Embed Size (px)
Citation preview

Br HeartJ 1984; 52: 178-85
Absent or occult pulmonary artery
PATRIZIA PRESBITERO,* CATHERINE BULL,t SHEILA G HAWORTH,MARC R DE LEVAL
From the Thoracic Unit, The Hospital for Sick Children, and the Department of Paediatric Cardiology, Institute ofChild Health, London
SUMMARY Of 12 patients with angiographically absent pulmonary artery, 11 were investigated surgi-cally. The previously occult pulmonary artery was found in 10 patients, in five of whom a vestige ofan intrapericardial artery was present and in five the artery was:patent only at the hilus, a gapexisting between the main pulmonary artery and the hilar vessel, and no artery was found in one. Allpatients with an intrapericardial artery had right ventricular outflow tract obstruction and a ductusdescending vertically from underneath the aortic arch. In those without an intrapericardial vessel theoccult artery was on the side opposite the aortic arch, and there was evidence of a ductus comingfrom the innominate artery on the side of the interruption. The occult pulmonary artery, whereidentified at operation, was usually joined initially to the systemic circulation. Ultimately, continuitybetween the hilar and main pulmonary artery may be established surgically. Where no intrapericar-dial vessel exists, however, a conduit may be required to bridge the gap.
It seems advisable to search for the occult artery as early in life as is feasible in the hope thatproviding a blood supply will ensure development of the vessel and normal lung growth.
The absence of a main branch of the pulmonary arterywas first described by Frantzel in 1868.1 Since thenseveral cases of patients with and without intracardiacanomalies have been reported. In 1954 McKim andWiglesworth2 and later Sotomora and Edwards3pointed out that the distal portion and intrapul-monary vessels of the so called "absent pulmonaryartery" are in fact usually present. McKim and Wig-lesworth2 also underlined an occasional relation be-
which part of the artery was absent, specificallywhether it was the intrapericardial or the more distalpart of the vessel near the hilus. The relation betweenthe absent pulmonary artery and the ductus arteriosuswas also considered as well as the embryologicalmechanism of this anomaly.
Patients and methods
tween the absence of a pulmonary artery and the per- From 1973 to 1982, 12 patients with apparent absencesistence of a ductus arteriosus on the same side as the of one pulmonary artery were seen at this- hospital.interruption. Perfusion of the hilar pulmonary artery We excluded from the study patients with an absentby a ductus, arising either from the aorta directly or pulmonary artery who had pulmonary atresia andfrom an innominate artery, was described as the distal major aortopulmonary collateral arteries feeding theductal origin of the pulmonary artery by Sotomora hilar and intrapulmonary arteries and those who hadand Edwards.3 an aortic origin of one pulmonary artery (hemitruncusWe reviewed 12 patients with angiographic absence arteriosus). Also excluded were patients with agenesis
of a main branch of the pulmonary artery, all but one of one lung. The age at which patients first came toof whom were investigated surgically. We established our notice ranged from 5 days to 12 years.
All the patients underwent at least one angiographicRequests for reprints to Dr M de Leval, Thoracic Unit, Hospital for examination, most having serial studies. In the searchSick Children, Great Ormond Street, London WCIN 3JH. for the absent artery contrast medium was injected
*Present address: Ospodale Molinette, Tonno, Italy. 4 into both the right ventricle and the systemic circula-resentadseMolinee,Torino,l.tion in all patients. In three patients, studied more
tPresent address: The Brompton Hospital, Fulham Road, Londoh SW3, recently,. pulmonary venous wedge injections were
Accepted for publication 6 March 1984 also performed. -All the angiograms were reviewed to178
on April 12, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.52.2.178 on 1 August 1984. D
ownloaded from

Table Angiographic data of 12 patients with absent pulmonary artery
Case Intracardiac Age at operation Affected pulmonary Side of aortic Intrapencardial Origin o ductusNo anatomy on absent artery artery arch PA ordimp
1 Normal - L R ? Aorta2 Normal 9 yr R L - R innom3 LPV obstruction I yr R L - Rinnom4 VSD 12 yr L R - L innom5 VSD 3 yr L R - L innom6 Fallot I yr L R - L innom7 Fallot 6 mth L R - Linnom8 Fallot 9 yr L L + Aorta9 Fallot l yr L L + Aorta10 Fallot 5 d L L + Aorta11 PA and IVS 3 yr L L + Aorta12 UVH and PA 10 yr L L + Aorta
R, right; L, left; LPV, left pulmonary vein obstruction; PA, pulmonary atresia; IVS, intact ventricular septum; UVH, univentricular heart;innom, innominate artery; VSD, ventricular septal defect; -, absent; +, present.
determine the side of the aortic arch and the presenceand origin of a ductus arteriosus or ductus dimple.Natural and surgically created alternative sources ofblood supply to the affected lung were alsodocumented. Eleven patients underwent at least onesurgical procedure. The aim was to look for the absentpulmonary artery and, when found, to connect it tothe main pulmonary artery or to the systemic circula-tion.
Results
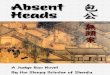
RADIOLOGICAL FINDINGSIn patients with a normal intracardiac anatomy or aleft to right intracardiac shunt, the chest x ray filmshowed that the lung on the affected side was smallerand had diminished pulmonary vascular markingscompared with the contralateral lung (Fig. 1).The affected pulmonary artery was on the opposite
side of the aortic arch in seven patients (cases 1-7),and this was the right side in two patients (cases 2 and
3). These seven patients had a variable intracardiacanatomy, some having a normal heart, some a left toright shunt, and others a low pulmonary blood flow(Table). In one of them (Fig. 2) a persistent ductusarteriosus had been shown on the left side at the firstangiocardiographic study (Fig. 2a); it had closed bythe time of the operation on that pulmonary artery(modified Blalock-Taussig shunt), as seen on thepostoperative angiocardiogram showing a ductusdimple and a patent shunt (Fig. 2b). In anotherpatient (Fig. 3) there was an absent right pulmonaryartery (Fig. 3a) and on that side a ductus dimple(Fig. 3b). At operation a pulmonary artery only at thehilus was found on the right side and was connected tothe main pulmonary artery with a vascular prosthesis(Fig. 3c).The absent pulmonary artery was on the side of the
aortic arch in five patients (cases 8-12). They all hadsevere right ventricular outflow tract obstruction. Inone of them the ductus was patent at the time of theinitial angiocardiogram and fed confluent pulmonary
a b i
Fig. 1 Chest x rayfilm showing a small and hypoperfused right lung in comparison with the left (a). Twoyears later, after a rightBlalock-Taussig shunt, the size of the right lung had increased (b).
Absent or occult pulmonary artety 179
on April 12, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.52.2.178 on 1 August 1984. D
ownloaded from

Presbitero, Bull, Haworth, Leval
e.
A:S
...... ,...g
..*...........
...S...a.;.-. j g:::.::
- :Xa '40Se:W.'t
... ;.:
aiFig. 2 Selective injection into a severely narrowed persistent ductus arteriosus arisingfrom a left innominate artery (right aortic arch)(a). The ductus was closed at the time of the operation and this is shown on the aortogram performed one year after a mofWiedBlalock-Taussig shunt (b).
arteries. Five years later angiocardiography failed toshow either the ductus or the left pulmonary artery(Fig. 4a, b).
SURGICAL FINDINGSOf all the 11 patients explored on the side of theabsent artery, the pulmonary artery was identifiednear or at the hilus in all but one, the exception beingthe oldest child aged 12 years (case 4). These 10patients included five in whom no intrapericardialvessel was found at operation (Table). In all of thesefive patients the hilar vessel was found to be in con-tinuity with a fibrous thread, the ligamentumarteriosum, arising from the innominate artery on theside opposite the aortic arch (Figs. 2 and 3).An intrapericardial element of the absent pulmon-
ary artery, continuous with a patent hilar pulmonaryartery, was found in five patients (cases 8-12). Themain and left pulmonary arteries were joined by ashort occluded segment. In three of the five patients(cases 8, 9, and 12) the interruption was a membraneat the junction between the left pulmonary artery andthe ligamentum arteriosum. In one patient (case 10)aged only 5 days a fresh thrombus occluded thelumen of the left pulmonary artery at its junction witha closed main pulmonary artery. In one patient (case11) a short atretic segment of intrapericardial arterywas identified, continuous with the hilar artery. In all
five patients a ligamentum arteriosum arising frombeneath the aorta on the side of the aortic arch wasfound at operation or necropsy.
In 10 patients in whom a pulmonary artery wasfound surgical procedures aiming to increase pulmo-nary blood flow included a systemic to pulmonaryartery shunt on that side in seven cases (Fig. 4c) and aconduit connexion between the main pulmonaryartery and the interrupted pulmonary artery in one(Fig. 3c). Furthermore, two patients without anintrapericardial pulmonary artery, who had had ashunt inserted, subsequently underwent connectionof the main pulmonary artery and the interruptedpulmonary artery. Fig. 5 shows one of these cases ofabsent right pulmonary artery with left aortic arch. Ashunt procedure was first performed on a small rightpulmonary artery. One year later that vessel wasappreciably larger (Fig. Sb). The right pulmonaryartery was then connected to the main pulmonaryartery with an 8 mm Gore-Tex prostlv,sis, and theshunt was closed (Fig. 5c). At the time of the secondoperation the proximal end of the right pulmonaryartery was excised together with the fibrous stringconnecting the pulmonary to the innominate artery.On microscopical examination a serial reconstructionof the tissue showed a closed ductus arteriosus withductal tissue extending into and occluding the rightpulmonary artery (Fig. 6).
180
*bz6... .4 ..-Z",
on April 12, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.52.2.178 on 1 August 1984. D
ownloaded from

Absent or occult pulmonary artery
c
Discussion
The present study confirms the pathological conclu-sions of McKim and Wiglesworth2 and Sotomoraand Edwards3 who pointed out, as, previously men-
tioned, that the distal portion and intrapulmonaryvessels of the so called absent pulmonary arteries are
in fact usually present. Thus the artery is usuallyoccult rather than absent.
Fig. 3 (a) Pulmonary angiogram showing absence of rightpulmonary artery. (b) Left ventricular angiogram showing aductus dimPle (arwed) ansingfrom a right imominate artery.(c) Pulmonary angiogram performed oneyear after comection ofthe right and main pulmonary artry with a Dacron conduit.
Although it is easy to understand why no intrapul-monary vessel opacifies from the systemic or pulmo-nary arterial circulation one would expect to be able toinject these occult arteries retrogradely by pulmonaryvenous wedge injection.4 Our three attempts at ven-ous wedge injection in this series were unhelpful. It isnot our practice to use general anaesthesia for cardiaccatheterisation. Injection into the pulmonary veins isa potent stimulus to coughing in the conscious
181
on April 12, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.52.2.178 on 1 August 1984. D
ownloaded from

Presbitero, Bull, Haworth, Leval
If .f ..
patient, and this may have impeded retrograde fillingof the pulmonary arteries in our patients.We have delineated two patterns of occult pulmo-
nary artery: patients with and without intrapericardialarteries. Typically, those without an intrapericardialpulmonary artery showed the anomaly on the sideopposite the aortic arch and had evidence of a ductuscoming from the innominate artery on the same side.
Fig. 4 Tetralogy ofFallot. As a neonate the left ventricularangiogram shows a left aortic arch with a persistent ductusarteriosus feeding co#luent pulmonary arteries (a). At the age ofSyears the left pulmonry artery is no longer visualised. ABlalock-Taussig shunt supplies the rightpulmonary artery (b). Aleft modfied Blalock-Taussig shunt was then perforned in theleft pulmonary artery (c).
Perhaps embryological atresia or early involution ofthe structure destined to become the intrapericardialartery on that side (the proximal part of the sixthaortic arch) is the primary defect in these cases. Thiscould occur if the heart is otherwise normal or whenany cardiac anomaly is present. If the sixth arch onthe side opposite the aortic arch does not persist themore primitive connexion with the intrapulmonary
182
a
n Amm
vI
[k-,.W.,::.., .uvmlb-
'M:4.4-
I
on April 12, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.52.2.178 on 1 August 1984. D
ownloaded from

Absent or occult pulmonary artery
b
ai
c
vessels may remain to feed the ipsilateral pulmonaryartery. This structure appears after birth to originatefrom the innominate artery and contains ductal tissue.If such an innominate ductus closes after birth theintrapulmonary artery on that side will lose its main
source of blood supply and not be demonstrable bycontrast injections into the pulmonary or systemic cir-culations. We have recorded this sequence of events
S Angiogram showing occult nghtpulnnary artery (a)ormal intracardiac anatomy. A shuntprocedure was mademail artery that was appreciably bigger oneyear later (b).essel was then connected to the mainpulmonary artery withthetic conduit and the shunt was closed (c).
in one of our patients (Fig. 2).The second group of patients had a small occluded
intrapericardial pulmonary artery in continuity withthe hilar vessels on the left side, best described as aninterrupted pulmonary artery. All had severe or com-plete right ventricular outflow tract obstruction andall were associated with a left ductus, whichdescended vertically from under the aortic arch.
183
1100",
on April 12, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.52.2.178 on 1 August 1984. D
ownloaded from

Presbitero, Bull, Haworth, Leval
Fig. 6 Photomicrographs showing(a) ductal tissue extendingfrom the ductus arteriosus (DA) into the right pulmonary artery (RPA)and (b) occluded right pulmonary artery immediately proximal to the closed ductus arteriosus.
AortoO % ..~~~~~~
DA*i
Fig. 7 Case 11: (a) Necropsy specimen showing occludedductus arteriosus (DA) protruding into the left pulmonary artery(LPA) leaving a lumen of less then 2 "m. (b) and (c)Photomicrographs ofa serial reconstruction showing occludedductus arteiosu (b) (original magnfication x 27) and orgin ofright (RPA) and leftpulmnary artery (LPA) (c); the kftpulmnary arteycons ductal issue extendingfrom the ductusarteiosus (original magnification x 35).
t,41~~~
\ o .:
184
on April 12, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.52.2.178 on 1 August 1984. D
ownloaded from

Absent or occult pulmonary artery
We postulate that patients in whom someintrapericardial artery is found at operation or nec-ropsy probably had confluent pulmonary arteries atsome stage. In one of our patients we have indeedevidence with serial angiograms that the anomaly wasacquired after birth and associated with the closure ofthe ductus (Fig. 4). A sling of ductus tissue can sur-round the aorta, opposite the insertion of a normal"horizontal" duct (which carries blood from the mainpulmonary artery to the descending aorta in fetal life);it has been postulated that constriction of such a duc-tus may lead to coarctation of the aorta.5 Patients withan interrupted pulmonary artery may represent theopposite lesion-"coarctation" of the pulmonaryartery at the site of inserton of a "vertical" ductus(which carries blood from the aorta to the pulmonaryartery in ductus dependent lesions).6 It is worth not-ing that stenosis at the origin of the left pulmonaryartery is a well described complication of tetralogy ofFallot and may well represent a lesion related to theocclusions we have described. In four such cases seenin recent years in our unit sequential angiographyshowed that stenosis occurred after birth and wasrelated to the closure of the ductus arteriosus. Thiswas confirmed by histological demonstration of ductaltissue, extending and protruding into the lumen of theleft pulmonary artery in one patient (Fig. 7).Having established that it is worth exploring the
patient for the occult artery, we have delineated twopatterns of the anomaly which may prove helpful inthe surgical management. In patients in whom thepulmonary artery on the side opposite the aortic archis absent there is unlikely to be an intrapericardialpulmonary artery, and a useful intrapulmonary vesselmay well be missed if only the pericardium isexplored-for example, through a sternotomy inci-sion. Moreover, these are the patients likely to requirea conduit to bridge the gap between the hilar andmain pulmonary artery when they come for completerepair. Conversely, in patients with interruption onthe side of the aortic arch the intrapericadial pulmo-nary artery is likely to be present and the gap shorterso that continuity is more readily established-forexample, with a patch.
In either group is seems advisable to search for themissing artery as early as possible as the vessel isunlikely to grow after the closure of the ductus
185
arteriosus; it may even be completely obliterated asseen in the 5 day old child (case 10), in whom a freshthrombus was found at operation. In experimentalanimals in which the left pulmonary artery was ligatedat birth the hilar and axial pulmonary arteries becamesmaller and were often obliterated by 4 to 6 months ofage in rapidly growing pigs, despite a satisfactorybronchial arterial supply to the intra-acinar pulmo-nary arteries.7 Such animals have a small lung withsmall alveoli. In the present study, the only patientwithout an identifiable hilar pulmonary artery wasaged 12, the oldest patient in the series.Thus all children with an interrupted pulmonary
artery should be assumed to have a pulmonary artery,if only at the hilus, into which it would be possible toinsert a prosthesis and so connect it to a systemicartery and ultimately to the pulmonary trunk. In thepresence of an intracardiac anomaly, blood flowshould be restored through the interrupted pulmo-nary artery as a first procedure. The intracardiacrepair can then be carried out later when the vascula-ture of both lungs has had time to benefit from themore even distribution of flow. The risk of intracar-diac repair may then be decreased.
References
1 Frantzel 0. Angeborener Defekt der rechten Lungenar-terie. Virchovs Arch [Pathol Anat] 1868; 43: 420.
2 McKim JS, Wiglesworth FW. Absence of the left pul-monary artery: a report of six cases with autopsy findingsin three. Am Heart J 1954; 47: 845-59.
3 Sotomora RF, Edwards JE. Anatomic identification ofso-called absent pulmonary artery. Circulation 1978; 57:624-33.
4 Singh SP, Rigby ML, Astley R. Demonstration of pul-monary arteries by contrast injection into pulmonaryvein. Br Heart J 1978; 40: 55-7.
5 Becker A, Anderson RH. Malformation of the aorticarch. In: Crawford T, ed. Pathology of congenital heartdisease. London: Butterworth, 1981: 321-38.
6 Santos MA, Moll JN, Drumond C, Araujo WB, RomaoN, Reis NB. Development of the ductus arteriosus inright ventricular outflow tract obstruction. Circulation1980; 62: 818-22.
7 Haworth SG, McKenzie SA, Fitzpatrick ML. Alveolardevelopment after ligation of left pulmonary artery innewborn pig: clinical relevance to unilateral pulmonaryartery. Thorax 1981; 36: 938-43.
on April 12, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.52.2.178 on 1 August 1984. D
ownloaded from