Embed Size (px)
Citation preview

3272019
123
Tintinallirsquos Emergency Medicine A Comprehensive Study Guide 8e
Chapter 233 Chapter 233 Acquired Bleeding DisordersAcquired Bleeding Disorders Robert W Shaer Sally A Santen
INTRODUCTIONINTRODUCTION
Normal regulation of bleeding is a complex process involving platelets and the coagulation system (seechapter 232 Tests of Hemostasis) Platelet defects typically manifest with petechiae and mucosal bleedingwhereas coagulation defects usually present as spontaneous or excessive hemorrhage Management ofsignificant acquired bleeding disorders should be discussed with a hematologist because there are oensubtleties in diagnosis and treatment
ACQUIRED PLATELET DEFECTSACQUIRED PLATELET DEFECTS
Circulating platelets provide the initial defense against bleeding Acquired platelet disorders may bequantitative (decreased number of circulating platelets) or qualitative (poorly functioning platelets) Bothsignificant thrombocytopenia and qualitative platelet dysfunction are commonly manifested by the presenceof nonpalpable petechiae oen most pronounced in the lower extremities and in areas where blood flow isrestricted Other typical findings may include purpura mucosal bleeding (gingival epistaxis) menorrhagiahemoptysis hematuria and hematochezia whereas deep tissue bleeding and hemarthrosis are lesscommon
Securing circulatory stability is the primary treatment priority in the bleeding patient Once this is done thehistory physical examination and directed laboratory testing are used to define the clinical syndromeRecent illness symptoms and medications are potentially relevant in the patient who appears to have aplatelet disorder Physical examination should assess for additional bleeding sites and the type of bleedingAssess for lymphadenopathy splenomegaly pallor or jaundice that suggests diagnoses such as leukemialymphoma systemic lupus erythematosus infectious mononucleosis or hemolytic anemia
THROMBOCYTOPENIATHROMBOCYTOPENIA
Quantitative defects that result in thrombocytopenia are caused by decreased production increased
destruction splenic sequestration platelet loss or a combination (Table 233-1Table 233-1)1 The etiologies ofthrombocytopenia are diverse and the pathologic mechanism is not always initially clear Viral infectionsmay impair thrombopoiesis due to direct infection of the megakaryocyte toxic eects of viral proteins orcytokines hemophagocytosis or production of antibodies that bind to platelets and enhance immuneLoading [Contrib]a11yaccessibility-menujs
3272019
223
Abbreviation HIV = human immunodeficiency virus
destruction2 A drug history is important because many medications have been implicated in causing
thrombocytopenia or impairing platelet function (Table 233-2Table 233-2)34
TABLE 233-1
Pathophysiology of Acquired ThrombocytopeniaPathophysiology of Acquired Thrombocytopenia
MechanismMechanism Associated Clinical ConditionsAssociated Clinical Conditions
Decreased platelet production Marrow infiltration (tumor or infection)
Viral infections (rubella HIV hepatitis C others)
Drugs (Table 233-2)
Radiation
Vitamin B12 andor folate deficiency
Increased platelet destruction Immune thrombocytopenia
Thrombotic thrombocytopenic purpura
Hemolytic-uremic syndrome
Disseminated intravascular coagulation
Viral infections (HIV mumps varicella Epstein-Barr virus)
Drugs (Table 233-2)
Platelet loss Excessive hemorrhage
Hemodialysis extracorporeal circulation
Splenic sequestration Sickle cell disease cirrhosis
Loading [Contrib]a11yaccessibility-menujs
3272019
323
Note 4+ to 1+ indicates relative incidence from more frequent to less frequent based on case reports
TABLE 233-2
Drugs That Produce Thrombocytopenia or Impair Platelet FunctionDrugs That Produce Thrombocytopenia or Impair Platelet Function
Produce ThrombocytopeniaProduce Thrombocytopenia Impair FunctionImpair Function
Heparin 4+ Aspirin
Gold salts 4+ Nonsteroidal anti-inflammatory drugs
Sulfa-containing antibiotics 4+ Glycoprotein IIbndashIIIa agents ticlopidine and clopidogrel
Quinine and quinidine 4+
Ethanol (chronic use) 4+ Penicillins and cephalosporins
Aspirin 3+ Calcium channel blockers
Indomethacin 3+ β-Adrenergic blockers propranolol
Rifampin 2+ Nitroglycerin
Abciximab and eptifibatide 2+ Antihistamines
Thiazides and furosemide 2+ Phenothiazines
Acyclovir 2+ Cyclic antidepressants
Procainamide 2+
Digoxin 2+
Cimetidine and ranitidine 2+
Phenytoin and valproate 1+
Penicillinscephalosporins 1+
A CBC will establish the presence and degree of thrombocytopenia and determine whether otherhematologic cell lines are aected A peripheral smear should be examined to assess platelet morphologyLoading [Contrib]a11yaccessibility-menujs
3272019
423
and evaluate other cell lines Rarely in vitro platelet agglutination occurs which leads to spuriously lowplatelet counts reported by automated cell counters (pseudothrombocytopenia) when collected inethylenediaminetetraacetic acidndashcoated blood tubes this can be detected by the presence of plateletclumping on a peripheral smear In this case a correct platelet count may be obtained by using citrated orheparin-anticoagulated blood tubes
Testing for human immunodeficiency virus and hepatitis C virus is recommended in cases of isolated
thrombocytopenia as low platelets may be the only readily apparent manifestation in early infections5 If theetiology of low platelets remains unclear further laboratory testing to evaluate for disorders such ashemolysis and disseminated intravascular coagulation (DIC) may be needed Although usually not necessaryin instances of isolated thrombocytopenia bone marrow biopsy may be obtained when malignancy or otherbone marrow pathologies are of concern
When circulating platelet levels decrease to below 10000 to 20000mm3 (10 to 20 times 109L) the risk ofspontaneous bleeding becomes concerning particularly for intracranial hemorrhage Additional risk factorsfor bleeding include age comorbid illness (ie renal disease liver disease connective tissue disease pepticulcer disease hypertension) fall risk and lifestyle activity With the exception of a few specific diseaseprocesses platelet transfusion in the nonbleeding patient should be considered when counts fall below
10000mm3 (10 times109L) or higher if other comorbid illnesses are present6 The cause of the plateletdeficiency may also influence the risk of bleeding At a given platelet level patients with immunethrombocytopenia (ITP) typically bleed less than patients with aplastic anemia as the younger platelets
present in ITP are more eective in hemostasis7
Immune Causes of ThrombocytopeniaImmune Causes of Thrombocytopenia
ITP is an acquired immune-mediated disorder in which circulating platelets typically fall to very low levels38
ITP results from antiplatelet antibodies that attack platelet surface glycoproteins such as glycoproteinIIbIIIa leading to peripheral platelet destruction There is evidence that the same antibodies lead to
impaired platelet production by megakaryocytes9 Despite very low platelet counts the circulating plateletsare not functionally impaired
Immune thrombocytopenia may be classified as primary (formerly known as idiopathic thrombocytopenicpurpura) or secondary when associated with other medical conditions (autoimmune disorders infections) or
drug exposures8 This distinction is of clinical importance as management of the underlying disorder ordiscontinuation of the drug in cases of secondary ITP may lead to normalization of the platelet count
Primary ITP may occur at any age with equal prevalence between genders with the exception of those age30 to 60 years in which women predominate Primary ITP is classified by duration of illness newly diagnosed
(diagnosis to 3 months) persistent (3 months to 12 months) and chronic (gt12 months)8 The majority ofadults with primary ITP progress to chronic illness
Loading [Contrib]a11yaccessibility-menujs
3272019
523
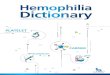
The most common presenting sign of ITP is a petechial rash (Figure 233-1AFigure 233-1A) Mild epistaxis gingival bleeding(Figure 233-1BFigure 233-1B) and menorrhagia in women of childbearing age may also be seen Except for petechiae andbruising the patient should have a normal physical examination
FIGURE 233-1FIGURE 233-1
Two patients with idiopathic thrombocytopenic purpura AA Petechiae with platelet count of 3000mm3 (3 times
109L) BB Gingival bleeding with platelet count of 5000mm3 (5 times 109L) [Image used with permission of JStephan Stapczynski MD]
Loading [Contrib]a11yaccessibility-menujs
3272019
623
The CBC should demonstrate normal cell lines except for the platelets A mild anemia may be seen if bleedingis present The peripheral smear should show large well-granulated platelets although they will be few innumber Bone marrow biopsy is not indicated unless clinical features are atypical If the evaluation supportsthe diagnosis of primary ITP then additional testing in the ED is not required
Treatment for ITP is initiated based on the risk of bleeding (Table 233-3Table 233-3) Major bleeding complications in
patients with platelets gt50000 mm3 (gt50 times 109L) are uncommon As most fatal bleeding complications
occur when platelet counts fall below 30000mm3 (30 times 109L) experts and guidelines recommend this level
as the threshold for initiating treatment of ITP in adults5691011 Bleeding risk correlates with lower plateletcounts and patient age greater than 60 a prior history of bleeding certain chronic illnesses and use ofmedications that alter hemostasis all heighten this risk Therefore certain patients may benefit from medical
treatment despite a platelet count exceeding 30000mm3 (30 times 109L) For all patients with primary ITPbleeding risk should be minimized including avoiding use of antiplatelet medications when possiblemaintenance of good blood pressure control optimized treatment of exacerbating comorbid conditions (ieliver disease renal disease) and addressing fall risks
Loading [Contrib]a11yaccessibility-menujs
3272019
723
TABLE 233-3
Treatment of Immune ThrombocytopeniaTreatment of Immune Thrombocytopenia
Platelet
transfusionlt10000ndash20000mm3 (lt10ndash20 times 109L) prophylactically to prevent bleeding
lt50000mm3 (lt50 times 109L) if actively bleeding
lt20000ndash50000mm3 (lt20ndash50 times 109L) if patient requires diagnostic puncture
lt50000ndash100000mm3 (lt50ndash100 times 109L) if patient requires invasive procedure
Corticosteroids Prednisone 1 milligramkg PO per day for 21 days then tapered or dexamethasone 20
milligramsm2 IV per day for 4 d
IV
immunoglobulin
1 gramkg IV per day for 3 d
Splenectomy Considered for refractory cases
About two thirds of children with primary ITP will have spontaneous resolution within 6 months of
diagnosis11 An antecedent viral infection is commonly reported Additionally the measles-mumps-rubellavaccination has been associated with the development of acute ITP although this is rare and occurs in less
than 1 per 25000 doses given12 The risk of severe bleeding complications appears to be rare in children
regardless of their absolute platelet count5813 Children without signs of active bleeding and goodpsychosocial support typically do not require hospitalization or medical treatment Good anticipatoryguidance should be provided to the family and the child should abstain from contact sports or activities thatmight place them at risk for head injury
First-line treatment for primary ITP generally includes corticosteroids typically prednisone 1 milligramkg
per day for 4 weeks (shorter courses may be considered for children)59101113 Initial response may not beseen for 4 to 14 days and peak eect can be expected between 7 and 28 days IV immunoglobulin may alsobe considered either alone or in combination with corticosteroids at a dose 1 gkgper day for 3 days Initialresponse to IV immunoglobulin is more rapid than corticosteroids occurring between 1 and 3 days withpeak eect seen between 2 and 7 days Side eects of IV immunoglobulin may include aseptic meningitistransient neutropenia acute kidney injury and transfusion reactionshypotension
Anti-Rho(D) immunoglobulin at 50 to 75 microgramskg for a single dose may also be considered as a first-
line treatment strategy in patients who are Rh(D) positive and have not undergone splenectomy14 Initialresponse rate and peak eect are similar to that seen with IV immunoglobulin Mild hemolysis can beexpected and rare serious or even fatal cases of intravascular hemolysis DIC and renal failure have beenreported with anti-Rho(D) use prompting the US Food and Drug Administration to administer a warningLoading [Contrib]a11yaccessibility-menujs
3272019
823
pertaining to its use in 2010 Second-line treatment modalities include splenectomy and use of neweragents such as the monoclonal antibody rituximab which blunts the autoimmune destruction of plateletsand thrombopoietin receptor agonists which stimulate platelet production (ie romiplostin eltrombopag)
In the event of life-threatening hemorrhage where hemostasis must be achieved rapidly IV corticosteroids
(such as dexamethasone) and IV immunoglobulin should be administered concomitantly13 Platelettransfusions should be initiated and doses two to three times the typical dose might be required due to
persistent autoimmune destruction6 Platelet transfusions may need to be repeated frequently until bleedingsubsides or targeted treatment modalities take eect Emergent splenectomy may be considered if all othertreatment options are exhausted
Drug-Induced Immune ThrombocytopeniaDrug-Induced Immune Thrombocytopenia
Over 200 drugs have been implicated in causing immune-mediated suppression of platelet production or
increased platelet destruction (Table 233-2)34 The clinical presentation is similar to ITP and thethrombocytopenia may severe Drug-induced thrombocytopenia typically occurs 5 to 14 days followinginitiation of a drug but may occur sooner if there has been recent prior exposure A careful history should notonly include prescribed medications but also herbal remedies and food and beverage use (ie quinine intonic water alcohol use tahini) Chronic alcohol use is a common cause of thrombocytopenia Plateletcounts typically normalize with cessation of the causative agent Heparin-induced thrombocytopenia causesa significant drop in platelets but patients are paradoxically hypercoagulable due to platelet activation (seechapter 239 Thrombotics and Antithrombotics)
Nonimmune Causes of ThrombocytopeniaNonimmune Causes of Thrombocytopenia
Thrombocytopenia may occur from various nonndashimmune-mediated causes (Table 233-1) In thromboticthrombocytopenic purpura and hemolytic-uremic syndrome thrombotic microangiopathy occurs whenvessel injury results in deposition of platelet-fibrin thrombi (see chapters 143 Oncologic and HematologicEmergencies in Children and 237 Acquired Hemolytic Anemia) DIC is also a well-described cause ofplatelet destruction In patients with marked hemorrhage large-volume fluid resuscitation may lead to adilutional thrombocytopenia Additionally certain bacterial rickettsial and viral infections can cause directtoxic destruction of platelets Thrombocytopenia specific to pregnancy may be a result of the hemolysisndashelevated liver enzymesndashlow platelets (HELLP) syndrome pre-eclampsia or gestational thrombocytopenia(see chapter 100 Maternal Emergencies aer 20 Weeks of Pregnancy and in the Postpartum Period)Finally an enlarged spleen can sequester a significant portion of the platelet pool
Thrombocytopenia is present in up to 70 of patients with chronic liver disease15 The etiology appearsmultifactorial Patients oen have underlying medical conditions related to their liver disease such as alcoholuse viral hepatitis or nutritional deficiencies that impair platelet production Thrombopoietin which isproduced by hepatocytes may be decreased Portal hypertension may lead to splenic sequestrationEndotoxemia from infection may promote platelet aggregation Some patients also demonstrate plateletLoading [Contrib]a11yaccessibility-menujs
3272019
923
autoantibodies The degree of quantitative thrombocytopenia may be mitigated by an increased level ofcirculating von Willebrand factor that is typically seen which promotes platelet adhesion For this reasonroutine platelet transfusion is not recommended in the absence of clinically significant bleeding However a
platelet count of gt50000mm3 (gt50 times 109L) should be achieved prior to invasive procedures (ie lumbar
puncture surgery liver biopsy)16
FUNCTIONAL PLATELET DISORDERSFUNCTIONAL PLATELET DISORDERS
Several disease processes can cause acquired qualitative or functional abnormalities of platelets (Table 233-Table 233-
44)17 In the myeloproliferative diseases platelets are oen dysfunctional even if the platelet count is normalor elevated Patients can have prolonged bleeding times and clinically significant bleeding To control acute
bleeding transfusion should be considered to raise the level of normal platelets to 50000mm3 (50 times 109L)In macroglobulinemia and related disorders the elevated level of viscous proteins interferes with plateletfunction Patients with clinically significant bleeding may require plasmapheresis to reduce the protein leveland correct hemostatic function
TABLE 233-4
Clinical Conditions Associated with Qualitative Platelet AbnormalitiesClinical Conditions Associated with Qualitative Platelet Abnormalities
Uremia
Liver disease
Disseminated intravascular coagulation
Antiplatelet antibodies (immune thrombocytopenia systemic lupus erythematosus)
Cardiopulmonary bypass
Myeloproliferative disorders (thrombocytosis polycythemia vera chronic myeloid leukemia acute
lymphocytic or myelogenous leukemia)
Dysproteinemias (multiple myeloma Waldenstroumlms macroglobulinemia)
von Willebrands disease (congenital or acquired)
Many drugs can influence platelet function (Table 233-2 and Table 233-5Table 233-5) Of these the most commonly usedare aspirin which produces an irreversible impairment in platelet aggregation and the nonsteroidal anti-inflammatory drugs clopidogrel and ticlopidine which produce temporary impairment in platelet adhesionand aggregation (see chapter 239)
Loading [Contrib]a11yaccessibility-menujs
3272019
1023
TABLE 233-5
Duration of Antiplatelet ActivityDuration of Antiplatelet Activity
DrugDrug OnsetOnset Duration of EectDuration of Eect
Aspirin 1 h Up to 7 d
Most nonsteroidal anti-inflammatory drugs 1 h 1 d
Piroxicam 1 h 2 d
Ticlopidine or clopidogrel 1ndash2 d 4ndash7 d
Thrombocytosis a platelet count exceeding 500000mm3 (500 times 109L) can be seen in many disordersincluding inflammatory reactions malignancy polycythemia and postsplenectomy Platelet function can benormal or abnormal depending on the underlying condition Therefore thrombocytosis can be associatedwith bleeding (mucosal ecchymotic GI) or thromboembolic (deep venous thrombosis portal or mesentericthrombosis splenic vein thrombosis) manifestations However these events are unusual even with platelet
counts in excess of 1000000mm3 (1000 times 109L)
ACQUIRED COAGULATION DISORDERSACQUIRED COAGULATION DISORDERS
Acquired coagulation disorders can result from underlying medical disease and autoimmune factorinhibitors
LIVER DISEASELIVER DISEASE
Acute and chronic liver disease is commonly associated with laboratory tests of impaired coagulationHepatocytes synthesize all of the coagulation factors and related regulatory proteins with the exception offactor VIII and von Willebrand factor Diseases aecting the hepatic parenchyma may result in a decreasedsynthesis of these factors including the vitamin Kndashdependent carboxylation of factors II (prothrombin) VIIIX and X Because vitamin K is a fat-soluble vitamin malabsorption can occur with processes that interferewith the absorption of fat-soluble vitamins including impaired bile acid metabolism (ie primary biliarycirrhosis) intrahepatic or extrahepatic cholestasis and treatment with bile acid binders Thus prolongedprothrombin time is common in patients with decompensated hepatic function Despite markedprolongations of prothrombin time and activated partial thromboplastin time (PTT) seen in advanced liverdisease and cirrhosis these tests poorly predict onset and severity of bleeding including bleeding from
esophageal varices or invasive procedures or surgery16181920 Although there may be marked reduction inprocoagulant proteins in liver disease there is typically a parallel decrease in the endogenous anticoagulantLoading [Contrib]a11yaccessibility-menujs
3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
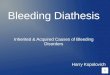
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
223
Abbreviation HIV = human immunodeficiency virus
destruction2 A drug history is important because many medications have been implicated in causing
thrombocytopenia or impairing platelet function (Table 233-2Table 233-2)34
TABLE 233-1
Pathophysiology of Acquired ThrombocytopeniaPathophysiology of Acquired Thrombocytopenia
MechanismMechanism Associated Clinical ConditionsAssociated Clinical Conditions
Decreased platelet production Marrow infiltration (tumor or infection)
Viral infections (rubella HIV hepatitis C others)
Drugs (Table 233-2)
Radiation
Vitamin B12 andor folate deficiency
Increased platelet destruction Immune thrombocytopenia
Thrombotic thrombocytopenic purpura
Hemolytic-uremic syndrome
Disseminated intravascular coagulation
Viral infections (HIV mumps varicella Epstein-Barr virus)
Drugs (Table 233-2)
Platelet loss Excessive hemorrhage
Hemodialysis extracorporeal circulation
Splenic sequestration Sickle cell disease cirrhosis
Loading [Contrib]a11yaccessibility-menujs
3272019
323
Note 4+ to 1+ indicates relative incidence from more frequent to less frequent based on case reports
TABLE 233-2
Drugs That Produce Thrombocytopenia or Impair Platelet FunctionDrugs That Produce Thrombocytopenia or Impair Platelet Function
Produce ThrombocytopeniaProduce Thrombocytopenia Impair FunctionImpair Function
Heparin 4+ Aspirin
Gold salts 4+ Nonsteroidal anti-inflammatory drugs
Sulfa-containing antibiotics 4+ Glycoprotein IIbndashIIIa agents ticlopidine and clopidogrel
Quinine and quinidine 4+
Ethanol (chronic use) 4+ Penicillins and cephalosporins
Aspirin 3+ Calcium channel blockers
Indomethacin 3+ β-Adrenergic blockers propranolol
Rifampin 2+ Nitroglycerin
Abciximab and eptifibatide 2+ Antihistamines
Thiazides and furosemide 2+ Phenothiazines
Acyclovir 2+ Cyclic antidepressants
Procainamide 2+
Digoxin 2+
Cimetidine and ranitidine 2+
Phenytoin and valproate 1+
Penicillinscephalosporins 1+
A CBC will establish the presence and degree of thrombocytopenia and determine whether otherhematologic cell lines are aected A peripheral smear should be examined to assess platelet morphologyLoading [Contrib]a11yaccessibility-menujs
3272019
423
and evaluate other cell lines Rarely in vitro platelet agglutination occurs which leads to spuriously lowplatelet counts reported by automated cell counters (pseudothrombocytopenia) when collected inethylenediaminetetraacetic acidndashcoated blood tubes this can be detected by the presence of plateletclumping on a peripheral smear In this case a correct platelet count may be obtained by using citrated orheparin-anticoagulated blood tubes
Testing for human immunodeficiency virus and hepatitis C virus is recommended in cases of isolated
thrombocytopenia as low platelets may be the only readily apparent manifestation in early infections5 If theetiology of low platelets remains unclear further laboratory testing to evaluate for disorders such ashemolysis and disseminated intravascular coagulation (DIC) may be needed Although usually not necessaryin instances of isolated thrombocytopenia bone marrow biopsy may be obtained when malignancy or otherbone marrow pathologies are of concern
When circulating platelet levels decrease to below 10000 to 20000mm3 (10 to 20 times 109L) the risk ofspontaneous bleeding becomes concerning particularly for intracranial hemorrhage Additional risk factorsfor bleeding include age comorbid illness (ie renal disease liver disease connective tissue disease pepticulcer disease hypertension) fall risk and lifestyle activity With the exception of a few specific diseaseprocesses platelet transfusion in the nonbleeding patient should be considered when counts fall below
10000mm3 (10 times109L) or higher if other comorbid illnesses are present6 The cause of the plateletdeficiency may also influence the risk of bleeding At a given platelet level patients with immunethrombocytopenia (ITP) typically bleed less than patients with aplastic anemia as the younger platelets
present in ITP are more eective in hemostasis7
Immune Causes of ThrombocytopeniaImmune Causes of Thrombocytopenia
ITP is an acquired immune-mediated disorder in which circulating platelets typically fall to very low levels38
ITP results from antiplatelet antibodies that attack platelet surface glycoproteins such as glycoproteinIIbIIIa leading to peripheral platelet destruction There is evidence that the same antibodies lead to
impaired platelet production by megakaryocytes9 Despite very low platelet counts the circulating plateletsare not functionally impaired
Immune thrombocytopenia may be classified as primary (formerly known as idiopathic thrombocytopenicpurpura) or secondary when associated with other medical conditions (autoimmune disorders infections) or
drug exposures8 This distinction is of clinical importance as management of the underlying disorder ordiscontinuation of the drug in cases of secondary ITP may lead to normalization of the platelet count
Primary ITP may occur at any age with equal prevalence between genders with the exception of those age30 to 60 years in which women predominate Primary ITP is classified by duration of illness newly diagnosed
(diagnosis to 3 months) persistent (3 months to 12 months) and chronic (gt12 months)8 The majority ofadults with primary ITP progress to chronic illness
Loading [Contrib]a11yaccessibility-menujs
3272019
523
The most common presenting sign of ITP is a petechial rash (Figure 233-1AFigure 233-1A) Mild epistaxis gingival bleeding(Figure 233-1BFigure 233-1B) and menorrhagia in women of childbearing age may also be seen Except for petechiae andbruising the patient should have a normal physical examination
FIGURE 233-1FIGURE 233-1
Two patients with idiopathic thrombocytopenic purpura AA Petechiae with platelet count of 3000mm3 (3 times
109L) BB Gingival bleeding with platelet count of 5000mm3 (5 times 109L) [Image used with permission of JStephan Stapczynski MD]
Loading [Contrib]a11yaccessibility-menujs
3272019
623
The CBC should demonstrate normal cell lines except for the platelets A mild anemia may be seen if bleedingis present The peripheral smear should show large well-granulated platelets although they will be few innumber Bone marrow biopsy is not indicated unless clinical features are atypical If the evaluation supportsthe diagnosis of primary ITP then additional testing in the ED is not required
Treatment for ITP is initiated based on the risk of bleeding (Table 233-3Table 233-3) Major bleeding complications in
patients with platelets gt50000 mm3 (gt50 times 109L) are uncommon As most fatal bleeding complications
occur when platelet counts fall below 30000mm3 (30 times 109L) experts and guidelines recommend this level
as the threshold for initiating treatment of ITP in adults5691011 Bleeding risk correlates with lower plateletcounts and patient age greater than 60 a prior history of bleeding certain chronic illnesses and use ofmedications that alter hemostasis all heighten this risk Therefore certain patients may benefit from medical
treatment despite a platelet count exceeding 30000mm3 (30 times 109L) For all patients with primary ITPbleeding risk should be minimized including avoiding use of antiplatelet medications when possiblemaintenance of good blood pressure control optimized treatment of exacerbating comorbid conditions (ieliver disease renal disease) and addressing fall risks
Loading [Contrib]a11yaccessibility-menujs
3272019
723
TABLE 233-3
Treatment of Immune ThrombocytopeniaTreatment of Immune Thrombocytopenia
Platelet
transfusionlt10000ndash20000mm3 (lt10ndash20 times 109L) prophylactically to prevent bleeding
lt50000mm3 (lt50 times 109L) if actively bleeding
lt20000ndash50000mm3 (lt20ndash50 times 109L) if patient requires diagnostic puncture
lt50000ndash100000mm3 (lt50ndash100 times 109L) if patient requires invasive procedure
Corticosteroids Prednisone 1 milligramkg PO per day for 21 days then tapered or dexamethasone 20
milligramsm2 IV per day for 4 d
IV
immunoglobulin
1 gramkg IV per day for 3 d
Splenectomy Considered for refractory cases
About two thirds of children with primary ITP will have spontaneous resolution within 6 months of
diagnosis11 An antecedent viral infection is commonly reported Additionally the measles-mumps-rubellavaccination has been associated with the development of acute ITP although this is rare and occurs in less
than 1 per 25000 doses given12 The risk of severe bleeding complications appears to be rare in children
regardless of their absolute platelet count5813 Children without signs of active bleeding and goodpsychosocial support typically do not require hospitalization or medical treatment Good anticipatoryguidance should be provided to the family and the child should abstain from contact sports or activities thatmight place them at risk for head injury
First-line treatment for primary ITP generally includes corticosteroids typically prednisone 1 milligramkg
per day for 4 weeks (shorter courses may be considered for children)59101113 Initial response may not beseen for 4 to 14 days and peak eect can be expected between 7 and 28 days IV immunoglobulin may alsobe considered either alone or in combination with corticosteroids at a dose 1 gkgper day for 3 days Initialresponse to IV immunoglobulin is more rapid than corticosteroids occurring between 1 and 3 days withpeak eect seen between 2 and 7 days Side eects of IV immunoglobulin may include aseptic meningitistransient neutropenia acute kidney injury and transfusion reactionshypotension
Anti-Rho(D) immunoglobulin at 50 to 75 microgramskg for a single dose may also be considered as a first-
line treatment strategy in patients who are Rh(D) positive and have not undergone splenectomy14 Initialresponse rate and peak eect are similar to that seen with IV immunoglobulin Mild hemolysis can beexpected and rare serious or even fatal cases of intravascular hemolysis DIC and renal failure have beenreported with anti-Rho(D) use prompting the US Food and Drug Administration to administer a warningLoading [Contrib]a11yaccessibility-menujs
3272019
823
pertaining to its use in 2010 Second-line treatment modalities include splenectomy and use of neweragents such as the monoclonal antibody rituximab which blunts the autoimmune destruction of plateletsand thrombopoietin receptor agonists which stimulate platelet production (ie romiplostin eltrombopag)
In the event of life-threatening hemorrhage where hemostasis must be achieved rapidly IV corticosteroids
(such as dexamethasone) and IV immunoglobulin should be administered concomitantly13 Platelettransfusions should be initiated and doses two to three times the typical dose might be required due to
persistent autoimmune destruction6 Platelet transfusions may need to be repeated frequently until bleedingsubsides or targeted treatment modalities take eect Emergent splenectomy may be considered if all othertreatment options are exhausted
Drug-Induced Immune ThrombocytopeniaDrug-Induced Immune Thrombocytopenia
Over 200 drugs have been implicated in causing immune-mediated suppression of platelet production or
increased platelet destruction (Table 233-2)34 The clinical presentation is similar to ITP and thethrombocytopenia may severe Drug-induced thrombocytopenia typically occurs 5 to 14 days followinginitiation of a drug but may occur sooner if there has been recent prior exposure A careful history should notonly include prescribed medications but also herbal remedies and food and beverage use (ie quinine intonic water alcohol use tahini) Chronic alcohol use is a common cause of thrombocytopenia Plateletcounts typically normalize with cessation of the causative agent Heparin-induced thrombocytopenia causesa significant drop in platelets but patients are paradoxically hypercoagulable due to platelet activation (seechapter 239 Thrombotics and Antithrombotics)
Nonimmune Causes of ThrombocytopeniaNonimmune Causes of Thrombocytopenia
Thrombocytopenia may occur from various nonndashimmune-mediated causes (Table 233-1) In thromboticthrombocytopenic purpura and hemolytic-uremic syndrome thrombotic microangiopathy occurs whenvessel injury results in deposition of platelet-fibrin thrombi (see chapters 143 Oncologic and HematologicEmergencies in Children and 237 Acquired Hemolytic Anemia) DIC is also a well-described cause ofplatelet destruction In patients with marked hemorrhage large-volume fluid resuscitation may lead to adilutional thrombocytopenia Additionally certain bacterial rickettsial and viral infections can cause directtoxic destruction of platelets Thrombocytopenia specific to pregnancy may be a result of the hemolysisndashelevated liver enzymesndashlow platelets (HELLP) syndrome pre-eclampsia or gestational thrombocytopenia(see chapter 100 Maternal Emergencies aer 20 Weeks of Pregnancy and in the Postpartum Period)Finally an enlarged spleen can sequester a significant portion of the platelet pool
Thrombocytopenia is present in up to 70 of patients with chronic liver disease15 The etiology appearsmultifactorial Patients oen have underlying medical conditions related to their liver disease such as alcoholuse viral hepatitis or nutritional deficiencies that impair platelet production Thrombopoietin which isproduced by hepatocytes may be decreased Portal hypertension may lead to splenic sequestrationEndotoxemia from infection may promote platelet aggregation Some patients also demonstrate plateletLoading [Contrib]a11yaccessibility-menujs
3272019
923
autoantibodies The degree of quantitative thrombocytopenia may be mitigated by an increased level ofcirculating von Willebrand factor that is typically seen which promotes platelet adhesion For this reasonroutine platelet transfusion is not recommended in the absence of clinically significant bleeding However a
platelet count of gt50000mm3 (gt50 times 109L) should be achieved prior to invasive procedures (ie lumbar
puncture surgery liver biopsy)16
FUNCTIONAL PLATELET DISORDERSFUNCTIONAL PLATELET DISORDERS
Several disease processes can cause acquired qualitative or functional abnormalities of platelets (Table 233-Table 233-
44)17 In the myeloproliferative diseases platelets are oen dysfunctional even if the platelet count is normalor elevated Patients can have prolonged bleeding times and clinically significant bleeding To control acute
bleeding transfusion should be considered to raise the level of normal platelets to 50000mm3 (50 times 109L)In macroglobulinemia and related disorders the elevated level of viscous proteins interferes with plateletfunction Patients with clinically significant bleeding may require plasmapheresis to reduce the protein leveland correct hemostatic function
TABLE 233-4
Clinical Conditions Associated with Qualitative Platelet AbnormalitiesClinical Conditions Associated with Qualitative Platelet Abnormalities
Uremia
Liver disease
Disseminated intravascular coagulation
Antiplatelet antibodies (immune thrombocytopenia systemic lupus erythematosus)
Cardiopulmonary bypass
Myeloproliferative disorders (thrombocytosis polycythemia vera chronic myeloid leukemia acute
lymphocytic or myelogenous leukemia)
Dysproteinemias (multiple myeloma Waldenstroumlms macroglobulinemia)
von Willebrands disease (congenital or acquired)
Many drugs can influence platelet function (Table 233-2 and Table 233-5Table 233-5) Of these the most commonly usedare aspirin which produces an irreversible impairment in platelet aggregation and the nonsteroidal anti-inflammatory drugs clopidogrel and ticlopidine which produce temporary impairment in platelet adhesionand aggregation (see chapter 239)
Loading [Contrib]a11yaccessibility-menujs
3272019
1023
TABLE 233-5
Duration of Antiplatelet ActivityDuration of Antiplatelet Activity
DrugDrug OnsetOnset Duration of EectDuration of Eect
Aspirin 1 h Up to 7 d
Most nonsteroidal anti-inflammatory drugs 1 h 1 d
Piroxicam 1 h 2 d
Ticlopidine or clopidogrel 1ndash2 d 4ndash7 d
Thrombocytosis a platelet count exceeding 500000mm3 (500 times 109L) can be seen in many disordersincluding inflammatory reactions malignancy polycythemia and postsplenectomy Platelet function can benormal or abnormal depending on the underlying condition Therefore thrombocytosis can be associatedwith bleeding (mucosal ecchymotic GI) or thromboembolic (deep venous thrombosis portal or mesentericthrombosis splenic vein thrombosis) manifestations However these events are unusual even with platelet
counts in excess of 1000000mm3 (1000 times 109L)
ACQUIRED COAGULATION DISORDERSACQUIRED COAGULATION DISORDERS
Acquired coagulation disorders can result from underlying medical disease and autoimmune factorinhibitors
LIVER DISEASELIVER DISEASE
Acute and chronic liver disease is commonly associated with laboratory tests of impaired coagulationHepatocytes synthesize all of the coagulation factors and related regulatory proteins with the exception offactor VIII and von Willebrand factor Diseases aecting the hepatic parenchyma may result in a decreasedsynthesis of these factors including the vitamin Kndashdependent carboxylation of factors II (prothrombin) VIIIX and X Because vitamin K is a fat-soluble vitamin malabsorption can occur with processes that interferewith the absorption of fat-soluble vitamins including impaired bile acid metabolism (ie primary biliarycirrhosis) intrahepatic or extrahepatic cholestasis and treatment with bile acid binders Thus prolongedprothrombin time is common in patients with decompensated hepatic function Despite markedprolongations of prothrombin time and activated partial thromboplastin time (PTT) seen in advanced liverdisease and cirrhosis these tests poorly predict onset and severity of bleeding including bleeding from
esophageal varices or invasive procedures or surgery16181920 Although there may be marked reduction inprocoagulant proteins in liver disease there is typically a parallel decrease in the endogenous anticoagulantLoading [Contrib]a11yaccessibility-menujs
3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
323
Note 4+ to 1+ indicates relative incidence from more frequent to less frequent based on case reports
TABLE 233-2
Drugs That Produce Thrombocytopenia or Impair Platelet FunctionDrugs That Produce Thrombocytopenia or Impair Platelet Function
Produce ThrombocytopeniaProduce Thrombocytopenia Impair FunctionImpair Function
Heparin 4+ Aspirin
Gold salts 4+ Nonsteroidal anti-inflammatory drugs
Sulfa-containing antibiotics 4+ Glycoprotein IIbndashIIIa agents ticlopidine and clopidogrel
Quinine and quinidine 4+
Ethanol (chronic use) 4+ Penicillins and cephalosporins
Aspirin 3+ Calcium channel blockers
Indomethacin 3+ β-Adrenergic blockers propranolol
Rifampin 2+ Nitroglycerin
Abciximab and eptifibatide 2+ Antihistamines
Thiazides and furosemide 2+ Phenothiazines
Acyclovir 2+ Cyclic antidepressants
Procainamide 2+
Digoxin 2+
Cimetidine and ranitidine 2+
Phenytoin and valproate 1+
Penicillinscephalosporins 1+
A CBC will establish the presence and degree of thrombocytopenia and determine whether otherhematologic cell lines are aected A peripheral smear should be examined to assess platelet morphologyLoading [Contrib]a11yaccessibility-menujs
3272019
423
and evaluate other cell lines Rarely in vitro platelet agglutination occurs which leads to spuriously lowplatelet counts reported by automated cell counters (pseudothrombocytopenia) when collected inethylenediaminetetraacetic acidndashcoated blood tubes this can be detected by the presence of plateletclumping on a peripheral smear In this case a correct platelet count may be obtained by using citrated orheparin-anticoagulated blood tubes
Testing for human immunodeficiency virus and hepatitis C virus is recommended in cases of isolated
thrombocytopenia as low platelets may be the only readily apparent manifestation in early infections5 If theetiology of low platelets remains unclear further laboratory testing to evaluate for disorders such ashemolysis and disseminated intravascular coagulation (DIC) may be needed Although usually not necessaryin instances of isolated thrombocytopenia bone marrow biopsy may be obtained when malignancy or otherbone marrow pathologies are of concern
When circulating platelet levels decrease to below 10000 to 20000mm3 (10 to 20 times 109L) the risk ofspontaneous bleeding becomes concerning particularly for intracranial hemorrhage Additional risk factorsfor bleeding include age comorbid illness (ie renal disease liver disease connective tissue disease pepticulcer disease hypertension) fall risk and lifestyle activity With the exception of a few specific diseaseprocesses platelet transfusion in the nonbleeding patient should be considered when counts fall below
10000mm3 (10 times109L) or higher if other comorbid illnesses are present6 The cause of the plateletdeficiency may also influence the risk of bleeding At a given platelet level patients with immunethrombocytopenia (ITP) typically bleed less than patients with aplastic anemia as the younger platelets
present in ITP are more eective in hemostasis7
Immune Causes of ThrombocytopeniaImmune Causes of Thrombocytopenia
ITP is an acquired immune-mediated disorder in which circulating platelets typically fall to very low levels38
ITP results from antiplatelet antibodies that attack platelet surface glycoproteins such as glycoproteinIIbIIIa leading to peripheral platelet destruction There is evidence that the same antibodies lead to
impaired platelet production by megakaryocytes9 Despite very low platelet counts the circulating plateletsare not functionally impaired
Immune thrombocytopenia may be classified as primary (formerly known as idiopathic thrombocytopenicpurpura) or secondary when associated with other medical conditions (autoimmune disorders infections) or
drug exposures8 This distinction is of clinical importance as management of the underlying disorder ordiscontinuation of the drug in cases of secondary ITP may lead to normalization of the platelet count
Primary ITP may occur at any age with equal prevalence between genders with the exception of those age30 to 60 years in which women predominate Primary ITP is classified by duration of illness newly diagnosed
(diagnosis to 3 months) persistent (3 months to 12 months) and chronic (gt12 months)8 The majority ofadults with primary ITP progress to chronic illness
Loading [Contrib]a11yaccessibility-menujs
3272019
523
The most common presenting sign of ITP is a petechial rash (Figure 233-1AFigure 233-1A) Mild epistaxis gingival bleeding(Figure 233-1BFigure 233-1B) and menorrhagia in women of childbearing age may also be seen Except for petechiae andbruising the patient should have a normal physical examination
FIGURE 233-1FIGURE 233-1
Two patients with idiopathic thrombocytopenic purpura AA Petechiae with platelet count of 3000mm3 (3 times
109L) BB Gingival bleeding with platelet count of 5000mm3 (5 times 109L) [Image used with permission of JStephan Stapczynski MD]
Loading [Contrib]a11yaccessibility-menujs
3272019
623
The CBC should demonstrate normal cell lines except for the platelets A mild anemia may be seen if bleedingis present The peripheral smear should show large well-granulated platelets although they will be few innumber Bone marrow biopsy is not indicated unless clinical features are atypical If the evaluation supportsthe diagnosis of primary ITP then additional testing in the ED is not required
Treatment for ITP is initiated based on the risk of bleeding (Table 233-3Table 233-3) Major bleeding complications in
patients with platelets gt50000 mm3 (gt50 times 109L) are uncommon As most fatal bleeding complications
occur when platelet counts fall below 30000mm3 (30 times 109L) experts and guidelines recommend this level
as the threshold for initiating treatment of ITP in adults5691011 Bleeding risk correlates with lower plateletcounts and patient age greater than 60 a prior history of bleeding certain chronic illnesses and use ofmedications that alter hemostasis all heighten this risk Therefore certain patients may benefit from medical
treatment despite a platelet count exceeding 30000mm3 (30 times 109L) For all patients with primary ITPbleeding risk should be minimized including avoiding use of antiplatelet medications when possiblemaintenance of good blood pressure control optimized treatment of exacerbating comorbid conditions (ieliver disease renal disease) and addressing fall risks
Loading [Contrib]a11yaccessibility-menujs
3272019
723
TABLE 233-3
Treatment of Immune ThrombocytopeniaTreatment of Immune Thrombocytopenia
Platelet
transfusionlt10000ndash20000mm3 (lt10ndash20 times 109L) prophylactically to prevent bleeding
lt50000mm3 (lt50 times 109L) if actively bleeding
lt20000ndash50000mm3 (lt20ndash50 times 109L) if patient requires diagnostic puncture
lt50000ndash100000mm3 (lt50ndash100 times 109L) if patient requires invasive procedure
Corticosteroids Prednisone 1 milligramkg PO per day for 21 days then tapered or dexamethasone 20
milligramsm2 IV per day for 4 d
IV
immunoglobulin
1 gramkg IV per day for 3 d
Splenectomy Considered for refractory cases
About two thirds of children with primary ITP will have spontaneous resolution within 6 months of
diagnosis11 An antecedent viral infection is commonly reported Additionally the measles-mumps-rubellavaccination has been associated with the development of acute ITP although this is rare and occurs in less
than 1 per 25000 doses given12 The risk of severe bleeding complications appears to be rare in children
regardless of their absolute platelet count5813 Children without signs of active bleeding and goodpsychosocial support typically do not require hospitalization or medical treatment Good anticipatoryguidance should be provided to the family and the child should abstain from contact sports or activities thatmight place them at risk for head injury
First-line treatment for primary ITP generally includes corticosteroids typically prednisone 1 milligramkg
per day for 4 weeks (shorter courses may be considered for children)59101113 Initial response may not beseen for 4 to 14 days and peak eect can be expected between 7 and 28 days IV immunoglobulin may alsobe considered either alone or in combination with corticosteroids at a dose 1 gkgper day for 3 days Initialresponse to IV immunoglobulin is more rapid than corticosteroids occurring between 1 and 3 days withpeak eect seen between 2 and 7 days Side eects of IV immunoglobulin may include aseptic meningitistransient neutropenia acute kidney injury and transfusion reactionshypotension
Anti-Rho(D) immunoglobulin at 50 to 75 microgramskg for a single dose may also be considered as a first-
line treatment strategy in patients who are Rh(D) positive and have not undergone splenectomy14 Initialresponse rate and peak eect are similar to that seen with IV immunoglobulin Mild hemolysis can beexpected and rare serious or even fatal cases of intravascular hemolysis DIC and renal failure have beenreported with anti-Rho(D) use prompting the US Food and Drug Administration to administer a warningLoading [Contrib]a11yaccessibility-menujs
3272019
823
pertaining to its use in 2010 Second-line treatment modalities include splenectomy and use of neweragents such as the monoclonal antibody rituximab which blunts the autoimmune destruction of plateletsand thrombopoietin receptor agonists which stimulate platelet production (ie romiplostin eltrombopag)
In the event of life-threatening hemorrhage where hemostasis must be achieved rapidly IV corticosteroids
(such as dexamethasone) and IV immunoglobulin should be administered concomitantly13 Platelettransfusions should be initiated and doses two to three times the typical dose might be required due to
persistent autoimmune destruction6 Platelet transfusions may need to be repeated frequently until bleedingsubsides or targeted treatment modalities take eect Emergent splenectomy may be considered if all othertreatment options are exhausted
Drug-Induced Immune ThrombocytopeniaDrug-Induced Immune Thrombocytopenia
Over 200 drugs have been implicated in causing immune-mediated suppression of platelet production or
increased platelet destruction (Table 233-2)34 The clinical presentation is similar to ITP and thethrombocytopenia may severe Drug-induced thrombocytopenia typically occurs 5 to 14 days followinginitiation of a drug but may occur sooner if there has been recent prior exposure A careful history should notonly include prescribed medications but also herbal remedies and food and beverage use (ie quinine intonic water alcohol use tahini) Chronic alcohol use is a common cause of thrombocytopenia Plateletcounts typically normalize with cessation of the causative agent Heparin-induced thrombocytopenia causesa significant drop in platelets but patients are paradoxically hypercoagulable due to platelet activation (seechapter 239 Thrombotics and Antithrombotics)
Nonimmune Causes of ThrombocytopeniaNonimmune Causes of Thrombocytopenia
Thrombocytopenia may occur from various nonndashimmune-mediated causes (Table 233-1) In thromboticthrombocytopenic purpura and hemolytic-uremic syndrome thrombotic microangiopathy occurs whenvessel injury results in deposition of platelet-fibrin thrombi (see chapters 143 Oncologic and HematologicEmergencies in Children and 237 Acquired Hemolytic Anemia) DIC is also a well-described cause ofplatelet destruction In patients with marked hemorrhage large-volume fluid resuscitation may lead to adilutional thrombocytopenia Additionally certain bacterial rickettsial and viral infections can cause directtoxic destruction of platelets Thrombocytopenia specific to pregnancy may be a result of the hemolysisndashelevated liver enzymesndashlow platelets (HELLP) syndrome pre-eclampsia or gestational thrombocytopenia(see chapter 100 Maternal Emergencies aer 20 Weeks of Pregnancy and in the Postpartum Period)Finally an enlarged spleen can sequester a significant portion of the platelet pool
Thrombocytopenia is present in up to 70 of patients with chronic liver disease15 The etiology appearsmultifactorial Patients oen have underlying medical conditions related to their liver disease such as alcoholuse viral hepatitis or nutritional deficiencies that impair platelet production Thrombopoietin which isproduced by hepatocytes may be decreased Portal hypertension may lead to splenic sequestrationEndotoxemia from infection may promote platelet aggregation Some patients also demonstrate plateletLoading [Contrib]a11yaccessibility-menujs
3272019
923
autoantibodies The degree of quantitative thrombocytopenia may be mitigated by an increased level ofcirculating von Willebrand factor that is typically seen which promotes platelet adhesion For this reasonroutine platelet transfusion is not recommended in the absence of clinically significant bleeding However a
platelet count of gt50000mm3 (gt50 times 109L) should be achieved prior to invasive procedures (ie lumbar
puncture surgery liver biopsy)16
FUNCTIONAL PLATELET DISORDERSFUNCTIONAL PLATELET DISORDERS
Several disease processes can cause acquired qualitative or functional abnormalities of platelets (Table 233-Table 233-
44)17 In the myeloproliferative diseases platelets are oen dysfunctional even if the platelet count is normalor elevated Patients can have prolonged bleeding times and clinically significant bleeding To control acute
bleeding transfusion should be considered to raise the level of normal platelets to 50000mm3 (50 times 109L)In macroglobulinemia and related disorders the elevated level of viscous proteins interferes with plateletfunction Patients with clinically significant bleeding may require plasmapheresis to reduce the protein leveland correct hemostatic function
TABLE 233-4
Clinical Conditions Associated with Qualitative Platelet AbnormalitiesClinical Conditions Associated with Qualitative Platelet Abnormalities
Uremia
Liver disease
Disseminated intravascular coagulation
Antiplatelet antibodies (immune thrombocytopenia systemic lupus erythematosus)
Cardiopulmonary bypass
Myeloproliferative disorders (thrombocytosis polycythemia vera chronic myeloid leukemia acute
lymphocytic or myelogenous leukemia)
Dysproteinemias (multiple myeloma Waldenstroumlms macroglobulinemia)
von Willebrands disease (congenital or acquired)
Many drugs can influence platelet function (Table 233-2 and Table 233-5Table 233-5) Of these the most commonly usedare aspirin which produces an irreversible impairment in platelet aggregation and the nonsteroidal anti-inflammatory drugs clopidogrel and ticlopidine which produce temporary impairment in platelet adhesionand aggregation (see chapter 239)
Loading [Contrib]a11yaccessibility-menujs
3272019
1023
TABLE 233-5
Duration of Antiplatelet ActivityDuration of Antiplatelet Activity
DrugDrug OnsetOnset Duration of EectDuration of Eect
Aspirin 1 h Up to 7 d
Most nonsteroidal anti-inflammatory drugs 1 h 1 d
Piroxicam 1 h 2 d
Ticlopidine or clopidogrel 1ndash2 d 4ndash7 d
Thrombocytosis a platelet count exceeding 500000mm3 (500 times 109L) can be seen in many disordersincluding inflammatory reactions malignancy polycythemia and postsplenectomy Platelet function can benormal or abnormal depending on the underlying condition Therefore thrombocytosis can be associatedwith bleeding (mucosal ecchymotic GI) or thromboembolic (deep venous thrombosis portal or mesentericthrombosis splenic vein thrombosis) manifestations However these events are unusual even with platelet
counts in excess of 1000000mm3 (1000 times 109L)
ACQUIRED COAGULATION DISORDERSACQUIRED COAGULATION DISORDERS
Acquired coagulation disorders can result from underlying medical disease and autoimmune factorinhibitors
LIVER DISEASELIVER DISEASE
Acute and chronic liver disease is commonly associated with laboratory tests of impaired coagulationHepatocytes synthesize all of the coagulation factors and related regulatory proteins with the exception offactor VIII and von Willebrand factor Diseases aecting the hepatic parenchyma may result in a decreasedsynthesis of these factors including the vitamin Kndashdependent carboxylation of factors II (prothrombin) VIIIX and X Because vitamin K is a fat-soluble vitamin malabsorption can occur with processes that interferewith the absorption of fat-soluble vitamins including impaired bile acid metabolism (ie primary biliarycirrhosis) intrahepatic or extrahepatic cholestasis and treatment with bile acid binders Thus prolongedprothrombin time is common in patients with decompensated hepatic function Despite markedprolongations of prothrombin time and activated partial thromboplastin time (PTT) seen in advanced liverdisease and cirrhosis these tests poorly predict onset and severity of bleeding including bleeding from
esophageal varices or invasive procedures or surgery16181920 Although there may be marked reduction inprocoagulant proteins in liver disease there is typically a parallel decrease in the endogenous anticoagulantLoading [Contrib]a11yaccessibility-menujs
3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
423
and evaluate other cell lines Rarely in vitro platelet agglutination occurs which leads to spuriously lowplatelet counts reported by automated cell counters (pseudothrombocytopenia) when collected inethylenediaminetetraacetic acidndashcoated blood tubes this can be detected by the presence of plateletclumping on a peripheral smear In this case a correct platelet count may be obtained by using citrated orheparin-anticoagulated blood tubes
Testing for human immunodeficiency virus and hepatitis C virus is recommended in cases of isolated
thrombocytopenia as low platelets may be the only readily apparent manifestation in early infections5 If theetiology of low platelets remains unclear further laboratory testing to evaluate for disorders such ashemolysis and disseminated intravascular coagulation (DIC) may be needed Although usually not necessaryin instances of isolated thrombocytopenia bone marrow biopsy may be obtained when malignancy or otherbone marrow pathologies are of concern
When circulating platelet levels decrease to below 10000 to 20000mm3 (10 to 20 times 109L) the risk ofspontaneous bleeding becomes concerning particularly for intracranial hemorrhage Additional risk factorsfor bleeding include age comorbid illness (ie renal disease liver disease connective tissue disease pepticulcer disease hypertension) fall risk and lifestyle activity With the exception of a few specific diseaseprocesses platelet transfusion in the nonbleeding patient should be considered when counts fall below
10000mm3 (10 times109L) or higher if other comorbid illnesses are present6 The cause of the plateletdeficiency may also influence the risk of bleeding At a given platelet level patients with immunethrombocytopenia (ITP) typically bleed less than patients with aplastic anemia as the younger platelets
present in ITP are more eective in hemostasis7
Immune Causes of ThrombocytopeniaImmune Causes of Thrombocytopenia
ITP is an acquired immune-mediated disorder in which circulating platelets typically fall to very low levels38
ITP results from antiplatelet antibodies that attack platelet surface glycoproteins such as glycoproteinIIbIIIa leading to peripheral platelet destruction There is evidence that the same antibodies lead to
impaired platelet production by megakaryocytes9 Despite very low platelet counts the circulating plateletsare not functionally impaired
Immune thrombocytopenia may be classified as primary (formerly known as idiopathic thrombocytopenicpurpura) or secondary when associated with other medical conditions (autoimmune disorders infections) or
drug exposures8 This distinction is of clinical importance as management of the underlying disorder ordiscontinuation of the drug in cases of secondary ITP may lead to normalization of the platelet count
Primary ITP may occur at any age with equal prevalence between genders with the exception of those age30 to 60 years in which women predominate Primary ITP is classified by duration of illness newly diagnosed
(diagnosis to 3 months) persistent (3 months to 12 months) and chronic (gt12 months)8 The majority ofadults with primary ITP progress to chronic illness
Loading [Contrib]a11yaccessibility-menujs
3272019
523
The most common presenting sign of ITP is a petechial rash (Figure 233-1AFigure 233-1A) Mild epistaxis gingival bleeding(Figure 233-1BFigure 233-1B) and menorrhagia in women of childbearing age may also be seen Except for petechiae andbruising the patient should have a normal physical examination
FIGURE 233-1FIGURE 233-1
Two patients with idiopathic thrombocytopenic purpura AA Petechiae with platelet count of 3000mm3 (3 times
109L) BB Gingival bleeding with platelet count of 5000mm3 (5 times 109L) [Image used with permission of JStephan Stapczynski MD]
Loading [Contrib]a11yaccessibility-menujs
3272019
623
The CBC should demonstrate normal cell lines except for the platelets A mild anemia may be seen if bleedingis present The peripheral smear should show large well-granulated platelets although they will be few innumber Bone marrow biopsy is not indicated unless clinical features are atypical If the evaluation supportsthe diagnosis of primary ITP then additional testing in the ED is not required
Treatment for ITP is initiated based on the risk of bleeding (Table 233-3Table 233-3) Major bleeding complications in
patients with platelets gt50000 mm3 (gt50 times 109L) are uncommon As most fatal bleeding complications
occur when platelet counts fall below 30000mm3 (30 times 109L) experts and guidelines recommend this level
as the threshold for initiating treatment of ITP in adults5691011 Bleeding risk correlates with lower plateletcounts and patient age greater than 60 a prior history of bleeding certain chronic illnesses and use ofmedications that alter hemostasis all heighten this risk Therefore certain patients may benefit from medical
treatment despite a platelet count exceeding 30000mm3 (30 times 109L) For all patients with primary ITPbleeding risk should be minimized including avoiding use of antiplatelet medications when possiblemaintenance of good blood pressure control optimized treatment of exacerbating comorbid conditions (ieliver disease renal disease) and addressing fall risks
Loading [Contrib]a11yaccessibility-menujs
3272019
723
TABLE 233-3
Treatment of Immune ThrombocytopeniaTreatment of Immune Thrombocytopenia
Platelet
transfusionlt10000ndash20000mm3 (lt10ndash20 times 109L) prophylactically to prevent bleeding
lt50000mm3 (lt50 times 109L) if actively bleeding
lt20000ndash50000mm3 (lt20ndash50 times 109L) if patient requires diagnostic puncture
lt50000ndash100000mm3 (lt50ndash100 times 109L) if patient requires invasive procedure
Corticosteroids Prednisone 1 milligramkg PO per day for 21 days then tapered or dexamethasone 20
milligramsm2 IV per day for 4 d
IV
immunoglobulin
1 gramkg IV per day for 3 d
Splenectomy Considered for refractory cases
About two thirds of children with primary ITP will have spontaneous resolution within 6 months of
diagnosis11 An antecedent viral infection is commonly reported Additionally the measles-mumps-rubellavaccination has been associated with the development of acute ITP although this is rare and occurs in less
than 1 per 25000 doses given12 The risk of severe bleeding complications appears to be rare in children
regardless of their absolute platelet count5813 Children without signs of active bleeding and goodpsychosocial support typically do not require hospitalization or medical treatment Good anticipatoryguidance should be provided to the family and the child should abstain from contact sports or activities thatmight place them at risk for head injury
First-line treatment for primary ITP generally includes corticosteroids typically prednisone 1 milligramkg
per day for 4 weeks (shorter courses may be considered for children)59101113 Initial response may not beseen for 4 to 14 days and peak eect can be expected between 7 and 28 days IV immunoglobulin may alsobe considered either alone or in combination with corticosteroids at a dose 1 gkgper day for 3 days Initialresponse to IV immunoglobulin is more rapid than corticosteroids occurring between 1 and 3 days withpeak eect seen between 2 and 7 days Side eects of IV immunoglobulin may include aseptic meningitistransient neutropenia acute kidney injury and transfusion reactionshypotension
Anti-Rho(D) immunoglobulin at 50 to 75 microgramskg for a single dose may also be considered as a first-
line treatment strategy in patients who are Rh(D) positive and have not undergone splenectomy14 Initialresponse rate and peak eect are similar to that seen with IV immunoglobulin Mild hemolysis can beexpected and rare serious or even fatal cases of intravascular hemolysis DIC and renal failure have beenreported with anti-Rho(D) use prompting the US Food and Drug Administration to administer a warningLoading [Contrib]a11yaccessibility-menujs
3272019
823
pertaining to its use in 2010 Second-line treatment modalities include splenectomy and use of neweragents such as the monoclonal antibody rituximab which blunts the autoimmune destruction of plateletsand thrombopoietin receptor agonists which stimulate platelet production (ie romiplostin eltrombopag)
In the event of life-threatening hemorrhage where hemostasis must be achieved rapidly IV corticosteroids
(such as dexamethasone) and IV immunoglobulin should be administered concomitantly13 Platelettransfusions should be initiated and doses two to three times the typical dose might be required due to
persistent autoimmune destruction6 Platelet transfusions may need to be repeated frequently until bleedingsubsides or targeted treatment modalities take eect Emergent splenectomy may be considered if all othertreatment options are exhausted
Drug-Induced Immune ThrombocytopeniaDrug-Induced Immune Thrombocytopenia
Over 200 drugs have been implicated in causing immune-mediated suppression of platelet production or
increased platelet destruction (Table 233-2)34 The clinical presentation is similar to ITP and thethrombocytopenia may severe Drug-induced thrombocytopenia typically occurs 5 to 14 days followinginitiation of a drug but may occur sooner if there has been recent prior exposure A careful history should notonly include prescribed medications but also herbal remedies and food and beverage use (ie quinine intonic water alcohol use tahini) Chronic alcohol use is a common cause of thrombocytopenia Plateletcounts typically normalize with cessation of the causative agent Heparin-induced thrombocytopenia causesa significant drop in platelets but patients are paradoxically hypercoagulable due to platelet activation (seechapter 239 Thrombotics and Antithrombotics)
Nonimmune Causes of ThrombocytopeniaNonimmune Causes of Thrombocytopenia
Thrombocytopenia may occur from various nonndashimmune-mediated causes (Table 233-1) In thromboticthrombocytopenic purpura and hemolytic-uremic syndrome thrombotic microangiopathy occurs whenvessel injury results in deposition of platelet-fibrin thrombi (see chapters 143 Oncologic and HematologicEmergencies in Children and 237 Acquired Hemolytic Anemia) DIC is also a well-described cause ofplatelet destruction In patients with marked hemorrhage large-volume fluid resuscitation may lead to adilutional thrombocytopenia Additionally certain bacterial rickettsial and viral infections can cause directtoxic destruction of platelets Thrombocytopenia specific to pregnancy may be a result of the hemolysisndashelevated liver enzymesndashlow platelets (HELLP) syndrome pre-eclampsia or gestational thrombocytopenia(see chapter 100 Maternal Emergencies aer 20 Weeks of Pregnancy and in the Postpartum Period)Finally an enlarged spleen can sequester a significant portion of the platelet pool
Thrombocytopenia is present in up to 70 of patients with chronic liver disease15 The etiology appearsmultifactorial Patients oen have underlying medical conditions related to their liver disease such as alcoholuse viral hepatitis or nutritional deficiencies that impair platelet production Thrombopoietin which isproduced by hepatocytes may be decreased Portal hypertension may lead to splenic sequestrationEndotoxemia from infection may promote platelet aggregation Some patients also demonstrate plateletLoading [Contrib]a11yaccessibility-menujs
3272019
923
autoantibodies The degree of quantitative thrombocytopenia may be mitigated by an increased level ofcirculating von Willebrand factor that is typically seen which promotes platelet adhesion For this reasonroutine platelet transfusion is not recommended in the absence of clinically significant bleeding However a
platelet count of gt50000mm3 (gt50 times 109L) should be achieved prior to invasive procedures (ie lumbar
puncture surgery liver biopsy)16
FUNCTIONAL PLATELET DISORDERSFUNCTIONAL PLATELET DISORDERS
Several disease processes can cause acquired qualitative or functional abnormalities of platelets (Table 233-Table 233-
44)17 In the myeloproliferative diseases platelets are oen dysfunctional even if the platelet count is normalor elevated Patients can have prolonged bleeding times and clinically significant bleeding To control acute
bleeding transfusion should be considered to raise the level of normal platelets to 50000mm3 (50 times 109L)In macroglobulinemia and related disorders the elevated level of viscous proteins interferes with plateletfunction Patients with clinically significant bleeding may require plasmapheresis to reduce the protein leveland correct hemostatic function
TABLE 233-4
Clinical Conditions Associated with Qualitative Platelet AbnormalitiesClinical Conditions Associated with Qualitative Platelet Abnormalities
Uremia
Liver disease
Disseminated intravascular coagulation
Antiplatelet antibodies (immune thrombocytopenia systemic lupus erythematosus)
Cardiopulmonary bypass
Myeloproliferative disorders (thrombocytosis polycythemia vera chronic myeloid leukemia acute
lymphocytic or myelogenous leukemia)
Dysproteinemias (multiple myeloma Waldenstroumlms macroglobulinemia)
von Willebrands disease (congenital or acquired)
Many drugs can influence platelet function (Table 233-2 and Table 233-5Table 233-5) Of these the most commonly usedare aspirin which produces an irreversible impairment in platelet aggregation and the nonsteroidal anti-inflammatory drugs clopidogrel and ticlopidine which produce temporary impairment in platelet adhesionand aggregation (see chapter 239)
Loading [Contrib]a11yaccessibility-menujs
3272019
1023
TABLE 233-5
Duration of Antiplatelet ActivityDuration of Antiplatelet Activity
DrugDrug OnsetOnset Duration of EectDuration of Eect
Aspirin 1 h Up to 7 d
Most nonsteroidal anti-inflammatory drugs 1 h 1 d
Piroxicam 1 h 2 d
Ticlopidine or clopidogrel 1ndash2 d 4ndash7 d
Thrombocytosis a platelet count exceeding 500000mm3 (500 times 109L) can be seen in many disordersincluding inflammatory reactions malignancy polycythemia and postsplenectomy Platelet function can benormal or abnormal depending on the underlying condition Therefore thrombocytosis can be associatedwith bleeding (mucosal ecchymotic GI) or thromboembolic (deep venous thrombosis portal or mesentericthrombosis splenic vein thrombosis) manifestations However these events are unusual even with platelet
counts in excess of 1000000mm3 (1000 times 109L)
ACQUIRED COAGULATION DISORDERSACQUIRED COAGULATION DISORDERS
Acquired coagulation disorders can result from underlying medical disease and autoimmune factorinhibitors
LIVER DISEASELIVER DISEASE
Acute and chronic liver disease is commonly associated with laboratory tests of impaired coagulationHepatocytes synthesize all of the coagulation factors and related regulatory proteins with the exception offactor VIII and von Willebrand factor Diseases aecting the hepatic parenchyma may result in a decreasedsynthesis of these factors including the vitamin Kndashdependent carboxylation of factors II (prothrombin) VIIIX and X Because vitamin K is a fat-soluble vitamin malabsorption can occur with processes that interferewith the absorption of fat-soluble vitamins including impaired bile acid metabolism (ie primary biliarycirrhosis) intrahepatic or extrahepatic cholestasis and treatment with bile acid binders Thus prolongedprothrombin time is common in patients with decompensated hepatic function Despite markedprolongations of prothrombin time and activated partial thromboplastin time (PTT) seen in advanced liverdisease and cirrhosis these tests poorly predict onset and severity of bleeding including bleeding from
esophageal varices or invasive procedures or surgery16181920 Although there may be marked reduction inprocoagulant proteins in liver disease there is typically a parallel decrease in the endogenous anticoagulantLoading [Contrib]a11yaccessibility-menujs
3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
523
The most common presenting sign of ITP is a petechial rash (Figure 233-1AFigure 233-1A) Mild epistaxis gingival bleeding(Figure 233-1BFigure 233-1B) and menorrhagia in women of childbearing age may also be seen Except for petechiae andbruising the patient should have a normal physical examination
FIGURE 233-1FIGURE 233-1
Two patients with idiopathic thrombocytopenic purpura AA Petechiae with platelet count of 3000mm3 (3 times
109L) BB Gingival bleeding with platelet count of 5000mm3 (5 times 109L) [Image used with permission of JStephan Stapczynski MD]
Loading [Contrib]a11yaccessibility-menujs
3272019
623
The CBC should demonstrate normal cell lines except for the platelets A mild anemia may be seen if bleedingis present The peripheral smear should show large well-granulated platelets although they will be few innumber Bone marrow biopsy is not indicated unless clinical features are atypical If the evaluation supportsthe diagnosis of primary ITP then additional testing in the ED is not required
Treatment for ITP is initiated based on the risk of bleeding (Table 233-3Table 233-3) Major bleeding complications in
patients with platelets gt50000 mm3 (gt50 times 109L) are uncommon As most fatal bleeding complications
occur when platelet counts fall below 30000mm3 (30 times 109L) experts and guidelines recommend this level
as the threshold for initiating treatment of ITP in adults5691011 Bleeding risk correlates with lower plateletcounts and patient age greater than 60 a prior history of bleeding certain chronic illnesses and use ofmedications that alter hemostasis all heighten this risk Therefore certain patients may benefit from medical
treatment despite a platelet count exceeding 30000mm3 (30 times 109L) For all patients with primary ITPbleeding risk should be minimized including avoiding use of antiplatelet medications when possiblemaintenance of good blood pressure control optimized treatment of exacerbating comorbid conditions (ieliver disease renal disease) and addressing fall risks
Loading [Contrib]a11yaccessibility-menujs
3272019
723
TABLE 233-3
Treatment of Immune ThrombocytopeniaTreatment of Immune Thrombocytopenia
Platelet
transfusionlt10000ndash20000mm3 (lt10ndash20 times 109L) prophylactically to prevent bleeding
lt50000mm3 (lt50 times 109L) if actively bleeding
lt20000ndash50000mm3 (lt20ndash50 times 109L) if patient requires diagnostic puncture
lt50000ndash100000mm3 (lt50ndash100 times 109L) if patient requires invasive procedure
Corticosteroids Prednisone 1 milligramkg PO per day for 21 days then tapered or dexamethasone 20
milligramsm2 IV per day for 4 d
IV
immunoglobulin
1 gramkg IV per day for 3 d
Splenectomy Considered for refractory cases
About two thirds of children with primary ITP will have spontaneous resolution within 6 months of
diagnosis11 An antecedent viral infection is commonly reported Additionally the measles-mumps-rubellavaccination has been associated with the development of acute ITP although this is rare and occurs in less
than 1 per 25000 doses given12 The risk of severe bleeding complications appears to be rare in children
regardless of their absolute platelet count5813 Children without signs of active bleeding and goodpsychosocial support typically do not require hospitalization or medical treatment Good anticipatoryguidance should be provided to the family and the child should abstain from contact sports or activities thatmight place them at risk for head injury
First-line treatment for primary ITP generally includes corticosteroids typically prednisone 1 milligramkg
per day for 4 weeks (shorter courses may be considered for children)59101113 Initial response may not beseen for 4 to 14 days and peak eect can be expected between 7 and 28 days IV immunoglobulin may alsobe considered either alone or in combination with corticosteroids at a dose 1 gkgper day for 3 days Initialresponse to IV immunoglobulin is more rapid than corticosteroids occurring between 1 and 3 days withpeak eect seen between 2 and 7 days Side eects of IV immunoglobulin may include aseptic meningitistransient neutropenia acute kidney injury and transfusion reactionshypotension
Anti-Rho(D) immunoglobulin at 50 to 75 microgramskg for a single dose may also be considered as a first-
line treatment strategy in patients who are Rh(D) positive and have not undergone splenectomy14 Initialresponse rate and peak eect are similar to that seen with IV immunoglobulin Mild hemolysis can beexpected and rare serious or even fatal cases of intravascular hemolysis DIC and renal failure have beenreported with anti-Rho(D) use prompting the US Food and Drug Administration to administer a warningLoading [Contrib]a11yaccessibility-menujs
3272019
823
pertaining to its use in 2010 Second-line treatment modalities include splenectomy and use of neweragents such as the monoclonal antibody rituximab which blunts the autoimmune destruction of plateletsand thrombopoietin receptor agonists which stimulate platelet production (ie romiplostin eltrombopag)
In the event of life-threatening hemorrhage where hemostasis must be achieved rapidly IV corticosteroids
(such as dexamethasone) and IV immunoglobulin should be administered concomitantly13 Platelettransfusions should be initiated and doses two to three times the typical dose might be required due to
persistent autoimmune destruction6 Platelet transfusions may need to be repeated frequently until bleedingsubsides or targeted treatment modalities take eect Emergent splenectomy may be considered if all othertreatment options are exhausted
Drug-Induced Immune ThrombocytopeniaDrug-Induced Immune Thrombocytopenia
Over 200 drugs have been implicated in causing immune-mediated suppression of platelet production or
increased platelet destruction (Table 233-2)34 The clinical presentation is similar to ITP and thethrombocytopenia may severe Drug-induced thrombocytopenia typically occurs 5 to 14 days followinginitiation of a drug but may occur sooner if there has been recent prior exposure A careful history should notonly include prescribed medications but also herbal remedies and food and beverage use (ie quinine intonic water alcohol use tahini) Chronic alcohol use is a common cause of thrombocytopenia Plateletcounts typically normalize with cessation of the causative agent Heparin-induced thrombocytopenia causesa significant drop in platelets but patients are paradoxically hypercoagulable due to platelet activation (seechapter 239 Thrombotics and Antithrombotics)
Nonimmune Causes of ThrombocytopeniaNonimmune Causes of Thrombocytopenia
Thrombocytopenia may occur from various nonndashimmune-mediated causes (Table 233-1) In thromboticthrombocytopenic purpura and hemolytic-uremic syndrome thrombotic microangiopathy occurs whenvessel injury results in deposition of platelet-fibrin thrombi (see chapters 143 Oncologic and HematologicEmergencies in Children and 237 Acquired Hemolytic Anemia) DIC is also a well-described cause ofplatelet destruction In patients with marked hemorrhage large-volume fluid resuscitation may lead to adilutional thrombocytopenia Additionally certain bacterial rickettsial and viral infections can cause directtoxic destruction of platelets Thrombocytopenia specific to pregnancy may be a result of the hemolysisndashelevated liver enzymesndashlow platelets (HELLP) syndrome pre-eclampsia or gestational thrombocytopenia(see chapter 100 Maternal Emergencies aer 20 Weeks of Pregnancy and in the Postpartum Period)Finally an enlarged spleen can sequester a significant portion of the platelet pool
Thrombocytopenia is present in up to 70 of patients with chronic liver disease15 The etiology appearsmultifactorial Patients oen have underlying medical conditions related to their liver disease such as alcoholuse viral hepatitis or nutritional deficiencies that impair platelet production Thrombopoietin which isproduced by hepatocytes may be decreased Portal hypertension may lead to splenic sequestrationEndotoxemia from infection may promote platelet aggregation Some patients also demonstrate plateletLoading [Contrib]a11yaccessibility-menujs
3272019
923
autoantibodies The degree of quantitative thrombocytopenia may be mitigated by an increased level ofcirculating von Willebrand factor that is typically seen which promotes platelet adhesion For this reasonroutine platelet transfusion is not recommended in the absence of clinically significant bleeding However a
platelet count of gt50000mm3 (gt50 times 109L) should be achieved prior to invasive procedures (ie lumbar
puncture surgery liver biopsy)16
FUNCTIONAL PLATELET DISORDERSFUNCTIONAL PLATELET DISORDERS
Several disease processes can cause acquired qualitative or functional abnormalities of platelets (Table 233-Table 233-
44)17 In the myeloproliferative diseases platelets are oen dysfunctional even if the platelet count is normalor elevated Patients can have prolonged bleeding times and clinically significant bleeding To control acute
bleeding transfusion should be considered to raise the level of normal platelets to 50000mm3 (50 times 109L)In macroglobulinemia and related disorders the elevated level of viscous proteins interferes with plateletfunction Patients with clinically significant bleeding may require plasmapheresis to reduce the protein leveland correct hemostatic function
TABLE 233-4
Clinical Conditions Associated with Qualitative Platelet AbnormalitiesClinical Conditions Associated with Qualitative Platelet Abnormalities
Uremia
Liver disease
Disseminated intravascular coagulation
Antiplatelet antibodies (immune thrombocytopenia systemic lupus erythematosus)
Cardiopulmonary bypass
Myeloproliferative disorders (thrombocytosis polycythemia vera chronic myeloid leukemia acute
lymphocytic or myelogenous leukemia)
Dysproteinemias (multiple myeloma Waldenstroumlms macroglobulinemia)
von Willebrands disease (congenital or acquired)
Many drugs can influence platelet function (Table 233-2 and Table 233-5Table 233-5) Of these the most commonly usedare aspirin which produces an irreversible impairment in platelet aggregation and the nonsteroidal anti-inflammatory drugs clopidogrel and ticlopidine which produce temporary impairment in platelet adhesionand aggregation (see chapter 239)
Loading [Contrib]a11yaccessibility-menujs
3272019
1023
TABLE 233-5
Duration of Antiplatelet ActivityDuration of Antiplatelet Activity
DrugDrug OnsetOnset Duration of EectDuration of Eect
Aspirin 1 h Up to 7 d
Most nonsteroidal anti-inflammatory drugs 1 h 1 d
Piroxicam 1 h 2 d
Ticlopidine or clopidogrel 1ndash2 d 4ndash7 d
Thrombocytosis a platelet count exceeding 500000mm3 (500 times 109L) can be seen in many disordersincluding inflammatory reactions malignancy polycythemia and postsplenectomy Platelet function can benormal or abnormal depending on the underlying condition Therefore thrombocytosis can be associatedwith bleeding (mucosal ecchymotic GI) or thromboembolic (deep venous thrombosis portal or mesentericthrombosis splenic vein thrombosis) manifestations However these events are unusual even with platelet
counts in excess of 1000000mm3 (1000 times 109L)
ACQUIRED COAGULATION DISORDERSACQUIRED COAGULATION DISORDERS
Acquired coagulation disorders can result from underlying medical disease and autoimmune factorinhibitors
LIVER DISEASELIVER DISEASE
Acute and chronic liver disease is commonly associated with laboratory tests of impaired coagulationHepatocytes synthesize all of the coagulation factors and related regulatory proteins with the exception offactor VIII and von Willebrand factor Diseases aecting the hepatic parenchyma may result in a decreasedsynthesis of these factors including the vitamin Kndashdependent carboxylation of factors II (prothrombin) VIIIX and X Because vitamin K is a fat-soluble vitamin malabsorption can occur with processes that interferewith the absorption of fat-soluble vitamins including impaired bile acid metabolism (ie primary biliarycirrhosis) intrahepatic or extrahepatic cholestasis and treatment with bile acid binders Thus prolongedprothrombin time is common in patients with decompensated hepatic function Despite markedprolongations of prothrombin time and activated partial thromboplastin time (PTT) seen in advanced liverdisease and cirrhosis these tests poorly predict onset and severity of bleeding including bleeding from
esophageal varices or invasive procedures or surgery16181920 Although there may be marked reduction inprocoagulant proteins in liver disease there is typically a parallel decrease in the endogenous anticoagulantLoading [Contrib]a11yaccessibility-menujs
3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
623
The CBC should demonstrate normal cell lines except for the platelets A mild anemia may be seen if bleedingis present The peripheral smear should show large well-granulated platelets although they will be few innumber Bone marrow biopsy is not indicated unless clinical features are atypical If the evaluation supportsthe diagnosis of primary ITP then additional testing in the ED is not required
Treatment for ITP is initiated based on the risk of bleeding (Table 233-3Table 233-3) Major bleeding complications in
patients with platelets gt50000 mm3 (gt50 times 109L) are uncommon As most fatal bleeding complications
occur when platelet counts fall below 30000mm3 (30 times 109L) experts and guidelines recommend this level
as the threshold for initiating treatment of ITP in adults5691011 Bleeding risk correlates with lower plateletcounts and patient age greater than 60 a prior history of bleeding certain chronic illnesses and use ofmedications that alter hemostasis all heighten this risk Therefore certain patients may benefit from medical
treatment despite a platelet count exceeding 30000mm3 (30 times 109L) For all patients with primary ITPbleeding risk should be minimized including avoiding use of antiplatelet medications when possiblemaintenance of good blood pressure control optimized treatment of exacerbating comorbid conditions (ieliver disease renal disease) and addressing fall risks
Loading [Contrib]a11yaccessibility-menujs
3272019
723
TABLE 233-3
Treatment of Immune ThrombocytopeniaTreatment of Immune Thrombocytopenia
Platelet
transfusionlt10000ndash20000mm3 (lt10ndash20 times 109L) prophylactically to prevent bleeding
lt50000mm3 (lt50 times 109L) if actively bleeding
lt20000ndash50000mm3 (lt20ndash50 times 109L) if patient requires diagnostic puncture
lt50000ndash100000mm3 (lt50ndash100 times 109L) if patient requires invasive procedure
Corticosteroids Prednisone 1 milligramkg PO per day for 21 days then tapered or dexamethasone 20
milligramsm2 IV per day for 4 d
IV
immunoglobulin
1 gramkg IV per day for 3 d
Splenectomy Considered for refractory cases
About two thirds of children with primary ITP will have spontaneous resolution within 6 months of
diagnosis11 An antecedent viral infection is commonly reported Additionally the measles-mumps-rubellavaccination has been associated with the development of acute ITP although this is rare and occurs in less
than 1 per 25000 doses given12 The risk of severe bleeding complications appears to be rare in children
regardless of their absolute platelet count5813 Children without signs of active bleeding and goodpsychosocial support typically do not require hospitalization or medical treatment Good anticipatoryguidance should be provided to the family and the child should abstain from contact sports or activities thatmight place them at risk for head injury
First-line treatment for primary ITP generally includes corticosteroids typically prednisone 1 milligramkg
per day for 4 weeks (shorter courses may be considered for children)59101113 Initial response may not beseen for 4 to 14 days and peak eect can be expected between 7 and 28 days IV immunoglobulin may alsobe considered either alone or in combination with corticosteroids at a dose 1 gkgper day for 3 days Initialresponse to IV immunoglobulin is more rapid than corticosteroids occurring between 1 and 3 days withpeak eect seen between 2 and 7 days Side eects of IV immunoglobulin may include aseptic meningitistransient neutropenia acute kidney injury and transfusion reactionshypotension
Anti-Rho(D) immunoglobulin at 50 to 75 microgramskg for a single dose may also be considered as a first-
line treatment strategy in patients who are Rh(D) positive and have not undergone splenectomy14 Initialresponse rate and peak eect are similar to that seen with IV immunoglobulin Mild hemolysis can beexpected and rare serious or even fatal cases of intravascular hemolysis DIC and renal failure have beenreported with anti-Rho(D) use prompting the US Food and Drug Administration to administer a warningLoading [Contrib]a11yaccessibility-menujs
3272019
823
pertaining to its use in 2010 Second-line treatment modalities include splenectomy and use of neweragents such as the monoclonal antibody rituximab which blunts the autoimmune destruction of plateletsand thrombopoietin receptor agonists which stimulate platelet production (ie romiplostin eltrombopag)
In the event of life-threatening hemorrhage where hemostasis must be achieved rapidly IV corticosteroids
(such as dexamethasone) and IV immunoglobulin should be administered concomitantly13 Platelettransfusions should be initiated and doses two to three times the typical dose might be required due to
persistent autoimmune destruction6 Platelet transfusions may need to be repeated frequently until bleedingsubsides or targeted treatment modalities take eect Emergent splenectomy may be considered if all othertreatment options are exhausted
Drug-Induced Immune ThrombocytopeniaDrug-Induced Immune Thrombocytopenia
Over 200 drugs have been implicated in causing immune-mediated suppression of platelet production or
increased platelet destruction (Table 233-2)34 The clinical presentation is similar to ITP and thethrombocytopenia may severe Drug-induced thrombocytopenia typically occurs 5 to 14 days followinginitiation of a drug but may occur sooner if there has been recent prior exposure A careful history should notonly include prescribed medications but also herbal remedies and food and beverage use (ie quinine intonic water alcohol use tahini) Chronic alcohol use is a common cause of thrombocytopenia Plateletcounts typically normalize with cessation of the causative agent Heparin-induced thrombocytopenia causesa significant drop in platelets but patients are paradoxically hypercoagulable due to platelet activation (seechapter 239 Thrombotics and Antithrombotics)
Nonimmune Causes of ThrombocytopeniaNonimmune Causes of Thrombocytopenia
Thrombocytopenia may occur from various nonndashimmune-mediated causes (Table 233-1) In thromboticthrombocytopenic purpura and hemolytic-uremic syndrome thrombotic microangiopathy occurs whenvessel injury results in deposition of platelet-fibrin thrombi (see chapters 143 Oncologic and HematologicEmergencies in Children and 237 Acquired Hemolytic Anemia) DIC is also a well-described cause ofplatelet destruction In patients with marked hemorrhage large-volume fluid resuscitation may lead to adilutional thrombocytopenia Additionally certain bacterial rickettsial and viral infections can cause directtoxic destruction of platelets Thrombocytopenia specific to pregnancy may be a result of the hemolysisndashelevated liver enzymesndashlow platelets (HELLP) syndrome pre-eclampsia or gestational thrombocytopenia(see chapter 100 Maternal Emergencies aer 20 Weeks of Pregnancy and in the Postpartum Period)Finally an enlarged spleen can sequester a significant portion of the platelet pool
Thrombocytopenia is present in up to 70 of patients with chronic liver disease15 The etiology appearsmultifactorial Patients oen have underlying medical conditions related to their liver disease such as alcoholuse viral hepatitis or nutritional deficiencies that impair platelet production Thrombopoietin which isproduced by hepatocytes may be decreased Portal hypertension may lead to splenic sequestrationEndotoxemia from infection may promote platelet aggregation Some patients also demonstrate plateletLoading [Contrib]a11yaccessibility-menujs
3272019
923
autoantibodies The degree of quantitative thrombocytopenia may be mitigated by an increased level ofcirculating von Willebrand factor that is typically seen which promotes platelet adhesion For this reasonroutine platelet transfusion is not recommended in the absence of clinically significant bleeding However a
platelet count of gt50000mm3 (gt50 times 109L) should be achieved prior to invasive procedures (ie lumbar
puncture surgery liver biopsy)16
FUNCTIONAL PLATELET DISORDERSFUNCTIONAL PLATELET DISORDERS
Several disease processes can cause acquired qualitative or functional abnormalities of platelets (Table 233-Table 233-
44)17 In the myeloproliferative diseases platelets are oen dysfunctional even if the platelet count is normalor elevated Patients can have prolonged bleeding times and clinically significant bleeding To control acute
bleeding transfusion should be considered to raise the level of normal platelets to 50000mm3 (50 times 109L)In macroglobulinemia and related disorders the elevated level of viscous proteins interferes with plateletfunction Patients with clinically significant bleeding may require plasmapheresis to reduce the protein leveland correct hemostatic function
TABLE 233-4
Clinical Conditions Associated with Qualitative Platelet AbnormalitiesClinical Conditions Associated with Qualitative Platelet Abnormalities
Uremia
Liver disease
Disseminated intravascular coagulation
Antiplatelet antibodies (immune thrombocytopenia systemic lupus erythematosus)
Cardiopulmonary bypass
Myeloproliferative disorders (thrombocytosis polycythemia vera chronic myeloid leukemia acute
lymphocytic or myelogenous leukemia)
Dysproteinemias (multiple myeloma Waldenstroumlms macroglobulinemia)
von Willebrands disease (congenital or acquired)
Many drugs can influence platelet function (Table 233-2 and Table 233-5Table 233-5) Of these the most commonly usedare aspirin which produces an irreversible impairment in platelet aggregation and the nonsteroidal anti-inflammatory drugs clopidogrel and ticlopidine which produce temporary impairment in platelet adhesionand aggregation (see chapter 239)
Loading [Contrib]a11yaccessibility-menujs
3272019
1023
TABLE 233-5
Duration of Antiplatelet ActivityDuration of Antiplatelet Activity
DrugDrug OnsetOnset Duration of EectDuration of Eect
Aspirin 1 h Up to 7 d
Most nonsteroidal anti-inflammatory drugs 1 h 1 d
Piroxicam 1 h 2 d
Ticlopidine or clopidogrel 1ndash2 d 4ndash7 d
Thrombocytosis a platelet count exceeding 500000mm3 (500 times 109L) can be seen in many disordersincluding inflammatory reactions malignancy polycythemia and postsplenectomy Platelet function can benormal or abnormal depending on the underlying condition Therefore thrombocytosis can be associatedwith bleeding (mucosal ecchymotic GI) or thromboembolic (deep venous thrombosis portal or mesentericthrombosis splenic vein thrombosis) manifestations However these events are unusual even with platelet
counts in excess of 1000000mm3 (1000 times 109L)
ACQUIRED COAGULATION DISORDERSACQUIRED COAGULATION DISORDERS
Acquired coagulation disorders can result from underlying medical disease and autoimmune factorinhibitors
LIVER DISEASELIVER DISEASE
Acute and chronic liver disease is commonly associated with laboratory tests of impaired coagulationHepatocytes synthesize all of the coagulation factors and related regulatory proteins with the exception offactor VIII and von Willebrand factor Diseases aecting the hepatic parenchyma may result in a decreasedsynthesis of these factors including the vitamin Kndashdependent carboxylation of factors II (prothrombin) VIIIX and X Because vitamin K is a fat-soluble vitamin malabsorption can occur with processes that interferewith the absorption of fat-soluble vitamins including impaired bile acid metabolism (ie primary biliarycirrhosis) intrahepatic or extrahepatic cholestasis and treatment with bile acid binders Thus prolongedprothrombin time is common in patients with decompensated hepatic function Despite markedprolongations of prothrombin time and activated partial thromboplastin time (PTT) seen in advanced liverdisease and cirrhosis these tests poorly predict onset and severity of bleeding including bleeding from
esophageal varices or invasive procedures or surgery16181920 Although there may be marked reduction inprocoagulant proteins in liver disease there is typically a parallel decrease in the endogenous anticoagulantLoading [Contrib]a11yaccessibility-menujs
3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
723
TABLE 233-3
Treatment of Immune ThrombocytopeniaTreatment of Immune Thrombocytopenia
Platelet
transfusionlt10000ndash20000mm3 (lt10ndash20 times 109L) prophylactically to prevent bleeding
lt50000mm3 (lt50 times 109L) if actively bleeding
lt20000ndash50000mm3 (lt20ndash50 times 109L) if patient requires diagnostic puncture
lt50000ndash100000mm3 (lt50ndash100 times 109L) if patient requires invasive procedure
Corticosteroids Prednisone 1 milligramkg PO per day for 21 days then tapered or dexamethasone 20
milligramsm2 IV per day for 4 d
IV
immunoglobulin
1 gramkg IV per day for 3 d
Splenectomy Considered for refractory cases
About two thirds of children with primary ITP will have spontaneous resolution within 6 months of
diagnosis11 An antecedent viral infection is commonly reported Additionally the measles-mumps-rubellavaccination has been associated with the development of acute ITP although this is rare and occurs in less
than 1 per 25000 doses given12 The risk of severe bleeding complications appears to be rare in children
regardless of their absolute platelet count5813 Children without signs of active bleeding and goodpsychosocial support typically do not require hospitalization or medical treatment Good anticipatoryguidance should be provided to the family and the child should abstain from contact sports or activities thatmight place them at risk for head injury
First-line treatment for primary ITP generally includes corticosteroids typically prednisone 1 milligramkg
per day for 4 weeks (shorter courses may be considered for children)59101113 Initial response may not beseen for 4 to 14 days and peak eect can be expected between 7 and 28 days IV immunoglobulin may alsobe considered either alone or in combination with corticosteroids at a dose 1 gkgper day for 3 days Initialresponse to IV immunoglobulin is more rapid than corticosteroids occurring between 1 and 3 days withpeak eect seen between 2 and 7 days Side eects of IV immunoglobulin may include aseptic meningitistransient neutropenia acute kidney injury and transfusion reactionshypotension
Anti-Rho(D) immunoglobulin at 50 to 75 microgramskg for a single dose may also be considered as a first-
line treatment strategy in patients who are Rh(D) positive and have not undergone splenectomy14 Initialresponse rate and peak eect are similar to that seen with IV immunoglobulin Mild hemolysis can beexpected and rare serious or even fatal cases of intravascular hemolysis DIC and renal failure have beenreported with anti-Rho(D) use prompting the US Food and Drug Administration to administer a warningLoading [Contrib]a11yaccessibility-menujs
3272019
823
pertaining to its use in 2010 Second-line treatment modalities include splenectomy and use of neweragents such as the monoclonal antibody rituximab which blunts the autoimmune destruction of plateletsand thrombopoietin receptor agonists which stimulate platelet production (ie romiplostin eltrombopag)
In the event of life-threatening hemorrhage where hemostasis must be achieved rapidly IV corticosteroids
(such as dexamethasone) and IV immunoglobulin should be administered concomitantly13 Platelettransfusions should be initiated and doses two to three times the typical dose might be required due to
persistent autoimmune destruction6 Platelet transfusions may need to be repeated frequently until bleedingsubsides or targeted treatment modalities take eect Emergent splenectomy may be considered if all othertreatment options are exhausted
Drug-Induced Immune ThrombocytopeniaDrug-Induced Immune Thrombocytopenia
Over 200 drugs have been implicated in causing immune-mediated suppression of platelet production or
increased platelet destruction (Table 233-2)34 The clinical presentation is similar to ITP and thethrombocytopenia may severe Drug-induced thrombocytopenia typically occurs 5 to 14 days followinginitiation of a drug but may occur sooner if there has been recent prior exposure A careful history should notonly include prescribed medications but also herbal remedies and food and beverage use (ie quinine intonic water alcohol use tahini) Chronic alcohol use is a common cause of thrombocytopenia Plateletcounts typically normalize with cessation of the causative agent Heparin-induced thrombocytopenia causesa significant drop in platelets but patients are paradoxically hypercoagulable due to platelet activation (seechapter 239 Thrombotics and Antithrombotics)
Nonimmune Causes of ThrombocytopeniaNonimmune Causes of Thrombocytopenia
Thrombocytopenia may occur from various nonndashimmune-mediated causes (Table 233-1) In thromboticthrombocytopenic purpura and hemolytic-uremic syndrome thrombotic microangiopathy occurs whenvessel injury results in deposition of platelet-fibrin thrombi (see chapters 143 Oncologic and HematologicEmergencies in Children and 237 Acquired Hemolytic Anemia) DIC is also a well-described cause ofplatelet destruction In patients with marked hemorrhage large-volume fluid resuscitation may lead to adilutional thrombocytopenia Additionally certain bacterial rickettsial and viral infections can cause directtoxic destruction of platelets Thrombocytopenia specific to pregnancy may be a result of the hemolysisndashelevated liver enzymesndashlow platelets (HELLP) syndrome pre-eclampsia or gestational thrombocytopenia(see chapter 100 Maternal Emergencies aer 20 Weeks of Pregnancy and in the Postpartum Period)Finally an enlarged spleen can sequester a significant portion of the platelet pool
Thrombocytopenia is present in up to 70 of patients with chronic liver disease15 The etiology appearsmultifactorial Patients oen have underlying medical conditions related to their liver disease such as alcoholuse viral hepatitis or nutritional deficiencies that impair platelet production Thrombopoietin which isproduced by hepatocytes may be decreased Portal hypertension may lead to splenic sequestrationEndotoxemia from infection may promote platelet aggregation Some patients also demonstrate plateletLoading [Contrib]a11yaccessibility-menujs
3272019
923
autoantibodies The degree of quantitative thrombocytopenia may be mitigated by an increased level ofcirculating von Willebrand factor that is typically seen which promotes platelet adhesion For this reasonroutine platelet transfusion is not recommended in the absence of clinically significant bleeding However a
platelet count of gt50000mm3 (gt50 times 109L) should be achieved prior to invasive procedures (ie lumbar
puncture surgery liver biopsy)16
FUNCTIONAL PLATELET DISORDERSFUNCTIONAL PLATELET DISORDERS
Several disease processes can cause acquired qualitative or functional abnormalities of platelets (Table 233-Table 233-
44)17 In the myeloproliferative diseases platelets are oen dysfunctional even if the platelet count is normalor elevated Patients can have prolonged bleeding times and clinically significant bleeding To control acute
bleeding transfusion should be considered to raise the level of normal platelets to 50000mm3 (50 times 109L)In macroglobulinemia and related disorders the elevated level of viscous proteins interferes with plateletfunction Patients with clinically significant bleeding may require plasmapheresis to reduce the protein leveland correct hemostatic function
TABLE 233-4
Clinical Conditions Associated with Qualitative Platelet AbnormalitiesClinical Conditions Associated with Qualitative Platelet Abnormalities
Uremia
Liver disease
Disseminated intravascular coagulation
Antiplatelet antibodies (immune thrombocytopenia systemic lupus erythematosus)
Cardiopulmonary bypass
Myeloproliferative disorders (thrombocytosis polycythemia vera chronic myeloid leukemia acute
lymphocytic or myelogenous leukemia)
Dysproteinemias (multiple myeloma Waldenstroumlms macroglobulinemia)
von Willebrands disease (congenital or acquired)
Many drugs can influence platelet function (Table 233-2 and Table 233-5Table 233-5) Of these the most commonly usedare aspirin which produces an irreversible impairment in platelet aggregation and the nonsteroidal anti-inflammatory drugs clopidogrel and ticlopidine which produce temporary impairment in platelet adhesionand aggregation (see chapter 239)
Loading [Contrib]a11yaccessibility-menujs
3272019
1023
TABLE 233-5
Duration of Antiplatelet ActivityDuration of Antiplatelet Activity
DrugDrug OnsetOnset Duration of EectDuration of Eect
Aspirin 1 h Up to 7 d
Most nonsteroidal anti-inflammatory drugs 1 h 1 d
Piroxicam 1 h 2 d
Ticlopidine or clopidogrel 1ndash2 d 4ndash7 d
Thrombocytosis a platelet count exceeding 500000mm3 (500 times 109L) can be seen in many disordersincluding inflammatory reactions malignancy polycythemia and postsplenectomy Platelet function can benormal or abnormal depending on the underlying condition Therefore thrombocytosis can be associatedwith bleeding (mucosal ecchymotic GI) or thromboembolic (deep venous thrombosis portal or mesentericthrombosis splenic vein thrombosis) manifestations However these events are unusual even with platelet
counts in excess of 1000000mm3 (1000 times 109L)
ACQUIRED COAGULATION DISORDERSACQUIRED COAGULATION DISORDERS
Acquired coagulation disorders can result from underlying medical disease and autoimmune factorinhibitors
LIVER DISEASELIVER DISEASE
Acute and chronic liver disease is commonly associated with laboratory tests of impaired coagulationHepatocytes synthesize all of the coagulation factors and related regulatory proteins with the exception offactor VIII and von Willebrand factor Diseases aecting the hepatic parenchyma may result in a decreasedsynthesis of these factors including the vitamin Kndashdependent carboxylation of factors II (prothrombin) VIIIX and X Because vitamin K is a fat-soluble vitamin malabsorption can occur with processes that interferewith the absorption of fat-soluble vitamins including impaired bile acid metabolism (ie primary biliarycirrhosis) intrahepatic or extrahepatic cholestasis and treatment with bile acid binders Thus prolongedprothrombin time is common in patients with decompensated hepatic function Despite markedprolongations of prothrombin time and activated partial thromboplastin time (PTT) seen in advanced liverdisease and cirrhosis these tests poorly predict onset and severity of bleeding including bleeding from
esophageal varices or invasive procedures or surgery16181920 Although there may be marked reduction inprocoagulant proteins in liver disease there is typically a parallel decrease in the endogenous anticoagulantLoading [Contrib]a11yaccessibility-menujs
3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
823
pertaining to its use in 2010 Second-line treatment modalities include splenectomy and use of neweragents such as the monoclonal antibody rituximab which blunts the autoimmune destruction of plateletsand thrombopoietin receptor agonists which stimulate platelet production (ie romiplostin eltrombopag)
In the event of life-threatening hemorrhage where hemostasis must be achieved rapidly IV corticosteroids
(such as dexamethasone) and IV immunoglobulin should be administered concomitantly13 Platelettransfusions should be initiated and doses two to three times the typical dose might be required due to
persistent autoimmune destruction6 Platelet transfusions may need to be repeated frequently until bleedingsubsides or targeted treatment modalities take eect Emergent splenectomy may be considered if all othertreatment options are exhausted
Drug-Induced Immune ThrombocytopeniaDrug-Induced Immune Thrombocytopenia
Over 200 drugs have been implicated in causing immune-mediated suppression of platelet production or
increased platelet destruction (Table 233-2)34 The clinical presentation is similar to ITP and thethrombocytopenia may severe Drug-induced thrombocytopenia typically occurs 5 to 14 days followinginitiation of a drug but may occur sooner if there has been recent prior exposure A careful history should notonly include prescribed medications but also herbal remedies and food and beverage use (ie quinine intonic water alcohol use tahini) Chronic alcohol use is a common cause of thrombocytopenia Plateletcounts typically normalize with cessation of the causative agent Heparin-induced thrombocytopenia causesa significant drop in platelets but patients are paradoxically hypercoagulable due to platelet activation (seechapter 239 Thrombotics and Antithrombotics)
Nonimmune Causes of ThrombocytopeniaNonimmune Causes of Thrombocytopenia
Thrombocytopenia may occur from various nonndashimmune-mediated causes (Table 233-1) In thromboticthrombocytopenic purpura and hemolytic-uremic syndrome thrombotic microangiopathy occurs whenvessel injury results in deposition of platelet-fibrin thrombi (see chapters 143 Oncologic and HematologicEmergencies in Children and 237 Acquired Hemolytic Anemia) DIC is also a well-described cause ofplatelet destruction In patients with marked hemorrhage large-volume fluid resuscitation may lead to adilutional thrombocytopenia Additionally certain bacterial rickettsial and viral infections can cause directtoxic destruction of platelets Thrombocytopenia specific to pregnancy may be a result of the hemolysisndashelevated liver enzymesndashlow platelets (HELLP) syndrome pre-eclampsia or gestational thrombocytopenia(see chapter 100 Maternal Emergencies aer 20 Weeks of Pregnancy and in the Postpartum Period)Finally an enlarged spleen can sequester a significant portion of the platelet pool
Thrombocytopenia is present in up to 70 of patients with chronic liver disease15 The etiology appearsmultifactorial Patients oen have underlying medical conditions related to their liver disease such as alcoholuse viral hepatitis or nutritional deficiencies that impair platelet production Thrombopoietin which isproduced by hepatocytes may be decreased Portal hypertension may lead to splenic sequestrationEndotoxemia from infection may promote platelet aggregation Some patients also demonstrate plateletLoading [Contrib]a11yaccessibility-menujs
3272019
923
autoantibodies The degree of quantitative thrombocytopenia may be mitigated by an increased level ofcirculating von Willebrand factor that is typically seen which promotes platelet adhesion For this reasonroutine platelet transfusion is not recommended in the absence of clinically significant bleeding However a
platelet count of gt50000mm3 (gt50 times 109L) should be achieved prior to invasive procedures (ie lumbar
puncture surgery liver biopsy)16
FUNCTIONAL PLATELET DISORDERSFUNCTIONAL PLATELET DISORDERS
Several disease processes can cause acquired qualitative or functional abnormalities of platelets (Table 233-Table 233-
44)17 In the myeloproliferative diseases platelets are oen dysfunctional even if the platelet count is normalor elevated Patients can have prolonged bleeding times and clinically significant bleeding To control acute
bleeding transfusion should be considered to raise the level of normal platelets to 50000mm3 (50 times 109L)In macroglobulinemia and related disorders the elevated level of viscous proteins interferes with plateletfunction Patients with clinically significant bleeding may require plasmapheresis to reduce the protein leveland correct hemostatic function
TABLE 233-4
Clinical Conditions Associated with Qualitative Platelet AbnormalitiesClinical Conditions Associated with Qualitative Platelet Abnormalities
Uremia
Liver disease
Disseminated intravascular coagulation
Antiplatelet antibodies (immune thrombocytopenia systemic lupus erythematosus)
Cardiopulmonary bypass
Myeloproliferative disorders (thrombocytosis polycythemia vera chronic myeloid leukemia acute
lymphocytic or myelogenous leukemia)
Dysproteinemias (multiple myeloma Waldenstroumlms macroglobulinemia)
von Willebrands disease (congenital or acquired)
Many drugs can influence platelet function (Table 233-2 and Table 233-5Table 233-5) Of these the most commonly usedare aspirin which produces an irreversible impairment in platelet aggregation and the nonsteroidal anti-inflammatory drugs clopidogrel and ticlopidine which produce temporary impairment in platelet adhesionand aggregation (see chapter 239)
Loading [Contrib]a11yaccessibility-menujs
3272019
1023
TABLE 233-5
Duration of Antiplatelet ActivityDuration of Antiplatelet Activity
DrugDrug OnsetOnset Duration of EectDuration of Eect
Aspirin 1 h Up to 7 d
Most nonsteroidal anti-inflammatory drugs 1 h 1 d
Piroxicam 1 h 2 d
Ticlopidine or clopidogrel 1ndash2 d 4ndash7 d
Thrombocytosis a platelet count exceeding 500000mm3 (500 times 109L) can be seen in many disordersincluding inflammatory reactions malignancy polycythemia and postsplenectomy Platelet function can benormal or abnormal depending on the underlying condition Therefore thrombocytosis can be associatedwith bleeding (mucosal ecchymotic GI) or thromboembolic (deep venous thrombosis portal or mesentericthrombosis splenic vein thrombosis) manifestations However these events are unusual even with platelet
counts in excess of 1000000mm3 (1000 times 109L)
ACQUIRED COAGULATION DISORDERSACQUIRED COAGULATION DISORDERS
Acquired coagulation disorders can result from underlying medical disease and autoimmune factorinhibitors
LIVER DISEASELIVER DISEASE
Acute and chronic liver disease is commonly associated with laboratory tests of impaired coagulationHepatocytes synthesize all of the coagulation factors and related regulatory proteins with the exception offactor VIII and von Willebrand factor Diseases aecting the hepatic parenchyma may result in a decreasedsynthesis of these factors including the vitamin Kndashdependent carboxylation of factors II (prothrombin) VIIIX and X Because vitamin K is a fat-soluble vitamin malabsorption can occur with processes that interferewith the absorption of fat-soluble vitamins including impaired bile acid metabolism (ie primary biliarycirrhosis) intrahepatic or extrahepatic cholestasis and treatment with bile acid binders Thus prolongedprothrombin time is common in patients with decompensated hepatic function Despite markedprolongations of prothrombin time and activated partial thromboplastin time (PTT) seen in advanced liverdisease and cirrhosis these tests poorly predict onset and severity of bleeding including bleeding from
esophageal varices or invasive procedures or surgery16181920 Although there may be marked reduction inprocoagulant proteins in liver disease there is typically a parallel decrease in the endogenous anticoagulantLoading [Contrib]a11yaccessibility-menujs
3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
923
autoantibodies The degree of quantitative thrombocytopenia may be mitigated by an increased level ofcirculating von Willebrand factor that is typically seen which promotes platelet adhesion For this reasonroutine platelet transfusion is not recommended in the absence of clinically significant bleeding However a
platelet count of gt50000mm3 (gt50 times 109L) should be achieved prior to invasive procedures (ie lumbar
puncture surgery liver biopsy)16
FUNCTIONAL PLATELET DISORDERSFUNCTIONAL PLATELET DISORDERS
Several disease processes can cause acquired qualitative or functional abnormalities of platelets (Table 233-Table 233-
44)17 In the myeloproliferative diseases platelets are oen dysfunctional even if the platelet count is normalor elevated Patients can have prolonged bleeding times and clinically significant bleeding To control acute
bleeding transfusion should be considered to raise the level of normal platelets to 50000mm3 (50 times 109L)In macroglobulinemia and related disorders the elevated level of viscous proteins interferes with plateletfunction Patients with clinically significant bleeding may require plasmapheresis to reduce the protein leveland correct hemostatic function
TABLE 233-4
Clinical Conditions Associated with Qualitative Platelet AbnormalitiesClinical Conditions Associated with Qualitative Platelet Abnormalities
Uremia
Liver disease
Disseminated intravascular coagulation
Antiplatelet antibodies (immune thrombocytopenia systemic lupus erythematosus)
Cardiopulmonary bypass
Myeloproliferative disorders (thrombocytosis polycythemia vera chronic myeloid leukemia acute
lymphocytic or myelogenous leukemia)
Dysproteinemias (multiple myeloma Waldenstroumlms macroglobulinemia)
von Willebrands disease (congenital or acquired)
Many drugs can influence platelet function (Table 233-2 and Table 233-5Table 233-5) Of these the most commonly usedare aspirin which produces an irreversible impairment in platelet aggregation and the nonsteroidal anti-inflammatory drugs clopidogrel and ticlopidine which produce temporary impairment in platelet adhesionand aggregation (see chapter 239)
Loading [Contrib]a11yaccessibility-menujs
3272019
1023
TABLE 233-5
Duration of Antiplatelet ActivityDuration of Antiplatelet Activity
DrugDrug OnsetOnset Duration of EectDuration of Eect
Aspirin 1 h Up to 7 d
Most nonsteroidal anti-inflammatory drugs 1 h 1 d
Piroxicam 1 h 2 d
Ticlopidine or clopidogrel 1ndash2 d 4ndash7 d
Thrombocytosis a platelet count exceeding 500000mm3 (500 times 109L) can be seen in many disordersincluding inflammatory reactions malignancy polycythemia and postsplenectomy Platelet function can benormal or abnormal depending on the underlying condition Therefore thrombocytosis can be associatedwith bleeding (mucosal ecchymotic GI) or thromboembolic (deep venous thrombosis portal or mesentericthrombosis splenic vein thrombosis) manifestations However these events are unusual even with platelet
counts in excess of 1000000mm3 (1000 times 109L)
ACQUIRED COAGULATION DISORDERSACQUIRED COAGULATION DISORDERS
Acquired coagulation disorders can result from underlying medical disease and autoimmune factorinhibitors
LIVER DISEASELIVER DISEASE
Acute and chronic liver disease is commonly associated with laboratory tests of impaired coagulationHepatocytes synthesize all of the coagulation factors and related regulatory proteins with the exception offactor VIII and von Willebrand factor Diseases aecting the hepatic parenchyma may result in a decreasedsynthesis of these factors including the vitamin Kndashdependent carboxylation of factors II (prothrombin) VIIIX and X Because vitamin K is a fat-soluble vitamin malabsorption can occur with processes that interferewith the absorption of fat-soluble vitamins including impaired bile acid metabolism (ie primary biliarycirrhosis) intrahepatic or extrahepatic cholestasis and treatment with bile acid binders Thus prolongedprothrombin time is common in patients with decompensated hepatic function Despite markedprolongations of prothrombin time and activated partial thromboplastin time (PTT) seen in advanced liverdisease and cirrhosis these tests poorly predict onset and severity of bleeding including bleeding from
esophageal varices or invasive procedures or surgery16181920 Although there may be marked reduction inprocoagulant proteins in liver disease there is typically a parallel decrease in the endogenous anticoagulantLoading [Contrib]a11yaccessibility-menujs
3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
1023
TABLE 233-5
Duration of Antiplatelet ActivityDuration of Antiplatelet Activity
DrugDrug OnsetOnset Duration of EectDuration of Eect
Aspirin 1 h Up to 7 d
Most nonsteroidal anti-inflammatory drugs 1 h 1 d
Piroxicam 1 h 2 d
Ticlopidine or clopidogrel 1ndash2 d 4ndash7 d
Thrombocytosis a platelet count exceeding 500000mm3 (500 times 109L) can be seen in many disordersincluding inflammatory reactions malignancy polycythemia and postsplenectomy Platelet function can benormal or abnormal depending on the underlying condition Therefore thrombocytosis can be associatedwith bleeding (mucosal ecchymotic GI) or thromboembolic (deep venous thrombosis portal or mesentericthrombosis splenic vein thrombosis) manifestations However these events are unusual even with platelet
counts in excess of 1000000mm3 (1000 times 109L)
ACQUIRED COAGULATION DISORDERSACQUIRED COAGULATION DISORDERS
Acquired coagulation disorders can result from underlying medical disease and autoimmune factorinhibitors
LIVER DISEASELIVER DISEASE
Acute and chronic liver disease is commonly associated with laboratory tests of impaired coagulationHepatocytes synthesize all of the coagulation factors and related regulatory proteins with the exception offactor VIII and von Willebrand factor Diseases aecting the hepatic parenchyma may result in a decreasedsynthesis of these factors including the vitamin Kndashdependent carboxylation of factors II (prothrombin) VIIIX and X Because vitamin K is a fat-soluble vitamin malabsorption can occur with processes that interferewith the absorption of fat-soluble vitamins including impaired bile acid metabolism (ie primary biliarycirrhosis) intrahepatic or extrahepatic cholestasis and treatment with bile acid binders Thus prolongedprothrombin time is common in patients with decompensated hepatic function Despite markedprolongations of prothrombin time and activated partial thromboplastin time (PTT) seen in advanced liverdisease and cirrhosis these tests poorly predict onset and severity of bleeding including bleeding from
esophageal varices or invasive procedures or surgery16181920 Although there may be marked reduction inprocoagulant proteins in liver disease there is typically a parallel decrease in the endogenous anticoagulantLoading [Contrib]a11yaccessibility-menujs
3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
1123
proteins such as protein C and antithrombin Therefore primary hemostasis may be relatively maintained Infact patients with liver disease may be susceptible to both increased bleeding and thrombosis Patients withliver disease and cirrhosis are twice as likely to develop unprovoked deep venous thrombosis and have a
relatively high incidence of portal venous thrombosis21
In the actively bleeding patient with liver disease attention to volume and circulatory status is paramountTransfusion of packed red blood cells should be used to maintain an adequate hemoglobin andhemodynamic stability Fresh frozen plasma transfusions or platelets should be transfused if significanthemorrhage (eg from esophageal varices) is associated with a coagulopathy or thrombocytopenia with a
platelet count below 60000mm3 (60 times 109L)16 Plasma transfusions should be used cautiously becausethey may incite thrombosis and expand intravascular volume exacerbating portal hypertension andincreasing the severity of variceal bleeding There is no evidence that recombinant activated factor VII or
four-factor prothrombin complex concentrate (Kcentrareg) provides benefit22 The benefit of vitamin K in these
patients has also been called into question and its routine use is not substantiated2223
Primary prevention of bleeding in patients with liver disease should focus on medical optimization of their
risk factors rather than treatment of abnormal tests of coagulation or thrombocytopenia1618 These includemanagement and prevention of portal hypertension treatment of esophageal varices management ofprimary causes for liver disease (ie alcohol use hepatitis C) optimization of renal function andmanagement and prevention of sepsisinfection
RENAL DISEASERENAL DISEASE
Patients with renal disease frequently manifest disorders of hemostasis Early renal impairment has beenassociated with a tendency for thrombosis relating to increased production of procoagulant factors as well as
decreased formation of tissue plasminogen activator24 In advanced renal disease bleeding complicationsare of particular concern due to qualitative platelet dysfunction from decreased ability to adhere to damagedendothelium and aggregate Patients with chronic kidney disease are at increased risk for minor bleeding(mucosal and cutaneous) and major bleeding (intracerebral and GI hemorrhage) Serum prothrombin timeactivated PTT and platelet counts are oen normal although bleeding time will usually be prolongedAbnormalities in platelet function can be due to direct eects of uremic toxins and impaired drugelimination Anemia itself has been associated with platelet dysfunction Thrombocytopenia can occur fromdialysis and the heparin used may also potentiate bleeding
Desmopressin is the most common agent used to correct bleeding in patients with uremic plateletdysfunction producing an increase in serum von Willebrand factor and enhancing the platelets ability to
aggregate25 The dose is 03 milligramkg SC or IV with a rapid onset and duration of action lasting at least 4hours Side eects are generally mild and include headache flushing minor hypotension tachycardianausea abdominal cramps and local site reaction Other strategies that improve platelet function includethe use of cryoprecipitate conjugated estrogens erythropoietin to improve anemia and hemodialysis to
Loading [Contrib]a11yaccessibility-menujs
3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
1223
remove toxins24 Platelet transfusions alone are generally ineective because the infused platelets quicklyacquire the platelet defect Cryoprecipitate and platelet transfusions should be reserved for life-threateningbleeding and should be used in combination with packed red blood cells desmopressin and conjugatedestrogens
DISSEMINATED INTRAVASCULAR COAGULATIONDISSEMINATED INTRAVASCULAR COAGULATION
DIC is an acquired syndrome characterized by inappropriate and widespread activation of the coagulationsystem resulting in intravascular thrombin generation small vessel thrombosis and consumption of clotting
factors and platelets26 Concomitant activation of the fibrinolytic system also occurs resulting in thebreakdown of fibrin clots and subsequent bleeding DIC is associated with a wide variety of precipitatingdisorders (Table 233-6Table 233-6)
Loading [Contrib]a11yaccessibility-menujs
3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
1323
TABLE 233-6
Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)Common Conditions Associated with Disseminated Intravascular Coagulation (DIC)
Clinical SettingClinical Setting CommentsComments
Infection
Bacterial
Viral
Fungal
Probably the most common cause of DIC 10ndash20 of patients with gram-negative
sepsis have DIC endotoxins stimulate monocytes and endothelial cells to express tissue
factor Rocky Mountain spotted fever causes direct endothelial damage DIC more likely
to develop in asplenic patients or cirrhosis septic patients are more likely to have
thrombosis than bleeding
Carcinoma
Adenocarcinoma
Lymphoma
Malignant cells may cause endothelial damage and allow the expression of tissue factor
as well as other procoagulant materials most adenocarcinomas tend to have thrombosis
(Trousseaus syndrome) whereas prostate cancer tends to have more bleeding DIC is
oen chronic and compensated
Acute leukemia DIC most common with promyelocytic leukemia blast cells release procoagulant
enzymes there is excessive release at time of cell lysis (chemotherapy) more likely to
have bleeding than thrombosis
Trauma DIC especially with brain injury crush injury burns hypothermia hyperthermia
rhabdomyolysis fat embolism hypoxia Massive bleeding can occur
Organ injury
Liver disease
Pancreatitis
May have chronic compensated DIC acute DIC may occur in the setting of acute hepatic
failure tissue factor is released from the injured hepatocytes Pancreatitis can activate
the coagulation cascade
Pregnancy Placental abruption amniotic fluid embolus septic abortion intrauterine fetal death
(can be chronic DIC) can have DIC in hemolysisndashelevated liver enzymesndashlow platelets
(HELLP) syndrome
Vascular disease Large aortic aneurysms (chronic DIC can become acute at time of surgery) giant
hemangiomas vasculitis multiple telangiectasias
Envenomation DIC can develop with bites of rattlesnakes and other vipers the venom damages the
endothelial cells bleeding is not as serious as expected from laboratory values
Loading [Contrib]a11yaccessibility-menujs
3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
1423
Clinical SettingClinical Setting CommentsComments
Acute lung injury
(ALI) or adult
respiratory
distress
syndrome
Microthrombi are deposited in the small pulmonary vessels the pulmonary capillary
endothelium is damaged 20 of patients with ALI develop DIC and 20 of patients with
DIC develop ALI
Transfusion
reactions such
as acute
hemolytic
reaction
DIC with severe bleeding shock and acute renal failure
PathogenesisPathogenesis
Although the diseases triggering DIC are diverse the common pathway of these illnesses is that they lead toan inappropriate loss of localization or compensated control in the intravascular activation of coagulation(Figure 233-2Figure 233-2) Immune inflammatory and coagulant pathways are involved Damaged endothelial cell wallstrigger activation of the intrinsic clotting cascade leading to thrombin generation and subsequentintravascular fibrin clot deposition Increased thrombin generation leads to consumption of anticoagulantregulatory proteins (ie protein C protein S and antithrombin) further potentiating thrombosis andischemic tissue damage Production of thrombin and fibrin indirectly activates tissue plasminogen activatorand the counterregulatory fibrinolytic system When hyperfibrinolysis occurs the hemostatic clots dissolveand bleeding ensues
FIGURE 233-2FIGURE 233-2
Pathophysiology of disseminated intravascular coagulation Refer to Pathogenesis section underDisseminated Intravascular Coagulation for details FDPs = fibrinfibrinogen degradation products
Loading [Contrib]a11yaccessibility-menujs
3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
1523
Clinical FeaturesClinical Features
Clinical features of DIC vary with the underlying precipitating illness27 Hypercoagulation may predominatein certain conditions such as sepsis where signs of ischemic end-organ failure are common and physicalfindings in these patients may include cutaneous gangrene or thrombotic purpura In other instances such asDIC associated with leukemia hyperfibrinolysis may predominate and clinical features may includepetechiae ecchymoses oozing from catheter or venipuncture sites or hematuria Certain DIC-relateddisorders such as trauma and obstetric complications tend to have both strong hypercoagulation andhyperfibrinolysis elements and lead to major bleeding complications (ie wounds intracranial GI) Yet otherconditions may be associated with mild and compensated DIC in which outward signs of thrombosis andbleeding are subclinical
Laboratory FindingsLaboratory Findings
The typical laboratory results in acute DIC (Table 233-7Table 233-7) include thrombocytopenia prolonged prothrombintime low fibrinogen level and elevation of fibrin-related markers (ie d-dimer fibrin degradation products
soluble fibrin) The most commonly observed abnormality is thrombocytopenia a progressive drop in theplatelet count is sensitive although not specific for DIC Depletion of coagulation factors is reflected by aprolonged prothrombin time Fibrinogen is an acute-phase reactant and may be normal or elevated in early
DIC Scoring systems have been developed and validated to aid in the diagnosis (Table 233-8Table 233-8)2829
Loading [Contrib]a11yaccessibility-menujs
3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
1623
Levels may be chronically elevated in patients with liver or renal disease
TABLE 233-7
Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)Laboratory Abnormalities Characteristic of Disseminated Intravascular Coagulation (DIC)2828
StudiesStudies ResultResult
Most UsefulMost Useful
Platelet count Usually low or dropping
Prothrombin time Prolonged
Fibrinogen level Usually low (fibrinogen is an acute-phase reactant so may actually start out
elevated) fibrinogen level lt100 milligramsdL (lt1 gramL) correlates with severe DIC
Fibrin degradation
products and d-
dimer
Elevated
HelpfulHelpful
Activated partial
thromboplastin time
Usually prolonged
Thrombin clotting
time
Prolonged (not sensitive)
Fragmented red
blood cells
Should be present (not specific)
Specific factor
assays
Extrinsic pathway factors are most aected (VII X V and II)
Factor II V VIIdagger X Low
Factor VIII (acute-
phase reactant)
Low normal high
Factor IX Low (decreases later than other factors)
Loading [Contrib]a11yaccessibility-menujs
3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
1723
daggerFactor VII is usually low early because it has the shortest half-life
Note A score of ge5 is compatible with overt DIC A score lt5 is suggestive (not airmative) for nonovert DIC
TABLE 233-8
International Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toInternational Society on Thrombosis and Haemostasis Scoring System for DIC When Associated Condition Known toCause Disseminated Intravascular Coagulation (DIC) Is PresentCause Disseminated Intravascular Coagulation (DIC) Is Present2929
TestTest PointsPoints
Platelet count
gt100000mm3 (gt100 times 109L) 0
50000ndash100000mm3 (50ndash100 times 109L) 1
lt50000mm3 (lt50 times 109L) 2
Fibrin-related marker (d-dimer fibrin degradation products)
Normal 0
Mildly elevated 2
Markedly elevated 3
Prothrombin time prolongation
lt3 s 0
3ndash6 s 1
gt6 s 2
Fibrinogen level
gt100 milligramsdL (gt1 gramL) 0
lt100 milligramsdL (lt1 gramL) 1
Loading [Contrib]a11yaccessibility-menujs
3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
1823
Abbreviations aPTT = activated partial thromboplastin time LMWH = low molecular weight heparin PT = prothrombin
time
Dierential DiagnosisDierential Diagnosis
Primary fibrinolysis is a rare syndrome whereby plasmin and fibrinolysis occur without the production ofthrombin Severe liver disease will also manifest with coagulation abnormalities and low platelets These twoentities can be dierentiated from DIC based on clinical history and laboratory tests The hematologicabnormalities in liver disease should be relatively stable in contrast to the worsening abnormalitiesassociated with acute DIC Additionally the d-dimer assay will usually be normal or minimally elevated in
both primary fibrinolysis and liver disease but is oen significantly elevated in DIC
TreatmentTreatment
Paramount to the management of DIC is the elimination of the underlying disorder whenever possibleTreatment strategies in DIC include blood product support and strategies to modulate thrombin formation
(Table 233-9Table 233-9)262729 Generally speaking blood products should only be administered when there is evidenceof bleeding
TABLE 233-9
Treatment of Disseminated Intravascular Coagulation (DIC)Treatment of Disseminated Intravascular Coagulation (DIC)
Treat underlying precipitating disorder volume resuscitation antibiotics external cooling
Platelet transfusions for thrombocytopenia lt50000mm3 (lt50 times 109L) and active bleeding
Fresh frozen plasma for prolonged PT or aPTT (gt15) or low fibrinogen (lt100 milligramsdL [1 gramL])
Fibrinogen concentrate for persistent low fibrinogen lt100 milligramsdL (lt1 gramL)
Vitamin K for prolonged PT
Consider LMWH when thrombotic events dominate clinical picture
Consider tranexamic acid for trauma-related DIC
Platelet transfusions are recommended in actively bleeding patients who have platelet counts below
50000mm3 (50 times 109L) and may be considered in those considered to be at high risk for bleeding (such as
DIC resulting from chemotherapy) when platelet counts fall below 10000 to 20000mm3 (10 to 20 times 109L)Plasma should be administered in bleeding patients when prothrombin timeactivated PTT exceeds 15 timesnormal or when fibrinogen levels fall below 150 milligramsdL (15 gramsL) The initial recommended doseis 15 mLkg although there is some evidence that 30 mLkg may be superior when volume overload is not ofconcern Fibrinogen concentrate should be considered when hypofibrinogenemia persists despite use ofplasma Patients with a prolonged prothrombin time should receive parenteral vitamin K
Loading [Contrib]a11yaccessibility-menujs
3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
1923
There is no proven benefit in DIC with other coagulation factor products such as three- or four-factorprothrombin complex concentrate or recombinant factor VIIa Although there is no evidence demonstratingimproved outcomes low-molecular-weight heparin may be considered in patients with DIC wherethrombotic complications predominate the clinical picture or in patients with evidence of early compensated
DIC29 Patients with DIC are at very high risk for developing venous thromboembolism and routineprophylaxis with low-molecular-weight heparin in the absence of major bleeding is recommendedAntifibrinolytic medications (ie tranexamic acid) should generally be avoided in patients with DIC One
notable exception is in trauma-related DIC where their use reduces mortality30
CIRCULATING INHIBITORS OF COAGULATIONCIRCULATING INHIBITORS OF COAGULATION
Acquired inhibitors of blood coagulation also known as circulating anticoagulants are antibodies directedagainst one or more of the coagulation factors Although inhibitors may develop spontaneously in previouslyhealthy patients with normal hemostasis most inhibitors develop in patients with hereditary bleedingdisorders who receive transfusion of plasma products Inhibitors have been described for most of thecoagulation factors the two most common inhibitors are factor VIII inhibitors and antiphospholipidantibodies Factor VIII inhibitors are specific inhibitors directed only against factor VIII as opposed toantiphospholipid antibodies including lupus anticoagulant and anticardiolipin antibodies which arenonspecific inhibitors directed against several of the coagulation factors Lupus anticoagulant andanticardiolipin antibodies oen result in thrombosis (see chapter 234 Clotting Disorders)
Factor VIII InhibitorsFactor VIII Inhibitors
Factor VIII inhibitors most commonly develop in patients with hemophilia A (see chapter 235 Hemophiliasand von Willebrands Disease) but can also develop spontaneously in patients with previously normal
hemostasis a condition termed acquired hemophilia3132 The incidence of spontaneously arising inhibitorsis raremdashestimated at 14 cases per 1 million persons per year Although uncommon it is important torecognize this clinical entity because the mortality rate approaches 22 The majority of acquiredhemophilia cases approximately 85 occur in the elderly In about half of cases inhibitors develop inassociation with preexisting disorders such as autoimmune disorders (systemic lupus erythematosusrheumatoid arthritis ulcerative colitis) and lymphoproliferative disorders (multiple myeloma Waldenstroumlmsmacroglobulinemia benign monoclonal gammopathy of uncertain significance) and in patients with allergicdrug reactions (penicillins sulfonamides phenytoin)
Patients without a prior bleeding history who develop factor VIII inhibitors can present with massivespontaneous ecchymoses hematomas and hematuria Laboratory studies classically show a normalprothrombin time normal thrombin clotting time and a greatly prolonged activated PTT that does notcorrect with mixing A factor VIIIndashspecific assay will show very low or absent factor VIII activity Other factor-specific assays should be normal or only slightly decreased Quantitative measurement of the inhibitor bythe Bethesda inhibitor assay is important for the emergency management of bleeding episodes Long-termmanagement of acquired factor VIII inhibitors is with steroids IV immunoglobulin cytotoxic agents orLoading [Contrib]a11yaccessibility-menujs
3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
2023
1
2
3
4
5
6
7
8
rituximab to suppress antibody production A hematologist should direct the management of an acuteclinically significant bleeding episode
There is no proven therapy to control bleeding episodes in patients with acquired factor VIII inhibitors33
Treatment options include administration of factor VIII three- or four-factor prothrombin complexrecombinant factor VIIa desmopressin acetate and plasmapheresis Additionally the use of aspirinnonsteroidal anti-inflammatory drugs and intramuscular injections should be avoided and conservative
therapies should be considered including compression and immobilization of the bleeding site3132
REFERENCESREFERENCES
Stasi R How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program 2012 191 2012[PubMed 23233580]
Smock KJ Perkins SL Thrombocytopenia an update Int J Lab Hematol 36 269 2014 [PubMed 24750673]
Chong BH Choi PY Khachigian L Perdomo J Drug-induced immune thrombocytopenia Hematol OncolClin North Am 27 521 2013
[PubMed 23714310]
Kenney B Stack G Drug-induced thrombocytopenia Arch Pathol Lab Med 133 309 2009 [PubMed 19195976]
Neunert C Lim W Crowther M et al The American Society of Hematology 2011 evidence-based practiceguideline for immune thrombocytopenia Blood 117 4190 2011
[PubMed 21325604]
Thiagarajan P Afshar-Kharghan V Platelet transfusion therapy Hematol Oncol Clin North Am 27 6292013
[PubMed 23714315]
Chong BH Primary immune thrombocytopenia understanding pathogenesis is the key to bettertreatments J Thromb Haemost 7 319 2009
[PubMed 19077111]
Rodeghiero F Stasi R Gernsheimer T et al Standardization of terminology definitions and outcomecriteria in immune thrombocytopenic purpura of adults and children report from an international workinggroup Blood 113 2386 2009
[PubMed 19005182] Loading [Contrib]a11yaccessibility-menujs
3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
2123
9
10
11
12
13
14
15
16
17
18
19
Stasi R Pathophysiology and therapeutic options in primary thrombocytopenia Blood Transfus 9 2622011
[PubMed 21251458]
Neunert CE Current management of immune thrombocytopenia Hematology 2013 276 2013 [PubMed 24319191]
Provan D Stasi R Newland AC et al International consensus report on the investigation andmanagement of primary immune thrombocytopenia Blood 115 168 2010
[PubMed 19846889]
Sauve LJ Bettinger J Scheifele D et al Postvaccination thrombocytopenia in Canada Pediatr Infect DisJ 29 559 2010
[PubMed 20160658]
Neunert CE Buchanan GR Imbach P et al Severe hemorrhage in children with newly diagnosedimmune thrombocytopenic purpura Blood 112 4003 2008
[PubMed 18698007]
Despotovic JM Neunert CE Is anti-D immunoglobulin still a frontline treatment option for immunethrombocytopenia Hematology Am Soc Hematol Educ Program 2013 283 2013
[PubMed 24319192]
Giannini EG Savarino V Thrombocytopenia and liver disease Curr Opin Hematol 15 473 2008 [PubMed 18695370]
Northup PG Caldwell JH Coagulation in liver disease a guide for the clinician Clin GastroenterolHepatol 11 1064 2013
[PubMed 23506859]
Hayward CP Diagnostic approach to platelet function disorders Transfus Apher Sci 38 65 2008 [PubMed 18291723]
Tripodi A Mannucci PM The coagulopathy of chronic liver disease N Engl J Med 365 147 2011 [PubMed 21751907]
Da Rocha EC DAmico EA Caldwell SH et al A prospective study of conventional and expandedcoagulation indices in predicting ulcer bleeding aer variceal band ligation Clin Gastroenterol Hepatol 7988 2009
[PubMed 19410018] Loading [Contrib]a11yaccessibility-menujs
3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
2223
20
21
22
23
24
25
26
27
28
29
Mannucci PM Tripodi A Liver disease coagulopathies and transfusion therapy Blood Transfus 11 322013
[PubMed 23058863]
Sogaard KK Horvath-Puho E Gronbaek H et al Risk of venous thromboembolism in patients with liverdisease a nationwide population-based case-control study Am J Gastroenterol 104 96 2009
[PubMed 19098856]
Shah NL Intagliata NM Northup PG Argo CK Caldwell SH Procoagulant therapeutics in liver disease acritique and clinical rationale Nat Rev Gastroenterol Hepatol 11 675 2014
[PubMed 25023035]
Saja MF Abdo AA Sanai FM et al The coagulopathy of liver disease does vitamin K help Blood CoagulFibrinolysis 24 10 2012
[PubMed 23080365]
Jala DI Chonchol M Targher G Disorders of hemostasis associated with chronic kidney disease SemThromb Hemost 36 34 2010
[PubMed 20391294]
Svensson PJ Bergqvist PB Juul KV Berntorp E Desmopressin in treatment of haematological disordersand in prevention of surgical bleeding Blood Rev 28 95 2014
[PubMed 24703870]
Toh CH Alhamdi Y Current consideration and management of disseminated intravascular coagulationHematology Am Soc Hematol Educ Program 2013 286 2013
[PubMed 24319193]
Wada H Matsumoto T Yamashita Y Diagnosis and treatment of disseminated intravascular coagulation(DIC) according to four DIC guidelines J Intensive Care 2 15 2014
[PubMed [no PMID]
Toh CH Hoots WK The scoring system of the Scientific and Standardisation Committee on DisseminatedIntravascular Coagulation of the International Society on Thrombosis and Haemostasis a 5-year overview JThromb Haemost 5 604 2007
[PubMed 17096704]
Wada H Thachil J Di Nisio M et al Guidance for diagnosis and treatment of disseminated intravascularcoagulation from harmonization of the recommendations from three guidelines J Thromb Haemost 11 7612013
[PubMed 23379279] Loading [Contrib]a11yaccessibility-menujs
3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs

3272019
2323
30
31
32
33
Shakur H Roberts I Bautista R et al Eects of tranexamic acid on death vascular occlusive events andblood transfusion in trauma patients with significant haemorrhage (CRASH-2) a randomized placebo-controlled trial Lancet 376 23 2010
[PubMed 20554319]
Franchini M Mannucci PM Acquired haemophilia A a 2013 update Thromb Haemost 110 1114 2013 [PubMed 24008306]
Webert KE Acquired hemophilia A Semin Thromb Hemost 38 735 2012 [PubMed 22941793]
Zeng Y Zhou R Duan X Long D Yang S Interventions for treating acute bleeding episodes in peoplewith acquired hemophilia A Cochrane Database Syst Rev 8 CD010761 2014
[PubMed 25165992]
McGraw HillCopyright copy McGraw-Hill Education
All rights reserved Your IP address is 99532511559953251155
Terms of Use bull Privacy Policy bull Notice bull Accessibility
Access Provided by Brookdale University Medical CenterSilverchair
Loading [Contrib]a11yaccessibility-menujs