Embed Size (px)
Citation preview

230 | april 2010 | volume 40 | number 4 | journal of orthopaedic & sports physical therapy
[ research report ]
1 Sports Medicine Fellow, Department of Orthopaedic Surgery, University of Michigan, Ann Arbor, MI. 2 Research Specialist, Department of Orthopaedic Surgery, University of
Michigan, Ann Arbor, MI. 3 House Officer, Department of Orthopaedic Surgery, University of Michigan, Ann Arbor, MI. 4 Undergraduate Student, Department of Orthopaedic Surgery, University of Michigan, Ann Arbor, MI. 5 Associate Professor, Department of Orthopaedic Surgery, University of Michigan, Ann Arbor, MI. 6 Assistant Professor, Department of Orthopaedic Surgery, University of Michigan, Ann Arbor, MI. This study was approved by The University of Michigan Institutional Review Board. Address correspondence to Dr James E. Carpenter, Department of Orthopaedic Surgery, The University of Michigan, 1500 E Medical Center Drive, Ann Arbor, MI 48109-0328. E-mail: [email protected]
Joy L. Long, MD1 • Ramon a. RubeRte thiele, MS2 • Jack G. Skendzel, MD3 • JonGeun Jeon4
RichaRd e. huGheS, PhD5 • bRuce S. milleR, MD6 • JameS e. caRpenteR, MD5
Activation of the Shoulder Musculature During Pendulum Exercises and Light Activities
there are a variety of rehabilitation protocols following rotator cuff repair. Many surgeons allow patients to begin gentle passive motion within a day of surgery, but active motion is generally restricted to prevent retear of the rotator cuff.30 Nevertheless,
Galatz et al15 reported retearing of the rotator cuff after surgical repair in over 75% of patients with large tears. While not all patients
waist and allows the arm to swing like a pendulum, moving in circles gener-ated by trunk motion. Burkhart et al5 ob-served, however, that patients sometimes mistakenly make this an active exercise, performing it incorrectly by using their shoulder muscles to swing the arm rather than simply allowing it to hang in a re-laxed state. This type of muscle activity would not be recommended immediately after rotator cuff repair.
Patients are usually interested in returning to activities of daily living (ADLs) as soon as possible after surgery. Although patients are asked to limit ac-tive use of the operative extremity im-mediately after surgery, they may still perform light activities, believing that their shoulder is protected in the sling. Light ADLs that are thought to be harm-less by the patient and that may not be addressed in the postoperative instruc-tions by the surgeon may activate the shoulder muscles and increase the ten-sion on the repair. Little is known about muscle activation in the rotator cuff muscles when simple ADLs, such as typ-ing, brushing teeth, and drinking water from a bottle, are performed.
The purpose of this study was to measure the EMG signal amplitude of
t StudY deSiGn: Prospective, single-group, repeated-measures design.
t obJectiVeS: To evaluate electromyographic (EMG) signal amplitude in the supraspinatus, in-fraspinatus, and deltoid muscles during pendulum exercises and light activities in a group of healthy subjects.
t backGRound: There are numerous rehabilita-tion protocols used after rotator cuff repair. One of the most commonly used exercises in these protocols is the pendulum. Patients can easily perform these exercises incorrectly, and may also perform light activities of daily living without knowing that they may be putting excessive stress on the repair. The effect of improperly performed pendulum exercises and light activities after rota-tor cuff repair is unknown.
t methodS: Muscle activity was recorded in 13 subjects performing pendulum exercises
incorrectly and correctly in both large (51-cm) and small (20-cm) diameters, and while typing, drink-ing, and brushing their teeth.
t ReSultS: Incorrect and correct large pendulums and drinking elicited more than 15% maximum voluntary isometric contraction in the supraspinatus and infraspinatus. The supraspi-natus EMG signal amplitude was greater during large, incorrectly performed pendulums than during those performed correctly. Both correct and incorrect large pendulums resulted in statistically higher muscle activity in the supraspinatus than the small pendulums.
t concluSion: Larger pendulums may require more force than is desirable early in rehabilitation after rotator cuff repair. J Orthop Sports Phys Ther 2010;40(4):230-237. doi:10.2519/jospt.2010.3095
t keY WoRdS: EMG, infraspinatus, rotator cuff, supraspinatus
with failure of their repair experience functional deficits equivalent to their preoperative status, it is imperative to optimize postoperative care, including rehabilitation, to limit recurrence.
One of the more commonly used ex-ercises after rotator cuff repair is the pendulum, which is also referred to as Codman’s exercise.6 To perform this ex-ercise, a patient leans forward at the
06 Long.indd 230 3/23/10 5:29:15 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Uni
vers
ity o
f B
righ
ton
on J
uly
17, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
0 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

journal of orthopaedic & sports physical therapy | volume 40 | number 4 | april 2010 | 231
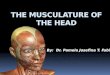
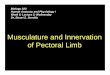
and 5 mm of the first and second wire exited the needle, respectively. The last 2 mm of insulation was stripped from each wire. The wires for the supraspinatus were placed approximately 2 cm superi-or to the midpoint of the scapular spine, and the wires for the infraspinatus were placed approximately 2 cm inferior to the midpoint of the scapular spine. Bipolar, pediatric-sized Ambu Blue Sensor Ag-AgCl electrodes (Ambu Inc, Glen Burnie, MD) were used for the surface recordings of the middle deltoid muscle. These oval-shaped electrodes were placed approxi-mately 3 cm distal to the lateral aspect of the acromion, with an interelectrode dis-tance of 2.2 cm. The technique for place-ment of the wire and surface electrodes was consistent with that described by Basmajian and De Luca.2 The locations of the electrodes are shown in FiGuReS 1 and 2. Proper placement of the electrodes was verified by noting an appropriate electri-cal response with resisted action of the muscle. One of the surface electrodes was also placed on the right olecranon as a ground.
Data were recorded at 1000 Hz on a Noraxon Myosystem 2000 EMG system (Noraxon, Inc, Scottsdale, AZ), collected on a computer using MotionMonitor software (Innovative Sports Training, Inc, Chicago, IL), and stored for offline data analysis. The system uses differen-tial amplifiers with a gain of 1000. There was an input impedance of 10 MΩ, a signal-to-noise ratio of less than 1 mV root-mean-square (RMS), and a com-mon-mode rejection ratio of 135 dB. The
data-processing approach was designed to represent the contraction dynamics of muscle, based on published EMG-driven muscle force prediction models.27,28 Signal processing began with full-wave rectifica-tion, followed by a 2-pass, fourth-order, low-pass Butterworth filter with a cutoff frequency of 3 Hz to obtain a signal for the ith muscle, ei (t). Then a recursive fil-ter was applied: uj (t) = αej (t – d) – β1uj (t – 1) – β2uj (t – 2), where uj(t) was the processed signal at time t, α was a gain for the muscle (α = .02), d was electrome-chanical delay (d = 40 ms), and β1 and β2 were coefficients for the recursive filter (β1 = –1.46 and β2 = 0.48). Muscle activation was then estimated from ui(t), assuming a linear relationship. The end product of this processing was an estimate of muscle activation.
One dependent measure was com-puted for each muscle for each trial: maximum normalized muscle activation. Normalization was done by dividing the activation of a muscle by its maximum muscle activation, computed from EMG data recorded during MVIC trials. The subject was asked to perform maximal isometric external rotation and abduc-tion movement to elicit MVIC for each
the supraspinatus, infraspinatus, and deltoid muscles in a group of healthy subjects who performed pendulums cor-rectly (using trunk motion to cause the arm to move) versus incorrectly (using shoulder musculature to cause the arm to move), and 3 ADLs that included typ-ing, brushing teeth, and drinking from a water bottle. We hypothesized that per-forming pendulum exercises incorrectly would elicit more muscle activity than performing pendulum exercises correctly, and that pendulum exercises and select light activities would not elicit more than 15% of the maximum voluntary isomet-ric contraction (MVIC) in the shoulder muscles.
methodS
approval was obtained from the University of Michigan Institu-tional Review Board prior to be-
ginning the study, and all subjects signed an informed consent document and were compensated. The subjects’ rights were protected during the course of the study. We recruited healthy, right-hand–domi-nant individuals aged 18 years or older. Exclusion criteria included any history of shoulder pain, injury, or surgery, use of an assistive device for ambulation, and inability to tolerate the study proto-col. The right shoulder was tested in all trials. Seventeen subjects were recruited to participate in this study. Two subjects were unable to complete the study due to vasovagal episodes, and 2 others were excluded due to technical problems ob-taining EMG data. Of the 13 subjects in our final analysis, 7 were males and 6 females, with an average age of 29 years (range, 20-57 years).
A physician sterilized and inserted 1 set of 50-mm, disposable, paired-wire electrodes (VIASYS Healthcare Inc, Madison, WI) through a 25-gauge needle, for EMG monitoring of the su-praspinatus and infraspinatus muscles. Each paired-wire electrode consisted of 2 strands of insulated nickel alloy wire. The wires were arranged so that 2 mm
FiGuRe 1. Location of wire electrodes for electromyographic data collection of the supraspinatus and the infraspinatus muscles.
FiGuRe 2. Location of surface electrodes for electromyographic data collection of the deltoid muscle.
06 Long.indd 231 3/23/10 5:29:16 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Uni
vers
ity o
f B
righ
ton
on J
uly
17, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
0 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

232 | april 2010 | volume 40 | number 4 | journal of orthopaedic & sports physical therapy
[ research report ]muscle. The isometric actions were per-formed by having the patient pull on a secured rope while standing. For abduc-tion, the elbow was in extension, for ex-ternal rotation, the elbow was in 90° of flexion and held against the torso (by the patient, not by a restrictive device). No sling was used. A rest EMG measurement was also obtained, with the patient sit-ting quietly at rest for at least 4 seconds. The average baseline muscle activation level at rest was determined and sub-tracted from all other values. The peak muscle activation was determined for each trial so that the peak percent MVIC could be calculated for each activity. The peak percent MVIC over the entire trial for each muscle during each activity was recorded for the individual subjects. The mean for all of the subjects was then ob-tained from these peak values, and the standard deviations were calculated. These methods are consistent with prior studies.20,22
The subject was then placed in a stan-dard sling and asked to complete the 3 ADLs in a previously determined ran-domized order. Typing was performed using a standard keyboard, and the height of the chair was adjusted for in-dividual comfort. Subjects were asked to type continuously, while three 4-second data sets were recorded. Similarly, each subject was given a toothbrush and asked to brush their teeth continuously while three 4-second data sets were recorded. For the drinking task, each subject was given an identical 0.5-L bottle of water. The subject was asked to take 2 sips of water, placing the bottle back on the table between sips. EMG activity was recorded for 3 trials of 2 sips each. No time limit was used. The subjects were not timed for this activity, as the intention was to allow the subjects to perform the task as they would normally.
Subjects were then instructed, using a combination of verbal explanation and demonstration by a physician, in how to perform pendulum exercises. In this study, correct pendulum exercises were the swinging or stooping exercises that
Codman6 originally described for the early postoperative period, which were meant to be a passive exercise for the shoulder. Alternatively, incorrect pendu-lum exercises were similar swinging ex-ercises performed using active motion of the shoulder muscles. The subjects were given as much time as they felt necessary to practice the pendulum exercise before the actual trials commenced. The subject performed the 4 types of pendulum exer-cises (large incorrect, large correct, small incorrect, and small correct) in a previ-ously determined, randomized order. The pendulum exercises were standardized by using a diagram of 10-cm-wide concen-tric circles, the largest of which was 51 cm and the smallest 20 cm in diameter, placed on the floor (FiGuRe 3). The sub-ject performed the pendulum exercise in either the incorrect or correct method for each size. Three revolutions of each pendulum were completed without any time limit. The diameter of the circle of the pendulum was assured by taping a laser pointer to the dorsal surface of the subject’s wrist and asking the subject to keep the laser essentially within a 10-cm-wide concentric circle. It was emphasized to the subject during the correct exer-cises that it was more important for the exercise to be passive than for the laser pointer to remain perfectly within the concentric circle diagram. The subject was also instructed to stop any correct pendulum trial if the subject perceived that the motion was active rather than passive.
Statistical analysisA power analysis was performed based on data collected in a pilot study of 3 sub-jects. It was based on detecting a differ-ence of 10% MVIC in the supraspinatus muscle, as the pilot data showed a stan-dard deviation of the difference between large active and passive pendulum exer-cises of 10.9% MVIC. It was determined that 12 subjects would be sufficient to provide 80% power, when controlling for type I error at 0.05 using a 2-sided test.
Statistical analyses were performed for both pendulum and ADL data. Nor-mal probability plots were prepared for each dependent variable, and it was de-termined that they were not sufficiently normal to justify using parametric statis-tical methods. Therefore, a Friedman test was used to implement a nonparametric repeated-measurements analysis of the pendulum data. This was a 2-by-2 model, with 1 factor being the experimental fac-tor of interest and the other factor being a subject. Significance was set at 0.05 for assessing main effects. When a main ef-fect was found, post hoc analyses were performed to assess pairwise differences using the method described by Pett.32 The method compares differences in average ranks, and it limits the overall type I er-ror to 0.05.
ReSultS
three activities (large cor-rect pendulums, large incorrect pendulums, and drinking from a
water bottle) showed a mean peak per-cent MVIC greater than 15% in the su-praspinatus and infraspinatus muscles. Mean peak percent MVIC and standard deviations for all activities are reported in the table. A graphic representation is included in FiGuReS 4 and 5.
Supraspinatus percent MVIC was af-fected by pendulum exercise (P.001). Post hoc analyses showed that the differ-ence in percent MVIC in the supraspi-natus between incorrect and correct pendulum exercises reached statistical significance for large-diameter pendu-
FiGuRe 3. Subject performing a pendulum exercise. The laser pointer falls within the outer dark concentric circle (arrow), indicating a large pendulum exercise.
06 Long.indd 232 3/23/10 5:29:17 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Uni
vers
ity o
f B
righ
ton
on J
uly
17, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
0 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

journal of orthopaedic & sports physical therapy | volume 40 | number 4 | april 2010 | 233
analysis was based on large pendulum data, no strong conclusions can be made
lums, but not for small-diameter pen-dulums. Because the statistical power
about the lack of differences found be-tween correct and incorrect performance of small pendulum exercises. The differ-ence in percent MVIC in the supraspina-tus for large versus small pendulums was significant for those performed both cor-rectly and incorrectly.
The statistical analysis also showed that drinking from a bottle of water had significantly higher muscle activation than typing for both the supraspinatus and the infraspinatus muscles.
diScuSSion
codman6 was one of the first to emphasize the complex nature of the shoulder joint, which allows for
equally complex motion. In 1944, Inman et al19 performed a study of shoulder mor-phology and function, as well as EMG analysis of shoulder musculature. They emphasized that shoulder muscle groups act synchronously during certain move-ments. This has important implications in rehabilitation after rotator cuff repair, because the desired effect is to maintain passive range of motion without stress-ing the repair. The effect of improperly performed postoperative pendulum ex-ercises and light ADLs after rotator cuff repair is largely unknown. Measuring the amount of muscle activation during tasks may provide information about the effect of activity on the rotator cuff. Our results indicate that the EMG activ-ity of the supraspinatus is higher when healthy subjects perform pendulum ex-ercises incorrectly in larger (51-cm diam-eter) circles, and a significant difference in activation of all 3 muscles was found between the large and small diameters for both the correctly and incorrectly performed pendulums.
Many previous researchers have exam-ined activation of the shoulder muscula-ture during active and isometric exercises for rehabilitation.1,8-10,14,17,20,23,33,41,44,47 Few, however, have looked at EMG data for ac-tivities that are meant to be passive.13,31,37,38 Dockery et al13 found approximately 5% MVIC in the rotator cuff by examining
tableMean (SD) EMG Signal Amplitude as Percent of MVIC for Activities
Abbreviations: EMG, electromyographic; MVIC, maximum voluntary isometric contraction.* Significant difference between small correct pendulum and large correct pendulum, P.05.† Significant difference between small correct pendulum and large incorrect pendulum, P.05.‡ Significant difference between small incorrect pendulum and large correct pendulum, P.05.§ Significant difference between small incorrect pendulum and large incorrect pendulum, P.05.|| Significant difference between large correct pendulum and large incorrect pendulum, P.05.¶ Significant difference between typing and drinking, P.05.# Significant difference between drinking and brushing teeth, P.05.** Significant difference between typing and brushing teeth, P.05.
Supraspinatus infraspinatus deltoid
Small correct pendulum 8.0 (6.3)*,† 14.4 (37.4)*,† 2.8 (2.0)*,†
Small incorrect pendulum 8.7 (5.1)§ 12.9 (25.8)§,‡ 4.0 (2.4)§
Large correct pendulum 13.7 (12.9)*,|| 22.4 (39.0)*,‡ 4.4 (2.7)*
Large incorrect pendulum 18.8 (15.6)†,§,|| 24.5 (41.2)§,† 6.0 (3.1)†,§
Typing 7.5 (5.1)¶ 12.0 (13.2)¶,** 2.1 (2.3)¶,**
Drinking 21.0 (20.4)¶,# 18.3 (14.8)¶ 4.4 (2.6)¶
Brushing teeth 12.1 (10.1)# 20.2 (21.3)** 4.1 (3.8)**
Small correct pendulum
Small incorrect pendulum
Large correct pendulum
Large incorrect pendulum
0.0 5.0 10.0 15.0 20.0 25.0 30.0 35.0 40.0
MVIC (%)
Deltoid Infraspinatus Supraspinatus
FiGuRe 4. Percent maximum voluntary isometric contraction (MVIC) for the pendulum exercises, with standard error.
06 Long.indd 233 3/23/10 5:29:18 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Uni
vers
ity o
f B
righ
ton
on J
uly
17, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
0 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

234 | april 2010 | volume 40 | number 4 | journal of orthopaedic & sports physical therapy
[ research report ]the supraspinatus, which is the muscle most commonly involved in rotator cuff tears.7,11,12,40,46 Kelly et al23 investigated EMG data for more intense ADLs, such as lifting 1- to 10-pound (0.5- to 4.5-kg) objects and washing the back, in subjects with symptomatic versus asymptomatic rotator cuff tears compared to healthy controls. The results of that study showed that the symptomatic patients had more EMG signal amplitude for the muscles of the torn rotator cuff tendon than the asymptomatic patients, which could ex-plain the disability of the symptomatic patients who were not compensating by using the surrounding shoulder muscula-ture.23 Interestingly, Kelly et al23 showed that the percent MVIC of the supraspi-natus was higher for all studied activities in patients with rotator cuff tears than in normal controls. For example, the activity of lifting a 1-pound (0.5-kg) weight to the level of the shoulder required less than 20% MVIC for controls but over 50% MVIC for patients with symptomatic ro-tator cuff tears.23 Although our tasks were not identical, the findings of Kelly et al23 do bring into the forefront the differences in EMG findings between healthy sub-jects and patients with rotator cuff tears. It is unclear whether patients who have had a rotator cuff repair would be more similar to a control subject or a patient with a rotator cuff tear.
While there is no definitive consensus opinion, previous reports of EMG data for the shoulder have considered activity levels of less than 20% to 25% MVIC to be low or minimal.20,29,36-38 Based on these reports, our study shows that there is at least moderate activity produced in the supraspinatus muscle by large incorrect pendulums and drinking in healthy sub-jects. However, the published EMG activ-ity designations are not standardized for percentage levels or for the definition of MVIC. For example, McCann et al29 used a different method to obtain MVIC than we used. Rather than a maximum iso-metric contraction, subjects in their study lifted a 2.25-kg weight, and the EMG out-put for this action was used as MVIC.29
surface EMG data for pendulum exercis-es, but he did not include fine-wire EMG nor did he study any ADLs. McCann et al29 studied multiple passive exercises, including the pendulum, using wire elec-trode EMG techniques. They found mini-mal activity in the supraspinatus, deltoid, and infraspinatus with pendulum exer-cises presumably performed correctly. No mention is made of the specific instruc-tions to the patient on how the exercises were to be performed.29 Smith et al36-38 have published EMG data for the immo-bilized shoulder to determine the safety of various exercises and activities after shoulder surgery. They recommended that certain motions, such as a backwards pulling motion, even if performed with the contralateral arm, should be avoided after rotator cuff repair, because the mus-cles in the operative extremity are not
quiescent.38 In several published papers, this group has studied various types of exercises, including scapulothoracic and contralateral limb movements; however, pendulum exercises and specific ADLs were not included, although some of the resisted motions were meant to simulate ADLs, such as opening a door or lifting a bag.36-38
Although standardizing ADLs is more difficult than standardizing specific re-habilitation exercises, we felt that it was important to have subjects perform ac-tual tasks rather than less-complicated motions associated with different activi-ties. While there have been some ergo-nomic studies involving keyboards that measure the EMG signal amplitude in some of the shoulder musculature dur-ing typing and similar activities, none of these studies look at the EMG data for
Brushing teeth
Typing
Drinking
0.0 5.0 10.0 15.0 20.0 25.0 30.0
MVIC (%)
Deltoid Infraspinatus Supraspinatus
FiGuRe 5. Percent maximum voluntary isometric contraction (MVIC) for tested activities of daily living, with standard error.
06 Long.indd 234 3/23/10 5:29:19 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Uni
vers
ity o
f B
righ
ton
on J
uly
17, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
0 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

journal of orthopaedic & sports physical therapy | volume 40 | number 4 | april 2010 | 235
Thus, their results may represent a lower overall muscle activity than studies that use a maximal isometric contraction, as we did. In an effort to be conservative, we designated muscle activation greater than 15% MVIC to be potentially indica-tive of higher loads than desirable in a newly repaired rotator cuff. Although our study involves healthy subjects, the goal is to help identify activities that may po-tentially be safely performed by a patient who has recently undergone rotator cuff repair. Fifteen percent MVIC correlates to 30 N of force, based on our estimates. This is lower than the lowest force (50 N) that we found in the literature for failure after cyclic loading of the rotator cuff.3-
5,16,24,25,34,35,39,42,45,48
We chose a threshold of 15% of maxi-mum activation for our data interpreta-tion, based on biomechanical calculations. One study using in vitro biomechanical testing of sutured supraspinatus defects indicated a 50% loss of repair at (mean SD) 206 88 cycles of loading at 44 15 N.3 A conservative value of 30 N was chosen as an upper limit of safe loading for the limited-repetition activities used in this study. Thirty-one N was estimated to be a percent of maximal contraction by the following procedure. Assuming supraspinatus muscle force can be mod-eled as the product of MVIC fraction (be-tween 0 and 1), muscle cross-sectional area (3.36 cm2),26 specific tension (62 N/cm2),18 and cosine of the fiber pennation angle (7.0°),26 15% MVIC corresponds to 31 N of force. While many assumptions were made in the determination of 15% MVIC and 31 N, we believe these num-bers to be conservative, yet useful for this and, potentially, future studies.
In analyzing our results, there are several reasons that large pendulum exercises could produce more muscle activity than small pendulum exercises. Performing the larger-diameter exercises may be more difficult than the smaller ex-ercises, making it harder for the subject to perform the pendulum passively. Al-ternatively, pendulum exercises may not be truly passive at all. If so, then a larger
exercise would require more muscle ac-tivity. Furthermore, although we focused on the supraspinatus, as this tendon is most frequently involved in rotator cuff tears, we did note that the data for the infraspinatus was less consistent overall. It is unclear whether even passive pen-dulum exercises may elicit relatively high muscle activation in the infraspinatus, at least in some individuals.
This study has several limitations. First, our instrumentation was limited to a 1000-Hz bandwidth. It has been reported that 5% of the power of the supraspinatus signal is greater than 510 Hz, when measured using fine-wire electrodes43; therefore, a small amount of signal may be aliased, given the sam-pling rate we used. Second, EMG is not a direct measurement of muscle force. While our EMG processing method was designed to include important elements of models to estimate muscle force from EMG, the method lacks a nonlinear transformation from muscle activation to muscle force. However, our nonparamet-ric statistical analysis is based only on the weak assumption of an ordinal scale of measurement.32 Because EMG-to-force mappings are monotonically increasing, our statistical results are independent of the exact functional relationship between computed muscle activation and muscle force.27 Third, the activity of the shoulder muscles in healthy subjects may not be representative of the activity of individu-als with a repaired rotator cuff muscle. Fourth, the average age of the volunteers is younger than the average age of pa-tients undergoing rotator cuff surgery.
If we anticipate that the findings in healthy individuals may approximate the findings in patients who have undergone rotator cuff repair, then some concern is raised about the rehabilitation of these patients postoperatively. If patients are going to perform pendulums without su-pervision, then it is important that they understand and remember to do the exercises passively in small circles (ap-proximately 20 cm in diameter). Those involved in the postoperative care of pa-
tients who have undergone rotator cuff repair may wish to consider these rec-ommendations when prescribing home exercise programs for individual patients. Currently, some clinicians and therapists instruct patients to perform pendulum exercises with the opposite arm sup-ported by a table. It is possible that sup-port of the contralateral limb may affect muscle activity in the affected shoulder during pendulum exercises. In our study, subjects were permitted to use a table for support of the contralateral limb, if pre-ferred, though most did not. Codman’s original description of the exercise did not mention contralateral arm support.
There are some patients who will lack the ability to perform pendulum exer-cises as prescribed, so supervised or as-sisted range-of-motion exercises may be safer for these individuals. Just as indi-vidual patients may perform pendulums incorrectly or differently, our subjects, although they underwent specific instruc-tion and were observed during the exer-cises, had some level of variability in the amount of muscle activity recorded with the different exercises. With regard to ADLs, those patients who wish to return to typing in the early phase after rotator cuff repair may be able to do so without placing excess strain on the repair. How-ever, even though the patient is able to perform a task, such as drinking from a bottle of water or brushing teeth, with the operative arm in a sling, the activity may not be entirely safe. Thus, patients may need specific instructions (restrictions) postoperatively for ADLs.
concluSion
Large pendulums and pendulums performed incorrectly generate more supraspinatus muscle activity in the
shoulder than smaller, correctly per-formed pendulum exercises. Based on this finding, we believe that it is possible that larger pendulum exercises may not be desirable early in rehabilitation after rotator cuff repair. In healthy individuals, drinking water from a bottle produces
06 Long.indd 235 3/23/10 5:29:20 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Uni
vers
ity o
f B
righ
ton
on J
uly
17, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
0 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

236 | april 2010 | volume 40 | number 4 | journal of orthopaedic & sports physical therapy
[ research report ]more supraspinatus muscle activity than typing. Drinking water from a bottle may also not be desirable immediately after rotator cuff repair. t
keY pointSFindinGS: Large pendulums and pendu-lums performed incorrectly generate more supraspinatus muscle activity than smaller, correctly performed pendulum exercises.implicationS: Smaller pendulums (20 cm in diameter) may be safer for patients who have had rotator cuff repair.caution: EMG is not a direct measure-ment of muscle force, so translation of EMG results to imply muscle force should be done with caution. Further, findings in healthy subjects may not replicate the findings in patients with rotator cuff repair.
ACKNOWLEDGEMENTS: The authors thank Chris Gatti for his assistance in MATLAB programming and data analysis, and Kristi Overgaard for her assistance with manuscript preparation and revision.
ReFeRenceS
1. Alpert SW, Pink MM, Jobe FW, McMahon PJ, Mathiyakom W. Electromyographic analysis of deltoid and rotator cuff function under vary-ing loads and speeds. J Shoulder Elbow Surg. 2000;9:47-58.
2. Basmajian JV, De Luca CJ. Muscles Alive: Their Functions Revealed by Electromyography. 5th ed. Baltimore, MD: Williams and Wilkins; 1985.
3. Bicknell RT, Harwood C, Ferreira L, et al. Cy-clic loading of rotator cuff repairs: an in vitro biomechanical comparison of bioabsorbable tacks with transosseous sutures. Arthroscopy. 2005;21:875-880. http://dx.doi.org/10.1016/j.arthro.2005.03.009
4. Burkhart SS, Diaz Pagan JL, Wirth MA, Atha-nasiou KA. Cyclic loading of anchor-based rotator cuff repairs: confirmation of the tension overload phenomenon and comparison of su-ture anchor fixation with transosseous fixation. Arthroscopy. 1997;13:720-724.
5. Burkhart SS, Johnson TC, Wirth MA, Athanasiou KA. Cyclic loading of transosseous rotator cuff repairs: tension overload as a possible cause of failure. Arthroscopy. 1997;13:172-176.
6. Codman EA. The Shoulder: Rupture of the Supraspinatus Tendon and Other Lesions in or
About the Subacromial Bursa. Malabar, FL: G. Miller and Co Medical Publishers, Inc; 1984.
7. Cook C, Burgess-Limerick R, Papalia S. The effect of upper extremity support on up-per extremity posture and muscle activity during keyboard use. Applied Ergonomics. 2004;35:285-292.
8. Cordasco FA, Wolfe IN, Wootten ME, Bigliani LU. An electromyographic analysis of the shoulder during a medicine ball rehabilitation program. Am J Sports Med. 1996;24:386-392.
9. Dark A, Ginn KA, Halaki M. Shoulder muscle recruitment patterns during commonly used ro-tator cuff exercises: an electromyographic study. Phys Ther. 2007;87:1039-1046. http://dx.doi.org/10.2522/ptj.20060068
10. David G, Magarey ME, Jones MA, Dvir Z, Turker KS, Sharpe M. EMG and strength correlates of selected shoulder muscles during rotations of the glenohumeral joint. Clin Biomech (Bristol, Avon). 2000;15:95-102.
11. Delisle A, Lariviere C, Plamondon A, Imbeau D. Comparison of three computer office work-stations offering forearm support: impact on upper limb posture and muscle activation. Ergonomics. 2006;49:139-160. http://dx.doi.org/10.1080/10610270500450739
12. Dennerlein JT, Johnson PW. Different com-puter tasks affect the exposure of the upper extremity to biomechanical risk factors. Ergonomics. 2006;49:45-61. http://dx.doi.org/10.1080/00140130500321845
13. Dockery ML, Wright TW, LaStayo PC. Elec-tromyography of the shoulder: an analysis of passive modes of exercise. Orthopedics. 1998;21:1181-1184.
14. Fujisawa H, Suenaga N, Minami A. Electromyo-graphic study during isometric exercise of the shoulder in head-out water immersion. J Shoul-der Elbow Surg. 1998;7:491-494.
15. Galatz LM, Ball CM, Teefey SA, Middleton WD, Yamaguchi K. The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg Am. 2004;86-A:219-224.
16. Goradia VK, Mullen DJ, Boucher HR, Parks BG, O’Donnell JB. Cyclic loading of rotator cuff re-pairs: A comparison of bioabsorbable tacks with metal suture anchors and transosseous sutures. Arthroscopy. 2001;17:360-364.
17. Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ. Electromyographic activity and applied load during shoulder rehabilitation exer-cises using elastic resistance. Am J Sports Med. 1998;26:210-220.
18. Ikai M, Fukunaga T. Calculation of muscle strength per unit cross-sectional area of human muscle by means of ultrasonic measurement. Int Z Angew Physiol. 1968;26:26-32.
19. Inman VT, Saunders M, Abbott LC. Observations on the function of the shoulder joint. J Bone Joint Surg Am. 1944;26:1-30.
20. Jenp YN, Malanga GA, Growney ES, An KN. Acti-vation of the rotator cuff in generating isometric shoulder rotation torque. Am J Sports Med.
1996;24:477-485. 21. Jobe FW, Moynes DR, Tibone JE, Perry J. An
EMG analysis of the shoulder in pitching. A sec-ond report. Am J Sports Med. 1984;12:218-220.
22. Kelly BT, Kadrmas WR, Speer KP. The manual muscle examination for rotator cuff strength. An electromyographic investigation. Am J Sports Med. 1996;24:581-588.
23. Kelly BT, Williams RJ, Cordasco FA, et al. Differ-ential patterns of muscle activation in patients with symptomatic and asymptomatic rotator cuff tears. J Shoulder Elbow Surg. 2005;14:165-171. http://dx.doi.org/10.1016/j.jse.2004.06.010
24. Kim DH, Elattrache NS, Tibone JE, et al. Bio-mechanical comparison of a single-row versus double-row suture anchor technique for rotator cuff repair. Am J Sports Med. 2006;34:407-414. http://dx.doi.org/10.1177/0363546505281238
25. Klinger HM, Steckel H, G. S, Buchhorn GH, Baums MH. Biomechanical comparison of double-loaded suture anchors using arthroscop-ic Mason-Allen stitches versus traditional transosseous suture technique and modified Mason-Allen stitches for rotator cuff repair. Clin Biomech (Bristol, Avon). 2007;22:106-111.
26. Langenderfer J, Jerabek SA, Thangamani VB, Kuhn JE, Hughes RE. Musculoskeletal parameters of muscles crossing the shoul-der and elbow and the effect of sarcomere length sample size on estimation of optimal muscle length. Clin Biomech (Bristol, Avon). 2004;19:664-670. http://dx.doi.org/10.1016/j.clinbiomech.2004.04.009
27. Lloyd DG, Besier TF. An EMG-driven musculosk-eletal model to estimate muscle forces and knee joint moments in vivo. J Biomech. 2003;36:765-776.
28. Manal K, Gonzalez RV, Lloyd DG, Buchanan TS. A real-time EMG-driven virtual arm. Comput Biol Med. 2002;32:25-36.
29. McCann PD, Wootten ME, Kadaba MP, Bigliani LU. A kinematic and electromyographic study of shoulder rehabilitation exercises. Clin Orthop Relat Res. 1993;179-188.
30. Millett PJ, Wilcox RB, 3rd, O’Holleran JD, Warner JJ. Rehabilitation of the rotator cuff: an evalua-tion-based approach. J Am Acad Orthop Surg. 2006;14:599-609.
31. Misamore GW, Ziegler D, Higgin botham G. Passive range of motion exercises of the shoul-der: an EMG analysis. J Shoulder Elbow Surg. 1993;2:S27.
32. Pett MA. Nonparametric Statistics for Health Care Research: Statistics for Small Samples and Unusual Distributions. Thousand Oaks, CA: SAGE Publications, Inc; 1997.
33. Reinold MM, Wilk KE, Fleisig GS, et al. Elec-tromyographic analysis of the rotator cuff and deltoid musculature during common shoulder external rotation exercises. J Orthop Sports Phys Ther. 2004;34:385-394. http://dx.doi.org/10.2519/jospt.2004.0665
34. Rossouw DJ, McElroy BJ, Amis AA, Emery RJ. A biomechanical evaluation of suture anchors in repair of the rotator cuff. J Bone Joint Surg Br.
06 Long.indd 236 3/23/10 5:29:21 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Uni
vers
ity o
f B
righ
ton
on J
uly
17, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
0 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

journal of orthopaedic & sports physical therapy | volume 40 | number 4 | april 2010 | 237
1997;79:458-461. 35. Smith CD, Alexander S, Hill AM, et al. A biome-
chanical comparison of single and double-row fixation in arthroscopic rotator cuff repair. J Bone Joint Surg Am. 2006;88:2425-2431. http://dx.doi.org/10.2106/JBJS.E.00697
36. Smith J, Dahm DL, Kaufman KR, et al. Electro-myographic activity in the immobilized shoulder girdle musculature during scapulothoracic exer-cises. Arch Phys Med Rehabil. 2006;87:923-927. http://dx.doi.org/10.1016/j.apmr.2006.03.013
37. Smith J, Dahm DL, Kotajarvi BR, et al. Elec-tromyographic activity in the immobilized shoulder girdle musculature during ipsilateral kinetic chain exercises. Arch Phys Med Rehabil. 2007;88:1377-1383. http://dx.doi.org/10.1016/j.apmr.2007.07.028
38. Smith J, Padgett DJ, Dahm DL, et al. Electro-myographic activity in the immobilized shoulder girdle musculature during contralateral upper limb movements. J Shoulder Elbow Surg. 2004;13:583-588. http://dx.doi.org/10.1016/S1058274604001259
39. Sward L, Hughes JS, Amis A, Wallace WA. The strength of surgical repairs of the rotator cuff. A biomechanical study on cadavers. J Bone Joint
Surg Br. 1992;74:585-588. 40. Szeto GP, Straker LM, O’Sullivan PB. A compari-
son of symptomatic and asymptomatic office workers performing monotonous keyboard work--1: neck and shoulder muscle recruitment patterns. Man Ther. 2005;10:270-280. http://dx.doi.org/10.1016/j.math.2005.01.004
41. Takeda Y, Kashiwaguchi S, Endo K, Matsuura T, Sasa T. The most effective exercises for strengthening the supraspinatus muscle: evalu-ation by magnetic resonance imaging. Am J Sports Med. 2002;30:374-381.
42. Tingart MJ, Apreleva M, Lehtinen J, Zurakowski D, Warner JJ. Anchor design and bone mineral density affect the pull-out strength of suture anchors in rotator cuff repair: which anchors are best to use in patients with low bone quality? Am J Sports Med. 2004;32:1466-1473.
43. Tomlinson DP, Vanadurongwan B, Henn F, et al. A spectral analysis of healthy rotator cuff muscula-ture electromyographic activity: surface and fine wire. Gait and Clinical Movement Analysis Soci-ety 13th Annual Meeting. Richmond, VA: 2008.
44. Uhl TL, Carver TJ, Mattacola CG, Mair SD, Nitz AJ. Shoulder musculature activation during up-per extremity weight-bearing exercise. J Orthop
Sports Phys Ther. 2003;33:109-117. 45. Waltrip RL, Zheng N, Dugas JR, Andrews JR.
Rotator cuff repair. A biomechanical com-parison of three techniques. Am J Sports Med. 2003;31:493-497.
46. Westad C, Mork PJ, Westgaard RH. Firing pat-terns of low-threshold trapezius motor units in feedback-controlled contractions and vocational motor activities. Exp Brain Res. 2004;158:465-473. http://dx.doi.org/10.1007/s00221-004-1925-y
47. Worrell TW, Corey BJ, York SL, Santiestaban J. An analysis of supraspinatus EMG activity and shoulder isometric force development. Med Sci Sports Exerc. 1992;24:744-748.
48. Zheng N, Harris HW, Andrews JR. Failure analy-sis of rotator cuff repair: a comparison of three double-row techniques. J Bone Joint Surg Am. 2008;90:1034-1042. http://dx.doi.org/10.2106/JBJS.G.00049
@ moRe inFoRmationWWW.jOSpT.OrG
GO GREEN By Opting Out of the Print Journal
JOSPT subscribers and APTA members of the Orthopaedic and Sports Physical Therapy Sections can help the environment by “opting out” of receiving the Journal in print each month as follows. If you are:
· A JOSPT subscriber: Email your request to [email protected] or call the Journal o�ce toll-free at 1-877-766-3450 and provide your name and subscriber number. · An APTA Orthopaedic or Sports Section member: Go to www.apta.org and update your preferences in the My Profile area of myAPTA. Select “myAPTA” from the horizontal navigation menu (you’ll be asked to login, if you haven’t already done so), then proceed to “My Profile.” Click on the “Email & Publications” tab, choose your “opt out” preferences and save.
Subscribers and members alike will continue to have access to JOSPT online and can retrieve current and archived issues anytime and anywhere you have Internet access.
06 Long.indd 237 3/23/10 5:29:21 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Uni
vers
ity o
f B
righ
ton
on J
uly
17, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
0 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.















![[ILO UNESCO WHO] CBR a Strategy for Rehabilita(BookFi.org)](https://img.pdfslide.us/doc/110x75/577cd0101a28ab9e78914bec/ilo-unesco-who-cbr-a-strategy-for-rehabilitabookfiorg.jpg)