Embed Size (px)
Citation preview

Activated Extracellular Signal-Regulated Kinase Is an IndependentPrognostic Factor in ClinicallyConfined Renal Cell CarcinomaLee Campbell, PhD1; Rosa Nuttall, M Pharm1; David Griffiths, MB BCh2; and Mark Gumbleton, PhD1
BACKGROUND: Extracellular signal-regulated kinase (ERK) promotes proliferation, metastasis, and poor
survival in cancers of the breast, lung, and liver. Advanced localized renal cell carcinoma (RCC) is extraordi-
narily treatment resistant and has high recurrence rates despite surgery. Limited data exist regarding the
prognostic significance of activated (phosphorylated) ERK in RCC. The authors hypothesized that activated
ERK (pERK) promotes disease progression and metastasis in localized RCC and may be of value as a bio-
marker to predict disease recurrence. METHODS: The expression profile of pERK was examined by immu-
nocytochemistry using a tissue microarray constructed from 174 drug treatment–naive patients who had
undergone radical nephrectomy for localized RCC. Levels of tumor-cell specific pERK were scored and cor-
related with clinicopathologic parameters of RCC and disease-free survival. RESULTS: Immunostaining for
pERK was present in 36% of all RCCs, with a predominance found in the clear cell histologic subtype. High
expression was associated with increased tumor size, increased TNM stage, and vascular invasion. Patients
with pERK-positive tumors had a mean disease-free survival of 4.19 years, compared with 6.38 years for
patients with pERK-negative tumors (P < .001). Cox regression models revealed pERK to be a significant in-
dependent predictor of disease-free survival, with a hazards score of 2.9 (P < .001), a value similar to tumor
grade (hazards ratio, 3.01; P < .001). CONCLUSIONS: Expression of pERK is an independent prognostic fac-
tor in RCC that is associated with advanced and aggressive pathologic features of renal tumors and pre-
dicts the onset of metastasis in patients with localized disease. Cancer 2009;115:3457–67. VC 2009
American Cancer Society.
KEY WORDS: biomarkers, ERK-1/2, prognostic factors, renal cell carcinoma, tyrosine kinase inhibitors.
Renal cell carcinoma (RCC) is a heterogeneous group of highly vascularized invasive kidney tumors,comprising clear cell or conventional (accounting for 60%-80% of all RCC cases), papillary, chromo-phobe, and collecting duct subtypes.1 Currently, RCC represents 3% of all cancers and 2% of all cancer-related deaths and is also 1 of the few cancers whose incidence and mortality rates are growing steadily
Received: October 29, 2008; Revised: December 30, 2008; Accepted: January 5, 2009
Published online: June 12, 2009 VC 2009 American Cancer Society
DOI: 10.1002/cncr.24389, www.interscience.wiley.com
Corresponding author: David Griffiths, MB BCh, Department of Pathology, School of Medicine, Cardiff University, Heath Park, Cardiff CF14 4XN, UK;
[email protected] or Mark Gumbleton PhD, Welsh School of Pharmacy, Cardiff University, King Edward VII Avenue, Cardiff CF10 3NB, UK;
1Welsh School Of Pharmacy, Cardiff University, Cardiff, United Kingdom; 2Department of Pathology, School of Medicine, Cardiff University, Cardiff,
United Kingdom
We thank Dr. Julia Gee, Mrs. Susan Kyme, and Mrs. Pauline Finley of the Tenovus Research Group (Cardiff University) for advice and assistance with
the immunocytochemistry procedures, and Chris von Ruhland for help with image acquisition.
Cancer August 1, 2009 3457
Original Article

worldwide.2,3 Approximately one-third of all RCCpatients will have established metastatic disease at firstpresentation; the remainder with clinically localizedtumors usually undergo curative radical nephrectomy.Approximately 35% to 45% of these will also eventuallydevelop disease recurrence with metastasis at distantsites.2,3 However, the clinical course of those presentingwith localized disease is difficult to predict, even withinpatients who have similar clinicopathologic parameters.This reflects intrinsic differences in the molecular and bio-logic profiles of individual tumors.4
Historically, survival rates for metastatic RCC rarely
exceed 5%, resulting from the inherently refractive nature
of tumors to standard chemotherapy, radiotherapy, and
hormonal therapy.5 The last decade, however, has wit-
nessed an explosion in the understanding of the biologic
behavior of renal neoplasms and the identification of how
key signaling cascades and their molecular determinants
integrate to drive disease progression. This preclinical evi-
dence has led to the emergence of rationally designed
novel drugs that specifically target these aberrant signaling
pathways.6-8 The most developed targeted therapies cur-
rently in use for the treatment of advanced localized and
metastatic RCC are sorafenib and sunitinib, 2 orally active
multikinase inhibitors, and temsirolimus, an inhibitor of
the mammalian target of rapamycin (mTOR).9 Indeed,
temsirolimus, when used as a single agent, is shown to sig-
nificantly improve overall survival of patients with meta-
static cancer compared with standard therapies for
RCC.10 Despite these advances, challenges within the
field still exist and include among others the need to 1)
optimize the use of such targeted therapies by identifying
patients with high-risk disease who are most likely to ben-
efit from their use as single agents or in combination, and
2) evaluate the efficacy of targeted therapies in nonclear
cell RCC subgroups for which no specific trials have been
reported.11 Therefore the utility of tumor biomarkers that
not only identify high-risk patients but also have value in
guiding treatment decisions for RCC is increasingly real-
ized.4,12-14
The epidermal growth factor receptor (EGF-R)/
Ras/extracellular signal-regulated kinase (ERK) axis is
shown to be mutationally activated or overexpressed in a
significant number (>30%) of all cancers.15 Once acti-
vated (phosphorylated), the terminal protein kinases,
ERK-1/2, are translocated to the nucleus, whereupon an
extensive array of transcription factors are activated,
including among others Elk-1, Fos, and Stat-3.16 These
regulatory mechanisms lead to global changes in gene
expression profiles that mainly, but not unequivocally,
result in promotion of cell growth. Aberrant ERK signal-
ing is associated with other cancer-related processes,
namely tumor angiogenesis, cell migration and invasion,
and drug resistance.17,18 Together this has led to intense
pharmaceutical interest in developing tyrosine kinase
inhibitors that target signal transduction cascades such
as the EGF-R/Ras/ERK and PI-3K/AKT/mTOR
cascades.19,20
Much of the current literature that lends support for
ERK-1/2 serving as a cancer driver has been generated by
the use of in vitro, ex vivo, and mouse cancer models, with
an actual paucity of studies that report its expression, ac-
tivity, and significance in clinical tumor specimens.21 Of
the clinical immunohistologic studies undertaken to date,
phosphorylated ERK (pERK) has been shown to correlate
with disease progression in melanoma,22 hepatocellular,23
and nonsmall cell lung carcinomas.24 In hepatocellular
carcinoma, pERK is predominantly expressed in poorly
differentiated tumors, and as such serves as a powerful
prognostic factor.23 In this latter study, pERK also was
found to be correlated with the presence of intrahepatic
metastasis, and could retrospectively predict disease recur-
rence in patients after the complete surgical removal of
initial tumors.23 Trends of increasing levels of pERK have
also been observed in late-stage disease in both lung carci-
noma23 and melanoma,22 but it is not an independent
prognostic factor in either disease when analyzed for
patient survival. Conversely, the expression of pERK-1/2
in endometrial cancer25 has been shown to be an inde-
pendent prognostic indicator associated with a favorable
prognosis. Specifically, patients whose tumors exhibited
low levels of pERK-1/2 actually had significantly lower
disease-free survival and worse overall survival.25 A di-
chotomy in the impact of activated ERK also exists within
the same cancer type. For example, in some breast cancer
patient cohorts, high activated ERK-1/2 levels are report-
edly associated with early stage tumors and negative
lymph node status, and predict long disease-free sur-
vival.21 In others, its high expression is reported to corre-
late with advanced localized or metastatic disease,
tamoxifen resistance, and reduced time to disease recur-
rence.26 These apparent contradictions may reflect the
Original Article
3458 Cancer August 1, 2009

disease stage and context dependency of ERK-1/2. In sup-
port of this notion, in vitro studies have shown that varia-
tions in the magnitude and spatiotemporal expression of
pERK-1/2 can either potentiate proliferation or alter-
nately drive cellular differentiation and senescence.27
The prognostic significance of activated ERK-1/2 in
RCC remains undetermined. To test the hypothesis that
constitutively activated ERK-1/2 may potentiate disease
progression in RCC, we have examined, using tissue
microarray technology, the expression of pERK-1/2 in
176 RCCs resected from patients who had undergone
radical nephrectomy for the treatment of localized disease.
The relative expression of activated ERK-1/2 was corre-
lated with clinical and pathologic variables of RCC, with
the overall aim of determining whether pERK-1/2 might
have prognostic value in RCC patients.
MATERIALS AND METHODS
Patient Selection
Archival tumor specimens were identified from the patho-
logic records and consisted of a consecutive series of 174
patients who had undergone curative radical nephrectomy
for primary kidney tumors presenting between 1992 and
1996. This series of patients (for which ethical approval
was granted by the National Health Service local research
ethics committee) has been previously described else-
where.28 Tissue blocks, histology reports, and slides were
available in all cases without a priori knowledge of clinical
outcome. For each renal carcinoma, a tissue block was
selected that contained a sample of peripheral tumor for
making the tissue microarray (TMA). Tumors were classi-
fied according to: the Hiedelberg system29 and Furhman
nuclear grade30; the presence or absence of any vascular
invasion (either microvascular invasion, renal vein inva-
sion, or inferior vena cava invasion)31; and whether or not
there was capsular invasion with cellular invasion of peri-
nephric fat.32 No patients had received drug treatment or
had evidence of lymph node or distant metastatic disease
before or at surgery.
The median age of the 174 patients was 65 years
(range, 34 years-88 years); 119 were men and 55 were
women. Complete clinical follow-up was performed as
previously described.31,33 Briefly, patients had been
reviewed annually as out-patients for 3 to 7 years (mean
follow-up, 4.3 years; median follow-up, 3.92 years [range,
0.3 years-8.09 years]) with the following information
extracted from their records: date of birth, sex, date of sur-
gery, date patient last seen, date on which recurrent or
metastatic disease was first identified, and date and cause
of death. For patients in whom the cause of death was
recorded as RCC but whose time of recurrence was
unavailable, the date of death was considered the endpoint
for disease-free survival.
TMA Construction and
Immunocytochemistry
The customized TMA was constructed with a Beechers
manual tissue arrayer (Beechers Instruments, Inc, Sun
Prairie, Wis) from archived paraffin-embedded renal tu-
mor samples. A single core of representative peripheral tu-
mor (0.6 mm in diameter) was punched from each donor
block, using a specific orientation transplanted into a pre-
molded recipient paraffin wax block. Peripheral tumor
refers to representative viable tumor tissue taken within 5
mm of the growing edge of the tumor. Additional cores
were taken from normal renal tissue (adjacent to some of
the tumors). Serial sections were cut from the resulting
TMA block onto cleaned adhesive glass slides (Superfrost
Plus, Microm International, Walldorf, Germany) at 4 lmthickness.
Array sections were dewaxed using a sequential series
of graded xylenes and alcohols. The detection of pERK-
1/2 was undertaken using previously published proce-
dures.26 Briefly, after removal of paraffin wax, the endoge-
nous peroxidase activity within the rehydrated tissue was
quenched (3% hydrogen peroxide for 5 minutes). Antigen
retrieval consisted of microwaving TMA sections in citric
acid (0.1 M, pH 6.0) for 30 minutes, followed by slide
cooling with running tap water. After draining, the sec-
tions were equilibrated in 20% normal human serum
(Golden West Biologicals Inc, Temecula, Calif) for 15
minutes at room temperature (diluent, phosphate-buf-
fered saline [PBS]). The primary rabbit antihuman
pERK-1/2 antibody (New England Biolabs, Hitchin,
UK) was applied to each section at a dilution of 1:25 and
incubated overnight at 4�C for a total of 16 hours. There-
after, the sections were washed (4 � 1 minutes) with PBS
(pH 7.3), and tissue was immunostained using the
DAKO rabbit Envision staining system (DAKO,
Prognostic Significance of pERK in RCC/Campbell et al
Cancer August 1, 2009 3459

Cambridge, UK) according to the manufacturer’s instruc-
tions. The TMA sections were counterstained with hema-
toxylin and finally mounted.
Controls and Scoring of Stained Specimens
Human breast cancer specimens, known to be positive for
pERK-1/2, were run in parallel and served as an appropri-
ate control for evaluation of staining in the kidney tissue.
Negative controls consisted of RCC TMA and breast can-
cer sections in which the primary antibody had been omit-
ted and replaced with 20% normal human serum
(isotypic control).
Scoring of tumor arrays was performed by a patholo-
gist (D.G.) and research associates (L.C. and R.N.) with-
out knowledge of other pathologic and clinical data.
Expression of pERK-1/2 was assessed semiquantitatively
accordingly to previously described criteria,28,33 with
slight modifications. This scoring system accounts for
both the intensity of immunostain within the nucleus and
cytoplasm of tumor cells and the percentage of tumor cells
involved in each core. Scoring was as follows: 0 indicates
no detectable reaction product (deposit) in tumor cells; 1
indicates very light diffuse or focal light deposit in tumor
cells; 2 indicates light diffuse or moderate focal deposit
(may include very small areas of heavy deposit); and 3
indicates tumor cores containing areas of heavy deposit in
most or all tumor cells.
Data and Statistical Analysis
Analysis of disease-free survival of patients with tumors
demonstrating different scores of staining for pERK-1/2
was performed using the Kaplan-Meier method using
the log-rank test, in which the first appearance of metas-
tasis was considered an event. Patients last seen alive
without metastasis or who died because of causes other
than RCC were considered censored at the date of last
contact or death, respectively. Scores were also con-
verted to a binary simple covariate designated positive
or negative by thresholding according to the most in-
formative split on the initial Kaplan-Meier analysis. For
pERK-1/2, a score of 0 was negative, and a score of 1 or
2 or 3 was positive. The association of positive pERK-
1/2 expression with recognized histologic tumor prog-
nostic variables (grade, size, vascular invasion, capsular
invasion, and tumor type) was examined by cross-tabu-
lation and the chi-square test.
Multivariate analysis by Cox regression was per-
formed to determine whether positive pERK-1/2 expres-
sion had influence on prediction of disease outcome in
relation to other clinical prognosticators for RCC. Previ-
ous analysis had already determined that the most influen-
tial covariates predicting disease-free survival of these
patients are Fuhrman grade (grades 1 and 2 and grades 3
and 4, respectively, are pooled for analysis), any degree of
vascular invasion (histological correlate of stage T2b), and
invasion of perinephric tissues (ie, capsular invasion and
histological correlate of stage T2a). When these covariates
are taken into consideration, tumor size and type were
found to have no influence on disease-free survival. There-
fore, in this current computation, pERK-1/2 was entered
into the multivariate analysis as an independent covariate,
using the enter function together with the covariates
grade, presence or absence of vascular invasion, and inva-
sion of perinephric tissue.
RESULTS
Immunohistochemistry for Activated ERK-
1/2 in Clinically Confined RCC
Of the 174 cases, 164 were assessable on the array; of
these, 60 (36%) stained positive for pERK-1/2. Immuno-
reactivity for pERK was detected in both the nucleus and
cytoplasm of tumor cells. In all cases examined, some
degree of cytoplasmic staining coexisted with nuclear
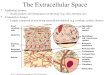
staining (Fig. 1). Cases that scored 1, in which staining
was predominantly light and diffuse, comprised 50% (30
of 60) of all pERK-positive cases. Moderate staining
(score 2) and more extensive heavy immunoreactivity
(score 3) accounted for 35% (21 of 60) and 15% (9 of 60)
of cases, respectively (Fig. 1).
Cross-tabulation of pERK-1/2 with conventional
determinants for RCC is shown in Table 1. Increased
expression levels of pERK-1/2 was found to be correlated
with tumor size (P ¼ .039), TNM staging (P ¼ .013),
and vascular invasion (P ¼ .022). No correlation was
observed between tumor grade and capsular invasion.
Notably increased expression of pERK-1/2 was found to
be significantly associated (P ¼ .006) with nonpapillary
tumors (of which 98% were of the clear cell type) when
Original Article
3460 Cancer August 1, 2009

FIGURE 1. This is a representative tissue microarray of clinically confined renal cell carcinoma demonstrating the immunohisto-
chemical expression intensity and pattern of phosphorylated extracellular signal-regulated kinase in tumors that were typically
(A) score 0 (negative), (B) score 1, (C) score 2, and (D) score 3.
Prognostic Significance of pERK in RCC/Campbell et al
Cancer August 1, 2009 3461

compared with the papillary subtype. It is interesting to
note that only 25 of 104 (24%) of patients with pERK-
negative tumors developed disease recurrence, compared
with 40% (12 of 30), 57% (12 of 21), and 56% (5 of 9) of
patients whose tumors had pERK positive scores of 1, 2,
and 3, respectively; note that pERK positive-tumors
accounted for 53% (29 of 54) of the total number of
recurrences within this patient cohort (Table 1).
Activated ERK-1/2 and Disease-free
Survival Analysis in Clinically Confined RCC
Univariate survival analysis (Kaplan-Meier) indicated that
patients with tumors that did not express pERK-1/2 had a
mean disease-free survival of 6.38 years (95% confidence
interval [95% CI], 5.80 years-6.96 years) compared with
4.83 years (95% CI, 3.68 years-5.98 years) for patient
samples scored as 1, 3.53 years (95% CI, 2.12 years-4.95
years) for patient samples scored as 2, and 3.93 years
(95% CI, 2.15 years-5.70 years) for patient samples
scored as 3. Therefore, increasing levels of pERK-1/2 in
tumor samples resected from RCC patients resulted in a
significantly (P ¼ .0017) shorter time to disease recur-
rence (Fig. 2 Top). This survival analysis also indicated
that patients whose tumors displayed any evidence of
pERK-1/2 staining had significantly shorter time to dis-
ease recurrence than patients whose tumors were negative
(Fig. 2 Top). This allowed a separate analysis to be under-
taken, in which tumors simply could be categorized as
positive or negative. In this analysis, patients with pERK-
1/2–positive tumors had a highly significant (P ¼ .0007)
reduced disease-free survival of 4.19 years (95% CI, 3.36
years-5.03 years), compared with 6.38 years (95% CI,
5.80 years-6.96 years) for patients with pERK-1/2–nega-
tive tumors (Fig. 2 Bottom). By implication, expression of
pERK-1/2 per se can be used to predict disease-free sur-
vival in patients with RCC.
Cox Regression Multivariate Analysis
By using multivariate Cox proportional hazards regression
models, we next evaluated whether the expression of
pERK-1/2 could be of prognostic value in the assessment
of primary renal tumors (Table 2). We have previously
shown31 the covariates of tumor grade, vascular invasion,
and capsular invasion to be influential prognostic factors
in RCC, but when tumor size and tumor type were not.
Therefore, tumor grade, vascular invasion, and capsular
invasion together with pERK were entered into the
model. The analysis revealed that pERK-1/2 was a
Table 1. Relation Between pERK-1/2 Expression Score and Conventional Clinicopathologic Parameters in Patients WithClinically Confined RCC*
Prognostic Indices Phosphorylated ERK-1/2† Recurrence,n (%)
0, n5104 1, n530 2, n521 3, n59 Total, n5164
Tumor grades 1 and 2 75 23 12 8 118 25 (21)
Tumor grades 3 and 4 29 7 9 1 46 29 (63)
TNM T1 50 13 3 1 67 10 (15)
TNM T2 28 5 8 2 43 10 (23)
TNM T3 and T4z 26 12 10 6 54 34 (63)
Tumor size <7 cm 55 17 4 3 79 17 (22)
Tumor size >7 cmz 49 13 17 6 85 37 (44)
Vascular invasion absent 71 15 11 4 101 18 (18)
Vascular invasion presentz 33 15 10 5 63 36 (57)
Capsular invasion absent 90 26 15 6 137 32 (23)
Capsular invasion present 14 4 6 3 27 22 (82)
Nonpapillaryz 84 29 21 8 142 51 (36)
Papillary 20 1 0 1 22 3 (14)
Recurrence, n (%) 25 (24) 12 (40) 12 (57) 5 (56) 54 (36%)
pERK indicates phosphorylated extracellular signal-regulated kinase; RCC, renal cell carcinoma.
* For information purposes, the percentage of disease recurrence in each category is included.
yFor contingency tables of the individual prognostic and pERK-1/2 covariates, the P values derived from chi-square testing are as follows: grade, P ¼ .755;
TNM T classification, P ¼ .013; tumor size, P ¼ .039; vascular invasion, P ¼ .022; capsular invasion, P ¼ .083; and nonpapillary versus papillary, P ¼ .006.
zDenotes statistical significance (P < .05) with respect to pERK-1/2.
Original Article
3462 Cancer August 1, 2009

significant influential predictor of shortened disease-free
survival with a hazards ratio (HR) of 2.96 (P < .001). Of
note, the predictive value of pERK-1/2 was significantly
higher than the HR of vascular invasion (HR, 1.58; P ¼.20) and only slightly lower than that of the powerful
and robust prognostic indicator tumor grade (HR, 3.01;
P< .001).
DISCUSSION
Previous clinicopathologic studies have shown that acti-
vated ERK is a reliable predictor of disease progression in
several diverse cancers that include malignancies of the
liver,23 lung,24 and breast.26 Oka et al34 demonstrated a
statistically significant association between pERK expres-
sion and grade in a small series of 25 patients with RCC.
However, they determined activated ERK levels through
Western blot analysis of whole tumor homogenates, an
approach that suffers from population averaging effects
of contaminating nontumor cells contributed by stromal
and vascular compartments. Although experimental
studies with renal cancer cell lines and tumor xenografts
have provided important insights into the role of pERK
in several disease processes, such as invasion and angio-
genesis,35-38 the significance of pERK with respect to
disease progression and survival of patients with RCC
remains unknown. In this current study, we used immu-
nocytochemistry and TMA technologies to examine the
prognostic relevance of pERK expression in 164 cases of
RCC. To allow the direct assessment of the role of
pERK expression in disease progression and to circum-
vent the issues of drug treatment and coexistent meta-
static disease in data interpretation, our unique patient
cohort was selected on the basis that subjects: 1) pre-
sented with clinically confined disease only, and 2) had
not received any therapy before surgery. Herein we pro-
vide what to our knowledge is the first demonstration
that pERK expression correlates with aggressive and
advanced histopathologic indices of RCC and poor dis-
ease-free survival. In addition, our analysis also demon-
strated that pERK serves as a highly significant and
independent prognostic biomarker that predicts disease
progression in RCC.
In this study, increased expression of pERK-1/2 was
found to be correlated with the conventional
Table 2. Multivariate Cox Regression Hazards Model forTime to Disease Recurrence
Prognostic Indice/ModelIncluding VascularInvasion (No.)
HR 95% CI P-value
Grade 1 and 2 (118) 1
Grade 3 and 4 (46) 3.01 1.59-5.72 <.001
No capsular invasion present (137) 1
Capsular invasion present (27) 4.04 2.12-7.69 <.001
No vascular invasion present (101) 1
Vascular invasion present (63) 1.58 0.78-3.19 .20
pERK-1/2 negative (104) 1
pERK-1/2 positive (60) 2.96 1.69-5.67 <.001
HR indicates hazards ratio; 95% CI, 95% confidence interval; pERK, phos-
phorylated extracellular signal-regulated kinase.
FIGURE 2. Kaplan-Meier metastasis-free survival plots of re-
nal cell carcinoma patients with clinically confined disease
are (Top) based on phosphorylated extracellular signal-regu-
lated kinase (pERK) score and (Bottom) stratified by ‘‘posi-
tive’’ versus ‘‘negative’’ pERK expression.
Prognostic Significance of pERK in RCC/Campbell et al
Cancer August 1, 2009 3463

clinicopathologic variables of tumor size and vascular
invasion. The association of pERK-1/2 with tumor size is
perhaps expected, given that ERK activation has been his-
torically connected with cell proliferation. Nevertheless,
this correlation is highly relevant, because tumor size is an
important prognosticator for patient survival in RCC,39
and is a histopathologic criterion that is incorporated into
the universally accepted TNM classification system used
for staging renal tumors.40 In addition to its direct effect
on cancer cell proliferation, pERK-1/2 may also contribute
to tumor size in RCC via the promotion of angiogenesis,
thereby maintaining the supply of oxygen and nutrients to
the tumor, affording uncompromised growth. Hypoxia-in-
ducible factor 1a (HIF-1a), a key molecule that facilitates
the process of angiogenesis in RCC, is a well-documented
substrate of ERK in several different cell types.41,42 The
cooperativity of HIF-1a and pERK-1/2 may explain the
high vascular nature of RCC tumors per se and hence the
correlation between pERK-1/2 and tumor size observed in
our current study. Consistent with this view, a recent study
has shown that the specific pharmacologic inhibition of
ERK is sufficient to suppress the growth and angiogenesis
of RCC tumor human xenografts in mice.37
During the final drafting of our current article, a
report by Lee et al43 was published that examined the
prognostic significance of pERK-1/2 in 328 patients with
RCC, comprising patients with localized and metastatic
clear-cell subtypes. These authors stratified patients into
low and high pERK-1/2 groups, and reported that
although pERK-1/2 expression did not reach any inde-
pendent prognostic significance, high pERK-1/2 expres-
sion as compared with low expression was correlated with
better disease-free survival, but only in patients whose
tumors measured<7 cm in greatest dimension; in tumors
measuring >7 cm, they did not demonstrate any correla-
tion between pERK-1/2 and survival. Increased tumor
size appears to be positively correlated with RCC progres-
sion. In our own study, restricted to localized RCC and
stratifying patients into positive and negative pERK-1/2
groups, we were able to demonstrate that pERK-1/2 was
an independent poor prognostic factor irrespective of tu-
mor size, although we did note a statistically higher inci-
dence of pERK-1/2 in tumors measuring >7 cm. In our
study, papillary tumors represented 13.4% of total RCCs
(22 of 164), which is typical of any given RCC patient
cohort. Analysis of the nonpapillary cohort still demon-
strated that increased pERK-1/2 levels served as a signifi-
cant predictor of disease recurrence in patients with
clinically confined RCC (P ¼ .018). Ethnic differences
between the patient cohort used in our study and that of
Lee et al cannot be dismissed as a basis for contrasting
findings. Ethnicity can provide for different genetic and
epigenetic backgrounds in common tumors that ulti-
mately impact on disease progression and response to
treatment. For example, EGF-R, a key upstream effector
molecule of ERK, demonstrates more frequent mutations
in Asian nonsmall cell lung carcinoma populations.44
Although immunohistochemistry provides opportunity
to determine both the global and cellular distribution of
pERK-1/2 within renal tumors, it does not allow discrimi-
nation between the exact involvement of the individual
activated ERK isotypes (ie, pERK-1 vs pERK-2) in disease
progression. The possibility exists that the mouse mono-
clonal antibody used in the study by Lee et al43 and the
rabbit polyclonal antibody used by ourselves in this cur-
rent study preferentially detect different isoforms of
pERK. Of note, gene ablation studies in mice and in vitro
cell lines have recently shown that ERK-2 predominately
drives Ras-dependent cell proliferation,45-47 whereas
ERK-1 can actually attenuate Ras-dependent tumor for-
mation.47 Using Affymetrix microarray technology,
Huang et al37 recently demonstrated elevated ERK-2 lev-
els in 174 cases of clear cell renal tumors.
Multiple reports have documented the importance
of microvascular tumor invasion as a robust and accurate
determinant of disease progression in RCC. Indeed, in
patients with low-grade and localized disease, vascular
invasion has been shown to be the most significant inde-
pendent prognosticator of all pathologic parameters
examined. The current study finding that pERK expres-
sion is strongly associated with the presence of vascular
invasion in clinically confined disease is highly relevant
and supports the inclusion of pERK status in staging
schemes and prognostic models for RCC that incorporate
tumor biomarkers alongside conventional parameters.
The clinical correlation between pERK expression and
invasion can be reconciled at the molecular level through
activated ERK induction of extracellular matrix-digesting
enzymes, facilitating cell migration, and invasion into sur-
rounding tissue.48-51 Recently, it has been demonstrated
that the invasive capacity of the human renal cell carci-
noma cell line Caki-2 is substantially increased on
Original Article
3464 Cancer August 1, 2009

sustained activation of ERK-1/2.38 The enhanced ERK-
mediated invasive ability of these cells resulting from up-
regulation of metalloproteinases 2 and 9, a mechanism
attenuated by the combination of small interfering RNA–
mediated down-regulation of ERK-1/2 and chemical in-
hibition of the RAS/RAF/ERK pathway using PD98059.
Furthermore, it has been reported that leptin36 can poten-
tiate the invasiveness of murine renal cancer cells in an
ERK-dependent manner. Collectively, such mechanistic
studies support the view that activated ERK has a direct
involvement in the process of vascular invasion and hence
the promotion of metastatic disease in RCC, a view fur-
ther corroborated by our current clinical findings.
In the current study, multivariate Cox regression
analysis determined that pERK was equivalent to tumor
grade with respect to its ability to predict disease recur-
rence, with calculated hazards scores of 2.96 and 3.01,
respectively. Surprisingly, we failed to demonstrate a cor-
relation or trend between pERK expression and tumor
grade. However, because they are independent of each
other and yet represent highly valid independent prognos-
ticators, both pERK and tumor grade may be viewed as
complementary determinants that could be effectively
used for the improved prediction of metastatic disease in
clinically confined RCC. Prognostic models incorporat-
ing individual biomarkers with standard clinical parame-
ters have been developed for RCC with good effect.52,53
For example, malignancy-associated biomarkers that
include, among others, PTEN, p53, and Ki-67 have been
ranked alongside several conventional RCC staging
schemes such as Fuhrman grade, TNM, and Eastern Co-
operative Oncology Group performance status. The re-
sultant integrated ‘‘clinical/biomarker’’ allows better
prediction of patient survival than either the panel of bio-
markers or clinicopathologic parameters alone.
With the emergence of cancer therapies that specifi-
cally target growth factor signaling pathways, attention
has focused on the immunohistochemical evaluation of
suitable biomarkers that can serve as a basis for patient
selection and also as markers of treatment response. ERK
represents a downstream convergence point for several
disparate growth factor signaling cascades, including
among others EGF-R, platelet-derived growth factor re-
ceptor (PDGF-R), and vascular endothelial growth factor
receptor (VEGF-R).16-18 In our study, we demonstrated
that pERK-1/2 positivity per se is sufficient to signifi-
cantly predict disease progression in RCC without the
need to discern between various degrees of expression and
ascertain its exact subcellular localization. However,
pERK-1/2 may also represent a reliable and robust bio-
marker for the selection of high-risk RCC patients who
may benefit from treatment with novel molecular targeted
therapies, and serve as an appropriate biomarker by which
to measure tumor response to such agents. Indeed, sorafe-
nib and sunitinib, both of which are multitargeted tyro-
sine kinase inhibitors (TKIs) of the PDGF-R and VEGF-
R, are indicated for use in RCC.8,54 Support for this
notion is gained from studies demonstrating that in cancer
patients treated with targeted TKIs, tumor tissue exhib-
ited lower levels of pERK post-treatment. Specifically, sig-
nificant correlations between reduced pERK and disease
stabilization or partial responses were observed after ther-
apy with sorafenib55 and erlotinib56 in patients with met-
astatic carcinomas of the head, neck,55 and colon,56
respectively.
In summary, the results of the current study indicate
that pERK-1/2 is an independent prognostic biomarker
that significantly predicts the onset of metastasis in clini-
cally confined RCC. In addition, we propose that pERK-
1/2 may be used to better select patients with renal cancer
who may benefit from treatment with specific molecular
targeted therapies and/or as a tumor marker to measure
and monitor treatment efficacy when using such agents.
Further validation is required in other patient cohorts.
Conflict of Interest Disclosures
The authors made no disclosures.
References
1. Corgna E, Betti M, Gatta G, Roila F, De Mulder PH.Renal cancer. Crit Rev Oncol Hematol. 2007;64:247-262.
2. Gupta K, Miller JD, Li JZ, Russell MW, Charbonneau C.Epidemiologic and socioeconomic burden of metastaticrenal cell carcinoma (mRCC): a literature review. CancerTreat Rev. 2008;34:193-205.
3. Novick AC. Kidney cancer: past, present, and future. UrolOncol. 2007;25:188-195.
4. Nogueira M, Kim HL. Molecular markers for predictingprognosis of renal cell carcinoma. Urol Oncol. 2008;26:113-124.
5. Figlin RA. Renal cell carcinoma: management of advanceddisease. J Urol. 1999;161:381-386; discussion 386-387.
Prognostic Significance of pERK in RCC/Campbell et al
Cancer August 1, 2009 3465

6. Chowdhury S, Larkin JM, Gore ME. Recent advances inthe treatment of renal cell carcinoma and the role of tar-geted therapies. Eur J Cancer. 2008;44:2152-2161.
7. Hutson TE, Figlin RA. Evolving role of novel targetedagents in renal cell carcinoma. Oncology (Williston Park).2007;21:1175-1180; discussion 1184, 1187, 1190.
8. Longo R, D’Andrea MR, Sarmiento R, Salerno F,Gasparini G. Integrated therapy of kidney cancer. AnnOncol. 2007;18(suppl 6):vi141-vi148.
9. Unnithan J, Rini BI. The role of targeted therapy in meta-static renal cell carcinoma. Sci World J. 2007;7:800-807.
10. Hudes G, Carducci M, Tomczak P, et al. Temsirolimus,interferon alfa, or both for advanced renal-cell carcinoma.N Engl J Med. 2007;356:2271-2281.
11. Schrader AJ, Olbert PJ, Hegele A, Varga Z, Hofmann R.Metastatic non-clear cell renal cell carcinoma: current thera-peutic options. BJU Int. 2008;101:1343-1345.
12. Haas NB, Uzzo RG. Targeted therapies for kidney cancerin urologic practice. Urol Oncol. 2007;25:420-432.
13. Park WH, Eisen T. Prognostic factors in renal cell cancer.BJU Int. 2007;99(5 pt B):1277-1281.
14. Patel PH, Chaganti RS, Motzer RJ. Targeted therapy formetastatic renal cell carcinoma. Br J Cancer. 2006;94:614-619.
15. Dhillon AS, Hagan S, Rath O, Kolch W. MAP kinase sig-nalling pathways in cancer. Oncogene. 2007;26:3279-3290.
16. Roberts PJ, Der CJ. Targeting the Raf-MEK-ERK mito-gen-activated protein kinase cascade for the treatment ofcancer. Oncogene. 2007;26:3291-3310.
17. Giehl K. Oncogenic Ras in tumour progression and metas-tasis. Biol Chem. 2005;386:193-205.
18. Reddy KB, Nabha SM, Atanaskova N. Role of MAP kinasein tumor progression and invasion. Cancer Metastasis Rev.2003;22:395-403.
19. Arslan MA, Kutuk O, Basaga H. Protein kinases as drug tar-gets in cancer. Curr Cancer Drug Targets. 2006;6:623-634.
20. Faivre S, Djelloul S, Raymond E. New paradigms in anti-cancer therapy: targeting multiple signaling pathways withkinase inhibitors. Semin Oncol. 2006;33:407-420.
21. Milde-Langosch K, Bamberger AM, Rieck G, et al. Expres-sion and prognostic relevance of activated extracellular-regulated kinases (ERK1/2) in breast cancer. Br J Cancer.2005;92:2206-2215.
22. Zhuang L, Lee CS, Scolyer RA, et al. Activation of theextracellular signal regulated kinase (ERK) pathway inhuman melanoma. J Clin Pathol. 2005;58:1163-1169.
23. Osada S, Kanematsu M, Imai H, Goshima S, Sugiyama Y.Evaluation of extracellular signal regulated kinase expressionand its relation to treatment of hepatocellular carcinoma.J Am Coll Surg. 2005;201:405-411.
24. Vicent S, Lopez-Picazo JM, Toledo G, et al. ERK1/2 isactivated in non-small-cell lung cancer and associated withadvanced tumours. Br J Cancer. 2004;90:1047-1052.
25. Mizumoto Y, Kyo S, Mori N, et al. Activation of ERK1/2occurs independently of KRAS or BRAF status in endome-trial cancer and is associated with favorable prognosis.Cancer Sci. 2007;98:652-658.
26. Gee JM, Robertson JF, Ellis IO, Nicholson RI. Phospho-rylation of ERK1/2 mitogen-activated protein kinase isassociated with poor response to anti-hormonal therapy anddecreased patient survival in clinical breast cancer. Int JCancer. 2001;95:247-254.
27. Ebisuya M, Kondoh K, Nishida E. The duration, magni-tude and compartmentalization of ERK MAP kinase activ-ity: mechanisms for providing signaling specificity. J CellSci. 2005;118(pt 14):2997-3002.
28. Campbell L, Jasani B, Edwards K, Gumbleton M, GriffithsDF. Combined expression of caveolin-1 and an activatedAKT/mTOR pathway predicts reduced disease-free survivalin clinically confined renal cell carcinoma. Br J Cancer.2008;98:931-940.
29. Kovacs G, Akhtar M, Beckwith BJ, et al. The Heidelbergclassification of renal cell tumours. J Pathol. 1997;183:131-133.
30. Fuhrman SA, Lasky LC, Limas C. Prognostic significanceof morphologic parameters in renal cell carcinoma. Am JSurg Pathol. 1982;6:655-663.
31. Griffiths DF, Verghese A, Golash A, et al. Contribution ofgrade, vascular invasion and age to outcome in clinicallylocalized renal cell carcinoma. BJU Int. 2002;90:26-31.
32. Thomas DH, Verghese A, Kynaston HG, Griffiths DF.Analysis of the prognostic implications of different tumourmargin types in renal cell carcinoma. Histopathology.2003;43:374-380.
33. Campbell L, Gumbleton M, Griffiths DF. Caveolin-1 over-expression predicts poor disease-free survival of patientswith clinically confined renal cell carcinoma. Br J Cancer.2003;89:1909-1913.
34. Oka H, Chatani Y, Hoshino R, et al. Constitutive activa-
tion of mitogen-activated protein (MAP) kinases in human
renal cell carcinoma. Cancer Res. 1995;55:4182-4187.
35. Carroll VA, Ashcroft M. Regulation of angiogenic factors
by HDM2 in renal cell carcinoma. Cancer Res. 2008;68:
545-552.
36. Horiguchi A, Sumitomo M, Asakuma J, et al. Leptin pro-
motes invasiveness of murine renal cancer cells via extracel-
lular signal-regulated kinases and rho dependent pathway.
J Urol. 2006;176(4 pt 1):1636-1641.
37. Huang D, Ding Y, Luo WM, et al. Inhibition of MAPKkinase signaling pathways suppressed renal cell carci-noma growth and angiogenesis in vivo. Cancer Res. 2008;68:81-88.
38. Inamoto T, Azuma H, Sakamoto T, et al. Invasive abilityof human renal cell carcinoma cell line Caki-2 is acceleratedby gamma-aminobutyric acid, via sustained activation ofERK1/2 inducible matrix metalloproteinases. Cancer Invest.2007;25:574-583.
Original Article
3466 Cancer August 1, 2009

39. Steiner T, Knels R, Schubert J. Prognostic significance oftumour size in patients after tumour nephrectomy for local-ised renal cell carcinoma. Eur Urol. 2004;46:327-330.
40. Lam JS, Klatte T, Patard JJ, et al. Prognostic relevance oftumour size in T3a renal cell carcinoma: a multicentre ex-perience. Eur Urol. 2007;52:155-162.
41. Michiels C, Minet E, Michel G, Mottet D, Piret JP, RaesM. HIF-1 and AP-1 cooperate to increase gene expression inhypoxia: role of MAP kinases. IUBMB Life. 2001;52:49-53.
42. Minet E, Michel G, Mottet D, Raes M, Michiels C. Trans-duction pathways involved in hypoxia-inducible factor-1phosphorylation and activation. Free Radic Biol Med.2001;31:847-855.
43. Lee HJ, Kim DI, Kang GH, Kwak C, Ku JH, Moon KC.Phosphorylation of ERK1/2 and prognosis of clear cell re-nal cell carcinoma. Urology. 2009;73:394-399.
44. Calvo E, Baselga J. Ethnic differences in response to epider-mal growth factor receptor tyrosine kinase inhibitors. J ClinOncol. 2006;24:2158-2163.
45. Fremin C, Ezan F, Boisselier P, et al. ERK2 but not ERK1plays a key role in hepatocyte replication: an RNAi-medi-ated ERK2 knockdown approach in wild-type and ERK1null hepatocytes. Hepatology. 2007;45:1035-1045.
46. Lefloch R, Pouyssegur J, Lenormand P. Single and com-bined silencing of ERK1 and ERK2 reveals their positivecontribution to growth signaling depending on their expres-sion levels. Mol Cell Biol. 2008;28:511-527.
47. Vantaggiato C, Formentini I, Bondanza A, Bonini C,Naldini L, Brambilla R. ERK1 and ERK2 mitogen-acti-vated protein kinases affect Ras-dependent cell signaling dif-ferentially. J Biol. 2006;5:14.
48. O-charoenrat P, Wongkajornsilp A, Rhys-Evans PH, EcclesSA. Signaling pathways required for matrix metalloprotei-
nase-9 induction by betacellulin in head-and-neck squa-mous carcinoma cells. Int J Cancer. 2004;111:174-183.
49. Sroka IC, Nagle RB, Bowden GT. Membrane-type 1 ma-trix metalloproteinase is regulated by sp1 through the dif-ferential activation of AKT, JNK, and ERK pathways inhuman prostate tumor cells. Neoplasia. 2007;9:406-417.
50. Tan X, Egami H, Abe M, Nozawa F, Hirota M, OgawaM. Involvement of MMP-7 in invasion of pancreatic cancercells through activation of the EGFR mediated MEK-ERKsignal transduction pathway. J Clin Pathol. 2005;58:1242-1248.
51. Tanimura S, Asato K, Fujishiro SH, Kohno M. Specificblockade of the ERK pathway inhibits the invasiveness oftumor cells: down-regulation of matrix metalloproteinase-3/-9/-14 and CD44. Biochem Biophys Res Commun.2003;304:801-806.
52. Kim HL, Seligson D, Liu X, et al. Using tumor markers topredict the survival of patients with metastatic renal cellcarcinoma. J Urol. 2005;173:1496-1501.
53. Kim HL, Seligson D, Liu X, et al. Using protein expres-sions to predict survival in clear cell renal carcinoma. ClinCancer Res. 2004;10:5464-5471.
54. Gollob JA, Wilhelm S, Carter C, Kelley SL. Role of Raf ki-
nase in cancer: therapeutic potential of targeting the Raf/
MEK/ERK signal transduction pathway. Semin Oncol.2006;33:392-406.
55. Elser C, Siu LL, Winquist E, et al. Phase II trial of sorafe-
nib in patients with recurrent or metastatic squamous cell
carcinoma of the head and neck or nasopharyngeal carci-
noma. J Clin Oncol. 2007;25:3766-3773.
56. Townsley CA, Major P, Siu LL, et al. Phase II study oferlotinib (OSI-774) in patients with metastatic colorectalcancer. Br J Cancer. 2006;94:1136-1143.
Prognostic Significance of pERK in RCC/Campbell et al
Cancer August 1, 2009 3467