Embed Size (px)
Citation preview

Africa’s Hidden Debt: facing the impact of future treatment costs on countries’ growth
NO 5
Meeting the lifetime costs of treatment for HIV/AIDS would nearly double the debt-to-GDP ratio for some countries in sub-Saharan Africa. Between 2015 and 2050, $110 billion will be needed to simply maintain HIV at current levels, while $293 billion would be needed to extend treatment to all HIV+ people and scale up prevention.
Actions for Policy Makers Identify the gap between resources and liabilities
for HIV/AIDS, and quantify the ‘hidden debt’ at both country level and international level.
Consider efficiencies across health budget and across development budget to minimize future debt.
Consider both international and domestic sources of innovative financing to expand HIV budget.
Convene discussion with donors as to what constitutes long-term equitable co-financing strategy for the epidemic.
Questions for Policy Makers Is the current HIV funding model fit-for-long-term
purpose?
What would more effective, resilient, equitable commitment mechanisms between donors and affected countries look like?
What would be achieved by ‘front-loading’ the costs of the longer-term response to HIV?
What are fair criteria for graduating from IDA for affected countries?
Progress and Complacency Progress and a declining incidence in HIV have led to complacency. Though 15 million people are now receiving ART worldwide, this constitutes only 70% of the target set in 2011 at the United Nations. In sub-Saharan Africa, only half the people who need ART receive it, and prevention interventions are below UNAIDS targets.
Hidden DebtSub-Saharan African countries that have committed to the HIV response and initiated people on ART have assumed future funding obligations which are currently unacknowledged.
In a recent paper, Atun et al (British Medical Journal 2016) estimate the long-term financing liabilities for HIV in sub-Saharan Africa over a period of next 35 years, 2015-2050. (see reference)
These financing needs pose not just a short-term budget challenge, but create long-term financing obligations, akin to sovereign debt.
As ‘hidden debt’, these obligations pose fiscal and debt sustainability challenges for the sub-Saharan countries
that lack domestic financial resources, fiscal flexibility and economic strength.
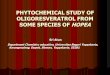
While in 2013 the ratio of debt to GDP was 24% in Kenya and 39% in Uganda, the addition of new funding obligations for HIV would see overall financial liabilities rise to 38% for Kenya, and 59% for Uganda (see figure 1 below).
Figure 1. Current External Debt-to-GDP ratio, HIV Debt-to-GDP ratio, Total Debt-to-GDP ratio (with HIV) for nine sub-Saharan African countires. Source: Atun et al (2016)
POLICY BRIEF # 5
Quantifying the CostsWe estimated future costs of addressing HIV in the nine countries in sub-Saharan Africa with the highest HIV burden: South Africa, Zimbabwe, Zambia, Malawi, Kenya, Uganda, Tanzania, Nigeria and Ethiopia, using the Goals module from Spectrum, a publicly available modelling tool developed by international collaborators.
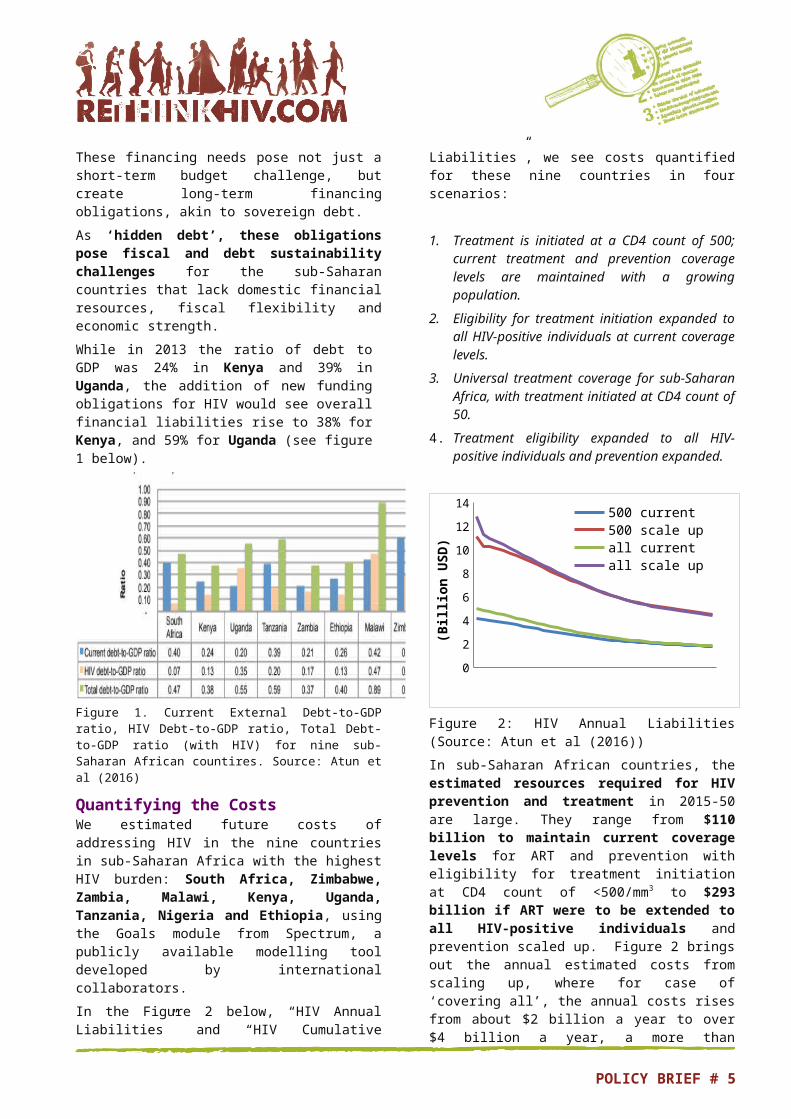
In the Figure 2 below, “HIV Annual Liabilities” and “HIV Cumulative Liabilities”, we see costs quantified for these nine countries in four scenarios:
1. Treatment is initiated at a CD4 count of 500; current treatment and prevention coverage levels are maintained with a growing population.
2. Eligibility for treatment initiation expanded to all HIV-positive individuals at current coverage levels.
3. Universal treatment coverage for sub-Saharan Africa, with treatment initiated at CD4 count of 50.
4. Treatment eligibility expanded to all HIV-positive individuals and prevention expanded.
20152018
20212024
20272030
20332036
20392042
20452048
0
2
4
6
8
10
12
14
500 current 500 scale up
all current all scale up
(Bill
ion
USD)
Figure 2: HIV Annual Liabilities (Source: Atun et al (2016))
In sub Saharan African countries, the ‐ estimated resources required for HIV prevention and treatment in 2015 50 are large. They range from ‐ $110 billion to maintain current coverage levels for ART and prevention with eligibility for treatment initiation at CD4 count of <500/mm3 to $293 billion if ART were to be extended to all HIV-positive individuals and prevention scaled up. Figure 2 brings out the annual estimated costs from scaling up, where for case of ‘covering all’, the annual costs rises from about $2 billion a year to over $4 billion a year, a more than doubling of the annual costs. Clearly, scaling up raises costs quite substantially, and should be weighed against the economic benefits from such an investment.
Pay now, save laterThere is a greater return-on-investment (ROI) by investing in HIV scale-up now to ensure high levels of coverage. This will reduce future expenditure by realising the long term preventive effects of ART‐ to reduce HIV transmission. These long term savings will‐ only be reaped if we invest now. Presently, it is uncertain where large portions of these financing needs will come from.
Traditional Domestic Sources of FundingDomestic financing is the most important source of funding for HIV. In 2014, only four of 48 sub Saharan‐ Africa countries had reached the Abuja target of allocating 15% of government budget to health. Fiscal space considerations mean that in the absence of economic growth or new revenue sources, government budgets will be constrained.
Potential new additional financing from traditional sources includes health insurance and social insurance as sub-Saharan countries move to implement universal health coverage.
Until new funds are available, government revenues need to be appropriately channelled to health and HIV budgets to realise greater impact.
Funding MismatchThere is a mismatch between the long-term funding needs for HIV and the short-term funding cycles of donor countries. The growing funding needs for HIV create ‘contingent liabilities’ for affected countries. Although these contingent liabilities may be ‘off balance sheet’ or ‘off budget’ in official terms, nonetheless they are long term liabilities that must be met.‐The global economic crisis and weak economic growth mean both traditional donors and governments of affected countries are reluctant to precisely quantify and officially accept HIV financing liabilities as long-term debt. Debt sustainability remains a critical issue for affected countries and donors alike.
The Role of International FinanceConcessional finance or debt guarantees from development agencies, such as the World Bank or AfDB should be considered to create more effective and predictable access to funding. HIV-affected countries could use debt guarantees to borrow on more favourable terms for critical investment in health and leverage international financial flows.
New financial instruments which unlock investment funds for affected countries, overseen by an international institution such as the Global Fund would help replace the short replenishment cycles that are at odds with long-term financing needs.
POLICY BRIEF # 5

Innovative Financing Offers Hope but a System Overhaul is RequiredBetween 2002-12, more than $6 billion was raised by international innovative financing instruments.
Innovative financing from social impact bonds, social development bonds, diaspora bonds, micro levy on‐ extractive industries and sovereign bonds securitised against future revenue streams from extractive industries, offer opportunities from international sources. Consumption taxes on alcohol and tobacco that improve health and raise revenue and removal of fossil-fuel subsidies offer possibilities for innovative
financing from domestic sources (see Atun et al, Journal of Global Health, 2016)
All of these options are helpful in expanding the budget envelope, but will have only marginal impact. In order to create a sustainable long-term response a new financing architecture is required. This will involve donors and affected countries thinking the unthinkable.
Action must be taken now to address the challenge of debt-sustainability posed by the HIV ‘hidden debt: an imperative for both affected countries and donors.
References
Atun, R., S. Silva, M. Ncube & A. Vassall (2016), Innovative Financing for HIV responses in Sub-Saharan Africa, Journal of Global health, 691), 010407.
Atun, Rifat., Angela Y Chang, Osondu Ogbuoji, Sachin Silva, Stephen Resch, Jan Hontelez and Till Bärnighausen(2016) Long-term financing needs for HIV control in sub-Saharan Africa in 2015 −2050: modelling study, British Medical Journal, BMJ Open 2016 6:doi: 10.1136/bmjopen-2015-009656
Kabajulizi, J. & Ncube, M. (2015). The economy wide impact of HIV/AIDS and the funding dilemma in Africa: Evidence from a dynamic life cycle horizon of Uganda: Blavatnik School of Government (BSG) Working Papers, BSG-WP-2015/006, University of Oxford.
The paper on which this RethinkHIV Policy Brief is based can be found at www.rethinkhiv.com, and has been published in British Medical Journal Open (2016).
RethinkHIV is a consortium of researchers who evaluate new evidence related to the costs, benefits, effects, fiscal implications and developmental impacts of HIV interventions in sub-Saharan Africa, in order to maximise contributions to the fight against HIV. The aim is to find ways of creating, optimising and sustaining fiscal space for domestic HIV investment, as well as exploring long-term, sustainable national and international financing mechanisms. RethinkHIV is funded by RUSH Foundation.
POLICY BRIEF # 5