Embed Size (px)
Citation preview

Active compression-decompression resuscitation: A hovel method of cardiopulmonary resuscitation
Chest compression is an important part of cardiopulmonary resuscitation (CPR), but it only aids circulation during a portion of the compression cycle and has been shown to only minimally increase blood flow to vital organs. The purpose of this study was to quantitate the short-term hemodynamic effects of CPR with a hand-held suction device that incorporates both active compression and decompression of the chest. The suction device was applied to the middle of the sternum and compared with standard manual CPR in eight nonventilated anesthetized dogs. Coronary perfusion pressure, systolic and diastolic aortic pressures, right atrial diastolic pressure, and the velocity time integral (an analog of cardiac output), which were obtained by means of transesophageal pulsed wave Doppler echocardiography from the main pulmonary artery, were measured every 30 seconds during CPR. Minute ventilation was measured over the last minute of each CPR technique. Both active compression-decompression CPR and standard CPR were sequentially performed for 2 minutes in random order 30 seconds after induced ventricular fibrillation. The CPR techniques consisted of 100 compressions per minute, with a compression depth of 1.5 to 2 inches and a 50% duty cycle. Coronary perfusion pressure, velocity time integral (cardiac output analog), minute ventilation, and systolic arterial pressure were all significantly improved by active compression-decompression CPR when compared with standard CPR. We conclude that active compression-decompression CPR is a simple technique that appears to improve coronary perfusion pressure, systolic arterial pressure, cardiac output, and minute ventilation in nonventilated animals when compared with standard CPR. Further research is necessary to determine the efficacy of this method in patients who are experiencing cardiac arrest. (AM HEART J 1992;124:1145.)
Todd J. Cohen, MD, Kelly J. Tucker, MD, Rita F. Redberg, MD, Keith G. Lurie, MD, Michael C. Chin, BS, John P. Dutton, BS, Melvin M. Scheinman, MD, Nelson B. Schiller, MD, and Michael L. Callaham, MD Sun Francisco, Calif.
Since the original description of manual cardiopul- monary resuscitation (CPR) by Kouwenhoven et al.’ in 1960, little has changed with regard to this technique. The American Heart Association cur- rently recommends manual CPR, which consists of active chest compression to a depth of 1.5 to 2 inches at a rate of 80 to 100 compressions per minute and a 50% duty cycle with passive chest expansion.2 This technique is known to be inefficient, since it produces less than one third of the normal cardiac output.3 A
From the Department of Medicine and the Cardiovascular Research Insti- tute, University of California, San Francisco.
Received for publication Mar. 5, 1992; accepted May 1, 1992.
Reprint requests: Todd J. Cohen, MD, Director of Electrophysiology, Car- diology Division. North Shore University Hospital-Cornell University Medical College, 300 Community Dr., Manhasset, Long Island, NY 11030.
4/l/40571
large number of studies have been performed in an effort to find a better technique for CPR that would improve perfusion and chances of resuscitation.4-12 To date, none of these methods have gained wide- spread acceptance as a preferred method of CPR.
Lurie et a1.13 described an episode of cardiac arrest in an elderly man. His son, who was not trained in standard CPR, applied a plunger to his father’s chest and proceeded to resuscitate him. The authors hy- pothesized that this form of resuscitation effectively provided both active compression and relaxation (decompression) of the chest. In addition, they thought this method may have facilitated ventila- tion.
The purpose of this study was to quantitate the short-term hemodynamic effects of resuscitation with a hand-held suction device that incorporates both active compression and decompression of the chest.
1145

1146 Cohen et al. November 1992
American Heart Journal
A
B
ml- ‘C I
STANDARD CPR
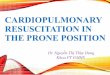
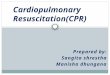
=-a ACDCPR Fig. 1. Right atria1 and ascending aortic pressure tracings during standard (panel A) and ACD CPR (panel B) in dog no. 1. Standard CPR resulted in a cardiac output of I.4 L/min, a systolic arterial pressure of 59 f 6 mm Hg, and no ventilation. ACD CPR produced a cardiac output of 3.2 L/min, a systolic arterial pressure of 85 mm Hg, and a minute ventilation of 5.3 L/min.
METHODS
This study was approved by the University of California, Committee on Animal Research and was performed in ac- cordance with the “Principles of Laboratory Animal Care” as formulated by the National Society of Medical Research and “Guide for Care and Use of Laboratory Animals,” which was prepared by the National Academy of Sciences and published by the National Institutes of Health (DHEW [NIH] Publication 85-23, revised 1985). The suction device was constructed from a rubber polymer and consisted of a large suction cup head (radius = 5.2 cm; height = 3 cm; thickness = 0.5 cm) and a handle.
For each experiment, the dogs were premeditated with fentanyl (0.04 mg/kg) and droperidol (2 mg/kg), anesthe- tized with pentobarbital sodium (7 to 12 mg/kg adminis- tered intravenously), and endotracheally intubated. The animals were not endotracheally ventilated during CPR, so that both ventilatory and hemodynamic effects of active compression-decompression (ACD) and standard CPR could be assessed. The long-haired dogs’ chests were shaved to provide a smooth surface for ACD suction-adhe- sion. Two micromanometer pressure transducers (model
no. 110-4, Camino Laboratories, San Diego, Calif.) were inserted through the femoral vein and artery and posi- tioned with the use of fluoroscopy in the right atrium and ascending aorta to record ascending aortic and right atria1 pressures. Ventricular fibrillation was induced by applica- tion of alternating current to the right ventricular apex via a 6F right ventricular quadripolar catheter.
Coronary perfusion pressure was determined by the dif- ference between mean aortic pressure and mean right atria1 pressure in diastole. Pulsed wave Doppler tracings, which were continuously obtained from the main pulmonary ar- tery, were used to determine the velocity time integral (VTI). The VT1 or stroke distance is an expression of the distance that an average red blood cell travels during each compression cycle. This is obtained by integrating the pulsed wave velocity profile over time.“-‘7 Cardiac output can be determined from the product of VTI, pulmonary arterial cross-sectional area, and compression rate. In a given animal, assuming that cross-sectional area and com- pression rates are constant, the VT1 represents an analog of cardiac output. The minute ventilation was determined by spirometry.
ACD resuscitation was performed with the suction cup placed in the middle or slightly to the right of the sternum (depending on the chest configuration). The CPR operator was positioned over the chest, on a stool, with hands on the handle of the ACD device. A downward force was applied to actively compress the suction cup head and the chest to the standard depth. Once the device and the chest were completely compressed, the operator pulled up on the handle, which pulled the chest back to a fully expanded position, without losing contact with the chest wall (chest decompression phase).
ACD CPR was compared with standard manual CPR in eight nonventilated anesthetized dogs (with weights of 10 to 30 kg). The first three animals were beagles with flat chests, such that when each animal was on its back, the suction cup could adhere directly to the middle of the ster- num. In five mongrel dogs with keel-shaped chests, the suction cup surface area exceeded the small keel-shaped area, and thus CPR was performed slightly off center; the animal was secured with a V-shaped stoichiometric device. Each animal was randomized (with the use of a random numbers table) to receive ACD and standard CPR sequen- tially for 2 minutes each.
The first experiment (pilot study) was performed at the end of a 30.minute defibrillation protocol after the dog be- came asystolic. The remainder of the experiments were performed again in healthy, hemodynamically stable ani- mals after 30 seconds of induced ventricular fibrillation. Each CPR method was performed at a rate of 100 com- pressions per minute. Compressions were synchronized to a metronome, and the depth and duty cycle were monitored by an American Heart Association Certified Advanced Cardiac Life Support instructor. The instructor gave con- tinuous feedback to the operator in an attempt to maintain a compression depth of 1.5 to 2 inches and a 509; duty cycle. After 2 minutes of use of the first technique, two transthoracic defibrillations were attempted (200 J and 400

Volume 124
Number 5
J). If successful, at least 5 minutes was allowed before re- induction of ventricular fibrillation and assessment of the second technique. If the defibrillation was unsuccessful, the second CPR technique was started immediately, and the recording of CPR data started 1 minute after the shock. This delay in recording hemodynamic data was created to minimize the immediate postshock effects of released en- dogenous catecholamines. Coronary perfusion pressure, systolic and diastolic aortic pressures, right atria1 diastolic pressures, and VT1 were recorded at 30, 60, 90, and 120 seconds of CPR. Hemodynamic measurements were ob- tained over a &second period before the measured time in- terval. Minute ventilation was determined between 60 and 120 seconds of CPR. In four dogs, arterial blood gases were obtained immediately after each CPR technique. In three dogs, end-tidal COs concentration was obtained at 30, 60, 90, and 120 seconds of each CPR technique (Nellcor PlOOO, Capnometer, Hayward, Calif.).
All data are presented as means + standard deviation. ACD CPR was compared with standard CPR with Stu- dent’s two-tailed t test. A p value of less than 0.05 was con- sidered statistically significant.
RESULTS
Fig. 1 shows the right atria1 and ascending aortic pressures that were obtained during standard and ACD CPR in animal no. 1. Fig. 2, A-F shows systolic and diastolic aortic pressures, right atria1 diastolic pressure, coronary perfusion pressure, minute venti- lation, and VT1 for each technique in each dog. ACD CPR resulted in significant increases in each mea- sured parameter, except diastolic aortic and right atria1 pressures, as compared with standard CPR. Specifically, when compared with standard CPR, ACD CPR increased coronary perfusion pressure (18 I 11 mm Hg during ACD CPR; 8 + 6 mm Hg during standard CPR; p < 0.02), VT1 (8.0 f 1.1 cm/ compression during ACD CPR; 4.4 + 1.4 cm/com- pression during standard CPR; p < O.OOOl), minute ventilation (4.2 + 1.4 L/min during ACD CPR; 2.0 + 1.2 L/min during standard CPR;p < 0.01); and systolic aortic pressure (58 k 19 mm Hg during ACD CPR; 44 +- 11 mm Hg during standard CPR; p < 0.01). Diastolic aortic and right atria1 pressures were not significantly different when the ACD tech- nique was used. Arterial blood gases that were obtained immediately after CPR in four dogs (dogs nos. 1,3,7, and 8) demonstrated a pH of 7.30 +- 0.18, PCOZ of 38 -t 24 mm Hg, and PO:! of 81 f 18 mm Hg after standard CPR. Values that were obtained after ACD CPR were similar, with a pH of 7.37 + 0.22, POZ of 103 k 53. mm Hg, and PCOZ of 35 + 19 mm Hg (p = NS for all values). In the first three dogs end-tidal COs tended to be higher with ACD CPR, 17 i 8 mm Hg with ACD as compared with 13 + 7 mm Hg with standard CPR, but this trend was not
a)
Active compression-decompression CPR 1147
ST” ACD
31 STD ACD
b)
ST0 AC0
STD ACD
STD AkD
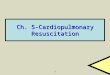
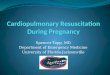
Fig. 2. Panels A-F show the systolic and diastolic aortic pressures, right atria1 diastolic pressures, coronary perfu- sion pressures, VTI, and minute ventilation in each dog for both ACD and standard CPR. Consistent increases were observed with systolic aortic pressure (p < O.Ol), coronary perfusion pressure (p < 0.02), VT1 (p < O.OOOl), and minute ventilation (p < 0.01) during ACD as compared with standard CPR.
statistically significant. In two of eight dogs (dogs nos. 2 and 8), ventricular fibrillation remained re- fractory to transthoracic defibrillation after standard CPR but converted spontaneously during ACD re- suscitation (Fig. 3, A and B). There were no dogs in which the reverse was true. Autopsies were per- formed in all animals after completion of the CPR protocol. No evidence of myocardial contusion or rib

1148 Cohen et al. November 1992
American Heart Journal
aa,oJ -. ____- -- -
STOP ACD CPR
-
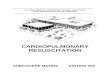
Fig. 3. Panels A and B show simultaneous recordings of the surface ECG and right atrial and ascending aortic pressure tracings during standard and ACD CPR in dog no. 8. After 2 minutes of standard CPR, 200 J and 300 J transthoracic shocks failed to terminate ventricular fibrillation, and ACD CPR was promptly instituted. Within the next 15 seconds, spontaneous ventricular activity was noted. After 1 minute, ACD CPR was stopped, and high-grade atrioventricular block was present but resolved shortly thereafter.
fracture was noted as a result of either CPR tech- nique.
DISCUSSION
This is the first study to demonstrate improved coronary perfusion pressure, VT1 (an analog of car- diac output), minute ventilation, and systolic arterial pressure through the use of ACD resuscitation. This new method of CPR employs a suction device that adheres to the anterior chest and thus facilitates chest expansion and compression. We speculate that venous return and cardiac filling are improved by the negative intrathoracic pressure, which produces the significant increase in cardiac output that was ob- served in our study.
Previously, complicated devices have been applied to the abdomen and chest to assist in ventricular fill- ing and CPR. In 1939, Eisenmenger described a large abdominal suction device called the “Biomotor” in an article entitled, “Suction and Air Pressure Over the Belly, Its Action and Applications.“” He dem- onstrated the circulation of India ink in a human ca- daver but was unable to successfully apply this device to patients who were experiencing cardiac arrest. Other devices such as the tank respirator or “iron
lung,” the cuirass, and the breathing jacket have been developed and implemented to assist ventilation in the patient with paresisI
Ohomoto et a1.20 described a method of CPR in which external cardiac massage and abdominal coun- termassage were applied by means of two machines in closed-chest dogs. Carotid and coronary flows were increased by 1.4 to 2 times with this method when compared with manual CPR. Recently manual ab- dominal counterpressure during CPR has been re- ported to improve survival after cardiac arrest in hu- man beings. 21 However, the hemodynamic improve- ments that were attained with all of these methods have usually been marginal.4-‘”
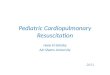
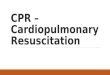
Fig. 4 shows the Active Compression-Decompres- sion resuscitator (Cardiopump, Ambu, International, Copenhagen, Denmark), which has been developed for use in human beings during cardiac arrest. This device consists of a circular handle to ensure stabil- ity, a calibrated gauge to monitor performance, and a suction cup to permit chest decompression without dislodgment. This device is currently undergoing clinical investigation in the United States, as well as abroad.
Our study has several limitations. First, a trained

volume 124 Number 5 Active compression-decompression CPR 1149
Fig. 4. The Active Compression-Decompression (ACD) resuscitator, which has been developed for use during cardiac arrest in human beings. This device permits both active chest compression (A) and active chest expansion or decompression (BJ.
observer monitored compression depth and duty cy- cle during both CPR techniques. A mechanical method for controlling both force and displacement would have been preferable, but in our efforts to de- velop such a device we found that it limited the ease and effectiveness of the decompression phase, so we had to rely on the observer method of controlling the depth of chest compression. This problem is similar to that. of many prior studies of cardiac arrest, which relied on human (and thus not completely standard- ized and reproducible) compression of the chest or abdomen. A second limitation is that this study was designed to assess the immediate effects of ACD CPR on both ventilation and circulation, and therefore animals were not ventilated during CPR. This design did in fact demonstrate that ACD CPR provided su- perior and physiologic ventilation. We do not believe the lack of ventilation affected the hemodynamic variables that we measured because of the similarity of the blood gas values in both treatment groups and the fact that they were both within the expected range during experimental cardiac arrest. The effects of ACD CPR on nonintubated dogs require further investigation. A further limitation is that we mea- sured hemodynamic variables, including coronary perfusion pressure, but did not directly measure cor- onary or cerebral perfusion or survival. Of note, end- tidal CO:! concentration has been shown to correlate well with coronary perfusion pressure and myocar- dial perfusion in cardiac arrest,22-26 and there was a trend toward increased end-tidal CO* concentration with the ACD technique. Future studies are neces- sary to determine the exact mechanism of augmented hemodynamics during ACD resuscitation and to measure to what degree this technique improves ce- rebral and myocardial perfusion, as well as survival.
The ACD CPR technique uses standard American Heart Association recommendations for CPR2 in conjunction with interposed active chest expansion. Use of the ACD device (Cardiopump) is a simple manual technique, which is easy to perform and re- quires no set-up time. Therefore it appears to be practical for first responders to apply this method during early CPR. This method also provides phys- iologic minute ventilation in intubated animals. We conclude that ACD CPR holds the promise of a much more effective method of CPR with a simple device that requires minimal training to use and that animal and human survival studies may be warranted.
ADDENDUM
After completion of this animal study, a study of similar design investigated ACD CPR in human be- ings late during cardiac arrest. This subsequent study confirmed that dramatic improvements in cardio- pulmonary circulation occur with ACD CPR as com- pared with standard CPR.27 REFERENCES
1.
2.
3.
4.
5.
6.
Kouwenhoven WB, Ing D, Jude JR, et al. Closed chest cardiac massage. JAMA 1960;173:1064-7. American Heart Association Standards and Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Care (ECC). JAMA 1986;255:2905-73. Del Guercio LRM, Coomaraswamy RP, State D. Cardiac out- put of other hemodynamic variable during external cardiac massage in man. N Engl J Med 1963;269:13898-1404. Koehler RC, Chandra N, Guerci AD, et al. Augmentation of cerebral perfusion of simultaneous chest compression and lung inflation with abdominal binding after cardiac arrest in dogs. Circulation 1983;67:266-75. Walker JW, Bruestle JC, White BC, et al. Perfusion of cere- bral cortex by use of abdominal counterpulsation during car- diopulmonary resuscitation. Am J Emetg Med 1984;2:<91-3. Crilev JM. Blaufuss AH. Kissel GL. Cough-induced cardiac com&essi& JAMA 1976;236:1246-50. -
7. Chandra N, Weisfeldt M, Tsitlik J, et al. Augmentation of

cardiac flow during cardiopulmonary resuscitation by ventila- tion at high airway pressure simultaneous with chest com- pression. Am J Cardiol 1981;48:1053-63.
8. Chandra N, Rudikoff M, Weisfeldt ML. Simultaneous chest compression and ventilation at high airway pressure during cardiopulmonary resuscitation. Lancet 1980;1:175-8.
9. Berryman CR, Phillips GM. Interposed abdominal compres- sion-CPR in human subjects. Ann Emerg Med 1984;13:226-9.
10. Kaplan BC, Civetta JM, Nagel EL, et al. The military antishock trousers in civilian pre-hospital emergency care. J Trauma 1973;13:843.
11. Bircher N, Safar P, Stewart R. A comparison of standard, “MAST”-augmented, and open-chest CPR in dogs. Crit Care Med 1980;8:147-52.
12. Halperin HR, Guerci AD, Chandra N, Herskowitz A, Tsitlik JE, Nistranea RA, Wurmb E, Weisfeldt ML. Vest inflation without simultaneous ventilation during cardiac arrest in dogs: improved survival from prolonged cardiopulmonary re- suscitation. Circulation 1986;74:1407-15.
13. Lurie KG, Lindo C, Chin J. CPR: The P stands for plumber’s helper. JAMA 1990;264:1661.
14. Sanders AB, Ewy GA, Taft TV. Prognostic and therapeutic importance of the aortic diastolic pressure in resuscitation from cardiac arrest. Crit Care Med 1984;12:871-3.
15. Lewis JF, Kuo LC, Nelson JG, et al. Pulsed Doppler echocar- diographic determination of stroke volume and cardiac out- put: clinical validation of two new methods using the apical window. Circulation 1984;70:425-31.
16. Meijboom EJ, Horowitz S, Valdez-Cruz LM, et al. A two-di- mensional Doppler echocardiographic method for calculation of pulmonary and systemic blood flow in a canine model with variable-sized left-to-right extracardiac shunt. Circulation 1983;68:437-45.
17. Arts MGJ, Roevros JMJG. On the instantaneous measure-
18.
19.
20.
21.
22.
23.
24.
November 1992 American Heart Journal
ment of blood flow by ultrasonic means. Med Hiol Km 1971;10:23-4. Eisenmenger R. Aug.und druckluft uber dem bauch, dereh Wirkung and anwesdunq. Wien Med Wochenschr 1939;31:8()7. Spalding JMK, Smith AC. Clinical practice and physiology o! artificial respiration. Oxford, England: Blackwell Scientific Publications, 1963:1-11. Ohomoto T, Miura I, Konno S. A new method of external car- diac massage to improve diastolic augmentation and prolnng survival time. Ann Thor Surg 1976;21:284-90. Sack JB, Kesselbrenner MB, Jarrad A, Bregman D. Effect of- interposed abdominal counterpulsation on resuscitation out- come during asystole and electromechanical dissociation [Ah- stract]. J Am Co11 Cardiol 1991;17:179A. Callaham M, Barton C. Prediction of outcome of cardiopul- monary resuscitation from end-tidal carbon dioxide concen- tration. Crit Care Med 1990;18:358-62. Garnett AR, Ornato JP, Gonzalez ER, Johnson EB. End-tidal carbon dioxide monitoring during cardiopulmonary resusci- tation. JAMA 1987;257:512-15. Sanders AB. Atlas M, Ewy GA, Kern KB, Bragg S. Expired pCO2 as an index of coronary perfusion pressure. Am J Emerg Med 1985;3:147-9.
25. Trevino RP, Bisera J. Weil MH, Rackow EC, Grundler WG. End-tidal CO2 as a guide to successful cardiopulmonary resuscitation: a preliminary report. Crit Care Med 1985;13:91 O- 11.
26. Sanders AB, Kern KB, Otto CW, Milander MM, Ewy GA. End-tidal carbon dioxide monitoring during cardiopulmonary resuscitation: a prognostic indicator for survival. JAMA 1989;262:1347-51.
27. Cohen TJ, Tucker KJ, Lurie KG, et al. Active compression- decompression: a new method of cardiopulmonary resuscita- tion JAMA 1992;267:2916-23.