Embed Size (px)
Citation preview

Margaret M. Kozak1, Jose G. Bazan2 , Daniel T. Chang2 1University of Central Florida, FL, USA, 2Stanford University, CA, USA
Acute Hematologic Toxicity in Patients Receiving Pelvic IMRT and Concurrent Chemotherapy
Acknowledgments
Drs. Daniel T. Chang and Jose G. Bazan at Stanford University for all of their help and support on this project.
Conclusions
LKB modeling confirms the expectation that incidence of HT3+ depends on type of chemotherapy received. Patients receiving pelvic IMRT ± 5FU seem to have better bone marrow tolerance than for irradiation concurrent with either Cisplatinum or MMC+5FU. Treatment with MMC+5FU has a lower TD50 and more steeply rising NTCP curve (i.e., smaller m) compared to treatment with Cis. Dose tolerance of PBM and the LSS subsite may be lower for patients treated with MMC+5FU compared to Cis.
Purpose/Objectives
To identify dosimetric parameters that correlate with acute hematologic toxicity (HT) in patients treated with whole pelvic IMRT and concurrent chemotherapy.
Introduction
An optimal radiation therapy treatment plan provides high tumor control while sparing adjacent normal tissues. This is necessary to prevent complications during and after treatment. In general, a high dose is delivered to the tumor and affected lymph nodes, with only low doses of radiation applied to the surrounding normal tissues. Although technology has improved substantially over the past several decades, it is not yet possible to completely spare normal tissues during radiation treatment. As such, patients progressing through treatment may experience skin desquamation, gastrointestinal side effects, and severe myelosuppression – common adverse effects that result in treatment interruptions.
Results
. Results A total of 26 patients experienced HT3+: 10/37 (27%) MMC+5FU; 14/32 (44%) Cis; 2/26 (8%) 5FU; 0/46 IMRT alone. PBM dosimetric parameters including mean dose were strongly correlated with HT3+ in the MMC+5FU group [26-fold increase in the odds ratio (OR) of HT3+ for V20 >75% compared to ≤ 75%, p=.0045], but not in the Cis group. Constrained optimization (0 < n ≤ 1) of the LKB model for HT3 gave parameter values n=1, m=0.09, and TD50=30 Gy for PBM in the MMC+5FU group. Exploratory calculations for the Cis group yielded n=0.94, m=0.48, and TD50=33 Gy. LSS dosimetric parameters were well correlated with HT3+ in both the MMC+5FU group (OR=18, p=.01 for patients with mean dose >median value 27 Gy versus <=27 Gy) and the Cis group (OR=5, p=.04, for patients with mean dose > median value 32.5 Gy versus <=32.5 Gy). Constrained optimization (0 < n ≤ 1) of the LKB model resulted in n=1, m=0.12, TD50=31 Gy for LSS in the MMC+5FU group and n=1, m=0.22, TD50=35 Gy for LSS in the Cis group. Neither the LKB model nor logistic regression were relevant for analyzing the 5FU and IMRT-only groups due to their very low rates of HT3+.
Materials/Methods
We assessed HT in 141 patients that received pelvic IMRT for anal, gynecologic, rectal or prostate cancers, 95 of whom received concurrent chemotherapy. Patients were separated into 4 groups based on chemotherapy received: Mitomycin+5-fluorouracil (MMC+5FU, 37/141); Cisplatinum ± 5FU (Cis, 32/141); 5FU alone (26/141); pelvic IMRT alone (46/141). Pelvic bone was contoured for each patient as a surrogate for pelvic bone marrow (PBM) and divided into sub-sites: ilium, lower pelvis (LP), and lumbosacral spine (LSS). The volumes of each region receiving 5 to 40 Gy (V5 to V40) were calculated. The endpoint for hematologic toxicity was grade 3 or higher (HT3+) leukopenia, neutropenia or thrombocytopenia. Normal tissue complication probability (NTCP) was calculated using the Lyman-Kutcher-Burman (LKB) model. Logistic regression was used to analyze association between HT3+ and dosimetric parameters.
Figure 1. Example of radiation treatment plan.!
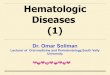
Table 1: Patient Characteristics!
Characteristic Value Chemotherapy MMC/5-FU Cisplatinum +/- 5-FU 5-FU RT alone
37 32 26 46
Age, median (range) MMC/5-FU Cisplatinum +/- 5-FU 5-FU RT alone
62 y (33-88 y) 59 y (45-78 y) 59.5 y (37-88 y) 59 y (33-85 y) 69 y (33-83 y)
Females/Males, No. MMC/5-FU Cisplatinum +/- 5-FU 5-FU RT alone
74/67 22/15 30/2 13/13 9/37
Type of Malignancy, No. Anal Cancer Gynecologic Cancers* Rectal Cancer Prostate Cancer
43 36 25 37
Body mass index, median (range) MMC/5-FU Cisplatinum +/- 5-FU 5-FU RT alone
26.3 (16.8 – 75) kg/m2 25.1 (18.8 – 47.7) kg/m2 25.6 (16.8 – 75) kg/m2 26.7 (20 – 37.9) kg/m2 27.9 (18.4 – 39.9) kg/m2
Radiation Dose to Primary Tumor, median (range) MMC/5-FU Cisplatinum +/- 5-FU 5-FU RT alone
54 Gy (50-59.4 Gy) 50.4 Gy (45-66.6 Gy) 50 Gy (45-60 Gy) 70 Gy (45-78 Gy)
Radiation Dose to Pelvis, median (range) MMC/5-FU Cisplatinum +/- 5-FU 5-FU RT alone
45 Gy (40 – 45 Gy) 48.6 Gy (45-51 Gy) 45 Gy (0-49.7 Gy) 50 Gy (43.2 – 51.2 Gy)
MMC/5-FU Cisplatinum +/- 5-FU
5-FU RT alone
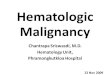
WBC Grade 0 Grade 1 Grade 2 Grade 3 Grade 4
7 7 15 5 3
3 6 9 11 3
14 6 4 2 0
23 16 7 0 0
ANC Grade 0 Grade 1 Grade 2 Grade 3 Grade 4
10 12 8 7 0
10 7 7 3 5
20 2 2 2 0
29 17 0 0 0
Hgb Grade 0 Grade 1 Grade 2 Grade 3 Grade 4
6 22 8 1 0
3 16 7 6 0
4 18 2 2 0
17 29 0 0 0
Platelets Grade 0 Grade 1 Grade 2 Grade 3 Grade 4
7 24 4 2 0
5 22 3 1 1
20 6 0 0 0
16 29 1 0 0
Any grade 3+ 10 (27%) 14 (44%) 2 (15%) 0%
Table 2: Hematologic Toxicity By Type of Treatment!
References 1. Ellis RE. The distribution of active bone marrow in the adult. Phys Med Biol. Jan 1961;5:255-258. 2. Bazan JG, Hara W, Hsu A, et al. Intensity-modulated radiation therapy versus conventional radiation therapy for squamous cell carcinoma of the anal canal. Cancer. Aug 1;117(15):3342-3351. 3. Mell LK, Schomas DA, Salama JK, et al. Association between bone marrow dosimetric parameters and acute hematologic toxicity in anal cancer patients treated with concurrent chemotherapy and intensity-modulated radiotherapy. Int J Radiat Oncol Biol Phys. Apr 1 2008;70(5):1431-1437. 4. Bazan JG. Normal Tissue Complication Probability Modeling of Acute Hematologic Toxicity in Patients Treated with Intensity-Modulated Radiation Therapy for Squamous Cell Carcinoma of the Anal Canal. Int J Radiat Oncol Biol Phys. 2012. (in press) 5. Tierney RM, Powell MA, Mutch DG, Gibb RK, Rader JS, Grigsby PW. Acute toxicity of postoperative IMRT and chemotherapy for endometrial cancer. Radiat Med. Nov 2007;25(9):439-445. 6. Chen CC, Lin JC, Jan JS, Ho SC, Wang L. Definitive intensity-modulated radiation therapy with concurrent chemotherapy for patients with locally advanced cervical cancer. Gynecol Oncol. Jul;122(1):9-13. 7. Lujan AE, Mundt AJ, Yamada SD, Rotmensch J, Roeske JC. Intensity-modulated radiotherapy as a means of reducing dose to bone marrow in gynecologic patients receiving whole pelvic radiotherapy. Int J Radiat Oncol Biol Phys. Oct 1 2003;57(2):516-521. 8. Morris M, Eifel PJ, Lu J, et al. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N Engl J Med. Apr 15 1999;340(15):1137-1143. 9. Greven K, Winter K, Underhill K, Fontenesci J, Cooper J, Burke T. Preliminary analysis of RTOG 9708: Adjuvant postoperative radiotherapy combined with cisplatin/paclitaxel chemotherapy after surgery for patients with high-risk endometrial cancer. Int J Radiat Oncol Biol Phys. May 1 2004;59(1):168-173. 10. Brixey CJ, Roeske JC, Lujan AE, Yamada SD, Rotmensch J, Mundt AJ. Impact of intensity-modulated radiotherapy on acute hematologic toxicity in women with gynecologic malignancies. Int J Radiat Oncol Biol Phys. Dec 1 2002;54(5):1388-1396. 11. Lhomme C, Fumoleau P, Fargeot P, et al. Results of a European Organization for Research and Treatment of Cancer/Early Clinical Studies Group phase II trial of first-line irinotecan in patients with advanced or recurrent squamous cell carcinoma of the cervix. J Clin Oncol. Oct 1999;17(10):3136-3142. 12. Albuquerque K, Giangreco D, Morrison C, et al. Radiation-related predictors of hematologic toxicity after concurrent chemoradiation for cervical cancer and implications for bone marrow-sparing pelvic IMRT. Int J Radiat Oncol Biol Phys. Mar 15;79(4):1043-1047. 13. Liang Y, Messer K, Rose BS, et al. Impact of bone marrow radiation dose on acute hematologic toxicity in cervical cancer: principal component analysis on high dimensional data. Int J Radiat Oncol Biol Phys. Nov 1;78(3):912-919. 14. Taylor A, Powell ME. Conformal and intensity-modulated radiotherapy for cervical cancer. Clin Oncol (R Coll Radiol). Aug 2008;20(6):417-425. 15. Du XL, Tao J, Sheng XG, et al. Intensity-modulated radiation therapy for advanced cervical cancer: A comparison of dosimetric and clinical outcomes with conventional radiotherapy. Gynecol Oncol. Dec 22. 16. Mell LK, Tiryaki H, Ahn KH, Mundt AJ, Roeske JC, Aydogan B. Dosimetric comparison of bone marrow-sparing intensity-modulated radiotherapy versus conventional techniques for treatment of cervical cancer. Int J Radiat Oncol Biol Phys. Aug 1 2008;71(5):1504-1510.