Embed Size (px)
Citation preview

ACTIVMOTION
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
GENERAL THEORY
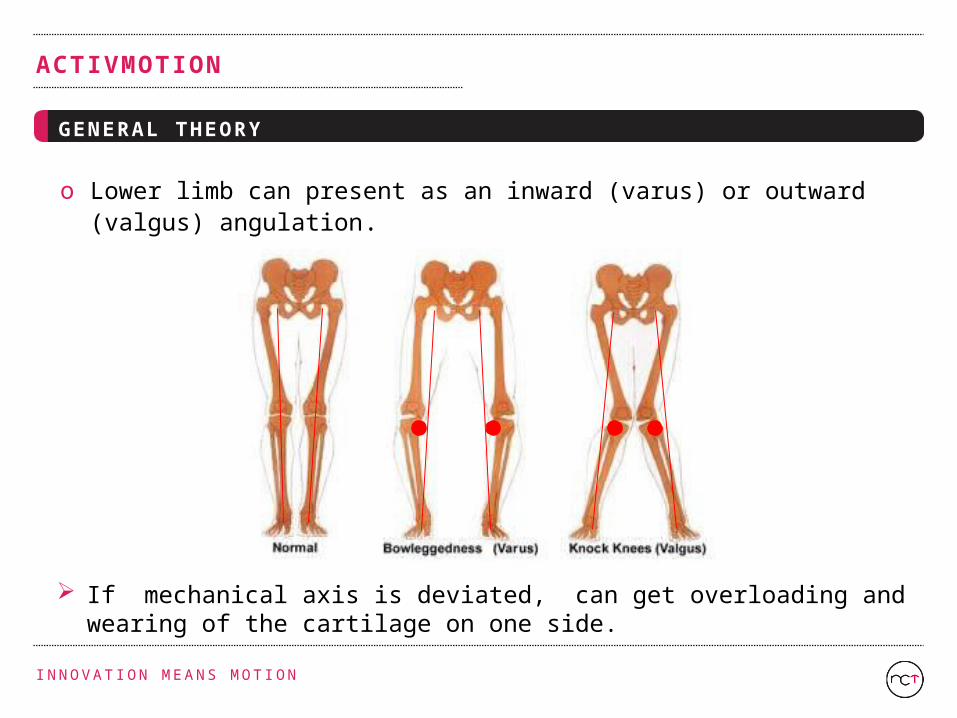
o Lower limb can present as an inward (varus) or outward (valgus) angulation.
If mechanical axis is deviated, can get overloading and wearing of the cartilage on one side.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
GENERAL THEORY
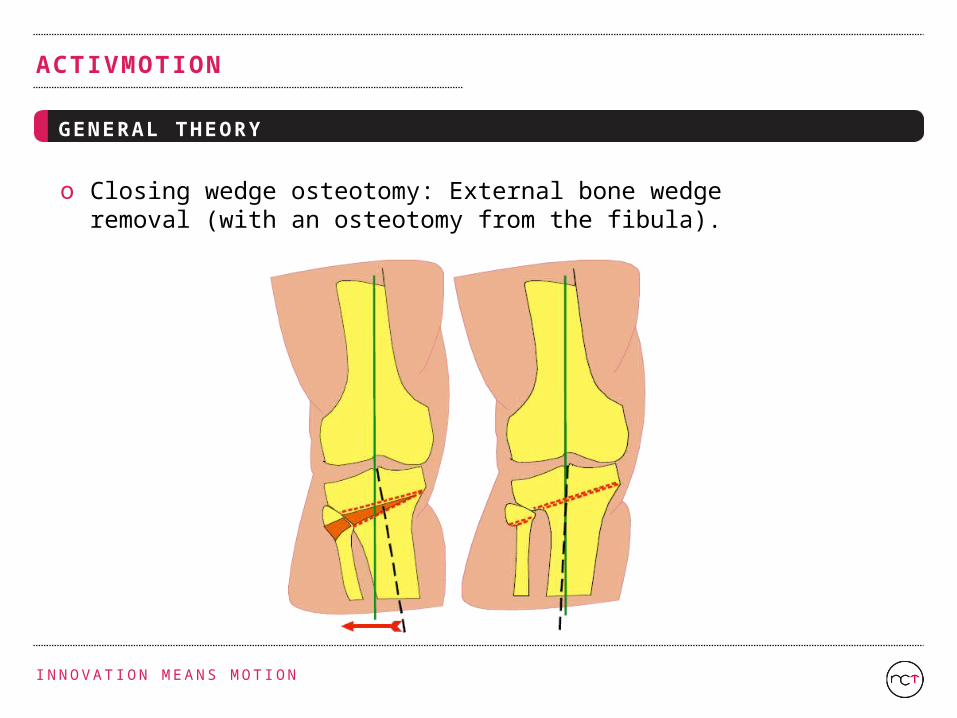
o Closing wedge osteotomy: External bone wedge removal (with an osteotomy from the fibula).
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
GENERAL THEORY
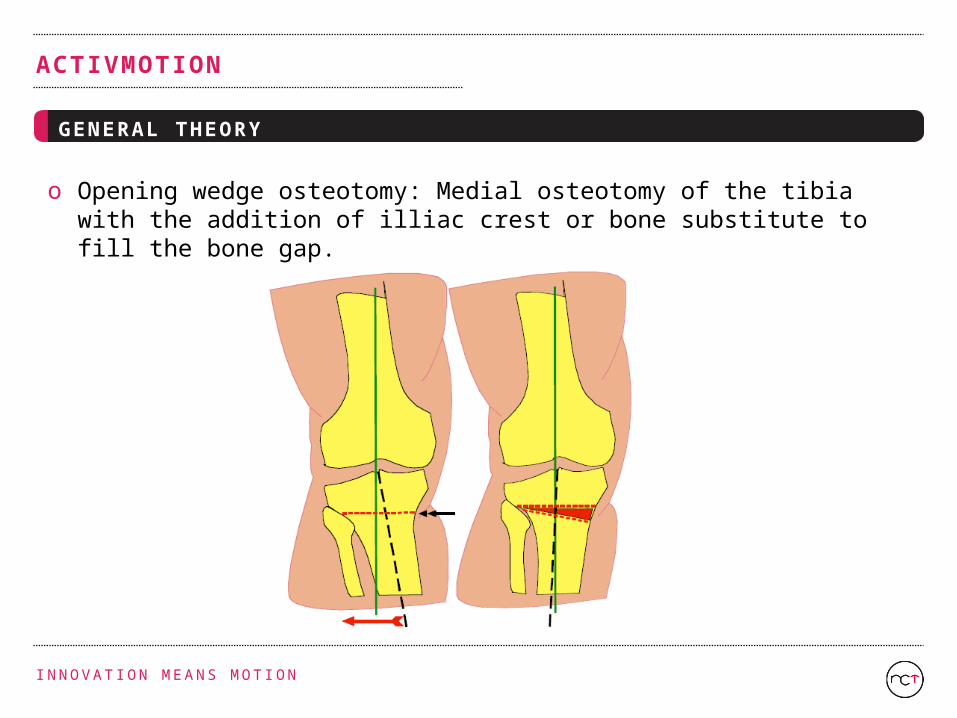
o Opening wedge osteotomy: Medial osteotomy of the tibia with the addition of illiac crest or bone substitute to fill the bone gap.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
STRESS DISTRIBUTION IN A HEALTHY KNEE
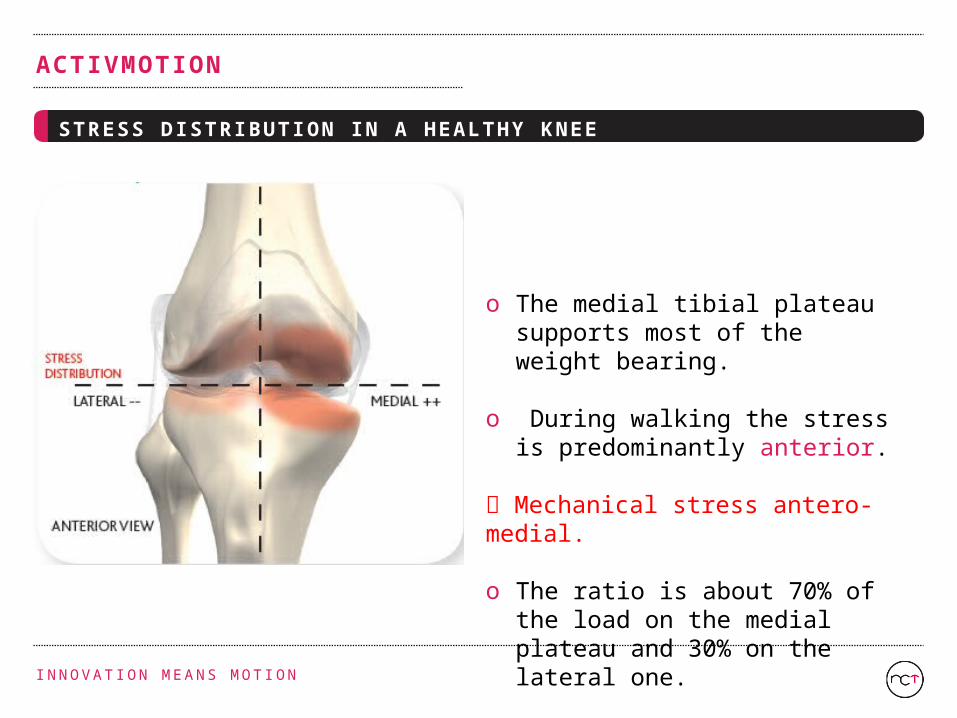
o The medial tibial plateau supports most of the weight bearing.
o During walking the stress is predominantly anterior.
Mechanical stress antero-medial.
o The ratio is about 70% of the load on the medial plateau and 30% on the lateral one.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
STRESS DISTRIBUTION IN A HEALTHY KNEE
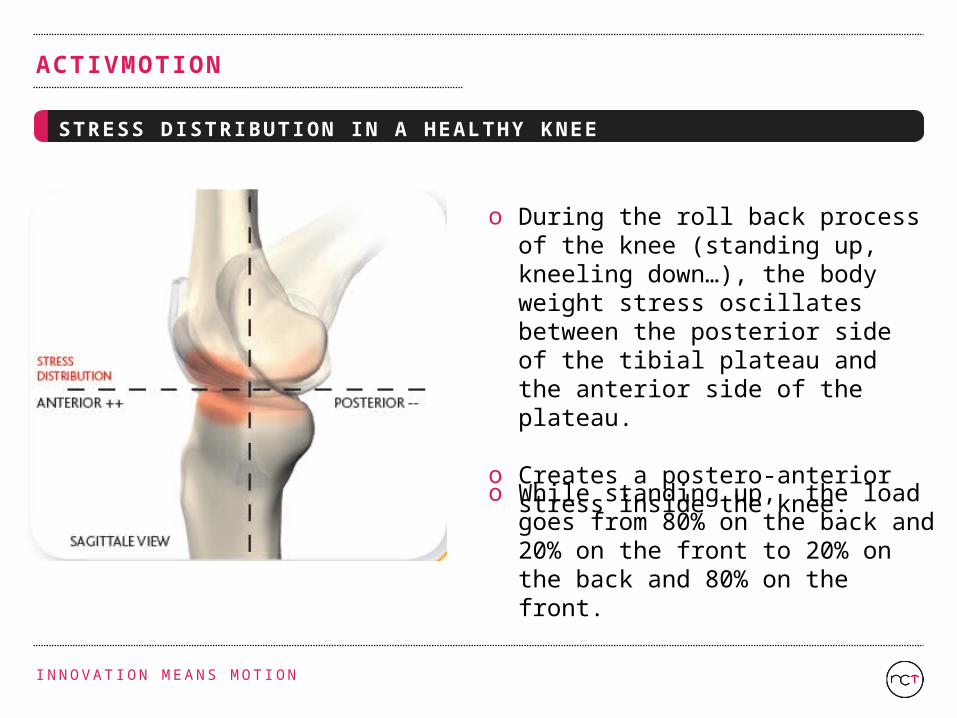
o During the roll back process of the knee (standing up, kneeling down…), the body weight stress oscillates between the posterior side of the tibial plateau and the anterior side of the plateau.
o Creates a postero-anterior stress inside the knee.
o While standing up, the load goes from 80% on the back and 20% on the front to 20% on the back and 80% on the front.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
STRESS DISTRIBUTION IN A KNEE IN VARUS
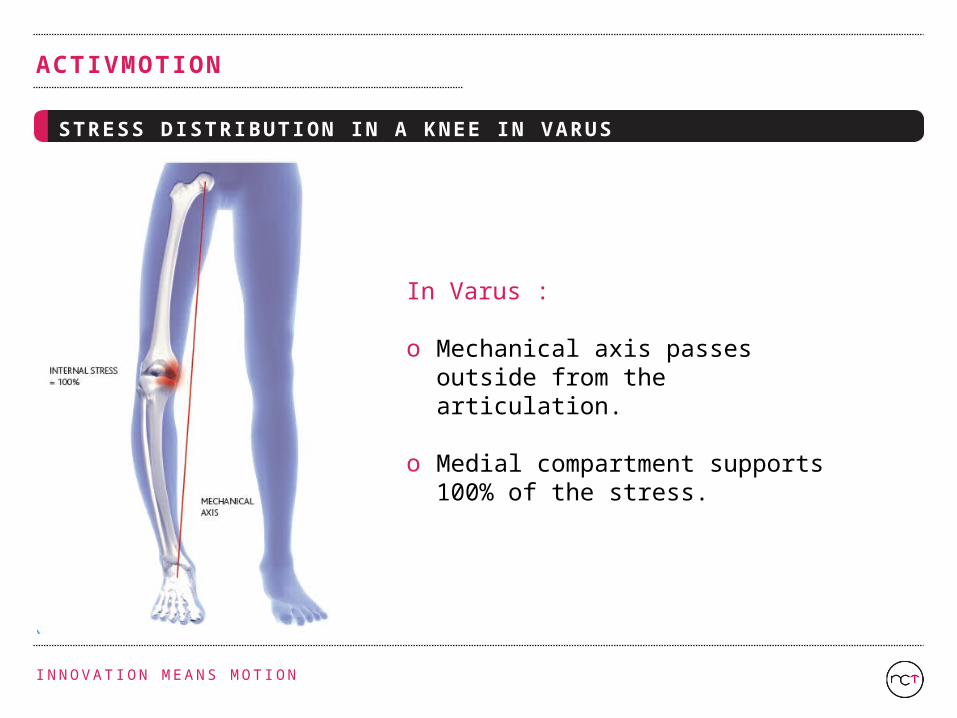
In Varus :
o Mechanical axis passes outside from the articulation.
o Medial compartment supports 100% of the stress.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
STRESS DISTRIBUTION IN A KNEE IN VARUS
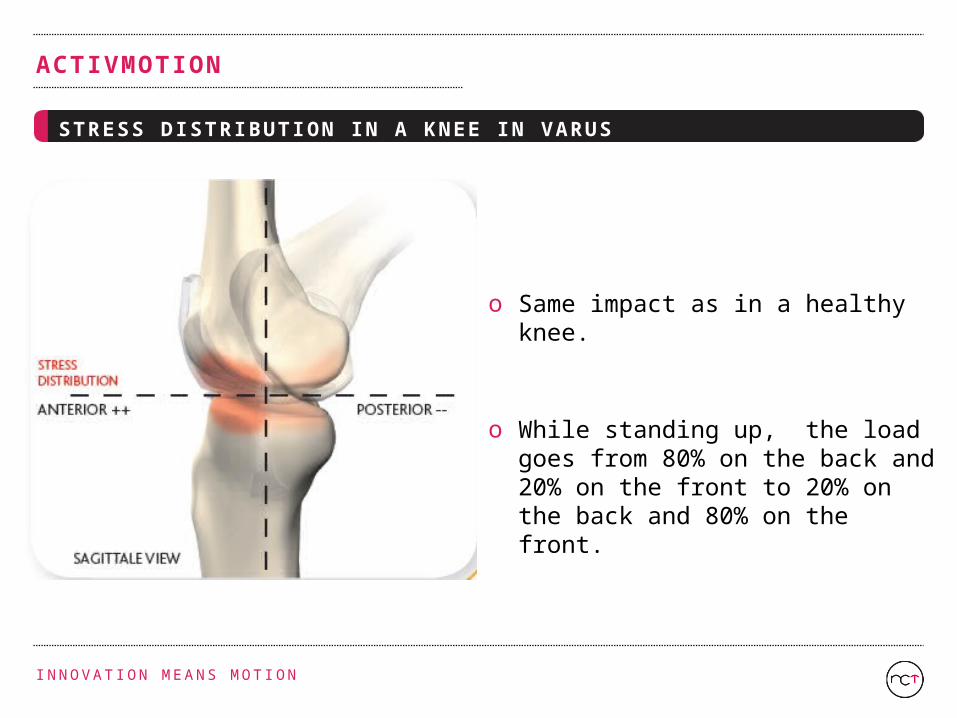
o Same impact as in a healthy knee.
o While standing up, the load goes from 80% on the back and 20% on the front to 20% on the back and 80% on the front.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
STRESS DISTRIBUTION IN A CORRECTED KNEE
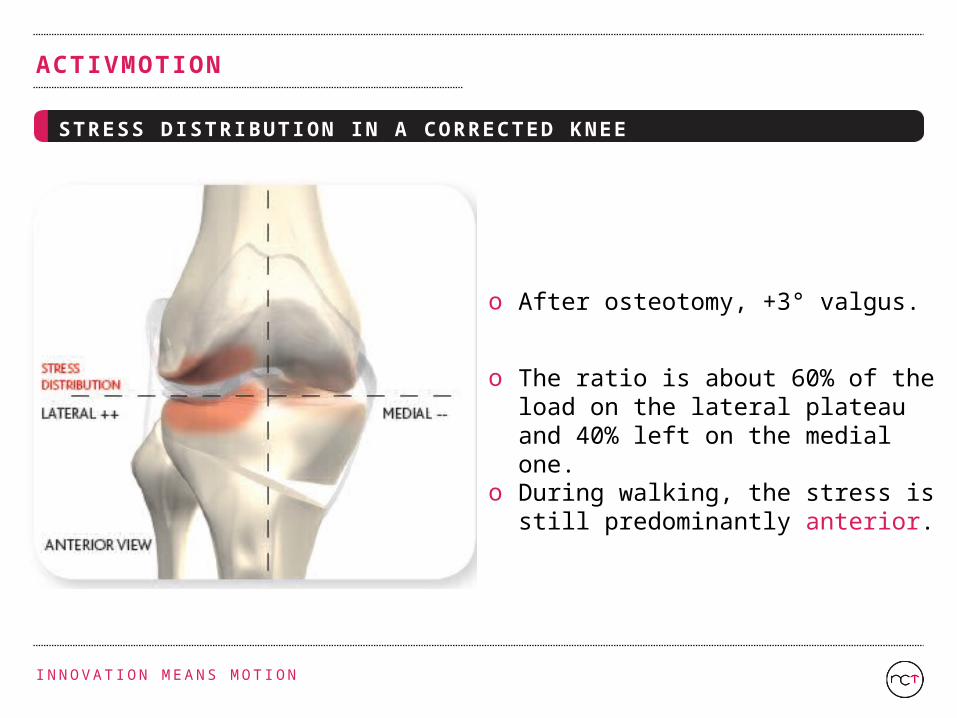
o The ratio is about 60% of the load on the lateral plateau and 40% left on the medial one.
o After osteotomy, +3° valgus.
o During walking, the stress is still predominantly anterior.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
STRESS DISTRIBUTION IN A CORRECTED KNEE
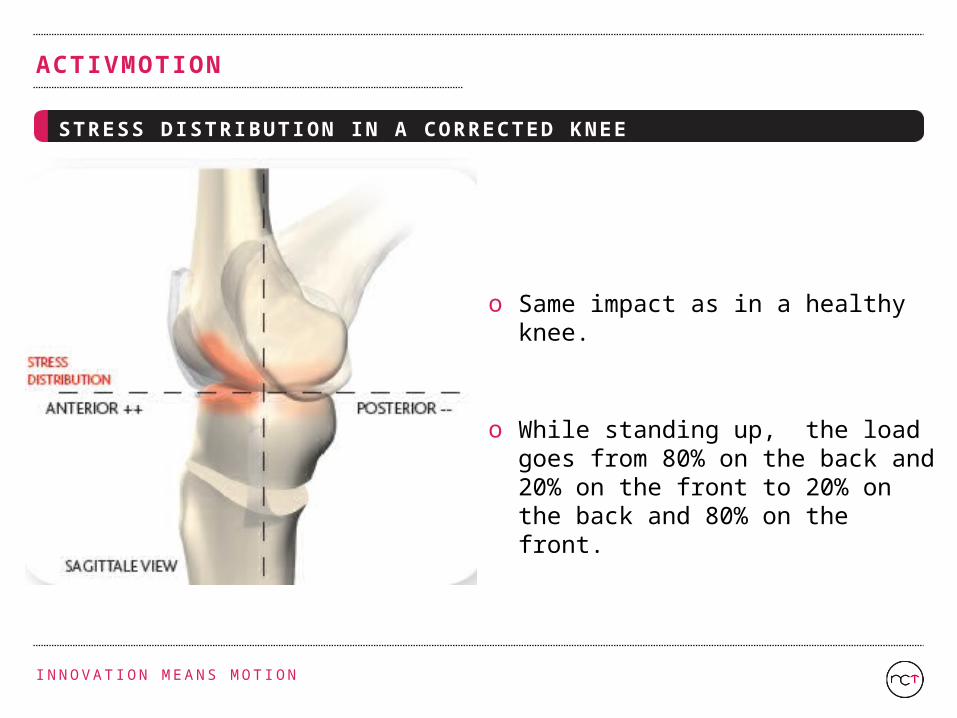
o Same impact as in a healthy knee.
o While standing up, the load goes from 80% on the back and 20% on the front to 20% on the back and 80% on the front.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
NEWCLIP ’S TECHNOLOGY AS PROBLEM SOLVER
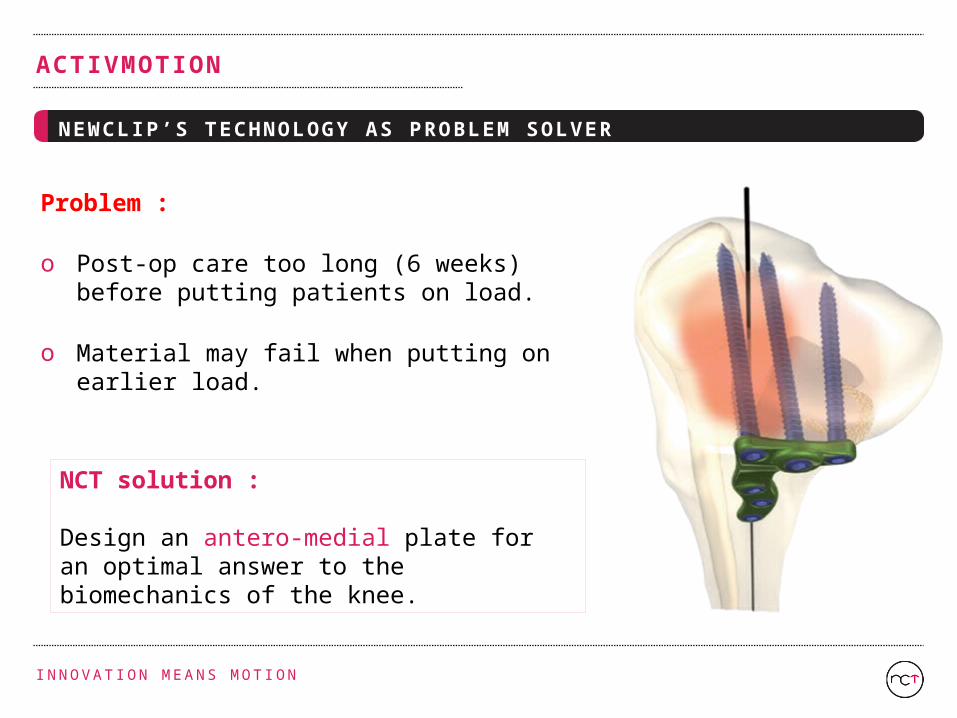
Problem :
o Post-op care too long (6 weeks) before putting patients on load.
o Material may fail when putting on earlier load.
NCT solution : Design an antero-medial plate for an optimal answer to the biomechanics of the knee.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
ACTIVMOTION CONCEPT
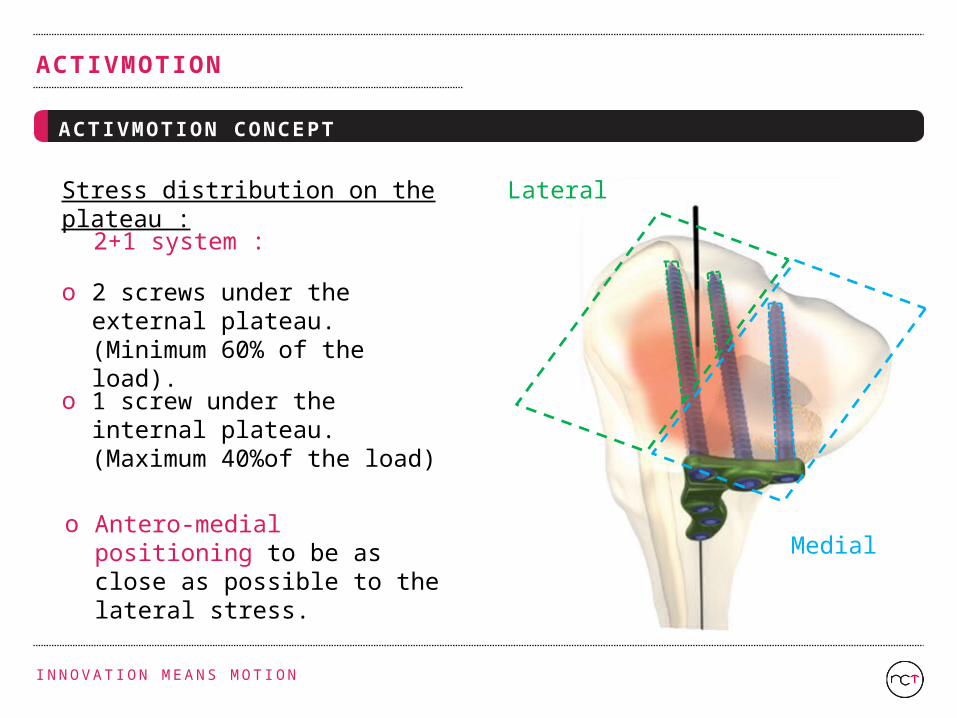
Stress distribution on the plateau :
o 2 screws under the external plateau. (Minimum 60% of the load).
o 1 screw under the internal plateau. (Maximum 40%of the load)
Lateral
Medial
2+1 system :
o Antero-medial positioning to be as close as possible to the lateral stress.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
STRESS ABSORPTION
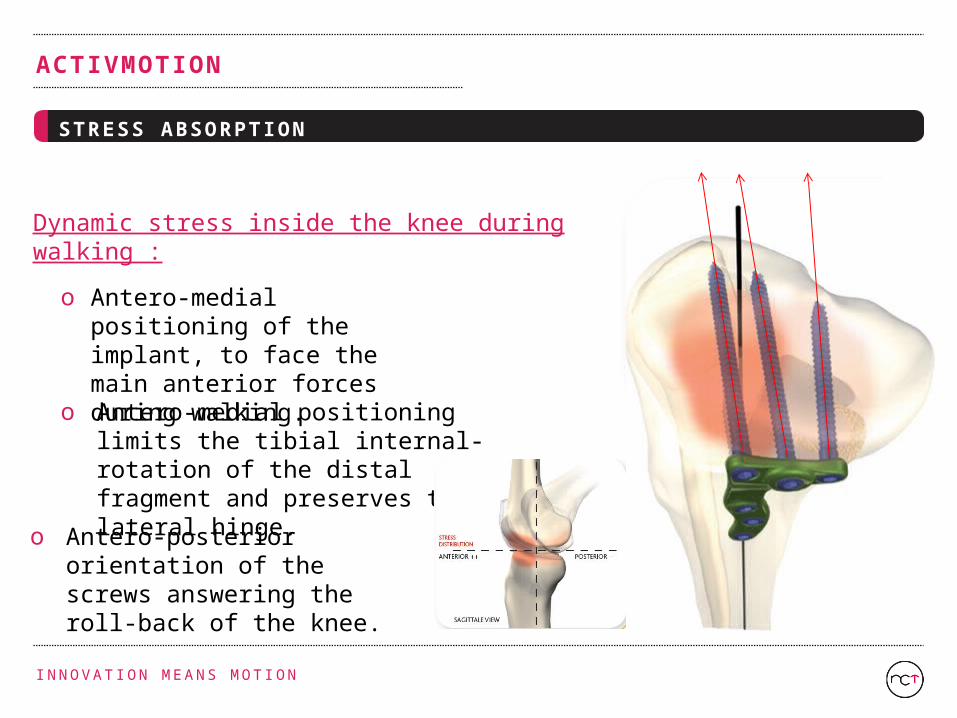
Dynamic stress inside the knee during walking :
o Antero-medial positioning of the implant, to face the main anterior forces during walking.
o Antero-posterior orientation of the screws answering the roll-back of the knee.
o Antero-medial positioning limits the tibial internal-rotation of the distal fragment and preserves the lateral hinge.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
STRESS ABSORPTION : SUMMARY
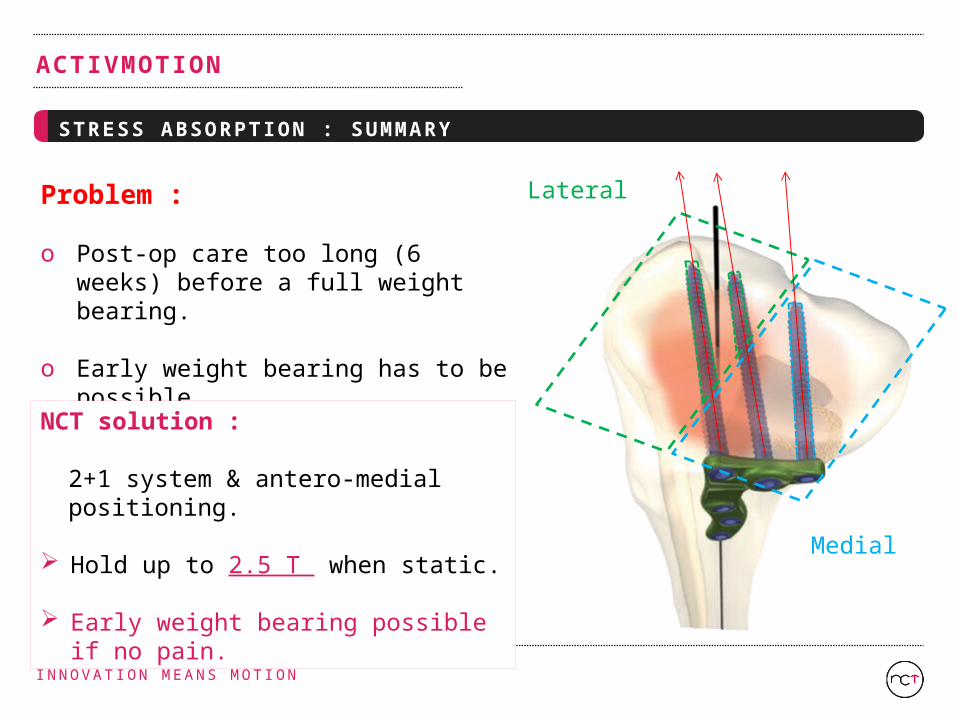
Problem :
o Post-op care too long (6 weeks) before a full weight bearing.
o Early weight bearing has to be possible.
NCT solution :
2+1 system & antero-medial positioning.
Hold up to 2.5 T when static.
Early weight bearing possible if no pain.
Lateral
Medial
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
NEWCLIP ’S TECHNOLOGY AS PROBLEM SOLVER
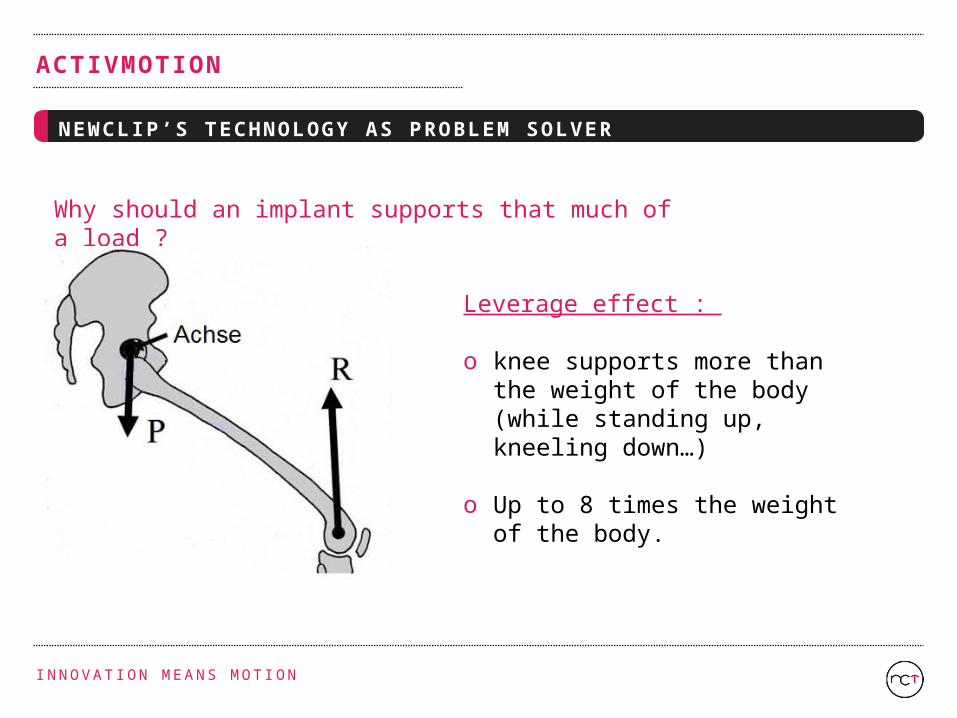
Why should an implant supports that much of a load ?
Leverage effect :
o knee supports more than the weight of the body (while standing up, kneeling down…)
o Up to 8 times the weight of the body.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
NEWCLIP ’S CONCEPT : SOLVING THE PROBLEM
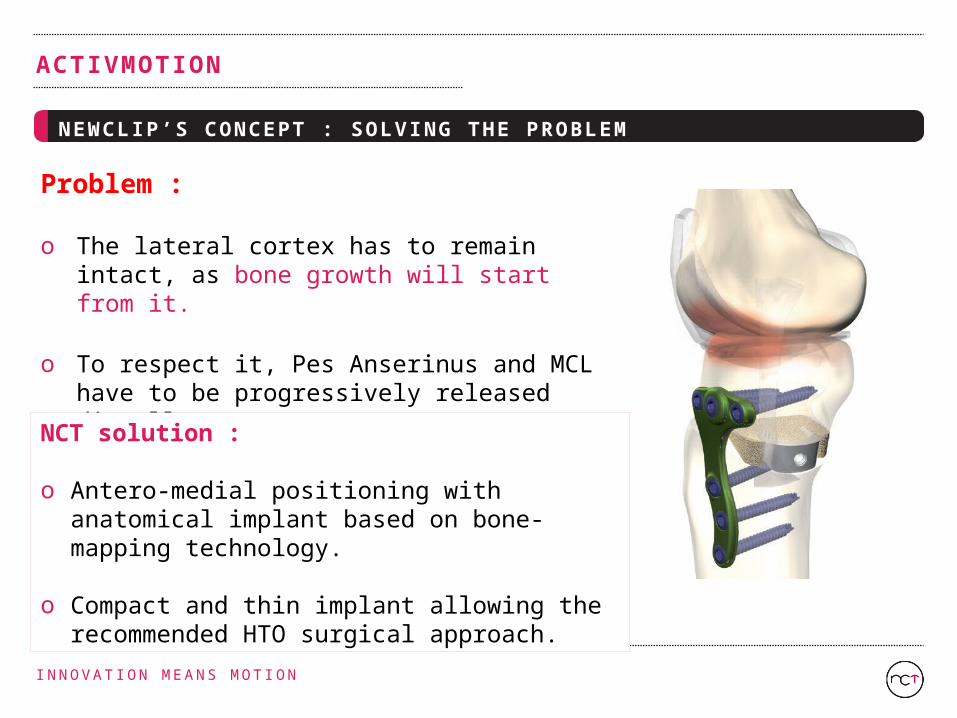
Problem :
o The lateral cortex has to remain intact, as bone growth will start from it.
o To respect it, Pes Anserinus and MCL have to be progressively released distally.
NCT solution :
o Antero-medial positioning with anatomical implant based on bone-mapping technology.
o Compact and thin implant allowing the recommended HTO surgical approach.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
HTO & ACL RECON
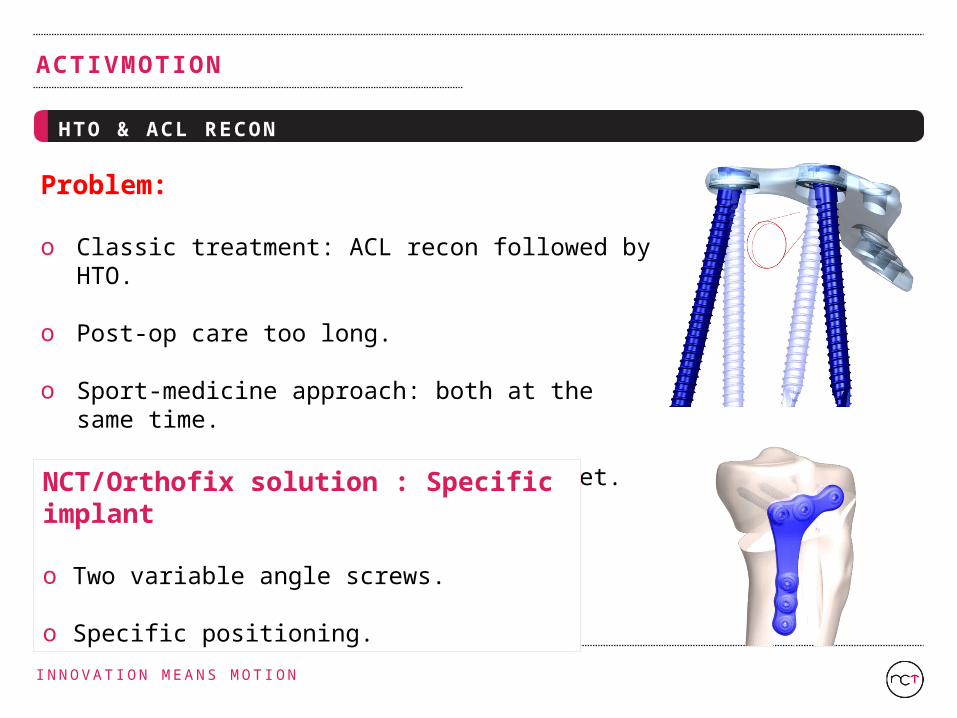
Problem:
o Classic treatment: ACL recon followed by HTO.
o Post-op care too long.
o Sport-medicine approach: both at the same time.
o No specific HTO implant on the market.
NCT/Orthofix solution : Specific implant
o Two variable angle screws.
o Specific positioning.

I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SURGICAL APPROACH
o An 8-cm slightly oblique vertical incision is made along the antero-medial surface, running over the joint space down to under the tibial tuberosity.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SURGICAL APPROACH
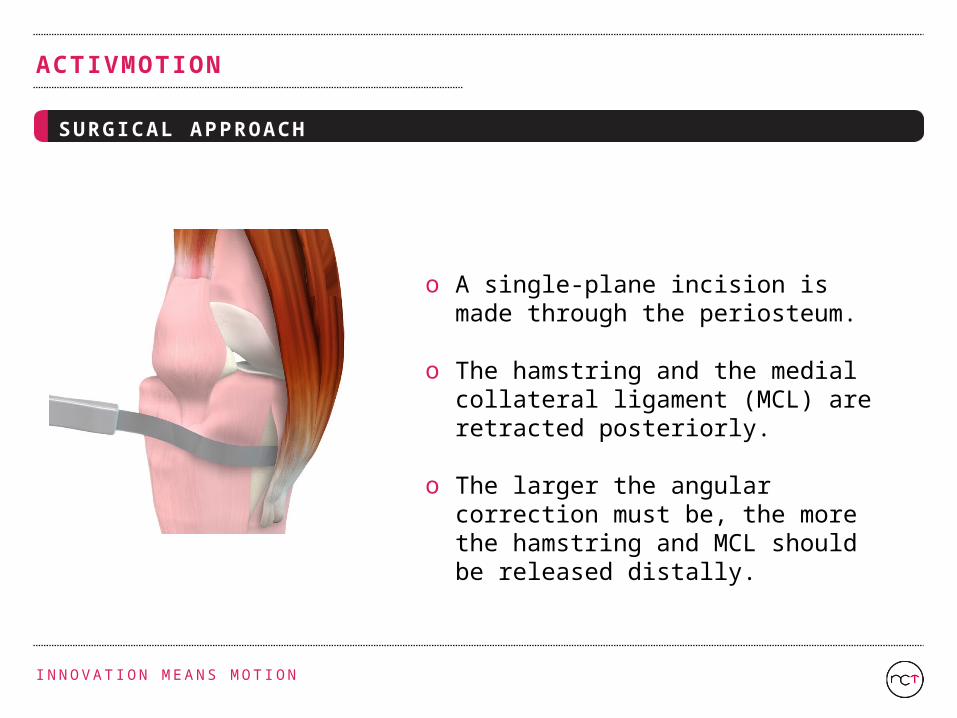
o A single-plane incision is made through the periosteum.
o The hamstring and the medial collateral ligament (MCL) are retracted posteriorly.
o The larger the angular correction must be, the more the hamstring and MCL should be released distally.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SURGICAL APPROACH
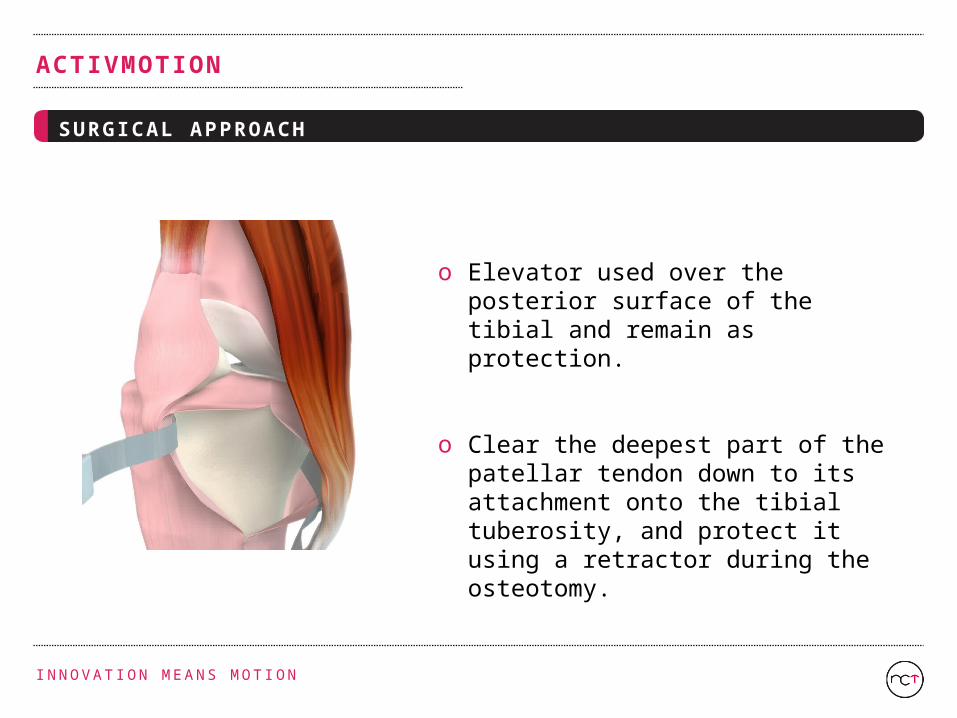
o Elevator used over the posterior surface of the tibial and remain as protection.
o Clear the deepest part of the patellar tendon down to its attachment onto the tibial tuberosity, and protect it using a retractor during the osteotomy.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SURGICAL TECHNIQUE
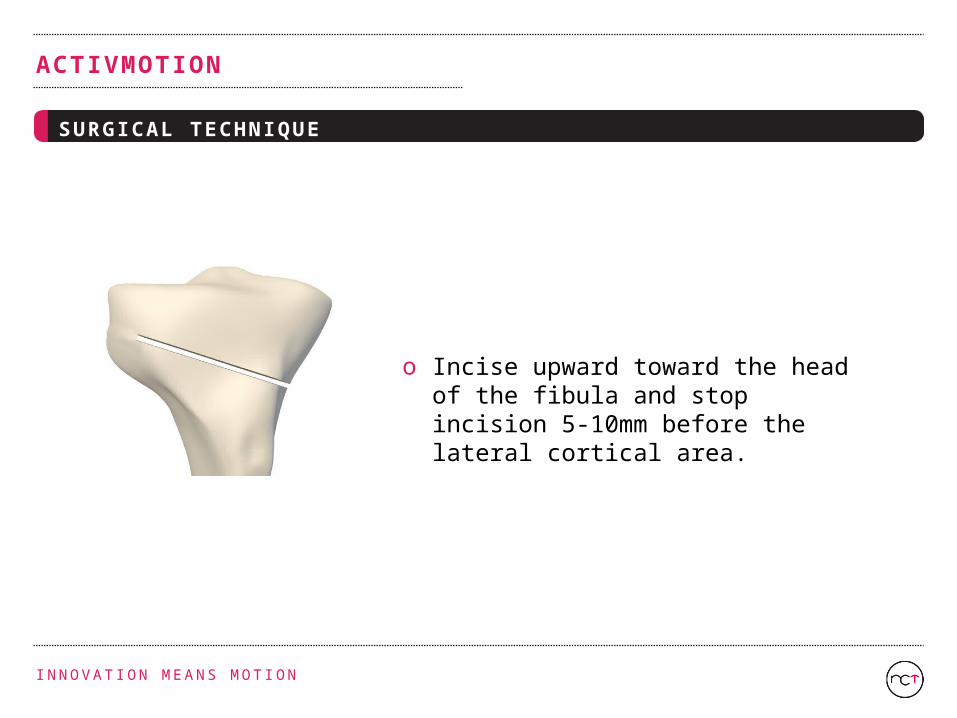
o Incise upward toward the head of the fibula and stop incision 5-10mm before the lateral cortical area.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SURGICAL TECHNIQUE
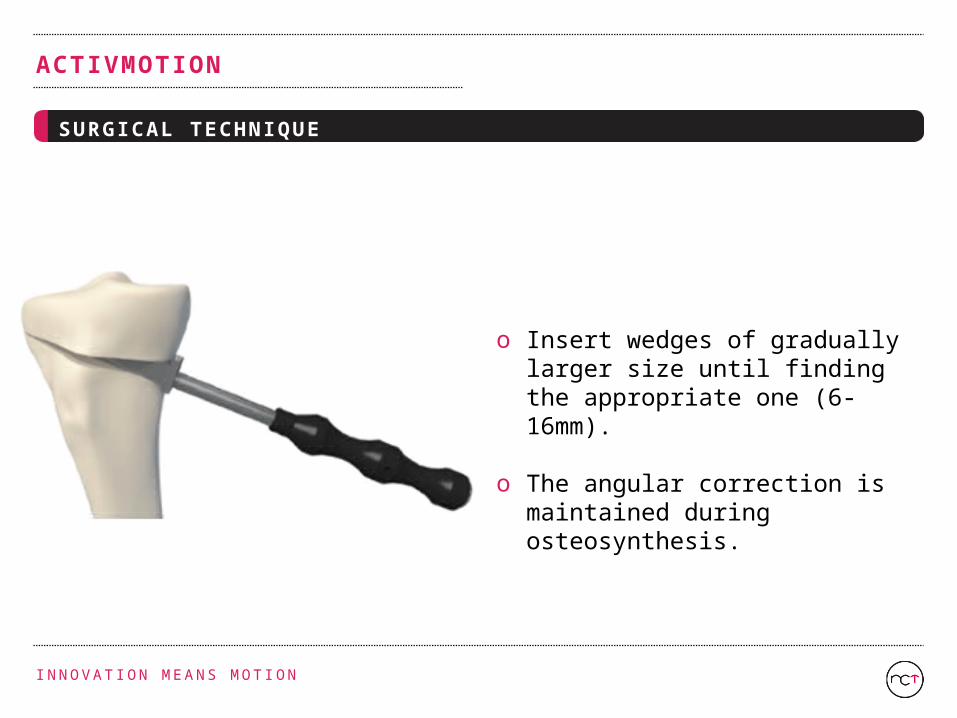
o Insert wedges of gradually larger size until finding the appropriate one (6-16mm).
o The angular correction is maintained during osteosynthesis.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SURGICAL TECHNIQUE
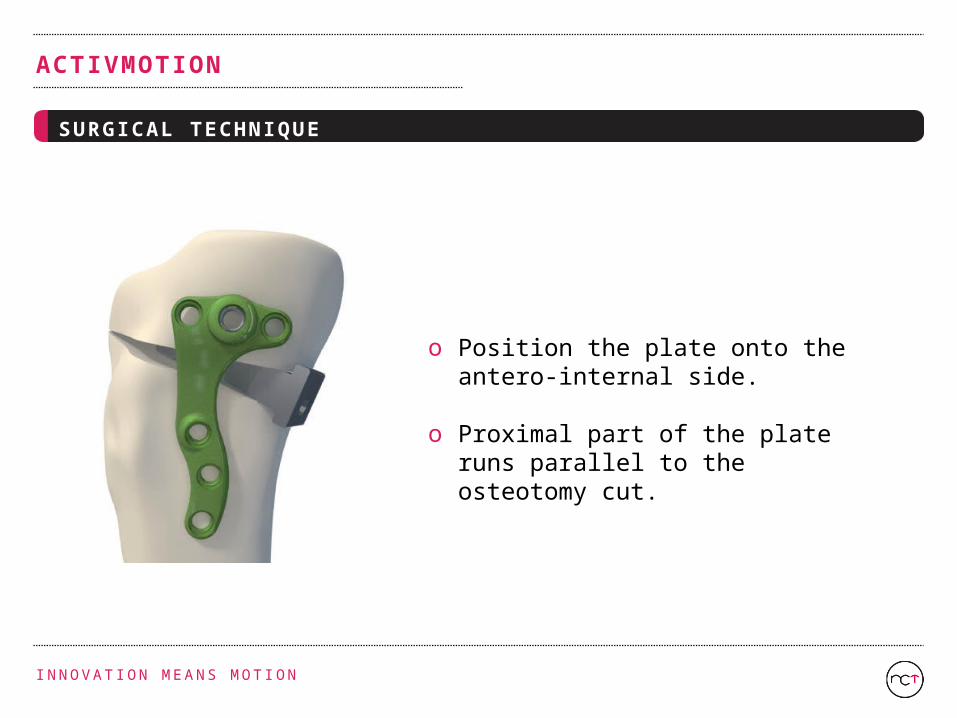
o Position the plate onto the antero-internal side.
o Proximal part of the plate runs parallel to the osteotomy cut.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SURGICAL TECHNIQUE
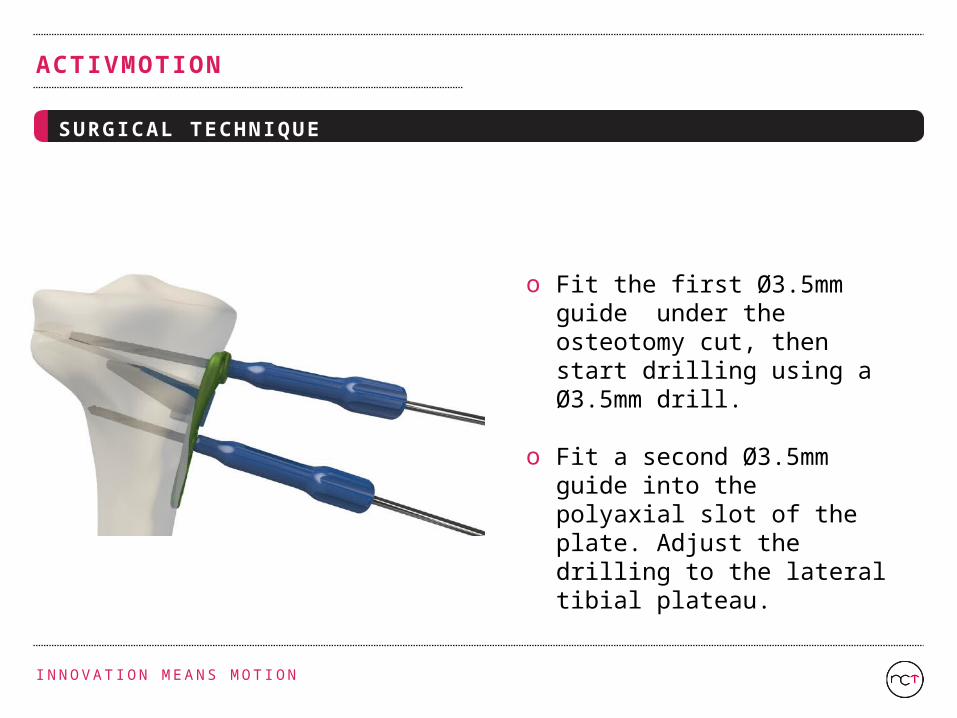
o Fit the first Ø3.5mm guide under the osteotomy cut, then start drilling using a Ø3.5mm drill.
o Fit a second Ø3.5mm guide into the polyaxial slot of the plate. Adjust the drilling to the lateral tibial plateau.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SURGICAL TECHNIQUE
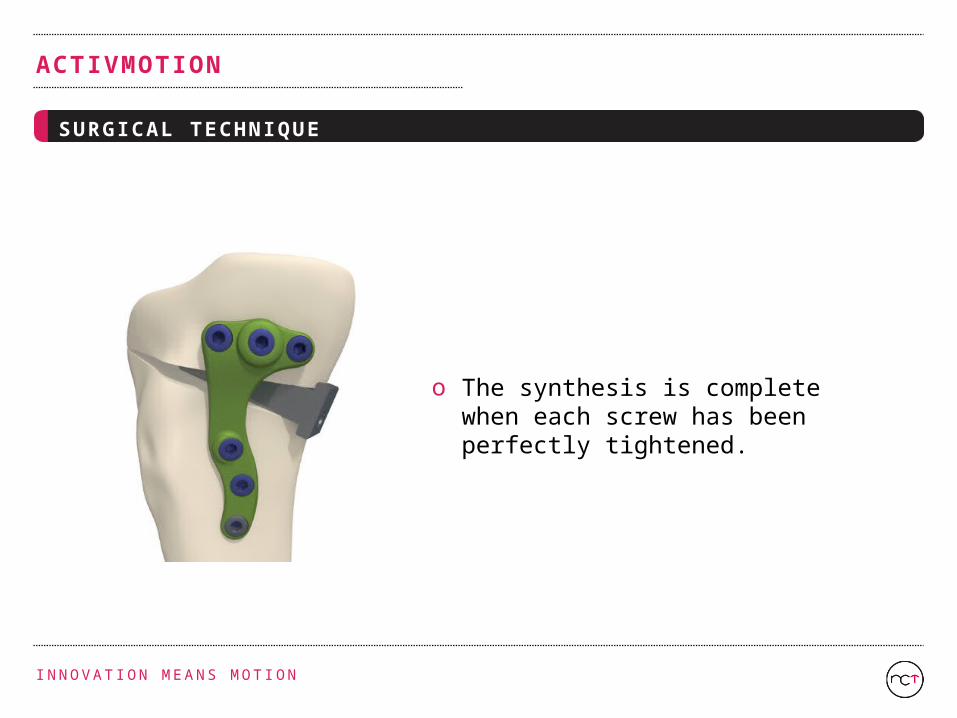
o The synthesis is complete when each screw has been perfectly tightened.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SURGICAL TECHNIQUE
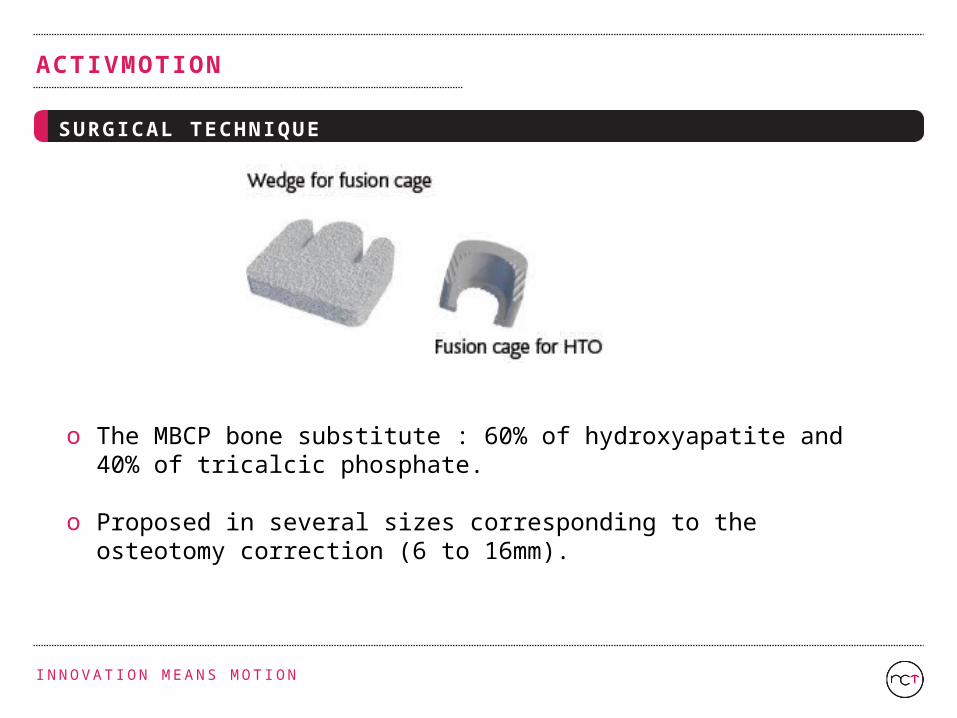
o The MBCP bone substitute : 60% of hydroxyapatite and 40% of tricalcic phosphate.
o Proposed in several sizes corresponding to the osteotomy correction (6 to 16mm).
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SURGICAL TECHNIQUE
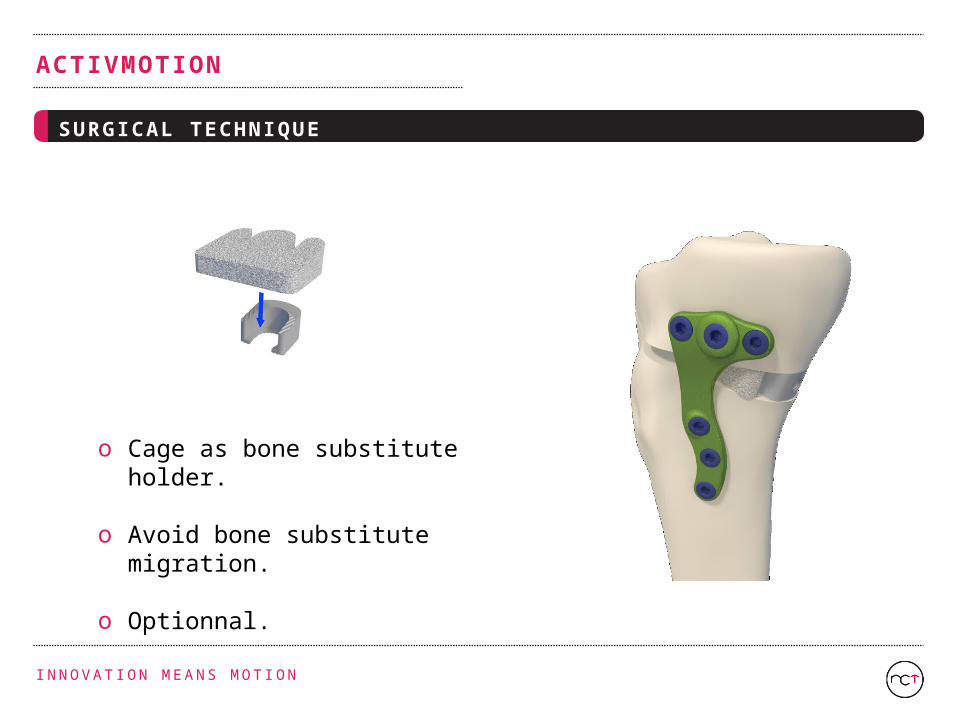
o Cage as bone substitute holder.
o Avoid bone substitute migration.
o Optionnal.
I N N O VAT I O N M E A N S M O T I O N
ACTIVMOTION
SUM UP
NCT innovation :
o 2 + 1 system.2 screws under external plateau, 1 screw under internal plateau for better weight bearing load care.
o Antero-internal positioning of the plate. orientation of the screws in the direction of the postero-anterior roll-back induced stress.
o Low profile implant Doesn’t interfere with the hamstring ligaments, patient don’t feel it under-skin.
o Combination of ACL reconstruction and HTO.Specific implant that leave room for the tunnel.