Embed Size (px)
Citation preview

An
ind
epen
den
t lic
ense
e of
the
Blu
e S
hie
ld A
ssoc
iatio
n
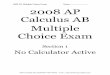
Active Choice® 750 80/60 For groups of 101 and above A health plan designed to allow insureds to be active participants in their own health care. The Active Choice Plan offers coverage for preventive care services at no charge and with no up-front deductible, as well as a $750 individual/$1,500 family “First Dollar Services” coverage for specified services. Each calendar year, the insured can spend this First Dollar Services coverage on any of these specified services, from an office visit to physical therapy benefits.
Covered Services Active Choice 750 80/60
Calendar Year In-Network Out-of-Pocket Maximum#,1 $3,000 / $6,000 (individual/family)
Preventive Health Services12 No charge for services rendered by Participating Providers
Cat
egor
y O
ne #
First Dollar Services2 Coverage Outpatient Professional & Diagnostic Services2
Office visits Diagnostic x-ray, imaging, pathology, and
laboratory and other testing services Durable Medical Equipment and Supplies2
Durable Medical Equipment Prosthetics/Orthotics Diabetes Care
$750 Individual/$1,500 Family (Each insured family member has access to the entire amount of the family First Dollar Services credit)
Then the Insured is responsible for charges up to the Calendar Year Out-of-Pocket Maximum
No
Dedu
ctib
le. N
o C
opay
men
t or C
oins
uran
ce
until
Firs
t Dol
lar S
ervi
ces
cove
rage
is sp
ent
Cat
egor
y Tw
o #
Outpatient & Inpatient Facility–Based Services Hospitalizations Surgeries (includes services in ambulatory
surgery center) Emergency room Chemotherapy
20% Participating Providers
40% Non-Participating Providers
(additional copayments apply to some services)
No
Dedu
ctib
le
Prescription Drugs A description of your outpatient prescription drug coverage is provided separately. If you do not have the separate drug summary that goes with this benefit summary, please contact your benefits administrator or call the Customer Service number on your identification card.
# Charges in excess of the allowable amount do not count toward the calendar year out-of-pocket maximum.
1) After the calendar year out-of-pocket maximum is met Blue Shield Life covers most services at 100 percent of the allowable amount.
2) For more information on First Dollar Services coverage, see page 2.

Categories of Care Active Choice Plans give you more control over your benefits and out-of-pocket expenses. Under this plan, you have affordable coverage across categories of healthcare services without paying up-front deductibles for Category One. In the first category, you receive a set amount of healthcare dollars - these dollars cover routine physician office services and outpatient professional and diagnostic services. At the same time, you have valuable protection against the costly impact of hospital services and prescription drugs through more traditional benefits of coinsurance and copayments. To help you understand each category of care, we've outlined your coverage below.
Category One. Coverage for Outpatient Professional and Diagnostic Services as well as Durable Medical Equipment and Supplies
For First Dollar Services coverage, each Calendar Year, the insured has a set amount to spend on the category of outpatient professional and diagnostic care:
With Active Choice 750 80/60 - Up to $750 per individual and $1,500 per family
(Each insured family member has access to the entire amount of the family First Dollar Services)
It's up to you to decide how to spend these amounts on the services covered under Category One, which provides for First Dollar Services coverage. This category includes a wide range of services to pick from, such as outpatient professional and diagnostic care, including physician office visits, testing, and mental health services. For these services you can choose your own physician from our broad, statewide network of participating providers, to stretch your dollars even further. If you choose a non-participating provider, First Dollar Services only cover the allowable amount, and you are responsible for the remainder of the costs. In addition, once the First Dollar Services coverage is spent, you are responsible for 100 percent of covered medical costs until the calendar year out-of-pocket maximum is met.
Also, as long as you are an insured of this plan through your current employer, you can roll over unused dollars starting from the current calendar year and thereafter in this category of care. Each insured family member may use any or all of the family carryover credit. Any amounts covered in this category do not apply to the calendar year out-of-pocket maximum.
Category Two. Coverage for Outpatient and Inpatient Facility Services – Including Emergency Care Services
When you need care the most, you can rely on immediate coverage. If an unexpected illness or injury happens, this coverage includes emergency care and surgery in hospitals and facilities (including professional services associated with such facility services). We share the cost of care with you at the following levels:
With Active Choice 750 80/60 - the insured pays 20 percent for participating providers, 40 percent of the allowable amount for non-participating providers. (additional copayments apply to some services)
Coverage for Prescription Drugs
To keep prescription drugs affordable, Active Choice Plans are paired with prescription drug coverage that provide immediate coverage for generic drugs.
No generic drug deductible Coverage includes covered brand-name drugs Prescription drug coverage includes no annual benefit maximums
The copayments and any applicable brand-name drug deductible for prescription drugs accrue to your calendar year out-of-pocket maximum
The following benefits and services do not accrue towards the calendar year out-of-pocket maximum. This means that coinsurance, copayments and charges for services that are not included in the calculation of the calendar year out-of-pocket maximum remain the insured’s responsibility, even after the out-of-pocket maximum has been reached.
Any charges above the allowable amounts. When insured’s use non-participating providers, they must pay the applicable
coinsurance or copayments plus any amount that exceeds Blue Shield Life’s allowable amount. These charges above the allowable amount do not count toward the calendar year out-of-pocket maximum.
First Dollar Services payments or First Dollar Services carryover credit.

Category One: Outpatient Professional and Diagnostic
Category Two: Outpatient & Inpatient Surgery
Active Choice® 750 80/60 Benefit Summary (For groups of 101 and above) Blue Shield of California Life & Health Insurance Company
Effective January 1, 2018
THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE CERTIFICATE OF INSURANCE AND GROUP POLICY SHOULD BE CONSULTED FOR A DETAILED DESCRIPTION OF COVERAGE BENEFITS AND LIMITATIONS.
Highlights: $750 individual / $1,500 family first dollar services amount A description of the prescription drug coverage is provided separately
The Active Choice Plan has two categories of benefit coverage.
Benefits Insured Responsibility Participating Providers1 Non-Participating Providers2
Calendar Year Medical Deductible $0 per Individual / $0 per FamilyCalendar Year Out-of-Pocket Maximum (Includes the plan deductible) (For many covered services)
$3,000 per individual / $6,000 per family
$10,000 per individual / $20,000 per family
Lifetime Benefit Maximum None
PREVENTIVE HEALTH BENEFITS (Covered preventive health services benefits are paid at 100% of the allowable amount)
Participating Providers1
Non-Participating Providers2
Preventive Health Services (as required by applicable Federal and California law)12
No Charge Not Covered
Family Planning Services (Includes counseling, consulting, education, insertion of IUD, as well as injectable and implantable contraceptives for women, and tubal ligations)
No Charge Not Covered
Breast Pump No Charge Not Covered
Covered Services First Dollar Services & Insured Responsibility Category One Services: Outpatient Professional and Diagnostic3
PROFESSIONAL SERVICES Participating Providers1 Non-Participating Providers2 Professional (Physician) Benefits
The $750 individual or $1,500 family First Dollar Services covers any combination of covered services and supplies. Each insured family member has access to the entire amount of the family First Dollar Services. These services are paid at 100 percent of the allowable amount.1 The insured is responsible for all charges above the $750 individual or $1,500 family First Dollar Services amount until the insured's maximum calendar year out-of-pocket amount has been reached.3 Once the insured's maximum calendar year out-of-pocket has been reached, covered services will be paid at 100 percent of the allowable amount. The insured's responsibility for charges over the allowable amount does not accrue to the calendar year out-of-pocket maximum.
Physician and specialist office visits
Teladoc consultation Outpatient diagnostic x-ray, imaging, pathology, laboratory and other testing services
Radiological and nuclear imaging (CT scans, MRIs, MRAs, PET scans and cardiac diagnostic procedures utilizing nuclear medicine)
Allergy Testing and Treatment Benefits
Allergy testing, treatment and serum injections
MENTAL HEALTH AND SUBSTANCE USE SERVICES4 Routine outpatient mental health and substance use services (includes professional/physician visits)
Non-routine outpatient mental health and substance use services (includes office-based behavioral health treatment, electroconvulsive therapy, intensive outpatient programs, psychological testing, office-based opioid treatment, partial hospitalization program, and transcranial magnetic stimulation)
CHIROPRACTIC BENEFITS
Chiropractic spinal manipulation (up to 12 visits per calendar year) ACUPUNCTURE BENEFITS
Acupuncture services (up to 20 visits per calendar year)
REHABILITATION AND HABILITATIVE BENEFITS (Physical, Occupational and Respiratory Therapy)

Office location (an additional facility copayment may apply when services are rendered in a hospital or skilled nursing facility)
SPEECH THERAPY BENEFITS
Office location (an additional facility copayment may apply when services are rendered in a hospital or skilled nursing facility)
PREGNANCY AND MATERNITY CARE BENEFITS12
Prenatal and postnatal physician office visits Professional services for delivery and inpatient hospital services are covered under "Hospitalization Services".
Abortion services (an additional facility copayment may apply when services are rendered in a hospital or outpatient surgery center)
FAMILY PLANNING BENEFITS Vasectomy (an additional facility copayment may apply when services are rendered in a hospital or outpatient surgery center)
DIABETES CARE BENEFITS
Devices, equipment, and non-testing supplies (for testing supplies, see Outpatient Prescription Drug Benefits)
Diabetes self-management training
DURABLE MEDICAL EQUIPMENT
Devices, equipment, and medical supplies
PROSTHETICS/ORTHOTICS
Prosthetic equipment and devices
Orthotic equipment and devices Covered Services Insured Coinsurance
Category Two Services: Outpatient & Inpatient Surgery – including emergency care services
OUTPATIENT SERVICES Participating Providers1 Non-Participating Providers2
Hospital Benefits (Facility Services)
Outpatient surgery performed at a free-standing ambulatory surgery center
$250 per surgery + 20% 40% up to $350 per day5
Outpatient surgery performed in a hospital or a hospital affiliated ambulatory surgery center
$400 per surgery + 20% 40% up to $350 per day5
Outpatient services for treatment of illness or injury and necessary supplies (except as described under "Rehabilitation and Habilitative Benefits" and "Speech Therapy Benefits")
20% 40% up to $350 per day5
Bariatric surgery6 (prior authorization is required; medically necessary surgery for weight loss, for morbid obesity only)
$400 per surgery + 20% 40% up to $350 per day5
HOSPITALIZATION SERVICES Hospital Benefits (Facility Services)
Physician services (associated with inpatient or outpatient surgery and procedures including pregnancy and maternity care and services for acute medical detoxification)
20% 40%
Inpatient non-emergency facility services (semi-private room and board, and medically-necessary services and supplies, including subacute care)
$500 per admission + 20% 40% up to $600 per day7
Bariatric surgery6 (prior authorization is required; medically necessary surgery for weight loss, for morbid obesity only)
$500 per admission + 20% 40% up to $600 per day7
Inpatient Skilled Nursing Benefits8,9 (combined maximum of up to 100 days per benefit period, prior authorization is required; semi-private accommodations)
Free-standing skilled nursing facility 20% 20%9
Skilled nursing unit of a hospital 20% 40% up to $600 per day7

EMERGENCY HEALTH COVERAGE Emergency room services not resulting in admission (copayment does not apply if the insured is directly admitted to the hospital for inpatient services)
$100 per visit + 20%
$100 per visit + 20%
Emergency room services resulting in admission (when the insured is admitted directly from the ER)
$500 per admission + 20% $500 per admission + 20%
Emergency room physician services 20% 20%AMBULANCE SERVICES
Emergency or authorized transport (ground or air) 20% 20%
PRESCRIPTION DRUG COVERAGE
A description of your outpatient prescription drug coverage is provided separately. If you do not have the separate drug summary that goes with this benefit summary, please contact your benefits administrator or call the Customer Service number on
your identification card. MENTAL HEALTH AND SUBSTANCE USE SERVICES4, 10
MHSA Participating Provider1
MHSA Non- Participating Providers2
Inpatient hospital services $500 per admission + 20% 40% up to $600 per day7
Inpatient physician services No Charge 40%
Residential care $500 per admission + 20% 40% up to $600 per day7
HOME HEALTH SERVICES Participating Provider1 Non- Participating Providers2
Home health care agency services8 (up to 100
visits per calendar year) 20% Not Covered11
Home infusion/home injectable therapy and infusion nursing visits provided by a home infusion agency
20% Not Covered11
Hospice Program Benefits11
Routine home care No Charge Not Covered11
Inpatient respite care No Charge Not Covered11
24-hour continuous home care No Charge Not Covered11
Short-term inpatient care for pain and symptom management
No Charge Not Covered11
Care Outside of Plan Service Area (Benefits provided through the BlueCard® Program for out-of-state emergency and non-emergency care are provided at the participating level of the local Blue Plan allowable amount when you use a BlueCross/BlueShield provider. The $500 individual or $1,000 family First Dollar Services amount covers any combination of outpatient professional services and supplies, including benefits provided through the BlueCard Program)
Within US: BlueCard Program See Applicable Benefit See Applicable Benefit
Outside of US: BlueCard Worldwide See Applicable Benefit See Applicable Benefit
Optional Benefits Optional dental, vision, infertility and hearing aid benefits are available. If your employer purchased any of these benefits, a description of the benefit is provided separately.
1 Unless otherwise specified, copayments/coinsurance are calculated based on allowable amounts. After the calendar year medical deductible is met, the insured is responsible for copayments/coinsurance for covered services from participating providers. Participating providers agree to accept Blue Shield Life’s allowable amount plus any applicable insured copayment or coinsurance as full payment for covered services.
2 Non-participating providers can charge more than Blue Shield Life’s allowable amounts. When insured’s use non-participating providers, they must pay the applicable deductibles, copayments or coinsurance plus any amount that exceeds the Blue Shield Life’s allowable amount. Charges above the allowable amount do not count toward the calendar year deductible, out-of-pocket maximum or First Dollar Services amounts.
3 After the First Dollar Services amount is reached, covered First Dollar Services will accrue to the calendar-year out-of-pocket maximum.
4 Mental Health and Substance use services are accessed through Blue Shield Life's Mental Health Service Administrator (MHSA) - using MHSA participating providers and MHSA non-participating providers. Only mental health and substance use services rendered by MHSA participating providers are administered by MHSA. Mental health and substance use services

rendered by MHSA non-participating providers are administered by Blue Shield Life.5 The maximum allowed charges for non-emergency surgery and services performed in a non-participating ambulatory surgery
center or outpatient unit of a non-participating hospital is $350 per day. Insured’s are responsible for the coinsurance and all charges in excess of $350 per day. Charges that exceed the allowable amount do not count toward the calendar year out-of-pocket maximum and continue to be owed after the maximum is reached.
6 Bariatric surgery is covered when prior authorized by Blue Shield Life; however, for insured’s residing in Imperial, Kern, Los Angeles, Orange, Riverside, San Bernardino, San Diego, Santa Barbara and Ventura Counties ("Designated Counties"), bariatric surgery services are covered only when performed at designated contracting bariatric surgery facilities and by designated contracting surgeons. Coverage is not available for bariatric services from any other participating provider and there is no coverage for bariatric services from non-participating providers. In addition, if prior authorized by Blue Shield Life, an insured in a Designated County who is required to travel more than 50 miles to a designated bariatric surgery facility will be eligible for limited reimbursement for specified travel expenses for the insured and one companion. Refer to the Certificate of Insurance for further details.
7 The maximum allowed charges for non-emergency hospital services received from a non-participating hospital is $600 per day. Insured’s are responsible for the coinsurance and all charges in excess of $600 per day. Charges that exceed the allowable amount do not count toward the calendar year out-of-pocket maximum and continue to be owed after the maximum is reached.
8 For plans with a calendar year medical deductible amount, services with a day or visit limit accrue to the calendar year day or visit limit maximum regardless of whether the calendar year medical deductible has been met.
9 Services may require prior authorization. When services are prior authorized, insured’s pay the participating provider amount.
10 Inpatient services for acute detoxification are covered under the medical benefit; see Hospital Benefits (Facility) Services for benefit details. Services for medical acute detoxification are accessed through Blue Shield Life using Blue Shield Life's participating providers or non-participating providers.
11 Services from non-participating providers, home health care, home infusion and hospice services are not covered unless prior authorized. When these services are prior authorized, the insured pays the participating provider copayment.
12 If you only receive preventive health services during a physician office visit, there is no copayment or coinsurance for the visit. If you receive both preventive health services and other covered services during the physician office visit, you may have a copayment or coinsurance for the visit.
Active Choice is a service mark of Blue Shield of California. Plan designs may be modified to ensure compliance with state and Federal requirements. A16286 (1/18)

Blue Shield of California50 Beale Street, San Francisco, CA 94105 blueshieldca.com
Notice Informing Individuals about Nondiscrimination and Accessibility Requirements
Discrimination is against the law
Blue Shield of California Life & Health Insurance Company complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability or sex. Blue Shield Life does not exclude people or treat them differently because of race, color, national origin, age, disability or sex.
Blue Shield Life:
• Provides aids and services at no cost to people with disabilities to communicate effectively with us such as:
- Qualified sign language interpreters
- Written information in other formats (including large print, audio, accessible electronic formats and other formats)
• Provides language services at no cost to people whose primary language is not English such as:
- Qualified interpreters
- Information written in other languages
If you need these services, contact the Blue Shield Life Civil Rights Coordinator.
If you believe that Blue Shield Life has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability or sex, you can file a grievance with:
Blue Shield Life & Health Insurance Company Civil Rights Coordinator P.O. Box 629007 El Dorado Hills, CA 95762-9007
Phone: (844) 831-4133 (TTY: 711) Fax: (916) 350-7405 Email: [email protected]
You can file a grievance in person or by mail, fax or email. If you need help filing a grievance, our Civil Rights Coordinator is available to help you.

blueshieldca.com
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services 200 Independence Avenue SW. Room 509F, HHH Building Washington, DC 20201 (800) 368-1019; TTY: (800) 537-7697
Complaint forms are available at www.hhs.gov/ocr/office/file/index.html.
Blu
e S
hie
ld o
f Ca
lifo
rnia
, an
ind
ep
en
de
nt
me
mb
er
of t
he
Blu
e S
hie
ld A
sso
cia
tion
A
4972
7 (1
0/16
)

blueshieldca.com
Notice of the Availability of Language Assistance ServicesBlue Shield of California Life & Health Insurance Company
Blu
e S
hie
ld o
f Ca
lifo
rnia
, an
ind
ep
en
de
nt
lice
nse
e o
f th
e B
lue
Sh
ield
Ass
oc
iatio
n
A20
275
(4/1
6)