Embed Size (px)
Citation preview
Acid Base Disorders
הפרעות בסיס חומצהKarl Skorecki
Tel: 8543250 1. asterisk indicates optional
2. you may contact me as noted above with questions

Hey- What’s the
peeH here anyway?
Definitions and Equations
1. Medical definition of acid-base status of a patient refers to [H+] of the extracellular fluid.
2. Normal [H+]ECF is 40nM/Litre (equivalent to pH 7.40)
3. Acidemia is a state wherein the [H+]ECF > 40 (pH < 7.40)Alkalemia is a state wherein the [H+]ECF < 40 (pH > 7.40)(Euphemia is a state wherein the [H+]ECF is normal).
Definitions and Equations (Cont.)
4. H+ + HCO3- H2CO3 H2O+CO2
40nM 25mM PCO2 = 40mmHg
40 25
40
Acidosis any process which increases PCO2/HCO3-
ratioAlkalosis any process which decreases PCO2/HCO3
- ratio
5. The ratio PCO2/HCO3 determines the [H+] (pH)
PCO2mmHgHCO3mmol/LH+nmol/L=25 •
Definitions and Equations (Cont.)
H+ = 25 •
PCO2
HCO3
6. Acidosis
Alkalosis
increases PCO2/HCO3 ratio
Metabolic: by lowering HCO3
Respiratory: by raising PCO2
decreases PCO2/HCO3 ratio
Metabolic: by raising HCO3
Respiratory: by lowering PCO2

הצעת חוק בסיסי החומצה וחוק איסור ”Base Excess”שם החוק: חוק איסור השימוש ב-שימוש בשמות הנדרסון, הסלבך.
וסטודנטים לרפואה בישראל כבר מספיק מסכנים הואילומבולבלים
ואין מרצה או פרופסור בעולם שמבינ/ה בעצמו/ה את והואילהנ"להמונחים
הצעת חוק זו באה לאסור לחלוטין את השימוש במונחים הנ"ל בכתב בעל-פה, במצגת, בביקור רופאים, בבית, בעבודה, ובכל
מקרה )למעט בהצעת החוק הנוכחית(: המפר את החוק לא יוכל לעשות רוטציה בשום מחלקה עונש
לנפרולוגיה המכבדת את עצמה, ויחוייב ללמוד את נושא בסיסי החומצה אך ורק במסגרת המחלקות הכירורגיות.
נערך ונחתם היום ע"י השר לענייני בסיסי חומצה
מדינת *ישראל
Definitions and Equations (Cont.)
H+ = 25 •
PCO2
HCO3
7. The four primary acid-base disturbances are: Metabolic acidosis (primary decrease in HCO3) Metabolic alkalosis (primary increase in HCO3) Respiratory acidosis (primary increase in PCO2) Respiratory alkalosis (primary decrease in PCO2)
8. - Can have none, one, two, or three of the above in combination.
- Can have any combination except? - The net result can leave [H+] normal/high
(acidemia) or low (alkalemia)

Metabolic Acidosis15 year-old with three week history of polyuria, polydipsia and 2 day history of nausea, abdominal pain, and weakness progressing to extreme drowsiness. Physical exam remarkable for rapid breathing, low blood pressure, and decreased level of consciousness.
Lab: Glucose 220[H+] 62.5 (pH 7.2)PCO2 25HCO3 10Na+ 142K+ 3.4Cl- 105
H+ = 25 •
PCO2
HCO3
Metabolic Acidosis (Cont.)
62.5 10
25
BUT:
HCO3 is low
PCO2 is also low
[H+] is high (low pH; patient is acidemic)
• Metabolic acidosis primary decrease in HCO3
• Maybe the patient has a metabolic acidosis
• What about the PCO2 ?

“Compensation” Rules• Each primary acid base disturbance is associated with an expected compensation
• If the primary disturbance is metabolic (HCO3), the expected compensation is respiratory (PCO2)
• If the primary disturbance is respiratory (PCO2), the expected compensation is metabolic (HCO3)
• The compensation “tries” to restore the H+ (pH) toward normal, but never quite makes it (why ? see later)
• The “expected” amount of compensation is different for each of the four primary acid-base disturbances and needs to be memorized
• The direction of the expected compensation is always in the same direction as the primary disturbance
Metabolic Acidosis
H+ = 25 •
PCO2
HCO3
compensation
primary
Metabolic Alkalosis
H+ = 25 •
PCO2
HCO3
compensation
primary
Respiratory Acidosis
H+ = 25 •
PCO2
HCO3
primary
compensation
Respiratory Alkalosis
H+ = 25 •
PCO2
HCO3
primary
compensation

15 year-old with diabetic comaH+ 62.5 (pH 7.2), PCO2 25, HCO3 10
H+ = 25 •
PCO2
HCO362.510
25
If primary metabolic acidosis, does the decrease in PCO2 represent an “appropriate” expected compensation ?
Metabolic acidosis:
Rule: for every decrease of 1 mmol/Litre in HCO3
there should be a decrease of 1 mmHg PCO2
Did this happen ?
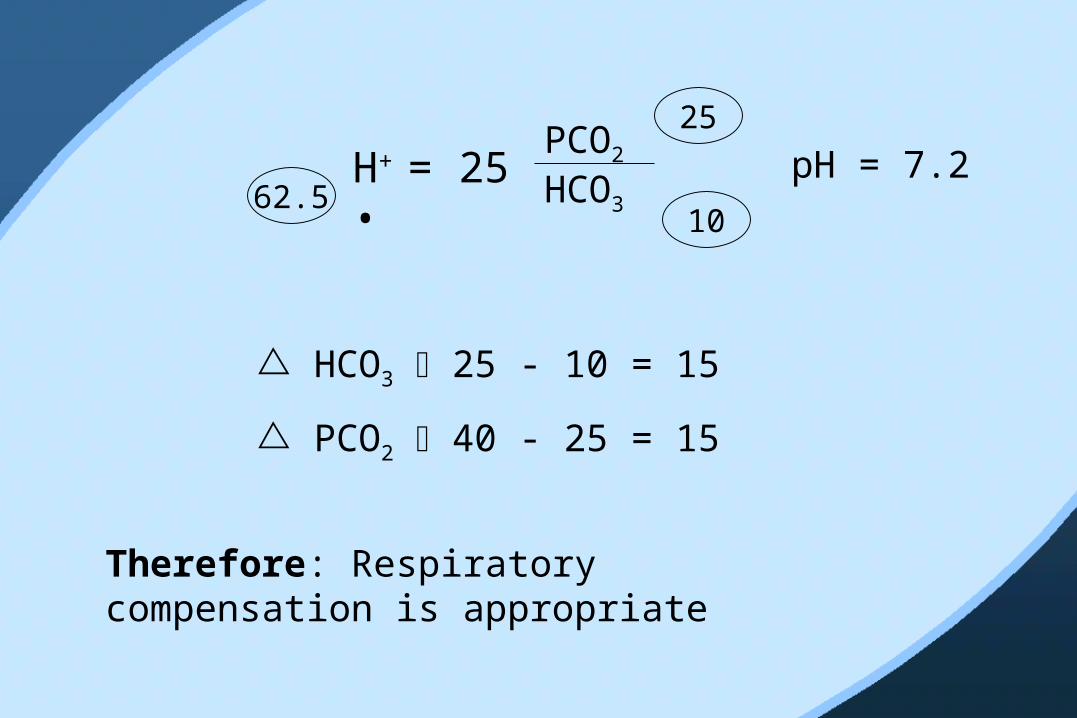
H+ = 25 •
PCO2
HCO362.510
25
pH = 7.2
HCO3 25 - 10 = 15
PCO2 40 - 25 = 15
Therefore: Respiratory compensation is appropriate
If respiratory compensation is appropriate, WHY is the patient still acidemic (p = 7.2) ?
After all, most people could hyper-ventilate further, even down to PCO2 of < 10
Answer:
*

The capacity for “respiratory
compensation” is what makes the
bicarbonate buffer system so useful, even
though the pK for is 6.8
(far from 7.4)
H2CO3
HCO3-
CO2
*
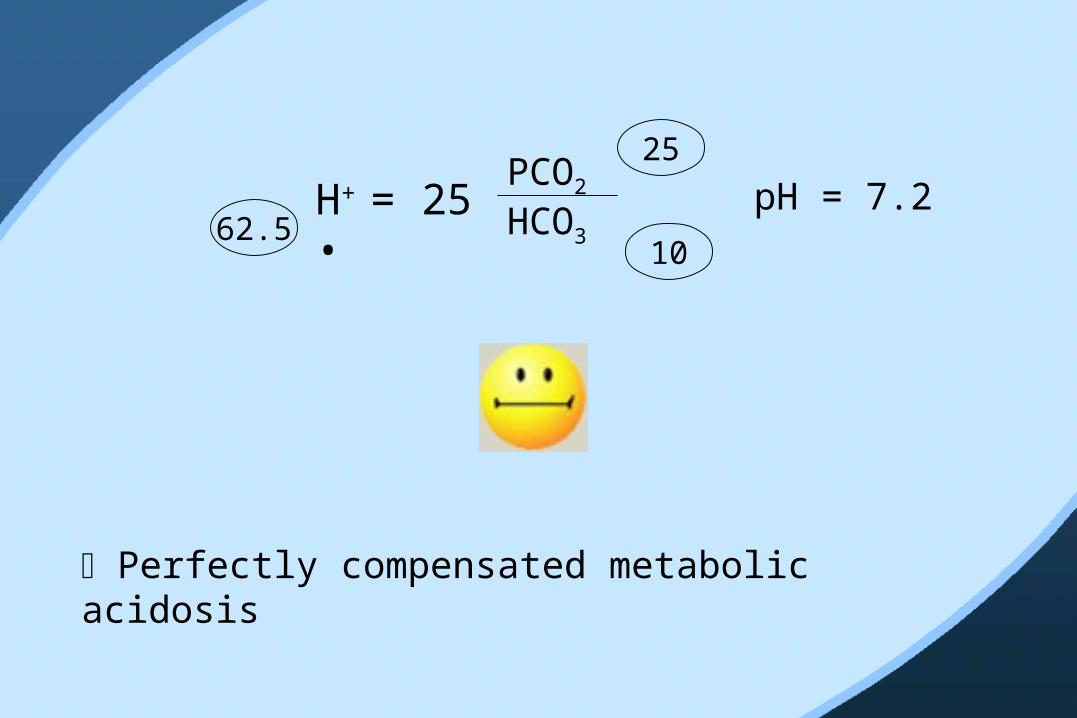
H+ = 25 •
PCO2
HCO362.510
25
pH = 7.2
Perfectly compensated metabolic acidosis

What if PCO2 remained “normal” ?
H+ = 25 •
PCO2
HCO310
40
H+ = 100 pH = 7.00
Metabolic acidosis + respiratory acidosis
clinical example ?
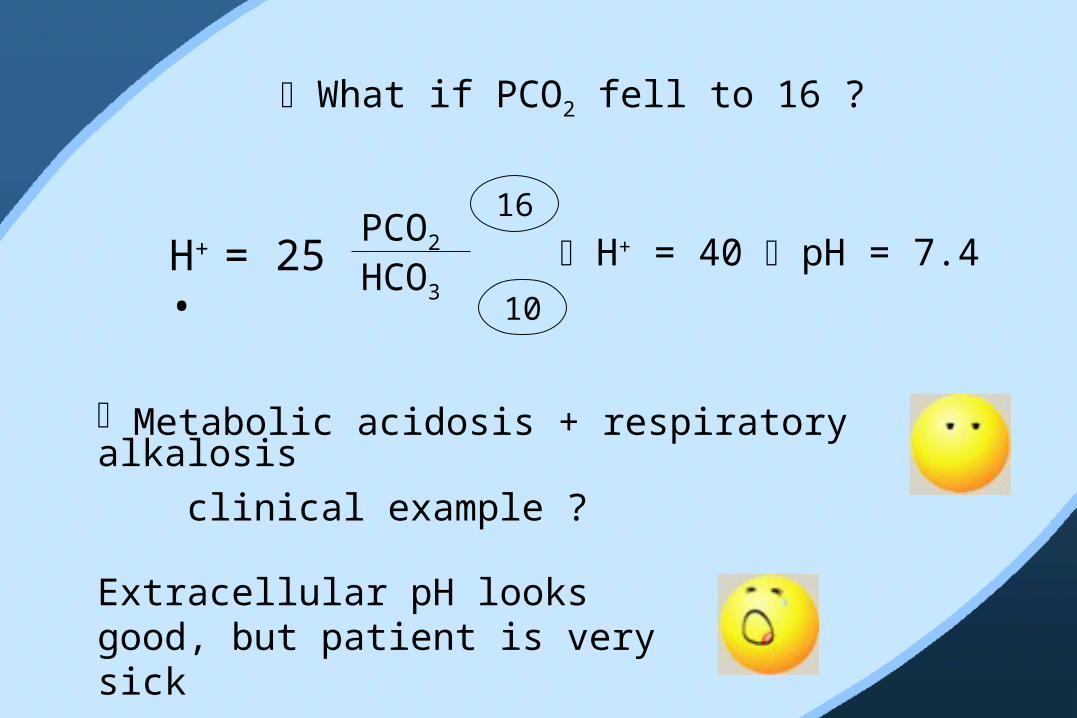
What if PCO2 fell to 16 ?
H+ = 25 •
PCO2
HCO310
16
H+ = 40 pH = 7.4
Metabolic acidosis + respiratory alkalosis
clinical example ?
Extracellular pH looks good, but patient is very sick
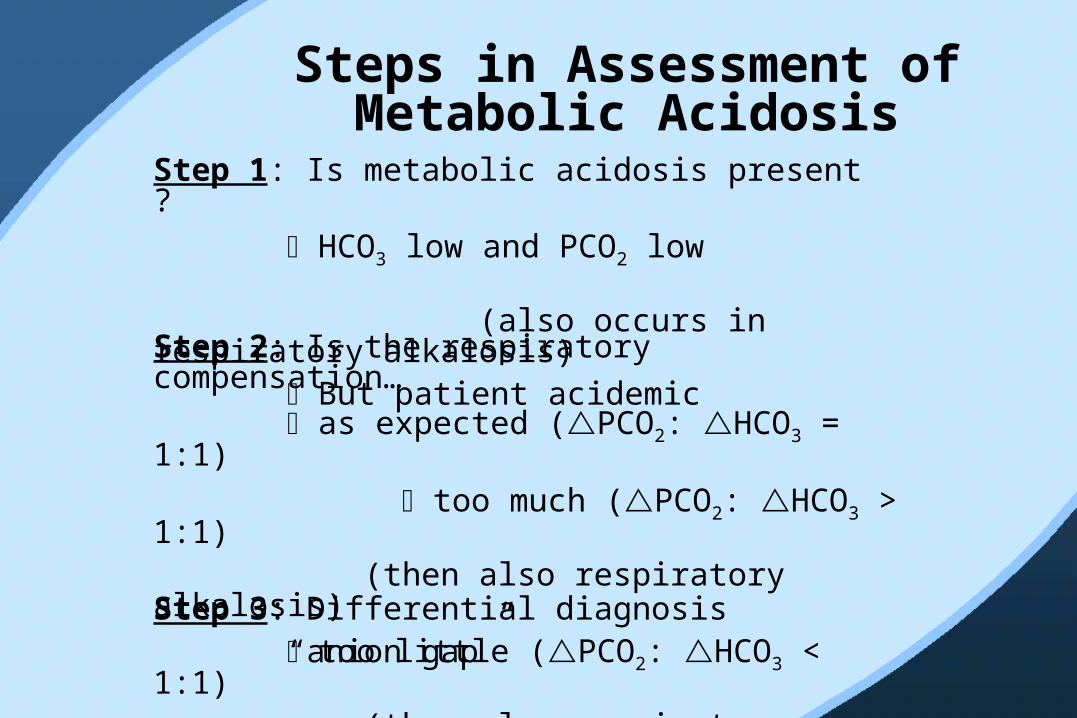
Steps in Assessment of Metabolic Acidosis
Step 1: Is metabolic acidosis present ? HCO3 low and PCO2 low
(also occurs in respiratory alkalosis) But patient acidemic Step 2: Is the respiratory compensation…
as expected (PCO2: HCO3 = 1:1)
too much (PCO2: HCO3 > 1:1) (then also respiratory alkalosis)
too little (PCO2: HCO3 < 1:1) (then also respiratory acidosis) Step 3: Differential diagnosis “anion gap”
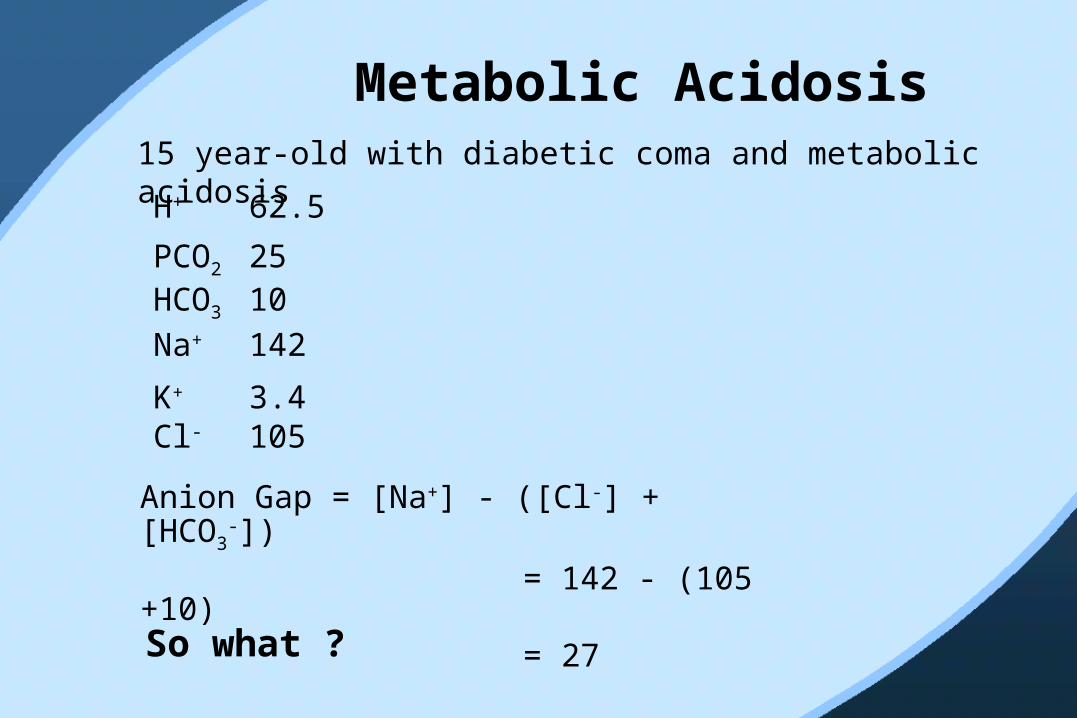
Metabolic Acidosis15 year-old with diabetic coma and metabolic acidosis
H+ 62.5
PCO2 25
K+ 3.4
HCO3 10Na+ 142
Cl- 105
Anion Gap = [Na+] - ([Cl-] + [HCO3-])
= 142 - (105 +10)
= 27
So what ?
Differential Diagnosis of Metabolic Acidosis “anion
gap”• Metabolic acidosis results from decrease in HCO3
-
• There are two ways whereby HCO3-
(a) titration of HCO3- by an acid
e.g. H+Ac + Na+HCO3- NaAc + H2O + CO2
(b) loss of NaHCO3 in urine or stool
• Process (a) and process (b) leave different “imprints” in the plasma chemistries
Process A titration of HCO3- by an acid
H+X- + NaHCO3- NaX + H2O + CO2
• Designate Na+, Cl-, and HCO3- as electrolytes
whose concentrations we chose to measure
• Normally: Na+ - (Cl- + HCO3-) = “anion gap”
140 - (103 + 25) = 12
• Process A: We do not routinely measure X- (we don’t know what it is at the beginning)
• Therefore, for every “X-” gained, there is one “HCO3
-” lost
• Therefore, “anion gap” will rise by one for every HCO3 titrated away
Metabolic Acidosis15 year-old with diabetic coma and metabolic acidosis H+ 62.5 PCO2 25HCO3 10Na+ 142K+ 3.4Cl- 105Anion Gap = 27
Normal anion gap is 12 anion Gap is 27 - 12 = 15 HCO3
- has decreased by 40 - 25 = 15 Gap = HCO3
-Therefore: anion gap type metabolic acidosis
Anion Gap Metabolic Acidosis
Only 4 categories:
Ketoacidosis - Diabetic- Alcoholic- Starvation
Lactic - Type A (ischemia, anoxia)- Type B (metabolic)
Uremic
Poisons - Methanol- Ethylene glycol- Salicylic acid- Other
Metabolic Acidosis15 year-old with diabetes, coma and extensive vomiting H+ 62.5 (pH 7.2)PCO2 25HCO3 10Na+ 142K+ 3.4Cl- 95
Anion Gap = 142 - (95 + 10) = 37
Gap 37 - 12 = 25 HCO3
- = 15
How can that be ?

Answer:
• Occult metabolic alkalosis
• If no metabolic acidosis, HCO3 would have been 35
• Metabolic acidosis is much more severe than reflected in HCO3 of 10 (35 10 Vs. 25 10)
• Consistent with vomiting
• More on metabolic alkalosis and vomiting after lunch

Metabolic AcidosisAnion Gap• Ketoacidosis• Lactic• Uremic• Poison
Non-Anion Gap• Rare: HCl poisoning
•Primary loss of HCO3-
renal - complicated
external (diarrhea, uretero-sigmoidostomy)
42 year-old presents with a 5-day history of severe watery diarrhea beginning 10 days after completing antibiotics for pyelonephritis
H+ 62.5 (pH 7.2)PCO2 25HCO3 10Na+ 140K+ 3.4Cl- 118
Anion gap 140 - (118 + 10) = 12

Why doesn’t the anion gap rise in a non-anion gap acidosis?
Anion gap = Na+ - (Cl- + HCO3-)
By definition, the HCO3- has decreased.
Therefore, if the anion gap hasn’t changed:
• Either the Na+ has decreased
• Or, the Cl- has increasedAnswer: The Cl- rises (hyperchloremic metabolic acidosis)
*
How does the Cl- know to increase ?Anion gap = Na+ - (Cl- + HCO3
-)In a non-anion gap metabolic acidosis there is either: Gain of HCl (rare HCl poisoning)
• So each HCO3- lost is accompanied by a Cl- gained
• Therefore no change in anion gap Primary loss of Na+ with HCO3
-
• So each HCO3- lost is accompanied by a Na+ lost
• If the Na+ really decreased 1:1 with the HCO3-,
then the anion gap wouldn’t change • But, that doesn’t happen (the body defends its
volume and osmolality and hates hypo Na+)• Therefore, the kidney reabsorbs Na+ with Cl-
and the Cl- increases
*

Non Anion Gap (Hyperchloremic) Metabolic
Acidosis
• HCl gain
• HCO3- loss
Extraneal
Renal
Diarrhea
Uretero-sigmoidostomy
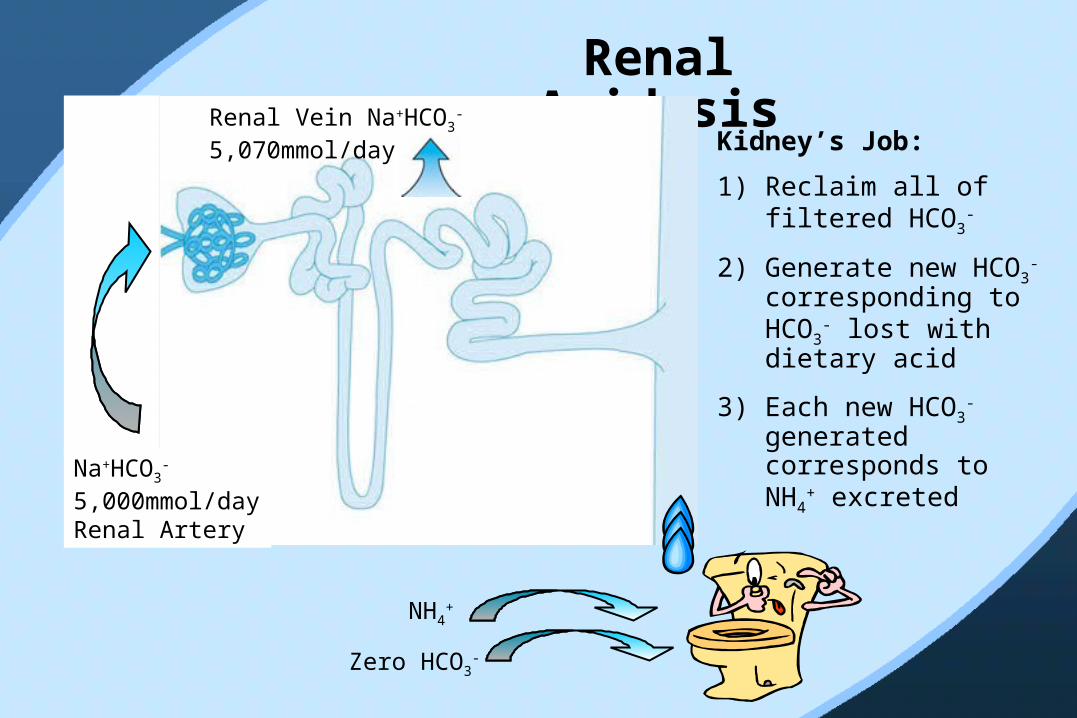
Renal AcidosisRenal Vein Na+HCO3
- 5,070mmol/day
Na+HCO3-
5,000mmol/day Renal Artery
NH4+
Zero HCO3-
Kidney’s Job:
1) Reclaim all of filtered HCO3
-
2) Generate new HCO3-
corresponding to HCO3
- lost with dietary acid
3) Each new HCO3-
generated corresponds to NH4
+ excreted

Renal Tubular Acidosis
HCO3-
5,000
4,000
Proximal• Failure to reclaim HCO3
-
genesis
HCO3-
4,000
4,000
steady-state
• bicarbonaturia • urine pH > 7
• no bicarbonaturia • urine pH < 6
Distal• Failure to excrete H+(NH4
+) and hence generate HCO3
-
Metabolic Acidosis70 year-old with glaucoma treated with acetazolamide (carbonic anhydrase inhibitor) presents with weakness. Physical examination: BP 100/50 (baseline 150/90)H+ 75 (pH 7.12)PCO2 45HCO3 15Na+ 139K+ 2.1Cl- 108Anion gap 12Urine pH 8
• Bicarbonate low, patient very acidemic
• Respiratory compensation respiratory acidosis
• Anion gap normal
Diagnosis: acetazolamide proximal RTAHypokalemia respiratory muscle weakness

Mixed Anion Gap + Non Anion Gap Metabolic Acidosis
70 year-old with glaucoma treated with acetazolamide (carbonic anhydrase inhibitor) presents with fever, severe abdominal pain (RUQ), jaundice and collapses. BP 60 systolic extremities; breathing: distressed.Lab:WBC 24,000 92% neutrophilsH+ 100 (pH 7.00)PCO2 20HCO3 5Na+ 140Cl- 113Anion gap 22Urine pH 8Acid-base diagnosis:
Likely scenario:
An anion gap metabolic acidosis can turn into a non-anion gap metabolic acidosis
HOW ?
If the anion accumulated in the plasma is excreted in the urine
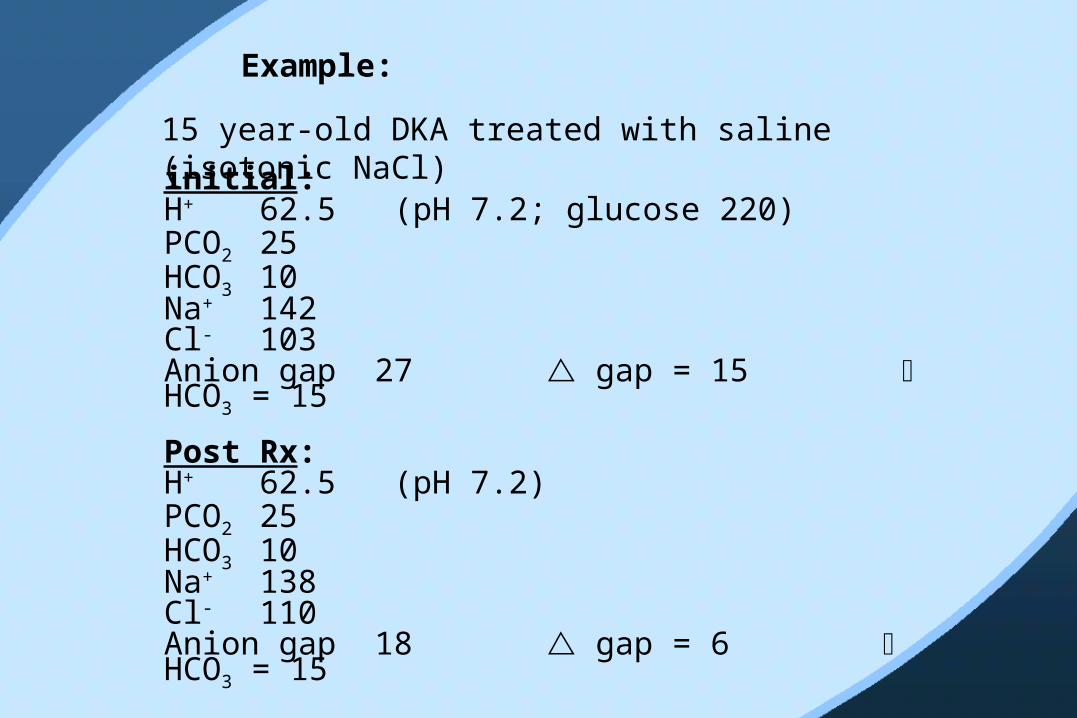
Example:
15 year-old DKA treated with saline (isotonic NaCl)initial:H+ 62.5 (pH 7.2; glucose 220)PCO2 25HCO3 10Na+ 142Cl- 103Anion gap 27 gap = 15 HCO3 = 15
Post Rx:H+ 62.5 (pH 7.2)PCO2 25HCO3 10Na+ 138Cl- 110Anion gap 18 gap = 6 HCO3 = 15

Where have all the extra unmeasured anions gone ?
Answer:
Pissed away as a result of saline volume expansion
Hint: Can measure gap in urine
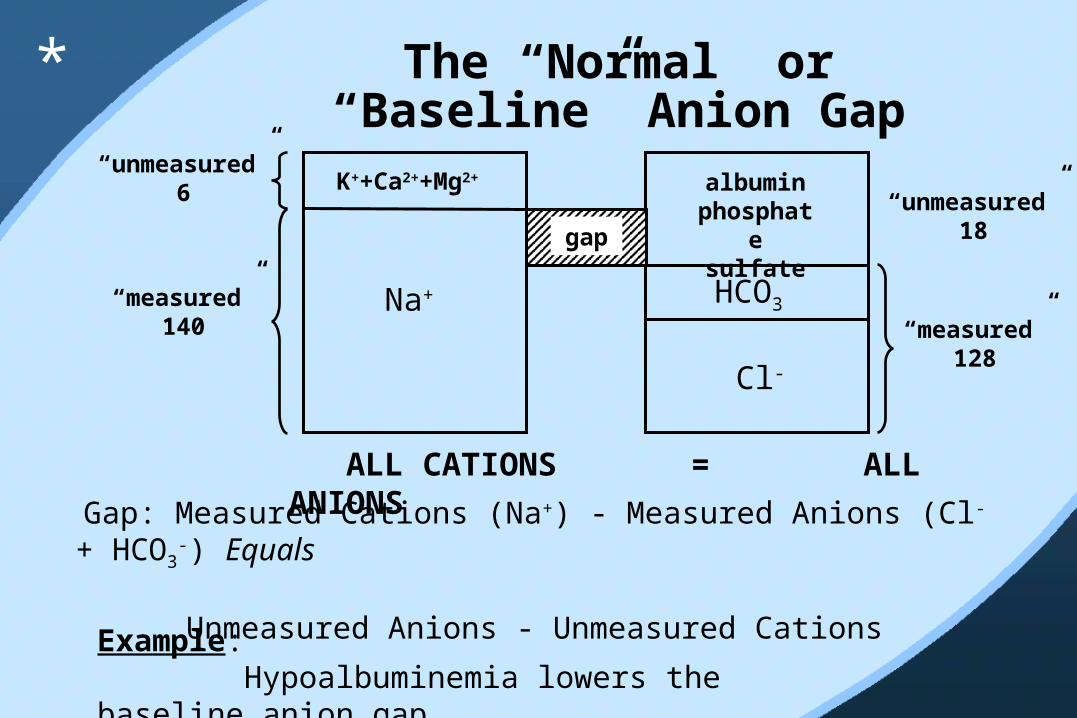
The “Normal” or “Baseline” Anion GapK++Ca2+
+Mg2+
Na+
Cl-
HCO3
gap
albumin phospha
te sulfate
“unmeasured”6
“measured” 140
“unmeasured”18
“measured” 128
ALL CATIONS = ALL ANIONSGap: Measured Cations (Na+) - Measured Anions (Cl- +
HCO3-) Equals Unmeasured Anions - Unmeasured Cations
Example: Hypoalbuminemia lowers the baseline anion gap
*
Metabolic Acidosis• Look at [H+] (pH)
HCO3-
PCO2
• [H+] high (pH low) metabolic acidosis HCO3
- low • Look at PCO2 to assess respiratory
compensation • Calculate anion gap• Compare anion gap to bicarbonate
H+ = 25 •
PCO2
HCO3
pH [H+] – not really necessary
1. Table on PALM2. Between 7.25 7.50
for every deviation of one pH unit from 7.40, the [H+] deviates correspondingly by 1mmol/litre in the opposite direction
3. Rule of 80% 7.00 1007.10 807.20 8 X 80 = 64 7.30 8 X 64 = 517.40 8 X 50 = 407.50 8 X 40 = 327.60 8 X 32 = 267.70 8 X 26 = 21
*
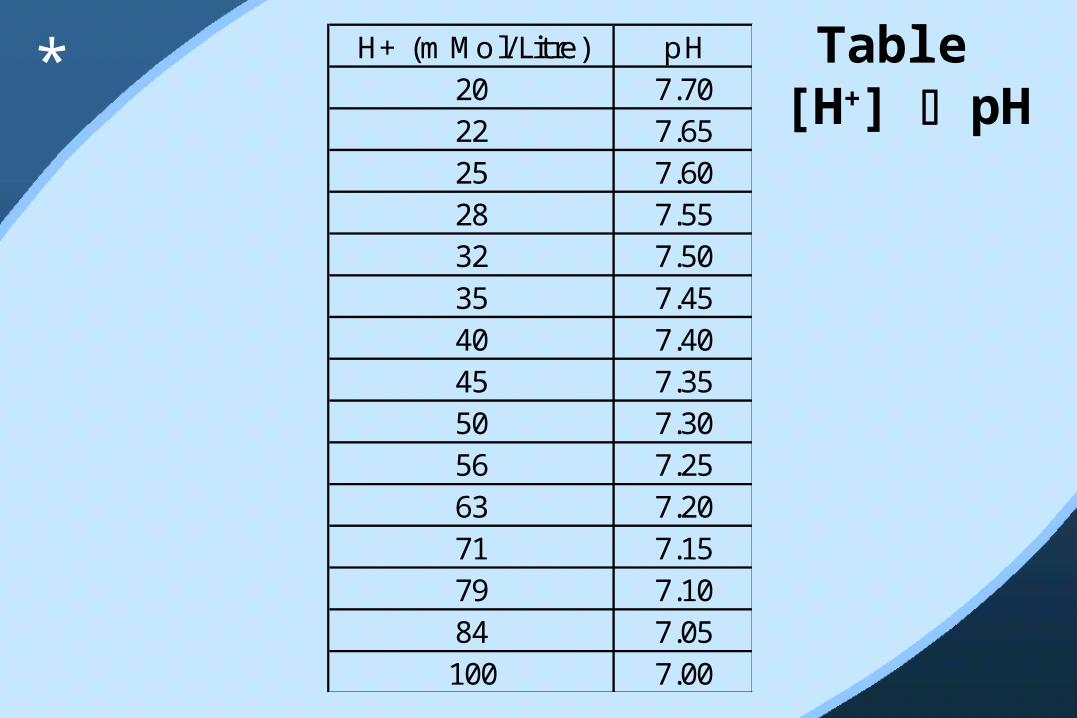
Table [H+] pH
H+ (mMol/Litre) pH20 7.7022 7.6525 7.6028 7.5532 7.5035 7.4540 7.4045 7.3550 7.3056 7.2563 7.2071 7.1579 7.1084 7.05100 7.00
*
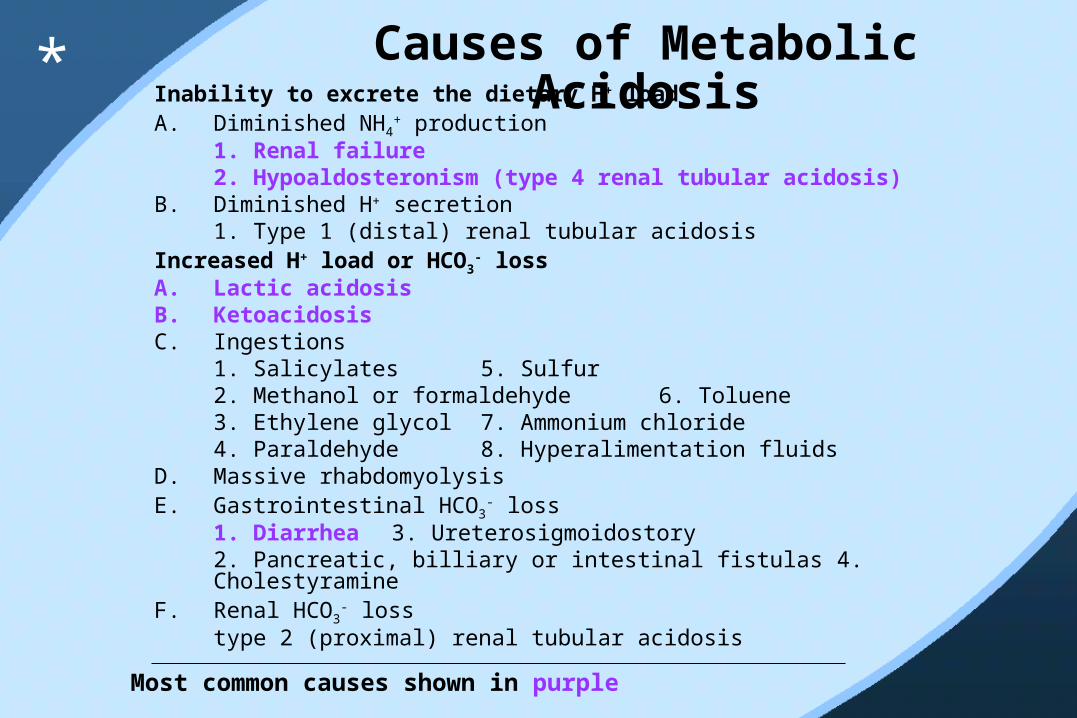
Causes of Metabolic AcidosisInability to excrete the dietary H+ load
A. Diminished NH4+ production
1. Renal failure 2. Hypoaldosteronism (type 4 renal tubular acidosis)
B. Diminished H+ secretion 1. Type 1 (distal) renal tubular acidosis
Increased H+ load or HCO3- loss
A. Lactic acidosis B. Ketoacidosis C. Ingestions
1. Salicylates 5. Sulfur2. Methanol or formaldehyde 6. Toluene 3. Ethylene glycol 7. Ammonium chloride 4. Paraldehyde 8. Hyperalimentation fluids
D. Massive rhabdomyolysis E. Gastrointestinal HCO3
- loss1. Diarrhea 3. Ureterosigmoidostory 2. Pancreatic, billiary or intestinal fistulas 4. Cholestyramine
F. Renal HCO3- loss
type 2 (proximal) renal tubular acidosis Most common causes shown in purple
*
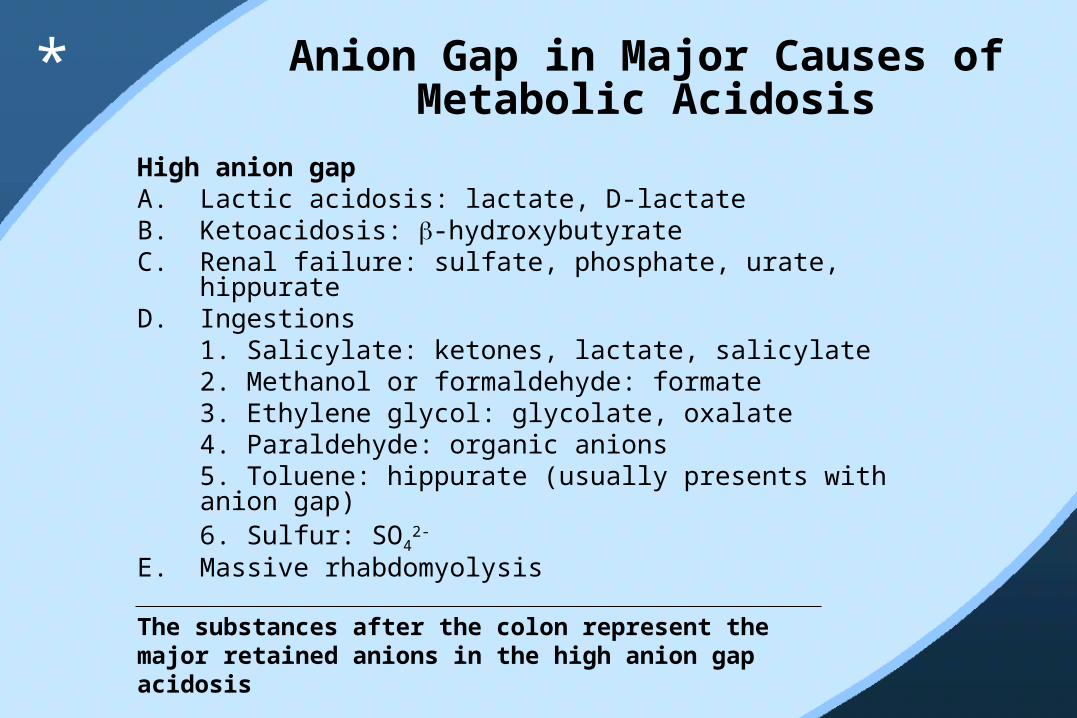
High anion gap A. Lactic acidosis: lactate, D-lactate B. Ketoacidosis: -hydroxybutyrate C. Renal failure: sulfate, phosphate, urate, hippurate D. Ingestions
1. Salicylate: ketones, lactate, salicylate
2. Methanol or formaldehyde: formate 3. Ethylene glycol: glycolate, oxalate
4. Paraldehyde: organic anions 5. Toluene: hippurate (usually presents with anion gap)6. Sulfur: SO4
2- E. Massive rhabdomyolysis
Anion Gap in Major Causes of Metabolic Acidosis
The substances after the colon represent the major retained anions in the high anion gap acidosis
*

Normal anion gap (hyperchloremic acidosis)Gastrointestinal loss of HCO3
-
1. Diarrhea Renal loss of HCO3
-
1. Type 2 (proximal) renal tubular acidosis C. Renal dysfunction
1. Some cases of renal failure 2. Hypoaldosteronism (type 4 renal tubular acidosis)3. Type 1 (distal) renal tubular acidosis
Ingestions: 1. Ammonium chloride 2. Hyperalimentation fluids
E. Some cases of ketoacidosis, particularly during treatment with insulin
Anion Gap in Major Causes of Metabolic Acidosis (cont.)
*

H+ = 25 •
PCO2
HCO3
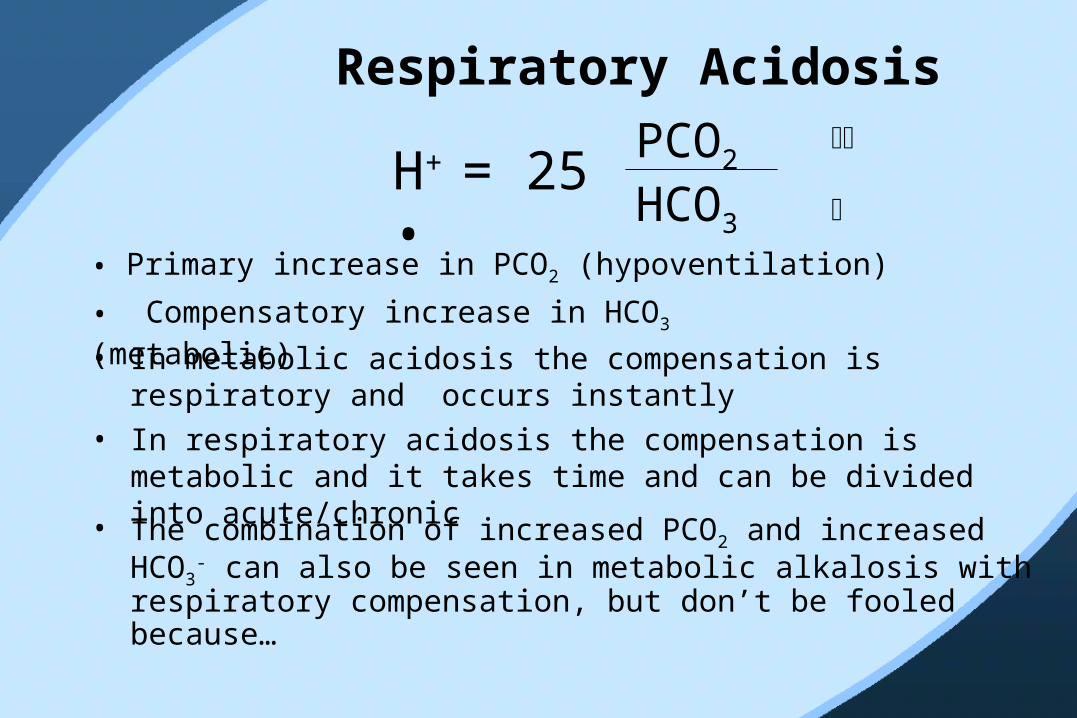
Respiratory Acidosis
• Primary increase in PCO2 (hypoventilation)
• The combination of increased PCO2 and increased HCO3-
can also be seen in metabolic alkalosis with respiratory compensation, but don’t be fooled because…
• In respiratory acidosis the compensation is metabolic and it takes time and can be divided into acute/chronic
• In metabolic acidosis the compensation is respiratory and occurs instantly
• Compensatory increase in HCO3 (metabolic)
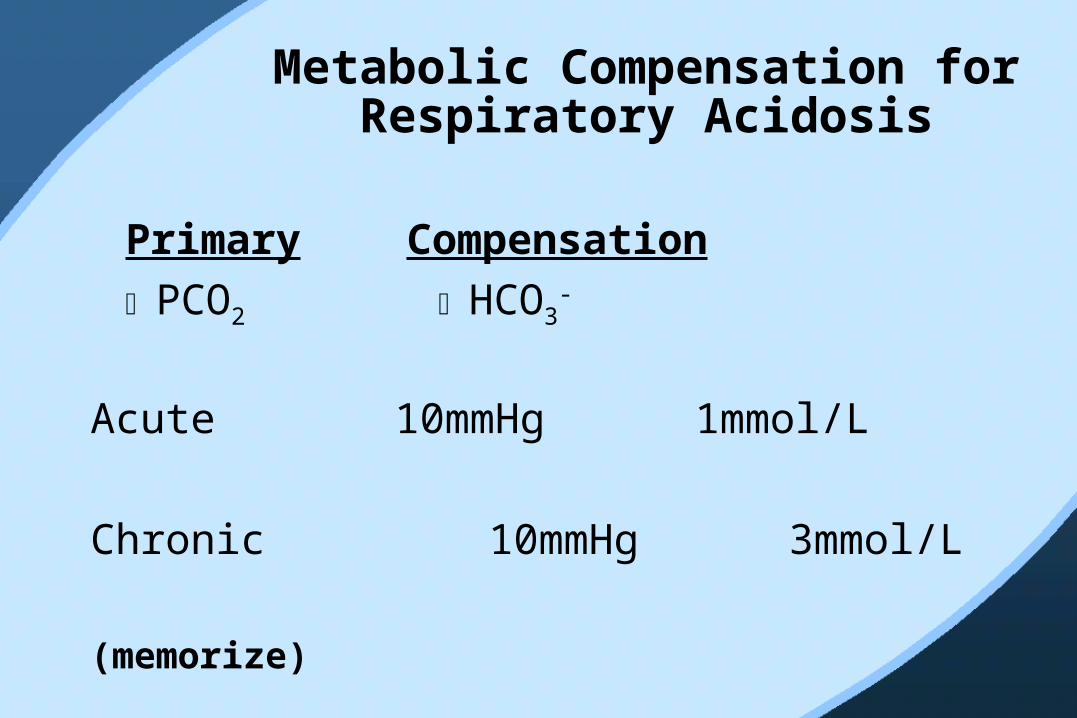
Metabolic Compensation for Respiratory Acidosis
Primary Compensation
PCO2 HCO3-
Acute 10mmHg 1mmol/L
Chronic 10mmHg 3mmol/L
(memorize)
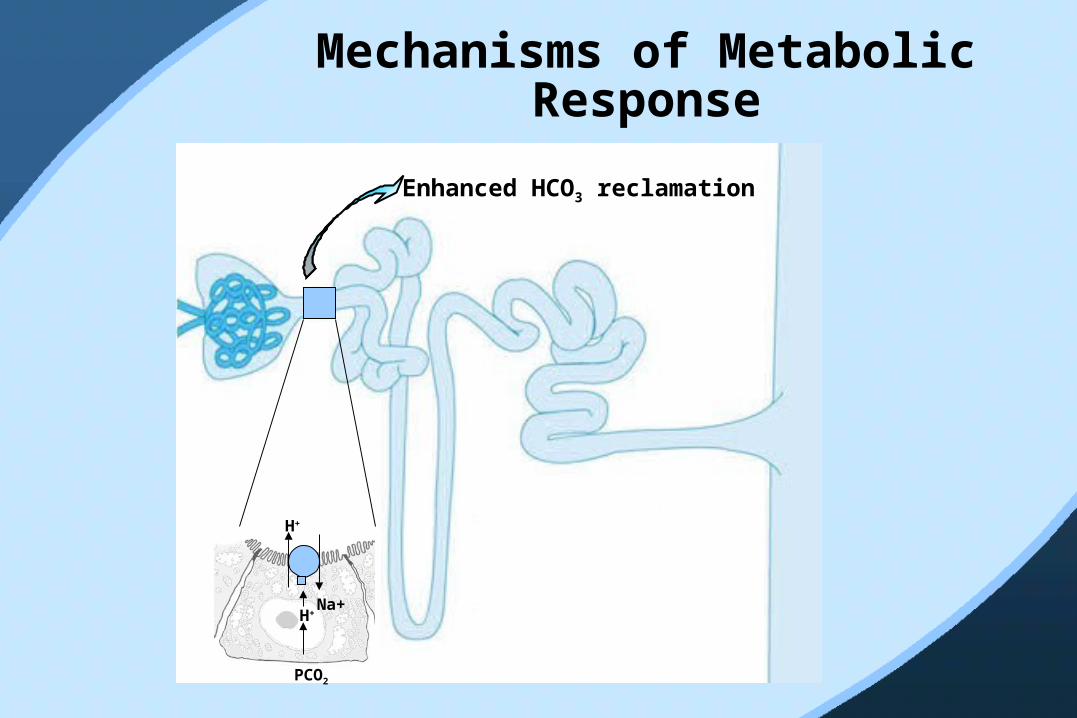
Mechanisms of Metabolic Response
H+
Na+
H+
PCO2
Enhanced HCO3 reclamation
Causes of Respiratory Acidosis (Hypoventilation)
Lungs
Brain
Chest wall + diaphragm
Airway
Causes of Acute and Chronic Respiratory
AcidosisInhibition of the medullary respiratory center A. Acute
1. Drugs: opiates, anesthetics, sedatives 2. Oxygen in chronic hypercapnia 3. Cardiac arrest4. Central sleep apena
B. Chronic 1. Extreme obesity (Pickwickian syndrome) 2. Central nervous system lesions (rare) 3. Metabolic alkalosis (although hypercapnia is an appropriate response to the rise in pH in this setting)
*

Causes of Acute and Chronic Respiratory
Acidosis (cont.)Disorders of the respiratory muscles and chest wallA. Acute
1. Muscle weakness: crisis in myasthenia gravis, periodic paralysis, aminoglycosides, Guillain-Barré syndrome, severe hypokalemia or hypophosphatremia
B. Chronic 1. Muscle weakness: spinal cord injury, poliomyelitis, amyotrophic lateral sclerosis, multiple sclerosis, myxedema 2. Kyphoscoliosis 3. Extreme obesity
Upper airway obstructionA. Acute
1. Aspiration of foreign body or vomitus2. Obstructive sleep apena 3. Laryngoispasm
*
Causes of Acute and Chronic Respiratory
Acidosis (cont.)Disorders affecting gas exchange across the pulmonarycapillary A. Acute
1. Exacerbation of underlying lung disease (including Increased CO2 production with high-carbohydrate diet) 2. Adult respiratory distress syndrome3. Acute cardiogenic pulmonary edema4. Severe asthma or pneumonia 5. Pneumothorax or hemothorax
B. Chronic 1. Chronic obstructive pulmonary disease: bronchitis, emphysema2. Extreme obesity
Mechanical ventilation
*
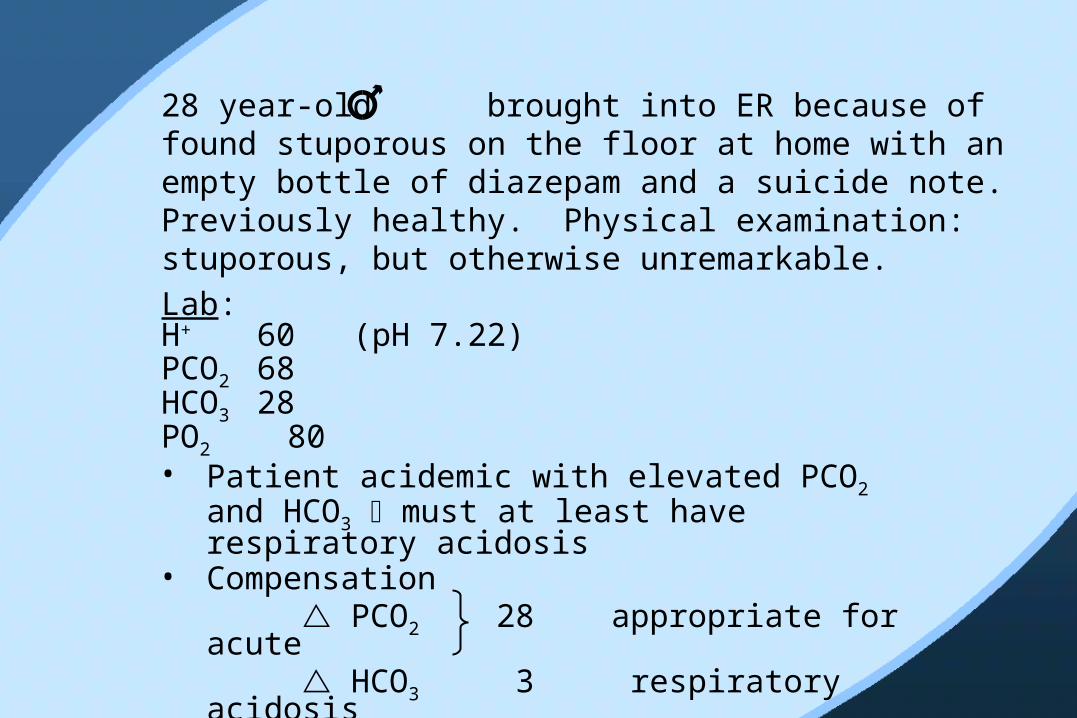
Lab:H+ 60 (pH 7.22)PCO2 68HCO3 28PO2 80
28 year-old brought into ER because of found stuporous on the floor at home with an empty bottle of diazepam and a suicide note. Previously healthy. Physical examination: stuporous, but otherwise unremarkable.
• Patient acidemic with elevated PCO2 and HCO3 must at least have respiratory acidosis
• Compensation PCO2 28 appropriate for acute HCO3 3 respiratory acidosis

Lab:H+ 100 (pH 7.00)PCO2 68HCO3 17Na+ 138 gap: 138 -
(98+17) = 23Cl- 98K+ 5.6Creat 4.8 CK 68,000 I.U.
28 year-old overdose has been lying on the floor for two days. Physical examination reveals extensive edema on the right side of the body. No urine in bladder
• Patient very acidemic, with high PCO2 and low HCO3-
• Combined respiratory and metabolic acidosis • Respiratory acidosis from drug overdose • Expected compensation: HCO3
- 28, but in reality: HCO3
- 17 HCO3 11• Anion gap 23: gap = 11• Anion gap metabolic acidosis:
rhabdomyalysis + renal failure
62 year-old with stable COPDLab:H+ 50 (pH 7.3)PCO2 60HCO3 30PO2 60
• Patient acidemic with elevated PCO2 elevated bicarbonate
• Chronic respiratory acidosis
• Expected compensation:
PCO2 20
HCO3 6
62 year-old with stable COPD and 1-day history of worsening cough, fever and dyspnea with drowsiness Lab:H+ 60 (pH 7.22)PCO2 80HCO3 33PO2 45
• Acute worsening of respiratory acidosis
• Expected compensation:
Chronic as before HCO3 to ~31
Acute further smaller HCO3 to ~33
• What is the most dangerous intervention, and if you make this mistake, what should you do ?
62 year-old with COPD and acute worsening reaches respiratory failure and is ventilated. ABG’s measured immediately after Lab:H+ 30 (pH 7.5)PCO2 40HCO3 33PO2 380
• What happened ?
• How will this affect weaning from ventilator ?
• What will her ABG’s look like if she extubates herself ?
62 year-old with COPD and respiratory failure on ventilator is treated with antibiotics and develops severe watery diarrheaLab:H+ 62.5 (pH 7.2)PCO2 50HCO3 20Na+ 142 (gap 12) Cl- 110
• Respiratory acidosis appropriately ventilated to PCO2 50
• Expected HCO3- is 25 + 3 = 28
Observed HCO3- is 20
Therefore: Metabolic acidosis 28 20• Anion gap not elevated: antibiotic induced diarrhea
H+ = 25 •
PCO2
HCO3
• Primary decrease in PCO2 (hyperventilation)
• Compensatory decrease in HCO3 (metabolic)• The metabolic compensation can be divided into
acute (minutes) and chronic (hours to days)• The compensation for chronic respiratory
alkalosis is the most complete, and nearly normalizes the pH
Respiratory Alkalosis
• The combination of low PCO2 and HCO3 was also seen in metabolic acidosis, but don’t be fooled, because…

Primary Compensation
PCO2 HCO3-
Acute 10mmHg 2mmol/L
Chronic 10mmHg 5mmol/L
(memorize)
Metabolic Compensation for
Respiratory Alkalosis

• Low PCO2 in proximal tubule• Inhibition of Na+-H+ exchanger• Decreased proximal reabsorption of filtered HCO3
-
• Bicarbonaturia
It’s always easier to lose something then to win something – that’s why this compensation is so complete
Mechanism for Metabolic
Compensation
Causes of Respiratory AlkalosisHypoxemia
A. Pulmonary disease: pneumonia, interstitial fibrosis emboli, edema
B. Congestive heart failure C. Hypotension or severe anemiaD. High-altitude residencePulmonary disease Direct stimulation of the medullary respiratory center A. Psychogenic or voluntary hyperventilation B. Hepatic failure C. Gram-negative septicemia D. Salicylate intoxication E. Postcorrection of metabolic acidosis F. Pregnancy and the lutheal phase of the menstrual cycle
(due to progesterone)G. Neurologic disorders: cerebrovascular accidents,
pontine tumorsMechanical ventilation
*
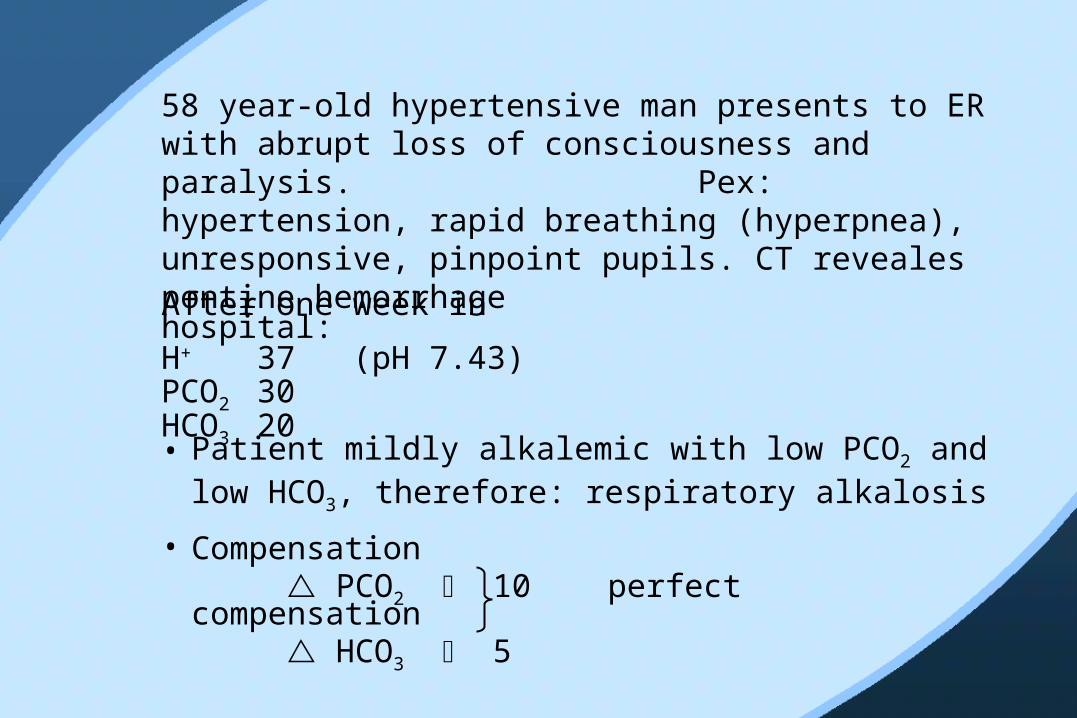
After one week in hospital:H+ 37 (pH 7.43)PCO2 30HCO3 20
58 year-old hypertensive man presents to ER with abrupt loss of consciousness and paralysis. Pex: hypertension, rapid breathing (hyperpnea), unresponsive, pinpoint pupils. CT reveales pontine hemorrhage
• Patient mildly alkalemic with low PCO2 and low HCO3, therefore: respiratory alkalosis
• Compensation PCO2 10 perfect compensation HCO3 5
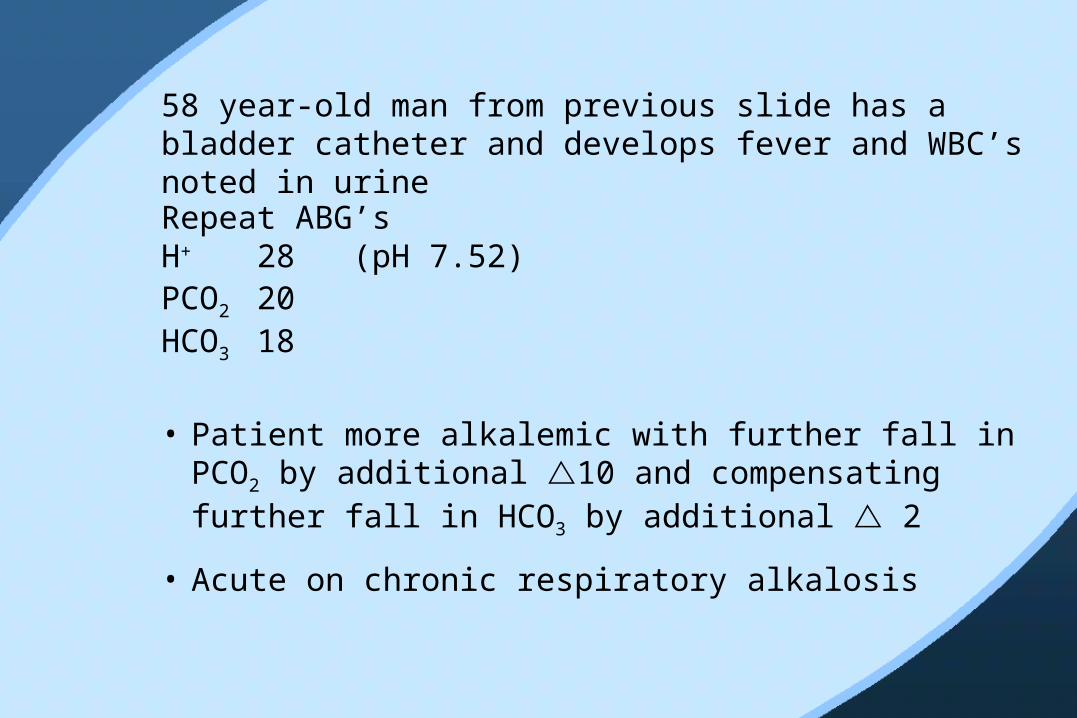
Repeat ABG’sH+ 28 (pH 7.52)PCO2 20HCO3 18
58 year-old man from previous slide has a bladder catheter and develops fever and WBC’s noted in urine
• Patient more alkalemic with further fall in PCO2 by additional 10 and compensating further fall in HCO3 by additional 2
• Acute on chronic respiratory alkalosis

Repeat ABG’s and chemistryH+ 50 (pH 7.30)PCO2 20HCO3 10Na+ 140Cl- 110 20 ( 8)
58 year-old man from previous slide now develops hypotension and shock
• L-lactate 8mmol/L
• Superimposed anion gap metabolic acidosis from septic shock lactic acidosis
• What if not aware of prior history and no prior ABG’s and given these values for the first time

H+ 50 (pH 7.30)PCO2 20HCO3 10Na+ 140Cl- 110 20
• Patient acidemic with low bicarbonate metabolic acidosis
• Expected PCO2 25 Observed PCO2 20 Therefore respiratory alkalosis • Anion gap 20 gap 8
Anion gap metabolic acidosis • But HCO3 15 > gap 8• Therefore: non anion gap metabolic acidosis
or compensation for respiratory alkalosis
Repeat lab testsH+ 100 (pH 7.00)PCO2 40HCO3 10Na+ 140 (gap 20)Cl- 110
58 year-old man from previous slide experiences cardiopulmonary arrest. After some initial confusion he is intubated and ventilated.
• Why has pH dropped ?
• Essentially behaving as uncompensated metabolic acidosis Anion gap component: sepsis and lactate Non-anion gap component: “post compensation for respiratory acidosis”
Repeat valuesH+ 40 (pH 7.40)PCO2 40HCO3 25Na+ 150Cl- 100
58 year-old man from previous slide with pontine hemorrhage, septic shock and ventilated, is given 3 ampules of NaHCO3 for acidemia
• pH, PCO2 and HCO3 are normal• Is there an acid-base disturbance ?• Was it right to give this much bicarbonate ?
Anion gap 25
• What would have been the right treatment ?
Metabolic AlkalosisProbably the worst thing to have and most complicated to understand
H+ = 25 •
PCO2
HCO3
• Primary increase in HCO3-
• Compensatory increase in PCO2

Compensation
• Not very consistent or reliable
• Approximately:
for every 1 HCO3
0.7 PCO2
• What limits this compensation and how could you prove it?

Pathogenesis
• Complicated and variable
• Two major categories:
Boring
Interesting

Boring
Bicarbonate load to someone with no kidneys
converse: if renal function is normal, the presence of metabolic alkalosis severe (interesting) homeostatic disturbance
Pathogenesis of Interesting Metabolic Acidosis• “Contraction” around HCO3
- space
• KCl depletion states
Volume expansion • mineralo corticoid
excess
Volume contraction• GI loss
- vomiting - GI suction- chloridorrhea (rare)
• Diuretics - loop - thiazide

“Contraction” Around HCO3 SpaceNormal 70Kg
TBW 42L
ECF14L
ICF28L
[HCO3] 25mmol/L 10mmol/L
HCO3 350 280
Total: 630
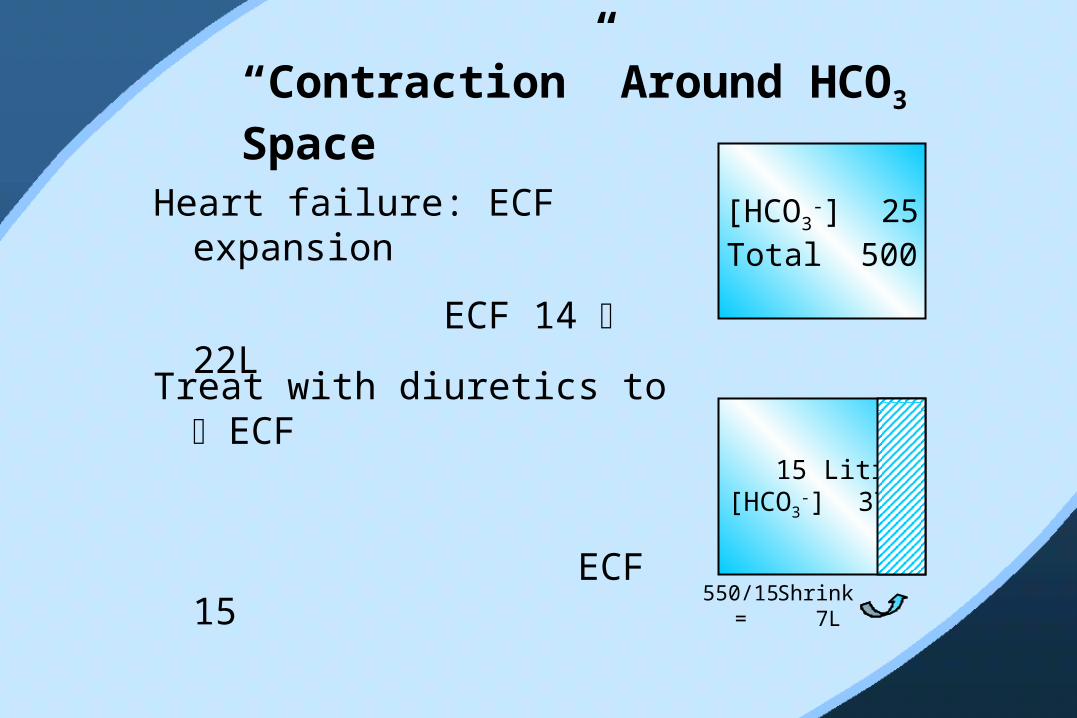
“Contraction” Around HCO3 Space
Heart failure: ECF expansion
ECF 14 22L
[HCO3-] 25
Total 500
Treat with diuretics to ECF
ECF 15
15 Litres[HCO3
-] 37
Shrink 7L
550/15 =
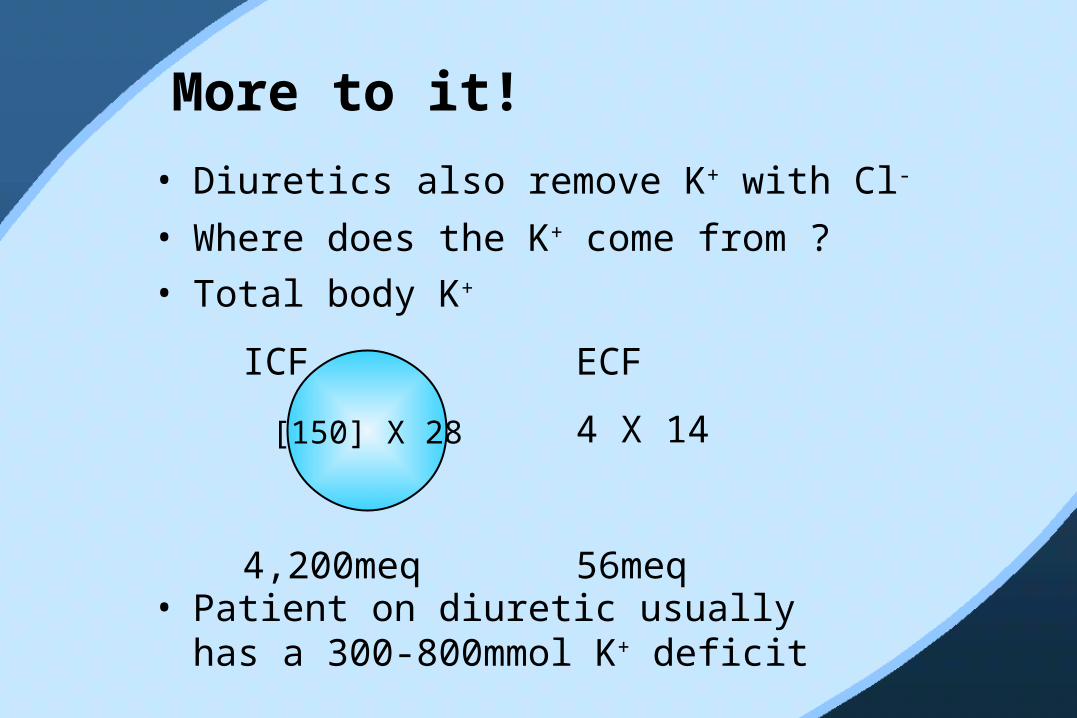
More to it!
• Diuretics also remove K+ with Cl-
• Where does the K+ come from ?• Total body K+
ICF ECF
4 X 14
4,200meq 56meq
[150] X 28
• Patient on diuretic usually has a 300-800mmol K+ deficit
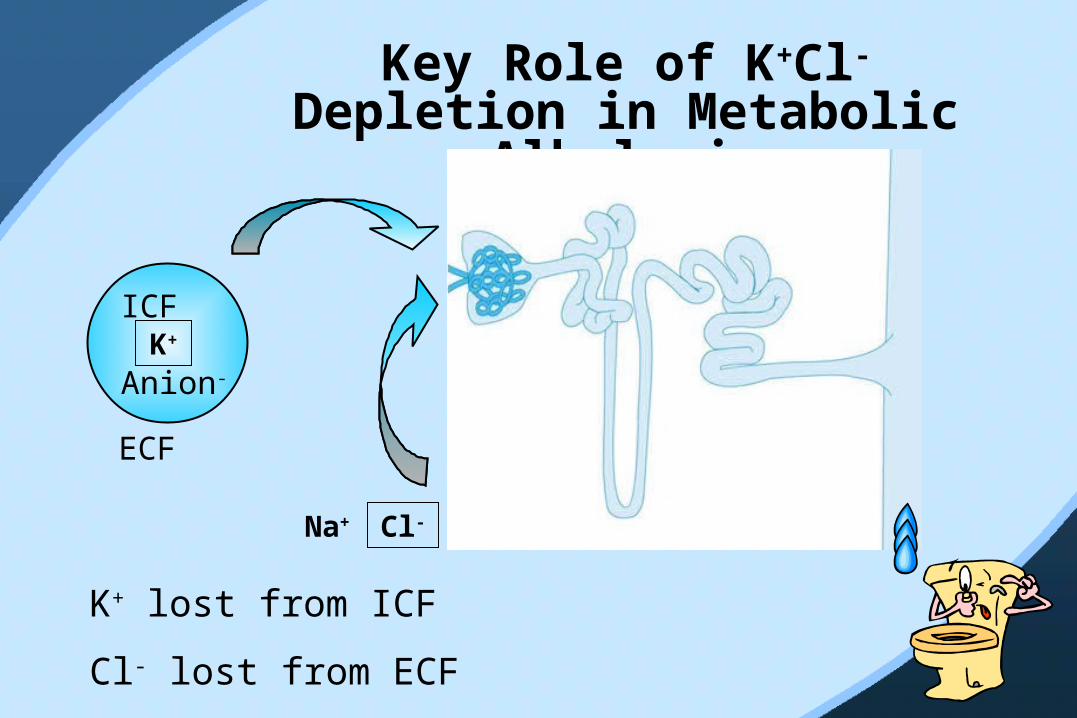
Key Role of K+Cl- Depletion in Metabolic
Alkalosis
ICF
Anion-
K+
Cl-Na+
ECF
K+ lost from ICF
Cl- lost from ECF
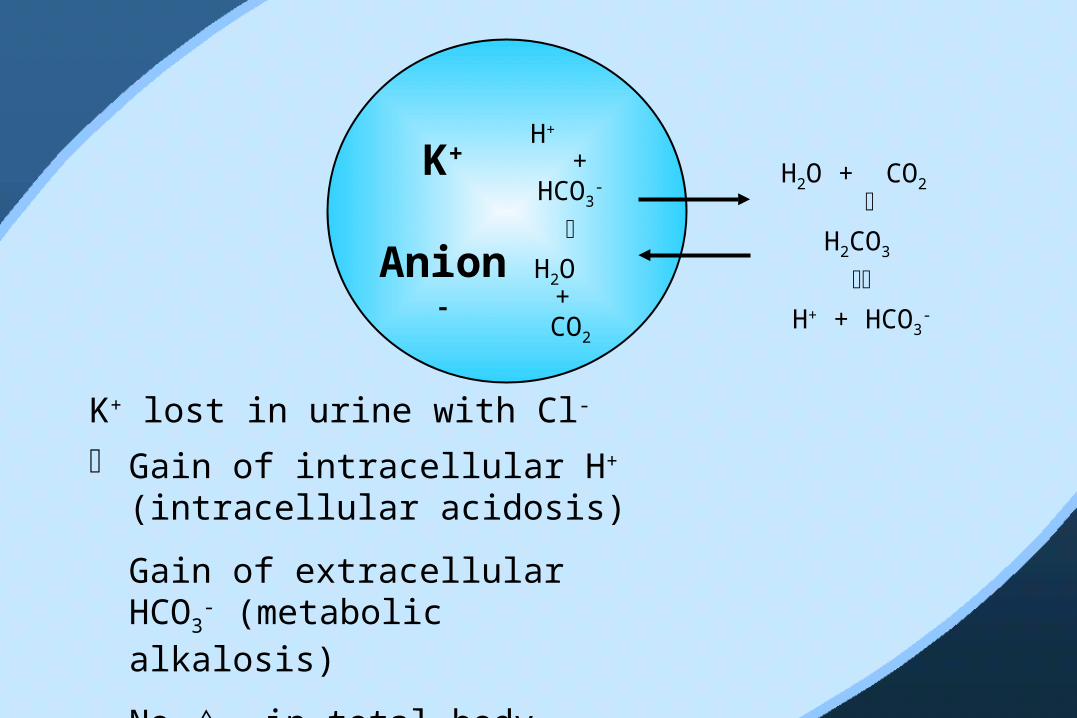
H+
+ HCO3
-
H2O
+ CO2
K+
Anion-
H2O + CO2
H2CO3
H+ + HCO3
-
K+ lost in urine with Cl-
Gain of intracellular H+ (intracellular acidosis)
Gain of extracellular HCO3-
(metabolic alkalosis)
No in total body buffer
Why do we care about acid-base disturbances ?
Clue to underlying disease
But are they bad in their own right ?
Answer: YES !
WHY ?
Main Reason:
Metabolic acidosis
Respiratory acidosis
Metabolic alkalosis
Intracellular
acidosis
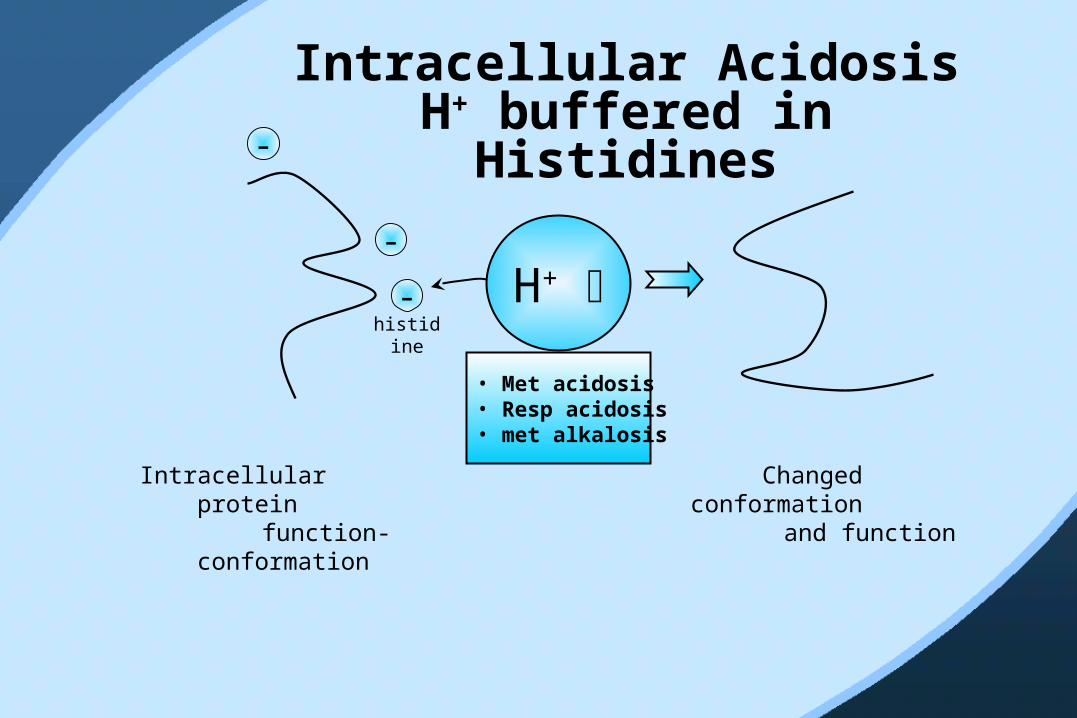
Intracellular Acidosis H+ buffered in Histidines
H+
• Met acidosis• Resp acidosis• met alkalosis
-
-
-
histidine
Intracellular protein
function-conformation
Changed conformation
and function
Summary of Diuretic-Induced Metabolic
Alkalosis1. Contraction
2. K+ depletion
3. Cl- depletion
4. Mineralocorticoid secondary to volume depletion

Two Most Common Causes of Metabolic
Alkalosis (with hypokalemia)
1. Diuretics (loop, thiazide)2. Vomiting (GI suction)

Key Ion transport Protein in the Nephron
*
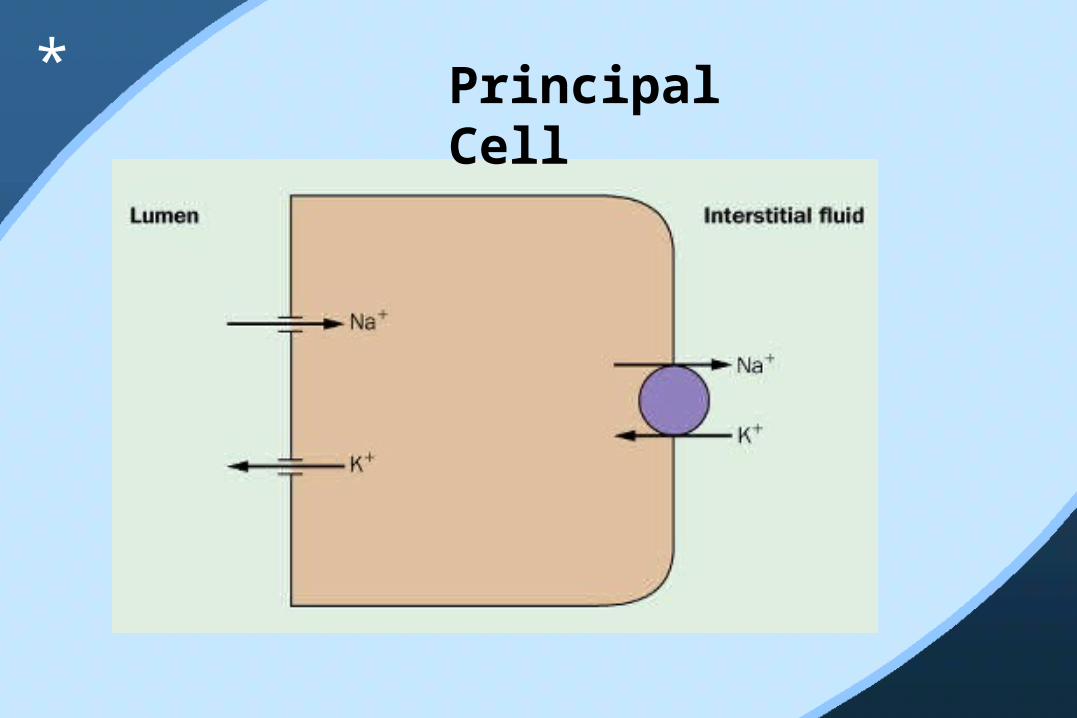
Principal Cell
*

Transport of Na+ in the Principal Cell of the Cortical
Collecting Duct
*

Secretion of H+ in the Intercalated Cell of the Cortical Collecting Duct
*
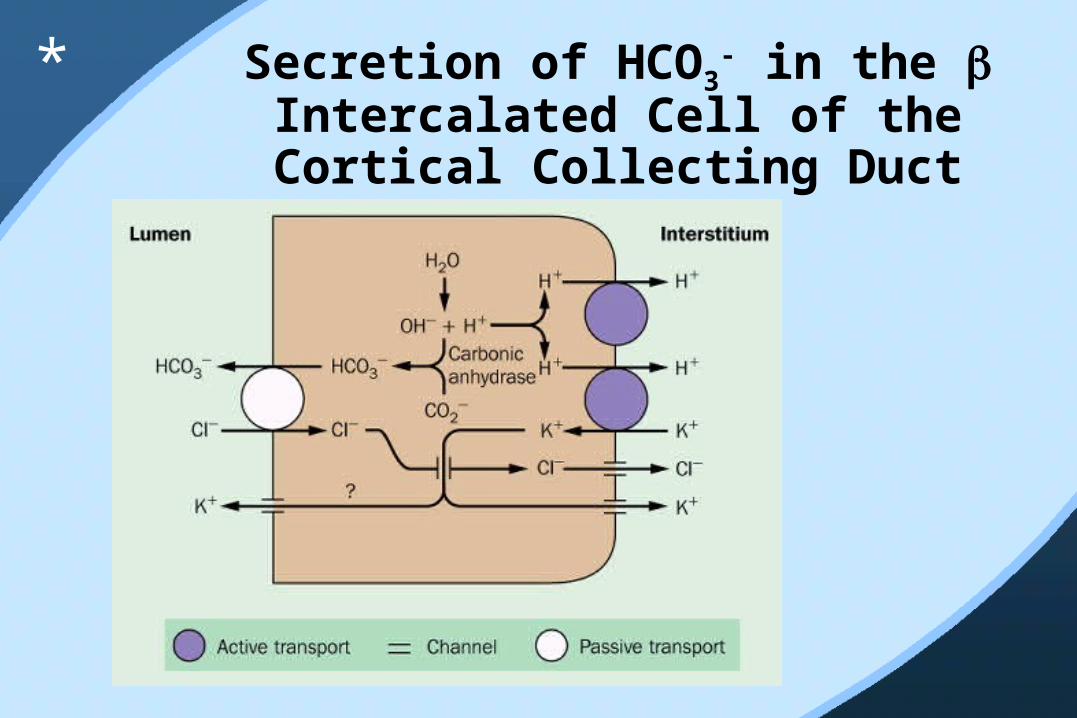
Secretion of HCO3- in the
Intercalated Cell of the Cortical Collecting Duct
*
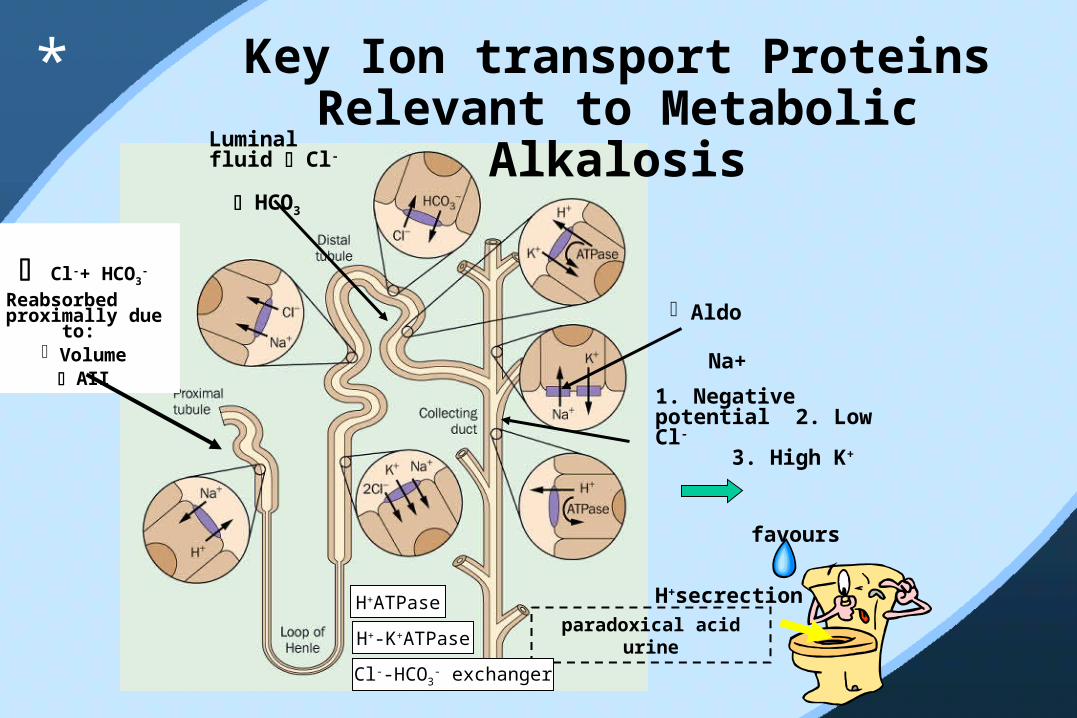
Key Ion transport Proteins Relevant to Metabolic
Alkalosis
Cl-+ HCO3-
Reabsorbed proximally due
to: Volume
AII
Luminal fluid Cl- HCO3
1. Negative potential 2. Low Cl- 3. High K+
favours
H+secrection
paradoxical acid urine
Aldo Na+
H+ATPase
H+-K+ATPase
Cl--HCO3- exchanger
*
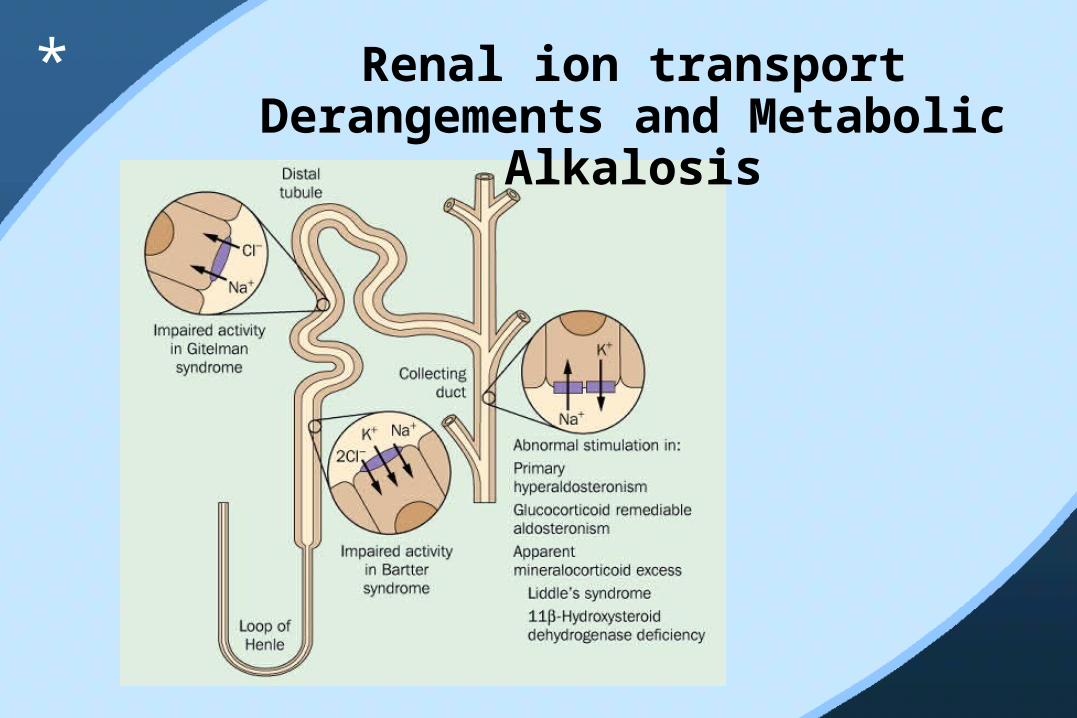
Renal ion transport Derangements and Metabolic
Alkalosis
*
H+ 31 (pH 7.49)PCO2 55HCO3 45PO2 68
45 year-old male smoker repeats reports one week of intractable profuse vomiting
PCO2 and HCO3-
• Metabolic alkalosis with respiratory compensation • Respiratory acidosis with metabolic compensation

Two ways to figure out:
1. Calculate A-a O2 gradient
= PIO2 – 1.25PCO2 – PaO2
= 150 – 69 – 68= 13Normal: lung disease not sufficient to cause chronic respiratory acidosis
2. Treat presumed metabolic alkalosis and expect PCO2 to normalize (and PO2 to rise)
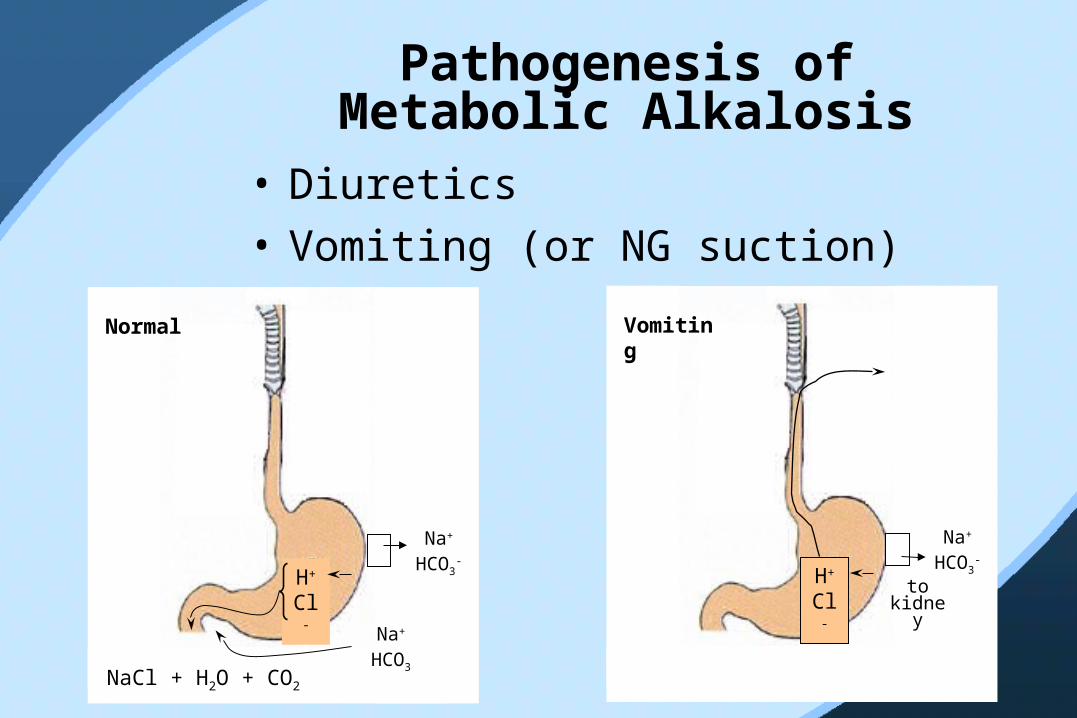
Pathogenesis of Metabolic Alkalosis
• Diuretics• Vomiting (or NG suction)
H+ Cl-
NaCl + H2O + CO2
Na+
HCO3
Na+
HCO3-
Normal
H+ Cl-
to kidne
y
Na+
HCO3-
Vomiting
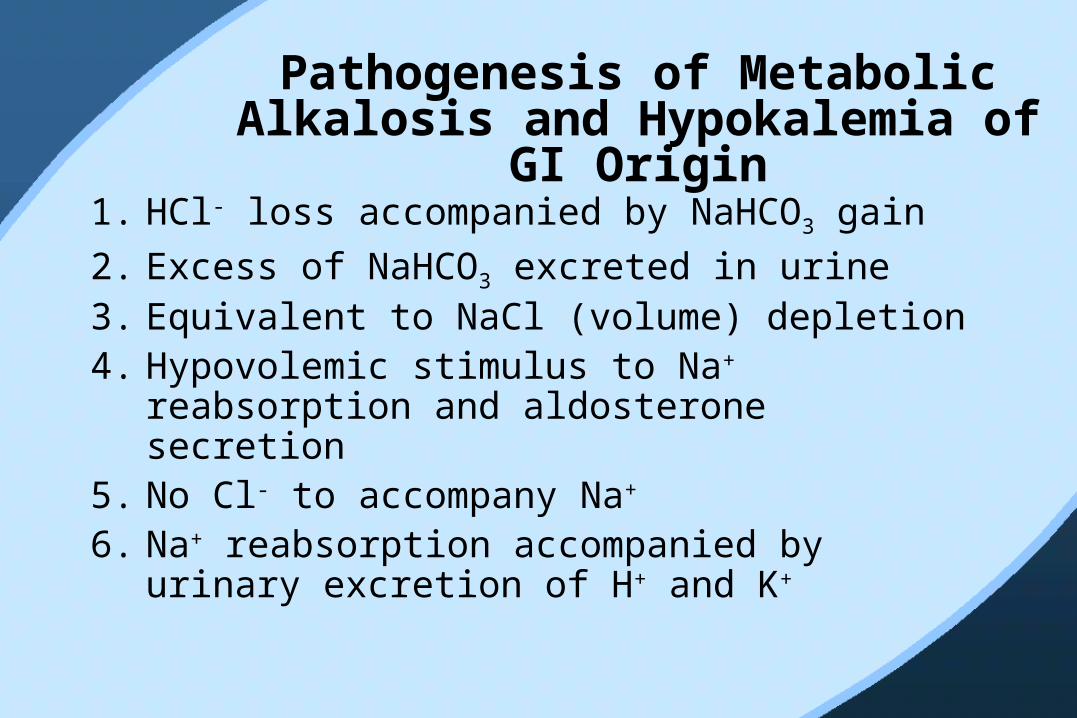
Pathogenesis of Metabolic Alkalosis and Hypokalemia of
GI Origin1. HCl- loss accompanied by NaHCO3 gain
2. Excess of NaHCO3 excreted in urine 3. Equivalent to NaCl (volume) depletion4. Hypovolemic stimulus to Na+
reabsorption and aldosterone secretion5. No Cl- to accompany Na+ 6. Na+ reabsorption accompanied by
urinary excretion of H+ and K+
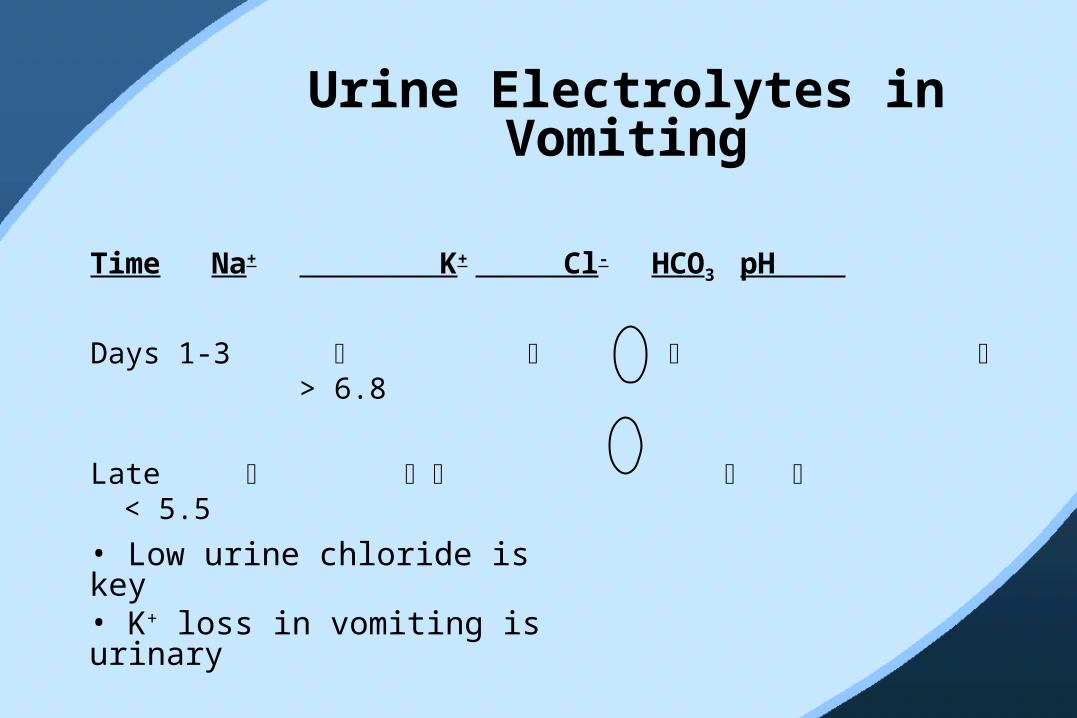
Urine Electrolytes in Vomiting
Time Na+ K+ Cl- HCO3
pH
Days 1-3 > 6.8
Late < 5.5
• Low urine chloride is key• K+ loss in vomiting is urinary

Loss of hydrogen A. Gastrointestinal loss
1. Removal of gastric secretions - vomiting or nasogastric suction 2. Antacid therapy, particularly with cation-exchange resin3. Chloride-losing diarrhea
B. Renal Loss 1. Loop or thiazide-type diuretics2. Mineralocorticoid excess3. Postchronic hypercapnia4. Low chloride intake 5. High-dose carbenicillin or other penicillin derivative 6. Hypercalcemia, including the milk-alkali syndrome
C. H+ movement into cells 1. Hypokalemia 2. Refeeding (?)
Most common causes shown in blue
Causes of Metabolic Alkalosis
*
Retention of bicarbonate A. Massive blood transfusionB. Administration of NaHACO3 C. Milk-alkali syndrome
Contraction alkalosisA. Loop or thiazide-type diureticsB. Gastric losses in patients with achlorhydia C. Sweat losses in cystic fibrosis
Causes of Metabolic Alkalosis (Cont.)
*
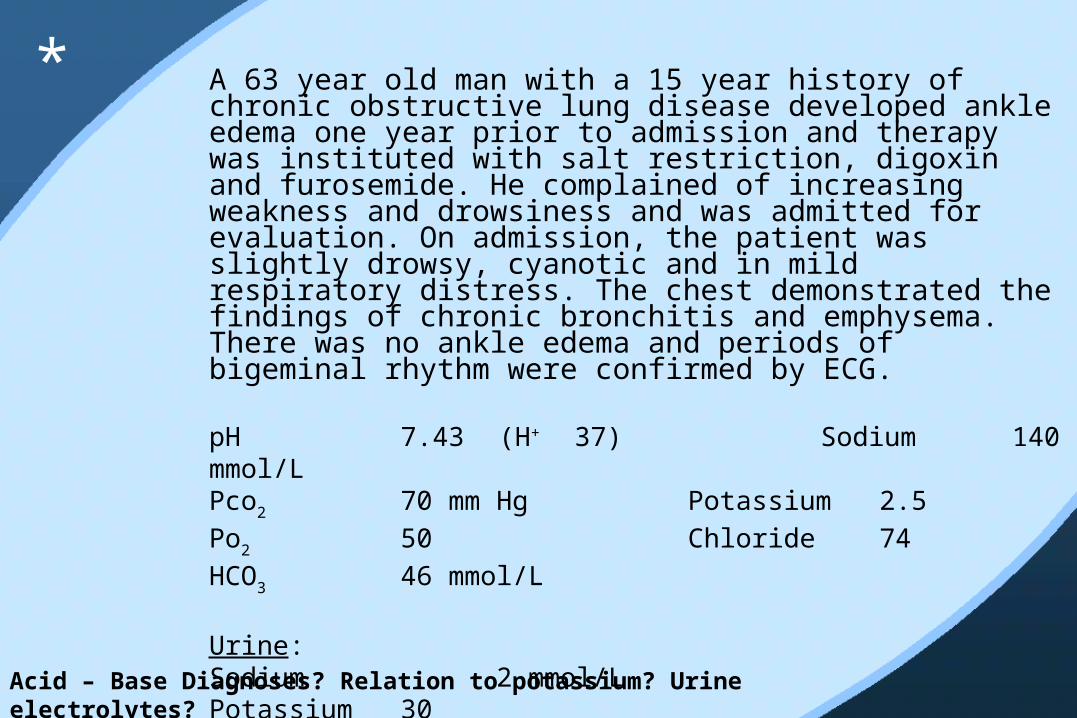
A 63 year old man with a 15 year history of chronic obstructive lung disease developed ankle edema one year prior to admission and therapy was instituted with salt restriction, digoxin and furosemide. He complained of increasing weakness and drowsiness and was admitted for evaluation. On admission, the patient was slightly drowsy, cyanotic and in mild respiratory distress. The chest demonstrated the findings of chronic bronchitis and emphysema. There was no ankle edema and periods of bigeminal rhythm were confirmed by ECG.
pH 7.43 (H+ 37) Sodium 140 mmol/LPco2 70 mm Hg Potassium 2.5Po2 50 Chloride 74HCO3 46 mmol/L Urine:Sodium 2 mmol/LPotassium 30Chloride 1
*
Acid – Base Diagnoses? Relation to potassium? Urine electrolytes?

The patient’s diuretic was discontinued, he was given supplemental KCl by mouth, and within four days his rhythm and ECG had normalized, and he felt stronger and more alert. Repeat evaluation showed: pH 7.32 Sodium 140 mmol/LPco2 65 mm Hg Potassium 4.4Po2 60 Chloride 100HCO3 33 mmol/L
*
Is he better or worse now with the lower pH? What treatment helped him?
H+ pH PCO2 HCO3 ___ Other________
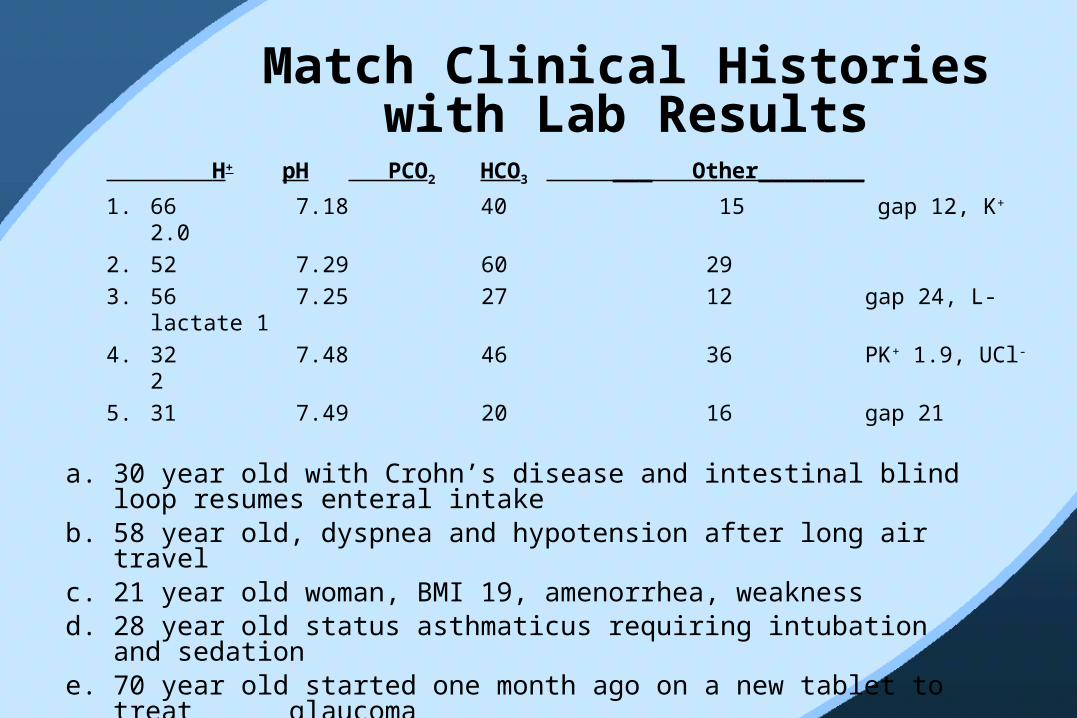
1. 66 7.18 40 15 gap 12, K+ 2.02. 52 7.29 60 293. 56 7.25 27 12 gap 24, L-lactate 14. 32 7.48 46 36 PK+ 1.9, UCl- 25. 31 7.49 20 16 gap 21
Match Clinical Histories with Lab Results
a. 30 year old with Crohn’s disease and intestinal blind loop resumes enteral intake
b. 58 year old, dyspnea and hypotension after long air travelc. 21 year old woman, BMI 19, amenorrhea, weaknessd. 28 year old status asthmaticus requiring intubation and
sedatione. 70 year old started one month ago on a new tablet to treat
glaucoma

pHank You!

Apetit!
Bon
*





























