Embed Size (px)
Citation preview

Active surveillance in prostate cancer
Dr John YaxleyUrological & robotic surgeon

Active Surveillance
“I hate doctors –They find things wrong with you!!”

Disconnect between the histological phenotypeand the historic clinical perception of a deadly disease

Active surveillance
Active surveillance is delayed curative treatment at the time of significant local progression
Limits adverse effects from treatment and maintains quality of life


Ongoing controversy....


PSA testing saves few lives and leads to risky and unnecessary treatments for large numbers of men.
Healthy men don’t need PSA testing for prostate cancer, panel says
Study: Surgery for early prostate cancer doesn't save lives

Eur Urol. 2013 ;63:428-35
15
Most men with curable disease who are untreated do not die within 10 years

PSA screening
Recent advances in prostate cancer detection, including PSA screening have diminished the incidence of high volume and aggressive tumours, with a stage shift to lower volume, lower stage cancer
PSA screening has been associated with a decrease in prostate cancer mortality
Many low grade cancers are unlikely progress to clinical symptoms and pose limited risk of death if left untreated

PSA screening
Despite its limitations, PSA has lead to a higher number of curable presentations
Randomised ERSPC study showed 21% reduction in PC deaths at 11 years and the randomised Swedish (Goteborg) trial showed a 44% reduction in PC death in the PSA screened arm at 14 years.
NNT to prevent 1 death is 12

Eur Urol. 2013 ;63:428-35
15
If prostate cancer mortality is used as the end-point, the follow-up must be ≥ 20 years.
Most men with curable disease who are untreated do not die within 10 years

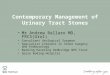
Cumulative risk of death from CaPGoetborg Study

Hitting the TargetUnnecessary
Surgery or radiotherapy
Unnecessary side effects of
impotence and
incontinence
Cure of Clinically
Significant Prostate Cancer

Active surveillance
The long term outcome of active surveillance depends on the ability to initiate delayed intervention when required, but avoid overtreatment in those who do not require it
Prostate cancer kills over 3000 Australian men each year, more than women die from breast cancer

Active surveillance
Increasingly PSA screened tumours may resemble asymptomatic prostate cancer detected at autopsy who died from other causes
The high prevalence of prostate neoplasms compared to the low lifetime risk of PC death raises the concern about overtreatment of low volume, low grade prostate cancer

Prostate cancer Research International: Active Surveillance
Criteria for inclusion
1. Histological proven adenocarcinoma of the prostate 2. Men should be fit for curative treatment 3. Clinical stage T1C or T2 4. Gleason score 3+3=6 5. One or 2 biopsy cores invaded with prostate cancer 6. PSA density less than 0.2 7. PSA ≤ 10 ng/mL 8. Participants must be willing to attend the follow-up visits 9. Adequate biopsy sampling

Active surveillance
Canadian study of 452 men by Klotz showed 10 y.r survival rate of low risk prostate cancer on active surveillance is 97.2%
Klotz et el J Clin Oncol 2010;28:126-31
Randomised study in PSA era showed radical prostatectomy did not decrease death rate compared to observation over a median 10 yr. follow up period in men with low risk prostate cancer Wilt et el N Engl J Med 2102; 367: 203-13

Evidence for AS• 450 men observed with active surveillance. Definitive treatment offered to those with
PSA Doubling Time (DT) of <3 years, Gleason ≥ 4+3 or unequivocal clinical progression. 30% of patients were upstaged and offered definitive treatment
* Klotz L et al. J Clin Onc. 2010 Jan 1;28(1):126-31.
Parameters Klotz et al
Age (median) 70.3 years
Length of Active Surveillance (median)
6.8 years [range 1 to 13]
Pre-treatment PSA median level (ng/ml)
5 to 10 (48%)
Gleason grade 5: 11%6: 70%7: 17%

Evidence for AS
* Klotz L et al. J Clin Onc. 2010 Jan 1;28(1):126-31.

Active surveillance outcomes
Prospective active surveillance program of 1,298 men since 1995
Overall, cancer specific and metastasis specific survival at 15 years are 69%, 99.9% and 99.4% for Gleason 3+3 malignancy
Cumulative incidence of grade reclassification is 31% at 15 years
Cumulative incidence of curative intervention at 15 years is 57%Tosoian J, Epstein J, Carter H et el J Clin Oncol
Oct 20;33(30)3379-3385

Defining active surveillance
Usually a PSA every 3-4 months for 2 years then every 6 months
Repeat biopsies, starting a 12 months post diagnosis then every 2-3 years thereafter
DRE on a yearly basis
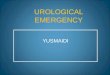
MRI now being evaluated / incorporated into protocols

Courtesy Professor Barentsz


MRI in active surveillance
3T MRI can detect significant prostate cancer in 90% of casesSmaledone J Urol
2010;183:138-43
Decreases the risk of under grading by 20-30% compared to standard 12 core TRUS
Hoeks et el 2012 Eur Urol 2012;62:902-9
Normal MRI may decrease the frequency of surveillance biopsies, especially if PSA stable

Why has prostate MRI improved ?
• 3T machine : Skyra at WMI• Addition of functional techniques to T2 WI• Improved sequencing protocols• Post processing software• PIRADS• Urologist – Radiologist collaboration
(>7000 mpMRI at WMI – 200/month)

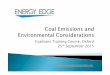
ADC Map b1400


DWI
Ca P → restricted water movement
→ Specificity
→ Indication of aggression
Tightly packed cellular tissue Organized glandular tissue

Gleason 3+3 on TRUSPlan for Active Surveillance
However lesion noted on MRI Target biopsy of lesion Gleason 4+5Patient proceeded to Robot RRP

Active surveillance outcomes
Systematic review of AS trials shows that the prostate cancer mortality risk is <3%, but the median follow up period of the studies is only 7 years.
Approximately one third of patients will require curative treatment during the follow up period for local progression, usually by radical prostatectomy Dall’Era et el Europ Urol 2012;61:1079-92

Triggers for intervention
Progression to higher grade or higher volume tumour on surveillance biopsy
PSA doubling time of < 3 years
Change in patient preference
Identify a significant lesion on MRI
Yaxley J et el Aus. Family Physician 42; Jan/Feb 2013, 74-76

69y low volume Gleason 3+3=6 prostate cancerOn active surveillance protocolMRI no significant tumour – ? avoid surveillance biopsies

64y PSA 6.9 and risingFocus Gleason 3+3 cancer – on active surveillanceAnterior tumour on MRI. - Gleason 3+4 on transperineal biopsy- proceeded to Robot prostatectomy

Novel biomarkers in active surveillance
PSA Isoforms
PCA 3
TMPRSS2:ERG
Oncotype DX prostate cancer assay
Others – kallikrein related peptidase 2, 4K score, CCP score (Polaris)

Conclusions
For patients with low risk prostate cancer, active surveillance is the preferred management stategy
For select patients, AS may be considered for low-volume Gleason 3+4 PC
Repeat biopsies showing higher grade or volume prostate cancer is a trigger for active treatment
More than half the patients remain on AS after >10 years follow up
Prostate cancer mortality risk at 10 years is <3%