Embed Size (px)
Citation preview

Acute Aortic Occlusion Secondary to Aspergillus Endocarditis in an Intravenous Drug Abuser
Jerry T. Light, Jr., MD, Mark Hendrickson, MD, William M. Sholes, MD, Darin A. Portnoy, BS, William H. Bell, 111, MD, Morris D. Kerstein, MD New Orleans, Louisiana
A 55year-old black man, an intravenous substance abuser who had an acute arterial embolus to the distal aorta originating from his mitral valve, was noted on pathologic examination of the clot to have aspergillosis emboli. The infective endocardltls also resulted in emboli to the brain with subsequent death. (Ann Vasc Surg 1991 ;5271-275).
KEY WORDS: Aspergillosis; emboli; cardiac valve endocarditis; drug abuse.
Acute arterial occlusion is an emergent vascular event caused by embolism, thrombosis, or trauma, requiring aggressive reperfusion. In the case of embolism, sources are mural thrombus, atrial fibril- lation, prosthetic valves, vegetative valve disease, atrial myxoma, or paradoxical emboli. Acute embo- lic occlusion can lead to distal ischemia and hy- poxia. Progressive tissue damage will occur with the sequelae of increasing morbidity and mortality. This report demonstrates a case of systemic embo- lism from fungal endocarditis and records the oc- currence of an aspergillosis embolism with distal aortic occlusion in an intravenous drug abuser. I t also reflects a literature search of the past 20 years.
CLINICAL SUMMARY A 55-year-old black man, an intravenous heroin
and cocaine abuser, arrived at the Emergency De- partment of Charity Hospital of Louisiana in New Orleans with crampy left calf pain, which had
From the Department of Siirgery, Tiilane University School of Medicine, New Orleans, Louisiana. Reprint requests: Morris D . Kerstein, MD, Department of Surgery, Hahnemann University, School of Medicine, Broad and Vine Streets, Philadelphia, Pennsylvania 1 91 02-1 1 92.
progressed to numbness and weakness over the prior 36 hours. Five days before presentation, the patient had noticed right calf pain and weakness, which resolved after two days. He was not aware of a temperature differential between his feet, denied fever or chills, and admittcd to uninterrupted intra- venous heroin and cocaine use.
Examination demonstrated no adenopathy, a murmur of mitral insufficiency, and equally cool lower extremities. No pulses were palpable at or beneath the inguinal ligaments bilaterally. On the left, S-1 and L-3 deep tendon reflexes were absent and motor strength was demonstrated to be 315 with flaccid muscle tone. A left S-1 paresthesia was also noted, The right-sided neurologic examination was normal.
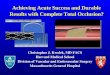
Doppler examination revealed absent distal pulses with faint, monophasic femoral signals, bi- laterally. Emergent aortogram with run-off through the left axillary artery was performed and showed minimal atherosclerosis and distal aortic occlusion (Fig. 1). The patient underwent bilateral femoral embolectomies with bilateral fasciotomies. Postop- eratively, the patient developed acute renal failure due tq myonecrosis, which responded to mannitol diures s and urine alkalization.
Fungal cultui-es of the embolus grew Aspergillus flavus. Serial blood cultures were negative. Human
27 I

272 ACUTE AORTIC OCCLUSION Ah’D ASPERGILLUS ENDOCARDITIS A Y N A I . ~ OF VASCULAR SURGERY
Fig. 1. Aortogram showing minimal atherosclerosis and distal aortic occlusion.
immunotrophic virus (HIV) status was negative (T4 = 16, T8 = 27, and T4ff8 = 0.6). An echocar- diogram demonstrated an anterior mitral valve leaf- let vegetation. Amphotericin B therapy was initi- ated. Subsequent embolization to the right common femoral artery required another embolectomy . Ten days after admission, the patient suffered a massive stroke (confirmed by computed tomography scan) and died as a result before mitral valve replacement could be performed. The necropsy findings were endocarditis with mitral vegetations and emboliza- tion to the femoral arteries, kidneys, and spleen. Examination of the head was not permitted by the family.
DISCUSSION The incidence of fungal endocarditis and embo-
lism is increasing and is usually associated with narcotics addiction, postcardiac surgery, prolonged intravenous antibiotic drug use, and the immune- compromised host [ 1,2]. Negative blood cultures are commonly associated with fungal endocarditis [3]. Currently, about 10% to 20% of all cases of endocarditis are culture negative. The fungal etiol- ogy of endocarditis in the United States over the past 50 years, however, is reported to be from 0.0% to 6.7% [1,4].
Overall, fungal infective endocarditis is uncom- mon, but increasing in incidence. Infective en- docarditis by Aspergillus is rare; only 14 cases of nonprosthetic heart valve infections have been de-
scribed [3,5,6]. Candida species account for about 75%, while Aspergillus species account for approx- imately 25% [3,5,6]. Embolism (major vessel, in- tracranial, and lower extremity), however, involves the two organisms with relative equality; it also distinguishes fungal endocarditis from that caused by bacteria. With mycotic emboli, the femoral site of embolization is most common. The second most common site is the aorta, but this occurs with only one-fourth the frequency of femoral emboli. Not uncommonly, subsequent fungal emboli occur, as in this patient. In addition, fungal endocarditis and emboli were more common in all high-risk groups: postcardiac surgery patients, patients undergoing prolonged intravenous antibiotic therapy, and her- oin addicts. A review of the literature shows blood culture-negative endocarditis with major vessel em- bolization to be apparently pathognomonic for a fungal etiology [3,5-8]; it should be presumptively treated as such.
This patient represents a report of aortic occlu- sion by Aspergillus embolism in an intravenous drug abuser. Addicts with infective endocarditis often have distinguishing features: the infection more often involves the tricuspid valve [1,61; the mitral valve is involved alone in only 10.8% of patients [ 1,6]; two-thirds of patients have no clinical evidence of underlying heart disease; and septic pulmonary emboli by plain radiography are present in 87% of patients. Parenteral drug addicts are usually diagnosed with tricuspid valve and, rarely, pulmonary valve endocarditis or pulmonary artery mycotic aneurysms. Their endocarditis is associ- ated with cellulitis, septic phlebitis, and invasive access lines. The prognosis is poor in intravenous drug abusers if they have congestive heart failure, extreme age, aortic or multiple valve involvement, or antimicrobial failure [ 1,6]. Death usually pro- ceeds from congestive heart failure (valve failure or myocardial damage), embolization, renal insuffi- ciency, or mycotic aneurysm rupture [ 1,6].
Aspergillosis is an opportunistic mycosis. Others include Cryptococcus, Candida, and Zygomycosis, all of which are usually invasive in immune-com- promised patients. Aspergiffus furnigatus is the usual agent of aspergillosis infection [91. The sec- ond most important species is Aspergillusflaws 191. Aspergillus species are ubiquitous in the environ- ment and are usually acquired by inhalation, al- though invasive procedures may lead to introduc- tion or implantation of the spores. Usual portals of entry are through the lungs or paranasal sinuses. In the immune-compromised patient, no granulation tissue develops. Instead, hemorrhagic infarction or bland necrosis with abundant hyphae growing in blood vessels or in colonies with radial arrays in tissue occurs. Aspergillus hyphae in tissues are easily missed on hematoxylin-eosin stained speci- mens. With periodic acid-Schiff (PAS) or Gomori

VOLUME NO 3 - 1991 ACUTE AORTIC OCCLUSION AND ASPERGILLUS E~DOCARDITIS 273
Fig. 2. Mitral valve aspergillus vegetation of patient.
methenamine silver stain, the hyphae are 2 to 4 microns wide, of even diameter, frequently septate, and dichotomously branched (Fig. 2).
Aspergillus may invade normal, damaged, or prosthetic cardiac valves [ 101. Aspergillus-induced endocarditis resembles bacterial endocarditis; how- ever, blood cultures are consistently negative. The classic vegetative lesion of infective endocarditis is along the line of closure of a leaflet on the atrial surface of the atrioventricular valves (Fig. 3), or the ventricular surface of the semilunar valves. In con- trast to less virulent mycoses, Aspergillus invades the myocardium. A fibrin-platelet thrombus ex- pands on damaged endocardium, acting as a trap to the spore and a barrier to phagocytes. Continued infection leads to mass enlargement of the vegeta- tion and endocardia1 invasion. The latter results in valve cusp erosion, chordae tendineae rupture, and myocardial abscess formation. The vegetations can break off and embolize to the brain, spleen, kid- neys, coronary arteries, and large arteries of the extremities [ 1,4]. Major vessel emboli (aortic, bra- chial, femoral, or popliteal) are more frequent in fungal endocarditis.
The majority of cases of aspergillus endocarditis are recognized after dissemination; i.e., emboliza-
tion [l 13. Echocardiography, however, can aid in the diagnosis. Several conclusions may be drawn concerning vegetations and embolism with refer- ence to two-dimensional and M-mode echocardiog- raphy (Fig. 4). Patients with vegetations seem to have a higher incidence of embolic events. While the converse does not preclude embolism, abrupt changes in the size of vegetations usually occur after embolization.
Combination chemotherapy with amphotericin B and flucytosine is recommended in fungal en- docarditis. Anlphotericin B, a polyene antifungal, binds to membrane sterols [1,4]. Flucytosine is a competitive inhibitor of pyrimidines. Intravenous amphotericin B is the drug of choice for invasive aspergillosis [ 1,4]. When treating with amphotericin B, results are better with early diagnosis, rapid initiation and dose advancement, and lesser degrees of immune suppression [3,5-81. A recommended maintenance dosage is 0.5 to 0.6 mglkglday of amphotericin €3, given up to a total dosage of 2.0 to 2.5 grams [4,6,9]. The use of an Aspergillus isolate with minimum inhibitory concentration determina- tion has no ready therapeutic interpretation as in bacterial assessment [9]. Flucytosine is also used in the treatment of aspergillosis; however, no ade-

ANNALS OF ACUTE AORTIC OCCLUSION AND ASPERGILLUS ENDOCARDITIS VASCULAR SUKGERY
Fig. 3. Aortic embolus. Gomori mesthenamine silver stain demonstrates aspergillus.
quate accumulated clinical data exist to judge flucy- tosine alone or even in combination with amphoter- icin B [4,6,9].
Early surgical intervention is recommended [3,5- 7). The generally accepted indications for surgical intervention in infectious endocarditis are: refrac- tory congestive heart failure, systemic emboliza- tion, uncontrolled infection, valve dysfunction, in-
Fig. 4. Ultrasound of rnitral valve (two-dimensional echocardiogram).

ACUTE AORTIC OCCLUSION A N D ASPERGILLUS ENDOCARDITIS 275 VOLUME No 3 - 1991
effective antimicrobials, mycotic aneurysms, prosthetic valve endocarditis, and perivalvular/ myocardial abscesses. In relative order of inci- dence, deaths from endocarditis in the United States over the past 50 years result from: congestive heart failure, embolism, mycotic aneurysm rupture, and the complications of cardiac surgery [3,5-71. Even with medical and surgical treatment, the mor- tality rate for fungal endocarditis with peripheral embolism is greater than 80% [3,5-71. In the United States’ literature, no patient with fungal valve en- docarditis of a prosthetic valve has survived with- out valve replacement [3,5-7,121.
Cardiac aspergillosis has been reported in an acquired immune deficiency syndrome (AIDS) pa- tient. The patient, a 32-year-old intravenous drug abuser with earlier hospitalization for oral and esophageal candidiasis, had a right hemispheric infarct and an Aspergillus fumigutus vegetation on his anterior mitral valve [13]. No aortic emboliza- tion in association with Aspergillus endocarditis was reported, yet other systemic embolizations occurred in 4 of 13 patients with AIDS and fungal endocarditis.
Another source of embolization is a mural throm- bus. Embolization from a mural thrombus invaded by Aspergillus has not been reported. However, Young and associates reported that, of 98 patients they reviewed, one had numerous mural thrombi invaded with aspergillus, [2].
In addition, the spread of invasive aspergillosis can cause thrombosis of the thoracic aorta. Byard and colleagues reported a patient with aortic throm- bosis resulting from fungal backgrowth into the aortic lumen [14]. Of final note, Aspergillus en- docarditis has also been associated with false, true, and pseudoaneurysms of the aorta [121.
CONCLUSION
In summary, Aspergillus endocarditis with embo- lization is uncommon and frequently fatal. Fungal endocarditis should be considered in any patient with unexplained fever, negative blood cultures, and evidence of ernbolization. This is especially true in intravenous drug abusers, immune-compro- mised patients, and those patients receiving long-
term parenteral drug therapy. Echocardiography will help to confirm the diagnosis. Prompt medical and surgical intervention appear to give these pa- tients the greatest hope of survival.
ACKNOWLEDGMENT We thank Gae 0. Decker-Garrad for editorial
assistance. ,
1
2
3
4
5
6.
7.
8.
9.
10.
1 1 .
12.
13.
14.
REFERENCES CARROLL K, CHEESEMAN S. Infective endocarditis. In: DALEN J, ALPERT JS (eds). Valvular Heart Disease, 2nd Edition. Boston: Little. Brown and Company, 1987, pp
YOUNG RC, BENNETT JE, VOGEL CL, et al. Aspergillo- sis: the spectrum of the disease in 98 patients. Medicine
RUBINSTEIN E. NORlEGA ER, SIMBERKOFF MS, et al. Fungal endocarditis: analysis of 24 cases and review of the literature. Medicine 1975;54:331-342. SCHELD WM. SANDE MA. Endocarditis and intravascu- lar infections. In: MANDEL A (ed). Infectious Diseases. New York: John Wiley & Sons, 1987, pp 504-530. KAMMER RB, UTZ JP. Aspergillus species endocarditis. Am J Med 1974;56:50fj-521. VO NM. RUSSELL JC, BECKER DR. Mycotic emboli of the peripheral vessels: analysis of 44 cases. Surgery 1981; 90:541-545. BARST RJ, PRICE AS, NEU HC. Aspergillus endocarditis in children: case report and review of the literature. Pediat- rics 1981;68:73-78. WEILAND D, FERGUSON RM, PETERSON PK, et al. Aspergillosis in 25 renal transplant patients. Ann Surg 1983; 198522629. BENNETT J. Aspergillus species. In: MANDEL A (ed). Infectious Diseases. New York: John Wiley & Sons, 1987, pp 1447-1452.
pergillus fumigatus endocarditis on a normal heart valve. South Med J 1983;76:506-508. SWENSSON EE, WILLMAN VL, PETERSON GJ. Acute aortic occlusion from aspergillosis in a healthy patient with survival. J Vasc Surg 1986;4:187-191. CORRIGAN C, HORNER S. Aspergillus endocarditis in association with a false aortic aneurysm. Clin Cardid 1988; fi:43@-432. HENOCHOWICZ S, MUSTAFA M, LAWBINSON WE, et al. Cardiac aspergillosis in acquired immune deficiency syndrome. A m J Curdiol 198535:1239-1240. BYARD RW, JIMENEZ CL, CARPENTER BF, et al. Aspergillus related aortic thrombosis. Can Med Assoc J 1987;136: 155-1 56.
54 1-575.
1970 ;49: 147-173.
VISHNIAVSKY N. SAGAR KB, MARKOWITZ SM. AS-
...