Embed Size (px)
Citation preview

British Journal of Urology (1998), 82, 290–291
POIN T OF TECHNIQU E
Access to the distal ureter after failure of direct visualureteroscopyP. ASLAN, B. MALLOY and G.M. PREMINGERThe Comprehensive Kidney Stone Center, Division of Urology, Department of Surgery, Duke University Medical Center, Durham,North Carolina, USA
Indications
Refinements in ureteroscope design have clearly playedan important part in the advancement of upper tractendoscopic surgery. The semi-rigid ureteroscope, whichcontains fibre-optic bundles, has some degree of flexi-bility that facilitates access to the ureter [1]. Despitethese advances, there are times when the semi-ureteroscope cannot negotiate the angle required togain access to the ureter, thereby limiting the oppor-tunity to perform minimally invasive surgery. Wedescribe a technique to gain access to the distal ureterwhen direct visual ureteroscopy with a semi-rigidureteroscope is not possible, using a ureteroscopicsheath originally designed for repeated access to therenal pelvis during flexible ureteroscopy. We used thistechnique in two patients; the first a 39-year-old manwith a ureterosigmoidostomy who had a 3×1.5 cmstone in his distal left ureter; and the second a 45-year-old woman with a ureteric injury after Burch colpo-suspension. Treated initially with antegrade insertion ofa ureteric stent, she subsequently had 6 cm of retainedstent in her distal left ureter.
Methods
In both cases, a percutaneous wire was placed acrossthe obstruction and into the bladder or reservoir. Atcystoscopy, the wire was grasped and a 10 cm, 18 Fballoon dilator was positioned over the wire, into theintramural ureter. An 18 F ureteric access sheath (Cook
a
b
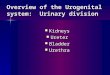
Fig. 1. a, Flexible ureteroscopy sheath and b, the fluoroscopicUrological, Spencer, IN, USA) was passed over the wireimage showing the flexible ureteroscopy sheath passing over theunder fluoroscopic guidance and gently manoeuvredguide-wire and into the left ureter.into the distal ureter, up to the stone or retained stent
(Fig. 1a). The semi-rigid ureteroscope passed easilythrough the sheath, adjacent to the wire, to the area ofinterest (Fig. 1b). The stone was completely fragmented, Comparison with other methodsand the stent removed.
In these two patients, the pathology was in the distalureter, inaccessible to routine semi-rigid ureteroscopy.To manage the problem retrogradely, the only alternative
290 © 1998 British Journal of Urology 82, 290–291

POINT OF TECHNIQUE 291
option was to use a flexible ureteroscope. However, the Referencessmall working channel of the flexible ureteroscope (com- 1 Conlin MJ, Marberger M, Bagley DH. Ureteroscopy: develop-
ment and instrumentation. Urol Clin North Am 1997;bined with limited instrumentation) makes this approach24: 25–42cumbersome, if not impossible. Other approaches have
2 Sullivan JW, Grabstald H, Whitmore WF Jr. Complicationsincluded ESWL for small, simple stones located in theof ureteroileal conduit with radical cystectomy: review ofrenal pelvis or the ureter, and was unsuitable in the336 cases. J Urol 1980; 124: 797–801present case [2]. An antegrade, percutaneous approach
would have required the use of the flexible ureteroscope,again with the attendant limitations of the small instru-ments required to treat the large stone or remove the
Authorsretained stent. Alternatively, both may have been treatedP. Aslan, MD, Urology Fellow.with an open procedure, with a significant increase inB. Malloy, MD, Urology Resident.post-operative morbidity.G.M. Preminger, MD, Professor of Urology.Correspondence: Dr G.M. Preminger, Division of Urology,Department of Surgery, Duke University Medical Center, DUMCAdvantagesBox 316, Room 305 Baker House, Durham, North Carolina,
In both cases, a minimally invasive procedure could be USA.performed. Although these types of cases are uncommon,we recommend that the urologist performing ureteros-copy have this ureteric sheath available to facilitateaccess to the ureter when routine access is not possible.
© 1998 British Journal of Urology 82, 290–291