Embed Size (px)
Citation preview
ACCELERATING CMS OUTCOMES DATA TO NEAR REAL TIME: CHALLENGES & SOLUTIONS
Rosemarie Hakim, PhD
CMS
2 Background
3
Medicare data have been available for research for decades
Privacy Act of 1974 allows use of identifiable data for research by a recipient who has provided CMS “with advance adequate written assurance that the record will be used solely as a statistical research or reporting record, and the record is to be transferred in a form that is not individually identifiable”
The Computer Matching and Privacy Protection Act of 1988 allows matching of federal records with non-federal records to produce aggregate statistical data without any personal identifiers
4 What Works Well Today
5
Available data
Chronic Condition Warehouse (CCW) A research database that contains
100% Medicare files and.. Medicaid files Assessment files Part D Prescription Drug Event data
for Fee-for-service institutional and non-institutional claims
Linked by a unique, unidentifiable beneficiary key allow analysis across the continuum of care
6
CCW contd.
Plan characteristics Pharmacy characteristics Prescriber characteristics Formulary file - beginning with year
2010 CCW data files may be requested for
any of the predefined chronic condition cohorts, or users may request a customized cohort(s) specific to research focus areas.
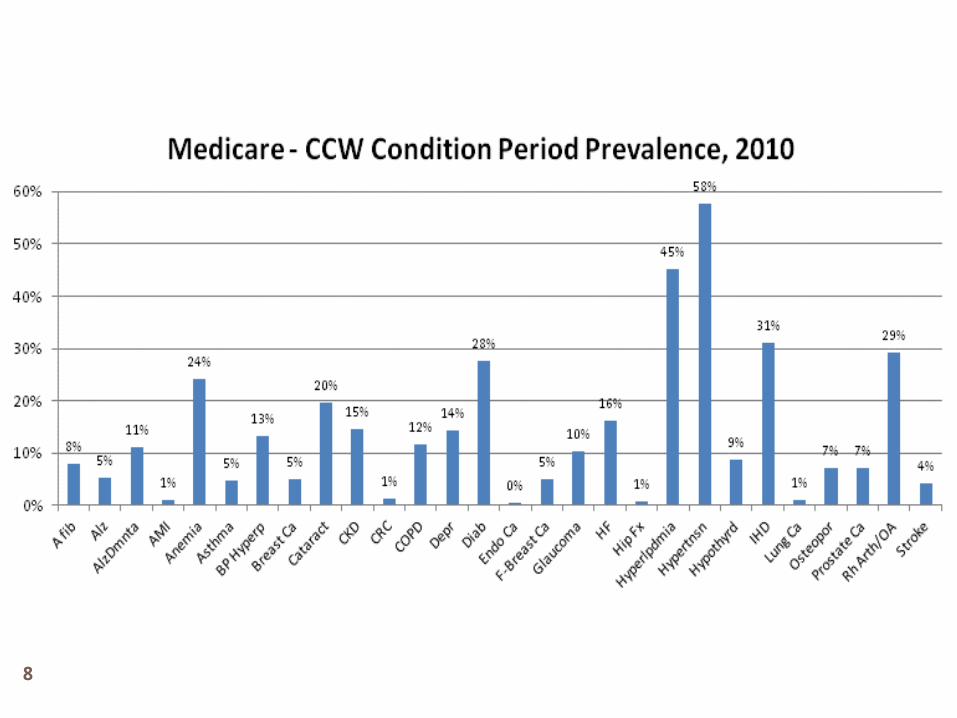
Chronic Conditions Dashboard
7
CCW conditions Acquired Hypothyroidism Acute Myocardial Infarction Alzheimer's Disease Alzheimer's Disease, Related
Disorders, or Senile Dementia
Anemia Asthma Atrial Fibrillation Benign Prostatic Hyperplasia Cancer, Colorectal Cancer, Endometrial Cancer, Breast Cancer, Lung Cancer, Prostate Cataract
Chronic Kidney Disease Chronic Obstructive
Pulmonary Disease Depression Diabetes Glaucoma Heart Failure Hip / Pelvic Fracture Hyperlipidemia Hypertension Ischemic Heart Disease Osteoporosis Rheumatoid Arthritis /
Osteoarthritis Stroke / Transient Ischemic
Attack
8
9
10
Other data available
Master Beneficiary Annual Summary File Durable Medical Equipment Medicare-Medicaid Linked Enrollee
Analytic Data Source MedPAR (Hospital and SNF) Outpatient Others (see ResDAC.org)
11
Strengths of CMS Administrative Data
Clinical validity - accurate and reliable: Admission and discharge dates, diagnoses, procedures, source of care,
demographics, place of residence, date of death, Link to Other CMS Datasets Population Coverage
>98% percent of adults age 65 and over are enrolled in Medicare. > 99% percent of deaths in the US among persons age 65 and older
are accounted > 45 million beneficiaries enrolled in the Medicare program, allowing
for detailed sub-group analysis with high statistical power. Linkage to External Data Sources:
US Census Registries Other providers (e.g. VA, Medicaid) National death index/State vital statistics Surveys (e.g. Health and Retirement Study) Provider Information
12
What Is Missing, Broken or Does Not Work Well Today
13
Reliance on billing codes
Conditions must be diagnosed to appear in the utilization files Some diseases (hypertension, depression and
diabetes) are underdiagnosed No information on care needed but not provided
Services that providers know will be denied may be not be submitted as bills
Diagnosis information may not be comprehensive enough for detailed analysis
Prevalence may be misinterpreted as incidence: knowing a person has a chronic disease does not reveal how long they have had the condition or the severity of their condition
The Part D prescription drug event file contains no diagnosis codes
14
Reliance on billing codes
Different care settings use different coding systems for procedures Inpatient care is coded using ICD-9 procedure codes Physician/supplier and DME data use CPT and
HCPCS codes Hospital outpatient care is a mix of CPT and
revenue center code No physiological measurements or test results Not all beneficiaries have Part D coverage Little information of unknown quality available
about managed care enrollees No information on services for which claims are
not submitted (e.g. immunizations provided at Walgreens)
15
Other limitations
Specific programing expertise needed to analyze claims
In most cases, complex statistical techniques needed to correct biases Propensity scores Missing data algorithms Data validation techniques Severity adjusters Sensitivity analyses Complex regressions
16Challenges and solutions
17
Research Data Time Lag
CCW data on 2-year lag for general research community
However – closer to real time data are available In 6 months 96.7% of inpatient and 96.9% of
outpatient claims are complete
How to get closer to real time data Affordable Care Act allows qualified entities to
acquire data for the evaluation of the performance of providers of services and suppliers
Data use agreement under a contract with CMS
18
Matching Data to Medicare Claims
Deterministic matchingUse unique personal identifiers (UPIs)
present in Medicare claims and in registry/trial data
GoodMatching SSNs
Better Matching SSNs and DOB
Best Matching SSNs, DOB, gender, and
provider
19
Matching Data without UPIs
No unique identifiers in data to be matched to claims
Good results can be obtained using non-unique variables: DOB or age Dates (admission, procedure date) Gender Hospital Geographic region Provider Diagnosis
20
Matching Data without UPIs contd.
Probabilistic (fuzzy) matchingUses wide range of potential identifiersComputes weights based on sensitivity
& specificity of identifier Weights used to calculate the
probability that 2 records refer to the same entity
21
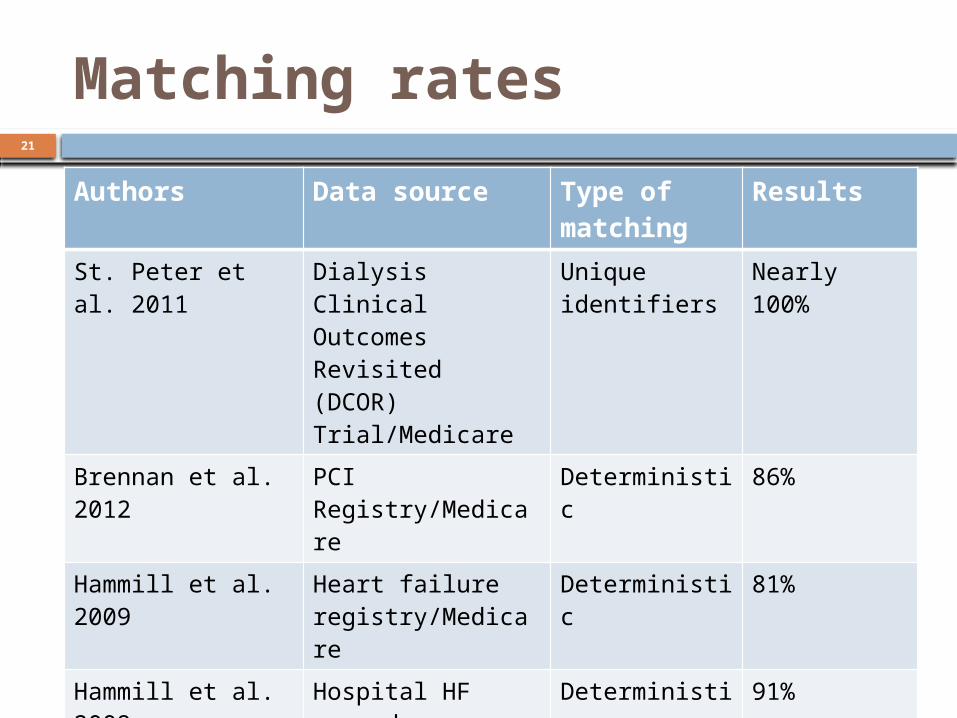
Matching rates
Authors Data source Type of matching
Results
St. Peter et al. 2011
Dialysis Clinical Outcomes Revisited (DCOR) Trial/Medicare
Unique identifiers
Nearly 100%
Brennan et al. 2012
PCI Registry/Medicare
Deterministic 86%
Hammill et al. 2009
Heart failure registry/Medicare
Deterministic 81%
Hammill et al. 2009
Hospital HF records /Medicare
Deterministic 91%
Setoguchi et al. 2012
ICD Registry/Medicare
Deterministic 61%
Setoguchi et al. 2012
ICD Registry/Medicare
Probabilistic 85%
CDC/NCHS 2003-2004 NHANES /Medicare
Probabilistic 98%
22
Short term priorities

23
Make Good Use of CMS Data Build linking capability into study or
registry Include capability to link to Medicare
claims data in informed consent Plan data collection to include important
linking variablesUse data for long term follow up for IDE
studies and RCTs
24
Make Good Use of CMS Data contd.
Develop expertise – use of administrative data is increasing Educational materials on CMS and
ResDAC websitesResDAC gives courses on using CMS
dataDevelop statistical expertise in using
administrative data -
25 Long Term Priorities
26
Health Data Initiatives
Office of Information Products and Data Analytics (OIPDA) Develops, manages, uses, and disseminates
data and information resources Goal of improving access to and use of CMS
data Manages the CMS Data Navigator - web-
based search tool CMS’ EHR incentive program – encourages
data interoperability and development of Health Information Exchanges
27
Thank you
Chronic Conditions Data Warehouse https://
www.ccwdata.org/web/guest/home
ResDAC http://www.resdac.org/
28