Embed Size (px)
Citation preview
ACUTE PERIODONTAL ACUTE PERIODONTAL CONDITIONSCONDITIONS
Dr shabeel pnDr shabeel pn
OVERVIEWOVERVIEW
Abscesses of the PeriodontiumAbscesses of the Periodontium Necrotizing Periodontal DiseasesNecrotizing Periodontal Diseases Gingival Diseases of Viral Origin-Gingival Diseases of Viral Origin-
HerpesvirusHerpesvirus Recurrent Aphthous StomatitisRecurrent Aphthous Stomatitis Allergic ReactionsAllergic Reactions
Abscesses of the Abscesses of the PeriodontiumPeriodontium
Gingival AbscessGingival Abscess
Periodontal AbscessPeriodontal Abscess
Pericoronal AbscessPericoronal Abscess
Gingival AbscessGingival Abscess
A localized purulent infection that A localized purulent infection that involves the marginal gingiva or involves the marginal gingiva or interdental papillainterdental papilla
Gingival AbscessGingival Abscess
Gingival AbscessGingival Abscess EtiologyEtiology
– Acute inflammatory response to foreign Acute inflammatory response to foreign substances forced into the gingivasubstances forced into the gingiva
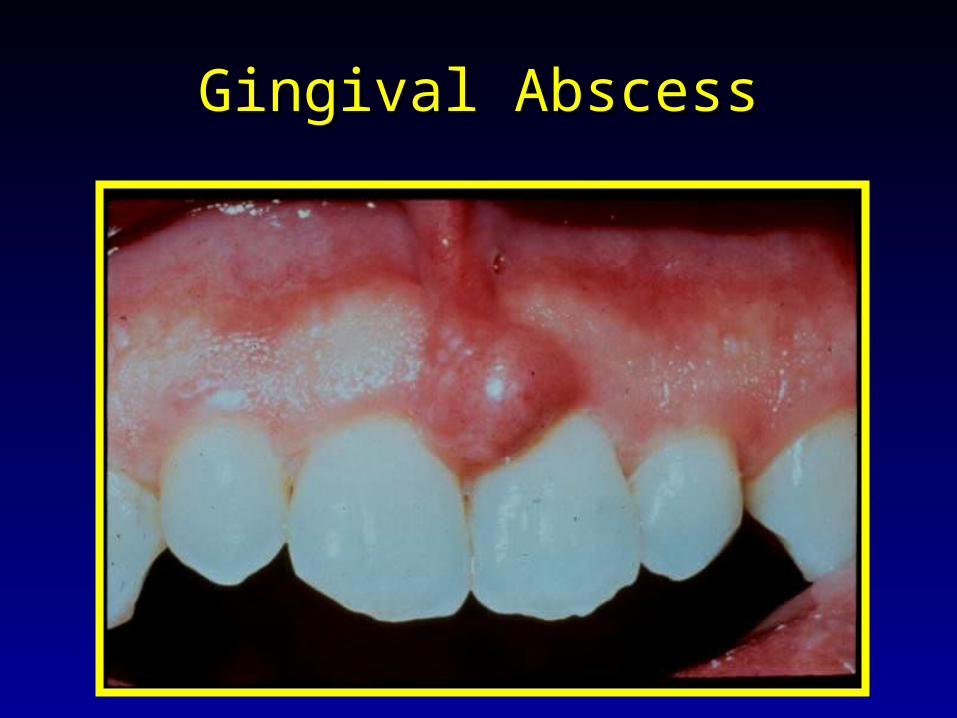
Clinical FeaturesClinical Features– Localized swelling of marginal gingiva or papillaLocalized swelling of marginal gingiva or papilla– A red, smooth, shiny surfaceA red, smooth, shiny surface– May be painful and appear pointedMay be painful and appear pointed– Purulent exudate may be presentPurulent exudate may be present– No previous periodontal diseaseNo previous periodontal disease
Gingival AbscessGingival Abscess
TreatmentTreatment– Elimination of foreign objectElimination of foreign object
– Drainage through sulcus with probe or light Drainage through sulcus with probe or light scalingscaling
– Follow-up after 24-48 hoursFollow-up after 24-48 hours
Periodontal AbscessPeriodontal Abscess
A localized purulent infection within the A localized purulent infection within the tissues adjacent to the periodontal tissues adjacent to the periodontal pocket that may lead to the destruction pocket that may lead to the destruction of periodontal ligament and alveolar of periodontal ligament and alveolar bonebone
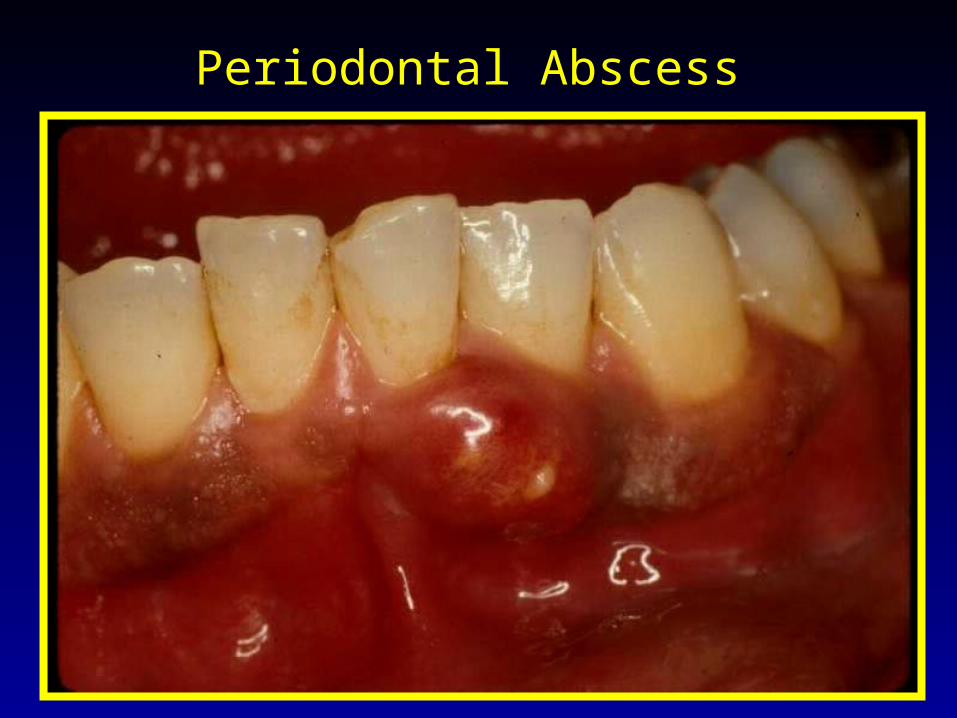
Periodontal Abscess
Periodontal AbscessPeriodontal Abscess
Usually pre-existing chronic periodontitis present!!!Usually pre-existing chronic periodontitis present!!! Factors associated with abscess developmentFactors associated with abscess development
– Occlusion of pocket orifice Occlusion of pocket orifice (by healing of marginal gingiva (by healing of marginal gingiva following supragingival scaling)following supragingival scaling)
– Furcation involvementFurcation involvement– Systemic antibiotic therapy Systemic antibiotic therapy (allowing overgrowth of resistant (allowing overgrowth of resistant
bacteria)bacteria)
– Diabetes MellitusDiabetes Mellitus
Periodontal AbscessPeriodontal Abscess
Clinical FeaturesClinical Features– Smooth, shiny swelling of the gingivaSmooth, shiny swelling of the gingiva– Painful, tender to palpationPainful, tender to palpation– Purulent exudatePurulent exudate– Increased probing depthIncreased probing depth– Mobile and/or percussion sensitiveMobile and/or percussion sensitive– Tooth usually vitalTooth usually vital
Periodontal Vs. Periapical Periodontal Vs. Periapical AbscessAbscess
Periodontal AbscessPeriodontal Abscess– Vital toothVital tooth– No cariesNo caries– PocketPocket– Lateral radiolucencyLateral radiolucency– MobilityMobility– Percussion sensitivity Percussion sensitivity
variablevariable– Sinus tract opens via Sinus tract opens via
keratinized gingivakeratinized gingiva
Periapical AbscessPeriapical Abscess– Non-vital toothNon-vital tooth– CariesCaries– No pocketNo pocket– Apical radiolucencyApical radiolucency– No or minimal mobilityNo or minimal mobility– Percussion sensitivityPercussion sensitivity– Sinus tract opens via Sinus tract opens via
alveolar mucosaalveolar mucosa
Periodontal AbscessPeriodontal Abscess
TreatmentTreatment– AnesthesiaAnesthesia– Establish drainageEstablish drainage
» Via sulcus is the preferred methodVia sulcus is the preferred method» Surgical access for debridementSurgical access for debridement» Incision and drainageIncision and drainage» ExtractionExtraction
Periodontal AbscessPeriodontal Abscess
Other Treatment Considerations:Other Treatment Considerations:
– Limited occlusal adjustmentLimited occlusal adjustment– AntimicrobialsAntimicrobials– Culture and sensitivityCulture and sensitivity
A periodontal evaluation following resolution of acute symptoms is essential!!!
Periodontal AbscessPeriodontal Abscess
Antibiotics Antibiotics (if indicated due to fever, malaise, (if indicated due to fever, malaise, lymphadenopathy, or inability to obtain drainage)lymphadenopathy, or inability to obtain drainage)
– Without penicillin allergyWithout penicillin allergy» PenicillinPenicillin
– With penicillin allergyWith penicillin allergy» AzithromycinAzithromycin» ClindamycinClindamycin
– Alter therapy if indicated by Alter therapy if indicated by culture/sensitivityculture/sensitivity
Pericoronal AbscessPericoronal Abscess
A localized purulent infection within the A localized purulent infection within the tissue surrounding the crown of a tissue surrounding the crown of a partially erupted toothpartially erupted tooth
Most common adjacent to mandibular Most common adjacent to mandibular third molars in young adults; usually third molars in young adults; usually caused by impaction of debris under the caused by impaction of debris under the soft tissue flapsoft tissue flap
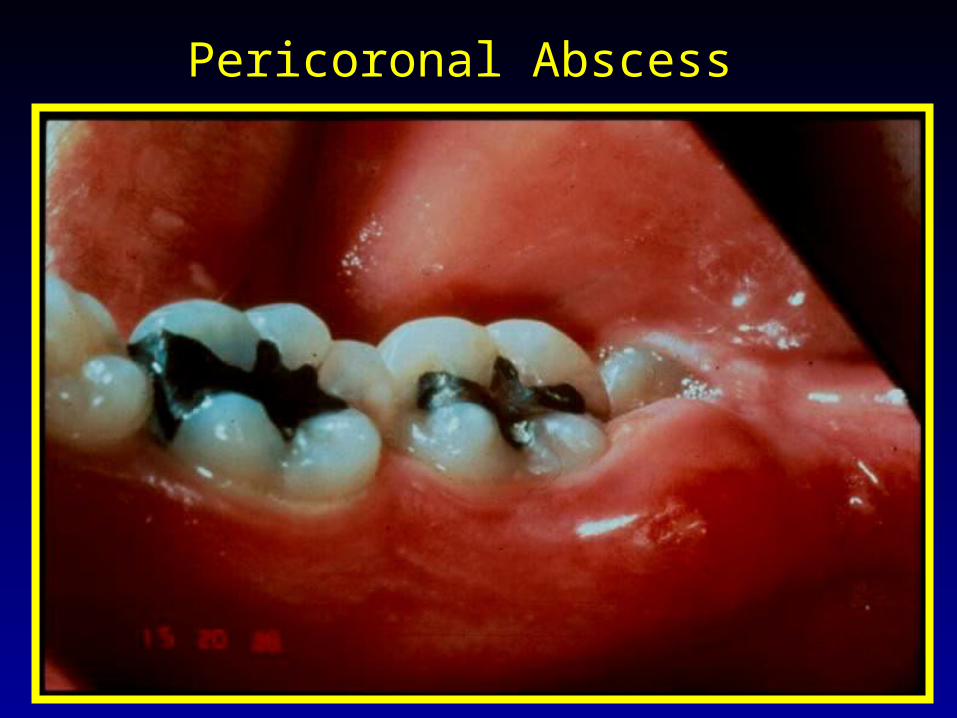
Pericoronal Abscess
Pericoronal AbscessPericoronal Abscess
Clinical FeaturesClinical Features– Operculum (soft tissue flap)Operculum (soft tissue flap)– Localized red, swollen tissueLocalized red, swollen tissue– Area painful to touchArea painful to touch– Tissue trauma from opposing tooth commonTissue trauma from opposing tooth common– Purulent exudate, trismus, Purulent exudate, trismus,
lymphadenopathy, fever, and malaise may lymphadenopathy, fever, and malaise may be presentbe present
Pericoronal AbscessPericoronal Abscess
Treatment OptionsTreatment Options– Debride/irrigate under pericoronal flapDebride/irrigate under pericoronal flap– Tissue recontouring Tissue recontouring (removing tissue flap)(removing tissue flap)
– Extraction of involved and/or opposing Extraction of involved and/or opposing toothtooth
– Antimicrobials Antimicrobials (local and/or systemic as (local and/or systemic as needed)needed)
– Culture and sensitivityCulture and sensitivity– Follow-upFollow-up
Necrotizing Periodontal Necrotizing Periodontal DiseasesDiseases
Necrotizing Ulcerative Gingivitis (NUG)Necrotizing Ulcerative Gingivitis (NUG)
Necrotizing Ulcerative Periodontitis Necrotizing Ulcerative Periodontitis (NUP)(NUP)
Necrotizing Ulcerative Necrotizing Ulcerative GingivitisGingivitis
An infection characterized by gingival An infection characterized by gingival necrosis presenting as “punched-out” necrosis presenting as “punched-out” papillae, with gingival bleeding and painpapillae, with gingival bleeding and pain

Necrotizing Ulcerative Gingivitis
Necrotizing Ulcerative Necrotizing Ulcerative GingivitisGingivitis
Historical terminologyHistorical terminology– Vincent’s diseaseVincent’s disease
– Trench mouthTrench mouth
– Acute necrotizing ulcerative gingivitis (ANUG)…Acute necrotizing ulcerative gingivitis (ANUG)…this terminology changed in 2000this terminology changed in 2000
Necrotizing Ulcerative Necrotizing Ulcerative GingivitisGingivitis
Necrosis limited to gingival tissuesNecrosis limited to gingival tissues Estimated prevalence 0.6% in general populationEstimated prevalence 0.6% in general population Young adults (mean age 23 years)Young adults (mean age 23 years) More common in CaucasiansMore common in Caucasians Bacterial floraBacterial flora
– Spirochetes (Spirochetes (Treponema Treponema sp.)sp.)– Prevotella intermediaPrevotella intermedia– Fusiform bacteriaFusiform bacteria
Necrotizing Ulcerative Necrotizing Ulcerative GingivitisGingivitis
Clinical FeaturesClinical Features– Gingival necrosis, especially tips of Gingival necrosis, especially tips of
papillaepapillae– Gingival bleedingGingival bleeding– PainPain– Fetid breathFetid breath– Pseudomembrane formationPseudomembrane formation
Necrotizing Ulcerative Necrotizing Ulcerative GingivitisGingivitis
Predisposing FactorsPredisposing Factors– Emotional stressEmotional stress– Poor oral hygienePoor oral hygiene– Cigarette smokingCigarette smoking– Poor nutritionPoor nutrition– ImmunosuppressionImmunosuppression
***Necrotizing Periodontal diseases are common in immunocompromised patients, especially those whoare HIV (+) or have AIDS
Necrotizing Ulcerative Necrotizing Ulcerative PeriodontitisPeriodontitis
An infection characterized by necrosis An infection characterized by necrosis of gingival tissues, periodontal ligament, of gingival tissues, periodontal ligament, and alveolar boneand alveolar bone
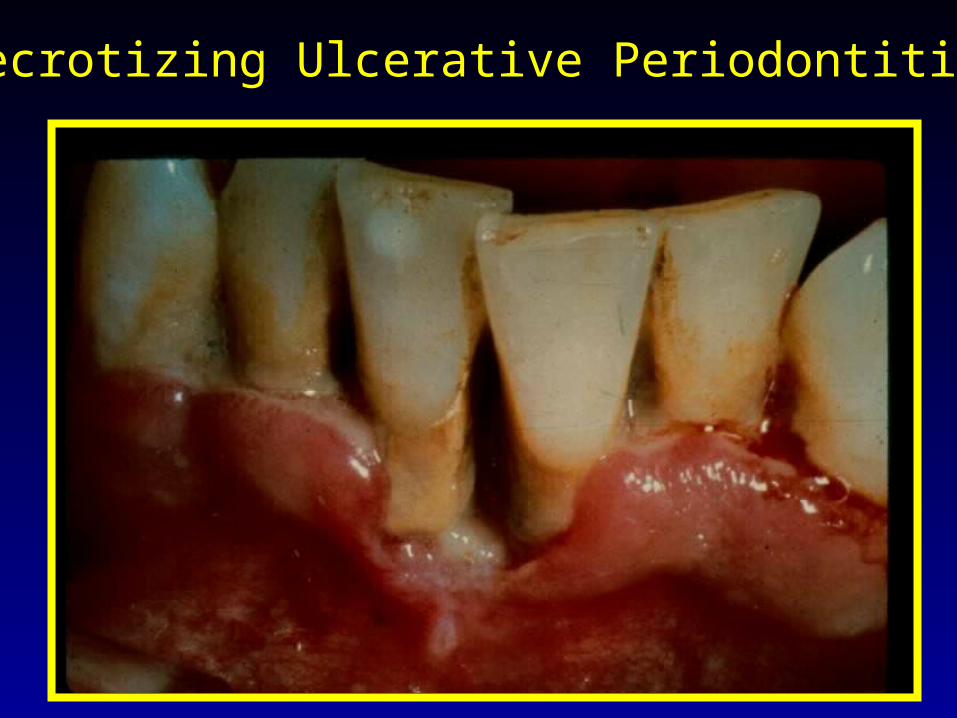
Necrotizing Ulcerative Periodontitis
Necrotizing Ulcerative Necrotizing Ulcerative PeriodontitisPeriodontitis
Clinical FeaturesClinical Features– Clinical appearance of NUGClinical appearance of NUG– Severe deep aching painSevere deep aching pain– Very rapid rate of bone destruction Very rapid rate of bone destruction – Deep pocket formation not evidentDeep pocket formation not evident
Necrotizing Periodontal Necrotizing Periodontal DiseasesDiseases
TreatmentTreatment– Local debridementLocal debridement– Oral hygiene instructionsOral hygiene instructions– Oral rinsesOral rinses– Pain controlPain control– AntibioticsAntibiotics– Modify predisposing factorsModify predisposing factors– Proper follow-upProper follow-up
Necrotizing Periodontal Necrotizing Periodontal DiseasesDiseases
TreatmentTreatment– Local debridementLocal debridement
» Most cases adequately treated by debridement Most cases adequately treated by debridement and sc/rpand sc/rp
» Anesthetics as neededAnesthetics as needed» Consider avoiding ultrasonic instrumentation due Consider avoiding ultrasonic instrumentation due
to risk of HIV transmissionto risk of HIV transmission
– Oral hygiene instructionsOral hygiene instructions
Necrotizing Periodontal Necrotizing Periodontal DiseasesDiseases
TreatmentTreatment– Oral rinses – (Oral rinses – (frequent, at least until pain subsides frequent, at least until pain subsides
allowing effective OH)allowing effective OH)» Chlorhexidine gluconate 0.12%; 1/2 oz 2 x dailyChlorhexidine gluconate 0.12%; 1/2 oz 2 x daily» Hydrogen peroxide/waterHydrogen peroxide/water» Povidone iodinePovidone iodine
– Pain controlPain control
Necrotizing Periodontal Necrotizing Periodontal DiseasesDiseases
TreatmentTreatment– Antibiotics (systemic or severe involvement)Antibiotics (systemic or severe involvement)
» MetronidazoleMetronidazole» Avoid broad spectrum antibiotics in AIDS patientsAvoid broad spectrum antibiotics in AIDS patients
– Modify predisposing factorsModify predisposing factors– Follow-upFollow-up
» Frequent until resolution of symptomsFrequent until resolution of symptoms» Comprehensive periodontal evaluation Comprehensive periodontal evaluation
following acute phase!!!!following acute phase!!!!
Gingival Diseases of Gingival Diseases of Viral OriginViral Origin
Acute manifestations of viral infections Acute manifestations of viral infections of the oral mucosa, characterized by of the oral mucosa, characterized by redness and multiple vesicles that easily redness and multiple vesicles that easily rupture to form painful ulcers affecting rupture to form painful ulcers affecting the gingiva.the gingiva.
Primary Herpetic Primary Herpetic GingivostomatitisGingivostomatitis
Classic initial infection of herpes simplex Classic initial infection of herpes simplex type 1type 1
Mainly in young children Mainly in young children
90% of primary oral infections are 90% of primary oral infections are asymptomaticasymptomatic

Primary Herpetic Gingivostomatitis
Primary Herpetic Primary Herpetic GingivostomatitisGingivostomatitis
Clinical FeaturesClinical Features– Painful severe gingivitis with ulcerations, Painful severe gingivitis with ulcerations,
edema, and stomatitisedema, and stomatitis– Vesicles rupture, coalesce and form ulcersVesicles rupture, coalesce and form ulcers– Fever and lymphadenopathy are classic Fever and lymphadenopathy are classic
featuresfeatures– Lesions usually resolve in 7-14 daysLesions usually resolve in 7-14 days
Primary Herpetic Primary Herpetic GingivostomatitisGingivostomatitis
TreatmentTreatment– Bed restBed rest– Fluids – forcedFluids – forced– NutritionNutrition– AntipyreticsAntipyretics
» Acetaminophen, not ASA due to risk of Reye’s Acetaminophen, not ASA due to risk of Reye’s SyndromeSyndrome
Primary Herpetic Primary Herpetic GingivostomatitisGingivostomatitis
TreatmentTreatment– Pain reliefPain relief
» Viscous lidocaineViscous lidocaine» Benadryl elixirBenadryl elixir» 50% Benadryl elixir/50% Maalox50% Benadryl elixir/50% Maalox
– Antiviral medicationsAntiviral medications» Immunocompromised patients Immunocompromised patients
Recurrent Oral HerpesRecurrent Oral Herpes
““Fever blisters” or “cold sores”Fever blisters” or “cold sores” Oral lesions usually herpes simplex virus Oral lesions usually herpes simplex virus
type 1type 1 Recurrent infections in 20-40% of those Recurrent infections in 20-40% of those
with primary infectionwith primary infection Herpes labialis commonHerpes labialis common Recurrent infections less severe than Recurrent infections less severe than
primaryprimary

Recurrent Oral Herpes
Recurrent Oral HerpesRecurrent Oral Herpes
Clinical FeaturesClinical Features– Prodromal syndromeProdromal syndrome– Lesions start as vesicles, rupture and leave Lesions start as vesicles, rupture and leave
ulcersulcers– A cluster of small painful ulcers on attached A cluster of small painful ulcers on attached
gingiva or lip is characteristicgingiva or lip is characteristic– Can cause post-operative pain following dental Can cause post-operative pain following dental
treatmenttreatment
Recurrent Oral HerpesRecurrent Oral Herpes
Virus reactivationVirus reactivation– FeverFever– Systemic infectionSystemic infection– Ultraviolet radiationUltraviolet radiation– StressStress– Immune system changesImmune system changes– TraumaTrauma– Unidentified causesUnidentified causes
Recurrent Oral HerpesRecurrent Oral Herpes
TreatmentTreatment– PalliativePalliative– Antiviral medicationsAntiviral medications
» Consider for treatment of immunocompromised Consider for treatment of immunocompromised patients, but not for periodic recurrence in patients, but not for periodic recurrence in healthy patientshealthy patients