Embed Size (px)
Citation preview
Central Annals of Vascular Medicine & Research
Cite this article: Aktan I, Abusamaan M, Shaw P, Battle R, Flors L, et al. (2017) Vasculo-Behçet’s Disease with Intra-Cardiac Mass, Pulmonary Artery Throm-bus, and Pulmonary Artery Aneurysms. Ann Vasc Med Res 4(1): 1047.
*Corresponding authorIdil Aktan, Department of Medicine, University of Virginia, 50 Belmont Ave, Apt 1010, Bala Cynwyd, PA 19004, USA, Tel: 610-639-4920; Email:
Submitted: 28 November 2016
Accepted: 14 December 2016
Published: 02 January 2017
ISSN: 2378-9344
Copyright© 2017 Aktan et al.
OPEN ACCESS
Keywords•Vasculo-behçet’s disease•Intra-cardiac mass•Pulmonary artery aneurysm
Case Report
Vasculo-Behçet’s Disease with Intra-Cardiac Mass, Pulmonary Artery Thrombus, and Pulmonary Artery AneurysmsIdil Aktan1*, Mazen Abusamaan2, Peter Shaw2, Robert Battle2, Lucia Flors3, Christopher M. Kramer2,3, and Aditya M. Sharma2
1Department of Medicine, University of Virginia, USA2Department of Medicine, Division of Cardiovascular Medicine, USA3Department of Radiology and Medical Imaging, University of Virginia School of Medicine, USA
Abstract
Behçet’s disease is a multi-system, inflammatory disorder with various clinical presentations. Vascular manifestations include arterial and venous thrombosis, aneurysms, and thrombophlebitis. Intra-cardiac mass is a rare presentation and is histologically composed of inflammatory cells, fibrosis, and thrombus. Treatment of vasculo-Behçet’s disease includes immune suppression, with consideration of anticoagulation depending upon the risk of bleeding from aneurysms. Invasive procedures should be deferred in patients with vasculo-Behçet’s disease because of the increased risk of aneurysm formation. We present a case of vasculo-Behçet’s disease complicated by intra-cardiac mass, pulmonary artery aneurysms, and pulmonary artery thrombus while providing a review of the variations in presentation, clinical outcomes, and management of vasculo-Behçet’s disease in context with existing literature.
INTRODUCTIONBehçet’s disease (BD) is a chronic, relapsing inflammatory
disease that can involve multiple organ systems, including cardiovascular, dermatologic, gastrointestinal, ocular, and nervous systems. The diagnostic criteria developed by the International Study Group (ISG) include a combination of aphthous ulcers, genital ulcers, ocular pathology, skin lesions, and positive pathergy test; multiple diagnostic and classification systems have been proposed due to the wide spectrum of clinical manifestations. The etiology of BD is unknown, but there is likely interplay of genetic and environmental factors. Most cases occur in Mediterranean and Middle Eastern countries and there is a genetic association with human leukocyte antigen (HLA)-B51. Numerous cardiac manifestations of BD have been reported, including pericarditis, cardiomyopathy, valvular disease, conduction system delays, and acute coronary syndrome [1,2]. Vasculo-Behçet’s is characterized by involvement of both arteries and veins of all sizes. The development of an intra-cardiac mass, while very rare, is more likely to be right-sided and occur in men [2].
CASE PRESENTATIONA nineteen-year-old African-American member of a collegiate
crew team presented to the cardiovascular medicine clinic after
developing exertional symptoms of dyspnea and pleuritic chest pain. He had associated symptoms of night sweats and weight loss for three months prior to presentation. His prior medical history was only notable for attention deficit disorder, managed with amphetamine-dextroamphetamine.
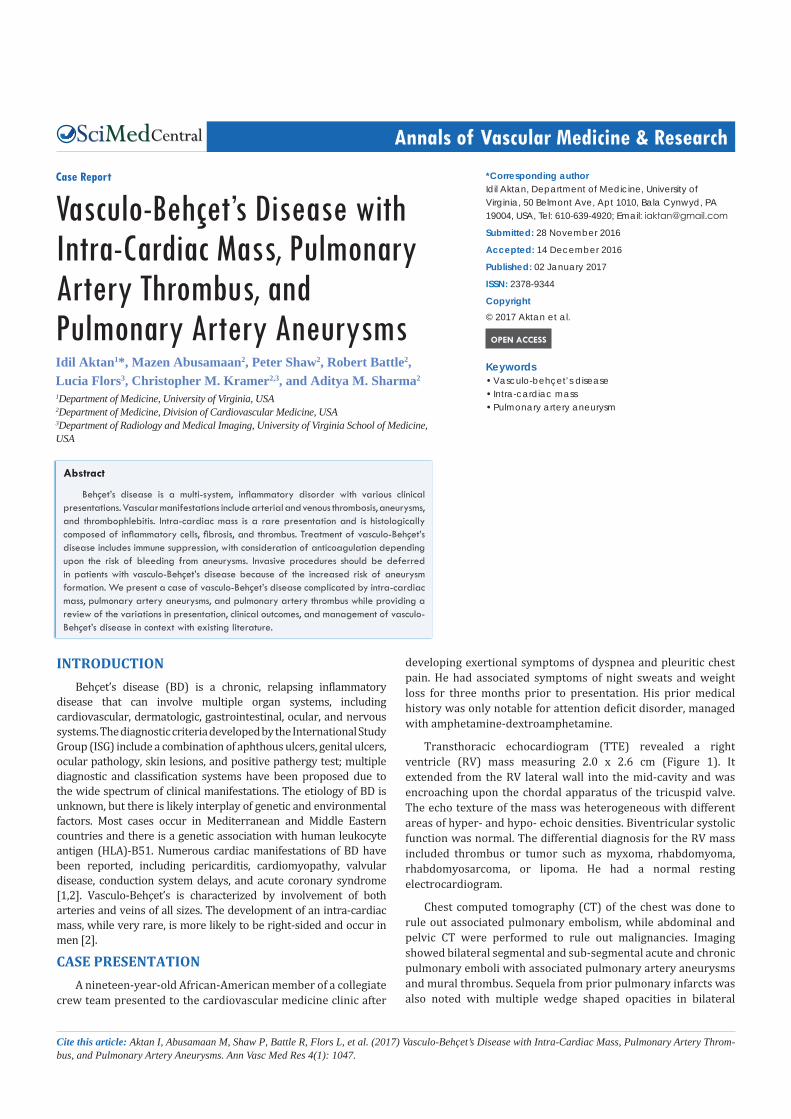
Transthoracic echocardiogram (TTE) revealed a right ventricle (RV) mass measuring 2.0 x 2.6 cm (Figure 1). It extended from the RV lateral wall into the mid-cavity and was encroaching upon the chordal apparatus of the tricuspid valve. The echo texture of the mass was heterogeneous with different areas of hyper- and hypo- echoic densities. Biventricular systolic function was normal. The differential diagnosis for the RV mass included thrombus or tumor such as myxoma, rhabdomyoma, rhabdomyosarcoma, or lipoma. He had a normal resting electrocardiogram.
Chest computed tomography (CT) of the chest was done to rule out associated pulmonary embolism, while abdominal and pelvic CT were performed to rule out malignancies. Imaging showed bilateral segmental and sub-segmental acute and chronic pulmonary emboli with associated pulmonary artery aneurysms and mural thrombus. Sequela from prior pulmonary infarcts was also noted with multiple wedge shaped opacities in bilateral
Central
Aktan et al. (2016)Email:
Ann Vasc Med Res 4(1): 1047 (2017) 2/4
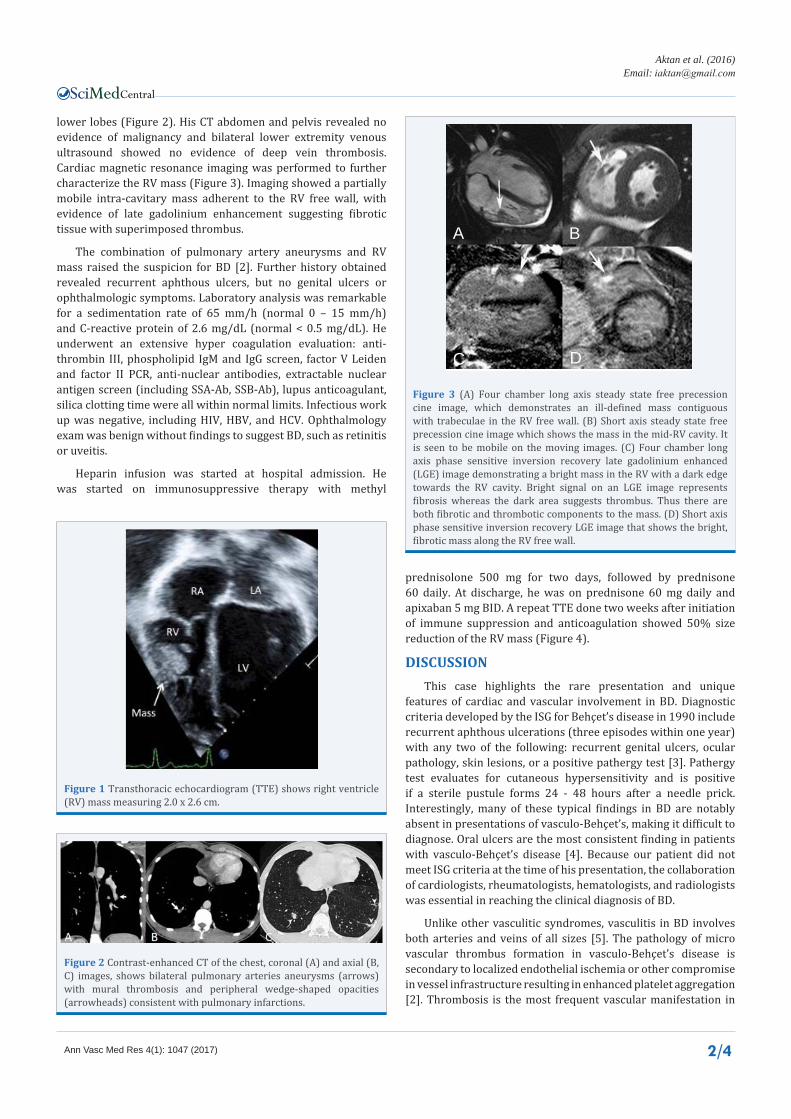
lower lobes (Figure 2). His CT abdomen and pelvis revealed no evidence of malignancy and bilateral lower extremity venous ultrasound showed no evidence of deep vein thrombosis. Cardiac magnetic resonance imaging was performed to further characterize the RV mass (Figure 3). Imaging showed a partially mobile intra-cavitary mass adherent to the RV free wall, with evidence of late gadolinium enhancement suggesting fibrotic tissue with superimposed thrombus.
The combination of pulmonary artery aneurysms and RV mass raised the suspicion for BD [2]. Further history obtained revealed recurrent aphthous ulcers, but no genital ulcers or ophthalmologic symptoms. Laboratory analysis was remarkable for a sedimentation rate of 65 mm/h (normal 0 – 15 mm/h) and C-reactive protein of 2.6 mg/dL (normal < 0.5 mg/dL). He underwent an extensive hyper coagulation evaluation: anti-thrombin III, phospholipid IgM and IgG screen, factor V Leiden and factor II PCR, anti-nuclear antibodies, extractable nuclear antigen screen (including SSA-Ab, SSB-Ab), lupus anticoagulant, silica clotting time were all within normal limits. Infectious work up was negative, including HIV, HBV, and HCV. Ophthalmology exam was benign without findings to suggest BD, such as retinitis or uveitis.
Heparin infusion was started at hospital admission. He was started on immunosuppressive therapy with methyl
prednisolone 500 mg for two days, followed by prednisone 60 daily. At discharge, he was on prednisone 60 mg daily and apixaban 5 mg BID. A repeat TTE done two weeks after initiation of immune suppression and anticoagulation showed 50% size reduction of the RV mass (Figure 4).
DISCUSSIONThis case highlights the rare presentation and unique
features of cardiac and vascular involvement in BD. Diagnostic criteria developed by the ISG for Behçet’s disease in 1990 include recurrent aphthous ulcerations (three episodes within one year) with any two of the following: recurrent genital ulcers, ocular pathology, skin lesions, or a positive pathergy test [3]. Pathergy test evaluates for cutaneous hypersensitivity and is positive if a sterile pustule forms 24 - 48 hours after a needle prick. Interestingly, many of these typical findings in BD are notably absent in presentations of vasculo-Behçet’s, making it difficult to diagnose. Oral ulcers are the most consistent finding in patients with vasculo-Behçet’s disease [4]. Because our patient did not meet ISG criteria at the time of his presentation, the collaboration of cardiologists, rheumatologists, hematologists, and radiologists was essential in reaching the clinical diagnosis of BD.
Unlike other vasculitic syndromes, vasculitis in BD involves both arteries and veins of all sizes [5]. The pathology of micro vascular thrombus formation in vasculo-Behçet’s disease is secondary to localized endothelial ischemia or other compromise in vessel infrastructure resulting in enhanced platelet aggregation [2]. Thrombosis is the most frequent vascular manifestation in
Figure 1 Transthoracic echocardiogram (TTE) shows right ventricle (RV) mass measuring 2.0 x 2.6 cm.
Figure 2 Contrast-enhanced CT of the chest, coronal (A) and axial (B, C) images, shows bilateral pulmonary arteries aneurysms (arrows) with mural thrombosis and peripheral wedge-shaped opacities (arrowheads) consistent with pulmonary infarctions.
A B
C D
Figure 3 (A) Four chamber long axis steady state free precession cine image, which demonstrates an ill-defined mass contiguous with trabeculae in the RV free wall. (B) Short axis steady state free precession cine image which shows the mass in the mid-RV cavity. It is seen to be mobile on the moving images. (C) Four chamber long axis phase sensitive inversion recovery late gadolinium enhanced (LGE) image demonstrating a bright mass in the RV with a dark edge towards the RV cavity. Bright signal on an LGE image represents fibrosis whereas the dark area suggests thrombus. Thus there are both fibrotic and thrombotic components to the mass. (D) Short axis phase sensitive inversion recovery LGE image that shows the bright, fibrotic mass along the RV free wall.

Central
Aktan et al. (2016)Email:
Ann Vasc Med Res 4(1): 1047 (2017) 3/4
BD [4]. In a 2014 review, Wu et al. found that the incidence of thrombosis was 12% in the Chinese BD population [4]. The nature of the thrombus was unique with tight adhesions to the venous wall. The risk of embolism is rare because of the more adherent nature of the thrombus [2]. In the 766hospitalized patients with BD, only 1% (8/766) had an intra-cardiac thrombus, which were histologically determined to be inflammatory cell infiltrates [4]. In another review by Mogulkoc et al., the cardiac mass was described as an organizing thrombus composed of inflammatory cells, with a mixture of granulocytes and mononuclear inflammatory cells [1]. Intra-cardiac thrombus appears to be the result of endomyocardial fibrosis, likely sequelae of vasculitis involving the endocardium, myocardium, or both [6].
Arterial lesions are less common than venous lesions. Saadoun et al. conducted a retrospective analysis of BD patients with arterial lesions, and compared them to patients without arterial lesions [5]. The mean age of BD patients with arterial lesions was 33 years, and most patients were European or North African. When comparing BD patients with arterial lesions to those without lesions, they were significantly more likely to be men (92% vs. 62%) and more likely to have venous involvement (81% vs. 30%) compared to patients without arterial lesions. In their subgroup analysis, they found that being male, having arterial involvement, and the number of BD exacerbations were all independently associated with lower survival rates (p < 0.0001) [5]. The most common arterial lesions were aneurysms (47.3%), followed by occlusions (36.5%), stenosis (13.5%), and aortitis (2.7%) [5]. Histology of arterial lesions showed fibrosis with inflammatory cell infiltrate composed of some combination of lymphoplasmacytes, polymorphonuclear cells, and eosinophils. Thrombosis of the vaso vasorum was also noted [5].
Approximately 5% of BD patients will have pulmonary vascular involvement [7,8]. The differential diagnosis for pulmonary artery aneurysms is short and includes mycotic aneurysms (such as syphilitics and tuberculous Rasmussen aneurysm), connective tissue abnormalities (such as Marfan syndrome and Ehlers-Danlos syndrome), and chronic pulmonary hypertension [8]. Traumatic and iatrogenic pseudo aneurysms
from catheterization should also be considered. The only vasculitides to cause pulmonary artery aneurysms are BD and the exceedingly rare BD variant, Hughes-Stovin Syndrome, which is defined by presence of deep venous thrombosis and pulmonary artery aneurysms [8].
The treatment backbone for BD is immune suppression, with the literature highlighting corticosteroids, cyclophosphamide, and azathioprine. Treatment specifically for pulmonary artery aneurysms is up for debate; cyclophosphamide is currently the preferred immune suppression. Unfortunately, there are no sufficient studies to help guide therapy. Azathioprine was studied for BD ocular disease [8], and reports of colchicine and anti-tumor necrosis factor agent use are also found in literature [9]. There is evidence that patients with arterial lesions had significantly fewer post-operative complications if they were on immune suppression [5].
The European League against Rheumatism (EULAR) recommends treatment of BD with vascular involvement with cyclophosphamide for a minimum of 2 years, followed by azathioprine [10]. Use of anticoagulation is actively debated given lack of evidence of its benefits in this group of patients and there is no recommendation for novel anticoagulants. EULAR does not comment on the use of anticoagulation in venous or arterial thrombosis. As mentioned, thrombi that occur in BD are composed of multiple inflammatory cell types and occur in locations due to local vessel injury. The risk of emboli is considered low given the increased adhesion of thrombus to the vessel wall and the risk of aneurysm bleed should be considered. Anticoagulation alone has not shown to reduce recurrence of thrombosis [11].
Prognosis for BD with vascular involvement is poor, with most patients dying at a relatively young age [7]. Hemoptysis can be a cause of death, but review of literature did not report a high association of anticoagulation with hemoptysis [5]. The risk-benefit of anticoagulation in vasculo-Behçet should be evaluated individually. It is important to avoid invasive imaging or procedures in patients with vasculo-Behçet, as it has been shown to increase risk of aneurysm formation. There was clinical deterioration reported in 50% of BD patients who underwent procedures [7].
To conclude, BD should be included in the differential diagnosis of intra-cardiac mass in young patients, even in the absence of classical features. An early collaborative approach with other sub-specialties, such as rheumatology and dermatology, is recommended as early treatment with immune suppression and anticoagulation can lead to improved survival [12]. The association of intra-cardiac mass with pulmonary artery aneurysms may be the key in the timely and accurate diagnosis of BD.
ACKNOWLEDGEMENTSThis research received no specific grant from any funding
agency in the public, commercial, or not-for-profit sectors. The Authors declare that there is no conflict of interest. This case was presented in the cases over cocktails session at the 27th Society for Vascular Medicine Annual Scientific Sessions in June 2016.
Figure 4 TTE two weeks after initiation of immunosuppression and anticoagulation, showing 50% size reduction of the RV mass.

Central
Aktan et al. (2016)Email:
Ann Vasc Med Res 4(1): 1047 (2017) 4/4
Aktan I, Abusamaan M, Shaw P, Battle R, Flors L, et al. (2017) Vasculo-Behçet’s Disease with Intra-Cardiac Mass, Pulmonary Artery Thrombus, and Pulmonary Artery Aneurysms. Ann Vasc Med Res 4(1): 1047.
Cite this article
REFERENCES1. Mogulkoc N, Burgess MI, Bishop PW. Intracardiac thrombus in
Behçet’s disease: a systematic review. Chest. 2000; 118: 479-487.
2. Selvi Aşker, Müntecep Aşker, Özgür Gürsu, Ridvan Mercan, Özgür Bülent Timuçin. A Behcet’s Disease Patient with Right Ventricular Thrombus, Pulmonary Artery Aneurysms, and Deep Vein Thrombosis Complicating Recurrent Pulmonary Thromboembolism. Case Reports in Pulmonology. 2013; 2013; 4.
3. [No authors listed]. Criteria for diagnosis of Behçet’s disease. International Study Group for Behçet’s Disease. Lancet. 1990; 335: 1078-1080.
4. Wu X, Li G, Huang X, Wang L, Liu W, Zhao Y, et al. Behçet’s disease complicated with thrombosis: a report of 93 Chinese cases. Medicine (Baltimore). 2014; 93: e263.
5. Saadoun D, Asli B, Wechsler B, Houman H, Geri G, Desseaux K, et al. Long-term outcome of arterial lesions in Behçet disease: a series of 101 patients. Medicine (Baltimore). 2012; 91: 18-24.
6. Huong DL, Wechsler B, Papo T, de Zuttere D, Bletry O, Hernigou A, et
al. Endomyocardial fibrosis in Behçet’s disease. Ann Rheum Dis. 1997; 56: 205-208.
7. Winer-Muram HT, Headley AS, Menke P, Eltorky M. Radiologic manifestations of thoracic vascular Behçet’s disease in African-American men. J Thorac Imaging. 1994; 9: 176-179.
8. Acican T, Gürkan OU. Azathiopine-steroid combination therapy for pulmonary arterial aneurysms in Behçet’s disease. Rheumatol Int. 2001; 20: 171-174.
9. Geri G, Wechsler B, Thi Huong du L, Isnard R, Piette JC, Amoura Z, et al. Spectrum of cardiac lesions in Behçet disease: a series of 52 patients and review of the literature. Medicine (Baltimore). 2012; 91: 25-34.
10. Hatemi G, Silman A, Bang D, Bodaghi B, Chamberlain AM, Gul A, et al. EULAR recommendations for the management of Behçet disease. Ann Rheum Dis. 2008; 67: 1656-1662.
11. Seyahi E. Behçet’s disease: How to diagnose and treat vascular involvement. Best Pract Res Clin Rheumatol. 2016; 30: 279-295.
12. Farouk H, Elsaid E, El-Chilali K. Diagnosis of Behçet’s Disease in Patients with Intracardiac Thrombi: A Real Big Challenge. Int J Rare Dis & Orphan Drugs. 2016; 1: 1001.





























