Embed Size (px)
DESCRIPTION
TCM Acu in Horses
Citation preview

Charts 1-23 (Appendix) show the location of the main APs used in conditions 1.1-1.6.
1.0. CLASSICAL TONIFICATION AND SEDATION POINTS
In TCM/Classical AP, the symptom picture, clinical exam, Chinese Pulses, facial and lingual colour etc may suggest energy (Qi) deficiency (hypoactive Qi = Xu) or excess (hyperactive Qi = Shi) in one or more Channels. Deficiency or excess Qi in a Channel can be corrected by many methods (herbal remedies, fasting, feeding, diuretics, bleeding, fluids, laxatives etc, as appropriate) but AP can also be used according to the Mother and Son Law of the Five Phase Cycle.
For Xu (deficiency) use Bu (tonification) needling: To stimulate (tonify) a weak Channel, one can needle its "Mother Point", manipulating the needle in Bu-style ("Tonification Mode", thrusting heavily and rapidly but lifting gently and slowly, while rotating the needle with small amplitude and low frequency).
For Shi (excess) use Xie (sedation) needling: To pacify (sedate) a hyperactive Channel, one can needle its "Son Point", manipulating the needle in Xie-style ("Sedation Mode", thrusting gently and slowly but lifting forcefully and rapidly, while rotating the needle with large amplitude and high frequency).
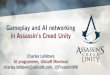
TONIFICATION AND SEDATION POINTS
PHASE METAL EARTH FIRE WATER FIRE WOOD
Mother Earth Fire Wood Metal Wood Water
Son Water Metal Earth Wood Earth Fire
PHASE METAL EARTH FIRE WATER FIRE WOOD
Channel LU LI ST SP HT SI BL KI PC TH GB LV
To Tonify: 09 11 41 02 09 03 67 07 09 03 43 08
To Sedate: 05 02 45 05 07 08 65 01 07 10 38 02
For example, in acute bacterial enteritis, with excess Qi in LI and SI Channels (Metal and Fire), one could sedate LI at the Son (Water) point of LI (LI02) and sedate SI at the Son (Earth) point of SI (SI08),
needling in Xie-style ("Sedation Mode"). One could also use fluids, demulcents, intestinal sedatives, antibacterials etc, as needed. In chronic bronchitis, with deficient Qi in the LU (Metal) Channel, one could tonify LU at its Mother (Earth) point (LU09), needling in Xu-style ("Tonification Mode"). These principles are explained in more detail in The Essentials of Chinese AP (Beijing 1993).
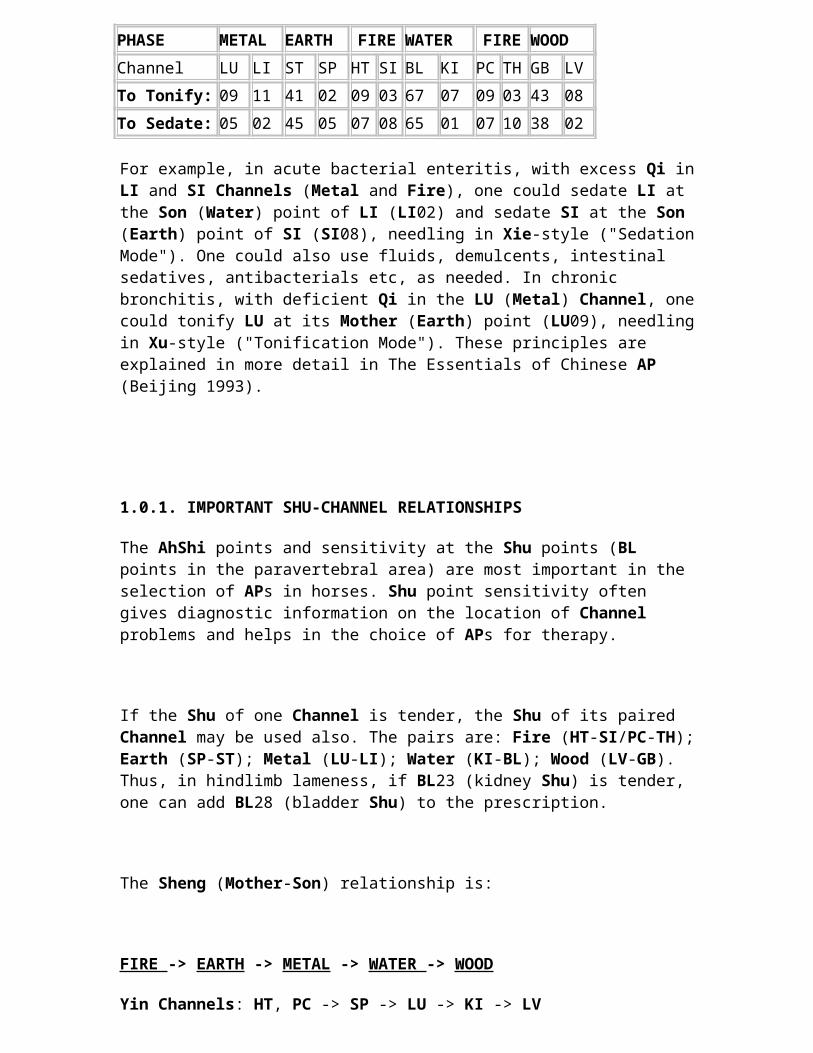
1.0.1. IMPORTANT SHU-CHANNEL RELATIONSHIPS
The AhShi points and sensitivity at the Shu points (BL points in the paravertebral area) are most important in the selection of APs in horses. Shu point sensitivity often gives diagnostic information on the location of Channel problems and helps in the choice of APs for therapy.
If the Shu of one Channel is tender, the Shu of its paired Channel may be used also. The pairs are: Fire (HT-SI/PC-TH); Earth (SP-ST); Metal (LU-LI); Water (KI-BL); Wood (LV-GB). Thus, in hindlimb lameness, if BL23 (kidney Shu) is tender, one can add BL28 (bladder Shu) to the prescription.
The Sheng (Mother-Son) relationship is:
FIRE -> EARTH -> METAL -> WATER -> WOOD
Yin Channels: HT, PC -> SP -> LU -> KI -> LV
(HT, PC nurtures SP; LV is nurtured by KI etc)
Yang Channels: SI, TH -> ST -> LI -> BL -> GB
(SI, TH nurtures ST; GB is nurtured by BL etc).
The Sheng (Mother-Son) relationship can be used clinically via the back Shu (Paravertebral BL) points:
The Mother point of HT is BL18 (LV) and of SI is BL19 (GB).

The Son point of HT is BL20 (SP) and of SI is BL21 (ST).
The Mother point of SP is BL15,14 (HT, PC) and of ST is BL27,22 (SI, TH).
The Son point of SP is BL13 (LU) and of ST IS BL25 (LI).
The Mother point of LU is BL20 (SP) and of LI is BL21 (ST).
The Son point of LU is BL23 (KI) and of LI is BL28 (BL).
The Mother point of KI is BL13 (LU) and of BL is BL25 (LI).
The Son point of KI is BL18 (LV) and of BL is BL19 (GB).
The Mother point of LV is BL23 (KI) and of GB is BL28 (BL).
The Son point of LV is BL15 (HT) and of GB is BL27 (SI).
The Mother point of PC is BL18 (LV) and of TH is BL19 (GB).
The Son point of PC is BL20 (SP) and of TH is BL21 (ST).
If there is weakness (deficiency) in a Channel, the Shu of the Mother Channel can help. If there is hyperactivity (excess energy) in a Channel, the Shu of the Son Channel can help. Thus, in weakness of KI, one could use the LU Shu (BL13) with other points; in weakness of LI, one could add the ST Shu (BL21). In excess of HT, one could add BL20 (SP Shu). In excess of ST, one could add BL25 (LI Shu). (See section 1.0. (above) for the more classical method).
Injury to Shu points, or to key APs, can have effects far more serious than "local injury" in a western sense. It may induce signs and symptoms in the associated organ or Channel and in related Channels. Injury to the paravertebral area from the withers to the tail, whether due to incompetent riding, badly fitting saddle etc must be identified and treated as quickly as possible.

Those who have not used AP in horses should study the references and, if possible, attend professional veterinary AP teaching seminars before trying to use the method. The information which follows is aimed at colleagues who know the basics of AP rather than at complete novices of the technique.
APs seem to have properties like magnetic vortices: they can receive and transmit electromagnetic signals. A point which is too deep to reach by the needle (such as KI24,25,26 on the chest wall medial to the shoulder muscles, or ST29,30 and SP12 in the abdominal muscles medial to the thigh muscles) can be acted upon by inserting a needle pointed towards the point, although the needle may not reach the point (M.J.C). The vortex theory is supported by the powerful effect of superficial implants in lameness of deep tissues or joints in horses and dogs. The implants (gold beads, orthopaedic suture wire etc) are dropped at whatever depth DeQi arrives (usually less than 1.5 inches (M.J.C). (See hip lameness, 1.1.5 below).
See Appendix 1 for details of the points and Channels (figures 1 to 26).
1.0.2. TING POINTS IN HORSES
The Ting Zones, located 1-2 cm above the hoof-hair junction, are the most distal points on each Channel. Are Thoresen (Norway) pioneered their diagnostic and therapeutic use in horses. He found that stimulation of a distant reactive body AP point on the affected Channel caused complete disappearance of the pitting in the reactive Ting Zone, within seconds. This effect was visible from several metres away. The speed of this reaction indicates that the reactivity at the Ting Zone is functional and it confirms the connection between the Ting Zone and the Channel concept of TCM.
Stimulation of the correct Ting Zones causes a biological response in the microcirculation and in the affected organ(s), part(s) or function(s) and can influence all other reactive Zones on the affected Channel, especially the Shu points, as well as the parts traversed by the Channel. Thoresen found (and we have confirmed) that needling the appropriate (usually reactive) Ting Zones can sedate ("satisfy", "cool" or obliterate reactivity from) reactive Shu points, or AhShi points elsewhere on the body within 2-15 minutes (and sometimes within 10 seconds).

Where more than 1 reactive Ting Zone is present, needling of the primary one (according to Five Phase Theory) is often followed by disappearance of the secondary Ting Zones within seconds.
Location of Ting Zones in horses
Zones 1 and 7 medial side of the fore and hind hoof respectively, 1-2 cm anterior to a line with the posterior edge of the coronet.
Zones 2 and 8 medial side of the fore and hind hoof respectively, about 1/2 of the distance between Zones 1 and 3 or 7 and 9 respectively.
Zones 3 and 9 anterior midline of the fore and hind hoof respectively.
Zones 4 and 10 lateral side of the fore and hind hoof respectively, about 1/2 of the distance between Zones 3 and 5 or 9 and 11 respectively.
Zones 5 and 11 lateral side of the fore and hind hoof respectively, 1-2 cm anterior to a line with the posterior edge of the coronet.
Zones 6 and 12 in the hollow of the heel of the fore and hind foot respectively, on a line joining the highest point of the horn on the medial and lateral side of the hoof.
Zone 1 (HT09) (forelimb, posterolateral zone) relates to the Heart Channel. The horse often pulls up towards the end of the race for no apparent reason, especially in very hot or very cold weather. There can be lameness in different joints, which may alternate from time to time. Although the HT Channel relates to the forelimb, the lameness may also affect a hindlimb. Zone 1 is often reactive in overexertion. (See Zone 5). It may be reactive in bruised sole/soft horn, laminitis and flexor tendon strain.
Zone 2 (SI01) (forelimb, mid lateral zone) relates to the Small Intestine Channel and arteries, especially the larger vessels. The symptoms may be similar to those of Zone 1 but are less obvious or

less severe. There are often intestinal problems, especially jejunal (colic, pain) and these often arise with change in feeding or a new supply of hay. This Zone often reacts in forelimb deep flexor tendon problems. It is often reactive together with Zones 10 and 11 (see below).
Zone 3 (TH01) (forelimb, anterior zone) relates to the Triple Heater Channel, skin microcirculation and especially to mucosae and joint cavities. There tends to be a recurrent sinusitis and the serous fluid in the joints is often too thin. The history often mentions frequent injections of hyaluronic acid. Zone 3 is often reactive in sore heels/heel haemorrhage, cracked heels and hoof-bend bleeders. The lesion in these cases is near Zones 6 and 12.
Zone 4 (LI01) (forelimb, mid medial zone) relates to the Large Intestine (Colon) Channel and to muscles of the forelimb and shoulder area. Faeces may smell sour and their consistency may vary widely. The case often shows purulent nasal discharges. Very often the horse pulls to one side in training or racing and does not want to lead, but prefers to run with a follower group. Trotters (which should not gallop) tend to gallop in the bends and may show signs of pain in the shoulder. Its therapeutic uses include neck problems, (reactive LI16-18, BL25), sinusitis, ankle (forelimb fetlock) problems and inside forelimb splint problems (M.J.C).
Zone 5 (LU11) (forelimb, posteromedial zone) relates to the Lung Channel. This Zone reacts often when the horse is forced to breathe dusty, stale or polluted air, or has been raced in cold weather. Zone 5 indicates whether left or right lung is affected. (The ipsilateral Zone is reactive). Zone 5 is nearly always reactive in overexertion (see Zone 1), in lung disorders and in poor quality horn (soft, easily cracked or too thin), bruised sole. Its therapeutic uses include respiratory problems, respiratory bleeders (reactive BL13, 13a, 41-47), inside forelimb splint problems, infection (M.J.C).
Zone 6 (PC09) (forelimb, between and above heel bulbs) relates to the Pericardium (Circulation-Sex) Channel, which influences the psyche and sexual hormones. The symptoms include changes in sexual behaviour, sweating, nervousness, forelimb superficial flexor tendon problems. Zone 6 is not a diagnostic Zone for beginners, as outlined below. It does not react in ways that can be detected manually by novices. It is included here to complete the systematic AP schema and because it is a valuable therapeutic Zone. Its choice is dictated by the history and symptoms.

Zone 7 (BL67) (hindlimb, posterolateral zone) relates to the Bladder Channel and the paravertebral muscles from neck to tail, in the area from the midline to 20-30 cm laterally. It relates to the hindlimb flexor tendons, especially the superficial flexors. In humans, the BL Channel is often related to headaches. Horses which are seen nodding, headpressing or headbanging often respond immediately to one treatment at Zone 7 and the response is longlasting.
Zone 8 (GB44) (hindlimb, mid lateral zone). The horse has no gallbladder but functions of the Gallbladder Channel in man are similar in the horse. Zone 8 relates to the GB Channel which relates to the back and head lateral to Zone 7, i.e. paravertebral in an area 30-60 cm lateral to the midline. It is strongly related to the hip joint and to the area of insertion of the Longissimus dorsi muscle to the tuber coxae. Marked pain sensitivity in the hip or tuber coxae area is usually associated with reactivity of Zone 8. The horse does not race well and pulls to one side. Trotters may gallop in the straight as well as on bends (see Zone 4). There may be recurrent colic (see Zone 2), especially at night. (Midnight is the hour of the GB energy in TCM).
Zone 9 (ST45) (hindlimb, anterior zone) relates to the Stomach Channel. This Channel relates to appetite, stomach function, mastitis and stamina in humans. Zone 9 is very important in cattle (mastitis) but horses rarely show reactivity at this Zone. It may be reactive in thoracic stiffness and in bone spavin. Its therapeutic uses include stifle problems, (reactive BL21, ST10, 25a, stifle points in the muscle groove below the tuber ischii), colic, toothache (M.J.C).
Zone 10 (LV01) (hind limb, mid medial zone) relates to the Liver Channel, digestion, food allergies, detoxification, eye diseases, problems of the medial hind leg muscles, also to general musculature and fitness. It is one of the most common to be found reactive in the horse. Its value in therapy is enormous. It is reactive in hind limb lameness, generalised muscle cramp (azoturia, tying-up syndrome, Monday morning disease, Easter disease, muscular dystrophy etc). Because of the importance of optimum muscle fitness in the horse, the importance of Zone 10 in diagnosis and therapy is obvious. It is also reactive in allergies (urticaria, food allergy etc) but not in dust allergy (see Zone 5). Zone 10 is often reactive together with Zones 2 and 11 (see).
Zone 11 (SP01) (hindlimb, posterolateral zone) relates to the Spleen-Pancreas Channel. In humans, this relates to digestion, reproduction, the muscles and the psyche. In horses, is diffuse. It is often reactive with Zones 2 and 10 (see). It may be used in prognosis with Zone 10 in muscle problems. If both Zones 10 and 11 are reactive together,

the prognosis is bad and recovery may take several months. Even in cases where is reactive on its own, the prognosis is bad. The signs often are confined to the hindquarter, especially during racing. A change of diet (especially hay) can shorten the recovery time when is reactive. Homoeopathic Arsenicum album D12 and Plumbum metallicum D30 (3 pillules each/day) also help to shorten recovery time by about 1 month in these cases.
Zone 12 (KI01) (hindlimb, between and above heel bulbs) relates to the Kidney Channel. The symptoms include stiffness or weakness of the lumbar area; stifle problems, bone problems (tendency to weakening, fracture, bone spavin etc), tendency to abortion and a very unreliable (dangerous) psyche. Nearly all horses with those symptoms benefit from treatment at Zone 12 and most horses between 1 to 2 years of age can also benefit from it. Zone 12 is not a diagnostic Zone for novices, as outlined below, as it does not react in ways that can easily be detected manually. It is included here to complete the systematic AP schema and because it is a valuable therapeutic Zone. Its choice is dictated by the history and symptoms.
Most details on the use of Ting Zones are from Thoresen's paper on the subject. We (Cain & Rogers), Peggy Fleming, Dominique Giniaux, Emiel van den Bosch and others, have confirmed the value of Ting Zone therapy in horses.
Clinical uses of Ting Points in horses
Ting points can be used in organic syndromes as well as in functional disorders. Thoreson has treated more than 10 cases of bone spavin. Zones 9 and 12 (ST and KI) were usually reactive. Treatment at these Zones, plus 2 Dermojet treatments of the reactive (pain) point on the ear, gave improvement in all cases and about 90% were clinically cured and remained sound for more than 1 year.
Abortion: Add the relevant Ting point, especially KI
Bone spavin: Add the relevant Ting point, especially ST, KI
Bronchitis/cough/lung disorders: Add the relevant Ting point, especially LU
Colic, acute: Add the relevant Ting point, especially LI, SI, KI, GB
Cracked heels arise when Channel blockage is present over a period. Use of Ting Points predictably cures cracked heels in 5-7 days, even in severe long-lasting cases, especially if LU or LI are involved (M.J.C).

Diarrhoea: Add the relevant Ting point, especially LI, SI, LV, SP, ST
Dust allergy: Add the relevant Ting point, especially LU, LI, TH
Flexor tendon strain: reactive Ting Zones especially from LI, PC, TH, KI, BL, HT, SI. The usual interval to clinical success was 1-35 days, (mean of 2 weeks) and most could resume full training in 3-6 weeks. In acute cases of tendovaginitis, training may be resumed in 1-2 weeks. Tendovaginitis: Add the relevant Ting point, especially TH, LI, SI
Food allergy: Add the relevant Ting point, especially LV
Headache (headpressing, headbanging, nodders): Add the relevant Ting point, especially GB, BL
Joint pain, arthritis, uncomplicated strains: all reactive Ting Zones
Lung bleeders: Add the relevant Ting point, especially LU
Male viciousness, hitter, biter: Add the relevant Ting point, especially SP, PC, KI
Overexertion: Add the relevant Ting point, especially HT, SI, LU
Polyarthritic shifting lameness: Add the relevant Ting point, especially HT, SI, TH
Pulls to one side (check atlas !): Add the relevant Ting point, especially LV, GB
Sexual/reproductive/Female infertility/Nymphomania: Add the relevant Ting point, especially HT, TH, KI, LV, PC
Skin: Add the relevant Ting point, especially LU, TH, SP, LV

Sole haemorrhage/trauma, soft horn: Add the relevant Ting point, especially LU, HT, SI
Tracheitis: Add the relevant Ting point, especially LI, LU
Tying-up syndrome: Add the relevant Ting point, especially LV, SP
Urticaria: Add the relevant Ting point, especially LV, LU
1.1 MUSCULOSKELETAL PROBLEMS
(Kothbauer; Westermayer; Jeffries; Hwang; Grady-Young; Kuussaari; White)
The paravertebral Shu are helpful diagnostic points to isolate Channel lameness. Once the Channel(s) are identified, all anatomical structures under or nearest to that Channel path are considered (and palpated). For example, the LI Channel passes through or near the intermediate and 3rd carpal bone, the inside shin, the osselet under the medial digital flexor tendon, the inside splint, anterior branch of suspensory ligament, shoulder bursa etc. In tenderness of BL25 (lumbar 4-5, large intestine Shu), the lameness may lie in those structures, if it is not due to primary strain of the lumbar area, or referred from the organ. Thus BL25 may relate to anterolateral forelimb lameness above the carpus or the anteromedial forelimb below the carpus. In such cases, apart from needling the affected Shu and other key points, one should balance the paired Channel of LI (LU) by needling BL13 (LU Shu).
Check for diagonal relationships. Forelimb lameness is often accompanied by AhShi (tenderness) at contralateral lumbosacral or hindlimb points (M.J.C). Also, hindlimb lameness is sometimes associated with AhShi points on the contralateral side of the neck.
Forelimb lameness: Add the relevant Ting point, especially LI, LU.
Hindlimb lameness: Add the relevant Ting point, especially SP, KI, LV.

Search for tender points in all local problems (neck, shoulder, elbow, back, thoracolumbar, lumbosacral, hip, stifle, laminitis etc). These are the Trigger Points (TPs), Pain Points, or AhShi Points. Check especially the paraspinal area (neck and interscapular area in forelimb problems; thoracolumbar and lumbosacral area in hindlimb problems).
Ovarian or uterine irritation in mares and fillies, may cause severe sporadic lameness due to referred pain (hindquarter, hunched or rigid back and, occasionally, forelimb lameness). This may occur in cystic ovary or at the time of ovulation if there is a lot of local haemorrhage. It is essential in such cases to check for AhShi points related to the ovary and uterus (see section 1.5 below).
Experts locate the Channel imbalances and choose points according to Five Phase Theory (Sheng and Ko Cycles) and the relevant Ting and/or Shu points. If the Command Points are dangerous to needle (too distal on the limbs or in other sensitive areas), they can be treated by painless methods (Laser, LACER etc). This minimises the number of needles and sessions needed. It also gives longer lasting results than the Cookbook method.
Use AhShi points, Local points, Region points. Consider points with potent actions: BL11 (bones & joints); BL40 (hindlimb & back); LI04 (forelimb & general effects); ST36 (hindlimb & general effects); ST44 (hindlimb); TH05 (forelimb); GB34 (hindlimb, muscles, tendons, neck, shoulder & elbow); GV03 (BaiHui) (hindlimb, lumbosacral area, general effects); BL23 (lumbosacral and hindlimb, adrenal point (all stress conditions), ovary/kidney/Vitamin D/parathyroid/bone point & general effects).
Problems of the back, sacral- and gluteal- area respond better and longer and need fewer sessions if AP is combined with spinal manipulative therapy (M.J.C).
Treat for 20 minutes, 2-4 times at intervals of 1-2 days (acute) or 3-7 days (chronic). White suggests electro-AP for 20 minutes, repeated every 12-24 hours in acute cases with severe pain or paralysis. Before using electro- AP, ensure that the horse has not had adverse electrical experience in the past (electric goad etc).

1.1.1. Soreback (thoracic, lumbar and sacral area) (Fig. 1)
(Cain; Kothbauer; Kuussaari; Klide; Grady-Young; Johnson; Rogers; White)
Search the back and paravertebral muscles for AhShi (tender) points. If the tail twitches during riding, this indicates AhShi at BL23 (kidney Shu). Use all AhShi points. Add BaiHui and points from BL18 (ICS 15) to BL26 (L5-L6) and BL28,30 (foramina S2,4) or points from BL17 (ICS 14) to BL25 (L4-L5) and BL27,29 (foramina S1,3). Use the more anterior points if the pain is more anterior. Consider also GV12; BL31,34,54 and the point at the meeting of the scapula and the anterior edge of the scapular cartilage (TH15 = TCVM PoChien).
Spinal and paravertebral muscle pain (cervical, thoracic, lumbar, sacral): Add the relevant Ting point, especially KI, GB, BL.
Lumbar weakness: Add the relevant Ting point, especially BL, KI, SI.
Treatment: injection, simple needling, electro-AP (20 seconds/needle) or Laser. Treat 1-2 times/week (usually every 5 days) for 2-10 times. In acute cases, with severe pain or paralysis, treat every 12-24 hours. Relapse within 6 months after successful treatment may be 5-50%.
1.1.2. Saddle-sore (Fig. 2)
(Cain; Grady-Young; Johnson; Rogers)
In all cases of "saddle-sore", check the design and fit of the saddle and the habits, skill, balance and of the usual rider. Advise on necessary correction of detected faults. Advise the use of high-quality saddle-pads (especially cellular, gel-filled saddle pads, for the first few weeks after treatment.
Pain, stiffness, rigidity in the area of the saddle, is treated as in 1.1.1, above. Tenderness near BL18 (liver Shu) may be associated with a muddy colour of the mucosa of the eye. (The liver controls the eye in TCVM).

Use AhShi points plus BL points, especially BL21,23,25. Add the relevant Ting point, especially ST, SP, GB, LV, HT, LU, as may be indicated by the findings of the AP examination.
Treatment: Inject procaine-B12 (9 ml 1% procaine + 1 ml B12; 3000 units/ml at each point), using 19g needle, depth 3-4 cm (or)
needle or electro-AP 20 minutes; 2/week; 2-4 times.
1.1.3. Shoulder lameness (Fig. 3)
(Cain; Kuussaari; Rogers; White)
Check for cervical subluxation, especially in the area C6 to T1. See the LI, SI and TH Channels (Appendix). Check TH16 (endocrine), BL22 (TH Shu, endocrine), BL27 (SI Shu), BL25 (LI Shu).
SI10, if still tender after proper Channel balancing, is diagnostic for LOCAL shoulder lameness (OCD). TH14 may be tender in shoulder lameness but true joint lameness (OCD) is rare. More often, the lameness is muscular, referred from subluxation of vertebrae C6-T1, via the brachiocephalicus m., attached to the humeroscapular joint. Painful shoulder or neck can cause spasm of that and other muscles and a choppy forward stride on the ipsilateral forelimb. If the problem is ovarian, treat BL22 (TH Shu) and the sensitivity at TH16 usually disappears. If the problem is shoulder lameness, treat TH14 and SI10, with BL22 and 27 (Shu of TH and SI). If the shoulder pain is referred from the neck, treat the neck, with vertebral adjustments, if needed (see 1.2.4).
The main points are: AhShi points located in the muscles of the neck, scapular, shoulder and paravertebral area, with points from BL11,22,27; GB21; TH05,14,15,16; LI15,17; SI09,10,13,17; LU01,01a; ST10.
Treatment: Electro-AP (10-20 seconds/point) or simple needling (20-30 minutes), 2-6 times (mean 3) at intervals of 3-7 days (mean 4). White suggests 20 minutes electro-AP every day in acute cases.

If the lameness is due to irreversible OCD, gold bead implants at ST10, LI17, SI09,10,13,17, BL22,27 can halt the progress of the condition. If done at 1-2 years of age, the result is very good: most can go on to full training and racing (M.J.C). Few cases relapse after successful treatment.
1.1.4. Elbow lameness (Fig. 4)
Lameness associated with AhShi points in the muscles behind the elbow is a good indication for AP. The points used are:
AhShi points in the area (check also the scapular and neck muscles)
Local points LI10,11,12; TH10; HT03; PC03; SI08
Region points (BL11; LI15; TH14; SI09 etc)
additional points from TH05; LI05
Treat by simple AP, electro-AP or point injection every 3-7 days for 1-3 times in recent cases and 3-8 times in chronic cases.
1.1.5. Hip and thigh lameness (Fig. 5)
(Cain; Rogers)
Hip and thigh lameness may be due to local muscle strain, hip arthritis, hip dysplasia or pain referred from the thoracolumbar area. Dysplasia is very common in horses. It is often misdiagnosed as stifle or hock lameness. In severe dysplasia, BL19,48 (GB Shu), GB29,30,31 are usually tender, making it possible to diagnose dysplasia pre-purchase (as in yearlings). Tenderness at all those points indicates a poor prognosis, even if the points are implanted. In mild cases, or in other cases of hip and thigh pain, needling those points gives very good results (M.J.C). In coxofemoral lameness of horses and dogs, insertion of gold beads towards the rim of the acetabulum (using a 16 g 30 mm needle) has powerful clinical effects, even though the beads are inches away from the acetabulum in horses.

Injection of irritant substances (such as copper compounds) over the sciatic nerve may cause sciatica with hip and thigh lameness (Rogers). BL25 may be tender in sciatica.
The points most effective on the hip and thigh are:
AhShi points in the thoracolumbar, sacral, hip-thigh and posterior thigh muscles.
Local points (GB29,30,31,32; BL30,36,37,38,54; ST31,32,33,34)
Region points (BaiHui; BL23,54)
Additional points from BL18,19,25,27,47,48, GB21,25a,34,39
Add the relevant Ting point, especially GB.
Treatment: as for elbow lameness.
1.1.6. Stifle and hock lameness (Fig. 6)
(Cain; Jeffries; Rogers)
Points BL36,36a,37 are diagnostic/therapeutic for the stifle. ST25a, at the lower, posterior edge of the tuber coxae (origin of tensor fascia lata) is also important. Add BL20,21, SP10, ST10 and point anterior to the origin of the biceps femoris (near BL35).
Tenderness at BL18,20,23 (LV, SP, KI) suggests inside stifle.
Tenderness at BL19,21,28 (GB, ST, BL) suggests outside stifle.
In stifle wear, Cain injects 10 ml Hypodermin (18g needle, 3 cm) towards BL40 in the intercondyloid fossa and adds SP09, ST36, GB34. Jeffries uses Sarapin (containing Vitamin B12 and C), 3 ml injected below the patella, medial and lateral to the patellar tendon at XiYan (Knee Eyes = ST35) and the point posteromedial to the patellar tendon; ST36 (12 ml); KI10 (5 ml); BL40 (4 ml, 5 cm deep).

In stifle lameness, point injection is excellent in 1-2 sessions. Walk the horse for 2 days before return to the track.
In hock lameness, tenderness at BL18,20 (LV, SP) can help to diagnose cunean tendon problems (inside hock). Tenderness at BL19,28 (GB, BL), and BL27 (SI Shu, Son of GB) can arise in curbs. Reactive GB can cause spasm of the biceps femoris muscle, resulting in hindlimb lameness.
In hock lameness, Local points (BL60, KI03) and BL30,35,53,38,39,40, ST36 (hock-related points) are used with reactive BL points (M.J.C). In bone spavin, add the relevant Ting point, especially ST, KI.
1.1.7. Laminitis, navicular disease, foot abscess (Fig. 7)
AP is successful in 80-90% of cases of laminitis in the short and longterm (Klide; Kuussaari). Acute cases respond faster than chronic cases. The most important points are FL21 and 22 (Klide and Kung's system). They are at the back of the hoof, at the medial and lateral cartilages (FL21) and in the centre of the hollow above the hoof (FL22).
Additional Local points are FL19 (two points on medial and lateral digital veins, dorsocaudal to fetlock) and FL20 (4-8 fen lateral to anterior of the coronet at the hoof-hair junction) (Klide).
Kuussaari also adds a point for the forelimb (behind the humerus in fossa between long and lateral heads of the triceps m. and the posterior edge of the deltoid m.).
Johnson also searches the paravertebral area. In laminitis and navicular disease, BL18 (liver Shu) and BL23 (kidney Shu) are often tender. Johnson adds these AhShi points and SI08 (forelimb) or BL40 (hindlimb). The veins (FL19) are bled only if there is heat in the coronary band. He may add BL11,12,13 as Region points in forelimb cases.
Cain punctures PC09 several times with a 16 gauge needle until the blood changes from tarry and dark to cherry red and normal viscosity.

He adds puncture of medial and lateral digital veins or other terminal points (LU11, LI01, ST45, SP01, HT09, SI01, BL67, KI01, PC09, TH01, GB44, LV01) with 18 or 20g needles. These points are at the coronary band. It is helpful to puncture the medial and lateral digital veins with 18 or 20g needle also.
Add the relevant Ting point, especially HT, SI.
Treatment: simple AP or electro-AP, 1-4 times (mean of 3 times) every 2-4 days (mean of 3 days) in recent cases (Kuussaari) or 1-12 times (mean of 6 times) every 3-7 days in chronic cases (Klide, Johnson). Use corrective shoeing, silicone pads and foot care to put pressure on the frog supplements the AP effect.
Laser on LI04; LU07 (10 seconds/session) may help AP treatment (Johnson).
Navicular disease is treated with similar points but success in navicular is not as well documented as in laminitis. One theory of navicular disease is that of poor blood supply to the area. Vasodilators and anticoagulants have been used in attempts to alleviate this. Vasodilation can follow AP at Local points but Region points, can help also:
Forelimb: LI11,15; TH05,14; SI09; BL11 etc
Hindlimb: GB30,34; ST36; BL40; BL23; BaiHui
Johnson claims excellent results in navicular disease. Treatment is to a maximum of 6 times in 3 weeks (some need less than this). He uses electro- AP, with 7-8 cm 26g needles. No twitch is necessary in most cases. Laser at LI04 and LU07 helps.
Foot abscess is treated as for laminitis or navicular disease (Johnson).
Hoof-bend bleeders, heelcracks, heel haemorrhage/sores: Add the relevant Ting point, especially TH (Thoresen).

1.1.8. Tendinitis, splints, curbs
(Cain)
Tendinitis and sheath inflammation may be helped by application of local Laser. Many veterinarians find that Laser is better than standard AP. Plum Blossom Needling has helped in problems of the superficial flexor tendons. Many cases of injury to the tendon sheath are misdiagnosed as tendon tears. Sheath injuries respond well to stimulation of Local and Channel points. Local circulation is enhanced. Intradermal or dermal needle implants, left in place for several days, help.
Magnets (500 gauss) with gold bead centres (CORIMAGS) may be glued on with Superglue. They are remarkably beneficial if used with Laser or AP.
Splints (especially inside) respond very well when the affected Channels are balanced. Inside splints are usually related to the ipsilateral stifle. The Channels LU, SP are those primarily involved, with LI and ST as secondary.
Curbs respond well to local therapy when the affected Channels (GB, LV) are balanced.
1.1.9. Azoturia, tying-up syndrome
(Cain)
Azoturia often accompanies the tying-up syndrome. CPK, SGOT levels usually are elevated in blood. The syndrome occurs especially in spring (season of Wood, GB-LV). It is a common racetrack problem and responds very well if GB-LV, SP-ST, KI-BL can be balanced. These are Wood, Earth, Water in the Five Phase Cycle. See the Sheng and Ko Cycles in classical AP. See section 1.0 and the Appendix.

1.2. NEUROLOGICAL PROBLEMS
1.2.1. Peripheral nerve paralysis (Fig. 8)
AP is of no real use in paralysis due to spinal transection, motor neuron
degeneration (German Shepherd syndrome) or severe damage to motor centres in the brain. It can accelerate recovery in paralysis with radiculopathy due to soft tissue inflammation or in CVA cases where paralysis is due mainly to vasospastic ischaemia of the motor centres. It helps to establish a cross-spinal reflex arc, which can be important in the salvage of a horse with traumatic "Wobbler Syndrome".
Peripheral nerve paralysis, especially that following trauma, also can be
helped by AP. The points are usually along the course of the affected nerve but points are often stimulated on the normal side also.
In brain or spinal paralysis in humans (such as arm paralysis after cerebrovascular accident or leg paralysis after polio), a chain of points along the nerve is used. For example, sciatic nerve:BL31,35,36,36a,37,38,40,57,60; GB30,31,34,39. Add BL19 (GB) and BL28 (BL) to balance Channels if GB and BL points are used. Add ST10 and BL21 if ST points are used.
In paralysis, electro-AP is better than simple needling but great care is needed to avoid electrical burns or electrolytic lesions in areas with sensory paralysis. Alternatively, inject the points with homoeopathic acid substances (ascorbic acid or HCl 9c). If definite improvement is not seen by 10 sessions, further AP is unlikely to be helpful.
1.2.2. Radial paralysis (Fig. 8)
(Cain; Hwang; Grady-Young; White)

Expect 90% success if recent case; 50-70% if paralysis is more than 2 weeks old. Use local AhShi points. Add points from LI04,10,11,15; LU01,01a, SI08,10; TH10,14 bilateral. Add BL27,22,13,25 respectively to balance the Channels if SI, TH, LU, LI points are used (M.J.C).
White suggests electro-AP for 30 minutes every day in acute cases. Others would treat every 3-7 days in chronic cases.
1.2.3. Facial paralysis (Fig. 8)
Points such as ST02-06; CV24; GV26; LI20 are used, depending on the nerve affected. In TCVM, the classic points are: SouKou; KaiGuan; BaoSai; FuTu. HouMen and HouYu on the neck (see White 1985) may be added to these. Add BL21 and BL25 to balance ST and LI points, if these are used (M.J.C).
1.2.4. Cervical ataxia (the Wobbler Syndrome) (Fig. 9)
(Cain; Jeffries; Rogers)
Early cases of ataxia in young horses can be helped or cured completely by AP. It is one of the most rewarding applications of AP therapy. Wobblers respond better and longer and need fewer sessions if AP is combined with spinal manipulative therapy (M.J.C). Adjustment of the neck vertebrae must accompany AP therapy for good success. Using adjustment and AP, Cain has restored to normal competitive ability many horses which had been sanctioned by insurance companies to be destroyed. In some cases, especially congenital and OCD cases, the ataxia was not fully cured but 90% of these were suitable for breeding, provided there was no history of genetic transmission. Jeffries has had similar success. Longstanding cases, with severe articular damage, have a poor prognosis.
Clinical experience in hundreds of cases suggests that 80% of cases are due to mechanical causes. A further 10-15% are genetically programmed. Gradual onset may be due to nutritional disorders, but these are rare.

The condition usually arises suddenly (overnight), due to trauma (a fall; being pulled up roughly by the training-rope; tie chains; being cast in the box). The earlier the case is treated, the better the success rate. Cure is impossible if the motor neurons are degenerated.
The signs include ataxia (especially of the hindlimbs), inability to turn sharply or to back-up properly (the horse may fall over if forced to do these movements). Some cases show obvious restriction of neck movement. The limbs (especially hind) may be placed heavily, as if the horse does not know when they should make contact with the ground. In milder cases or in cases of spontaneous improvement (rare !), the only signs may be slight awkwardness or restricted ability to turn sharply, (excessive abduction of the hindlimb on turning), toeing of the ground at the walk or turn and heavy placement of the hindlimbs.
There is usually, if not always, vertebral misalignment with consequent pressure on cervical nerves or compression of the spinal cord. The primary sites are at C5, C6, C7, T1, atlas, C2, C3. Rear ataxia relates to an autonomic reflex arc from the C6 sympathetic ganglion. This affects the whole sympathetic chain to the lumbar plexus. Vertebral adjustments must be made to ensure integrity of the cord and nerves. A successful adjustment is confirmed when the horse gives a good "wet dog shake". If this does not occur, the adjustment is not successful. In long-lasting cases, AP must be done first to release the spasticity of the intervertebral muscles and ligaments.
Wobblers are treated similarly to cases of cervical syndrome in humans, with symptomatic treatment for hindlimb problems in the later stages. The initial results can be very dramatic, with marked improvement after 1-3 sessions. However, full cure (full coordination and total elimination of all signs) may take up to 30 sessions. Thus, treatment of wobblers may be impractical on economic grounds except for valuable bloodstock or loved pets.
GB20 and 21 are essential in treating wobblers and neck pain. GB20 can be injured easily by bad riders and by tie-chains in stalls. This can cause subluxation of the atlas, requiring chiropractic adjustment. AP alone, in such cases, gives poor or only temporary relief.
Cervical problems involve one or more of the Yang Channels of the forelimb (LI, TH, SI) or hindlimb (ST, GB, BL) or the GV Channel (see the Appendix below). Check the Shu points of all the Yang Channels and check for AhShi on the GV line. As most of the Yang Channels

are involved, careful Five Phase balancing is necessary for full athletic recovery (see section 1.0 above and the Appendix).
A careful search is made for AhShi points (neck, paravertebral, especially thoracolumbar and sacral area). All AhShi points are used. They are often absent in Wobblers.
Points for Neck and Forelimb weakness:
JiuWei; GB20,21; TH14,16; BL11; LI16,17; ST10; GV10,11,12 (withers)
emergence points of dorsal cervical nerves;
emergence of 2nd cervical nerve (SI17);
emergence of spinal accessory nerve;
Additional points: BL13,19,21,22,23,25,27,28; GV00 (tip of the tail), GV03 (BaiHui),04,
Points for Hindlimb weakness: BL29 (or 30); GB30,31,32,34,39; BL40
These points relate to the deep musculature of the neck, nuchal ligament, supraspinous ligament, lumbosacral plexus and sacral plexus.
In horses under 3 years old, AP and adjustment is combined with Adequan i/m (2 vials initially, 2 at 5 days and 2 at 2 weeks later). If used before 3 years of age, this helps to promote healing of any cartilaginous damage.
Treatment: Simple AP (20 minutes) or electro-AP (20 minutes) every 3-7 days for 4-30 times, as needed. Advise exercise on short and long rope (left and right turning), backing exercise, neck exercise (using carrot to persuade horse to do lateral and vertical movements).
If improvement is noted, allow 3-4 weeks between courses of 3-5 sessions of AP. Full cure may take up to 12 months.

Cain and Jeffries use point injection of the AhShi points plus points on the BL, GB, LV, ST, SP Channels (the hindlimb Channels), as indicated by tenderness at the Shu points for these Channels. Once improvement occurs, point stapling can be used for longterm stimulation (up to 12 months) and to reduce the number of visits needed (Jeffries). Cain usually injects the points with homoeopathic NaOH 10c and uses LACER (light stimulation) in horses over 3 years old.
Rogers' experience with wobblers (4 cases, AP but no adjustment) was that two were destroyed within 18 months. AP did not help sufficiently to ensure the jockey's safety in competitive racing, although it did improve the coordination markedly (Case 1) and completely but with relapse in Case 2. Case 3 was a foal which responded very well. Case 4 was a yearling which responded well to two sessions but was not presented for further treatment, owing to the death of the owner. One year later, the horse was OK.
1.3. GASTROINTESTINAL PROBLEMS (Fig. 10)
AP can help in many g/i/t problems, including diarrhoea, constipation, indigestion, colic, windsucking, gastritis, enteritis etc. When AP is accompanied with Herbal Medicine, success rates are higher and last longer (M.J.C).
The most important points for g/i/t problems in the horse are on the BL and GV Channels (area T11-S4). The more anterior points are mainly for LV, SP, ST problems. Intestinal problems are treated mainly by points in the area T18-S4. Rectal problems relate to the sacral points, such as BL29,30,33,34.
In TCVM, GuanYuanShu is placed about 2 hands from the GV line, just behind the last rib. This point is most important in gastric and intestinal problems, including colic and windsucking. It is in the position of BL50 in the transposition system, lateral to BL21 (the Shu point of the stomach). Human GuanYuanShu (BL26) is between the transverse processes of L5-L6. It (with BL25) relates to uterus and large intestine in humans.
1.3.1. Colic (Fig. 11)
(Cain; Kuussaari; Kothbauer; White)

AP can give 100% success to a single treatment in acute cases of sand colic and gas colic (but not in surgical cases). It is useful in intestinal distension also.
AP can be by simple needling (20 minutes) or by electro-AP (20 minutes). Cain gives strong, repeated stimulation to all points except GV26. That point should not be overstimulated in conscious animals, as it may cause shock.
The important points are: BL50 (2 hands from GV line, behind last rib); CV12 (midway navel to xiphoid, on ventral midline). To these may be added three points behind BL50, level with vertebrae L3,4,5 (Kothbauer's BL51-1,51-2,51-3 (old 46-1,46-2 and 46-3)), SP21,21a, LI17, BL20,21,25,27, GV01, ST36, GB25a, GV26, ST02.
1.3.2. Windsucking, crib-biting (Fig. 12)
Horses which suck wind and are cribbers usually have chronic digestive problems, especially chronic or mild gastritis (Kuussaari). They may show colic, tympany and flatulence. Successful treatment of the digestive disorder is associated with disappearance of windsucking in 67% of cases but longterm success in crib-biters is much less (29%) (Kuussaari). Workers at Tuft's University have shown that windsucking and cribbing causes endorphin release, similar to "runners' high". They have been able to control cribbing by injecting naloxone.
The important points are BL50; PiShu; WeiShu; AnHua; SanChuan; ChiChia (GV12).
Treatment: simple AP (20-30 minutes) or electro-AP (20 seconds/point) for 2-6 times (mean of 3), at intervals of 2-5 days (mean of 4 days) (Kuussaari). White (1985) gives two new points on the upper and lower ends of the brachiocephalic muscle (YINQI 1 and 2) for this condition.
Treatment by strong electro-AP every 12-24 hours for 0.5-4 hours/time, on 9-29 occasions was said to be successful. Relapse was

predicted unless a muzzle was used and the feed-pot lowered to the ground.
Thus, at present, Kuussaari's points seem to be a better combination.
1.3.3. Gastric ulcer, diarrhoea
P.A.M.R. treated 2 suckling foals with gastric ulcer and 3 adult horses with chronic idiopathic diarrhoea. The important points are BL20,21,25,27; GV03; ST36; PC06; AhShi points in the paravertebral area.
Treatment: electro-AP (20 minutes) for 2-5 times (mean of 3), at intervals of 7 days. Success: 2/2 foals recovered within days (2 sessions) but only 1/3 adults recovered within 2 weeks (3-5 sessions).
1.4. RESPIRATORY PROBLEMS (Fig. 13)
See the LU and SP Channels in the Appendix. Despite textbook claims and reports from some clinicians, Kothbauer and Kuussaari had poor success with AP in equine respiratory conditions. When AP is accompanied with Herbal Medicine, success rates are higher and last longer in respiratory disorders (bleeders etc)- (M.J.C)
Important points for upper respiratory problems are in the area of the trachea (CV22,23; ST09,10; GV14,15 etc) or nose (LI20; YinTang; GV26 etc).
Important points for lower respiratory conditions are the BL and GV points in the area T3-T10 (BL13-17,42-46; GV09-12 ) and points in the intercostal spaces (ICSs) over the lung area.
1.4.1. Bronchospasm, heaves, bronchitis (Fig. 14)

The late Drs. Grady-Young and Westermayer reported good success (50-85%) in early cases of heaves (before alveolar rupture occurs). AhShi points in the lung area were used. BL13 and 43 were usually tender. Points were selected from: BL13,14,15,42,43,44; LU01,01a,07,09; PC06; KI10,27; ST19; GV14,17,19,20; HT01; LI04,20; ST36,45; TH01 (depending on other signs).
Treatment: simple AP, 15-20 minutes at intervals of 3-7 days for 4-8 times. Success depends on the seriousness of the pathology.
Grady-Young used Laser on the Shu points for the lung and on other points in the lung reflex area (behind the scapula) in Pasteurella pneumonia in cattle. He reported good success. He also suggested its use in respiratory conditions in horses but gave no statistics of its success.
1.4.2. Bleeders, lung haemorrhage, epistaxis (Fig. 15)
The diagnostic and therapeutic success of AP in bleeders is excellent (Cain; Jeffries). A history of sudden fading in a race, together with tenderness at the Shu and other reflex points for lung (below the posterior edge of the scapula and behind the scapular cartilage in the area of BL17, BL42-46 and GV09) indicates lung or nose bleeder in 95% of cases. The SP Channel points (BL20 (SP Shu), SP21,21a) are always tender in bleeders.
If vertebrae C1-T8 are intact (normal neck movement and no AhShi in the neck and anterior withers area), sensitivity along the outer BL line (BL42-46 (old BL37-41) from T8 through T14, together with sensitivity at BL13 and 20 suggests a lung bleeder. Bleeding usually occurs in the right lung, thus the right side is usually sensitive, especially on BL42-46, although left BL13 and 20 (Mother of LU) are also tender. These points are diagnostic for lung bleeders, even when endoscopic examination may be negative. There is evidence that Bleeding may be transmitted genetically. One of Cain's mares had 5 bleeders. Such mares should not be bred. However, 80-85% of non-genetically determined bleeders in Cain's practice do so because of abuse of drugs (banamine, phenylbutazone, aspirin, androgenic anabolics etc) or due to stress (pain from any source causing hypertension).
Identify and balance all affected Channels; stimulate the lung (BL13) and its Mother (BL20, SP Shu). This is the best treatment. The points

used are the AhShi points and TianPing; BaiHui and two other GV points between these points. AhShi points may be injected with 2 ml of Vitamin B12 + C solution and 1 ml in the GV points. BL17 (diaphragm and haemorrhage point) is especially good in haemorrhage, anaemia and blood diseases. BL17 and 18 (liver Shu) influence liver function also and may improve prothrombin formation and blood clot formation. Herbs to strengthen the Qi of LU and SP help also. These methods are not effective in genetically affected cases.
The therapeutic success can reach 90% if AP is given 4-24 hours before the race (Jeffries).
1.4.3. Rhinitis, sinusitis (Fig. 16)
Grady-Young claimed c. 95% success with simple AP or Laser. Treatment was 20 minutes, 3-5 times, every 3-4 days. The points are chosen from CV23; GV25; SP21; LV13; BL18; GB25; ST09; SI16 and AhShi points over the lung and chest area. Other Local points (YinTang; TaiYang, LI20; GV26; ST02,03 etc) can be used also.
1.5. REPRODUCTIVE PROBLEMS (Fig. 17)
The Channels most often involved in reproductive problems are SP, KI, TH. Their Shu points are BL20,23,22 respectively. Their Mu points are LV13, GB24, CV05. There is also an ovary point in the paralumbar fossa and point TH16 (endocrine) is a useful distant point. Local points include WeiKen (GV02), BaiHui (GV03), MingMen (GV04), BL51,28,35. Occasionally BL14 (PC Shu) and the GV point in between may be tender in breeding problems. Sensitivity at TH16 usually disappears when BL22 (TH Shu, endocrine) is treated (M.J.C).
The most important points for reproductive disorders and for the genital organs are in the lumbosacral area. A simple guide is to imagine the female organs (ovary to vulva) as a straight tube. The ovaries relate to APs in the area T18-L3 (points such as BL21,22,23,50,51,52; TianPing; GV05,04). The vulva/anus/perinaeum relate to the area from S3 to the tailhead (points such as BL29,30,33,34,35,54; GV01,02). The other organs (tubes, uterine horn, uterine body, cervix, vagina) relate to intermediate points.

Kothbauer recommends BL22,23,52; GV04 for the ovary and BL27,28,31; BaiHui; CV06 for the uterus. Johnson reports excellent results with these points in cases of uterine atony, metritis, embryonic reabsorption etc.
If one had to remember 4 points for reproductive/genital disorders, they should be: BL23 (between transverse wings of L2-L3) for the ovary; BL26 (between transverse wings of L5-L6) for the uterus; BaiHui (lumbosacral space) for the cervix and BL28 (lateral to sacral foramen 2) for the vagina/bladder.
There are other points (Fig. 18). The abdominal Channels include ST, SP, BL, KI, GB, LV, CV, GV. Local points (points nearest the target organs) on ANY of these Channels influence the organs. Although most importance is attached to the GV and BL points (lumbosacral area), GB26-28 (paralumbar fossa and under the external angle of the ilium) are sometimes tender in mares with ovarian problems, especially cysts. Points over the iliac wing (between the tuber coxae and the iliac crest) may also be tender in uterine disorders.
In disorders of the reproductive system and genitalia, (as in all other clinical uses of AP !) Treat the AhShi (tender) points. A few points (whether tender or not) for the affected organ may be added and CV02,03,04; BL54; LV02 may be considered as additional points. SP06 is regarded as a point with special action on the inguinal area, genitalia and reproductive function of males and females.
Westermayer suggested treatment for 20-30 minutes for 2-4 times (mean of 3), at intervals of 5 days.
1.5.1. Anoestrus (Fig. 9)
(Cain; Kuussaari; Hwang; Grady-Young; Johnson; White)
See section 1.5.
In anoestrus mares, points in the area L3-S4 (BL23-34; BL52-54), points along the KI Channel and SP06 are palpated for tenderness. AhShi (tender) points are treated. Other points in anoestrus include: BL22,23; SP6; YanChi; YungChi; BaiHui; XieQi; CV01,05,08; GV01.

Treatment: 20-30 minutes simple AP (deep needling to reach the broad ligament in the posterior lumbar points), or electro-AP (20 seconds/point or 20-30 minutes/time). Moxa may be combined with simple AP (Hwang; Johnson). Moxa should not be used where there are inflammable materials (straw bedding etc in stalls, barns etc). Always consider fire hazard before moxa is used. Laser was also good (Grady-Young).
Kuussaari: Treat 1-5 times (mean 2 times) at intervals of 2-5 days (mean 3 days).
Hwang: Treat with needle + moxa for 10 minutes for 5-10 times at intervals of 1-2 days and expect oestrus within 2 weeks.
Grady-Young: Laser (20 minutes total to do all points) 3-8 times at intervals of 3-4 days. Mares cycled after session 6 (after 3 weeks).
Johnson: Needle + moxa (20 minutes) on 10 cm, 20 gauge needles. Inject BL40 and Laser SP06; ST36 and (sometimes) BL11.
White: BaiHui (8-10 cm deep); YanChi (18-23 cm deep); GV01 (20-25 cm deep; needle directed forwards and up to lie under the sacrum). Electro-AP, 20-30 minutes, 1-3 times at intervals of 2 days.
1.5.2. Cystic ovary (Fig. 20)
(Cain; Jeffries; Grady-Young; Johnson)
See section 1.5.
Luteal cysts often are associated with metritis or pyometra. They may be expressed manually (per rectum) in many cases (Grady-Young). Follicular cysts are usually associated with nymphomania. Cystic ovaries often cause neck and shoulder lameness and thoracolumbar lameness on the same side (M.J.C). See the TH, GB and LV Channels (Appendix). If BL22 is tender, check TH16.
Points in area L2-S1 (BL22-27,51,52; GV04) and in the para-lumbar fossa and under the tuber coxae (GB26,27,28) are examined for tenderness. Check BL18,19 (LV Shu and GB Shu) also and TH16
(endocrine point). All AhShi (tender) points are used. Other points are chosen from: BL22-29; SP06,15; LV14; GB25,25a; ST36; BaiHui; YanChi.
Jeffries and Johnson also inject 10 ml of 2% procaine solution into the broad ligament on each side of the cervix, using a special 50-60 cm needle. This method was successfully used in cows by Kothbauer and Greiff for many years. It is called paracervical injection or neural therapy.
Treatment: Simple AP; injection of homoeopathic NaOH 9d solution + Vit B12 and Ascorbic acid; Laser. The choice is individual preference.
Jeffries: Injection method plus paracervical injection, 2 times. Success is 5-15% better in luteal cysts than in follicular cysts.
Grady-Young: Laser (20 minutes total to do all points) 3-5 times at interval of 3-4 days. Skip 3 oestrus periods before breeding.
Johnson: Needle + moxa (20 minutes) on 10 cm, 20 gauge needles. Inject BL40 and Laser SP06; ST36 and (sometimes) BL11.
1.5.3. Repeat breeders (Fig. 21)
(Cain; Jeffries; Grady-Young; Johnson; Rogers; White)
See section 1.5.
In the investigation and treatment of repeaters, it is assumed that the stallion has been examined and been found to be fertile, potent and that ejaculation is normal.
Repeating may be due to ovarian disease, failure of the ovum to reach the uterus (salpingitis etc), failure to implant (metritis etc) or early death of the embryo.

The lumbosacral area and the paralumbar fossa area are examined for AhShi points, as above. All AhShi points are used. It is not possible to give just one prescription for repeaters, as the cause and the organs involved differ as described. The general principle is: AhShi points + points for the affected organ(s) or function(s).
Thus a selection must be made from points such as: BaiHui; YanChi; BL22-34,51-54,58; GB25,25a,26-28; GV01,02,04; SP06; KI06; LV03; CV02-06 etc.
Treatment: Simple AP; injection of homoeopathic NaOH 9d solution + Vit B12 and Ascorbic acid; Laser. The choice is individual preference.
Jeffries: Treat as for ovarian cysts.
Grady-Young: Laser (20 minutes total to do all points) 3-8 times at intervals of 3-4 days.
Johnson: needle + moxa (20 minutes) on 10 cm, 20 gauge needles. Inject BL40 and Laser SP06; ST36 and (sometimes) BL11
White: Electro-AP, 20-30 minutes, 1-3 times at GV01,04; BaiHui; YanChi; BL24
1.5.4. Reproductive problems in stallions (Fig. 22)
(Cain; Johnson)
See section 1.5.
Male disorders (oligospermia, libido loss, reluctance to mount or pain on mounting) can be treated successfully by AP in the stallion and the bull (Kothbauer).
Testicle points correspond with ovary points (see embryology of kidney, testis, ovary). The main points are BL21,22,23,50,51,52; TianPing; GV04,05 and SP06.

Penis points correspond with vagina points (see embryology of these organs). The main penis points are BL29,30,33,34,35,54; GV01,02 and SP06.
The principles of selecting points in male disorders are the same as in the female:
: AhShi points in area L2-S4 and in the paralumbar fossa, iliac area
: points for the affected organ(s) and functions.
1.6. OTHER CLINICAL USES
1.6.1. Anxiety, nervousness, especially in filly (Fig. 23)
Cain found that extremely nervous, "freaked-out" horses may become somnambulistic and impossible to needle because all points become sensitive (flight of fight syndrome). These horses quieten down when injected with 3 ml naloxone solution. They can be needled successfully then (see section 1.3.2).
The main Channels for nervousness are the HT and PC (Fire) Channels. Key points are BL15,14,22; PC06 (M.J.C). SI18 and TH17 are tranquillizer points.
Gold bead implants (using a 16 gauge, 3.5 cm needle) in BL14,15,43,44; LI17; SP21 and CV17 give good results (M.J.C). He used 2 beads/point. The beads were inserted under local anaesthesia or sedation and are left in situ permanently.
Sweating, nervousness: Add the relevant Ting point, especially PC.
1.6.2. Skin problems
(Cain)

The skin is Metal (LU, LI). Skin problems are more common in late autumn (Metal) and late winter (Water, KI-BL). Excess activity in TH (Fire) can weaken LU (Metal) (via the Ko Cycle). This manifests as poor hair coat (LU controls skin). Balancing LU, TH and KI enhances local treatment remarkably.
CONCLUSIONS
The main methods of stimulating the AP response in horses are point injection (very fast), or simple needling or electroneedling for 20 minutes.
Classical AP gives better and more longlasting results than Cookbook AP, especially in complicated cases. Cookbook AP is useful for beginners and can give good or excellent results in simple cases but beginners are advised to study AP in depth to get the best results. This is not as difficult as it might seem. The classical concepts can be learned from AP courses, such as those given by IVAS.
Point selection for local problems includes the relevant Ting Point(s), plus AhShi (tender) points which remain after that. Other points include: Local points, Region points, points with special or generalised action and (most of all) the paravertebral Shu point(s) for affected organ(s) or function(s). This includes the use of Shu points in superficial problems which may not have direct organic involvement. For example, BL13 and 25 (Shu points for the LU and LI Channels) are indicated as part of a prescription to help resolve pain of an inside forelimb splint (in the Channel area of LU and LI). Similarly, BL23,28 (Shu of KI and BL) are indicated in capped hock (Channel area of KI and BL). One or two distant points on a Channel passing through the problem area, or a chain of points along an affected nerve also help.
Some key points are:
BL11,23 bones, joints;
BL13,43 lung;
BL18, GV09 liver;
BL23, BaiHui adrenal, urogenital, hindquarter;
BL25, BaiHui hindgut;

GB20,21 neck;
GB34, TH15 muscles;
LI11, GV14, ST36 immunostimulation.
ST36, BL21 stomach and appetite;
TH15, GB21 forequarter;
A high clinical success rate can be attained in 1-3 sessions at 1-3 day intervals (recent or acute cases) or in 1-10 sessions at 4-7 day intervals in longstanding or chronic cases. However, beginners should study the principles of AP before attempting to use the system.
Treatment effects last longer when Ting points are used. This has been found to be essential in therapy of long-lasting or chronic cases.
There are other methods of point selection (earpoints, hoof points etc) and of point stimulation (magnets, staples, implants, Dermojet, Laser etc) but these methods must be regarded as experimental until adequate documentation and comparative clinical trials are available.
See the Appendix for point locations and references.
TRADITIONAL VERSUS TRANSPOSITION SYSTEM OF AP IN HORSES
Traditional Chinese Veterinary Medicine (TCVM) includes herbal medicine and acupuncture (AP). The TCVM system of AP concentrates on the location and uses (diagnostic and therapeutic) of isolated AP points (APs). TCVM does not show a Channel system in animals. Its concepts of diagnosis and therapy are very difficult for westerners to master.
Texts on the TCVM system in horses are scarce. They include those by Hwang, Klide & Kung, Kothbauer, Lin, White and the late Erwin Westermayer. Readers are referred to those texts for details.

The human AP system is based on Channel concepts. It is much better integrated than the TCVM system. Therefore, it is much easier to learn. Once the human system is mastered, its principles can be applied in animals by transposing the anatomical location and functions of the human AP point system to animals. This transposition system is very useful in the horse, especially in painful local conditions. The greatest difficulty is in locating points below the carpus or tarsus. It may be better to use TCVM points in these areas. The TCVM system differs from the transposition system in some respects but the two systems are basically very similar and either may be used alone or they may be combined.
Cookbook prescriptions for common conditions, body organs and parts in humans are listed in Appendices 1-3 of the paper on "Choice of points for particular conditions" (Rogers 1996). Those prescriptions may be applied in the horse although they are extracted from texts on humans.
The horse has no gallbladder but some GB points have important local uses. These codes are the same as those used in the Cookbook prescriptions, as mentioned above.
In this paper, the transposition system is used mainly, except for some TCVM points, which are described below.
1. TCVM POINTS IN THE HORSE
See the texts, listed at the end of the Appendix, for a complete list of names, locations and uses of TCVM points.
The following are a few of the TCVM points mentioned in the paper:
AnHua between spines of T8-T9
BaoSai in jaw muscles behind last molar
ChiChia between spines of T3-T4 (= GV12)
ZhongFu LU01 in some texts: behind shoulder joint in 2nd intercostal space (ICS 2). AP analgesia point with TH08.

FuTu behind occipital protuberance
XieQi 2 cun lateral to root of tail, in bicipital groove
JiuWei 9 points on the upper lateral neck. Point 1 is 6.5 cm behind the base of the ear, 4 cm from the mane (Fig. 7). Point 9 is 4 cm anterior to scapula, 6 cm from the mane. The other points are at equal intervals between these points
KaiGuan in jaw muscles behind molar 3
BaiHui lumbosacral space (GV03)
PiShu 1 hand from GV line in 3rd last ICS
SanChuan between spines of T4-T5
SouKou behind oral canthus
TianPing thoracolumbar space
WeiShu 3 spaces in front of PiShu
YanChi one third distance from tuber coxae to dorsal midline
YinTang midline of forehead, between the eyes
YungChi between the free ends of the transverse processes of L5-L6
FL 2 PoChien at anterior junction of scapula and its cartilage (TH15)
FL 4 PoLan one third distance down anterior edge of scapula
FL 7 ChangFeng 5 cun post. inf. to shoulder joint point in fossa between long and lateral heads of triceps m., behind humerus, at anterior edge of deltoid m. (LI13)
FL12 JianYu hole below upper head of humerus at its anterior edge
FL13 JianWaiShu Just behind and below shoulder joint
FL19 ChanWan on lat. and med. digital veins dorsoposterior to fetlocks
FL20 TiMen midpoint of med. and lat. cartilages at back of hoof. Needle from behind.
FL21 TiMen midpoint of lat. and med. cartilages at back of hoof. Needle from behind.
FL22 ChienChiu centre of pit in hollow above back of hoof

2. TRANSPOSITION SYSTEM
At this time there is no International Standard Chart to show the location of the Channel points (LU, LI, ST, SP, HT, SI, BL, KI, PC, TH, GB, LV, CV, GV) in horses. To locate the Channel points in horses, one can transpose the locations of human points to similar anatomical locations in the horse.
Figures 1-26 respectively show the approximate locations of the equine Channel points. These charts must be taken as provisional. They are for teaching purposes only, as they may help the beginner to locate the more important areas for treatment, especially if using Cookbook Prescriptions (Appendix 1-3 in Rogers 1996) or the points recommended for the conditions discussed in the clinical part of this paper.
From extensive clinical experience in equine AP, MJC made many corrections to earlier charts prepared by PAMR. MJC's locations are often (but not always) similar to those of other experts (Giniaux, Kothbauer; Westermayer etc). Emiel van den Bosch DVM, G. van Heuvelstraat, Ramsel, Belgium (Fax: 32-1656-1374) published very fine charts (Acupuncture Points and Meridians in the Horse, 1995). We recommend those charts to equine acupuncturists.
Location of GV and BL points in the thoracic area must take 18 pairs of ribs into account. Apart from the rib area, transposition of other GV points (GV01-04, 14-28) and BL points (BL01-12, 36-40 (old BL50-54) and 55-60) are similar to human positions:
GV01 Midline between anus and coccyx (as in human)
GV02 Dorsal midline in sacrococcygeal space (as in human)
GV 03 (BaiHui) in midline in lumbosacral space (L4-L5 space in human)
GV04 (MingMen) in midline in L2-L3 space, between left and right BL23 (KI Shu) (as in human). Some equine vets put it between left and right BL23a, in L3-L4 space.
GV 05 Dorsal midline in L1-L2 space (as in human), between left and right BL22 (TH Shu)
GV06-10 are located by counting 2 spaces for each point forward from GV05 (below spine of L1), with GV10 below spine T10

GV06 (TianPing): Dorsal midline behind the dorsal spine of T18 (thoracolumbar) space, between left and right BL21 (ST Shu)
GV07 Dorsal midline, 2 spaces before GV06 (behind spine of T16), between left and right BL19 (GB Shu)
GV08 Dorsal midline, 2 spaces before GV07 (behind spine of T14)
GV09 Dorsal midline, 2 spaces before GV08 (behind spine of T12), between left and right BL17 (Diaphragm, Haemorrhage, Blood point)
GV10 Dorsal midline, 2 spaces before GV09 (behind spine of T10), between left and right BL15
GV11-12 are found by counting 3 spaces/point forward from GV10 or backward fromGV13.
GV11 Dorsal midline, 3 spaces behind GV12 (behind spine of T7)
GV12 Dorsal midline, 3 spaces behind GV13 (behind spine of T4), between left and right BL12
GV 13 Dorsal midline in T1-T2 space (as in human)
GV14 Dorsal midline in C7-T1 space (as in human)
GV15-28 as in human
The Shu points (Organ-associated points or paravertebral reflex points) run parallel to the GV line, in humans about 1.5 inches and in horses about 1 hand from the GV line. They are covered under the BL Channel (see below).
The Mu (Abdominal Alarm) points are used in diagnosis and therapy in humans and small animals. The Mu points are: Lung = LU01,01a; Colon, large intestine = ST25; Stomach = CV12; Spleen-Pancreas = LV13; Heart = CV14; Small Intestine = CV04; Bladder = CV03; Kidney = GB25,25a; Pericardium, Heart Constrictor = CV17; Triple Heater = CV05; Gallbladder = GB24; Liver = LV14. Because of the danger to the operator, CV03,04,05 and ST25 are seldom needled in horses but CV12,14,17, GB24,25, LV13,14, LU01,01a are relatively easy to needle. Horses tolerate Shiatsu (deep massage) of awkward points and this can be very useful.
LV13,14 (Mu points of SP, LV) are very powerful points for balancing the Yin Channels, especially when coupled with SP21,21a (linking point for all Yin Channels, the Luo point for all Luo points).

T8 and L4: LU & LI Channels (Metal) (FIGURES 1 & 2)
LU (Lung) and LI (Large Intestine, Colon) are related in Metal. When Shu point tenderness or clinical signs indicate Channel imbalance, treat the Shu point and the Shu of the paired Channel. LU Shu is BL13,42 and LI Shu is BL25. LU Mu is LU01,01a and LI Mu is ST25.
When treating LU problems, the Mother (SP) Channel must be balanced and stimulated (BL20) and the Son (KI) Channel must be assessed (BL23) and treated, if needed.
When treating LI problems, the Mother (ST) Channel must be balanced and stimulated (BL21) and the Son (BL) Channel must be assessed (BL28) and treated, if needed.
Metal may be used to support weakness of Water. Thus, BL13 (LU) may help weak KI and BL25 (LI) may help weak BL.
The LU Channel runs from the lung to the anterior edge of the lower third of the scapula (LU01a), level with the base of T1 (M.J.C), to just lateral to the biceps tendon (05). It then runs down the anteromedial edge of the radius (06,07,08) and carpus (09), down the inner splint to the medial sesamoid (10) and medial heel (LU11). Internal branches go to the colon.
Traditional texts place LU01 in ICS 2, just behind the shoulder joint.
BL13,42 (LU Shu) may show acute tenderness with inside forelimb splints, check ligament, inside carpal, inside suspensory and sesamoid problems. They (and BL42-46) are usually tender in acute respiratory problems (see 1.4.2).
LU01,01a relates to the inside forelimb and carpus.

The LI Channel runs from the centre of the medial aspect of the pedal joint (LI01), up the medial side of the pastern, fetlock, to the top of the inner splint (04) and carpus (05). It ascends the forearm, curving anterolaterally, to the front of the elbow joint (11), to the point of the shoulder (15), to the nerve plexus at the base of C6-C7 (17), to the lateral side of the larynx (18), teeth and nostrils (LI20). Internal branches go to the colon and lung.
LI04 is near the upper head of the inner splint.
BL25 (LI Shu) may be tender in problems of the sacroiliac joint/ligament, the iliolumbar ligament, the inside splint, the 3rd and intermediate carpal bones, the elbow and shoulder, misalignment of vertebrae C6-T1, larynx, teeth, sinuses etc. It may be tender also in colic and impaction and in gluteal problems.
LI16 relates to the shoulder and inside carpus, fetlock and pastern.
LI17 has powerful effects, similar to LI04 in humans. It affects the sympathetic ganglion, producing endorphin-like effects and blocking the sympathetic nervous system. It is very tender in subluxation of C6, C7 or T1. Tenderness at LI17 may arise in shoulder, outside arm, inside carpus and fetlock. It may also arise ipsilateral to lumbar pain (BL25, LI Shu) or in contralateral hindlimb lameness.
LI18 relates to the forelimb shins.
T9 and L1: PC & TH Channels (Fire) (FIGURES 9 & 10)
PC (Pericardium, Circulation-Sex, Heart Constrictor) and TH (Triple Heater) are related in Fire. When Shu point tenderness or clinical signs indicate Channel imbalance, treat the Shu point and the Shu of the paired Channel. PC Shu is BL14,43 and TH Shu is BL22. PC Mu is CV17 and TH Mu is CV05.
When treating PC problems, the Mother (LV) Channel must be balanced and stimulated (BL18) and the Son (SP) Channel must be assessed (BL20) and treated, if needed.

When treating TH problems, the Mother (GB) Channel must be balanced and stimulated (BL19) and the Son (ST) Channel must be assessed (BL21) and treated, if needed.
Fire may be used to support weakness of Earth. Thus, BL14 (PC) may help weak SP and BL22 (TH) may help weak ST.
The PC Channel arises in the pericardium, runs to the medial side of the olecranon (PC01), to the medial side of the biceps tendon (03), down the medial side of the leg in the ulnar-radial groove (04,05,06,07), down by the inner splint (08), to the coronary band (over the medial plantar digital vein) (PC09). Internal branches go to the Triple Heater.
BL14,43 (PC Shu, pericardium) may show tenderness in cases similar to BL15,44 (see) and in anxiety and psychological problems.
PC points (BL14,43, PC06) are used in nervousness/psychological disorders and PC09 is a useful point to bleed in laminitis (M.J.C). Some females with breeding problems show sensitivity of BL14 (PC Shu) and GV10 (beside BL14). (See TH Channel also).
The TH Channel arises at the lateral side of the coronary band (over the lateral plantar digital vein) (TH01). It ascends the anterolateral side of the metacarpus (3) and carpus (04) and then follows the lateral ulnar-radial groove (05-08) and anterior edge of the olecranon (09,10). It runs behind and parallel to the humerus (10-13) to the lateral side of the shoulder joint (between the joint and the scapular spine, TH14). Then it runs to the anterior edge of the scapula at the junction with the scapular cartilage (15), to the dorsal side of the C3-C4 joint on the brachiocephalicus m. (16), to the posterior side of the ear (17). It runs over the root of the ear (18-22) and ends behind the lateral canthus of the eye (TH23). Internal branches go to the PC and the endocrine centres.
The TH Channel is important in endocrine disorders, especially in female infertility (M.J.C). TH14,16 are often sensitive in ovarian problems, cyst, oestrus). TH14 may be tender in shoulder lameness, but true joint lameness (OCD) is rare. More often, shoulder lameness is muscular, referred from subluxation of vertebrae C6-T1, via the
brachiocephalicus m., attached to the humeroscapular joint. Painful ovary or neck can cause spasm of that and other muscles and a choppy forward stride on the ipsilateral forelimb. If the problem is ovarian, treat BL22 (TH Shu) and the sensitivity at TH16 usually disappears. If the problem is shoulder lameness, treat TH14 and SI10, with BL22 and 27 (SI Shu). If the shoulder pain is referred from the neck, treat the neck (see 1.2.4).
TH16 may be tender in problems of the ovary/testis and in pain of the outside forelimb.
Excess activity in TH (Fire) can weaken LU (Metal) (via the Ko Cycle). This manifests as poor hair coat (LU controls skin) (M.J.C).
BL22 (TH Shu) may be tender in endocrine imbalance (thyroid, gonads, adrenal), in disorders of thermoregulation (non-sweaters), psychological problems, neck problems of the spinal accessory nerve (mid-cervical) and in neck vertebral misalignments. It may be tender in thoracolumbar problems, post-castration pain, cryptorchidism, inguinal ring problems (see BL23) and pain of the outside forelimb.
TH05 is used in shoulder problems and in navicular disease.
TH17 is a tranquillizer point.
T10 and S1: HT and SI Channels (Fire) (FIGURES 5 and 6)
HT (Heart) and SI (Small Intestine) are related in Fire. When Shu point tenderness or clinical signs indicate Channel imbalance, treat the Shu point and the Shu of the paired Channel. HT Shu is BL15,44 and SI Shu is BL27. HT Mu is CV14 and SI Mu is CV04.
When treating HT problems, the Mother (LV) Channel must be balanced and stimulated (BL18) and the Son (SP) Channel must be assessed (BL20) and treated, if needed.

When treating SI problems, the Mother (GB) Channel must be balanced and stimulated (BL19) and the Son (ST) Channel must be assessed (BL21) and treated, if needed.
Fire may be used to support weakness of Earth. Thus, BL15 (HT) may help weak SP and BL27 (SI) may help weak ST.
The HT Channel arises in the heart, runs to the posteromedial side of the shoulder joint (HT01), to the anteromedial side of the elbow (medial to the biceps tendon (03) and down the posteromedial side of the arm (04-06) and carpus (07), to the medial sesamoid (08) and the medial bulb of the fore heel (HT09). Internal branches go to the small intestine.
BL15,44 (HT Shu) may be tender in problems of the posterior side of the forelimb, tendons, sesamoids, heel bulb bruises, elbow (rare), circulatory function. BL14,15 (PC, HT) may be tender in anxiety and nervousness.
The SI Channel arises at the back of the outside bulb of the foreleg coronary band (SI01), ascends to the sesamoid (02,03), along the outer splint (04), along the posterolateral edge of the carpus (05), to the lateral side of the ulnar-humeral notch (06,07), to the olecranon (08), to the first muscular groove behind the shoulder joint (09), to a deep hole just below and behind the lower limit of the scapular spine (10). Then it zig-zags up the scapular spine (11,12) to the edge of the scapular cartilage (13) at T4-T5. Then it runs down and forwards to the side of C7 at the centre of the C6-C7 joint (15), to the centre of the C4-C5 joint (16), to the lower edge of the C2-C3 joint (17), to the malar bone (18) and the anterolateral root of the ear (SI19). Internal branches go to the small intestine and heart.
The SI Channel is very important. It is involved in many race-track injuries. It is used to treat bowed tendons, inferior check ligament injury, posterior branch of suspensory at outside sesamoid, "windgalls", and annular ligament damage. Subluxation of the lower neck (C6-T1), or of the atlas, or sacrococcygeal injury (in the starting gate, or in transport, due to backing-up), sacral plexus (parasympathetic) damage may involve the SI Channel (BL27, SI15,16). Reflex lameness in the superficial gluteal muscles at GB30 may arise in GB imbalance (GB is the Mother of SI). The SI is often involved in shoulder lameness. SI09,10,13 and the SI Shu (BL27), its Mother Shu (Wood-GB Shu, BL19) and its Son Shu (Earth-ST Shu, BL21) are indicated in such cases (see 1.1.3).

BL27 (SI Shu) may be tender in problems of the posterior side of the forelimb, tendons, sesamoids, heel bulb bruises, elbow (rare), sacral nerve plexus, biceps femoris, intestinal function.
SI10, if still tender after proper Channel balancing, is diagnostic for LOCAL shoulder lameness (OCD) - see 1.1.3.
SI13, at the edge of the scapular cartilage at the highest point of the
withers (see GV11,12 below) is very important in neck and thoracic muscle pain. The bursa between the nuchal and the supraspinous ligaments is very easy to injure. Needling SI13, GV11,12 in such cases is useful but proper Channel balancing, using BL19 (GB, Mother of SI) and BL21 (ST, Son of GB) is important.
SI17 is related to the outside sesamoid, suspensory ligament and lameness at the posterior side of the forelimb. It also relates to ipsi- and contra- lateral lower sacral injury, hindlimb lameness and all neck problems.
SI18 is a tranquillizer point.
BL16 (GV Shu) and BL17 (Diaphragm/blood/haemorrhage Shu)
BL16 and 17 are used for local problems as well as special effects. Their helper (outer) points are BL45 and 46 respectively.
BL16 (GV Shu) is used to increase or reduce GV activity. It assists the supraspinous ligament. Problems of the ligament are common in racehorses because they seldom have the opportunity to fully stretch their neck and paraspinal muscles (grazing, drinking from streams, rolling etc are seldom allowed !). Weakness of the supraspinal and nuchal ligaments predispose to neck and back problems and to tender bursae on top of the withers.
BL17 (Diaphragm Shu) is used for diaphragm/blood/haemorrhage problems. It helps in anaemia (increased PCV and Hb), bleeders (prothrombin and reduced blood pressure in lung vessels), other

respiratory problems (to stimulate breathing in neonatal foals) (with GV26). It is an immunostimulant point (with GV14, ST36, LI11), useful in viral diseases.
BL19 (GB Shu) is associated with whirlbone, outside stifle, outside hock, outside hind splint, curb.
T14 and 15: LV and GB Channels (Wood) (FIGURES 12 and 11)
LV (Liver) and GB (Gallbladder) are related in Wood. When Shu point tenderness or clinical signs indicate Channel imbalance, treat the Shu point and the Shu of the paired Channel. LV Shu is BL18,47 and GB Shu is BL19,48. LV Mu is LV14 and GB Mu is GB24.
When treating LV problems, the Mother (KI) Channel must be balanced and stimulated (BL23) and the Son (HT, PC) Channels must be assessed (BL15,14) and treated, if needed.
When treating GB problems, the Mother (BL) Channel must be balanced and stimulated (BL28) and the Son (SI, TH) Channels must be assessed (BL27,22) and treated, if needed.
Wood may be used to support weakness of Fire. Thus, BL18 (LV) may help weak HT or PC and BL19 (GB) may help weak SI or TH. Weakness or excess activity in Wood (LV, GB) can have profound effect on the ovarian/endocrine system (via TH - Fire-, Son of Wood). Such cases often have thoracolumbar pain (near BL18,19,22 - Shu of LV, GB, TH) and may also have spasm and a choppy stride in the ipsilateral shoulder/ forelimb, via TH16 (see TH Channel).
The LV Channel runs from the medial bulb of the hind heel (LV01), up the posteromedial edge of the pastern, medial sesamoid (02), along the inner splint (03), to the anteromedial side of the hock (04), up the inner side of the leg (05-07), to the posterior edge of the medial epicondyle of the femur (08). It runs along the inner thigh behind the femur to the inside of the hip joint. Then it runs to the tip of rib 17 (LV13, SP Mu) and ends behind rib 9, one hand above the level of the olecranon (LV14, LV Mu). Internal branches to the liver, eye and "gallbladder" function.
Deficiencies are more common than excesses in the LV Channel. Therefore, adding more energy (by correct feeding, HERBAL medicine

(fresh dandelions in spring) and lipotropic agents) are needed to obtain the optimal response.
The LV Channel is used with GB points in disorders of Wood. BL18,47 (LV Shu), LV13 (SP Mu) and LV14 (LV Mu) helps in myositis, azoturia, tying-up syndrome; to regulate SGOT, CPK, serum albumin and globulin; as immunoregulators; in allergies and eye problems (especially in spring (Wood); to regulate hoof-horn growth (Wood controls the nails) and in breeding problems (Wood is Mother of Fire (TH, PC)).
BL18 (LV Shu) may be tender in allergy (elevated globulin levels), muddy colour of the eye mucosa, lacrimation and conjunctivitis, problems of muscles, tendons, ligaments, azoturia, myositis, (tying-up syndrome), elevated CPK, SGOT in blood. The LV controls the eye in TCVM.
LV13,14 (Mu points of SP, LV) are very powerful points for balancing the Yin Channels, especially when coupled with SP21,21a (linking point for all Yin Channels, the Luo point for all Luo points).
The GB Channel begins at the lateral canthus of the eye (GB01). It runs to the ear (02), loops to the temporal (03-09) and post-auricular area (10-12) to above the eye (14), to the wing of the atlas (GB20). Then it follows the wings of the cervical vertebrae to the upper edge of the body of T1 half- way down the front edge of the scapula (GB21). It follows the lateral thorax to ICS 10 (GB24, SP Mu), then to the tip of rib 18 (GB25, KI Mu), forms a triangle of points (GB26-28) under the external iliac angle, curves around the hip joint (GB29,30), then down the lateral thigh behind the femur (31,32) to the posterior edge of the lateral epicondyle of the femur (GB33), the upper anterior notch between the fibula and tibia (GB34). It follows the lateral side of the leg to the lateral side of the hock (35-40), over the outer splint (41), the outer side of the fetlock (43), to end on the lateral side of the coronary band (GB44). Internal branches go to the liver and "gallbladder" function. A branch joins 25 to 25b just above the tuber coxae and rejoins 30. The tuber coxae point 25b is useful with BL19 in GB Channel problems, when BL19 (GB) is tender. Cain puts GB25a (another KI Mu) half way between the costochondral junction of rib 18 (GB25) and the lumbar muscles.
The GB is one of the most frequently used Channels (after the BL) in the horse. The GB and LV Channels are important in myositis and azoturia (tying- up syndrome), especially in spring (season of Wood).

Wood relates to muscle, tendon, ligament and the Krebs cycle (LV). Imbalance of Wood relates to build-up of lactic acid, impaired blood buffering, elevated SGOT, CPK and arginase in blood. Balancing the Wood (GB, LV) is essential for muscle health and liver metabolism. Water (KI, BL), Fire (HT, SI, PC, TH), Earth (SP, ST) and Metal (LU, LI) can all interact with Wood. All must be in balance for full health.
In hindlimb lameness due to reflex spasm of the superficial gluteal muscle (may arise in damage to the sacral plexus, or due to backing up against fixed objects), the local point (GB30) must be balanced by BL19 (GB Shu) and BL27 (SI Shu; Fire is Son of Wood).
BL19 (GB Shu) may be tender in problems of muscles, tendons, ligaments, azoturia, myositis, (tying-up syndrome), elevated CPK, SGOT in blood. In curbs, tenderness can arise at BL19 (GB), BL28 (BL Shu, the Mother of GB) and BL27 (SI Shu, Son of GB). Reactive GB can cause spasm of the biceps femoris muscle, resulting in hindlimb lameness.
GB20 and 21 are essential in treating wobblers and neck pain. GB20 can be injured easily by bad riders and by tie-chains in stalls. This can cause subluxation of the atlas, requiring chiropractic adjustment. AP alone, in such cases, gives poor or only temporary relief.
T17 and T18: SP and ST Channels (Earth) (FIGURES 4 and 3)
SP (Spleen-Pancreas) and ST (Stomach) are related in Earth. When Shu point tenderness or clinical signs indicate Channel imbalance, treat the Shu point and the Shu of the paired Channel. SP Shu is BL20,49 and ST Shu is BL21,50. SP Mu is LV13 and ST Mu is CV12.
When treating SP problems, the Mother (HT, PC) Channels must be balanced and stimulated (BL15,14) and the Son (LU) Channel must be assessed (BL13) and treated, if needed.
When treating ST problems, the Mother (SI, TH) Channels must be balanced and stimulated (BL27,22) and the Son (LI) Channel must be assessed (BL25) and treated, if needed.

Earth may be used to support weakness of Metal. Thus, BL20 (SP) may help weak LU and BL21 (ST) may help weak LI.
The SP Channel runs from the medial side of the coronary band of the hind heel (SP01), up the inner side of the pastern (03), by the inner splint (04), along the anteromedial hock (05), up the inside leg behind the tibia (06-08), to the inner stifle behind the tibial head (09). It runs up the inner thigh to the lateral abdomen to the tip if rib 15 (15). It curves along the thorax to the ICS 4 (SP20) and ends in ICS 10 (SP21, controller of all Yin Channels, the Luo of all Luo points). Internal branches go to the spleen-pancreas, stomach and the muscles.
BL20 (SP Shu) may be tender in disorders of blood, circulation, spleen, pancreas; in digestive disorders, impaction, colic; in lameness of the inside hindlimb/stifle/hock (cunean tendon) and in thoracolumbar injury. The SP points (BL20 (SP Shu), SP21,21a) are always tender in bleeders.
Cain locates a point (SP21a) about 1 hand above the olecranon, in ICS 5. This point has similar diagnostic and therapeutic functions to SP21. It is located on the large plexus of the posterior thoracic nerves at the posterior border of the latissimus dorsi muscle. SP21,21a show extreme sensitivity with imbalance of ANY Channel, especially a Yin Channel (LU, SP, HT, KI, PC, LV). These points can be used with LV13,14 (Mu of SP, LV) to balance all Yin energies. SP21,21a are very powerful points. Be careful that the horse does not fall on you! This has happened to Cain. Check these points after ANY treatment. If the Channels are balanced, SP21,21a should not be tender. If they are, additional therapy is needed.
The ST Channel begins below the eye (ST01), runs to the oral canthus (04), masseter (06), the temporomandibular joint (07). It runs down the neck (09), along the ventral edge of the sternocephalicus to ST10 (about one hand cranial to the point of the shoulder). It runs along the ventrolateral thorax to ST25 (LI Mu, level with navel), into the groin and towards the anterior of the hip joint. It runs down the lateral thigh, parallel with the cranial edge of the femur (31-34), to the hole lateral to the patellar tendon (ST35), to 1 hand below the tibial tuberosity, lateral to the tibia, between the long and lateral digital extensor muscles (36). It continues down the anterolateral leg (37-40), to the anterolateral side of the hock (41), down the anterior side of the shin and pastern (43,44). It ends at the coronary band on the anterolateral side of the hind foot (ST45). Internal branches go to the stomach and spleen- pancreas. A branch goes from ST25 to the origin of the tensor fascia lata (25a) (at the lowest, posterior edge of the tuber coxae), to

return to ST31. The tensor fascia lata point (25a) is used with BL21 (ST) in stifle lameness when BL21 (ST) is sensitive.
BL21 (ST Shu) may be tender in digestive disorders, impaction, colic, in anterolateral hindlimb lameness, stifle lameness, sacrosciatic ligament, sacral pain at the origin of the biceps femoris, thoracolumbar injury. ST10 (on sternocephalicus m.) relates to BL21. BL21 may be tender in shoulder pain when sternocephalicus is involved. This is common.
ST10 relates to the ipsilateral stifle, especially if BL21 is tender.
ST36 is used as a Local point for the stifle.
L2 and S2: KI and BL Channels (Water) (FIGURES 8 and 7)
KI (Kidney) and BL (Bladder) are related in Water. When Shu point tenderness or clinical signs indicate Channel imbalance, treat the Shu point and the Shu of the paired Channel. KI Shu is BL23,52 and BL Shu is BL28,53. KI Mu is GB25,25a and BL Mu is CV03.
When treating KI problems, the Mother (LU) Channel must be balanced and stimulated (BL13) and the Son (LV) Channel must be assessed (BL18) and treated, if needed.
When treating BL problems, the Mother (LI) Channel must be balanced and stimulated (BL25) and the Son (GB) Channel must be assessed (BL19) and treated, if needed.
Water may be used to support weakness of Wood. Thus, BL23 (KI) may help weak LV and BL28 (BL) may help weak GB.
The KI Channel runs from the hollow between the bulbs of the hind heels (KI01), up the back of the metatarsals to the posteromedial side of the hock (02-06). It ascends the inner leg (07-09) to the medial stifle, one hand behind the medial epicondyle of the femur (10). It runs

up the inner thigh to the groin (11), and along the ventral abdomen, 3 fingers lateral to the midline, to reach KI16 (lateral to navel) and KI22 (on the rib-cartilage of the 6th rib). From here, it runs inside the forelimb muscles, along the thorax, to end at KI27, in the ICS 1, at the sternum. KI27 can be reached by a 10 cm needle through the anterior superficial pectoral m. Internal branches go to the kidney, bones, ear, spinal cord, adrenal, ovary, bladder.
BL23 (KI Shu) is between the wings of L2-L3. It relates to the inside of the hindlimb. BL23 and 47 may be tender in urogenital (renal, gonadal), adrenal and fertility disorders and in thoracolumbar problems. It may be tender with BL22 (TH) in lameness related to psoas muscles, post-castration pain, cryptorchidism, inguinal ring problems, inside hindlimb problems. In those cases, BL23 is helped by KI03,07,10 and BL28 (BL Shu). If the tail twitches during riding, this indicates AhShi at BL23.
The BL Channel is the most important. Its clinical uses include diagnosis and treatment (via the Shu points). BL points are used in almost every AP prescription. BL points from C1-S4 correspond with superficial branches of spinal nerves in the sympathetic (neck-lumbar) and para-sympathetic (sacral) areas.
The BL Channel runs from the medial canthus of the eye (BL01), up the forehead (02,03), and head medial to the ears (04-09), to the wing of the atlas (10), to the notch at the anterior upper edge of the scapula, just behind the tip of the spine of T2 (BL11) and T3 (BL12) beside the high point of the withers. The inner and outer BL lines run paravertebrally from T3-S4. Key landmarks are BL13,42 below spine of T8, at posterior edge of the scapular cartilage; BL21,50 just behind last rib; BL23,52 between wings of L2-L3; BL32,28,53 (medial to lateral) at 2nd sacral hole. The Channel continues down the posterolateral thigh in the muscle groove from just above the tuber ischii (BL54a) to below the tuber ischii (BL36,36a,37) to the popliteal area (BL38,39,40), down the posterolateral leg (BL55-59), to the notch between the Achilles tendon and the lower head of the tibia (BL60), over the lateral hock (BL61,62), down the outer splint (BL63-65) and sesamoid (BL66), to end at the coronary band at the lateral bulb of the hind heel (BL67). Internal branches go to the kidney, bladder and pelvic functions.
In humans, the sequence of Shu points (BL13-30) is:
Below level of spine of T3-T7 (BL13-17): LU, PC, HT, GV, Diaphragm-Blood-Haemorrhage
Below level of spine of T9-T12 (BL18-21): LV, GB, SP, ST
Below level of spine of L1-L5 (BL22-26): TH, KI-ovary, QiHaiShu, LI, GuanYuanShu
Below level of spine of S1-S4 (BL27-30): SI, BL, ZhongLuShu, BaiHuanShu
In the horse, pending careful provocation tests, one can transpose BL21 as in humans (just behind the last rib). The area just behind the posterior edge of the junction between the scapula and the scapular cartilage is consistently tender in lung disease (bleeders etc)- M.J.C. This point is below the spine of T8. It is taken to be BL13 (lung Shu). Another BL13 point is directly dorsal to this, at the edge of the scapular cartilage. Thus, it is easy to locate BL13 and BL21. The simplest way to locate BL12-20 is as follows:
There are 9 points between (and including) BL13-21. BL17 can be taken as mid-way between them. The remaining points (BL14-16 and BL18-20) can be located easily by counting forward or backward from BL17.
However, more accurate locations of equine Shu points BL13-21 (LU, PC, HT, GV, Diaphragm-Blood-Haemorrhage, LV, GB, SP and ST respectively) are as follows:
HORSE THORACIC SHU POINTS
BL13 FeiShu = LU Shu: Below the dorsal spine of T8, at caudal edge of scapular cartilage in 8th intercostal space (ICS 8) (M.J.C). It relates to the inside of the forelimb. Its partner is BL42
BL14 JueYinShu = PC Shu: Below the dorsal spine of T9 (ICS 9). It relates to the inside of the forelimb. Its partner is BL43.
BL15 XinShu = HT Shu: Below the dorsal spine of T10 (ICS 10), lateral to GV10. It relates to the inside of the forelimb. Its partner is BL44.
BL16 DuShu = GV Shu: Below the dorsal spine of T11 (ICS 11). It relates to the dorsal surface of the back and local (nearby) organs and their functions. Its partner is BL45.
BL17 GeShu = Diaphragm-Blood-Haemorrhage Shu: Below the dorsal spine of T12 (ICS 12). It relates to diaphragm, blood diseases, and immunity. Its partner is BL46.

BL18 GanShu = LV Shu: Below the dorsal spine of T14 (14th ICS, or 4th last). It relates to the inside of the hindlimb. Its partner is BL47.
BL19 DanShu = GB Shu: Below the dorsal spine of T16 (16th ICS, or 2nd last). It relates to the outside of the hindlimb. Its partner is BL48.
BL20 PiShu = SP Shu: Below the dorsal spine of T18 (last ICS). It relates to the inside of the hindlimb. Its partner is BL49.
HORSE LUMBAR SHU POINTS
BL21 WeiShu = ST Shu: Below the dorsal spine of L1, just behind last rib. It relates to the anterolateral side of the hindlimb. Its partner is BL50.
BL22 SanJiaoShu = TH Shu: A key Endocrine point, behind the wings of L1. It relates to the lateral neck and the outside of the forelimb and to endocrine problems, especially reproductive. Its partner is BL51.
BL23 ShenShu = KI Shu: Between the wings of L2-L3. (Cain and Glardon find the latter place the more important. It relates to the inside of the hind limb and to KI-gonad-adrenal and bone function. Its partner is BL52.
BL24 QiHaiShu = Qi Sea Shu: Behind the wings of L4.
BL25 DaChangShu = LI Shu: Behind the wings of L5, behind a line between the most anterior point of the left and right external angle of the ilium. It relates to the outside of the forelimb. It may be tender in colic and sciatica.
BL26 GuanYuanShu = Gate Origin Shu, Uterus Shu: Behind the wings of L6, before a line between the highest points of the left and right tuber coxae.
HORSE SACRAL SHU POINTS
BL27 XiaoChangShu = SI Shu: Lateral to sacral foramen 1; it relates to the back of the forelimb. BL31 is medial to it.
BL27a Unnamed = another SI Shu: lateral to GV02 (sacrococcygeal space). This point is more reactive than the classical BL27 in SI problems. It is very close to, if not the same as Cain's sacral hip-stifle point. It has the same functions as BL27.
BL28 PangGuanShu = BL Shu: lateral to sacral foramen 2, at the top of the muscle crease. It relates to the posterior side of the hindlimb. BL32 is medial to it. Its lateral partner in humans is BL53.

BL28a Unnamed = another BL Shu: lateral to coccygeal 2, in the groove just posterior to the origin of the biceps femoris, about 2 inches behind BL27a. This point is more reactive than the classical BL28 in BL problems (M.J.C). It has the same functions as BL28, as have BL32. BL28,28a (BL) may be tender in urogenital (renal, gonadal) disorders, in sacral problems, in all problems of the spinal column (from the atlas to the sacrum). BL28 is important in cervical misalignment, in sacrococcygeal injury (in transport etc), in stress-related pain of the semimembranosus and semitendinosus muscles. It is used also in GB-related (see BL19) lameness; Water (BL) is the Mother of Wood (GB) in the Sheng cycle.
BL29 ZhongLuShu = Middle of Back Shu: lateral to sacral foramen 3. BL33 is medial to it.
BL30 BaiHuanShu = White Circle Shu, Anus: lateral to sacral foramen 4. BL34 is medial to it. Its lateral partner in humans is BL54.
In humans, the Outer paravertebral BL line (O = points BL41-52, between vertebrae T2 and L2) has a relationship to the Inner (I) line:
O (41 to 52) = I (12 to 23) + 29, i.e. points BL12,41 / 13,42 / ... / 23,52 / are functional pairs.
The outer (O) point is in the SAME ICS, lateral to the inner (I) point. The same relationship applies in the horse. The outer BL line relates to the parasympathetic nervous system. In particular, BL42 (ICS 8 in the horse; partner of BL13) is sensitive in lung bleeders, especially on the right side.
Human points BL53 and 54 are lateral to BL28 and 30 (lateral to sacral foramina 2 and 4 respectively). In horses, BL53 is just behind the anterior edge of the external angle of the ilium, lateral to BL26; BL54 is level with coccygeal 1-2 space, below and in front of BL28a. BL54a is below BL53, in the muscle crease just at the tuber ischii. BL54 and 54a are used in hip and thigh problems.
BL24 (QiHaiShu) and BL26 (GuanYuanShu)
These points are used mainly for local effects, as in lumbar and sacral disorders. There is a traditional horse point GuanYuanShu behind last rib. It is active on gastrointestinal problems and should not be confused with BL26, which has effects on the uterus. BL24,26 may be active in disorders of the lumbosacral ligaments, sciatica, pain at the insertion of the longissimus dorsi, iliosacral ligament, middle gluteal muscle, sacrosciatic ligament, sacral nerve plexus.

The lumbar Shu (BL21,22,23,24,25,26: ST, TH, KI, QiHaiShu, LI, GuanYuanShu) reflect the sympathetic nervous (cervicolumbar) and endocrine systems.
The sacral Shu (BL27,28,29,30: SI, BL, ZhongLuShu, BaiHuanShu) reflect the parasympathetic nervous system (craniosacral).
CV Channel (FIGURE 13)
The CV (Conception Vessel) Channel runs in the ventral midline, from CV01 (between the anus and the vulva/root of the penis, along the perinaeum above the penis or mammary gland, to the navel (CV08), to the tip of the xiphoid (CV14), to the manubrium sterni (CV22), to the hollow above the larynx (CV23), to the centre of the lower lip (CV24). This Channel is important in humans as Mu points for BL, SI, TH, ST, HT, PC (CV03,04,05,12,14,17 respectively) are on it. In the horse, points CV03-08 can be dangerous to needle but CV12,14,17 are relatively easy to needle. Horses, however, often tolerate Shiatsu (deep massage) of awkward points. CV12 is located midway between the navel and the xiphoid. CV17 is located about 1 hand anterior to the caudal border of the olecranon, on the sternum.
Shiatsu at CV05 can be used with AP at other points in endocrine/autonomic disorders (lack of sweating, breeding problems, thyroid problems). CV08,12 are useful in colic (Shiatsu or massage with heat-producing liniment).
CV01 + GV01 are useful to stimulate initial defecation in neonatal foals.
Stimulation of the clitoris (YinTi) produces a strong extensor reflex of the hindlimbs. This is of clinical use in dogs with posterior paresis: if marked extensor reflex is not produced, the prognosis is poor (M.J.C). In cows, warm Laser stimulation of the clitoris can help in the treatment of infertility.
CV23 (needling or Laser) is useful in pharyngitis (M.J.C).

GV Channel (FIGURE 14)
The GV (Governing Vessel) Channel runs in the dorsal midline from GV01, (between the anus and the root of the tail), to the sacrococcygeal space (WeiKen, GV02), to the lumbosacral space (BaiHui, GV03), to the L2-L3 space (GV04), to the T5-T6 space (GV11), to the T3-T4 space (GV12), to the top of the head (GV20), to the midpoint between the nostrils, at their lower limit (GV26). It ends at GV28, between the upper lip and the upper gum.
The GV is a very important Channel in humans. Its points have similar functions to their nearest BL points. In the horse, because it can be difficult to penetrate the dorsal midline between L1 and T8, points GV05-10 are not used often. However, GV01,02,03,04,11,12,14 and 26 are very important points. GV01-04 are used in problems of the hindquarter, genitourinary system and hindgut.
When a Shu point is injured (from trauma, external or internal causes), the GV point or the dorsal spinal process nearest it is usually tender and should be treated. Very superficial picks (just slightly subdermal) are all that is needed.
GV01 + CV01 are useful to stimulate initial defecation in neonatal foals. The tip of the tail (GV00) is a special action point, used in shock and recumbency.
GV11 and 12, at the highest point of the withers, are related clinically to GV14 in humans (antifebrile point, antiasthmatic point, problems of the neck, thoracic limb and upper thoracic spine). GV11,12 often are tender in cervical problems in horses. They are as important to the forequarter as BaiHui (GV03) to the hindquarter. After adjustment of subluxated neck vertebrae (see 1.2.4), balance at GV11,12 can be obtained by pricking superficially with a 22g needle. The points can be injected with 0.1 ml homeopathic NaOH 9d. This releases spasm at the origin of the trapezius, latissimus, rhomboideus, serratus and other deep muscles attached to the withers. Occasionally, BL14 (PC Shu) and the GV point in between may be tender in breeding problems (M.J.C). The withers area is very prone to pressure injury from the pommel of the saddle or from bad riders, who ride too far forward. This is the site of fistulous withers and a point easy to injure the bursae of the supraspinous ligaments/neck muscle attachments.
GV26, the Shock Point, is useful in emergencies in all species. It is effective in stimulating respiration and circulation in the newborn foal. GV01 + CV01 are useful to stimulate initial defecation in neonatal foals.
SUMMARY
1. Veterinary acupuncture (AP) is based primarily on human AP principles and the choice of points for particular conditions is very similar to the choice for similar human conditions.
2. Using a Hewlett-Packard Minicomputer, data from over 55 textbooks and clinical articles were stored. Frequency-ranked prescriptions for >1100 clinical conditions were generated from the computer database.
3. The Top Twenty Points from each prescription were extracted from the database summary. From this list, the most important points for major body regions (head, neck, thoracic limb, thorax, nose, throat, shoulder, elbow, lung, stomach, etc) and common symptoms (shock, nausea, vomiting, diarrhoea, fever, etc) were extracted.
4. Appendix 1 comments on the use of the point Index, the structure of the Index and the code and name of each point. Appendices 2 and 3 list the points. Examples of methods of point selection for specific conditions and for more complex syndromes (combinations of symptoms) are given in the text.
5. Advantages and disadvantages of the COOKBOOK METHOD of point selection are discussed in relation to holistic (traditional) AP.
INTRODUCTION
Western veterinary AP is based primarily on transposition of human AP principles to animal patients. To select effective points for therapy, one makes appropriate adjustments for differences in anatomy, location of peripheral nerves, and temperament of the animal (Rogers, 1980b; Molinier, 1983; Westermayer, 1981). There are some texts on traditional veterinary AP and some Western experts have produced texts which are based on traditional points. Others have written texts on the transposition method. Advantages and disadvantages of the transposition method have been discussed elsewhere (Rogers, 1982b).
Studies of the electrical resistance of skin in dogs, horses and cattle have confirmed the existence of REPP (reactive electropermeable points) at locations predictable from the human AP system (Janssens; Krueger; Greiff; Kothbauer). In AP research with primates, laboratory animals (mice, rats, guinea pigs, rabbits) and larger species, the human transposition system is the one used routinely to locate points such as LU01; LI04,11,15,20; ST09,25,36; SP06,09; HT07; BL points; PC06; TH05,08,14,17; GB20,30,34; LV03,14; GV26 etc. The clinical and experimental effects of stimulating these points have been

confirmed worldwide in the past 10 years in many animal species (laboratory, farm, domestic and zoo).
Uses of the computer in AP and the advantages and disadvantages of computer -generated prescriptions were discussed elsewhere (Rogers 1984 a, b). Many professionals still refuse to use a computer. I believe that this refusal stems from fear (that they will not be able to master it) and ignorance of what a modern computer can and cannot do. Traditionally-trained acupuncturists may scorn the idea of cookbooks (although they use their own favourite prescriptions - a poor Cookbook). They would be horrified at the idea of computerising AP.
COOKBOOK AP: Many have told me that "prescription AP", especially the free availability of prescriptions, do AP a disservice. They assume that the cowboys (quacks, charlatans, get-rich-quick merchants) will proliferate and thrive if such information is freely available. I do not believe this. I would prefer to see AP develop rapidly. This will not happen if we must wait for a high percentage of the professions to develop to Master Acupuncturist status. The use of AhShi therapy and cookbooks brings more professionals into the active AP field than any other method that I know.
This paper discusses computer-based AP prescriptions for selected areas and symptoms under 3 main headings
: computer AP databases
: prescriptions for major body areas, functions, subregions
: prescriptions for common symptoms
It has taken me more than 11 years to amass these data. Therefore I ask each of you to treat the material as copyright. You are welcome to use it for clinical, study and research purposes, but not for commercial publication in text, computerised, microfiche form, etc. You are free to make personal copies for friends or colleagues, but only on condition that they also agree to respect the copyright.
The Channel and Point coding used throughout this text is: LU, LI, ST, SP, HT, SI, BL, KI, PC, TH, GB, LV, CV, GV; ST08 (TouWei) is on the temple, BL41 (FuFen) is at T2 and BL40 (WeiZhong) is in the popliteal crease. This is the same as that used by IVAS. The alphanumeric code and name of each point is shown in Appendix 1. As there is no internationally accepted coding system to-date, you are urged to check my coding system (Appendix 1) at this stage and to compare it with the one which you use. This is most important to prevent confusion and error.
COMPUTER AP DATABASES
The larger the database, the more points are filed under any given region, symptom or condition. However, the first 6-10 points listed (in order of descending citation score) are the most important for routine use. For example, in the most recent summary of the database, 401

points were listed from a base of 44 texts for the treatment of sequelae (hemiplegia, paralysis) of CVA or polio. The Top Ten points were:
Ranking 1 2 3 4 5 6 7 8 9 10Point LI04 LI11 ST36 GB34 ST06 GB30 ST04 LI15 TH05 GB39Score .86 .79 .77 .74 .73 .72 .68 .66 .62 .62
The Maximum score possible was .964. The bottom 10 points were:
Ranking 392 393 394 395 396 397 398 399 400 401Point CV13 CV17 BL65 LI01 ST23 BL07 KI20 GB06 GB43 LV06Score .02 .02 .02 .02 .02 .02 .02 .02 .02 .02
The scores have been rounded up or down to the second decimal place. Clearly, the first list would be expected to give better therapeutic results than the second list above.
However, selection of the Top Ten points in the above list would not necessarily be the best selection for a CVA sequel which was primarily mutism or aphasia. For such cases, the top 10 points are:
Ranking 1 2 3 4 5 6 7 8 9 10Point CV23 GV15 HT05 LI04 Z 21 TH03 GB02 TH17 NZ32 SI19Score .82 .72 .44 .37 .27 .23 .23 .21 .20 .18
(From a total of 71 possible points listed by 27 texts, maximum possible score was .952)
The differences between the Top Ten points for CVA and the Top Ten points for aphasia underline the need for formulating specific questions for the computer search. Where possible, one should search the database for general data (CVA), general region (head, neck, thoracic limb etc), specific region (arm, leg, hip, etc), specific nerve (mandibular, hypoglossal, radial etc). Where specific symptoms are marked (aphasia, incontinence, etc) they should also be searched.
The greatest volume of data refers to the abdomen and its organs/functions. Although there are points listed for "abdomen", "digestive upsets", "reproductive disorders" etc, these lists should be used as guidelines for general study or general consideration. In specific cases, it is preferable to search under the most relevant symptom or condition, such as "vomiting", "diarrhoea", "constipation" etc, rather than "digestive upset" or "metritis", "infertility", "impotence", "oligospermia" etc, rather than "reproductive disorders".
The database covers >1100 headings (regions, organs, conditions, symptoms, etc). The printout of the complete listing for the Top Twenty points runs to some 160 pages of full-width (132-character) computer paper. In one hour, it is not possible to cover these data. Therefore, I have chosen to list the Top Twenty points for about 130 of the major body regions and their subregions and organs (Appendix 2). The Top Twenty points for about 130 of the more common symptoms are also listed (Appendix 3).

PRESCRIPTIONS FOR MAJOR BODY AREAS, FUNCTIONS, SUB-REGIONS AND COMBINATIONS OF SIMILAR CONDITIONS
In the database (see Appendices 1,2,3) points are filed under separate condition codes such as:
040201 Shoulder area (unspecified conditions)
040202 Clavicle: APA for fracture reduction
040203 Shoulder: APA for dislocation reduction
040205 Shoulder, scapula : pain .. ache.. .arthritis etc
040211 Shoulder, scapular: paralysis
040219 Deltoid: myofascial syndrome
Using the computer, it was possible to combine information to retrieve all points used in, for example, all conditions of "shoulder, clavicle and scapular area" (a total of 181 points from 45 references). In this way, the entire database was summarised by amalgamation of data for major body areas, functions, subregions and combinations of similar conditions.
The Top Twenty points and their scores are listed in Appendix 2. These lists should prove useful in the study of AP and as reference material for teaching seminars. They do not, however, supplant the lists of points for specific symptoms but should be seen as general guidelines in the choice of points.
PRESCRIPTIONS FOR COMMON SYMPTOMS
The database was searched for a cross-section of common symptoms, especially those relating to the musculoskeletal system (pain, paralysis) and to major body functions. The Top Twenty points and their scores for some 130 symptoms or conditions are listed in Appendix 3. It must be remembered that only the Top Twenty points are given here. There are many other points which could be considered, especially if a number of symptoms occur together. In complicated cases, for example, neurogenic vomiting and dehydration in the dog, points for the main symptom (vomiting: PC06; ST36; CV12; ST25) could be combined with supportive therapy (fluid replacement).
In cases of anaesthetic emergency or respiratory arrest, main points (GV26, KI01) could be combined with artificial respiration (though the latter is seldom needed if the points are stimulated strongly). In cases where cardiac arrest has also occurred, point PC06 (very powerful on heart and lungs) could be added to GV26, KI01, and open or closed heart massage, defibrillation or other methods would be added.
Please scan Appendices 1, 2 and 3 now, and then return to the discussion which follows.
MASTER POINTS FOR CHANNEL THERAPY
Apart from the 66 Command Points, there are other powerful points to redistribute Qi between imbalanced Channels. These are the Shu-Back Association (Reflex) Points, the Mu-Front Alarm Points, the Luo-Passage (Connecting Points between the Phase-Mate Channels within one Phase), the Xi-Cleft Points, the Test Points, the Ryodoraku (Japanese Points), and the HE (Sea Points). The latter points are not the same as the HO points on the Channels. In addition there is an Hour Point (the Phase point of a Channel, for example the Earth Point of SP, the Water point of BL etc). SP21 is the Great Luo point (Luo point of all the Yin Channels).
Taken together, the 66 Command/Su Points, plus the Shu, Mu, Luo, Xi, Test, Ryodoraku, HE, Hour and SP21 Points are called the Master Points of AP.
The Five Phase Points Tonic Sedat.Affected COS Wood Fire Earth Metal Water point point Yuan LuoLV (Wood-Yin ) 01 02 03 04 08 08 02 03 05GB (Wood-Yang) 41 38 34 44 43 43 38 40 37HT (Fire-Yin ) 09 08 07 04 03 09 07 07 05SI (Fire-Yang) 03 05 08 01 02 03 08 04 07PC (Fire-Yin ) 09 08 07 05 03 09 07 07 06TH (Fire-Yang) 03 06 10 01 02 03 10 04 05SP (Earth-Yin ) 01 02 03 05 09 02 05 03 04ST (Earth-Yang) 43 41 36 45 44 41 45 42 40LU (Metal-Yin ) 11 10 09 08 05 09 05 09 07LI (Metal-Yang) 03 05 11 01 02 11 02 04 06KI (Water-Yin ) 01 02 03 07 10 07 01 03 04BL (Water-Yang) 65 60 54 67 66 67 65 64 58
Xi- RYODO HE Cleft HOUR Test -RAKU (SEA)Affected COS Shu Mu point point point point pointLV (Wood-Yin ) BL18 LV14 06 01 08 03 -GB (Wood-Yang) BL19 GB24 36 41 33-39 40 GB34HT (Fire-Yin ) BL15 CV14 06 08 07-09 07 -SI (Fire-Yang) BL27 CV04 06 05 03-04 05 ST39PC (Fire-Yin ) BL14 CV17 04 08 04 07 -TH (Fire-Yang) BL22 CV05 07 06 04-10 04 BL53 SP (Earth-Yin ) BL20 LV13 08 03 09 02 -ST (Earth-Yang) BL21 CV12 34 36 34-36 43 ST36 LU (Metal-Yin ) BL13 LU01 06 08 06 09 -LI (Metal-Yang) BL25 ST25 07 01 11 05 ST37KI (Water-Yin ) BL23 GB25 05 10 07 05 -BL (Water-Yang) BL28 CV03 63 66 59-60 65 BL54
1. In disorder of the associated Channel-Organ System (COS), there is usually tenderness on palpation of the Yuan, Mu, Shu and Test points. The Test points may feel cold in Yin states and hot in Yang states. The RYODORAKU points are electro-sensitive diagnostic points

used in Japanese diagnosis. Their readings are hypo- in Yin and hyper- in Yang states.
2. All MASTER points, except Shu, Mu and HE points, are on their respective Channels and lie between the elbow and finger or between the knee and toe.
3. The Yuan-Luo combination uses the Yuan of the affected Channel with the Luo of the Phase-Mate Channel, i.e in lung disease, LU09 (Yuan of LU) plus LI06 (Luo of LI).
An examination of most of the listings in Appendices 2 and 3 shows that the Top Ten points obey the basic laws of choosing AP points. In summary, these laws suggest a choice of points from:
a. AhShi points (including Trigger Points, tender scars, fibrositic nodules etc)
b. Local points (which also meet condition (d)).
c. Distant points on the Channel through the affected area or on the Channel of the affected organ. A chain of points on the affected Channel is said to be specially powerful.
d. Points on the affected nerve, the nerve supply related to the affected organ or area, or in the same or a nearby spinal nerve segment.
e. Encircling the problem area; "Fore and Aft" points; combination of Yin side and Yang side points (medial/lateral; anterior/posterior).
f. Combination of Mu and Shu (Front Alarm + Back Association) points.
g. Combination of affected Yuan and Luo of Mate (Source Point of the affected Channel plus Passage point of its Phase-Mate Channel (LU-LI; ST-SP; HT-SI; BL-KI; PC-TH; GB-LV).
h. Xi-Cleft point of affected Channel.
i. One or more of the Five Phase Points (Energetic balancing points).
j. Symptomatic points (traditionally known to have marked effect for the specific symptoms, for example, GV26 in shock, emergencies; PC06 in nausea or vomiting).
k. Extra-Channel points ("New" or "Strange" points, points not on the Main Channels), especially those effective for the condition, e.g. NX04 (TingChuan) in asthma.
l. Points on the Phase-Mate of the affected Channel (e.g.) ST points in spleen diseases; SP points in stomach diseases.
m. TianYing point (OT02, centre of the goitre etc).

n. One point on each of the 4 limbs (e.g. LI04 and ST44, both bilateral, in tonsillitis or toothache).
Let us examine the Top Ten points from some prescriptions (Appendices 2,3) in detail under three basic headings:
1. Local conditions or regions
2. Conditions of specific internal organs or their functions
3. Generalised conditions and complex syndromes.
In each of these conditions, codes (a) to (n) mentioned above are used to show the laws observed by the points in the Top Ten list.
1. LOCAL CONDITIONS OR REGIONS: Let us pick problems of the eye, nose, neck, shoulder, elbow, lowback, hip and knee (stifle) as examples from Appendix 1:
EYE: BL01 (b); LI04 (c, as the LI Channel connects to ST Channel at the eye); GB2O (c);also Wood (GB,LV) controls the eyes; ST01 (b); Z09 (b, k); BL02 (b); ST02 (b); GB14 (b,c (Wood)); TH23 (b); BL18 (liver controls eyes. BL18 is Shu point of liver, b). The combination BL01, ST01, Z 09, GB14 meets law (e) above and is very useful in eye diseases. 7/10 of these points are local points.
NOSE: LI04 (c,g,i,j); LI20 (b); GB20 (j); GV23 (c); LI11 (c,i,j); GV14 (c,j); Z 03 (b,k); BL07 (c); LI19 (b); ST02 (b). The combination LI20, Z 03, ST02 also meets law (e). 4/10 of these points are local points.
NECK: GB2O (b); GV14 (b); LI04 (c,g,i); BL10 (b); SI03 (c,i.j); LI11 (c,i,j); OT01 (AhShi point - a); GB21 (b,c depending on site of problem); GB39 (c,j); SI15 (b). The combination GB20,21, BL10, GV14, SI15 also meets law (e). 5/10 of these points are local.
SHOULDER area: LI15 (b,j); LI11 (c,i,j); TH14 (b,j); Sl11 (b); Sl09 (b); LI04 (e,g,j); OT01 (a); Sl10 (b); OT05 (local points, b); BL11 (d ,j ). A combination of SI09, LI15 and a new point l" above anterior axillary crease is known as the "shoulder triplet". The combination meets law (e) above and has powerful effects in shoulder conditions. 6/10 of these points are local points.
ELBOW: LI11 (b,i,j); TH05 (c,j); LI04 (c,g,i); HT03 (b,i); LU05 (b,i); LI10 (b); OT01 (a); LI12 (b); TH10 (b); SI07 (c). 6/10 of these points are local.
LOWBACK: BL23 (b,j); BL40 (c,i,j); GB30 (c, linked to lowback via BL Channel, d,j); BL60 (c,i,j); GB34 (c (via BL link), i,j); BL25 (b); BL37 (c); GV04 (b); BL57 (c); BL31 (b). 4/10 of these points are local.
HIP: GB30 (b,j); GB34 (c,i,j); GB29 (b); GB31 (c); BL40 (c via link to GB Channel, i,j); BL60 (c,i,j); OT01 (a); GB39 (c,i,j); ST36 (d,i); LV08 (-). Although only 2/10 of these points are local, 2 of the top 3 points are local.

KNEE: GB34 (b,i,j); BL40 (b,i,j); L 16 (b,k); ST35 (b); SP09 (b); ST36 (c,i); ST34 (b); LV08 (c); OT01 (a); GB31 (c). The first05 of these points are the most commonly used combination (obeying law e) and all are local points.
In the eight local conditions discussed above, seven have a local point as the first in the list (the 8th has a local point as second on the list).
2. CONDITIONS OF INTERNAL ORGANS AND THEIR FUNCTIONS: Let us consider the Top Ten points in five of the conditions in Appendix 2. Close examination of other lists in the appendices will show that they follow similar logic.
PLEURA: BL42, BL47, BL43, KI23, KI22, BL13, GB32 (7/10 points) are on the thorax or dorsal paravertebral area (local). Two of the other three (ST12, BL11) are at the thoracic inlet and the 10th point (GB44) obeys law (c).
HEART, PERICARDIUM: Only 3 of the Top Ten (BL15, BL14, CV17) are over or near the organs. They obey laws (b), (d), (e) and (f). Six of the remainder (PC06, PC07, HT05, PC05, PC07, PC04) are on the HT or PC Channel (laws c, i, j). The 10th point (ST36) is a Master Point, with many functions, including effects on HT and PC.
COUGH, GENERAL: BL13, CV22, GV12, BL12, CV17 (5 of the top 10 points) are over the thorax, trachea or dorsal paravertebral area. They obey laws (b), (d), (e), (f), (j). Three points (LU05,07, 10) are on the LU (lung) Channel (laws c, i). The remaining two points (ST4O, GV14) meet laws c and i.
LIVER: 6/10 points (BL18,19,20,48; GV09; LV13) are over or near the liver. They obey laws b, d, e, f, j. The remaining four points (LV03, ST36, GB34, SP06) are master points. They obey laws c, g, i, j.
GENITALIA FEMALE AND REPRODUCTION: 6/10 points are in the lumbosacral innervation area (low abdomen or l/s paravertebral area). They are: CV03,04,06; GV04; GB26; BL32. They obey laws (b), (d), (e), (j). The four remaining points (SP06,10; LV03; ST36) are Master Points with major effect on low abdomen and its functions. They obey laws (c), (i), (j).
2a. IF AN ORGAN OR FUNCTION HAS NO NAMED CHANNEL, points can be chosen from combinations relating to the nearest organs, or Channels, or functions. For example, suppose there were no entries for the following organs:
Thymus: consider points from combinations for heart, lungs, stomach (nearest organs) and immunity (a closely allied function).
Diaphragm, oesophagus: consider heart, lung, stomach combination.
Appendix: consider lower right abdomen and large intestine combinations + immunity.

Adrenal (beside kidney): consider kidney combinations.
Ovary, tubes, uterus: consider kidney, bladder, low abdominal and large intestinal combinations.
Vagina, vulva, scrotum, testicles, penis: these are controlled by the 3 Leg Yin Channels (SP, LV, KI). Consider points on these Channels + points for low abdomen, bladder.
3. GENERALISED CONDITIONS AND COMPLEX SYNDROMES: Generalised conditions include metabolic, hormonal, toxic, general autonomic upsets, etc (such as gout, diabetes, food poisoning, shock, neurasthenia, etc). Although one symptom may be dominant, it is usual to have a number of symptoms and abnormalities occurring together.
For example, in gout, the presenting symptom may be pain in the big toe (or other joint), but other symptoms could include liver enlargement + pain; headaches; irritability; blurred vision; tiredness, etc. The comprehensive treatment would entail dietary advice (possibly involving food allergy/intolerance testing) and increased fluid intake. AP would be aimed at the more severe symptom (say toe pain) but other points (especially LV and GB) would be aimed at the other symptoms. The liver is central in gout and many allergies. Treat the liver.
In diabetes mellitus, polyuria, neuropathy and other signs can arise. Dietary advice, together with points for diabetes (see Appendix 2) the local regions affected by neuropathy and the kidney (Appendices 1 and 2) would be indicated.
In food poisoning, vomiting and diarrhoea would be tackled by points such as CV12, PC06, ST25,36,37 but other symptoms (dehydration, prostration etc) would best be tackled by fluid replacement. Medication (kaolin, chlorodyne) can assist the gastrointestinal symptoms.
In shock, points like GV26, KI01, ST36, PC06 can be of immediate help but accurate diagnosis of the pathology is essential and would indicate other interventions (surgery, if severe internal bleeding; fluids, stimulants, warmth, etc where indicated).
In neurasthenia, insomnia, excitement etc, the HT and PC Channels control these functions in traditional belief. Consider HT, PC points.
DISCUSSION
1. IN MOST LOCAL PROBLEMS (joint, muscle, superficial organ etc) the best prescription combines AhShi points and local points + distant points on the affected or related Channel. It is important to check the location as regards the nerve supply and the Channel. For example, the best combination for pain in the medial epicondyle of the humerus will not be identical to the best combination for the lateral epicondyle. However, in traditional AP, it is not enough to pick any

local point. (Some local points are better than others, or, at least, are more frequently recommended than others).
Modern neurophysiological concepts of AP stress that adequate stimulation of the affected or related NERVES will produce results as good as the traditional method but adequate clinical or research testing of the traditional versus modern (nerve theory) methods has not been done. For the moment, I give the benefit of the doubt to the traditional system, which has stood the test of time.
2. IN DISEASE OF INTERNAL ORGANS, the most important points lie near the organ in the thoracoabdominal area or in the paravertebral area (the Mu, Shu and Huatochiachi (X 35) points, CV and GV points). Where the organ has a named Channel (LU, LI, ST, SP, HT, SI, BL, KI, PC, GB, LV) it is common to include one or more points on that Channel (distant as well as local points). Also, the course of the Channel is important. For example, the liver, kidney and spleen Channels traverse the inner thighs and groin area. Distant points on these Channels are important in genital and lower abdominal conditions.
In general, if a symptom or abnormal function can be traced to a specific COS, treat that COS. If more than one symptom/organ system is involved, choose a combination of points which will influence all the major symptoms or upset organs.
3. IN ACUTE SERIOUS CONDITIONS, WITH MULTIPLE SYMPTOMS AND PATHOLOGY, it is unwise to rely solely on AP. AP can often give considerable help (using points as indicated by the main symptoms and pathology) but conventional or unconventional (complementary) therapies may need to be used as well.
4. IN CHRONIC COMPLICATED CASES, where immediate life-threatening symptoms or pathology are absent, one can rely more on AP as the main therapy (in cases amenable to treatment). At all times, however, the aim of good medicine is to help the patient to the greatest extent, with the minimum of side effects. Therefore, it is good practice to use whatever complementary therapies seem best indicated.
Analysis of the database indicates that points from the list: LI04,11;
ST25,36; SP06; HT07; BL23,40; PC06; TH05; GB20,34; LV03; CV06,12; GV04,12,14,20,26 arise in a high proportion of cases. In complex cases, if one has difficulty in deciding on a prescription, it is advisable to include a few points from that list.
LIMITATIONS OF COOKBOOK AP: How would one treat the following syndrome? The patient had the following symptoms (at different times) during a period of 6 years, beginning two years after radical right lung surgery: recurrent haemorrhagic nephritis; cystitis; right-sided sciatica; right- sided paravertebral pain (C6 - T4 area); right-sided headache and bouts of acute conjunctivitis (right); right ear tinnitus; waking at

night with severe pain along the SI Channel of the arm to the little finger, with the arm in spasm.
To try cookbook prescriptions in such a case would be second-rate AP. There was obviously a connection between all these symptoms (all relate to SI, BL, KI) and most were right sided symptoms. On examination, the patient's thoracotomy scar was badly twisted, with adhesions on the right BL line. This was the clue. Blockage of the Qi flow (traditional concept) or reflex irritation effects (Western concept) could cause all of these symptoms via the Chinese SI-BL-KI energy cycle. Treatment was physiotherapy + injection of the scar plus a few AP sessions using BL points. All symptoms were successfully cleared. Cookbooks have their limitations and Chefs do not need them.
CONCLUSIONS
Cookbooks or computerised prescribing is very valuable for beginners and for those working in a clinic. However, one should not rely too much on machines or computers. Computers need electrical power. In national disaster and warfare, and in many of the developing countries, electrical power, batteries etc may be unavailable where they are needed most. Therefore, it is important for the development of medicine and veterinary medicine that as many professionals as possible should study the basics of AP. This learning process can be accelerated by interaction with a computerised database (Rogers 1984a). Adequate knowledge of AP will enable it to be used more widely in field work (large animal work, medics and paramedics in the bush).
Although the data reported here (Appendices 1,2,3) are but a small fraction of the database, it is obvious that for most conditions, the Top Ten Points usually will be worth considering. However, in some complicated cases, points not in the Top Ten may be most relevant. The statistical method is very useful for population medicine, but it may be disastrous for the unfortunate patients who need individually designed care.
As a general rule, if a Cookbook prescription does not produce definite results by 2-3 sessions, it is necessary to (a) change the choice of points, or (b) consider other therapies, or (c) regard yourself as unable to assist.
The enthusiastic amateur AP practitioner will get useful results with the COOKBOOK but more complicated or deeply rooted problems require more holistic (traditional + modern + complementary + intuitive) therapy. Therefore, I strongly encourage you to continue your study of Chinese AP in depth. To get the best results, use the cookbook as the first-line of attack (in conditions amenable to AP) but be prepared to fall back on traditional and other methods if results do not follow quickly (Rogers 1984b). This assumes that the user is trained in basic AP and is able to interpret the point selections.

When using the prescriptions given in this paper, please note (a) the number of references in the prescriptions, (b) the maximum possible score, (c) the score of each point in the list (calculated by ratio to the maximum possible score), and (d) the variation in scores between points. If there are few references, the prescription may be of doubtful value. If the maximum possible score is (say) .90 and the max. score for any point is (say) less than .40, the prescription may be doubtful. If there is little variation between the scores and all scores are greater than .40, various combinations of points should be equally effective.
Remember that the best prescriptions usually combine AhShi points, LOCAL points, DISTANT points and (if internal organs are involved) Mu + Shu + Yuan + Luo combinations. Thus, the wheel turns full circle. The traditional methods of point selection were best after all. Modern technology has merely re-invented the wheel !
CHOICE OF POINTS IN AP THERAPY
Rogers 1987 lists the methods of choosing points for the treatment of human back pain. Similar points and reasoning are used in animals. The points depend on the organs and parts involved. The most common combination of points is: all TPs, plus 1-2 LOCAL points (near the affected organ or part), plus 1-2 DISTANT points on meridians passing through, near or related to the affected parts. If an organ is thought to be involved, its SHU point is used, whether tender or not. To this can be added the MU (abdominal alarm) point.
In low-backpain patients, GB30, 34 and BL54, 60 are useful distant points. In animals, the lumbo-sacral space is called PAIHUI. (In humans, PAIHUI (VG20) is on the top of the head).
The combination of TPs, PAIHUI, BL23, 26, 30, 54, 60, GB30, 34, covers most backpain below the ribs, including radiating sciatic pain. The combination of TPs, BL13, 16, 21, TH15, SI 9 covers most thoracic backpain. The combination of TPs, GB20, 21, TH15, CO17, ST38 (or GB34) covers most neck pain.
Other useful points are:
PAIHUI (all problems below the ribs); BL11 (joints); BL16 (spinal column); CO 4 (forelimb & general effects); BL21, ST36 (hindlimb, appetite and general effects); ST44 (hindlimb); TH 5 (forelimb); GB34 (hindlimb, muscles, tendons, neck, shoulder and elbow); BL23 (lumbo- sacral and hindlimb; adrenal point, stress conditions; ovary/kidney/Vitamin D/para-
thyroid/bone point and general effects).
However, many point combinations are possible. Examples of these are given below and the locations are shown in attached figures.
METHODS USED IN AP THERAPY

Simple needling: In horses, special AP needles or hypodermic needles 19-26 gauge, 2-6 inches long are used. In dogs, human AP needles or hypodermic needles 26-30 gauge, 0.5-2 inches long are used. Sterile needles are inserted into the points. Cleansing of the skin before insertion of the needle is a cosmetic exercise unless the skin is wet or visibly dirty. The needles are left in situ for 20 minutes. Twirling and pecking of the needle is done every few minutes. Cases are treated at intervals of 1 - 2 days in acute or 3 - 7 days in chronic cases. Acute cases may require 1 to 3+ sessions to recovery. Chronic cases may need 1 to 10+ sessions.
Electroneedling: Needles are inserted as usual. Output leads from special electrostimulators are used to deliver electrical stimuli to the needles. Session length and intervals between sessions are as for simple needling. An advantage claimed for electro-AP is that it requires fewer sessions. This, however, is doubtful. Strong, painful needle manipulation is as good as electro-AP, but electro-AP leaves the operator free to talk, take notes etc. In cases of paralysis and in severe pain, electro-AP may be better than simple needling. White suggests electro-AP treatment every 12-24 hours in acute cases with severe pain or paralysis. Electro-AP is also the usual method used to obtain AP analgesia for surgery in animals.
Point injection: This is an effective, rapid and safe method in horses and dogs. It is very useful in busy practice. In horses, 1-5 ml is injected at each point; in dogs, .5-1.5 ml. The solution may be .5-1.0% procaine in saline, saline alone, saline-B12, Impletol, homoeopathic solutions etc. Choice of solution depends on practitioner preference- all methods are used. Point injection also allows the use of drug-therapy, when needed. The Dermojet (high-pressure skin injector) is also used.
Massage: It shortens recovery time if animal handlers are shown the techniques of massage. TPs and other important AP points can be marked or clipped. Massage for 2 minutes/point every 1-2 days between AP sessions is very useful. In the horse, I demonstrate massage by fist-pounding to the horse's tolerance. In the dog, I demonstrate deep massage with the thumbs (for spinal areas) or other methods for limb muscles.
Ultrasound: Standard equipment may be used. Different probes are available for diifferent parts- body surface, orifices etc. A contact jelly is essential. Output is .25-1.0 watts. Time 15-60 seconds/point. The method is painless and non-invasive but is not as well documented as the needling or injection methods.
LASER: Low power laser (1-5 mW) and higher power (5-10 mW) has been used in horses and dogs instead of needling. Three types are common: He-Ne (632 nm wavelength), infrared (902 nm) and diode lacers (not true laser light). Laser is painless and non-invasive but its penetration is shallow. It is not possible to assess laser effectiveness at this time.
Some users report excellent results (for instance Martin and Klide 1987) in backpain in the horse but others say the laser is not as good

as needling. All agree that laser is excellent for local (superficial) problems, such as septic wounds, tendonitis, granulomas, ulcers, eye problems etc. It may be useful in Earpoint AP. However, at this time, Earpoint AP is also not as well documented as classical AP and TP therapy.
Implants: Skin staples, implant of sutures, platinum-, gold- or surgical beads or wire can be used to stimulate the AP points. Klide has used implants effectively to control epilepsy in dogs. Cain has used them to control nervousness in fillies. Others have used them in backpain and other conditions. They are very effective (implants around the acetabulum) in treating hip dysplasia in dogs. However, the method needs more documentation before acceptance as a routine procedure.


















![Conflict in the Workplace [ACU MACRR]](https://img.pdfslide.us/doc/110x75/55a9b8eb1a28abd5488b465b/conflict-in-the-workplace-acu-macrr.jpg)