Embed Size (px)
Citation preview

OriginalArticle
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
Decisionmodelonthedemographicprofilefortuberculosiscontrolusingfuzzylogic
ModelodedecisãosobreoperfildemográficoparaocontroledatuberculoseusandológicaFuzzy
LaisaRibeirodeSá1,JordanadeAlmeidaNogueira2,RoneiMarcosdeMoraes31Nurse,MasterinModelsofDecisionandHealth.PhDStudentatthePostgraduatePrograminModelsofDecisionandHealth,UniversidadeFederaldaParaíba(UFPB).Joãopessoa,PB,Brazil.E-mail:[email protected],PhDinNursing.AssociateProfessoroftheHealthSciencesCenter,UFPB.JoãoPessoa,PB,Brazil.E-mail:[email protected],PhDinAppliedComputing.AssociateProfessoroftheDepartmentofStatistics,UFPB.JoãoPessoa,PB,Brazil.E-mail:[email protected].
ABSTRACT
Thisstudyaimedtodescribetherelationshipbetweendemographic factorsandthe involvementof tuberculosisby
applyingadecisionsupportmodelbasedonfuzzylogictoclassifytheregionsaspriorityandnon-priorityinthecityof
JoãoPessoa,stateofParaíba(PB).Asdatasource,weusedtheNotifiableDiseasesInformationSystembetween2009
and2011.Wechosethedescriptiveanalysis,relativerisk(RR),spatialdistributionandfuzzylogic.Thetotalof1,245
casesremainedinthestudy,accountingfor37.02%ofcasesin2009.Highandlowriskclusterswereidentified,andthe
RR was higher among men (8.47), with 12 clusters, and among those uneducated (11.65), with 13 clusters. To
demonstratethefunctionalityofthemodelwaselectedtheyearwithhighestnumberofcases,andthemunicipality
districtwithhighestpopulation.Themethodologyidentifiedpriorityareas,guidingmanagerstomakedecisionsthat
respectthelocalparticularities.
Descriptors:Tuberculosis;RelativeRisk(PublicHealth);SpatialAnalysis;FuzzyLogic;PublicHealthNursing.
RESUMO
Objetivou-sedescreverarelaçãoentreos fatoresdemográficoseoacometimentodatuberculose,aplicando-seum
modelodesuporteàdecisãobaseadoemlógicafuzzyparacategorizaçãodoslocaisemprioritáriosenãoprioritários,
nacidadedeJoãoPessoa-PB.Comofontededados,utilizou-seoSistemadeInformaçãodeAgravosdeNotificação,
entre2009e2011.Optou-seporanálisedescritiva,riscorelativo(RR),distribuiçãoespacialelógicafuzzy.Permaneceu
noestudo1245casos,sendoqueoanode2009,foiresponsávelpor37,02%doscasos.Identificou-seconglomerados
dealtoebaixorisco,sendoqueoRRfoimaiorentreoshomens(8,47),com12conglomerados,entreaquelessem
escolaridade(11,65),com13conglomerados.Parademonstrarafuncionalidadedomodelo,elegeu-seoanocommaior
númerodecasoseumbairrodomunicípiocommaiorcontingentepopulacional.Ametodologiapermitiuidentificar
áreasprioritáriasdirecionandogestoresparadecisõesquerespeitemasparticularidadeslocais.
Descritores:Tuberculose;RiscoRelativo;AnáliseEspacial;LógicaFuzzy;EnfermagememSaúdePública.

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
224
INTRODUCTION
Tuberculosis (TB) isan infectiousdiseaseof chronic
evolution with sufficient diagnostic and therapeutic
resources for a proper and successful clinical
management. Despite the available technology, the
disease incidence is still high, with alarming numbers.
Estimates from the World Health Organization (WHO)
indicatethediseaseasthesecondleadingcauseofdeath
worldwide.TBwasthebasiccauseof1.4milliondeathsin
2011,and8.7millionpeoplefellillinthesameyear(1).
Althoughinrecentyears,Brazilhashownadeclinein
the number of cases, it still occupies the 19th position
among 22 countries, concentrating 80% of the
tuberculosisburdenintheworldandthe104thposition
relative to the incidence rate. In 2012 were reported
70,047newcases,correspondingtoanincidencerateof
36.1/100,000 inhabitants(1). Every year about 4,500
peoplediefromtuberculosis,therefore,thisisthefourth
leadingcauseofdeathfrominfectiousdiseasesandthe
leadingcauseofdeathamongAIDSpatients(2).
In 2012, in the state of Paraíba, located in
northeasternBrazil,werereported1,132newcasesofthe
disease, with an incidence rate of 29.7/100,000 in
habitants. The state capital, João Pessoa, presented an
incidencerateof46.4/100,000inhabitantsfornewcases.
Overthepast10years,thisindicatorhasshownafalling
trend,similartotheincidencerateinBrazil(2).
The studies agree that TB is conditioned to social
aspects, where poverty and poor sanitary conditions
determinants, together with the weaknesses of
management and organization of health services
collaborate to the increase and/or permanence of the
diseaseincidencerates(3–5).
Thus, new answers must be found to promote
fairness, ensuring access to patients, seeking not only
their care and well-being, but in a broader sense, the
consolidation of the Unified Health System (SUS) in its
guidelines.Thealternativeslieinthereadjustmentofthe
health care system in the assistance to these patients,
redefinition of procedures and organizational charts,
redefinition of institutional missions of civil society
entities, and the search for alternatives to solve the
problem. Among those alternatives, communication
shouldoccupyaprominentplace(6).
In thisperspective,andwiththesignificantnumber
ofTBcases,arosetheneedtoanalyzethedemographic
profileofthediseaseinthecityofJoãoPessoa(stateof
Paraíba – PB) to facilitate the decision-making process
related to thisdisease.As thevariablesassociatedwith
the involvement of tuberculosis have some degree of
uncertainty, a systembasedon fuzzy rulesbecomesan
interesting alternative for a decisionmodel that allows
thecategorizationofpriorityregionsusingeachvariable
separately.
Studies using the proposed model in various
morbidities were found in the literature, but only
assessingcasesintheirentirety(7-8).However,nostudies
associating cases of tuberculosis according to
demographic variables through a spatial analysis were
found,andthisisproposedinthepresentstudy.
Given the above, this study aimed to describe the
relationship between demographic factors and the
involvement of tuberculosis. It also applied a decision
supportmodelbasedonfuzzylogictoclassifytheregions
aspriorityandnon-priority,accordingtoeachvariable.
METHODS
Thisisanepidemiological,retrospectivestudy,based
onrecordsoftuberculosiscasesinthecityofJoãoPessoa.
It included the cases reported in the database of the
Notifiable Diseases Information System (Sinan) of the
Health Secretariat of the state of Paraíba between 1
January2009and31December2011.Thestudyexcluded
all cases inwhich data could lead to systematic errors,
such as cases from other municipalities without
informationaboutthehomedistrict.
Subsequently, was held a database refinement to
identifythevariablesofinterest:theyearofnotification,
gender,educational level,district (residenceunitof the
notified case and not necessarily where the infection

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
225
occurred). These data were arranged in a spreadsheet
and analyzed according to the frequency and
proportional distribution to generate the relative risk
(RR), spatial scan statistic (CSS) and fuzzy logic. From
thesevariables,tablesandgraphsweregeneratedfora
betterpresentationofresults.
TheBrazilianCensusconductedinBrazilintheyears
2000and2010wasusedtocalculatetheincidencerates.
The denominators were estimated from projections of
theresidentpopulationinthecity,usingthepopulation
baseof1,000inhabitantsineachdistrictofJoãoPessoa.
Therelativerisk(RR)wasrepresentedbytheratioof
the incidence rate in adistrict dividedby the incidence
rateoftheentireregion(JoãoPessoa).Theuseofmaps
to spatially represent the RR allowed primary analyzes,
suchas the identificationof regions thatpresented the
highest and lowest risks of disease occurrence. The RR
wasdividedintoclassintervals,previouslyestablishinga
color for each interval(9). Risk maps were prepared
accordingtotheyearofoccurrenceandvariablestudied
(total, gender and educational level). For the
interpretationoftheRRmap,thefollowingcriteriawere
defined(Table1):
Table1:Interpretationofclassesofrelativerisk*.RelativeRisk InterpretationofRelativeRisk
Greaterthanorequalto0andlessthan0.5
Districtswheretherelativeriskrangedfrom0to0.5,i.e.,relativerisklowerthanhalftheoverallriskofthestudyarea.
Greaterthanorequalto0.5andlessthan1.0
Districtswheretherelativeriskrangedfrom0.5to1.0,i.e.,higherthanhalftheoverallriskofthestudyarea.
Greaterthanorequalto1.0andlessthan1.5
Districtswheretherelativeriskrangedfrom1.0to1.5,sotherelativeriskisgreaterthantheoverallriskofthestudyareainlessthan50%.
Greaterthanorequalto1.5andlessthan2.0
Districtswheretherelativeriskrangedfrom1.5to2.0,sotherelativeriskishigherthantheoverallriskofthestudyareainmorethan50%.
Greaterthanorequalto2.0 Districtswheretherelativeriskwashigherthan2.0.*Adaptedtable(7-8,10).
Subsequently, the CSS method was used to detect
spatial clusters, allowing to outline the critical regions
using graphical computational algorithms. For spatial
analysis,weadopted theprobabilisticmodelofPoisson
thatassociates thearea informationwitha singlepoint
withinthepolygon,thecentroid,whichisthemasscenter
ofeachregionofthestudiedarea(11).
IntheCSSmethod,therestrictionisinrelationtothe
percentage of the population at risk, determining the
increaseofthesearchradiusuptoβ%ofthepopulation.
Thisstudyusedβ%ofthepopulationof1%,3%,5%and
10%. The maps from the respectiveβ% should be
comparedwiththeriskmapofeveryyeartofindthemap
thatbestfits.Thus,fromavisualinspectionofthemaps
representingthephenomenonunderstudy,wecompare
theCSSmapwith theriskmap,opting for theCSSmap
that most closely resembles the risk map. The spatial
clustersidentifiedwerepresentedonmapsinwhichthe
reddotsrepresentthecentroids(11).
After the spatial analysis, was applied the decision
model based on fuzzy logic. The fuzzy logic originates
fromtheconceptoffuzzysetsandrepresentsascheme
capable of translating inaccurate information into
numerical values, making it possible to solve problems
thatclassicallogiccouldnotsolve(12).Then,afuzzysetis
definedasaclassofobjectswithcontinuousdegreesof
association. This set is characterized by membership
functions assigned to each object of the set, varying
betweenzeroandone(13).
One of the most common ways to express this
knowledgeisthroughrulesofthecondition-actiontype.
Thus, all knowledge is represented by a set of rules in

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
226
which the conditions are established from a set of
linguistic terms, which are associated with the
input/outputvariables.Therefore,thefuzzyruleisaunit
capableofcapturingsomespecificknowledge(14).
Atthisstage,werecreatedtheinputvariables(total
relative risk, totalCSS, female relativerisk, female CSS,
male relative risk, male CSS, uneducated relative risk,
educated CSS, educated relative risk - at least literate,
educatedCSS-atleastliterate)andtheoutputvariables
(priorityandnon-priority)andthemembershipfunctions
foreachofthem.Eachofthesevariableshasitslinguistic
termsrepresentingafuzzyset(14).Inthefinalresult,itwas
possibleto identifythepriorityandnon-priorityregions
ofthecityofJoãoPessoa,withtheirrespectivedegrees
ofmembership.
TheethicalaspectsestablishedbyResolution196/96,
which regulates research on humans, were respected.
Sincethisisastudywithsearchinasecondarydatabase,
we used the Institutional Consent term issued by the
MunicipalSecretariatofHealthinJoãoPessoa-PBunder
number20.900/2013.
RESULTS
Intheperiodbetween2009and2011,werereported
1,329casesoftuberculosisinthecityofJoãoPessoa-PB.
Basedonthe inclusioncriteria,1,245casesremained in
thestudy,ofwhich461(37.02%)werereportedin2009,
417(33.49%)in2010and367(29.47%)in2011.Themale
genderwaspredominant(853/68.5%),aswellassubjects
withsomelevelofeducation(983/78.95%).
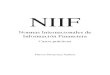
Toexemplify,intheanalysisofrelativeriskandCSS,
were used the maps of tuberculosis in João Pessoa in
2009, for the total, female, male, uneducated and
educated (Figure 1).Note thatmapswere built for the
entirestudyperiod.
The map of total RR showed the behavior of
tuberculosisinthedistrictsofJoãoPessoa-PB,wherethe
RRvariedbetween0and5.90per1,000inhabitants.The
spatialanalysisofcasesthroughstatisticalCSSidentified
clustersa thighand low risk.Nineteendistricts showed
spatial clusters for the year 2009, with 5%of the
population.ComparingthemapoftotalCSSwiththemap
of total risk, there is a coincidence of regionswith the
greatest RR ratios and those with significant spatial
clusters.
AnalyzingthemapsofriskandCSSbygender,theRR
washigher amongmen (8.47),with thepresenceof 12
clusters. The RR was lower among women, reaching a
maximum value of 4.66. However, the CSS method
identified 13 significant clusters. In the analysis of the
male population,was also observed that somedistricts
showed RR two or more times higher when compared
withthetotalRRandthefemalegender.
In relation to theeducational level, theRR reached
11.65amonguneducatedcasesand6.76amongeducated
individuals. In both groups were identified 13 clusters,
andinthefirst,therewasahigherconcentrationinthe
districtsofthecentralareaofthecityand/ordistrictswith
economicallyvulnerablepopulation.

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
227
Figure1:MapsofrelativeriskandCSSoftuberculosiscasesaccordingtoresidencedistrict.JoãoPessoa,PB,Brazil,2009.
Intheanalysisoffuzzyvariablesinvolvingrelativerisk
weredefinedfivelinguisticterms,namely:veryhighrisk,
highrisk,mediumrisk,verylowriskandlowrisk(Chart1).
The following membership functions of the fuzzy
variables were of trapezoidal type: total relative risk,
female relative risk, male relative risk, uneducated

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
228
relative risk, educated relative risk. The binary
membership function for theresultsof theCSSmethod
were named withScan and withoutScan. The following
membership functions of fuzzy variables were of
triangular type: total CSS, female CSS, male CSS,
uneducatedCSSandeducatedCSS.Theoutputvariable
obtainedpriorityandnon-priorityasalinguisticterm,and
membershipfunctionsoftrapezoidaltype(Chart1).
Chart1:MembershipfunctionsoftheinputvariablesofrelativeriskandCSS,andmembershipfunctionsoftheoutput
variable.JoãoPessoa,PB,Brazil,2009.
Fortheconstructionoftherulesdatabase,wereused
tenfuzzyvariablesobtainedthroughtheannualmapsof
therelativeriskandCSSmapsfortotal,female,maleand
uneducatedpopulation,aswellaseducatedpopulation.
Fivebankswerecreatedwithtenrulesdefinedforeach,
totaling 50 rules. Some of these rules are presented
belowforexemplification:
• IF (total relative risk is veryhigh)AND (total scan is
withScan),THEN(decisionispriority)
• IF (total relative risk is veryhigh)AND (total scan is
withoutScan),THEN(decisionisnon-priority);
After construction of the rules, was applied the
decisionmodelbasedonfuzzylogictoclassifythedistricts
aspriorityandnon-priorityfortuberculosisinrelationto
gender, educational level and total. This model was
appliedtoeachsetofrulesforall64districts,inallyears,
demonstrating its functionality. It canbeused as a low
cost method by managers and professionals, for an
effectivecombatofthemorbidityaccordingtothetarget
populationandtheregionsconsideredaspriority.

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
229
Toexemplifytheapplicationofthemodelbasedon
fuzzylogic,wechoseadistrictwithhighpopulationand
the year 2009, a periodwith the highest occurrence of
cases(Charts2-4).
Each column representsamembership function for
eachof thevariables intherule.Eachrowrepresentsa
rulethat isactivatedaccordingtothe inputdata,which
mayormaynotactivatethelastcolumn,accordingtothe
value of the input variables. Thus, the output function
shows the suggestion of decision to be made by the
manager for the district; as priority (partially or
completelyfilledbybluecolorontherightside)orasnon-
priority(partiallyorcompletelyfilledbybluecoloronthe
leftside).
Followingthesameconception,themodelconfirmed
the expected result, in which the elected district was
classified as priority in relation to the total population
(Chart2),malegender(Chart3)andeducated(Chart4).
Itwasclassifiedasnon-priorityinrelationtothefemale
gender(Chart3)anduneducated(Chart4).

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
230
Chart2:ResultofthetotallinguisticfuzzymodelinthedistrictofMangabeira-JoãoPessoa,PB,2009.

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
231
Chart3.A:ResultofthemaleandfemalelinguisticfuzzymodelinthedistrictofMangabeira-JoãoPessoa,PB,2009.

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
232
Chart3.B:ResultofthemaleandfemalelinguisticfuzzymodelinthedistrictofMangabeira-JoãoPessoa,PB,2009.

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
233
Chart4.A:ResultoftheuneducatedandeducatedlinguisticfuzzymodelinthedistrictofMangabeira-JoãoPessoa,PB,2009.

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
234
Chart4.B:ResultoftheuneducatedandeducatedlinguisticfuzzymodelinthedistrictofMangabeira-JoãoPessoa,PB,2009.

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
235
DISCUSSION
The disease concentration in the most populous
districtsorthoseoflowereconomicclassmaybedueto
itscharacterizationasasocialproblem,resultingfromthe
interactionofseveralfactors,amongwhichthelowfamily
income, poor education, poor/non-existent housing,
large families, high density communities, food
malnutrition, alcoholism, associated diseases,migration
flows,deficiencyofthehealthsystem(15)
.
Themajorityof studies foundcorroborate the local
scenebecause they characterize thedisease as a social
problemresultingfromtheinteractionofseveralfactors,
ofwhichthemostcitedwerethemalegender,lowfamily
income, poor education, poor/non-existent housing,
large families, alcoholism, smoking,mental illness,AIDS
andoccupationalrisk(4,16–20)
.
Thegenderasariskfactorcanbejustifiedbythefact
thathistoricallymenseekhealthservicesforpreventive
controlwithlessfrequency,especiallywhenitcomesto
basichealthcare,andgenderissuesareverystrongwhen
itcomestothehealth-diseaseprocess(21)
.
The actions related to care have always been
associatedwithwomen,andtheaccessofmentohealth
services is hindered by labor issues, when there is a
mismatch between the health services hours and the
workinghoursofmalesubjects.Asaresult,mentendto
searchforhealthservicesaftertheworseningofclinical
picture.Inadditiontobeseenasthehomeproviders,and
feeling more difficulty in expressing themselves, men’s
needsarenotmetinstantly.
In relation to educational level, the study results
showthatmostofthecasesreportedoccurineducated
people.However, theapplicationof thedecisionmodel
found thatmost districts were classified as priority for
uneducatedpeople,confirmingthisisalsoariskfactorfor
TB.Corroborating theabove in termsof education, the
longerthedurationofstudies,thelessertheoccurrence
of TB, showing that more years of study result in less
occurrenceofTB(22)
.
Thedecisionmodelbasedonfuzzylogicisconsidered
afundamentalmethodologicalsupporttorespondtothe
healthprocessuncertainties and the illnessof subjects.
Moreover, it improves the understanding of individual
riskandisessentialinepidemiologicalstudies.
The theory of fuzzy sets appears as a useful
methodological tool in social areas by shaping the
uncertainties inherent in its phenomena, especially in
epidemiology(23)
. Several epidemiological studies show
theimportanceofthetheoryoffuzzysetswhenstudying
the health and disease process, contributing in the
construction of diagnostics and expert systems. Among
thestudiesusingthetheoryoffuzzysetssatisfactorily,we
canhighlightafew:applicationoffuzzyclustersmodelfor
analysis and identification of different types of
tuberculosis(24)
;creationofa fuzzymodeltopredict the
resultofTBcaseswithongoingtreatment(25)
.
CONCLUSION
Theresultsshowedthatthedecisionmodelbasedon
fuzzylogicisalowcosttoolandallowedtheclassification
ofallthecitydistrictsaspriorityornon-priority,according
to each variable, enabling the visualization of
peculiarities, and guiding managers for decisions that
respecttheparticularitiesofeachlocation.Notethatthis
is an innovative approach because it visualizes the
totality, aswell as eachvariable separately, allowing to
know the vulnerability of each region for the effective
combatofthemorbidity.
Thus, a further understanding of the vulnerable
populations to the disease and the region become
possible,whichfacilitatesthedefinitionofpublicpolicies
forthepriorityandspecificareasandthepopulationof
thatregion.Also,policiesforthecombatandprevention
of morbidity can be defined together with health
professionals,makingitpossibletodecreasetheonsetof
tuberculosis.

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
236
REFERENCES1.WHO.GlobalTuberculosisReport2014[Internet].WorldHealth
Organization.2014[acessoem:30jun2015].Disponívelem:
http://apps.who.int/iris/bitstream/10665/137094/1/97892415648
09_eng.pdf?ua=1.
2.MinistériodaSaúde.SistemaNacionaldeVigilânciaemSaúde.
RelatóriodeSituação.Paraíba[Internet].5ªed.Brasília:Ministério
daSaúde;2011[acessoem:30jun2015].Disponívelem:
http://bvsms.saude.gov.br/bvs/publicacoes/sistema_nacional_vigil
ancia_saude_pb_5ed.pdf.
3.CostaARF,FalkinhamJO,LopesML,BarrettoAR,FelicioJS,Sales
LHM,etal.OccurrenceofNontuberculousMycobacterial
PulmonaryInfectioninanEndemicAreaofTuberculosis.PLoSNegl
TropDis[Internet].2013[acessoem:30jun2015];7(7):e2340.
Disponívelem:http://dx.plos.org/10.1371/journal.pntd.0002340.
4.XimenesRAA,AlbuquerqueMFPM,SouzaWV,MontarroyosUR,
DinizGTN,LunaCF,etal.Isitbettertoberichinapoorareaor
poorinaricharea?Amultilevelanalysisofacase-controlstudyof
socialdeterminantsoftuberculosis.IntJEpidemiol.2009[acesso
em:30jun2015];38(5):1285-96.Disponívelem:
http://dx.doi.org/10.1093/ije/dyp224.
5.SantosMLSG,VendraminiSHF,GazettaCE,OliveiraSAC,Villa
TCS.Poverty:socioeconomiccharacterizationattuberculosis.Rev
LatAmEnfermagem.2007[acessoem:30jun2015];15(spe):762-7.
Disponívelem:http://dx.doi.org/10.1590/S0104-
11692007000700008.
6.PortaldaSaúde[Internet].Brasília:MinistériodaSaúde(BR).
[acessoem:02out2013].Disponívelem:
http://portal.saude.gov.br/portal/saude/profissional/visualizar_te
xto.cfm?idtxt=31101.
7.SousaACA.Modelodedecisãosobreosmunicípiosprioritários
paraocontroledaAIDSnoestadodaParaíbausandológicaFuzzy[dissertação].JoãoPessoa:UniversidadeFederaldaParaíba;2012.
8.CostaDCS.Tomadadedecisãobaseadaemlógicafuzzyena
distribuiçãoespacialdamortalidadeporacidentesdetrânsitona
cidadedeJoãoPessoa–PB[dissertação].JoãoPessoa:
UniversidadeFederaldaParaíba;2011.
9.CâmaraG,DavisC.Introdução:Porquegeoprocessamento?
[Internet].SãoJosédosCampos:InstituiçãoNacionaldePesquisas
Espaciais;2001[acessoem:30jun2015].Disponívelem:
http://bibdigital.sid.inpe.br/rep-
/sid.inpe.br/sergio/2004/04.19.13.48.
10.MedronhoRdeA,BlochKV,WerneckGL.Epidemiologia.
Atheneu;2009.685p.
11.KulldorffM,NagarwallaN.Spatialdiseaseclusters:Detection
andinference.StatMed[Internet].1995[acessoem:30jun
2015];14(8):799–810.Disponívelem:
http://dx.doi.org/10.1002/sim.4780140809.
12.MoraesR.Fuzzyexpertsystemsarchitectureforimage
classificationusingmathematicalmorphologyoperators.InfSci
(Ny)[Internet].2002[acessoem:30jun2015];142(1-4):7–21.
Disponívelem:http://dx.doi.org/10.1016/S0020-0255(02)00154-8.
13.ZadehLA.Fuzzysets.InfControl[Internet].1965[acessoem:
30jun2015];8(3):338–53.Disponívelem:
http://dx.doi.org/10.1016/S0019-9958(65)90241-X.
14.PassinoKM,YurkovichS.Fuzzycontrol[Internet].MenloPark:
Addison-Wesley;1998[acessoem:30jun2015].Disponívelem:
http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.131.44
94&rep=rep1&type=pdf.
15.SantoLALA,SantosPCH,MoreiraME.Perfilclínico,
epidemiológicoelaboratorialdospacientescomtuberculoseem
hospitaluniversitáriodaregiãodoValedoParaíba,EstadodeSão
Paulo.BEPABolEpidemiológicoPaul[Internet].[acessoem:30jun
2015];6(68):14–21.Disponívelem:
http://periodicos.ses.sp.bvs.br/scielo.php?script=sci_arttext&pid=
S1806-42722009000800002&lng=pt&nrm=iso&tlng=pt.
16.SantosAPG,PachecoAG,StaviackA,GolubJE,ChaissonRE,
RollaVC,etal.SafetyandeffectivenessofHAARTintuberculosis-
HIVco-infectedpatientsinBrazil.IntJTubercLungDis[Internet].
2013[acessoem:30jun2015];17(2):192–7.Disponívelem:
http://dx.doi.org/10.5588/ijtld.11.0831.
17.SantosRMZ,AmadorA,SouzaWV,AlbuquerqueMFPM,
DawsonSP,Ruffino-NettoA,etal.ADynamicAnalysisof
TuberculosisDisseminationtoImproveControlandSurveillance.
PLoSOne[Internet].2010[acessoem:30jun2015];5(11):e14140.
Disponívelem:http://dx.doi.org/10.1371/journal.pone.0014140.
18.MoreiraTR,ZandonadeE,MacielELN.Riscodeinfecção
tuberculosaemagentescomunitáriosdesaúde.RevSaudePublica
[Internet].2010[acessoem:30jun2015];44(2):332–8.Disponível
em:http://dx.doi.org/10.1590/S0034-89102010000200014.
19.MeloTEMP,ResendesAPC,Souza-SantosR,BastaPC.
Distribuiçãoespacialetemporaldatuberculoseemindígenase
nãoindígenasdeRondônia,AmazôniaOcidental,Brasil.CadSaude
Publica[Internet].2012[acessoem:30jun2015];28(2):267–80.
Disponívelem:http://dx.doi.org/10.1590/S0102-
311X2012000200006.
20.RozaDL,Caccia-BavaMCGG,MartinezEZ.Spatio-temporal
patternsoftuberculosisincidenceinRibeirãoPreto,StateofSão
Paulo,southeastBrazil,andtheirrelationshipwithsocial
vulnerability:aBayesiananalysis.RevSocBrasMedTrop
[Internet].2012[acessoem:30jun2015];45(5):607–15.Disponível
em:http://dx.doi.org/10.1590/S0037-86822012000500013.
21.AraújoAC.Políticanacionaldeatençãointegralàsaúdedo
homem:elementosparaodebate[Internet].2013[acessoem:30
jun2015].Disponívelem:
http://dspace.bc.uepb.edu.br:8080/xmlui/handle/123456789/757.
22.VasconcelosCH,EvangelistaMSN,FonsecaFR,BarreiraD,
Dell’OrtiD.Estudodadistribuiçãodatuberculose(TB)nosEstados
doAmazonaseRioGrandedoSul(2006a2009).CadSaúde
Coletiva[Internet].2011[acessoem:30jun2015];19(4):461-6.
Disponívelem:
http://www.cadernos.iesc.ufrj.br/cadernos/images/csc/2011_4/ar
tigos/csc_v19n4_461-466.pdf.
23.AlvesAA.AsMedidasdeRiscoClássicaseasdeRiscoFuzzi.Rev
BrasCiênciasdaSaúde[Internet].2012[acessoem:30jun
2015];16(1):85–92.Disponívelem:
http://dx.doi.org/10.4034/RBCS.2012.16.01.13.
24.ImianvanA.A.OJC.Fuzzyclustermeansexpertsystemforthe
diagnosisoftuberculosis.GlobalJournalofComputerScienceand
Technology[Internet].2011[acessoem:30jun2015];11(6):41-8.
Disponívelem:
http://computerresearch.org/index.php/computer/article/view/78
0.
25.KalhoriSRN,ZengXJ.FuzzyLogicApproachtoPredictthe
OutcomeofTuberculosisTreatmentCourseDestination.In:

SáLR,NogueiraJA,MoraesRM.
Rev.Eletr.Enf.[Internet].2015apr./jun.;17(2):223-37.Availablefrom:http://dx.doi.org/10.5216/ree.v17i2.27643.
237
ProceedingsoftheWorldCongressonEngineeringandComputer
Science2009VolIIWCECS2009,October20-22,2009,San
Francisco,USA[Internet].2009[acessoem:30jun2015].
Disponívelem:
http://www.iaeng.org/publication/WCECS2009/WCECS2009_pp77
4-778.pdf.
Received:12/11/2013.
Accepted:09/15/2014.
Published:06/30/2015.