-
Acute
HIV
infec-on
and
Prospects
for
Op-mizing
the
Immune
Response
with
Quan-ta-ve
Modeling
Eric
Rosenberg,
MD
Associate
Professor
of
Medicine
MassachuseDs
General
Hospital
Harvard
Medical
School
-
47
year
old
male
Present
to
MGH
ED
with
an
8
day
history
of
:
Fever
to
102.5
Headache
Photophobia
Myalgias
and
arthralgias
Nausea
and
vomi-ng
3rd
visit
to
health
care
system
-
47
year
old
male
Addi-onal
history:
MSM
Recent
unprotected
sex
with
an
HIV
infected
partner
PMH:
prior
history
of
syphilis
Exam:
Fever
Cervical
lymphadenopathy
Rash
(started
on
torso
spread
to
limbs
and
scalp)
-
Diagnosis
Acute
HIV
Infec-on
-
Viral
Infec-ons
and
Immunity
• Three
outcomes
of
a
viral
infec-on
– Death
– Eradica-on
– Chronic
infec-on
Latency
Viral
ac-vity
-
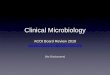
Chronic Infection: Viral Latency and Replication
Immune
Response
VZV,
HSV,
EBV,
CMV
HIV
-
HIV infection
J. Coffin, XI International Conf. on AIDS, Vancouver, 1996
-
Acute
HIV
Infec-on
-
Acute
HIV
Infec-on
Early
events
and
Diagnosis
CTL
-
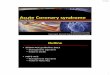
The
level
of
HIV
in
the
blood
stream
following
seroconversion
predicts
disease
progression
HIV
Vira
l Loa
d
One year
Rapid Progression
Slow Progression
28, 240
59, 987
11,843
Interquartileranges
Lyles et al, 2000
-
Par-al
Control
Why
can’t
the
immune
system
more
effec-vely
control
HIV
replica-on?
-
Viral factors
Host immune responses
Host genetic factors
-
New virus assembly
Neutralizing Antibodies
B cell
-
• Viral
debris
• Rapid
evolu-on
and
diversifica-on
• Inadequate
T
cell
“help”
Why
do
neutralizing
an-bodies
fail?
-
New virus assembly
2-3 Days
CTL
Solublefactors
-
If
CTL
are
present,
why
is
the
immune
response
not
more
effec-ve
in
HIV
infec-on?
-
An-gen
Presen-ng
Cell
Class
II
CD4+
Th
Cell
CD4
HIV‐Specific
T
Helper
Cells
are
impaired
in
all
stages
of
disease
TCR
1.
Ac-va-on
2. Clonal
expansion
3.
Cytokine
secre-on
-
Cri-cal
rela-onship
between
CD4
and
CD8
-
What
happens
to
HIV‐specific
T
helper
cells?
-
Acute
HIV
infec-on
-
Acute
HIV
Infec-on
Early
events
and
Diagnosis
CTL
-
Treatment
Should
individuals
with
Acute
HIV‐1
infec-on
be
treated
with
an-retroviral
therapy?
-
Advantages
Disadvantages
Preserva-on
of
HIV‐specific
cellular
immune
responses
Toxici-es
and
unknown
long‐term
risks
Opportunity
for
structured
treatment
interrup-on
Short‐
and
long‐term
clinical
benefits
are
not
well‐defined
Lowering
of
HIV‐1
set
point
Resistance
acquisi-on
Limita-on
of
viral
evolu-on
and
diversity
Limita-on
of
future
an-retroviral
therapy
op-ons
Decreased
transmission
Quality
of
life
impact
Mi-ga-on
of
acute
retroviral
symptoms
Cost
Kassutto et al, Clinical Infectious Diseases 2006
-
HIV‐Specific
T
helper
cells
Can
treatment
ini-ated
during
acute
HIV
infec-on
preserve
HIV‐specific
T
helper
cells?
-
What
happens
to
HIV‐specific
T
helper
cells?
Pathogenesis
hypothesis:
•
HIV‐specific
T
helper
cell
responses
are
generated
and
subsequently
lost
during
acute
infec-on
Treatment
hypothesis:
•
Treatment
with
ARV
during
acute
infec-on
will
protect
these
responses
from
being
lost
-
Ac-va-on
&
Expansion
Impairment
Infec-on
CD4
cells
Class
II
CD4
TCR
-
Ac-va-on
&
Expansion
An-retroviral
therapy
CD4
cells
Class
II
CD4
TCR
-
Characteristic Acute Early total n Median age (years)
[IQR] 35
[31,39] 37
[34,43] 102
Male gender (%) 94 94 102 HIV Risk Factor
MSM (%) 82 81 94
White race (%) 77 78 102
Mean baseline VL (copies/mL)
(range)
5.61 million
(11,000-95 million)
382,000 (2800-2.95
million) 75
Mean baseline CD4 (cells/mm3)
(range)
445 (42-1093)
567 (170-981) 100
Kassutto et al, CID 2006
-
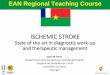
control chronic acute acute LTNP 1
10
100
1000
Rx No
Rx
S0mula0
on
inde
x
Rosenberg et al, Science 1997
Elite controllers
-
Clinical
Point
•
Immune
damage
occurs
in
the
earliest
stages
of
acute
HIV
infec-on:
there
appears
to
be
a
“window
of
opportunity”
to
reverse
this
damage
with
treatment
•
Highly
drug
resistant
virus
can
be
transmiDed
during
acute
infec-on:
viral
genotyping
is
recommended
if
treatment
is
ini-ated
-
Treatment
Interrup-on
If
treatment
during
acute
infec-on
restores
immune
responses
similar
to
the
elite
controller
phenotype…
Can
treatment
ini-ated
during
acute
HIV
infec-on
be
discon-nued?
-
Lessons from Berlin Lisziewicz et al, NEJM 340 (21), 1999
-
Augment
HIV‐specific
immunity
Hypothesis
-
Can
therapy
be
discon-nued?
• Will
HIV‐1‐specific
immune
responses
generated
and
maintained
during
acute
infec-on
be
enough
to
control
viremia?
• Can
a
“snap‐shot”
of
autologous
virus
further
boost
the
immune
system?
-
Mul-ple
Treatment
Interrup-ons
36
-
Can
therapy
be
discon-nued?
-
“STI”
Structured
treatment
interrup-on
Several
paDerns
have
emerged
– Failure
– Transient
control
of
viremia
with
sudden
loss
of
containment
– Control
(
durability?)
• This
strategy
works
50%
of
the
-me…
Are
we
doing
it
correctly?
Rosenberg et al, Nature 2000 Kaufmann et al, PLoS Med 2004
-
Treatment
Interrup-on
Strategies
Terminal
Treatment
Discon-nua-on
39
-
40
Terminal
Treatment
Discon-nua-on
• ACTG
5187
• Four
gene
DNA
vaccine
•
20
subjects
treated
during
acute
HIV
infec-on
•
Randomized
to
DNA
vaccine
versus
placebo
•
Amer
4th
vaccina-on
(week
30),
ARV
was
discon-nued
Rosenberg,
et
al:
PLoSOne,
2010
-
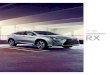
1. Median viral load in placebo group (3.7 log10) 5,012
copies/ml
2. This is markedly different from expected VL based on MAC’s
data (28,000 copies)
3. CD4 counts remained stable during treatment interruption
HIV
RNA
Terminal
Treatment
Interrup-on
Rosenberg,
et
al:
PLoSOne,
2010
-
Future
Direc-ons:
Sor-ng
it
all
out
• More
ques-ons
then
answers…
•
Is
treatment
interrup-on
a
viable
clinical
strategy?
•
Should
individuals
with
acute
infec-on
be
treated
at
all?
• Can
we
rely
on
clinical
trials
to
sort
it
all
out?
-
Future
Direc-ons
:Modeling
Biomedical
Problems
• Mul-disciplinary
collabora-on
is
essen-al
MGH‐NCSU
• Physician‐Scien-sts
do
not
understand
math!
•
Be
prepared
for
skep-cism
•
Be
the
“science
behind
the
science”
-
Smarter
Trial
Design
•
In
the
absence
of
clinical
data,
physicians
rely
on
“experience”,
“expert
opinion”
and
“educated
guessing”
• Can
sophis-cated
mathema-cal
and
sta-s-cal
models
of
Acute
HIV
infec-on
more
effec-vely
design
clinical
trials?
-
Popula-on
Based
Simula-on
100
“virtual”
pa-ents
-
Conclusions…
•
The
early
events
in
acute
HIV
infec-on
may
represent
a
unique
“window
of
opportunity”
for
treatment
•
It
is
not
known
whether
treatment
during
acute
infec-on
is
the
correct
thing
to
do
•
STI
may
have
a
role
in
management
of
treated
during
acute
infec-on
but
op-mal
approach
not
known.
•
Can
Quan-ta-ve
modeling
be
used
to
op-mize
the
design
and
conduct
of
clinical
trials?
-
Acknowledgements
• The
MGH
Team
– Marcus
Alpeld
– Todd
Allen
–
Jenna
Rychert
– Daniel
Kaufmann
– Bruce
Walker
–
Suzanne
Bazner
– Lindsay
Jones
•
The
NCSU
Team
– H.
T.
Banks
– Marie
Davidian
–
Shuhua
Hu
-
Solid
Organ
Transplanta-on
-
Solid
Organ
Transplanta-on
•
Every
transplant
requires
a
Donor
and
a
Recipient
•
Unless
the
donor
and
recipient
are
a
perfect
gene-c
match,
the
recipient
immune
system
will
reject
the
transplanted
organ
•
Rejec-on
ul-mately
results
in
failure
of
the
transplanted
organ
•
Every
transplant
recipient
must
take
immunosuppressive
therapy
to
prevent
rejec-on
•
-
Solid
Organ
Transplanta-on
•
Every
transplant
recipient
must
take
immunosuppressive
therapy
to
prevent
rejec-on
•
Transplant
recipients
are
pharmacologically
immunosuppressed
and
therefore
much
more
suscep-ble
to
serious
infec-on
•
A
major
problem
in
immunosuppressed
pa-ents
is
the
reac-va-on
of
latent
viruses
such
as
CMV,
VZV,
HSV
and
EBV
-
The Balance of Immunosuppression
Infec-on
Rejec-on
-
Latency vs re-activation: a delicate balance
Immune pressure
May result in rejection
Viral replication
Viral latency
-
Latency vs re-activation: a delicate balance
Immune pressure
Viral replication
Intermittent periods of viremia and control
-
Can
modeling
be
used
to
inform
and
op-mize
immunosuppression
strategies?
-
What is measurable? – Donor and Recipient tissue type/
genetics – Serologic status – Pre-transplantation immune
responses – Post-transplantation immune responses – Drug-level of
immunosuppression* – Levels of viremia over time – Graft function
– Tissue activity (via biopsy) – Activity of other viruses