therapy has proven effective once it is established (63). Strategies for prevention include early identification of patients at risk, consideration to either delay
LWBK1580-CH132_p1651-1665.indd 1658 01/08/17 6:58 PM

CHAPTER 132 acute renal injury 1659
of the investigation, or using alternative modality until kid-ney function can be optimized. Likewise, every effort should be made correct volume depletion and discontinue potential nephrotoxins. There is no evidence to support the routine use of diuretics, mannitol or dopamine. Studies have shown that periprocedure hydration and use of nonionic iso-osmolar (e.g., iodixanol) radiocontrast media can reduce the risk (64–67). Several randomized trials and meta-analyses have suggested potential benefit with the use of N-acetylcysteine or sodium bicarbonate; however, further definitive evidence is pending (68,69). Their effectiveness in already fluid-resuscitated ICU patients, however, remains unknown.
aKi in association with Mechanical Ventilation
Most critically ill patients require mechanical ventilation (MV), either for disease-specific indications such as acute respiratory distress syndrome (ARDS) or simply for routine postoperative care. The application of positive pressure MV, particularly with positive end-expiratory pressure (PEEP), can have important physiologic effects on kidney function. Experimental and clini-cal studies have clearly established an association between MV and PEEP and alterations in kidney function. This can occur through several mechanisms, including alterations in cardio-vascular function, alterations in neurohormonal activation, abnormalities in gas exchange, and alterations in systemic inflammatory mediators (70,71).
The positive pressure applied during MV acts to increase intrathoracic, intrapleural, and intra-abdominal pressures, both during inspiration and for the duration of the respira-tory cycle. This increase in intrathoracic pressure, moni-tored clinically by changes in mean airway pressure, can act to reduce intrathoracic blood volume, decrease transmural pressure, reduce right ventricular preload, increase right ven-tricular afterload, exert alterations to pulmonary vascular resistance and volume, and contribute to changes in left ven-tricular filling and geometry. The result of these effects may be a decrease in cardiac output and renal perfusion. Similarly, raised intrathoracic pressure, by altering transmural pressures and reducing cardiac output, can act to unload intrathoracic baroreceptors. This initiates a cascade of compensatory neu-rohormonal events characterized by increased systemic and renal sympathetic nervous activity, increased activation of the renin–angiotensin–aldosterone system, increased secretion of vasopressin, and a reduction in release of atrial natriuretic peptide. These culminate in altered renal perfusion and kidney excretory function. Renal function may not be impaired per se with MV, but rather, may appropriately respond to stimuli by reducing osmolar, sodium, and water clearance. In addi-tion, acute hypoxemia and/or hypercapnia, both commonly encountered in patients with ARDS, can act to alter systemic hemodynamics and increase systemic inflammation, both of which may exert negative effects on renal perfusion and func-tion. Particular strategies of MV, specifically in ARDS, are now recognized to contribute to or provoke ventilator-induced lung injury (VILI). Evidence now suggests that the pathophysiology of VILI is multifactorial and results from the combined effects of volutrauma (excessive tidal or end-expiratory volumes), barotrauma (excessive end-inspiratory peak and plateau pressures), atelectatic trauma (cyclical opening and closing of alveolar units), and biotrauma (local release of inflammatory
mediators from injured lung) (72). Such injurious MV can ini-tiate a cascade of events that increases systemic inflammation and adversely impact kidney function (73).
aKi in association with intra-abdominal Hypertension/abdominal compartment syndrome
Intra-abdominal hypertension (IAH) and abdominal com-partment syndrome (ACS) can worsen kidney function and precipitate AKI. Mechanical compression on abdominal and thoracic vessels results in diminished venous return, conges-tion, increased renal venous pressure, which leads to renal interstitial edema. This coupled with renal arterial vasocon-striction due to compensatory renin–angiotensin–aldosterone system activation contributes to impaired perfusion pressure across the renal circulation. Patients with IAH progressing to ACS commonly present with marked abdominal distension, measured IAP above 15 mmHg, and increasing serum creati-nine and oliguria. ACS is commonly associated with major trauma or large burn injuries, complex intra-abdominal sur-geries, pancreatitis or ruptured aneurysms, and in patients receiving large volume resuscitation.
Identification of IAH/ACS requires a high index of suspi-cion among susceptible patients, and should include the routine measurement of bladder pressures. Management is generally supportive and includes optimization of sedation, neuromus-cular blockade, patient repositioning, nasogastric and rectal decompression, draining fluid collections and optimizing fluid balance through minimizing nonessential fluid, administration of diuretics or if necessary, initiation of RRT. In those with refractory ACS and sustained IAH above 20 mmHg, surgical decompression should be considered (74).
GeneRAL MAnAGeMent
The most common clinical picture seen in the ICU is that of a patient who has sustained or is experiencing a major systemic insult such as trauma, sepsis, myocardial infarction, severe hem-orrhage, cardiogenic shock, or major surgery. When the patient arrives in the ICU, resuscitation is typically well underway, or surgery may have just been completed. Despite such efforts, the patient is already anuric or profoundly oliguric, and the serum creatinine is rising, and a metabolic acidosis is developing; serum potassium and phosphate levels may be rapidly rising as well. In these critically ill patients with AKI, multiple organ dysfunction—with the need for MV and vasoactive drugs—is common. Fluid resuscitation is typically undertaken in the ICU with the guidance of invasive hemodynamic monitoring. Vasoactive drugs are often used to restore mean arterial pres-sure (MAP) to acceptable levels, typically greater than 65 to 70 mmHg (see Figure 132.3). The patient may improve over time, and urine output may return with or without the assis-tance of diuretic agents (Fig. 132.4). If urine output does not return, however, RRT needs to be considered. If the cause of AKI has been removed, and the patient has become physiologi-cally stable, slow recovery occurs within 4 to 5 days to as long as 3 or 4 weeks. In some cases, urine output can be above nor-mal for several days. If the cause of AKI has not been adequately remedied, the patient remains gravely ill, the kidneys do not recover, and death from multiorgan failure may occur.
LWBK1580-CH132_p1651-1665.indd 1659 01/08/17 6:58 PM

1660 SECTion 14 rEnal disEasE and dysFunction
fluid resuscitation
Intravascular volume must be maintained or rapidly restored, and this is often best done using invasive hemodynamic moni-toring such as with central venous catheter, arterial cannula, and pulmonary artery catheter or pulse contour cardiac out-put catheters. Oxygenation must be maintained. An adequate hemoglobin concentration, usually at least more than 7.0 g/dL must be maintained or immediately restored. Once intravas-cular volume has been restored, some patients remain hypo-tensive with MAP less than 70 mmHg. In these patients, autoregulation of RBF may be lost. Restoration of MAP to near-normal levels may increase GFR (75–77). Such elevations in MAP, however, require the addition of vasopressor drugs (75–77). In patients with pre-existing hypertension or reno-vascular disease, a MAP of 75 to 80 may still be inadequate. Experimental evidence suggests that vasopressor support in hypotensive sepsis increases renal blood flow (Fig. 132.5) and renal medullary blood flow (Fig. 132.6). The renal protective role of additional fluid therapy in a patient with a normal or increased cardiac output and blood pressure is questionable. Despite these resuscitation measures, renal failure may still develop if cardiac output is inadequate. This may require a variety of interventions from the use of inotropic drugs to the application of ventricular assist devices.
fluid therapy
Fluid therapy is the cornerstone of resuscitation of the criti-cally ill patient, and is the primary strategy for preservation of kidney function in the setting of increases in serum creati-nine and/or urea, and oliguria. However, evolving evidence
has suggested there may be negative consequences to overly aggressive fluid therapy for both renal and nonrenal organ function. A large multicentre study found no significant differ-ence in the incidence of AKI when comparing fluid resuscita-tion with crystalloid to albumin in critically ill patients (78). However, some synthetic colloid therapies, such as hydroxy-ethyl starches (HES), are associated with higher risk of AKI and need for RRT in critically ill patients (79,80). Although the exact mechanism(s) remain uncertain, HES solutions may influence intrarenal hemodynamics or glomerular filtration through alterations in vascular oncotic pressure. Recent data have also focused on the composition of crystalloid solutions and the risk of adverse events. The preferential use of balanced crystalloid solutions such as Ringer’s lactate and plasmalyte have been shown to reduce the risk of iatrogenic metabolic acidosis, and AKI, including severe AKI requiring RRT (81).
In critically ill patients, once apparent optimization of hemo-dynamics and intravascular volume status has been achieved, there is little evidence to support continued aggressive fluid resuscitation to improve kidney function. Rather, fluid over-load in AKI is associated with less favorable outcomes, includ-ing higher utilization of RRT, higher mortality, and reduced likelihood of renal recovery (82,83). Additionally, there is evidence to suggest that such continued fluid administration and a positive cumulative balance can contribute to notable deteriorations in nonrenal organ function, in particular, lung function (84,85). The ARDS Clinical Trials Network com-pleted the largest randomized trial assessing fluid therapy in patients with acute lung injury (ALI) (86). This trial compared restrictive and liberal strategies for fluid management in 1,000 critically ill patients, mostly with pneumonia or sepsis, and evidence of with ALI. At 72 hours, those receiving a restrictive
200p < 0.0001
* Norepinephrine added
Norepinephrine
Dopamine
Urin
e O
utpu
t (m
l/hr)
180
160
140
120
100
80
60
40
20
0BSL 1 hour 6 hours
FiGURe 132.4 diagram showing the effect of norepineph-rine on urine output compared to high-dose dopamine in patients in septic shock. urine output is more effectively restored with norepinephrine infusion when given alone as an alternative to high-dose dopamine or after high-dose dopamine has failed. bsl, baseline.
80
% C
hang
e in
RB
F
60
40
20
0
−20
−40 Bas
e lin
e
Sep
sis
Nor
ep in
eph
rine
−60
1
2
3
4
5
6
7
8 FiGURe 132.5 diagram showing the changes in renal blood flow (rbF) during experimental E. coli–induced septic shock in sheep. the addition of norepinephrine increased renal blood flow.
LWBK1580-CH132_p1651-1665.indd 1660 01/08/17 6:58 PM

CHAPTER 132 acute renal injury 1661
fluid strategy had a near neutral fluid balance, whereas those in the liberal strategy were positive above 5 L. While the study failed to show a difference in mortality between the strategies, a restrictive strategy improved lung function, increased in ven-tilator-free days, and reduced ICU length of stay. Moreover, those in the restrictive group had a trend toward a reduced utilization of RRT.
avoidance of nephrotoxins
In patients with established AKI, as well in those at increased risk, avoidance of nephrotoxins is a priority to prevent iatro-genic overt or worsening AKI and delay of renal recovery. In circumstances where there are no options other than to use a nephrotoxin, for example, with certain antimicrobials or cal-cineuron inhibitors, therapeutic drug monitoring and careful dose adjustment, in multidisciplinary consultation with phar-macy, should be undertaken. The perceived benefits and risks of receiving contrast media for diagnostic imaging should be carefully evaluated; and where applicable, delay or choosing alternative imaging modalities should be undertaking in those at high risk where possible.
renal Protective Drugs
Following acute resuscitation, hemodynamic optimization, and attention to nephrotoxin use, it is unclear whether the use of additional pharmacologic measures is of further benefit to the kidneys.
Renal Dose or low-Dose Dopamine
Evidence of the efficacy or safety of its administration in critically ill patients is lacking. However, this agent is a tubular diuretic and occasionally increases urine output. This may be incorrectly interpreted as an increase in GFR. Furthermore, a large phase III trial in critically ill patients showed low-dose dopamine to be as effective as placebo in the prevention of AKI (87).
Mannitol
A biologic rationale exists for its use, as is the case for dopa-mine. However, no controlled human data exist to support its clinical use. The effect of mannitol as a renal protective agent remains questionable.
loop Diuretics
These agents may protect the loop of Henle from ischemia by decreasing its transport-related workload. Animal data are
encouraging, as are ex vivo experiments. There are no double-blind randomized controlled studies of suitable size to prove that these agents reduce the incidence of AKI. However, there are some studies, which support the view that loop diuret-ics may decrease the need for RRT in patients developing AKI (88). They appear to achieve this by inducing polyuria, which allows for easier control of volume overload, acidosis, and hyperkalemia, three major triggers for RRT in the ICU. Because avoiding RRT simplifies treatment and reduces cost of care, loop diuretics are commonly used in patients with AKI, especially in the form of continuous infusion.
Other agents
Other agents such as theophylline, urodilatin, and anarit-ide (a synthetic atrial natriuretic factor) have also been proposed. Studies so far, however, have been either been experimental, too small, or have shown no beneficial effect. In a randomized double-blind, placebo-controlled trial, fenoldopam has been shown to attenuate the deterioration in serum creatinine typically seen in septic patients (89). Studies of fenoldopam in other situations, however, have failed to show a benefit (90). Thus, its role in AKI remains uncertain. Similarly, in a single-center study, rhANF has been shown to attenuate renal injury in higher-risk patients having cardiac surgery (91), but a large multicenter study of AKI failed to show a benefit (92). Many more investigations are urgently needed in this field.
MAnAGeMent oF eStABLiSheD AKi
The principles of management of established AKI should always include the following:• Confirmation of probable cause• Elimination of potential contributors• Institution of disease-specific therapy if applicable• Prevention and management of AKI-related complications
with maintenance of physiologic homeostasis while allow-ing recovery to occurComplications such as encephalopathy, pericarditis, myop-
athy, neuropathy, electrolyte disturbances, or other major elec-trolyte, fluid, or metabolic derangements should never occur in a modern ICU. They can be prevented by several measures, which vary in complexity from fluid restriction to the initia-tion of RRT.
1
2
3
4
5
6
7
8
300
% c
hang
e in
med
ulla
ry fl
ow
250
200
150
100
50
0
−50
Baseli
ne
Norep
ineph
rine
Sepsis
−100FiGURe 132.6 diagram showing the changes in medullary renal blood flow during experimental septic shock in sheep induced by E. coli administration. the addition of norepi-nephrine increased medullary blood flow.
LWBK1580-CH132_p1651-1665.indd 1661 01/08/17 6:58 PM

1662 SECTion 14 rEnal disEasE and dysFunction
Nutritional support should be started early and contain adequate calories, around 30 to 35 kcal/kg/d, as a mixture of carbohydrates and lipids. Sufficient protein of at least 1 to 2 g/kg/d must be administered. There is no evidence that spe-cific renal nutritional solutions are useful. Vitamins and trace elements should be administered at least according to their recommended daily allowance. The role of newer immunonu-tritional solution remains controversial. The enteral route is preferred to the use of parenteral nutrition.
Hyperkalemia—a serum potassium level of greater than 6 mmol/L—must be promptly treated either with insulin and dextrose administration, the infusion of bicarbonate if acido-sis is present, the administration of nebulized salbutamol, or all of the above combined. If the “true” serum potassium is more than 7 mmol/L, or if electrocardiographic signs of hyper-kalemia appear, calcium gluconate—10 mL of 10% solution administered IV—should also be used. The above measures are temporizing actions while RRT is being arranged. The presence of hyperkalemia is a major life-threatening indication for the immediate institution of RRT.
Metabolic acidosis is almost always present but rarely requires treatment per se. Anemia requires correction to maintain a hemoglobin of at least 70 g/L. More aggressive transfusion needs individual patient assessment (93). Drug therapy must be adjusted to take into account the effect of the decreased clearances associated with loss of kidney function. Stress ulcer prophylaxis is advisable and should be based on H2-receptor antagonists or proton pump inhibitors in selected cases. Assiduous attention should be paid to the prevention of infection.
Fluid overload can be prevented by the avoidance of administration of nonessential fluids and the judicious use of loop diuretics. However, if the patient is oliguric, the only way to avoid fluid overload is to institute RRT at an earlier stage. Marked azotemia, defined as a urea more than 40 mmol/L (BUN [blood urea nitrogen] of 112 mg/dL) or a creatinine level more than 400 µmol/L (4.5 mg/dL) is undesirable and should probably be treated with RRT unless recovery is immi-nent or already under way and a return toward normal values is expected within 24 to 48 hours.
In critically ill patients with life-threatening complications from AKI, referral for RRT should occur without delay. In general, relative few patients develop these severe complica-tions. Accordingly, the decision to start RRT is often more complex and occurs amid a number of factors such as conser-vative therapy to manage fluid accumulation is failing coupled with evidence of worsening electrolyte disorders, acidosis or azotemia. Whether the early initiation of RRT in the absence of these indications improves survival remains unproven (94); however, it is advisable to start RRT in anticipation of compli-cations rather need to urgently rescue patients. Indeed, recent data have shown these complications have an independent and attributable contribution to mortality to critically ill patients with AKI. The ideal modality to support critically ill patients with AKI remains unresolved. In general, in hemodynamically or physiologically unstable patients, patients should be pref-erentially treated initially with continuous renal replacement therapy (CRRT) rather than intermitted forms of hemodi-alysis (IHD) in an ICU setting. While no definitive evidence has shown a survival advantage with one particular modality, recent data support the greater likelihood of recovery of kid-ney function and dialysis independence among those initially
treated with CRRT (95). Evidence from two large multicenter randomized trials showed no added benefit higher intensity-dose RRT compared to lower intensity-dose RRT with fewer metabolic complications (96,97). For a more comprehensive evidence-based review of the principles of RRT in AKI, review the KDIGO Clinical Practice Guidelines for AKI (4).
FURtheR DiAGnoStiC inveStiGAtionS
An etiologic diagnosis of AKI must always be established. Although such diagnosis may be obvious on clinical grounds, in many patients it is best to consider all possibilities and exclude common treatable causes by simple investigations. One such investigation includes microscopic examination of the urinary sediment. Urinalysis is a simple and noninvasive test that yields important diagnostic information and patterns suggestive of specific syndromes. The finding of dysmorphic red blood cells (RBC) or RBC casts is virtually diagnostic of active glomerulonephritis or vasculitis. Heavy proteinuria sug-gests some form of glomerular disease. White blood cell casts can suggest either interstitial nephropathy or infection. Simi-larly, a normal urinalysis can provide important information and can suggest that AKI is more likely to be transient or due to an obstructive cause. Finally, examination of urine will pro-vide evidence of whether a urinary tract infection is present.
Several additional investigations may be necessary to estab-lish the diagnosis. Evidence of marked anemia in the absence of blood loss may suggest acute hemolysis, thrombotic micro-angiopathy, or paraproteinemia related to malignancy. In microangiopathic hemolytic anemia, a peripheral blood smear will typically show evidence of hemolysis with the presence of schistocytes; the additional measurement of lactic dehydroge-nase, haptoglobin, unconjugated bilirubin, and free hemoglo-bin are needed. If paraproteinemia due to multiple myeloma or lymphoma is suspected, serum and urine protein electro-phoresis and serum calcium should be measured. A history of recent cancer diagnosis or chemotherapy should prompt the measurement of uric acid for tumor lysis syndrome.
In patients with a possible mechanism for muscle injury, cre-atinine kinase and free myoglobin for possible rhabdomyolysis should be determined. If an elevated anion gap metabolic aci-dosis is present with suggestion of a toxic ingestion, ethylene glycol, methanol, and salicylates should be measured.
Systemic eosinophilia may be a clue suggesting systemic vasculitis, allergic interstitial nephritis, or atheroembolic dis-ease. The measurement of specific antibodies—antiglomeru-lar basement membrane (GBM), antineutrophil cytoplasmic antibodies (ANCA), antinuclear antibodies (ANA), anti-DNA, antismooth muscle, and so forth—or cryoglobulins are extremely useful screening tests to support the diagnosis of vasculitis or certain types of collagen vascular diseases or glomerulonephritis.
Imaging by renal ultrasonography is a rapid noninva-sive investigation principally designed to rule out evidence of obstruction, stones, cysts, masses, or overt renovascular dis-ease. A chest radiograph may be important both to assess for pulmonary complications of AKI and if a diagnosis of systemic vasculitis is considered. In the occasional patient, a percutane-ous renal biopsy becomes necessary to confirm the diagnosis,
LWBK1580-CH132_p1651-1665.indd 1662 01/08/17 6:58 PM

CHAPTER 132 acute renal injury 1663
determine the severity of renal injury, guide therapy, and evalu-ate prognosis and potential for recovery (98). A renal biopsy is indicated when a thorough noninvasive investigation has failed to yield the diagnosis, when transient and postrenal causes have been excluded, and prior to the administration of poten-tially toxic immunosuppressive therapy. A renal biopsy can be performed under ultrasound guidance with local anesthetic in critically ill patients undergoing MV without additional risks when compared to standard conditions.
PRoGnoSiS
AKI can independently influence both short- and long-term prognosis. In hospitalized patients, mortality is estimated at 20% among all those developing AKI; however, this rate is greatly influenced by the severity of renal injury. The prog-nosis is worse for critically ill patients and those where RRT becomes necessary. The in-hospital mortality for critically ill patients with AKI is estimated at 50% to 60% (yet can range between 30% and 80% depending on the case-mix) (18,19,99–102). It is frequently stated that patients die with AKI rather than of AKI. However, growing evidence suggests that better uremic control and more intensive artificial kidney support may improve survival by perhaps 30% (103–105). Such evidence supports a careful and proactive approach to the treatment of critically ill patients with AKI, which is based on the prevention of uncontrolled uremia, and fluid overload.
AKI is also associated with significant morbidity. AKI is associated with greater susceptibility to infection/sepsis, pro-longed duration and delayed weaning from MV, and longer or unanticipated stays in ICU and hospital. Perhaps more impor-tantly, AKI is a clear risk factor for development of CKD. In addition to CKD, recent data have also suggested survivors of AKI remain at increased long-term risk infection, major car-diovascular events, malignancy, and higher health services use (18,19,106).
Failure to recover function can have both individual patient and broader health care implications. Persistent CKD or need for long-term RRT can negatively influence the health status and quality of life of patients, and contribute to considerable annual health care expenditures. Recovery to independence from RRT occurs in an estimated 68% to 85% of critically ill patients by hospital discharge and generally peaks by 90 days (18,19). Studies have shown that older patients and those with pre-existing comorbid illnesses such as CKD or advanced car-diovascular disease are less likely to recover function whereas those with septic AKI may be more likely to recover function. Several other potentially modifiable factors have been linked with improved rates of recovery including timely initiation of RRT when indicated, initial use of continuous rather than intermittent RRT, early and adequate nutritional support. Whether adjuvant erythropoietin and routine use of loop diuretics can influence kidney prognosis and promote early recovery remain controversial.
In those who survive an episode of AKI, the long-term health status, including quality of life, functional status, and hospital discharge location, are also now considered important indicators of morbidity. These patients frequently describe limitations in daily activities, difficulties with mobil-ity, and high levels of sleep disturbance, fatigue, anxiety, and depression. However, quality of life is often described as being
generally good and perceived as acceptable, despite evidence of being considerably lower than that of the general popula-tion (107–110).
• Restoring MAP within the autoregulatory range for blood flow to the kidney—65 to 110 mmHg—is impor-tant in maintaining the GFR. Once the patient has been adequately fluid resuscitated, and the cardiac output is known to be adequate, MAP should be corrected within autoregulation with the use of norepinephrine.
• Low-dose dopamine has been extensively studied, meta-analyzed, and assessed for the prevention and treatment of AKI. Although it probably increases urine output through its tubular diuretic effect, it does not maintain or improve the GFR or improve outcome.
• In an adequately fluid-resuscitated patient as described above, if the cardiac output is adequate or high, and the MAP is adequate or normal, there is no “renal” benefit to be gained by giving additional intravenous fluids. Such fluids often precipitate extravascular com-plications and have no appreciably beneficial effect on GFR. In these circumstances, support with RRT should be considered.
Key Points
ACKnoWLeDGMentSDr. Bagshaw is supported by a Canada Research Chair in Critical Care Nephrology.
references 1. Bellomo R, Ronco C, Kellum JA, et al. Acute Dialysis Quality Initiative
with acute renal failure: definition, outcome measures, animal models, fluid therapy and information technology needs. The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8(4):R204–R212.
2. Uchino S, Bellomo R, Goldsmith D, et al. An assessment of the RIFLE criteria for acute renal failure in hospitalized patients. Crit Care Med. 2006;34:1913–7.
3. Hoste EA, Clermont G, Kersten A, et al. RIFLE criteria for acute kid-ney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Crit Care. 2006;10(3):R73.
4. KDIGO. KDIGO clinical practice guidelines on acute kidney injury. Kid-ney Int. 2012;2(1):8–12.
5. Pickering JW, Endre ZH. GFR shot by RIFLE: errors in staging acute kid-ney injury. Lancet. 2009;373(9672):1318–1319.
6. Doi K, Yuen PS, Eisner C, et al. Reduced production of creatinine lim-its its use as marker of kidney injury in sepsis. J Am Soc Nephrol. 2009;20(6):1217–1221.
7. Ralib A, Pickering JW, Shaw GM, Endre ZH. The urine output definition of acute kidney injury is too liberal. Crit Care. 2013;17(3):R112.
8. Prowle JR, Liu YL, Licari E, et al. Oliguria as predictive biomarker of acute kidney injury in critically ill patients. Crit Care. 2011;15(4):R172.
9. Macedo E, Malhotra R, Claure-Del Granado R, et al. Defining urine out-put criterion for acute kidney injury in critically ill patients. Nephrol Dial Transpl. 2011;26(2):509–515.
10. Mandelbaum T, Lee J, Scott DJ, et al. Empirical relationships among oli-guria, creatinine, mortality, and renal replacement therapy in the critically ill. Intensive Care Med. 2013;39(3):414–419.
11. Macedo E, Malhotra R, Bouchard J, et al. Oliguria is an early predic-tor of higher mortality in critically ill patients. Kidney Int. 2011;80(7): 760–767.
12. Bagshaw SM, Langenberg C, Bellomo R. Urinary biochemistry and microscopy in septic acute renal failure: a systematic review. Am J Kidney Dis. 2006;48(5):695–705.
LWBK1580-CH132_p1651-1665.indd 1663 01/08/17 6:58 PM

1664 SECTion 14 rEnal disEasE and dysFunction
13. Langenberg C, Wan L, Bagshaw SM, et al. Urinary biochemistry in experimental septic acute renal failure. Nephrol Dial Transplant. 2006;21(12):3389–3397.
14. Kanbay M, Kasapoglu B, Perazella MA. Acute tubular necrosis and pre-renal acute kidney injury: utility of urine microscopy in their evaluation: a systematic review. Int Urol Nephrol. 2010;42(2):425–433.
15. Carvounis CP, Nisar S, Guro-Razuman S. Significance of the fractional excretion of urea in the differential diagnosis of acute renal failure. Kidney Int. 2002;62(6):2223–2229.
16. Perazella MA, Coca SG, Hall IE, et al. Urine microscopy is associated with severity and worsening of acute kidney injury in hospitalized patients. Clin J Am Soc Nephrol. 2010;5(3):402–408.
17. Susantitaphong P, Cruz DN, Cerda J, et al. World incidence of AKI: a meta-analysis. Clin J Am Soc Nephrol. 2013;8(9):1482–1493.
18. Bagshaw SM, Laupland KB, Doig CJ, et al. Prognosis for long-term sur-vival and renal recovery in critically ill patients with severe acute renal failure: a population-based study. Crit Care. 2005;9(6):R700–R709.
19. Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294(7):813–818.
20. de Mendonca A, Vincent JL, Suter PM, et al. Acute renal failure in the ICU: risk factors and outcome evaluated by the SOFA score. Intensive Care Med. 2000;26(7):915–921.
21. McCarthy JT. Prognosis of patients with acute renal failure in the inten-sive-care unit: a tale of two eras. Mayo Clin Proc. 1996;71(2):117–126.
22. Tran DD, Cuesta MA, Oe PL. Acute renal failure in patients with severe civilian trauma. Nephrol Dial Transpl. 1994;9(Suppl 4):121–125.
23. Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39(5):930–936.
24. Feest T, Round A, Hamad S. Incidence of severe acute renal failure in adults: results of a community based study. BMJ. 1993;306:481–483.
25. Kheterpal S, Tremper KK, Heung M, et al. Development and validation of an acute kidney injury risk index for patients undergoing general surgery: results from a national data set. Anesthesiology. 2009;110(3):505–515.
26. Goldstein SL, Kirkendall E, Nguyen H, et al. Electronic health record identification of nephrotoxin exposure and associated acute kidney injury. Pediatrics. 2013;132(3):e756–e767.
27. Selby NM, Crowley L, Fluck RJ, et al. Use of electronic results report-ing to diagnose and monitor AKI in hospitalized patients. Clin J Am Soc Nephrol. 2012;7(4):533–540.
28. Silvester W, Bellomo R, Cole L. Epidemiology, management, and outcome of severe acute renal failure of critical illness in Australia. Critical Care Med. 2001;29(10):1910–1915.
29. Langenberg C, Bellomo R, May C, et al. Renal blood flow in sepsis. Crit Care. 2005;9(4):R363–R374.
30. Langenberg C, Bellomo R, May CN, et al. Renal vascular resistance in sepsis. Nephron Physiol. 2006;104(1):p1–p11.
31. Langenberg C, Wan L, Egi M, et al. Renal blood flow in experimental septic acute renal failure. Kidney Int. 2006;69(11):1996–2002.
32. Gomez H, Ince C, De Backer D, et al. A unified theory of sepsis-induced acute kidney injury: inflammation, microcirculatory dysfunction, bioenergetics, and the tubular cell adaptation to injury. Shock. 2014;41(1): 3–11.
33. Lucas CE, Rector FE, Werner M, Rosenberg IK. Altered renal homeostasis with acute sepsis: clinical significance. Arch Surg. 1973;106(4):444–449.
34. Rector F, Goyal S, Rosenberg IK, Lucas CE. Renal hyperemia in associated with clinical sepsis. Surg Forum. 1972;23(0):51–53.
35. Brenner M, Schaer GL, Mallory DL, et al. Detection of renal blood flow abnormalities in septic and critically ill patients using a newly designed indwelling thermodilution renal vein catheter. Chest. 1990;98(1): 170–179.
36. Di Giantomasso D, Morimatsu H, May CN, Bellomo R. Intrarenal blood flow distribution in hyperdynamic septic shock: effect of norepinephrine. Crit Care Med. 2003;31(10):2509–2513.
37. Hotchkiss RS, Swanson PE, Freeman BD, et al. Apoptotic cell death in patients with sepsis, shock, and multiple organ dysfunction. Crit Care Med. 1999;27(7):1230–1251.
38. Wan L, Bellomo R, Di Giantomasso D, Ronco C. The pathogenesis of septic acute renal failure. Curr Opin Crit Care. 2003;9(6):496–502.
39. Jo SK, Cha DR, Cho WY, et al. Inflammatory cytokines and lipopolysac-charide induce Fas-mediated apoptosis in renal tubular cells. Nephron. 2002;91(3):406–415.
40. Messmer UK, Briner VA, Pfeilschifter J. Tumor necrosis factor-alpha and lipopolysaccharide induce apoptotic cell death in bovine glomerular endo-thelial cells. Kidney Int. 1999;55(6):2322–2337.
41. Bonegio R, Lieberthal W. Role of apoptosis in the pathogenesis of acute renal failure. Curr Opin Nephrol Hypertens. 2002;11(3):301–308.
42. Imai Y, Parodo J, Kajikawa O, et al. Injurious mechanical ventilation and end-organ epithelial cell apoptosis and organ dysfunction in an experimen-tal model of acute respiratory distress syndrome. JAMA. 2003;289(16): 2104–2112.
43. Bastin AJ, Ostermann M, Slack AJ, et al. Acute kidney injury after cardiac surgery according to Risk/Injury/Failure/Loss/End-stage, Acute Kidney Injury Network, and Kidney Disease: Improving Global Outcomes clas-sifications. J Crit Care. 2013;28(4):389–396.
44. Gueler F, Rong S, Park JK, et al. Postischemic acute renal failure is reduced by short-term statin treatment in a rat model. J Am Soc Nephrol. 2002;13(9):2288–2298.
45. Noiri E, Nakao A, Uchida K, et al. Oxidative and nitrosative stress in acute renal ischemia. Am J Physiol Renal Physiol. 2001;281(5):F948–F957.
46. Starkopf J, Zilmer K, Vihalemm T, et al. Time course of oxidative stress during open-heart surgery. Scand J Thorac Cardiovasc Surg. 1995;29 (4):181–186.
47. Ishizuka S, Nagashima Y, Numata M, et al. Regulation and immuno-histochemical analysis of stress protein heme oxygenase-1 in rat kidney with myoglobinuric acute renal failure. Biochem Biophys Res Commun. 1997;240(1):93–98.
48. Gines P, Guevara M, Arroyo V, Rodes J. Hepatorenal syndrome. Lancet. 2003;362(9398):1819–1827.
49. Nadim MK, Kellum JA, Davenport A, et al. Hepatorenal syndrome: the 8th International Consensus Conference of the Acute Dialysis Quality Ini-tiative (ADQI) Group. Crit Care. 2012;16(1):R23.
50. Arroyo V, Guevara M, Gines P. Hepatorenal syndrome in cirrhosis: patho-genesis and treatment. Gastroenterology. 2002;122(6):1658–1676.
51. Sort P, Navasa M, Arroyo V, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bac-terial peritonitis. N Engl J Med. 1999;341(6):403–409.
52. Guevara M, Gines P, Fernandez-Esparrach G, et al. Reversibility of hepa-torenal syndrome by prolonged administration of ornipressin and plasma volume expansion. Hepatology. 1998;27(1):35–41.
53. Fabrizi F, Dixit V, Martin P. Meta-analysis: terlipressin therapy for the hepatorenal syndrome. Aliment Pharmacol Ther. 2006;24(6):935–944.
54. Guevara M, Gines P, Bandi JC, et al. Transjugular intrahepatic portosys-temic shunt in hepatorenal syndrome: effects on renal function and vaso-active systems. Hepatology. 1998;28(2):416–422.
55. Brensing KA, Textor J, Perz J, et al. Long term outcome after transjugular intrahepatic portosystemic stent-shunt in non-transplant cirrhotics with hepatorenal syndrome: a phase II study. Gut. 2000;47(2):288–295.
56. Holt SG, Moore KP. Pathogenesis and treatment of renal dysfunction in rhabdomyolysis. Intensive Care Med. 2001;27(5):803–811.
57. Heyman SN, Brezis M, Reubinoff CA, et al. Acute renal failure with selec-tive medullary injury in the rat. J Clin Invest. 1988;82(2):401–412.
58. Bonventre JV. Mechanisms of ischemic acute renal failure. Kidney Int. 1993;43(5):1160–1178.
59. di Mari JF, Davis R, Safirstein RL. MAPK activation determines renal epi-thelial cell survival during oxidative injury. Am J Physiol. 1999;277(2 Pt 2): F195–F203.
60. Portilla D, Mandel LJ, Bar-Sagi D, Millington DS. Anoxia induces phos-pholipase A2 activation in rabbit renal proximal tubules. Am J Physiol. 1992;262(3 Pt 2):F354–F360.
61. Bennett WM, Luft F, Porter GA. Pathogenesis of renal failure due to ami-noglycosides and contrast media used in roentgenography. Am J Med. 1980;69(5):767–774.
62. Cunha MA, Schor N. Effects of gentamicin, lipopolysaccharide, and con-trast media on immortalized proximal tubular cells. Renal Failure. 2002;24 (6):687–690.
63. Bagshaw SM, Culleton BF. Contrast-induced nephropathy: epidemiology and prevention. Minerva Cardioangiol. 2006;54(1):109–129.
64. Aspelin P, Aubry P, Fransson SG, et al. Nephrotoxic effects in high-risk patients undergoing angiography. N Engl J Med. 2003;348(6):491–499.
65. Merten GJ, Burgess WP, Gray LV, et al. Prevention of contrast-induced nephropathy with sodium bicarbonate: a randomized controlled trial. JAMA. 2004;291(19):2328–2334.
66. Mueller C, Seidensticker P, Buettner HJ, et al. Incidence of contrast nephropathy in patients receiving comprehensive intravenous and oral hydration. Swiss Med Wkly. 2005;135(19–20):286–290.
67. Stevens MA, McCullough PA, Tobin KJ, et al. A prospective randomized trial of prevention measures in patients at high risk for contrast nephropa-thy: results of the P.R.I.N.C.E. Study. Prevention of Radiocontrast Induced Nephropathy Clinical Evaluation. J Am Coll Cardiol. 1999;33(2):403–411.
68. Bagshaw SM, Ghali WA. Acetylcysteine for prevention of contrast-induced nephropathy after intravascular angiography: a systematic review and meta-analysis. BMC Med. 2004;2:38.
LWBK1580-CH132_p1651-1665.indd 1664 01/08/17 6:58 PM

CHAPTER 132 acute renal injury 1665
69. Tepel M, van der Giet M, Schwarzfeld C, et al. Prevention of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. N Engl J Med. 2000;343(3):180–184.
70. Kuiper JW, Groeneveld AB, Slutsky AS, Plotz FB. Mechanical ventilation and acute renal failure. Crit Care Med. 2005;33(6):1408–1415.
71. Pannu N, Mehta RL. Mechanical ventilation and renal function: an area for concern? Am J Kidney Dis. 2002;39(3):616–624.
72. Ricard JD, Dreyfuss D, Saumon G. Ventilator-induced lung injury. Curr Opin Crit Care. 2002;8(1):12–20.
73. Ranieri VM, Suter PM, Tortorella C, et al. Effect of mechanical ventila-tion on inflammatory mediators in patients with acute respiratory distress syndrome: a randomized controlled trial. JAMA. 1999;282(1):54–61.
74. Mohmand H, Goldfarb S. Renal dysfunction associated with intra-abdom-inal hypertension and the abdominal compartment syndrome. J Am Soc Nephrol. 2011;22(4):615–621.
75. Albanese J, Leone M, Garnier F, et al. Renal effects of norepinephrine in septic and nonseptic patients. Chest. 2004;126(2):534–539.
76. Bellomo R, Kellum JA, Wisniewski SR, Pinsky MR. Effects of norepineph-rine on the renal vasculature in normal and endotoxemic dogs. Am J Resp Crit Care Med. 1999;159(4 Pt 1):1186–1192.
77. Bourgoin A, Leone M, Delmas A, et al. Increasing mean arterial pressure in patients with septic shock: effects on oxygen variables and renal func-tion. Crit Care Med. 2005;33(4):780–786.
78. Finfer S, Bellomo R, Boyce N, et al. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med. 2004;350(22):2247–2256.
79. Myburgh JA, Finfer S, Bellomo R, et al. Hydroxyethyl starch or saline for fluid resuscitation in intensive care. N Engl J Med. 2012;367(20): 1901–1911.
80. Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med. 2012;367(2):124–134.
81. Chowdhury AH, Cox EF, Francis ST, Lobo DN. A randomized, controlled, double-blind crossover study on the effects of 2-L infusions of 0.9% saline and plasma-lyte(R) 148 on renal blood flow velocity and renal cortical tissue perfusion in healthy volunteers. Ann Surg. 2012;256(1):18–24.
82. Payen D, de Pont AC, Sakr Y, et al. A positive fluid balance is associ-ated with a worse outcome in patients with acute renal failure. Crit Care. 2008;12(3):R74.
83. Grams ME, Estrella MM, Coresh J, et al. Fluid balance, diuretic use, and mortality in acute kidney injury. Clin J Am Soc Nephrol. 2011;6(5):966–973.
84. Sakr Y, Vincent JL, Reinhart K, et al. High tidal volume and positive fluid balance are associated with worse outcome in acute lung injury. Chest. 2005;128(5):3098–3108.
85. Simmons RS, Berdine GG, Seidenfeld JJ, et al. Fluid balance and the adult respiratory distress syndrome. Am Rev Resp Dis. 1987;135(4): 924–929.
86. Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354(24): 2564–2575.
87. Bellomo R, Chapman M, Finfer S, et al. Low-dose dopamine in patients with early renal dysfunction: a placebo-controlled randomised trial. Aus-tralian and New Zealand Intensive Care Society (ANZICS) Clinical Trials Group. Lancet. 2000;356(9248):2139–2143.
88. Shilliday IR, Quinn KJ, Allison ME. Loop diuretics in the management of acute renal failure: a prospective, double-blind, placebo-controlled, ran-domized study. Nephrol Dial Transpl. 1997;12(12):2592–2596.
89. Morelli A, Ricci Z, Bellomo R, et al. Prophylactic fenoldopam for renal protection in sepsis: a randomized, double-blind, placebo-controlled pilot trial. Crit Care Med. 2005;33(11):2451–2456.
90. Bove T, Landoni G, Calabro MG, et al. Renoprotective action of fenoldo-pam in high-risk patients undergoing cardiac surgery: a prospective, double-blind, randomized clinical trial. Circulation. 2005;111(24):3230–3235.
91. Sward K, Valsson F, Odencrants P, et al. Recombinant human atrial natri-uretic peptide in ischemic acute renal failure: a randomized placebo- controlled trial. Crit Care Med. 2004;32(6):1310–1315.
92. Chertow GM, Lazarus JM, Paganini EP, et al. Predictors of mortality and the provision of dialysis in patients with acute tubular necrosis. The Auriculin Anaritide Acute Renal Failure Study Group. J Am Soc Nephrol. 1998;9(4):692–698.
93. Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Trans-fusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med. 1999;340(6):409–417.
94. Karvellas CJ, Farhat MR, Sajjad I, et al. A comparison of early versus late initiation of renal replacement therapy in critically ill patients with acute kidney injury: a systematic review and meta-analysis. Crit Care. 2011;15(1):R72.
95. Schneider AG, Bellomo R, Bagshaw SM, et al. Choice of renal replace-ment therapy modality and dialysis dependence after acute kidney injury: a systematic review and meta-analysis. Intensive Care Med. 2013; 39(6):987–997.
96. VA/NIH ATN Trial Investigators, Palevsky PM, Zhang JH, et al. Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med. 2008;359(1):7–20.
97. RENAL Trial Investigators, Bellomo R, Cass A, et al. Intensity of continu-ous renal-replacement therapy in critically ill patients. N Engl J Med. 2009; 361(17):1627–1638.
98. Korbet SM. Percutaneous renal biopsy. Semin Nephrol. 2002;22(3): 254–267.
99. Liano F, Junco E, Pascual J, et al. The spectrum of acute renal failure in the intensive care unit compared with that seen in other settings. The Madrid Acute Renal Failure Study Group. Kidney Int Suppl. 1998;66:S16–S24.
100. Mehta RL, Pascual MT, Soroko S, et al. Spectrum of acute renal failure in the intensive care unit: the PICARD experience. Kidney Int. 2004; 66(4):1613–1621.
101. Ympa YP, Sakr Y, Reinhart K, Vincent JL. Has mortality from acute renal failure decreased? A systematic review of the literature. Am J Med. 2005;118(8):827–832.
102. Nisula S, Kaukonen KM, Vaara ST, et al. Incidence, risk factors and 90-day mortality of patients with acute kidney injury in Finnish intensive care units: the FINNAKI study. Intensive Care Med. 2013;39(3):420–428.
103. Ronco C, Bellomo R, Homel P, et al. Effects of different doses in con-tinuous veno-venous haemofiltration on outcomes of acute renal failure: a prospective randomised trial. Lancet. 2000;356(9223):26–30.
104. Schiffl H, Lang SM, Fischer R. Daily hemodialysis and the outcome of acute renal failure. N Engl J Med. 2002;346(5):305–310.
105. Saudan P, Niederberger M, De Seigneux S, et al. Adding a dialysis dose to continuous hemofiltration increases survival in patients with acute renal failure. Kidney Int. 2006;70(7):1312–1317.
106. Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int. 2012;81(5):442–448.
107. Ahlstrom A, Tallgren M, Peltonen S, et al. Survival and quality of life of patients requiring acute renal replacement therapy. Intensive Care Med. 2005;31(9):1222–1228.
108. Korkeila M, Ruokonen E, Takala J. Costs of care, long-term prognosis and quality of life in patients requiring renal replacement therapy during intensive care. Intensive Care Med. 2000;26(12):1824–1831.
109. Maynard SE, Whittle J, Chelluri L, Arnold R. Quality of life and dialysis decisions in critically ill patients with acute renal failure. Intensive Care Med. 2003;29(9):1589–1593.
110. Morgera S, Kraft AK, Siebert G, et al. Long-term outcomes in acute renal failure patients treated with continuous renal replacement therapies. Am J Kidney Dis. 2002;40(2):275–279.
LWBK1580-CH132_p1651-1665.indd 1665 01/08/17 6:58 PM