Embed Size (px)
Citation preview

HUMAN RESOURCES FOR HEALTHAction Framework for the Western Pacific Region (2011–2015)
WHO Western Pacific RegionPUBLICATION
ISBN-13 978 92 9061 574 3
http://www.wpro.who.int/hrh

27

HUMAN RESOURCES FOR HEALTHAction Framework for the
Western Pacific Region (2011–2015)

ii
WHO Library Cataloguing in Publication Data
Human resources for health: Action framework for the Western Pacific Region (2011–2015)
1. Delivery of health care–manpower. 2. Health manpower. 3. Health resources. 4. Health policy. I. World Health Organization Regional Office for the Western Pacific.
ISBN 978 92 9061 574 3 (NLM Classification: WB 55 )
© World Health Organization 2012
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). For WHO Western Pacific Regional Publications, request for permission to reproduce should be addressed to the Publications Office, World Health Organization, Regional Office for the Western Pacific, P.O. Box 2932, 1000, Manila, Philippines, (fax: +63 2 521 1036; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.

iiiContents
1. BACKGROUND 11.1 Purpose 1
1.2 Global and regional context 2
1.3 Primary health care, now more than ever 3
1.4 Regional progress in strengthening human resources for health (HRH) 4
2. CRITICAL GAPS AND CHALLENGES 62.1 Cross-sectoral planning and policy alignment 6
2.2 Health sector financing and governance 6
2.3 HRH databases, information management systems and strategic plans 7
2.4 Workforce shortages and maldistribution 7
2.5 Implementation of HRH plans 8
2.6 Education and training 8
2.7 Informal health workers 9
2.8 Research, analysis, monitoring and evaluation 10
3. HUMAN RESOURCES FOR HEALTH ACTION FRAMEWORK (2011–2015) 113.1 HRH Vision 2020 11
3.2 HRH Action Framework 11
3.3 Key result areas, strategic objectives and core indicators 13
3.4 Expected results 17
3.5 Results-based HRH Action Framework 17


11. BACKGROUND
1.1 PURPOSE
Many health systems in the Western Pacific Region remain beset by a health workforce crisis: absolute shortages of qualified health workers; inequitable distribution of workers and inefficient skill mix; training and education poorly matched to patient and population needs; and financial constraints with poor motivation and retention in most lesser-resourced countries.
The Regional Strategy on Human Resources for Health (2006–2015), endorsed in resolution WPR/RC57.R7 by the WHO Regional Committee in 2006, guided the collaborative actions of WHO and Member States in strengthening health workforce responsiveness to population health needs through enhanced health system performance and service quality.
These actions included strengthening of national human resource strategic planning and human resources for health (HRH) information systems; reviews and updating of regulatory systems; initiatives addressing the quality and relevance of health professional education; analyses of policy options for rural and remote retention in selected countries, along with publication of global evidence-based policy recommendations on the same issue; and the formulation and dissemination of subregional and global codes of practice for the international recruitment of health workers.

2Despite this progress, there remains an urgent need for intensified, collaborative and multisectoral HRH actions to improve universal coverage and access to quality health services in order to reduce population health inequities and achieve better health outcomes for all.
1.2 GLOBAL AND REGIONAL CONTExT
Many countries face similar challenges in providing equitable access to quality health services for all and improving health outcomes. A sufficient health workforce, adequately prepared and equitably distributed, is necessary for creating strong health systems. However, developing and maintaining an equitably distributed, competent and effective health workforce is an ongoing struggle for many countries, requiring innovative, collaborative and comprehensive national and international planning and strategic actions.
The Western Pacific Region is making better progress towards the health-related Millennium Development Goals (MDG) than other WHO regions. However, progress is unequally spread within and between countries, with rural and poor populations lagging behind. Progress towards achievement of MDG 4 and 5 targets, reduced child mortality and improved maternal health, requires a multi-dimensional approach to service delivery, incorporating core HRH elements, integrated with information management systems, essential medicines, equipment and technologies, financing, service delivery, leadership and governance.1,2
The Region also grapples with mounting negative effects of climate change, health risks, ongoing natural disasters and other public health emergencies. While globalization is accelerating worldwide transmission of communicable diseases, health disparities are widening, populations including health workers are aging, and the burden of chronic conditions is
1 Western Pacific Regional Strategy for Health Systems Based on the Values of Primary Health Care. Manila, WHO Regional Office for the Western Pacific, 2010.
2 Dawson A. Towards a comprehensive approach to enhancing the performance of health workers in maternal, neonatal and reproductive health at community level: Learning from experiences in the Asia and Pacific regions. Discussion paper 2. Sydney, Human Resources for Health Knowledge Hub, 2010.

3increasing. Estimates suggest that the number of older people in this Region will grow faster than in any other WHO region.3
Four out of every five deaths in the Western Pacific Region are due to the most common noncommunicable diseases (NCD)—cancer, cardiovascular disease, chronic respiratory conditions and diabetes.4 The poorest people have the highest burden of NCD, as they have greater exposure to risk factors and less access to preventive and therapeutic services. Health systems in the Region are developing more integrated and comprehensive models of prevention, risk reduction and care provision that use available resources more efficiently and reduce disease complications.
1.3 PRIMARy HEALTH CARE, NOW MORE THAN EvER
A resolution to strengthen health systems based on the values and principles of primary health care (PHC) was endorsed at the fifty-ninth session of the WHO Regional Committee for the Western Pacific. The resolution (WPR/RC59.R4) urges Member States to develop and implement strategies for health systems strengthening and PHC to achieve improved health outcomes for their people, especially those who are poor or otherwise most vulnerable. The common values of PHC and the right to health underpin the Western Pacific Regional Strategy for Health Systems Based on the Values of Primary Health Care as well as the Regional Health Financing Strategy for the Asia Pacific Region (2010–2015), which aims for universal coverage by quality health services without excessive household financial burden.
The crucial role of HRH in the context of health systems strengthening, primary health care renewal, universal access and equity was the focus of a mid-term review of the Regional Strategy on Human Resources for Health (2006–2015). Technical norms at global and regional levels have also been recently developed to further support countries in addressing the challenges of health workforce strengthening, and implementing the agreed regional resolutions. These norms include global evidence-based guidelines
3 Gender, Health and Ageing. Geneva, World Health Organization, 2003.
4 Seoul Declaration on Noncommunicable Disease Prevention and Control in the Western Pacific Region. Seoul, World Health Organization, 2011.

4on increasing access to health workers in remote and rural areas,5 a global code of practice for the international recruitment of health personnel,6 and a Pacific code for the migration of health workers.7
1.4 REGIONAL PROGRESS IN STRENGTHENING HUMAN RESOURCES FOR HEALTH (HRH)
Three WHO meetings have been organized to review challenges and progress in implementing the Regional Strategy on Human Resources for Health (2006–2015) and to propose an action framework to further guide and scale up implementation.8,9,10 Consultations during these meetings, technical reviews of national progress by key strategic result areas in 2009, and a mid-term review of the strategy in 2011 provided the basis for a fairly comprehensive assessment of the current situation of HRH in the Region and the identification of priority issues. The assessment was also informed by reports from Member States, project documents and numerous other publications.
Recognizing the importance of the health workforce in achieving population health goals and the links these have to broader socioeconomic goals, national governments are stepping up efforts to resolve HRH challenges, as evidenced by the formation of high-level, multisectoral committees or taskforces and the issuance of HRH decrees in many countries.
5 Global policy recommendations: increasing access to health workers in remote and rural areas through improved retention. Geneva, World Health Organization, 2010.
6 WHO Global Code of Practice on the International Recruitment of Health Personnel. Geneva, World Health Organization, 2010 (http://www.who.int/hrh/migration/code/code_en.pdf, accessed 6 June 2011).
7 Pacific Code of Practice for Recruitment of Health Workers and Compendium. Endorsed at the Seventh Meeting of Ministers of Health for Pacific Island Countries, Port Vila, Vanuatu, 12 to 15 March 2007 (http://www.wpro.who.int/NR/rdonlyres/6B618EAA-B30B-4CFA-8038-A9F145174895/0/Pacificcodeofpractice.pdf, accessed 6 June 2011).
8 Meeting on the Regional Strategy and Initiatives on Human Resources for Health, Manila, WHO Regional Office for the Western Pacific, 24–26 August 2009.
9 Meeting on Nursing Education and Human Resources for Health, Nadi, Fiji, WHO Regional Office for the Western Pacific, 7–11 February 2011.
10 Meeting on an Action Framework fro the Regional Strategy on Human Resources for Health, Manila, WHO Regional Office for the Western Pacific, 4–6 April 2011.

5Across the Region, countries have been responding to the HRH challenges by strengthening health workforce strategic planning and human resource management systems. Actions taken include improvements in the collection and sharing of population and health data; better links between workforce planning and health service and educational sector planning; steps to reorient health services towards primary health care, health promotion and integrated care provision across the continuum of care; and the testing of strategies to reduce access barriers for disadvantaged groups.
Countries have intensified efforts to improve human resources production and development. Examples include increased participation of minority groups in the health workforce; and concerted interventions in multiple countries to strengthen the quality and relevance of education and training. Evaluations of such interventions are limited.
Improved HRH management practices have resulted in reviews of skills-mix, roles and functional requirements of health workers, with the aim of improving their motivation and performance. Implementation of evidence-based interventions to increase retention in rural and remote areas, as well as strategies to mitigate effects of migration, have resulted in some improvements to the geographic distribution of health workers.
Governance, leadership and partnerships have been addressed through the introduction, review and/or strengthening of legislative and regulatory frameworks and improved coordination of stakeholders and partners; capacity-building in HRH strategic planning and management; improving the quality and safety of service delivery; and the establishment and sustaining of regional HRH, nursing and midwifery networks.
Despite these efforts, insufficient progress has been made in the delivery of universally accessible quality health services.

6 2. CRITICAL GAPS AND CHALLENGES
Intensified strategic actions are required to address absolute shortages of qualified health workers; unbalanced distribution of workers and inefficient skill mix; training and education poorly matched to patient and population needs; and lack of motivation and retention in most lesser-resourced countries. Increased sustainable financing of HRH is imperative for workforce strengthening and scaling up.
2.1 CROSS-SECTORAL PLANNING AND POLICy ALIGNMENT
Health workforce planning and policy alignment across sectors, including health, education, finance and labour, are currently lacking in many countries. More attention must be spent on facilitating policy dialogue and joint decision-making across sectors with multiple stakeholders, including all relevant ministries, the public–private service delivery sector, professional associations, nongovernmental and faith-based organizations, consumers and communities, and technical and donor partners.
2.2 HEALTH SECTOR FINANCING AND GOvERNANCE
HRH policies, plans and interventions call for strong political commitment and sustained financial investments to support workforce scaling up in areas of greatest need, i.e. employment costs and pre-service education.11 In the Western Pacific Region, little has been done to increase health sector funding even though the consequences of inadequate investment
11 Efficiency and effectiveness of aid flows towards health workforce development: Exploratory study based on four case studies from Ethiopia, the Lao People’s Democratic Republic, Liberia and Mozambique. Geneva, World Health Organization, 2011.

7are widely recognized. As such, many countries are struggling to improve the recruitment, deployment, retention and performance of the health workforce. In countries with chronically under-resourced health facilities, the salaries of health workers are significantly lower than the cost of living and payment is sometimes delayed. Government resource constraints, as well as inadequate investments and inefficient resource mobilization, including insufficient use of fiscal space,12 are factors that make it difficult for countries to achieve universal access to quality health services. Reductions in out-of-pocket payments for health services and improved financial risk protection and safety nets, especially for the poor and vulnerable population segments, are essential in overcoming financial barriers to access to quality services.
2.3 HRH DATABASES, INFORMATION MANAGEMENT SySTEMS AND STRATEGIC PLANS
In most lesser-resourced countries, databases and other data sources, as well as HRH information management systems (IMS), even if they exist, do not provide policy-makers and planners with the necessary minimum data sets (MDS) to enable full workforce analyses by sex, age, location (rural or urban) and ethnicity. Furthermore, governments have not completely or consistently identified health service priorities, or delineated the functions and staffing norms for different facilities or services, further limiting the effectiveness of workforce planning efforts.
2.4 WORKFORCE SHORTAGES AND MALDISTRIBUTION
Workforce shortages and maldistribution of health workers are problems shared throughout the Region, though the seriousness of the problems varies from country to country. Cambodia, the Lao People’s Democratic Republic, Papua New Guinea, Solomon Islands, Samoa, Vanuatu and Viet Nam continue to face acute overall shortages of health workers (doctors, nurses and midwives), with a density of less than
12 Fiscal space is defined as room in the government’s budget that allows it to provide resources for desired purpose without jeopardizing the sustainability of its financial position or the stability of the economy.

82.3 per 1000 population. 13,14 Overall, the Region has insufficient numbers of essential groups of health personnel, including: qualified tutors/faculty for education and training; mental health personnel; community-based nurses and midwives and selected categories of medical specialists; adequately trained health facility and equipment engineers and maintenance personnel; and, in the Pacific islands, local, low-cost prosthetic makers. All countries also have workforce distribution inequities with most health workers found in urban areas, leaving rural areas underserved.
2.5 IMPLEMENTATION OF HRH PLANS
While many countries have HRH plans in place to address workforce issues, it is clear that implementation is not easy. Even when HRH priorities are clearly delineated, there may still be inadequate strategic action planning and budgetary support to adequately address urgent HRH needs. Disconnects still exist between health services and educational and workforce planning, contributing to inefficiencies and misalignment in training, deployment and uptake into the workforce. Limited capacity for human resource management at the national, provincial and facility levels, limited cross-sectoral and multi-stakeholder involvement and other underlying, constraining health system factors all contribute to the difficulties countries have in following through on policy-level commitments, and implementing strategies and plans.
2.6 EDUCATION AND TRAINING
The standards and quality of education and training of health professionals remain below par in many countries, resulting in a health workforce that is ill-prepared to effectively respond to rapidly changing, complex health systems and population health challenges surrounding ageing and the growing burden of noncommunicable diseases. Faculty in lesser-resourced countries typically lack clinical expertise as well as formal preparation in education, teaching and learning. They tend to impart knowledge, interpersonal skills and clinical practices that are outdated and not
13 Human Resources for Health Forum Discussion Papers. Port Moresby, National Department of Health, Papua New Guinea, 2008.
14 Country Health Information Profiles. Manila, WHO Regional Office for the Western Pacific, 2010.

9evidence-based. As such, students do not acquire the necessary clinical reasoning skills for safe practice. Basic entry-to-practice competencies of new graduates are negatively influenced by gaps between classroom learning and mentored clinical learning as well as inadequate clinical supervision and role-modelling. Safe and quality services are continually eroded by shortages of formally prepared educators as well as multiple inadequacies in the promotion of student-centred, experiential learning, problem-solving and critical thinking within the clinical context. Though the production of the health workforce requires scaling up, educational institutions in most lesser-resourced countries are ill-equipped to do so due to human and other resource constraints, without severe compromises in educational quality.
2.7 INFORMAL HEALTH WORKERS
Informal health workers, including community health workers, traditional practitioners and lay caregivers, are playing increasingly important roles in the primary health care systems of most countries to compensate for workforce shortages. The HRH challenges of the formal workforce apply to the informal workforce, to an even greater extent, as many informal health workers do not receive salaries or supervision. Insufficient comparative and analytical data exist regarding their education, deployment, utilization, retention and effectiveness in the Region. While informal health workers have multiple titles and varying types and depth of training, studies and experience have shown that they can play important roles in child survival, maternal health and management of infectious diseases,15,16 as well as health literacy, community empowerment and resilience, all of which contribute to improved health. There is a potential for better primary health care system coverage through the use of adequately trained and supported community or informal health workers, who are deployed to complement the work of health professionals but not to serve as direct substitutes for health professionals.17
15 Haines A. et al. Achieving child survival goals: potential contribution of community health workers. The Lancet, 2007, 369:2121.
16 Lewin S. et al. Lay health workers in primary and community health care for maternal and child health and the management of infectious diseases. Cochrane Database of Systematic Reviews, 2005.
17 Lin V., Ridoutt L. and Hollingsworth B. What incentives are effective in improving the deployment of health workers in primary health care settings in Asia and the Pacific? Manila, WHO Regional Office for the Western Pacific, (pre-publication, May 2011).

102.8 RESEARCH, ANALySIS, MONITORING AND EvALUATION
The growing amount of analysis and research being undertaken throughout the Region will inform policy development and planning, but more is needed to capture the unique characteristics of each country and its health workforce. To date, much of the research has been directed at better understanding the workforce situation, and the underlying causes of particular problems. There has been little investigation of the impact of interventions taken to resolve problems; however, in many countries, not enough time has passed for such impacts to be felt, and resources for monitoring or independent analysis are limited.

113. HUMAN RESOURCES FOR HEALTH ACTION FRAMEWORK (2011–2015)
Countries in the Western Pacific Region are working hard to address the challenges of developing and sustaining a health workforce that is sufficient, competent, responsive and adequately supported to meet population health needs. Although many workforce challenges are common to all countries, their unique health systems and political, socioeconomic and topographical situations necessitate workforce policies and strategic interventions specific to each country context. As countries address these challenges, they are guided by a universal vision.
3.1 HRH vISION 2020
Universal coverage for access to quality health services, particularly for the most vulnerable and excluded groups, with improved patient and community health outcomes, through a balanced distribution and efficient skill mix of a multi-professional, motivated workforce able to prevent and manage a full range of conditions and empower people and communities to manage their own health needs as fully as possible.
3.2 HRH ACTION FRAMEWORK
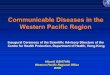
The HRH Action Framework, depicted in Figure 1, was designed to achieve the HRH Vision 2020. The Framework’s six interlinked action fields —human resource management systems, policy, finance, education, partnership and leadership—must all be taken into account in health workforce development and overall health system improvement. The Framework highlights the need for multisectoral and multi-stakeholder

12collaboration and other factors critical for sustainable HRH and health service improvements.18
While the HRH Action Framework is applicable in all countries, the way it is used is influenced by the elements specific to the country context, including the labour market. The outcomes of applying the Framework are also influenced by the strength of other components in the health system (e.g. availability of medical products and equipment, health care financing and health information).
Figure 1: HRH Action Framework for WHO Western Pacific Region
The revised HRH Action Framework (2011–2015) serves as a guide for WHO, governments and partners as they plan and implement concerted actions for health workforce development based on analysis of current and future needs.
18 World Health Report 2006: Working together for health. [Adapted from the Human Resources for Health Technical Framework: achieving a sustainable health workforce, p. 137]. Geneva, World Health Organization, 2006
(http://www.who.int/hrh/tools/en/index.html, accessed 14 May 2011).
Critical Success FactorsResults-focused planning and practicesSystem-linked alignmentKnowledge-based decision-makingLearning-oriented perspectivesInnovative solutionsComprehensive and integrated approaches
BETTERHEALTH
OUTCOMES
ImprovedHealth
WorkforceOutcomes
Critical Success Factors Country-led initiativesGovernment-supported actionsMulti-sector engagementMulti-stakeholder involvementDonor alignmentGender sensitivity
EquityEffectiveness
EfficiencyAccessibility
Responsiveness
BETTERHEALTH
SERVICES
Preparation & Planning
Sit
uatio
n A
naly
sis Im
plem
entation
Monitoring & Evaluation
Service DeliveryHealth Care Financing
Medical Products and Technologies
Health InformationGovernance
Policy
Leadership
Partnership Education
FinanceHumanResourcesfor HealthSystems
Country specific contextincluding labour market

133.3 KEy RESULT AREAS, STRATEGIC OBjECTIvES AND CORE
INDICATORS
The HRH Action Framework was revised to take into account increasing health system complexities, changing health needs and system demands posed by ageing populations and noncommunicable diseases, and the corresponding growing need for scaled-up health workforce education and training to maintain competencies. As such, the revised Framework is comprised of four key result areas, rather than the three identified in the original version,19,20 as well as corresponding strategic objectives and core monitoring and evaluation indicators guiding the implementation of actions.
Key Result Area 1 Strategic Objectives
Health workforce strategic response to evolving and unmet population health and health service needs.
Ensure that health workforce plans and strategies respond to population and service needs, particularly those of the most vulnerable and excluded groups, evolving health worker functions, and technological advances.
Core monitoring and evaluation indicators
• Existenceofafundedhumanresourcesplanaddressingpopulationneedsandpriority HRH areas.
• Numberofhealthworkersoverallper10000populationaswellasnumberofdoctors, nurses and midwives per 10 000 population.
• Distributionofhealthworkersbyruralandurbanlocation(asdefinedbycountryofficial documents).
Strengthening of HRH minimum data sets is required for workforce production and effective deployment. Analysing policy options and implementing more efficient and effective HRH skill mix, aligned with minimum packages of service delivery at all levels are important
19 Regional Strategy on Human Resources for Health (2006–2015). Manila, World Health Organization, 2007.
20 Workforce management is addressed with workforce utilization and retention as it lays the foundation for improved retention. Partnerships have been more fully addressed in key result area 4, in recognition of the need for coordinated, collaborative and sustained action in support of the HRH Vision 2020.

14areas that need to be strengthened to better inform the policy-making process. Reporting on and analysing trends, using agreed-upon sets of core monitoring and evaluation indicators, are essential in monitoring the implementation of plans. Furthering the consistent and systematic dissemination of research findings and application of evidence to policy-formulation and practice is of utmost importance.
Key Result Area 2 Strategic Objectives
Health workforce education, training and continuing competence.21
Develop and continually upskill an inter-professional, flexible, competent workforce able to prevent and manage a full range of conditions and empower people and communities to manage their own health needs as fully as possible.
Core monitoring and evaluation indicators
• Annualnumberofgraduatesofhealthtraininginstitutions,brokendownbycategoryof health professional.
• Percentageofhealthprofessionalgraduatesemployedinthehealthsectorwithin12months after graduation.
• Evidenceofimplementationofnationalorstandardizedinstitutionalcompetencyexamination for each health professional cadre.
• Percentageofgraduatesineachhealthprofessionalcadrepassingthenationalcompetency examination on the first attempt.
Establishing21and applying academic standards, entry-to-practice competencies and faculty development initiatives, with continual strengthening of regulatory frameworks and the operational work of regulatory bodies, are important actions to improve quality education, practice standards and accreditation capacities in Member States. Subsequent to a global analysis of the current state of health professional education, the independent Commission on Education of Health Professionals has called for all health professionals in all countries to “be educated to mobilize knowledge and to engage in critical reasoning and
21 “Continuing competence” is a newer version of the concept of “professional development” that ensures individual as well as collaborative/team learning to enable “all health professionals to engage effectively in a process of lifelong learning aimed squarely at improving patient care and population health.” The Future of Nursing: Leading Change, Advancing Health. Institute of Medicine, 2011.

15ethical conduct so that they are competent to participate in patient and population-centred health systems as members of locally responsive and globally connected teams … to assure universal coverage of the high-quality comprehensive services that are essential to advance opportunity for health equity within and between countries.”22
Key Result Area 3 Strategic Objectives
Health workforce utilization, management and retention.
Maximize functions of the health workforce, staff and skill mix efficiency and management and retention to improve service delivery in terms of equity, universal access, quality and effectiveness.
Core monitoring and evaluation indicators
Management
• Numberofcountrieswithevidenceofformulationorimplementationofprofessionalcompetencies and standards and of quality assurance mechanisms to ensure competence of health professionals.
• Numberofcountrieswithevidenceofaperformanceappraisalsysteminplace.
Skill mix
• Birthsattendedbytrainedhealthpersonnel/totalbirths.
Recruitment and rural/remote retention
• Percentageofvacantpostsannuallyasapercentageofallrecruitsand/ortotalnumber of vacant posts, broken down by geographical location (rural, urban).
• Totalnumberofhealthworkersrecruitedtorural,underservedareasannually.
Migration
• Annualattritionrateofhealthworkersbycadreorpercentageofhealthworkersleaving the health sector.
Improving the management, retention, participation and motivation of the health workforce requires application and testing of innovative interventions including bundled packages of incentives, other effective retention strategies, effective performance management at all levels, and an adequate skill mix, as countries struggle to achieve better health outcomes using their existing workforce.
22 Bhutta Z et. al. Education of health professionals for the 21st century: a global independent commission. The Lancet, 2010, 375:1137–1138.

16 Key Result Area 4 Strategic Objectives
Health workforce governance, leadership and partnerships for sustained HRH contributions to improved population health outcomes.
Strengthen health workforce cross-sectoral planning, policy coherence, regulations and partnerships to ensure the delivery of universally accessible, effective, evidence-based, quality and safe services.
Core monitoring and evaluation indicators
• Numberofcountrieswithevidenceofexisting,activeHRHpartnershipsandnetworks with products/outputs addressing workforce efficiency and effectiveness.
• Evidenceofnationallyenactedpoliciesaddressingtermsandconditionsofwork.
• Evidenceofnationallyenactedpoliciesaddressingquality,includinginfectioncontrol.
• Evidenceofup-to-date,reliablehealthworkforceregistrationdatabases.
Government-wide, multi-stakeholder approaches are required to address the contextual labour market and health systems strengthening issues underlying HRH shortages, particularly those in rural, remote and other underserved areas.
Sustainable workforce investments require prioritized and costed human resource plans addressing resources required; necessary increased investments; analysis of improved fiscal space utilization as well as taking into account the timeline and the predictability of external funding.
Integrated, coordinated donor support is essential to avoid fragmented, donor-driven or other potentially disruptive support that greatly impairs healthy system functioning. Multiple types of donor support could be applied in the following ways: strengthening of the HRH IMS; infrastructure strengthening or rebuilding of educational institutions; faculty development; innovative curricular changes; and ongoing technical support in lieu of financial contributions.
Unless adequate resources are secured, lack of investment will continue to be a major barrier to resolving many of the key HRH challenges, regardless of the appropriateness of other actions taken by governments and development partners.

173.4 ExPECTED RESULTS
Concerted action by WHO and Member States, in close collaboration with stakeholders, partners and donors, can be expected to result in some key achievements, including:
• increasednumbersofcountrieswithstrengthened,costedandimplemented national HRH plans and HRH management capacities;
• improvedHRHinformationsystemsandminimumdatasetssupported by a growing body of regional shared databases;
• scaledupinvestmentsinpre-serviceeducationandcontinuingcompetence;
• regulatoryandpolicyanalysisandupdatesenablingfullfunctionalutilization of all cadres of health workers, including policies and interventions addressing rural and remote recruitment and retention;
• growingbodyofliteratureandresearch,aswellasapplicationofevidence to planning, policy-formulation and practice; and
• improvedandexpandedcross-sectoralpartnershipsanddialogueformore coherent planning, policy-making and more sustainable HRH financing.
3.5 RESULTS-BASED HRH ACTION FRAMEWORK
The strategic actions chosen to address priority HRH challenges in the next five years are clustered within the four key result areas. The actions are further categorized into macro-level structural input, operational or organizational actions, processes or steps, expected outputs, outcomes and impacts. Thus the results-based action framework serves as a stepwise approach to changes and an overall assessment of progress and performance in the four key HRH domains or key result areas, within the context of national health system strengthening.

18
Key
res
ult
area
1: H
ealt
h w
ork
forc
e st
rate
gic
res
po
nse
to e
volv
ing
and
unm
et p
op
ulat
ion
heal
th a
nd h
ealt
h se
rvic
e ne
eds
Str
ateg
ic o
bje
ctiv
e: E
nsur
e th
at h
ealth
wor
kfor
ce p
lans
and
str
ateg
ies
resp
ond
to
pop
ulat
ion
and
ser
vice
nee
ds,
par
ticul
arly
tho
se o
f the
mos
t vu
lner
able
and
exc
lud
ed g
roup
s,
evol
ving
hea
lth w
orke
r fu
nctio
ns, a
nd t
echn
olog
ical
ad
vanc
es.
Mac
ro-l
evel
str
uctu
ral i
nput
O
per
atio
nal p
roce
sses
O
utp
uts
Out
com
es
Imp
act
Info
rmat
ion
man
agem
ent
syst
ems
(IMS
)•
Est
ablis
hed
foca
lpoi
ntfo
rH
RH
IMS
for
dat
a co
llect
ion,
dis
sem
inat
ion
and
ana
lysi
s;•
Info
rmat
ion
syst
ems
for
pol
icy
and
pla
nnin
gin
pla
ce;
•A
ctio
np
lan,
tim
elin
ean
dt
arge
tsin
pla
ce
for
stre
ngth
enin
g H
RS
IMS
;•
Min
imum
HR
Hd
ata
sets
est
ablis
hed
,lin
ked
to
defi
nitio
ns, d
ata
sour
ces;
and
•N
umb
ero
fhea
lthw
orke
rsp
er1
000
0p
opul
atio
n as
wel
l as
num
ber
of d
octo
rs,
nurs
es a
nd m
idw
ives
per
10
000
pop
ulat
ion
for
bot
h th
e p
ublic
and
priv
ate
sect
ors.
Info
rmat
ion
man
agem
ent
syst
ems
(IMS
)•
Est
ablis
hed
mec
hani
sms
for
tran
spar
ency
in in
form
atio
n sh
arin
g;•
Con
tinue
da
ndim
pro
ved
ev
iden
ce-b
ased
dec
isio
n-m
akin
g in
HR
H a
naly
sis
and
rep
ortin
g;•
Incr
ease
dk
now
led
ge,d
ata
acq
uisi
tion
from
the
priv
ate
sect
or
and
the
lab
our
forc
e an
d m
arke
t;
and
•In
crea
sed
acc
essi
bili
tya
nds
harin
gof
wor
kfor
ce d
ata
bas
es a
cros
s d
epar
tmen
ts, l
evel
s an
d s
ecto
rs.
Info
rmat
ion
man
agem
ent
syst
ems
(IMS
)•
Ap
plic
atio
nof
HR
Hin
form
atio
nfo
rd
ecis
ion-
mak
ing
and
pol
icy
form
ulat
ion
at a
ll le
vels
;•
Priv
ate
sect
orw
orkf
orce
dat
ain
tegr
ated
into
nat
iona
l IM
S;
•E
asily
acc
essi
ble
,sha
red
wor
kfor
ce
dat
abas
es u
sed
for
wor
kfor
ce a
naly
ses
and
pla
nnin
g;•
Num
ber
ofn
atio
nald
ata
poi
nts
ont
he
stoc
k an
d d
istr
ibut
ion
of h
ealth
wor
kers
p
rod
uced
with
in p
ast
thre
e ye
ars;
and
•C
urre
ntn
umb
era
ndd
istr
ibut
ion
of
heal
th w
orke
rs.
•In
crea
sed
p
opul
atio
n ac
cess
to
an
adeq
uate
, co
mp
eten
t,
pro
duc
tive
and
sup
por
ted
w
orkf
orce
for
qua
lity
heal
th c
are.
•In
crea
sed
lif
e-ex
pec
tanc
y;•
Incr
ease
de
qui
ty,
resp
onsi
vene
ss o
f hea
lth
serv
ices
;•
Red
uced
mor
talit
yan
d
bur
den
of d
isea
se a
s m
easu
red
by:
- un
der
-5 m
orta
lity;
-
mat
erna
l mor
talit
y
ratio
;-
mor
talit
y b
y ca
use
of
dea
th b
y se
x an
d a
ge-
TBp
reva
lenc
e;•
Red
uctio
nin
ca
use-
spec
ific
mor
talit
y an
d m
orb
idity
.

19
Key
res
ult
area
1: H
ealt
h w
ork
forc
e st
rate
gic
res
po
nse
to e
volv
ing
and
unm
et p
op
ulat
ion
heal
th a
nd h
ealt
h se
rvic
e ne
eds
Str
ateg
ic o
bje
ctiv
e: E
nsur
e th
at h
ealth
wor
kfor
ce p
lans
and
str
ateg
ies
resp
ond
to
pop
ulat
ion
and
ser
vice
nee
ds,
par
ticul
arly
tho
se o
f the
mos
t vu
lner
able
and
exc
lud
ed g
roup
s,
evol
ving
hea
lth w
orke
r fu
nctio
ns, a
nd t
echn
olog
ical
ad
vanc
es.
Mac
ro-l
evel
str
uctu
ral i
nput
O
per
atio
nal p
roce
sses
O
utp
uts
Out
com
es
Imp
act
HR
H s
trat
egic
pla
ns•
HR
Hp
lan
bas
edo
nso
und
situ
atio
nan
alys
is u
sing
wor
kfor
ce p
lann
ing
mod
els
and
too
ls;
•W
orkf
orce
pol
icy
ors
trat
egy
add
ress
ing
pop
ulat
ion
need
s an
d w
orkf
orce
res
pon
se
in t
erm
s of
gen
der
, eq
uity
, vul
nera
bili
ty;
and
•H
RH
pla
nin
tegr
ated
into
nat
iona
lhea
lth
pla
n.
HR
H s
trat
egic
pla
ns•
Form
atio
n,o
per
atio
nan
d
fund
ing
of a
dis
tinct
tea
m o
r un
it re
spon
sib
le fo
r an
alys
is, H
RH
p
lann
ing;
•P
rovi
sion
ofc
ost
estim
ates
an
d in
put
into
ove
rall
HR
H c
ost
estim
ates
by
all l
evel
s of
the
hea
lth
syst
em;
•P
riorit
izat
ion
ofH
RH
pla
n,w
ith
cost
ing
at in
div
idua
l ele
men
t le
vels
in
clus
ive
of: i
mm
edia
te t
rain
ing
cost
s, lo
nger
-ter
m e
mp
loym
ent
cost
s, a
nd b
road
er h
ealth
sys
tem
co
sts;
•P
riorit
ized
HR
Ha
ctio
np
lan
det
aile
d w
ith w
orkf
orce
tar
gets
b
y na
tiona
l min
imum
dat
a se
t ca
tego
ries
and
tim
e fr
ame;
•Fo
rmal
gov
ernm
ent
end
orse
men
t/ap
pro
val o
f HR
H p
lan;
•O
per
atio
nali
mp
lem
enta
tion
oft
he
HR
H p
lan;
and
•R
egul
arr
evie
wa
ndr
evis
ion
of
HR
H p
lan
bas
ed o
n an
ong
oing
ev
alua
tion
and
op
erat
iona
l re
sear
ch.
HR
H s
trat
egic
pla
ns•
Exi
sten
ceo
fafu
nded
,prio
ritiz
edH
RH
p
lan
add
ress
ing
pop
ulat
ion
need
s an
d
iden
tified
prio
rity
HR
H a
reas
: -
Nat
iona
l HR
H p
lan
inte
grat
ed in
to
natio
nal p
olic
ies
and
pla
ns-
Pro
ject
ed H
RH
nee
ds
for
pub
lic a
nd
priv
ate
sect
ors
incl
uded
in H
RH
pla
n;•
Imp
lem
enta
tion
ofn
atio
nalH
RH
p
lan
with
mon
itorin
g an
d e
valu
atio
n m
echa
nism
s an
d d
evel
opm
ent
of
natio
nal e
valu
atio
n p
lan;
pre
par
atio
n of
re
por
ts b
ased
on
eval
uatio
ns.
•In
crea
sed
p
opul
atio
n ac
cess
to
an
adeq
uate
, co
mp
eten
t,
pro
duc
tive
and
sup
por
ted
w
orkf
orce
for
qua
lity
heal
th c
are.
•In
crea
sed
lif
e-ex
pec
tanc
y;•
Incr
ease
de
qui
ty,
resp
onsi
vene
ss o
f hea
lth
serv
ices
;•
Red
uced
mor
talit
yan
d
bur
den
of d
isea
se a
s m
easu
red
by:
- un
der
-5 m
orta
lity;
-
mat
erna
l mor
talit
y
ratio
;-
mor
talit
y b
y ca
use
of
dea
th b
y se
x an
d a
ge-
TBp
reva
lenc
e;•
Red
uctio
nin
ca
use-
spec
ific
mor
talit
y an
d m
orb
idity
.

20
Key
res
ult
area
2: H
ealt
h w
ork
forc
e ed
ucat
ion,
tra
inin
g a
nd c
ont
inui
ng c
om
pet
ence
Str
ateg
ic o
bje
ctiv
e: D
evel
op a
nd c
ontin
ually
up
skill
an
inte
r-p
rofe
ssio
nal,
flexi
ble
, com
pet
ent
wor
kfor
ce a
ble
to
pre
vent
and
man
age
a fu
ll ra
nge
of c
ond
ition
s an
d e
mp
ower
p
eop
le a
nd c
omm
uniti
es t
o m
anag
e th
eir
own
heal
th n
eed
s as
fully
as
pos
sib
le.
Mac
ro-l
evel
str
uctu
ral i
nput
O
per
atio
nal p
roce
sses
O
utp
uts
Out
com
es
Imp
act
Cro
ss-s
ecto
ral p
olic
y-m
akin
g, p
lann
ing
•Fo
rmat
ion
ofh
igh-
leve
lcro
ss-s
ecto
ralw
orki
ng
grou
p o
r st
akeh
old
er c
omm
ittee
tas
ked
with
p
olic
y an
alys
is a
nd p
lann
ing
to e
nsur
e th
at
univ
ersa
lly a
cces
sib
le, q
ualit
y se
rvic
es a
re
del
iver
ed a
nd p
opul
atio
n he
alth
nee
ds
are
met
th
roug
h he
alth
wor
ker
educ
atio
n an
d c
ontin
ued
ca
pac
ity-b
uild
ing;
and
•P
olic
yan
alys
isc
arrie
do
uta
nds
trat
egic
p
lans
dev
elop
ed t
o im
pro
ve p
rimar
y an
d
seco
ndar
y ed
ucat
ion
and
to
ensu
re t
hat
heal
th
pro
fess
iona
l ap
plic
ants
and
stu
den
ts m
eet
entr
y re
qui
rem
ents
and
suc
cess
fully
com
ple
te
pro
gram
mes
.
Cro
ss-s
ecto
ral p
olic
y-m
akin
g,
pla
nnin
g•
Form
ale
ndor
sem
ent/
reco
gniti
ono
fna
tiona
l cro
ss-s
ecto
ral s
take
hold
er
com
mitt
ee;
•E
vid
ence
ofa
ctiv
een
gage
men
tof
rel
evan
t se
ctor
s, c
onsu
mer
s,
com
mun
ities
and
pro
fess
iona
l or
gani
zatio
ns in
dev
elop
ing
and
im
pro
ving
com
pet
ency
-bas
ed h
ealth
p
rofe
ssio
ns e
duc
atio
n; a
nd•
Rev
iew
and
per
iod
icu
pd
atin
gof
en
try-
to-p
ract
ice
com
pet
enci
es,23
p
ract
ice
stan
dar
ds
to m
eet
new
ly
emer
ging
rol
es, a
nd c
hang
ing
pop
ulat
ion
need
s.
Cro
ss-s
ecto
ral p
olic
y-m
akin
g,
pla
nnin
g•
Ava
ilab
led
ata
one
stim
ates
oft
otal
co
st o
f ed
ucat
ion
per
cad
re;
•In
nova
tive
mod
els
ofe
duc
atio
nal
del
iver
y an
d q
ualit
y im
pro
vem
ent
eval
uate
d a
nd r
epor
ted
on,
in
volv
ing:
res
ourc
e sh
arin
g,
clin
ical
ly c
onte
xtua
lized
lear
ning
, in
ter-
pro
fess
iona
l ed
ucat
ion
and
/or
ed
ucat
ion/
pra
ctic
e m
odel
s of
se
rvic
e d
eliv
ery;
•E
vid
ence
ofs
calin
gup
and
ev
alua
tion,
ap
plic
atio
n of
less
ons
lear
nt fr
om e
duc
atio
nal p
rod
uctio
n an
d q
ualit
y in
itiat
ives
;•
Ad
equa
ten
umb
ero
fhea
lth
pro
fess
iona
l ed
ucat
iona
l in
stitu
tions
with
dev
elop
men
t ne
eds
rece
ivin
g te
chni
cal a
nd
finan
cial
sup
por
t fo
r fa
culty
and
p
rogr
amm
e st
reng
then
ing;
and
•In
crea
sed
bud
geta
rya
lloca
tions
an
d fi
nanc
ial s
upp
ort
for
heal
th
pro
fess
ions
ed
ucat
ion
inst
itutio
ns.
•In
crea
sed
p
opul
atio
n ac
cess
to
an
adeq
uate
, co
mp
eten
t,
pro
duc
tive
and
su
pp
orte
d w
orkf
orce
fo
r q
ualit
y he
alth
ca
re.
•In
crea
sed
lif
e-ex
pec
tanc
y;•
Incr
ease
de
qui
tya
nd
resp
onsi
vene
ss o
f he
alth
ser
vice
s;•
Red
uced
mor
talit
yan
d b
urd
en o
f d
isea
se a
s m
easu
red
b
y: -
und
er-5
chi
ld
mor
talit
y;
- m
ater
nal m
orta
lity
r
atio
; -
mor
talit
y b
y m
ajor
cau
se o
f dea
th b
y
sex
and
age
;-
TB
pre
vale
nce;
•R
educ
tion
in
caus
e-sp
ecifi
c m
orta
lity
and
m
orb
idity
.
Hea
lth
Pro
fess
ions
Ed
ucat
ion
•A
cad
emic
acc
red
itatio
nb
ody
and
reg
ulat
ory
syst
ems
esta
blis
hed
to
ensu
re q
ualit
y, q
uant
ity,
rele
vanc
e an
d c
omp
eten
cies
for
wor
k p
ositi
ons;
•E
stab
lishe
dc
ore
com
pet
enci
es23
for
all c
adre
s of
hea
lth p
rofe
ssio
nals
.
Hea
lth
Pro
fess
ions
Ed
ucat
ion
•R
egul
ara
cad
emic
qua
lity
imp
rove
men
tm
eetin
gs; a
ctio
ns t
aken
, eva
luat
ed a
nd
reco
rded
; and
inte
rnal
and
ext
erna
l as
sess
men
ts b
ench
mar
ked
aga
inst
es
tab
lishe
d n
atio
nal a
nd g
lob
al
acad
emic
qua
lity
stan
dar
ds.
Hea
lth
Pro
fess
ions
Ed
ucat
ion
•A
nnua
lnum
ber
ofg
rad
uate
sof
he
alth
tra
inin
g in
stitu
tions
bro
ken
by
cate
gory
of h
ealth
wor
ker;
•N
atio
nalo
rst
and
ard
ized
in
stitu
tiona
l com
pet
ency
ex
amin
atio
n in
pla
ce fo
r ea
ch
heal
th p
rofe
ssio
nal c
adre
.

21
23
“Com
pete
ncie
s” d
o no
t rep
rese
nt ta
sks,
but
rath
er h
ighe
r-le
vel c
ompe
tenc
ies
(app
lied
know
ledg
e; a
ttitu
des;
ski
lls; c
linic
al d
ecis
ion-
mak
ing
proc
esse
s) e
ssen
tial f
or th
e pr
ovis
ion
of s
afe
care
in c
linic
al s
ituat
ions
acr
oss
all c
are
setti
ngs.
Key
res
ult
area
2: H
ealt
h w
ork
forc
e ed
ucat
ion,
tra
inin
g a
nd c
ont
inui
ng c
om
pet
ence
Str
ateg
ic o
bje
ctiv
e: D
evel
op a
nd c
ontin
ually
up
skill
an
inte
r-p
rofe
ssio
nal,
flexi
ble
, com
pet
ent
wor
kfor
ce a
ble
to
pre
vent
and
man
age
a fu
ll ra
nge
of c
ond
ition
s an
d e
mp
ower
p
eop
le a
nd c
omm
uniti
es t
o m
anag
e th
eir
own
heal
th n
eed
s as
fully
as
pos
sib
le.
Mac
ro-l
evel
str
uctu
ral i
nput
O
per
atio
nal p
roce
sses
O
utp
uts
Out
com
es
Imp
act
Hea
lth
Pro
fess
ions
Ed
ucat
ion
•A
cad
emic
qua
lity
stan
dar
ds
and
ind
icat
ors
esta
blis
hed
, ap
ply
ing
inte
rnat
iona
l sta
ndar
ds/
guid
elin
es t
o as
sess
:-
pro
gram
me
grad
uate
s;-
pro
gram
me
dev
elop
men
t an
d r
evis
ion,
in
clud
ing
reso
urce
s;-
pro
gram
me
curr
icul
um;
- ac
adem
ic fa
culty
and
sta
ff;
- p
rogr
amm
e ad
mis
sion
;•
Facu
ltyd
evel
opm
ent
pro
gram
me
esta
blis
hed
fo
r co
ntin
ued
pro
fess
iona
l gro
wth
and
num
ber
of
qua
lified
, ski
lled
ed
ucat
ors
incr
ease
d,
incl
udin
g cl
inic
al e
duc
ator
s/p
rece
pto
rs;
•M
echa
nism
sp
utin
pla
cefo
rm
ento
ring
and
co
achi
ng fa
culty
, sta
ff a
nd s
tud
ents
;•
HR
Ht
rack
ing
ofn
umb
ero
fent
rant
sin
to
heal
th p
rofe
ssio
nal t
rain
ing
pro
gram
mes
(with
na
tiona
lly a
pp
rove
d c
urric
ulum
) with
in la
st t
hree
ye
ars,
with
tre
nd a
naly
sis
and
pol
icy
optio
ns;
and
•N
umb
ero
fstu
den
tsin
med
ical
,nur
sing
and
m
idw
ifery
pre
-ser
vice
ed
ucat
ion
pro
gram
mes
, p
er q
ualifi
ed in
stru
ctor
mon
itore
d, w
ith p
olic
y in
terv
entio
ns t
o en
sure
qua
lity.
Hea
lth
Pro
fess
ions
Ed
ucat
ion
•Im
ple
men
tatio
nof
reg
ular
facu
lty
app
rais
als,
facu
lty d
evel
opm
ent
and
re
por
ting
of p
rogr
ess;
•D
ata
onin
crea
sed
facu
ltyr
eten
tion,
in
crea
sed
num
ber
of e
duc
ator
s, a
nd
imp
rove
d c
omp
eten
cies
;•
Cur
ricul
arc
onte
nt,c
omm
unity
ro
tatio
ns, s
ervi
ce a
rran
gem
ents
and
stud
ent
asse
ssm
ents
refl
ect
cap
acity
d
evel
opm
ent
in r
ural
and
vul
nera
ble
p
opul
atio
n he
alth
;•
Rat
ioo
fsta
ff(f
acul
ty,p
rece
pto
rs)t
ost
uden
t;•
Ann
ualt
rain
ing
bud
get
per
wor
ker;
•A
nnua
lnum
ber
ofd
ays
for
cont
inui
ng
pro
fess
iona
l dev
elop
men
t (C
PD
); an
d•
Per
cent
age
ofs
taff
rec
eivi
ngC
PD
.
Hea
lth
Pro
fess
ions
Ed
ucat
ion
•P
erce
ntag
eof
gra
dua
tes
in
each
cad
re p
assi
ng n
atio
nal
com
pet
ency
exa
min
atio
n on
the
fir
st a
ttem
pt
(dat
a m
onito
red
, re
por
ted
and
eva
luat
ed t
o en
sure
q
ualit
y, s
afe
com
pet
enci
es fo
r p
ract
ice)
.
•In
crea
sed
p
opul
atio
n ac
cess
to
an
adeq
uate
, co
mp
eten
t,
pro
duc
tive
and
su
pp
orte
d w
orkf
orce
fo
r q
ualit
y he
alth
ca
re.
•In
crea
sed
lif
e-ex
pec
tanc
y;•
Incr
ease
de
qui
tya
nd
resp
onsi
vene
ss o
f he
alth
ser
vice
s;•
Red
uced
mor
talit
yan
d b
urd
en o
f d
isea
se a
s m
easu
red
b
y: -
und
er-5
chi
ld
mor
talit
y;
- m
ater
nal m
orta
lity
r
atio
; -
mor
talit
y b
y m
ajor
cau
se o
f dea
th b
y
sex
and
age
;-
TB
pre
vale
nce;
and
•R
educ
tion
in
caus
e-sp
ecifi
c m
orta
lity
and
m
orb
idity
.
Co
ntin
uing
co
mp
eten
ce
•E
stab
lishm
ent
ofin
tegr
ated
coo
rdin
ated
p
rogr
amm
e fo
r co
ntin
uing
com
pet
ence
and
lif
elon
g le
arni
ng o
f all
heal
th p
rofe
ssio
nals
.
Co
ntin
uing
co
mp
eten
ce•
Sca
ling
upin
tegr
ated
,com
pet
ency
-b
ased
con
tinue
d le
arni
ng p
rogr
amm
es
for
ind
ivid
uals
and
tea
ms.
Co
ntin
uing
co
mp
eten
ce•
Pol
icie
san
dp
roce
sses
inp
lace
th
at s
upp
ort
the
cont
inui
ng
com
pet
ence
of i
ndiv
idua
ls a
nd
team
s, w
ith a
ccom
pan
ying
ev
alua
tion
dat
a.

22
24
Ski
ll m
ix u
sual
ly r
efer
s to
the
mix
of p
osts
, gra
des
or o
ccup
atio
ns in
an
orga
niza
tion.
It m
ay a
lso
refe
r to
the
com
bina
tion
of a
ctiv
ities
or
skill
s ne
eded
for
each
job
in t
he o
rgan
izat
ion.
In
: Buc
han
J. a
nd D
al P
oz M
. Ski
ll m
ix in
the
heal
th c
are
wor
kfor
ce: r
evie
win
g th
e ev
iden
ce. B
ulle
tin o
f the
Wor
ld H
ealth
Org
aniz
atio
n, 2
002,
80:
575–
580.
Key
res
ult
area
3: H
ealt
h w
ork
forc
e ut
iliza
tio
n, m
anag
emen
t an
d r
eten
tio
n
Str
ateg
ic o
bje
ctiv
e: M
axim
ize
heal
th w
orkf
orce
util
izat
ion,
man
agem
ent,
ski
ll m
ix, r
ecru
itmen
t an
d r
eten
tion
to im
pro
ve s
ervi
ce d
eliv
ery
in t
erm
s of
eq
uity
, uni
vers
al a
cces
s,
qua
lity
and
eff
ectiv
enes
s.
Mac
ro-l
evel
str
uctu
ral i
nput
O
per
atio
nal p
roce
sses
O
utp
uts
Out
com
es
Imp
act
Man
agem
ent
•C
omp
rehe
nsiv
e,c
oher
ent
mac
ro-l
evel
hu
man
res
ourc
e m
anag
emen
t (H
RM
) st
rate
gy, p
olic
ies
and
pla
n as
par
t of
the
ov
eral
l nat
iona
l HR
H p
lan,
ad
dre
ssin
g:-
staf
f sup
ply
, rec
ruitm
ent
need
s,
pro
cess
es;
- w
orki
ng c
ond
ition
s, h
ealth
, saf
ety;
- se
ttin
g p
ay le
vels
and
ince
ntiv
e p
acka
ges;
- ha
rmon
izin
g re
latio
ns b
etw
een
staf
f, an
d
team
wor
k/in
ter-
pro
fess
iona
l tea
mw
ork;
- la
bou
r re
latio
ns,
skill
s-re
qui
rem
ents
and
ski
ll m
ix;
- p
erfo
rman
ce m
anag
emen
t—op
timiz
ing
pro
duc
tion
and
qua
lity
of c
are,
su
per
visi
on, p
rofe
ssio
nal c
aree
r d
evel
opm
ent,
job
des
crip
tions
, and
p
erfo
rman
ce a
pp
rais
al; a
nd•
Est
ablis
hed
pol
icie
san
dt
rain
ing
pro
gram
me
for
all s
enio
r st
aff f
or H
RM
sk
ill d
evel
opm
ent
and
up
dat
ing.
Man
agem
ent
•P
artic
ipat
ory
staf
finv
olve
men
tin
p
lann
ing
and
cha
ngin
g H
RM
at
faci
lity
leve
l;•
Str
ong,
act
ive
HR
Ma
ndle
ader
ship
sk
ill d
evel
opm
ent
at a
ll le
vels
su
pp
ortin
g p
rod
uctiv
ity, c
omp
eten
ce,
resp
onsi
vene
ss, t
eam
wor
k an
d
pro
ble
m-s
olvi
ng;
•In
stitu
tiona
lpol
icie
sth
ata
reg
end
er-
spec
ific;
pla
ns a
dd
ress
ing
satis
fact
ory,
fa
vour
able
wor
king
con
diti
ons:
eq
uip
men
t an
d s
upp
lies,
infr
astr
uctu
re,
sup
por
t se
rvic
es, r
egul
atio
ns o
f wor
k,
lines
of a
utho
rity,
dec
isio
n-m
akin
g,
acco
unta
bili
ty, e
thic
al a
nd u
neth
ical
b
ehav
iour
, rec
ogni
tion.
Man
agem
ent
•N
umb
ero
fsen
ior
staf
fat
prim
ary
heal
th c
are
faci
litie
s w
ho r
ecei
ved
in
-ser
vice
man
agem
ent
trai
ning
(with
na
tiona
lly a
pp
rove
d c
urric
ulum
) in
pas
t 12
mon
ths;
and
•P
erce
ntag
eof
hea
lths
ervi
ce
pro
vid
ers
at p
rimar
y he
alth
car
e fa
cilit
ies
who
rec
eive
d p
erso
nal
sup
ervi
sion
a m
inim
um o
f eve
ry s
ix
mon
ths.
•In
crea
sed
p
opul
atio
n ac
cess
to
an
adeq
uate
, co
mp
eten
t,
pro
duc
tive
and
sup
por
ted
w
orkf
orce
for
qua
lity
heal
th c
are.
•In
crea
sed
lif
e-ex
pec
tanc
y;•
Incr
ease
de
qui
tya
nd
resp
onsi
vene
ss o
f he
alth
ser
vice
s
(hea
lth w
orke
r, p
atie
nt,
co
mm
unity
sat
isfa
ctio
n
surv
eys)
;•
Hea
ltho
utco
mes
(urb
an
as c
omp
ared
to
rura
l, im
pov
eris
hed
are
as);
•R
educ
edm
orta
lity
and
b
urd
en o
f dis
ease
as
mea
sure
d b
y: -
und
er-5
chi
ld
mor
talit
y; -
mat
erna
l mor
talit
y
rat
io;
- m
orta
lity
by
maj
or
c
ause
of d
eath
by
s
ex a
nd a
ge;
-T
Bp
reva
lenc
e;a
nd•
Red
uctio
nin
ca
use-
spec
ific
mor
talit
y an
d m
orb
idity
.S
taff
and
ski
ll-m
ix e
ffici
ency
24
•H
RH
ana
lyse
sof
op
tions
for
imp
rove
d
effic
ienc
y an
d e
ffec
tiven
ess,
with
in lo
cal
cont
ext
of p
opul
atio
n ne
eds,
alte
rnat
ive
mod
els
of s
ervi
ce p
rovi
sion
, evo
lvin
g sk
ills/
com
pet
enci
es a
nd a
ssur
ance
of
qua
lity,
and
saf
ety.
Ski
ll m
ix a
nd e
ffici
ency
•In
stitu
tiona
l/fac
ility
ski
llm
ixa
naly
ses,
ad
just
men
ts o
r ne
w in
trod
uctio
ns w
hich
m
axim
ize
heal
th b
enefi
ts, o
utco
mes
w
hile
mai
ntai
ning
or
red
ucin
g co
sts.
Sta
ff a
nd s
kill-
mix
effi
cien
cy
•A
naly
sis,
eva
luat
ion
ofin
terv
entio
ns
mat
chin
g st
aff s
kill,
com
pet
ency
mix
to
car
e ne
eds
of s
pec
ific
pop
ulat
ions
.

23
Key
res
ult
area
3: H
ealt
h w
ork
forc
e ut
iliza
tio
n, m
anag
emen
t an
d r
eten
tio
n
Str
ateg
ic o
bje
ctiv
e: M
axim
ize
heal
th w
orkf
orce
util
izat
ion,
man
agem
ent,
ski
ll m
ix, r
ecru
itmen
t an
d r
eten
tion
to im
pro
ve s
ervi
ce d
eliv
ery
in t
erm
s of
eq
uity
, uni
vers
al a
cces
s,
qua
lity
and
eff
ectiv
enes
s.
Mac
ro-l
evel
str
uctu
ral i
nput
O
per
atio
nal p
roce
sses
O
utp
uts
Out
com
es
Imp
act
Rec
ruit
men
t p
olic
y fr
amew
ork
s ad
dre
ss:
•re
crui
tmen
tof
stu
den
tsfr
omr
ural
,un
der
serv
ed a
reas
; and
•
oblig
ator
yse
rvic
eag
reem
ents
and
/or
othe
r in
cent
ives
for
man
dat
ory
pra
ctic
e ro
tatio
ns in
rur
al o
r un
der
serv
ed a
reas
.
Ret
enti
on
•C
aree
rp
athw
ayfr
amew
orks
inp
lace
lin
ked
to
cont
inue
d c
omp
eten
cy
dev
elop
men
t, p
erfo
rman
ce a
sses
smen
t,
qua
lity
and
fina
ncia
l, no
n-fin
anci
al in
cent
ives
;•
Suc
cess
ion
pla
nnin
gp
olic
ies,
pla
ns
for
lead
ersh
ip d
evel
opm
ent,
mob
ility
, ro
tatio
n; a
nd•
Ret
entio
np
olic
ies
and
pro
gram
mes
ad
dre
ssin
g:
- sa
lary
sta
ndar
ds;
- co
nditi
ons
of s
ervi
ce;
- in
cent
ives
, rew
ard
s lin
ked
to
per
form
ance
; and
- fa
vour
able
wor
k en
viro
nmen
ts a
imed
at
incr
easi
ng s
atis
fact
ion
rete
ntio
n.
Rec
ruit
men
t an
d r
eten
tio
n•
Wor
kloa
da
ndo
ther
stu
die
sim
ple
men
ted
to
add
ress
and
rec
tify
HR
H
imb
alan
ces
bet
wee
n le
vels
of c
are
and
ur
ban
and
rur
al a
reas
;•
Dat
aav
aila
bili
tyo
fdis
trib
utio
nof
hea
lth
wor
kers
(by
occu
pat
ion/
spec
ializ
atio
n,
regi
on, p
lace
of w
ork
and
sex
);•
Pol
icie
san
alys
ed,i
mp
lem
ente
da
nd
eval
uate
d fo
r ob
ligat
ory
com
mun
ity
serv
ice
to r
ural
and
/or
urb
an
und
erse
rved
are
as a
nd p
opul
atio
ns;
•B
und
led
pac
kage
sof
ince
ntiv
est
osu
pp
ort
dep
loym
ent,
rec
ruitm
ent
and
re
tent
ion
bei
ng im
ple
men
ted
and
ev
alua
ted
;•
Num
ber
ofh
ealth
wor
kers
new
ly
recr
uite
d a
t p
rimar
y he
alth
car
e fa
cilit
ies
in t
he p
ast
12 m
onth
s (a
s p
erce
ntag
e of
p
lann
ed r
ecru
itmen
t ta
rget
); •
Num
ber
ofd
ays
ofh
ealth
wor
ker
abse
ntee
ism
rel
ativ
e to
the
tot
al n
umb
er
of s
ched
uled
wor
king
day
s ov
er a
giv
en
per
iod
am
ong
staf
f at
PH
C fa
cilit
ies;
and
•P
erce
nto
fhea
lthw
orke
rsw
ithin
tent
ion
to s
tay
in o
r le
ave
the
rura
l are
as.
Dat
a sh
ow
ing
incr
ease
d m
oti
vati
on
and
inte
ntio
n to
rem
ain
in w
ork
pla
ce•
Job
sat
isfa
ctio
nof
rur
ala
ndu
rban
hea
lth
wor
kers
•P
atie
nts
atis
fact
ion
(and
ana
lysi
sof
rur
al
as c
omp
ared
to
urb
an s
atis
fact
ion)
Rec
ruit
men
t to
rur
al, r
emo
te,
und
erse
rved
are
as a
nd r
eten
tio
n•
Incr
ease
ins
tate
dp
refe
renc
esfo
rw
orki
ng in
rur
al/r
emot
e, u
nder
serv
ed
area
s;
•To
taln
umb
ero
fhea
lthw
orke
rs
recr
uite
d t
o ru
ral,
und
erse
rved
are
as;
•P
rop
ortio
nof
new
gra
dua
tes
ente
ring
into
pra
ctic
e in
rur
al, r
emot
e or
un
der
serv
ed a
reas
; •
Pro
por
tion
ofh
ealth
wor
kers
sta
ying
in
rur
al a
reas
(sta
bili
ty in
dex
or
rete
ntio
n ra
te) i
n p
ast
12 m
onth
s;•
Leng
tho
fser
vice
inr
ural
are
as;a
nd•
Den
sity
ofh
ealth
wor
kers
inr
ural
ar
eas
com
par
ed t
o ur
ban
are
as.
•In
crea
sed
p
opul
atio
n ac
cess
to
an
adeq
uate
, co
mp
eten
t,
pro
duc
tive
and
sup
por
ted
w
orkf
orce
for
qua
lity
heal
th c
are.
•In
crea
sed
lif
e-ex
pec
tanc
y;•
Incr
ease
de
qui
tya
nd
resp
onsi
vene
ss o
f he
alth
ser
vice
s
(hea
lth w
orke
r, p
atie
nt,
co
mm
unity
sat
isfa
ctio
n
surv
eys)
;•
Hea
ltho
utco
mes
(urb
an
as c
omp
ared
to
rura
l, im
pov
eris
hed
are
as);
•R
educ
edm
orta
lity
and
b
urd
en o
f dis
ease
as
mea
sure
d b
y: -
und
er-5
chi
ld
mor
talit
y; -
mat
erna
l mor
talit
y
rat
io;
- m
orta
lity
by
maj
or
c
ause
of d
eath
by
s
ex a
nd a
ge;
-T
Bp
reva
lenc
e;a
nd•
Red
uctio
nin
ca
use-
spec
ific
mor
talit
y an
d m
orb
idity
.

24
Key
res
ult
area
3: H
ealt
h w
ork
forc
e ut
iliza
tio
n, m
anag
emen
t an
d r
eten
tio
n
Str
ateg
ic o
bje
ctiv
e: M
axim
ize
heal
th w
orkf
orce
util
izat
ion,
man
agem
ent,
ski
ll m
ix, r
ecru
itmen
t an
d r
eten
tion
to im
pro
ve s
ervi
ce d
eliv
ery
in t
erm
s of
eq
uity
, uni
vers
al a
cces
s,
qua
lity
and
eff
ectiv
enes
s.
Mac
ro-l
evel
str
uctu
ral i
nput
O
per
atio
nal p
roce
sses
O
utp
uts
Out
com
es
Imp
act
Tra
nsit
ions
, att
riti
ons
and
exi
ts
(mig
rati
on)
HR
H m
inim
um d
ata
sets
con
tain
ess
entia
l d
ata
elem
ents
, in
shar
ed d
atab
ase
•C
oher
ent,
cro
ss-s
ecto
ralH
RH
pol
icie
sad
dre
ssin
g cr
oss-
bor
der
rec
ruitm
ent,
m
igra
tion,
ret
urn
mig
ratio
n.
Tra
nsit
ion,
att
riti
ons
and
exi
ts
(mig
rati
on)
•In
crea
sed
tra
ckin
gan
da
naly
sis
ofa
llel
emen
ts o
f HR
H m
inim
um d
ata
sets
•N
umb
ero
fdoc
tors
,nur
ses
and
m
idw
ives
pro
duc
ed o
r gr
adua
ted
in a
ye
ar•
Num
ber
ofd
octo
rs,n
urse
s,m
idw
ives
im
mig
ratin
g in
tern
atio
nally
in a
yea
r, a
s sh
are
of t
otal
num
ber
in e
ach
wor
kfor
ce
cate
gory
.•
Pro
por
tion
ofn
atio
nally
tra
ined
hea
lth
wor
kers
as
com
par
ed t
o fo
reig
n-tr
aine
d
heal
th w
orke
rs e
nter
ing
the
coun
try
annu
ally
Tra
nsit
ion,
att
riti
ons
and
exi
ts
(mig
rati
on)
•S
tock
san
dfl
ows
ofh
ealth
wor
kers
—d
ata
avai
lab
ility
and
tre
nd a
naly
sis
bas
ed o
n H
RH
min
imum
dat
a se
ts•
Str
engt
hene
dp
olic
yco
here
nce
add
ress
ing
inte
rnat
iona
l rec
ruitm
ent
and
in-c
ount
ry h
ealth
sys
tem
, p
opul
atio
n he
alth
nee
ds
•R
egul
arly
up
dat
eda
nda
vaila
ble
H
RH
MD
S d
ata,
rep
ortin
g on
num
ber
of
hea
lth w
orke
rs t
rain
ed a
bro
ad
ente
ring
coun
try
annu
ally
, rel
ativ
e to
num
ber
of n
atio
nally
tra
ined
gr
adua
tes
•In
crea
sed
p
opul
atio
n ac
cess
to
an
adeq
uate
, co
mp
eten
t,
pro
duc
tive
and
sup
por
ted
w
orkf
orce
for
qua
lity
heal
th c
are.
•In
crea
sed
lif
e-ex
pec
tanc
y;•
Incr
ease
de
qui
tya
nd
resp
onsi
vene
ss o
f he
alth
ser
vice
s
(hea
lth w
orke
r, p
atie
nt,
co
mm
unity
sat
isfa
ctio
n
surv
eys)
;•
Hea
ltho
utco
mes
(urb
an
as c
omp
ared
to
rura
l, im
pov
eris
hed
are
as);
•R
educ
edm
orta
lity
and
b
urd
en o
f dis
ease
as
mea
sure
d b
y: -
und
er-5
chi
ld
mor
talit
y; -
mat
erna
l mor
talit
y
rat
io;
- m
orta
lity
by
maj
or
c
ause
of d
eath
by
s
ex a
nd a
ge;
-T
Bp
reva
lenc
e;a
nd•
Red
uctio
nin
ca
use-
spec
ific
mor
talit
y an
d m
orb
idity
.

25
Key
res
ult
area
4: H
ealt
h w
ork
forc
e, g
ove
rnan
ce, l
ead
ersh
ip a
nd p
artn
ersh
ips
for
sust
aine
d H
RH
co
ntri
but
ions
to
imp
rove
d p
op
ulat
ion
heal
th o
utco
mes
Str
ateg
ic o
bje
ctiv
e: S
tren
gthe
n he
alth
wor
kfor
ce c
ross
-sec
tora
l pla
nnin
g, p
olic
y co
here
nce,
reg
ulat
ions
and
par
tner
ship
s to
ens
ure
the
del
iver
y of
uni
vers
ally
acc
essi
ble
, ef
fect
ive,
evi
den
ce-b
ased
, qua
lity
and
saf
e se
rvic
es.
Mac
ro-l
evel
str
uctu
ral i
nput
sO
per
atio
nal p
roce
sses
Out
put
sO
utco
mes
Imp
act
Go
vern
ance
•E
xist
ence
ofa
cro
ss-s
ecto
raln
atio
nal
coor
din
atio
n b
ody
(incl
udin
g he
alth
, p
lann
ing,
ed
ucat
ion,
fina
nce,
lab
our,
p
ublic
or
civi
l ser
vice
com
mis
sion
) or
form
al m
echa
nism
s fo
r H
RH
str
ateg
ic
pla
nnin
g, in
clud
ing
app
licat
ion
of
lab
our
mar
ket
dat
a, s
take
hold
er
coor
din
atio
n, a
nd H
RH
sus
tain
ed
inve
stm
ents
;•
Coh
eren
tcr
oss-
sect
oral
HR
Hp
olic
ies
dev
elop
ed a
nd im
ple
men
ted
for
pro
duc
tion,
dis
trib
utio
n, u
tiliz
atio
n an
d is
sues
sur
roun
din
g m
igra
tion;
•O
ngoi
nge
valu
atio
nof
pol
icie
san
d o
utco
mes
to
ensu
re H
RH
re
spon
sive
ness
to
evol
ving
pop
ulat
ion
heal
th n
eed
s w
ithin
PH
C c
onte
xt a
nd
chan
ging
mod
els
of h
ealth
ser
vice
d
eliv
ery;
and
•P
olic
yan
dm
echa
nism
ses
tab
lishe
d
for
don
or a
nd p
artn
er s
upp
ort.
Go
vern
ance
•M
ulti-
stak
ehol
der
invo
lvem
ent
inH
RH
pla
nnin
g,
eval
uatio
n an
d p
olic
y-m
akin
g (in
clud
ing
pub
lic
and
priv
ate
sect
ors,
inte
rnat
iona
l and
nat
iona
l N
GO
s, fa
ith-b
ased
org
aniz
atio
ns, c
ivil
soci
ety,
p
rofe
ssio
nal a
ssoc
iatio
ns, m
ultin
atio
nal a
nd
bila
tera
l dev
elop
men
t p
artn
ers,
glo
bal
hea
lth
initi
ativ
es);
•In
nova
tive
inte
rven
tion
mod
els
eval
uate
da
nd
rep
orte
d o
n; p
olic
y b
riefs
issu
ed o
n H
RH
prio
rity
issu
es/n
eed
s;•
Don
ors
foru
mc
ond
ucte
dfo
ral
ignm
ent
and
ha
rmon
ized
act
iviti
es; a
nd•
Mec
hani
sms
toe
nsur
ece
rtai
nle
velo
floc
al
auto
nom
y ov
er H
RH
fina
ncia
l, m
ater
ial,
hum
an
reso
urce
s fo
r lo
cally
dev
elop
ed s
trat
egie
s,
mat
chin
g he
alth
wor
ker
need
s an
d e
ssen
tials
p
acka
ges
of c
are
del
iver
y at
all
leve
ls.
Go
vern
ance
•H
RH
pla
nd
evel
oped
and
ev
alua
ted
with
par
ticip
atio
n of
var
ious
sta
keho
lder
s an
d
sect
ors;
•H
RH
pol
icy
inte
grat
ion
into
oth
er
sect
or p
olic
ies
and
pro
gram
mes
;•
Com
mitm
ent
ofn
atio
nal
gove
rnm
ent
and
inte
rnat
iona
l co
mm
unity
to
HR
H p
lan
imp
lem
enta
tion
and
su
stai
nab
ility
:-
cost
ed H
RH
pla
n;-
com
mitm
ent
to a
pp
rop
riate
or
incr
ease
d a
lloca
tion
from
na
tiona
l sou
rces
;-
rece
ipt
of d
onor
fund
ing;
and
- d
ata
avai
lab
ility
: HR
H
exp
end
iture
s as
% o
f pub
lic
exp
end
iture
s an
d G
DP
.
•In
crea
sed
p
opul
atio
n ac
cess
to
an
adeq
uate
, co
mp
eten
t,
pro
duc
tive
and
sup
por
ted
w
orkf
orce
for
qua
lity
heal
th c
are.
•In
crea
sed
lif
e-ex
pec
tanc
y•
Incr
ease
de
qui
ty,
resp
onsi
vene
ss o
f hea
lth
serv
ices
•R
educ
edm
orta
lity
and
b
urd
en o
f dis
ease
as
mea
sure
d b
y:
- u
nder
-5 c
hild
mor
talit
y
- m
ater
nal m
orta
lity
rat
io
- m
orta
lity
by
maj
or
cau
se o
f dea
th b
y
s
ex a
nd a
ge
-T
Bp
reva
lenc
e•
Red
uctio
nin
ca
use-
spec
ific
mor
talit
y an
d m
orb
idity
Lead
ersh
ip a
nd
par
tner
ship
s •
Lead
ersh
ipc
apac
ity-b
uild
ing
pol
icie
san
d s
truc
ture
s in
pla
ce; a
nd•
Est
ablis
hmen
tof
net
wor
ksa
nd
par
tner
ship
s of
rel
evan
t co
mm
itted
le
ader
s an
d s
take
hold
ers.
Lead
ersh
ip a
nd p
artn
ersh
ips
•M
echa
nism
sfo
rca
pac
ity-b
uild
ing
and
up
grad
ing
in p
lace
at
all l
evel
s;•
Str
engt
hene
dc
apac
ities
in:
- d
ata
liter
acy,
ana
lysi
s, r
epor
ting
skill
s;-
anal
ysis
, gen
erat
ion
and
ap
plic
atio
n of
ev
iden
ce a
nd r
esea
rch;
- us
e of
too
ls a
nd t
echn
ique
s fo
r H
RH
sys
tem
;
Lead
ersh
ip a
nd p
artn
ersh
ips
•O
per
atio
nalr
esea
rch
and
ev
alua
tion
stud
ies
imp
lem
ente
d
and
rep
orte
d o
n•
Evi
den
cea
ndr
esea
rch
app
lied
to
cha
nges
in H
RH
pol
icie
s,
pra
ctic
es, s
ervi
ce d
eliv
ery
mod
els,
ski
ll, s
taff
mix
, etc
.•
Pol
icy
reco
mm
end
atio
ns
adap
ted
and
imp
lem
ente
d b
y go
vern
men
t

26
Key
res
ult
area
4: H
ealt
h w
ork
forc
e, g
ove
rnan
ce, l
ead
ersh
ip a
nd p
artn
ersh
ips
for
sust
aine
d H
RH
co
ntri
but
ions
to
imp
rove
d p
op
ulat
ion
heal
th o
utco
mes
Str
ateg
ic o
bje
ctiv
e: S
tren
gthe
n he
alth
wor
kfor
ce c
ross
-sec
tora
l pla
nnin
g, p
olic
y co
here
nce,
reg
ulat
ions
and
par
tner
ship
s to
ens
ure
the
del
iver
y of
uni
vers
ally
acc
essi
ble
, ef
fect
ive,
evi
den
ce-b
ased
, qua
lity
and
saf
e se
rvic
es.
Mac
ro-l
evel
str
uctu
ral i
nput
sO
per
atio
nal p
roce
sses
Out
put
sO
utco
mes
Imp
act
Lead
ersh
ip a
nd p
artn
ersh
ips
- in
stitu
tiona
l eco
nom
ic, q
ualit
y an
d e
qui
ty
asse
ssm
ents
and
ove
rall
pol
icy
anal
ysis
; and
- ge
nera
tion,
ana
lysi
s, d
isse
min
atio
n an
d
app
licat
ion
of e
vid
ence
;•
Net
wor
ksa
ndp
artn
ersh
ips
have
form
ala
ims,
ob
ject
ives
, op
erat
ing
pro
ced
ures
, wor
kpla
ns,
mon
itorin
g an
d e
valu
atio
n of
wor
k; a
nd•
Net
wor
kex
pan
sion
,str
engt
heni
ng,s
usta
inab
ility
,in
crea
sed
col
lab
orat
ion
and
pro
duc
tivity
.
Lead
ersh
ip a
nd p
artn
ersh
ips
•D
isse
min
atio
nan
dp
ublic
atio
nof
out
put
s an
d t
echn
ical
w
ork
pro
duc
ts r
esul
ting
from
ne
twor
ks a
nd p
artn
ersh
ips
•In
crea
sed
p
opul
atio
n ac
cess
to
an
adeq
uate
, co
mp
eten
t,
pro
duc
tive
and
sup
por
ted
w
orkf
orce
for
qua
lity
heal
th c
are.
•In
crea
sed
lif
e-ex
pec
tanc
y•
Incr
ease
de
qui
ty,
resp
onsi
vene
ss o
f hea
lth
serv
ices
•R
educ
edm
orta
lity
and
b
urd
en o
f dis
ease
as
mea
sure
d b
y:
- u
nder
-5 c
hild
mor
talit
y
- m
ater
nal m
orta
lity
rat
io
- m
orta
lity
by
maj
or
cau
se o
f dea
th b
y
s
ex a
nd a
ge
-T
Bp
reva
lenc
e•
Red
uctio
nin
ca
use-
spec
ific
mor
talit
y an
d m
orb
idity
Reg
ulat
ion
and
saf
ety
•E
xist
ence
ofn
atio
nalp
olic
yfr
amew
ork
for
wor
kfor
ce h
ealth
and
sa
fety
; qua
lity
imp
rove
men
t, in
clud
ing
infe
ctio
n co
ntro
l; sa
fe, i
mp
rove
d
wor
king
con
diti
ons;
•R
egul
ator
yb
odie
ses
tab
lishe
dfo
rre
gula
tion
and
ove
rsig
ht m
echa
nism
s,
with
flex
ibili
ty;
•R
evie
wa
ndu
pd
atin
gof
reg
ulat
ory
fram
ewor
k to
ena
ble
all
cad
res
to
wor
k to
full
func
tiona
l cap
aciti
es w
hile
m
aint
aini
ng s
afet
y of
the
pub
lic; a
nd•
Hea
lthw
orke
rre
gist
ratio
nsy
stem
and
fu
ll d
atab
ase
esta
blis
hed
.
Reg
ulat
ion
and
saf
ety
•P
olic
yen
actm
ent
for
imp
rove
dw
orki
ng
cond
ition
s at
all
leve
ls, i
n al
l fac
ilitie
s; a
nd•
Sys
tem
s,m
onito
ring,
eva
luat
ion
and
ac
coun
tab
ility
mec
hani
sms
for
qua
lity
imp
rove
men
t, h
ealth
and
saf
ety,
imp
rove
d
wor
king
con
diti
ons
at fa
cilit
y le
vel f
or p
ublic
and
p
rivat
e fa
cilit
ies.
Reg
ulat
ion
and
saf
ety
•H
ealth
pro
fess
iona
lreg
istr
atio
nsy
stem
dat
a up
to
dat
e an
d
accu
rate
for
bot
h p
rivat
e an
d
pub
lic s
ecto
rs;
•In
crea
sing
num
ber
ofp
ublic
and
p
rivat
e fa
cilit
ies
with
pol
icie
s,
syst
ems
for
qua
lity
imp
rove
men
t (in
clud
ing
infe
ctio
n co
ntro
l),
heal
th a
nd s
afet
y, a
nd im
pro
ved
w
orki
ng c
ond
ition
s;•
Pub
lica
cces
san
dt
rans
par
ency
in
wor
kfor
ce r
egis
trat
ion,
lic
ensu
re, d
isci
plin
ary
dat
a; a
nd•
Reg
ular
sur
veys
and
rep
ortin
gof
faci
lity
qua
lity
and
saf
ety
dat
a b
ench
mar
ked
with
nat
iona
l, re
gula
tory
and
/or
accr
edita
tion
stan
dar
ds
and
ind
icat
ors.

27

HUMAN RESOURCES FOR HEALTHAction Framework for the Western Pacific Region (2011–2015)
WHO Western Pacific RegionPUBLICATION
ISBN-13 978 92 9061 574 3
http://www.wpro.who.int/hrh