Embed Size (px)
Citation preview

Accountability in Breast and Colorectal Cancer Care
Omar M. Rashid MD, JD
Complex General Surgical Oncology Fellow

Introduction
Over the last 15 years there has been a coordinated effort
to improve the quality of cancer care in the U.S.
&
to transition cancer care to “value-based care.”

IntroductionProvide background on these measures
Review salient issues in quality reporting
Present the experience at Moffitt
Discuss future directions in quality

Introduction1999: “Ensuring Quality Cancer Care”
Conclusions:
There is a wide quality gap for many Americans in their experience within the cancer care delivery system.
There is a need to implement a quality monitoring system utilizing a core set of indicators.

IntroductionCollaborative effort of multiple national organizations, including ACS, the National Initiative for Cancer Care Quality (NICCQ):
Review of the literature
36 quality measures in breast cancer
25 quality measures in colorectal cancer
Evaluation of care provided to patients in 5 U.S. cities diagnosed in 1998 with Stage I - III breast cancer and Stage II - III colorectal cancer.

IntroductionCollaborative effort of multiple national organizations, including ACS, the National Initiative for Cancer Care Quality (NICCQ):
Adherence to breast cancer metrics :
13 - 97% individual indicators<85% for 18/36 indicators
Adherence to colorectal cancer metrics:
57 - 93% individual indicators<85% for 14/25 indicators

IntroductionCollaborative effort of multiple national organizations, the Quality Oncology Practice Initiative (QOPI):
Focused on individual institutions (address criticisms of focusing on population based data)
Provided medical oncology practices tool for self-examination using medical record chart abstraction
Evaluated 7 oncology groups in the U.S. in 11 quality indicators at 2 time points, 6 months apart (e.g. patient safety, evidence based and patient-centered care).
Findings: significant variation in adherence to 8 of the 11 indicators (73%), supporting NICCQ findings

IntroductionCollaborative effort of multiple national organizations, including the ACS Commission on Cancer, ASCO, and NCCN, facilitated by the National Quality Forum (NQF):
Evaluate quality measures for breast and colorectal cancer to determine which should be implemented as accountability measures
Accountability measures are used for public reporting, payment incentive programs, and provider selection by consumers, health plans, or purchasers.

IntroductionCollaborative effort of multiple national organizations, including the ACS Commission on Cancer, ASCO, and NCCN, facilitated by the National Quality Forum (NQF) formed two panels made up of breast and colorectal experts in surgery, radiotherapy, medical oncology, health care consumers and health services research:
Importance: the extent to which a measure reflects variation that has the potential for improvement;
Scientific acceptability: that a measure is reliable, valid, precise, and adaptable to patient preference;
Usability: information produced as part of the measure could be used to make decisions and/or take actions, and that reported performance levels were statistically, and clinically meaningful;
Feasibility: that data can be obtained within the normal flow of clinical care and that implementation of the measure was achievable.

IntroductionCollaborative effort of multiple national organizations, including the ACS Commission on Cancer (ACoC), ASCO, and NCCN, facilitated by the National Quality Forum (NQF):
4 process-based accountability measures in cancer
care:
3 for breast cancer
1 for colorectal cancer
1 outcome-based accountability measure in colorectal cancer
1 surveillance measure in colorectal cancer

Breast Cancer Process Measure
Tamoxifen or third generation aromatase inhibitor is considered or administered within 1 year (365 days) of diagnosis for women with AJCC T1cN0M0, or Stage II or Stage III hormone receptor positive breast cancer. (HT)
Case Eligibility Criteria:
• Women only
• Adults – patients >=18 at time of diagnosis
• First or only cancer diagnosis
• Primary tumors of the breast
• Epithelial tumors required to be staged according to the AJCC 6th and 7th Editions.
• Solid tumors only
• Invasive tumors only
• No reported clinical or pathological evidence of metastatic disease
• All or part of first course of treatment was performed at Moffitt Cancer Center

Breast Cancer Process Measure
Radiation therapy is administered within 1 year (365 days) of diagnosis for women under age 70 receiving breast conserving surgery for breast cancer. (BCS)
Case Eligibility Criteria:
• Women only
• Adults – patients >=18 at time of diagnosis
• First or only cancer diagnosis
• Primary tumors of the breast
• Epithelial tumors required to be staged according to the AJCC 6th and 7th Editions.
• Solid tumors only
• Invasive tumors only
• No reported clinical or pathological evidence of metastatic disease
• All or part of first course of treatment was performed at Moffitt Cancer Center

Breast Cancer Process Measure
Combination chemotherapy is considered or administered within 4 months (120 days) of diagnosis for women under 70 with AJCC T1cN0M0, or Stage II or III hormone receptor negative breast cancer. (MAC)
Case Eligibility Criteria:
• Women only
• Adults – patients >=18 at time of diagnosis
• First or only cancer diagnosis
• Primary tumors of the breast
• Epithelial tumors required to be staged according to the AJCC 6th and 7th Editions.
• Solid tumors only
• Invasive tumors only
• No reported clinical or pathological evidence of metastatic disease
• All or part of first course of treatment was performed at Moffitt Cancer Center

Colorectal Cancer Process Measure
Adjuvant chemotherapy is considered or administered within 4 months (120 days) of diagnosis for patients under the age of 80 with AJCC Stage III (lymph node positive) colon cancer. (ACT)
Case Eligibility Criteria:
• Adults – patients >=18 at time of diagnosis
• First or only cancer diagnosis
• Primary tumors of the colon and rectum
• Epithelial tumors required to be staged according to the AJCC 6th and 7th Editions.
• Solid tumors only
• Invasive tumors only
• No reported clinical or pathological evidence of metastatic disease
• All or part of first course of treatment was performed at Moffitt Cancer Center

Colorectal Cancer Outcome Measure
At least 12 regional lymph nodes are removed and pathologically examined for resected colon cancer. (12RLN)
Case Eligibility Criteria:
• Adults – patients >=18 at time of diagnosis
• First or only cancer diagnosis
• Primary tumors of the colon and rectum
• Epithelial tumors required to be staged according to the AJCC 6th and 7th Editions.
• Solid tumors only
• Invasive tumors only
• No reported clinical or pathological evidence of metastatic disease
• All or part of first course of treatment was performed at Moffitt Cancer Center

Colorectal Cancer Surveillance Measure
Radiation therapy is considered or administered within 6 months (180 days) of diagnosis for patients under the age of 80 with clinical or pathologic AJCC T4N0M0 or Stage III receiving surgical resection for rectal cancer.
Although this measure was not endorsed by the NQF, it is supported by the ACoC, the National Comprehensive Cancer Network (NCCN), and the American Society of Clinical Oncology (ASCO).

Cancer Program Practice Profile Reports (CP3R)
The Web-based Cancer Program Practice Profile Reports (CP3R) offer local providers comparative information to assess adherence to and consideration of standard of care therapies for major cancers.
This reporting tool provides a platform from which to promote continuous practice improvement to improve quality of patient care at the local level and also permits hospitals to compare their care for these patients relative to that of other providers.
The aim is to empower clinicians, administrators, and other staff to work cooperatively and collaboratively to identify problems in practice and delivery and to implement best practices that will diminish disparities in care across CoC-accredited cancer programs.

The Commission on Cancer has developed a mechanism, the Rapid Quality Reporting System (RQRS), that enables accredited cancer programs to report data on patients concurrently, provide hospitals notification of treatment expectations, and show a hospital its year-to-date concordance rate relative to the state, other similar hospitals, and hospitals at the national level.
RQRS Eligibility
1) Cancer program is currently CoC accredited.
2) All CoC programs wishing to participate in RQRS must have a Hospital registrar, Cancer Program Administrator, Cancer Liaison Physician and Cancer committee chair with CoC Datalinks access and up-to-date unique contact (e- mail) information. Where the CLP and the CCC are the same individual, this requirement is waived.

Absolute adherence to the quality measures is collected and reported without explanation for reasons for non-adherence.
The threshold requirement of 90% or greater is set as the standard for quality care.

Quality in Cancer Care
How does this approach compare to other efforts to improve the quality of cancer care?
How well do these metrics actually measure quality?
Will improving compliance actually improve quality?

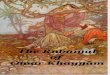
Cancer CenterAccreditation
Centralized Gastric Cancer
Treatment
Treatment Guidelines
Uniform Surgical
Approach
Process Measures for Gastric
Cancer
Public Reporting of Institutional
Survival Outcomes
Public Health Early
Detection Screening
Efforts
U.S. X X
Europe X
Japan X X X X X X
Korea X X X
China X X X
Table 2. Summary of systems-based measures to improve gastric cancer care and outcomes, as instituted by country.
*Rashid OM, Prabhakaran S, Song K, Wong J. Gastric Cancer: Risk Factors, Treatment, and Clinical Outcomes. “Geographical Differences in Risk Factors, Systems, and Outcomes in Gastric Cancer.” (In Press)

Quality in Cancer Care
A retrospective review was performed of all eligible cases of breast and colon cancer reported to the American College of Surgeons (ACS) at a single institution from 2008 – 2012.
Coding for compliance was performed using the ACS Commission on Cancer standards for accountability measures for breast and colon cancer.
Timing-based quality indicators for stage I-III breast cancer include radiation therapy administered within 1 year (BXT), hormonal therapy within 1 year (BHT), and adjuvant chemotherapy within 120 days of diagnosis (BAT); for stage III colon cancer, the measure is adjuvant chemotherapy within 120 days of diagnosis (CCT).

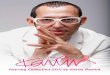
Breast Cancer Process Measure
312 BAT
272 Adherent 40 Non-adherent
5 Lost35 Delayed Treatment
14.8 DaysDX AT
10.6 Days 13.5 Days 27 Days
83.7 DaysDX AT
16.2 Days 49.1 Days 98.3 Days
1stVisit
Surgery Med Onc
1stVisit
Surgery Med Onc

BAT A*
N=312
BAT NA*N=40
p value
Diagnosis to Adjuvant Therapy 65.1±
27.8
147.4±
41.3
3.7x10-16
Diagnosis to 1st visit 14.8±
19.0
83.7±
42.1
1x10-8
1st visit to Surgery 10.6±
6.3
16.2±
4.8
0.1
Surgery to Med/Rad Onc 13.5±
7.3
49.1±
13.8
2x10-19
Med/Rad Onc to Adjuvant Therapy 27.0±
14.5
98.3±
27.5
2x10-19

BAT
Number of cases 312 (%)
Non-adherent 40 (12.8)
REASON FOR NON-ADHERENCE N=40
-Lost to follow up 5 (12.5)
-Patient refusal 0 (0)
-Treatment delay 35 (87.5)
REASON FOR DELAY N=35
--Patient choice 11 (31.4)
--Outside delay 19 (54.3)
--Diagnosis by suspicion 4 (11.4)
--Insurance delay 1 (2.9)
--Other procedure 0 (0)
--2nd malignancy 0 (0)
--Complications 0 (0)

Colorectal Cancer Process Measure
122 CCT
106 Adherent 16 Non-adherent
2 Lost14 Delayed Treatment
6.7 Days DX CT
10 Days 36.6 Days 17.9 Days
38.2 Days DX CT Surgery
35.7 Days 63.2 Days 24.7 Days
1stVisit
Med Onc Surgery
1stVisit
Med Onc

CCT A
N=106
CCT NA
N=16
p value
Dx to Adjuvant Therapy
68.7±24.5 159.5±51 2x10-6
Dx to 1st visit
6.7±12.2 38.2±30.8 0.005
1st visit to Surgery
10.0±14.5 35.7±22.7 0.004
Surgery to Med Onc
36.6±11.4 63.2±42.7 0.04
Med Onc to Adjuvant Therapy
17.9±18.9 24.7±19.8 0.26

CCT
Number of cases 122 (%)
Non-adherent 16 (13.1)
REASON FOR NON-ADHERENCE N=16
-Lost to follow up 2 (12.5)
-Patient refusal 0 (0)
-Treatment delay 14 (87.5)
REASON FOR DELAY N=14
--Patient choice 6 (42.9)
--Outside delay 4 (28.6)
--Diagnosis by suspicion 2 (14.3)
--Insurance delay 1 (7.1)
--Other procedure 0 (0)
--2nd malignancy 0 (0)
--Complications 1 (7.1)

Breast Cancer Process Measure
28.4 DaysXTSurgery
12 Days 37.6 Days 75.3 Days
48.7 DaysDX XT
15 Days 142.2 Days 284.4 Days
897 BXT
842 Adherent 55 Non-adherent
14 Lost 11 Refused30 Delayed Treatment
DX1stVisit
Rad Onc
1stVisit
Surgery Rad Onc

BXT A*
N=842
BXT NA*N=55
p value
Diagnosis to Adjuvant Therapy 112.9±
74.5
426.6±
166.6
2x10-5
Diagnosis to 1st visit 28.4±
36.2
48.7±
64.7
0.03
1st visit to Surgery 12.0±
5.6
15.0±
6.1
2x10-4
Surgery to Med/Rad Onc 37.6±
24.8
142.2±
55.5
2x10-5
Med/Rad Onc to Adjuvant Therapy 75.3±
49.6
284.37±
111.1
2x10-5

BXT
Number of cases 897 (%)
Non-adherent 55 (6.1)
REASON FOR NON-ADHERENCE N=55
-Lost to follow up 14 (25.5)
-Patient refusal 11 (20)
-Treatment delay 30 (54.5)
REASON FOR DELAY N=30
--Patient choice 4 (13.3)
--Outside delay 22 (73.3)
--Diagnosis by suspicion 2 (6.7)
--Insurance delay 1 (1.8)
--Other procedure 0 (0)
--2nd malignancy 0 (0)
--Complications 1 (1.8)

Breast Cancer Process Measure
35.5 Days
1,349 Adherent 84 Non-adherent
35 Lost49 Delayed Treatment
1,433 BHT
DX HT12.8 Days 50.4 Days 100.8 Days
76.8 DaysDX HT
15 Days 142.0 Days 283.9 Days
1stVisit
Surgery Med Onc
1stVisit
Surgery Med Onc

BHTA*
N=1349
BHT NA*
N=84
p value
Diagnosis to Adjuvant Therapy 198.3±
82.6
425.9±
99.1
4x10-20
Diagnosis to 1st visit 35.5±
42.9
76.75±
81.3
9x10-5
1st visit to Surgery 12.8±
5.3
15.0±
5.0
6x10-5
Surgery to Med/Rad Onc 50.4±
28.5
142.0±
33.0
8x10-23
Med/Rad Onc to Adjuvant Therapy 100.8±
56.9
283.9±
66.0
8x10-23

BHT
Number of cases 1,433 (%)
Non-adherent 84 (5.9)
REASON FOR NON-ADHERENCE N=84
-Lost to follow up 35 (41.7)
-Patient refusal 0 (0)
-Treatment delay 49 (58.3)
REASON FOR DELAY N=49
--Patient choice 21 (42.9)
--Outside delay 12 (24.5)
--Diagnosis by suspicion 5 (10.2)
--Insurance delay 2 (4.1)
--Other procedure 1 (2)
--2nd malignancy 1 (2)
--Complications 6 (12.2)

Quality in Cancer Care
Our center averaged an annual compliance with the adjuvant therapy measures of approximately 90%.
Larger scale studies are indicated to determine whether:
refinements in coding guidelines that account for patient preferences
clear diagnosis dates
cross-facility care
could better reflect quality of care, and also promote improved patient-centered multidisciplinary management.

Quality in Cancer Care

Quality in Cancer Care

September, 2013: “Delivering high-quality cancer care: charting a new course for a system in crisis”
Annual cost of cancer care from 2004 to 2010 increased from $72 billion to $125 billion.
Recommendations:
more patient centered care
better coordination among disciplines
mandatory national publicly reported cancer care quality program
develop “meaningful quality measure for cancer care with a focus on outcome measures”

1. Hewitt M, Simone JV: Ensuring quality cancer care. Washington, D.C, Institute of Medicine and National Research Council, 1999
2. Schneider EC, Epstein AM, Malin JL, et al: Developing a system to assess the quality of cancer care: ASCO's National Initiative on
Cancer Care Quality. Journal of Clinical Oncology 15:2985-2991, 2004
3. Malin JL, Schneider EC, Epstein AM, et al: Results of the National Initiative for Cancer Care Quality: how can we improve the quality of
cancer care in the United States? Clinical Oncology 24:626-634, 2006
4. Neuss MN, Desch CE, McNiff KK, et al: A process for measuring the quality of cancer care: the Quality Oncology Practice Initiative. Journal of
Clinical Oncology 23:6233-6239, 2005.
5. Desch CE et al. American Society of Clinical Oncology/National Comprehensive Cancer Network Quality Measures. JCO, vol 26, num
21, 2008.
6. American Society of Clinical Oncology/National Comprehensive Cancer Network Quality Measures. JCO, vol 26, num 21, 2008).
7. Stewart, Andrew K., et al. "The Rapid Quality Reporting System: A new quality of care tool for CoC-accredited cancer programs." J
Registry Manag 38.1 (2011): 61-63.
8. Levit, Laura, et al. "Delivering high-quality cancer care: charting a new course for a system in crisis." Institute of Medicine. Washington,
DC: Institute of Medicine (2013).
9. Mariotto, A. B., K. R. Yabroff, Y. Shao, E. J. Feuer, and M. L. Brown. 2011. Projections of the cost of cancer care in the United States:
2010-2020. Journal of the National Cancer Institute 103(2):117-128.
10. Rashid OM, Prabhakaran S, Song K, Wong J. Gastric Cancer: Risk Factors, Treatment, and Clinical Outcomes. “Geographical
Differences in Risk Factors, Systems, and Outcomes in Gastric Cancer.” (In Press)
References

AcknowledgmentsDavid Shibata, MD, FACS Chief of Colorectal Oncology
Christine Laronga, MD, FACSChair of FL ACS CoC
Tom W. Ross, MS, RPh Director of quality and safety
Karen A. Coyne RN, CTR, MScDirector cancer registry
Angela Reagan,Coordinator, Research Program
Vernon K. Sondak, MD, FACSProgram Director

QUESTIONS ???????







![asksource.info1402525][Dissert… · Web viewDisability under Occupation: . At the Congruence between Conflict, Religion, & Society in Palestine. Name: Omar Rashid. Student Registration](https://img.pdfslide.us/doc/110x75/5fd686b13b8df653b56e16ea/1402525dissert-web-view-disability-under-occupation-at-the-congruence-between.jpg)