Embed Size (px)
Citation preview
Acute Cholangitis
Prasanth Patcha, MD 24 April 2014
www.downstatesurgery.org
Case
87F hx of hypothyroid, dementia sent from SNF to ED for AMS and fever; Called by ED for hypotension, LFT’s; PSH: sigmoidectomy, end colostomy (volvulus) Multiple PEG tubes 103.4 77/44 104
www.downstatesurgery.org
Case
3/31 17:31h cbc 6.19 / 15 / 46 / 243 82% bmp 140 / 4.9 / 101 / 20 / 17 / 1.48 / 88 lft 7.2 / 3.8 / 183 / 197 / 584 / 6.6 (Db 4.6) LA 5.4
www.downstatesurgery.org

www.downstatesurgery.org
www.downstatesurgery.org

Case
4/1/14 0240h CBC 22.9 / 11.8 / 36 / 236 79% BMP 141 / 3.7 / 111 / 16 / 18 / 1.82 / 107 LFT 5.5/ 2.9 / 123 / 144 / 382 / 4.9 ABG 7.29 / 36 / 199 / 98 / 17 / -8.0
www.downstatesurgery.org
Case
• Intubated overnight in SICU for AMS
• Pressor therapy by AM
• Emergent ERCP – sphincterotomy – stent placed – stones extracted
www.downstatesurgery.org

Case
• Immediate improvement
• Weaned from pressors
• Extubated several days later
• Presently tolerating diet, awaiting discharge planning
www.downstatesurgery.org
Acute Cholangitis
• Ascending infection / inflammation of the
biliary tree
• Extremely rapid deterioration
www.downstatesurgery.org
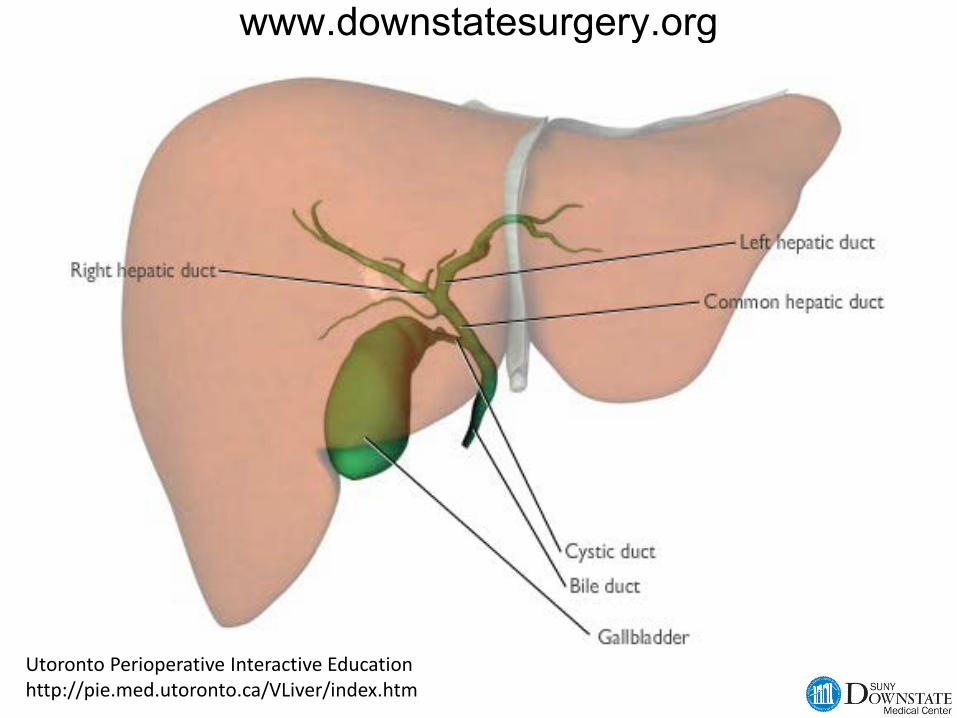
Utoronto Perioperative Interactive Education http://pie.med.utoronto.ca/VLiver/index.htm
www.downstatesurgery.org
Epidemiology
• Median age 50 – 60
• Obstruction
– secondary choledocholithiasis (most common) – primary choledocholithiasis (Asians) – proximal obstruction
www.downstatesurgery.org
Pathophysiology
• Despite communication – bile usu sterile
• Bacterial overgrowth leads to increase in pressure – lymphatic/venous congestion – bacterial dissemination
www.downstatesurgery.org

Pathophysiology
• Instrumentation largely implicated
– stents – drains – strictures – ERCP – 0.5 to 1.7% of cholangitis
www.downstatesurgery.org
Pathophysiology
G- E coli Klebsiella Enterobacter G+ Enterococcus An Bacteroides Clostridium
www.downstatesurgery.org
Presentation
• Charcot’s Triad – fever – jaundice – RUQ pain
• Reynold’s Pentad – AMS – hypotension
<50%
www.downstatesurgery.org
Diagnosis
• Clinical Dx using radiography and lab values as supportive
• Need high suspicion in elderly or immunocompromised
• Or especially those with known biliary issues
www.downstatesurgery.org
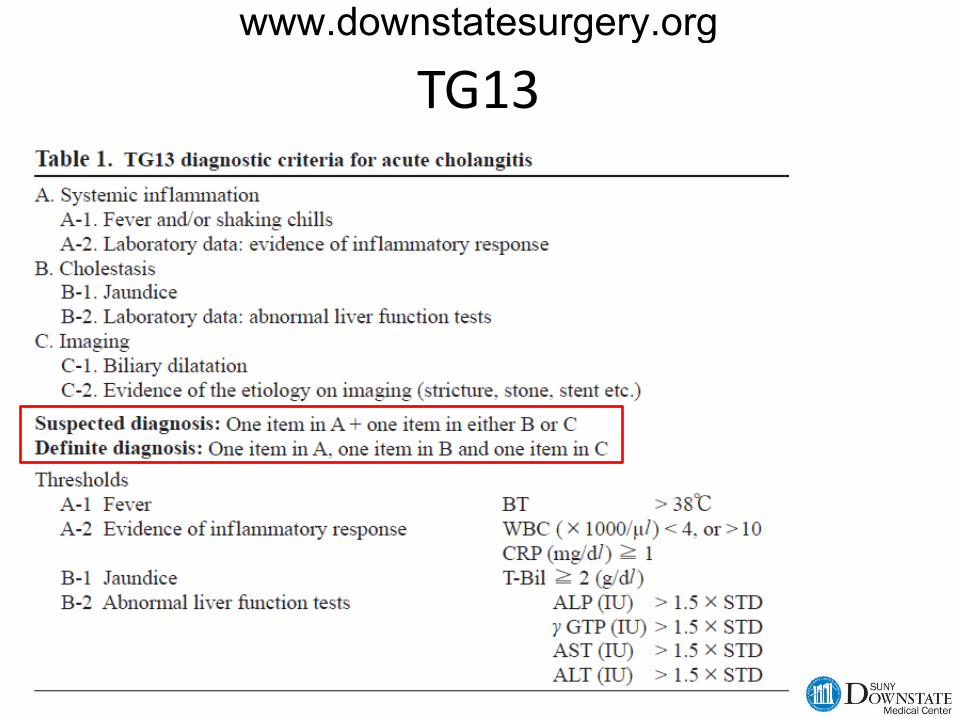
TG13 www.downstatesurgery.org
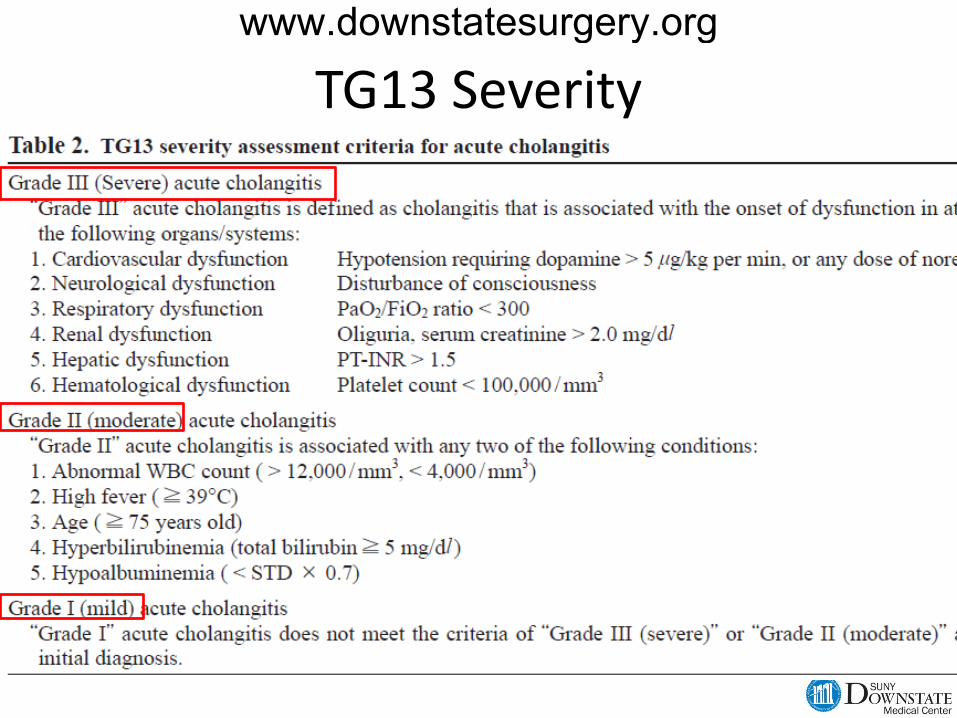
TG13 Severity
www.downstatesurgery.org

Tokyo LOL www.downstatesurgery.org
www.downstatesurgery.org
Treatment
• Resuscitation
• BCx Then abx;
• EARLY DRAINAGE from below, or above
www.downstatesurgery.org

Treatment
• ERCP
• PTC
• If fail then OR – 40% mortality – Place T-tube and run
www.downstatesurgery.org
References Cameron, et al. Current Surgical Therapy. Sabiston. Textbook of General Surgery. Mayumi, T, et al. Tokyo Guidelines 2013.
www.downstatesurgery.org