Embed Size (px)
Citation preview

3/2/2017
1
The Nervous System:
A Basic Approach to Recognizing Neuropathology
Julie Dylla Moczygemba, PA-CNeurosurgery
Department of Veteran Affairs
Course Objectives Review of Basic Neuroanatomy
Review Physical Exam of brain, spine, peripheral nerves, neuromuscular system
Workshop practice on Cranial Nerve Exam, Upper Extremity Exam, Lower Extremity Exam
Case studies

3/2/2017
2

3/2/2017
3

3/2/2017
4
NeuroAssessment
Brain
Cerebellum
Cranial Nerves
Cervical
Lumbar
Peripheral nerves
Neuro Assessment ToolsReflex hammer
Tuning fork
Safety pin, monofilament
Tuning fork
Ophthalmoscope
Visual Acuity card
Cotton swab or tissue
Soap and or coffee

3/2/2017
5
Gestalt Psychology
"The whole is other than the sum of the parts"
Kurt Koffka
Presenting symptom“How are you feeling?”
Headaches? Trauma? Pain? Worsening pain? Uncontrolled pain? Use Pain scale
Nausea/Vomiting?
Numbness?
Weakness?
Difficulty swallowing?
Change in voice?
Anxious?
Abnormal body movement?
Trouble staying awake?
**** Does the family see a change???? ****
History of Present IllnessOnset- events around the initial symptoms
Provoke- Alleviating and aggravating factors
Quality- burning, sharp, cutting, aching, change since onset
Region/Radiation
Severity- Pain Scale
Time- start time, occurred before?, sudden, gradual
Associated symptoms- numbness, paresthesias, “swelling”, “cold” sensation, edema
Adaptations

3/2/2017
6
Physical Exam
Focused exam
Identify trauma
Vital signs
Review of all medications
Labs
EEG
Imaging--CT, MRI, CTA, MRA, plain xrays, Bone Density studies, PET scans, Angiograms
Vital SignsRespirations- quality, pattern, distress, rate
Heart Rate- regular, brady, tachy, rhythm
Blood Pressure
Temperature
Pain level
Oxygen Saturation- RA or O2?
Review of MedicationsPrescribed- steroids, blood thinners,
antihypertensives, pain medications, gabapentin, pregabalin, amitrityline, dilantin, keppra, parkinsons, restless leg
OTC- tylenol, nsaids
Illicit- marijuana, cocaine, opiates, stimulants
Herbs, holistic, teas – Kratom?, fish oil
Hormone replacement- cortisone, thyroid
Taking prescriptions as prescribed?
Changes in prescription recently

3/2/2017
7
Past Medical History Seizures, Parkinson's, Tremor, Huntington disease
Migraines- cluster, ice pic, acephalgic, with aura, without aura, abdominal… ~21 different types
Cerebral aneurysm
Low back , neck pain, trauma
Cancer Diabetes
Untreated infection, prolonged infection, use of unclean needles, Dental work
TIA, Stroke, Wax/Wane difficulty in mentation or use of extremity
Chemical exposure, frostbite Bowel/Bladder problems
hydrocephalus
Depression, Anxiety
Past Surgical HistoryAneurysm clipping
Spine surgery
Craniotomy
Craniectomy- skull defect
Extremity Surgeries- knee replacement , carpal tunnel, ulnar decompression, shoulder
Abdominal surgery- free air, manipulation of peritoneal catheters/shunts, malabsorption
Labs and Imaging BMP- Sodium, OsmolalityCBC-H/H, WBC, PlateletsCoagCulturesUrine electrolytes, osmolalityB12, Vitamin D, toxins Hormone levels- cortisol, prolactin, TSH AED levels- DilantinCSF studies – Lumbar puncture, drain tapCT, MRI, Bone Density, MRA, CTA, Angio, plain xraysEMG, nerve conduction study

3/2/2017
8
Cerebrospinal fluidCSF production
Clear fluid
Produced by choroid plexus
450-750 ml/day in adults
25ml/day in peds
Absorbed by arachnoid villi, choroid plexus and lymphatics
Rate of absorption is pressure dependent
CSF studies
CSF studies include WBC, RBC, protein, glucose
In adults, CSF normally has 0-5 lymphocytes otherwise there should be no polys(PMN’s) or RBC’s
Protein 30mg/dl
Glucose 40-80 mg/dl
Focused Neuro Exam
Where do we start?
General Appearance alone, family present or outside the room
level of consciousness
dress and hygiene
posture
symmetry
involuntary movement, tremors at rest or motion, tics
behavior- consistent with pain, irritable,
what is on their bedside table
lines, IV, drips, monitors

3/2/2017
9
Inspection and Palpation
Inspect for atrophy, signs of trauma (ecchymosis, open wounds, rhinorrhea, otorrhea), incisions for errythema, edema, drainage
Palpation of skull, spine, shunt sites (head and peritoneum)
Cerebral ExamMini-mental exam
Cerebellum- Balance, coordination
GCS, Brain Death
ICP- intracranial pressure should be equal to central venous pressure 8-12mmhg, Monroe-Kellie Hypothesis
Motor exam
Ulnar drift
Sensory exam
Cranial Nerve exam
Mini Mental Status Exam Date orientation Place orientation Register 3 objects Serial sevens Recall 3 objects Naming Repeat a phrase Verbal commands Written commands Writing DrawingScoring 24-30 wnl, </= 23 cognitive impairment (needs further testing)

3/2/2017
10
Cerebellar function
Finger to nose
Point to Point
Heel to shin
Rapid alternating movement
Gait- Tandem, Poor balance- Veers
Rhomberg???
Glascow Coma Scale
Eye Opening 1-4
Verbal Response 1-5
Best Motor Response 1-6
Maximum Score 15
Minimum Score 3T
Glascow Coma ScaleEye Opening
4 awake and alert, looking around, watching tv, can wake with soft touch or normal voice
3 sleeping but awake easily with a loud voice, may fall back to sleep without verbal stimulus
2 patient wakes to painful stimulus
1 does not wake at all to painful stimulus

3/2/2017
11
Glascow Coma ScaleVerbal Response
5 “oriented” x4 (person, place, date and to reason they are in the hospital or to their health problem)
4 confused or disoriented- does not meet above criteria for orientation
3 inappropriate words- not only confused, but is using words that are out of context
2 incomprehensible sounds
1 none
Glascow Coma ScaleMotor Response
6 obeys commands
5 localizes to pain
4 withdraws to pain
3 abnormal flexion posturing, decorticate (pull in to the core/chest)
2 abnormal extension posturing, decerebrate
1 none
http://accesspharmacy.mhmedical.com/data/Books/gano24/gano24_c012f013.png

3/2/2017
12
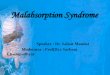
Brain Death ExamGCS 3T
1. Absence of Brainstem reflexes- fixed pupils, absent corneal reflex, absent oculovestibular reflex, absent oculocephalicreflex, absent gag
2. Apnea test
3. No response to deep central pain
4. Vitals- core temp > 32.2, SBP > 90mmhg (must have the absence of complicating conditions such as hypothermia, intoxication, shock, drug induced coma
Observation period- varies on injury, need for clinical confirmatory tests, anoxic brain injury, 0-24 hours
Intracranial Monitoring and Assessment
Normal ICP in adults= <10-15mmhg
Cerebral perfusion pressure(CPP) =MAP-ICP
Normal CPP in an adult is >50mmhg
Intracranial hypertension=>20mmhg
Primary causes of elevated ICP >15mmhg
Cerebral edema
Hyperemia: normal response to a head injury
Traumatic masses: epidural, subdural, and intraparenchymalhemorrhages, foreign body, depressed skull fractures
hydrocephalus
Hypoventilation
Systemic hypertension
Venous sinus thrombosis
Increased muscle tone and Valsalva maneuver as a result of agitation or posturing
Sustained posttraumatic seizures (status epilepticus)

3/2/2017
13
Secondary causes of elevated ICPDelayed epidural
hematoma
Delayed acute subdural hematoma
Delayed traumatic intracerebral hemorrhage
Cerebral vasospasm- as seen in subarachnoid hemorrhage
Severe ARDS
Delayed edema-more common in pedi
hyponatremia
Cerebral Motor and Sensory Exam
Homunculus

3/2/2017
14
Cerebral Exam- PearlsCerebral aneurysm rupture around the circle of Willis-->
subarachnoid hemorrhage--> worst headache, n/v, altered consciousness, sentinel bleed
Seizure- abnormal movement of the entire body or a body part which may or may not be associated with head turning, hallucinations, tingling, flashing lights, flushing, pallor, sweating, deja vu, dreamlike states, illusions. May be followed by aphasia, paralysis, loss of time (absence), impaired consciousness.
Migraine - unilateral head pain, ice pic, aura(contralateral), cluster, associated with n/v, light/sound sensitivity, plegia
Cerebral Exam- PearlsStroke- hemiplegia, facial droop, speech impairment,
hypertension, hypotension, hemianesthesia, visual field deficits
Brain tumor- visual field deficits, ataxia, headaches, seizures, weight loss, hx cancer
Meningitis- Meningismus(stiff neck, dural irritation), headache, AMS, fever, rash, (caused particles in the subarachnoid space-blood, virus, bacteria, chemicals)
Subdural hematoma- GCS, hx head injury, hx blood thinners, elderly, alcoholic, ulnar drift, ataxia, hemiparesis, fatigue/sleepy

3/2/2017
15
http://www.jkns.or.kr/fulltext/Fig/0042002100f2.jpg
Cranial Nerve Exam

3/2/2017
16
Cranial Nerve ExamCN I Olfactory- smell
CN II Optic- vision
CN III Oculomotor- eyelid movement, eye movement , parasympathetic pupil control
CN IV Trochlear- turns eye down and out
CN V Trigeminal- Facial sensation, chewing
CN VI Abducens-Lateral eye deviation
CN VII Facial- Facial muscle control
Cranial Nerve Exam CN VIII Vestibulocochlear- hearing, equilibrium
CN IX Glossopharyngeal- taste, senses carotid blood pressure
CN X Vagus-slows heart rate, stimulates digestion, senses aortic blood pressure
CN XI Spinal Accessory- shoulder strength and turning of the head, swallowing
CN XII Hypoglossal- movement and protrusion of the tongue

3/2/2017
17
CN 0- Terminal NervePhermones- studied in animals and humans and studied in humans. Thought to play in a role in the release of luteinizing hormone (LHRH) and is therefore thought to play role in reproductive behavior.
CN 1- Olfactory (Sensory)Transmits sense of smell to the brain
Coffee
Soap
Damage occurs commonly with head injuries, sinus surgery. Associated CSF rhinorrhea?

3/2/2017
18
CN II- Optic Nerve (Sensory) Transmits images on retina to the brain
Visual acuity (eye chart test)
Visual fields
Papillae function
Fundus (optic disc to cup ratio)
CN III- Oculomotor (mainly motor)Motor to most eye movements and sphincter pupillae,
medial rectus, inferior oblique, superior rectus, inferior rectus
Eye movement - up, down, inward/down
Eyelid placement- ptosis?
Eye displaced inferiorly and laterally
Fixed and dilated pupil, constrict with pilocarpine?--think intracranial
Pupil ExamPupil reaction (1-9mm)
Pinpoint pupils opioid and parasympathetic medications (pilocarpine)
Dilated pupils sympathomimetic meds, adrenaline, compression/damage of the ipsilateral cervical sympathetic chain, amphetamines, LSD, Atropine, psychedelic cocaine, mushrooms, Ecstasy, 3rd Cranial Nerve palsy, cataract surgery
Accommodation- CN II and CN III, pupil dilation with distance vision and pupil constriction with near vision
Convergence- Medial rectus, pupil constriction
Papilledema- Optic disc swelling (elevated ICP)

3/2/2017
19
Anisocoria (unequal pupils)Mydriasis (blown pupil)
Vision
Acuity
Double vision-CN defect
Peripheral Field-
Optic Chiasm-> Sellar mass
Mass along the Optic Radiation anywhere from the Occipital lobe through the Optic nerve.

3/2/2017
20
CN IV- Trochlear (Motor)Superior Oblique- depresses and rotates eye laterally
Think… LR6 SO4
Motor test: Eye movement , vertical/horizontal double vision
Superior Oblique Palsy- Stroke, trauma, birth, concussion, whiplash, aneurysm
CN V- Trigeminal (Sensory and Motor)
Sensory: Face sensation, corneal sensation
Motor: mastication muscles
Sensory test:
V1 Ophthalmic nerve
V2 Maxillary nerve
V3 Mandibular nerve
Corneal reflex- touch cornea with soft cotton swab
Motor test: Clench jaws, palpate masseter
CN V problems Trigeminal neuralgia
CN VI-Abducens (mainly motor)Motor: Lateral rectus (SO4 LR6)
Motor test: Eye abduction
Lateral rectus palsy- diabetes, stroke, trauma, viral illness, brain tumor, vascular inflammation, severe infections, migraines, elevated ICP

3/2/2017
21
CN VII- Facial (Sensory and Motor)Sensory: anterior 2/3 of tongue
Motor: muscles of facial expression, posterior belly of the digastric muscle, stylohyoid, stapedius, salivary glands secretion (except parotid), lacrimal gland
Sensory test: Taste- sweet, salty
Motor test: Raise eye brows, close eyes tightly, show teeth, puff out cheeks
Facial Nerve Palsy Bell’s Palsy
CN VIII- Vestibulocochlear (mostly sensory)
Vestibular-equilibrium
Cochlear- hearing
Mediates sensation of sound, rotation and gravity essential for balance and movement
Cochlear- rub fingers, tap fingers, snap
Vestibular- Syringe ears with water
Tuning fork
CN IX-Glossopharyngeal (Sensory and Motor)
Sensory- Taste for posterior 1/3 of the tongue and palatine tonsils
Motor- secretion from parotid gland, stylopharyngeus-elevates larynx and pharynx, dilates pharynx to allow passage of large food bolus
Gag reflex – tests CN IX sensory
CN X (Vagus) motor

3/2/2017
22
CN X-Vagus (Sensory and Motor)Sensory Taste (posterior 1/3 tongue), outer ear, meninges
MotorMuscles used in swallowing and speech, heart rate control (parasympathetic), peristalsis
Motor test: Gag reflex (sensory IX, motor X), phonation, swallowing , heart rate
Sensory: Taste, ear manipulation may cause coughing
CN XI- Spinal Accessory (Motor)Motor: Sternocleidomastoid, trapezius
Motor test: Shoulder shrug, head turning
CN XII-Glossopharyngeal (motor)Motor: Movement of the tongue
Motor test: Move protruded tongue side to side

3/2/2017
23
Cranial Nerve Exam Practice
Spine Assessment

3/2/2017
24
Neuro Spine AssessmentMotor- myotome
Sensory- dermatome
Reflexes- UMN vs LMN, Deep Tendon
Gait
Pain - radiation, reproducible with walking, coughing, sneezing, moving head, at night, am, pm
Tinels, straight leg raise
Muscle Strength Grading 5-> Normal strength
4-> Movement against resistance
4- slight resistance
4 moderate resistance
4+ strong resistance
3-> Movement against gravity
2-> Movement with gravity eliminated
1-> Trace or flicker of contraction. No joint motion
0-> No evidence of contractility
Cervical Spine-MyotomeC 3-4--> C4 nerve root- trapezius,
origination of phrenic n.
C4-5--> C5 nerve root - deltoid (arm abduction)
C5-6--> C6 - biceps, wrist extensors
C6-7--> C7- triceps, finger flexors and extensors
C7-T1--> C8- triceps, finger flexors

3/2/2017
25
Sensory Hemifacial pain- Trigeminal Nerve Dermatome pain- Nerve Root Impingement Peripheral Nerve distribution- CTS, guyon canal, cubital
tunnel, tarsal tunnel, Peroneal, Lateral Femoral Cutaneous Hemianesthesia- Thalamic stroke Sock distribution numbness-Peripheral Neuropathy Shoulder pain with abdominal free air- phrenic n.
irritation
Think symmetry and nerve distribution patterns. Use monofilament, pointer on reflex hammer, soft tissue, safety pin, light touch

3/2/2017
26
SensoryVibration
Position Sense- proprioception
Pin prick
Temperature
Light touch
Higher sensory functions
Deep Tendon Reflexes C6 nerve root- biceps tendon
C7 nerve root- triceps tendon
C6, C7 Brachioradialis- Supinator
L2,L3,L4 nerve roots - knee jerk reflex
S1 nerve root- ankle jerk
Upper motor neuronBrain and spinal cord injury
Hyperreflexia
+babinski
Clonus – 1-2 beats may be normal
+Hoffmann (cervical)
Spasticity
Bladder urgency, urge incontinence, frequency
Muscle cramping
Lhermittes

3/2/2017
27
Hoffmann’s reflex- UMNLift patient’s relaxed hand at the wrist with your non-dominant hand and take your dominant hand and place your thumb over the patient’s middle fingernail and put your index finger under the patient’s middle fingertip and flick the patient’s nail with your thumb. Watch for finger flexion response.
Gait Toe and heel Steppage Tandem SpasticWide basedMagneticAtaxicAntalgic
Observe rising from the sitting position. Wide based? Shuffle? Small steps? Speed? Ambulatory aides?
Balance and CoordinationBalance requires input from 2 of 3 inputs to the cortex
1. Visual confirmation of position
2. Non-visual confirmation of position (vestibular and proprioception)
3. Cerebellum
Rhomberg??

3/2/2017
28
Upper extremityCervical nerve root impingement
Brachial plexus
Ulnar nerve
Median Nerve
Serratus AnteriorC5,C6, C7- long thoracic nerve
Winging of scapula with wall push ups
Brachial plexusC5, C6, C7- wings from heaven, scapula
elevation
Tinels over the brachial plexus
Severe whole arm pain
History of arm injury

3/2/2017
29
Radial Nerve PalsySaturday night palsy caused by compression
of the radial nerve at the mid upper arm for an extended period of time
Painless wrist drop
Wrist extension 0/5
Ulnar NerveTinels at the cubital tunnel or guyon canal
Dropping things
Hyphothenar wasting
Pinky adduction weakness
Pinky and ring finger contraction spasms
Intrinsic wasting
Intrinsic weakness
Numbness of pinky and ring finger and medial middle finger

3/2/2017
30
Median Nerve+tinels at volar wrist
+phalens
Abductor pollicus weakness ( point thumb to floor and back to patient)
Abduction of pinky to thumb
Thenar wasting
Upper Extremity Exam PracticeVisual inspect for atrophy
Motor Exam –finger (abductors, adductors, flexors, extension and opposition) grips, wrist extensor/flexor, biceps, triceps, deltoid
Sensory Exam-Dermatome (nerve roots C4-8), median n., ulnar n., radial n.
Reflexes –biceps, triceps, brachioradialis, knee, ankle, crossed adductors
Proprioception-great toe
Tinels at wrist (carpal tunnel and guyon canal), elbow, brachial plexus
Gait- spastic, toe/heel

3/2/2017
31
Upper Extremity Neuro Exam Practice
Lower extremityLumbar nerve root impingement- herniated
disc, osteophytes
Cauda Equina Syndrome
Lumbar Plexitis
Peroneal nerve Palsy
Lateral Femoral Cutaneous- meralgia paresthetica
Peripheral Neuropathy
Lumbar spineHip flexor T12, L1, L2, L3- iliopsoas m.Hip adductor L2,L3,L4 -obturator n.Hip adductor L5 or gluteal n.Knee extensor L2,L3,L4 -femoral n., quadriceps m.Knee flexor - L5, S1- hamstring m.Dorsiflexor/inversion -L4, deep peroneal n., tibialis
anterior m.Dorsiflexor, EHL - L5, deep peroneal n., anterior
tibialis m. Plantarflexor, S1, gastrocnemius m.

3/2/2017
32
Lumbar Spine- nerve impingementL 4-5--> L4, knee jerk (can be absent after knee
surgeries especially knee replacement), quad weakness
Lateral disc at L5-S1--> L5, dorsiflexor weakness, EHLweakness, dermatomal numbness (top of foot to great toe), unable to heel gait, common herniation, distinguish between peroneal palsy
Medial disc at L5-S1 --> S1, toe gait weakness, calf and bottom of foot numbness, plantar flexor weakness, absent Ankle jerk (also seen in peripheral neuropathy)
Lower motor neuronClauda Equina syndrome- sacral anesthesia, urinary retention and overflow incontinence, focal lumbar radicular weakness, paraplegia, focal anesthesia, poor or no rectal tone.
Cause: sudden large herniated disc, large tumor causing severe cauda stenosis

3/2/2017
33
Peroneal PalsyProlonged pressure on lateral distal knee at
tibial head, painless foot drop
Can occur after knee surgery or injury
Lumbar plexitisPainful burning in multiple dermatomes of
one leg
Diabetes

3/2/2017
34
Lower Extremity Exam PracticeVisual inspection for atrophy
Motor Exam
hip flex, knee extension, dorsiflex, extensor hallicus longus, plantar flex, knee flexion
Gait- Toe, heel
Sensory Exam- Dermatome, peripheral nerve, sock distribution
Lower Extremity Exam
Reflex- Knee and Ankle, Clonus**, Babinski** (If has + UMN signs, must do UE exam including hoffmans)
Tinels at iliac crest
Straight Leg raise (tested when knee extended during motor exam)
Lower Extremity Neuro Exam Practice

3/2/2017
35
Case presentation #1
61 yo WM with Brooks-Spiegler syndrome (multiple dermatologic neoplasms) presented to the ER with progressive left sided weakness, short term memory , balance and vision problems and decreased in concentration over the past several months.
Physical ExamOverall, affect pleasant and appropriate, oriented to
self and place but not time, calculation slow.
Grossly preserved strength throughout. Left drift present.
Left homonymous hemianopsia. EOMs intact. Facial movement, sensation intact.
Sensation--light tough appears intact however proprioception impaired on the left side and some left/right confusion present.

3/2/2017
36
Case presentation #2Mr. P is a 44 y/o m with hx of chronic neck pain
presents with worsening right arm pain x 2 years. Has associated tingling and numbness of the right hand, specifically the middle 2 fingers and for arm. Worse when turning the head to the right. This position also reproduces arm pain in the same distribution. Has associated pain in the right shoulder and hand with motion and the symptoms do not wake him at night. Denies lhermittes, b/b problems, balance disturbances, finger infacility, dropping things.
Medications – Case #2Lithium 450mg bid
Lexapro 20mg daily
Gabapentin 300mg at bedtime
Hydrocodone 10mg q6 hour prn
Flexeril 10mg daily
Methacarbamol ?dose
tramadol 50mg bid prn
Physical Exam- Case #2Healthy WM, NAD, GCS 15, MAEW
Gait: steady, good stride
Strength testing: Right Left
Deltoid 5/5 5/5
Biceps 5/5 5/5
Triceps 4/5 5/5
Wrist flex 5/5 5/5
Wrist ext. 5/5 5/5
Grip 5/5 5/5
Interossei 5/5 5/5

3/2/2017
37
Physical Exam- Case #2DTR's Right LeftBiceps 2/4 2/4Triceps 0/4 2/4Brachiorad. 2/4 2/4Knee 2/4 2/4Ankle 2/4 2/4
Hoffman's - negativeBabinski – not testedClonus - negativeCrossed tibioadductors- not tested
Physical Exam- Case #2
Tender right trapezius and rotator cuff
Negative tinels at the wrist and elbow
+spurlings- reproducible arm symptoms

3/2/2017
38
Case Presentation #3Pt is a 38 yo male who has had >10 years of low back pain with intermittent lower extremity pain, radicular in nature. ~6 weeks ago, he was washing his car and the next day had a worsening of his low back pain. He came into the ER and was to follow up with neurosurgery in clinic with an MRI of his lumbar spine but for various reasons did not come to clinic. He was instructed upon discharge if his symptoms worsen to immediately return to the ER. 1 week later, he began having lower extremity weakness and urine dribbling. He presents today to the ER after 3 weeks of the above listed symptoms which include low back pain, bilateral lower extremity burning, mainly L5 distribution, bilateral lower extremity weakness, and urinary dribbling.

3/2/2017
39
Physical Exam-Case #3 Motors: 5/5 BUE 4+/5 BLE all muscle groups except dorsiflexion 4/5 bilateral dorsiflexion, very slow to initiate dorsiflexion
but once initiated can resist moderate force sensation to soft touch diminished in bilateral feet sensation to temperature grossly intact Knee jerk 2+/4 bilateral Ankle jerk 0/4 bilateral No clonus Normal response to sole stroke (babinski) Normal rectal tone Post void bladder scan 40cc

3/2/2017
40
Case Presentation #4(April 2016)
50 y/o female with hx of obesity, depression, HTN, uterine fibroids, presents to the ER for pelvic pain that radiates to the lower legs bilaterally, is a 8-9/10, sharp burning, intermittent.
Exam:
Motor 5/5
2+ DTR
-SLR
Labs, pelvic studies, plain xrays all normal, hcg negative, UA neg
Plan: consider MRI , NS consult
methylprednisolone 4mg dose pack
gabapentin 300mg po QHS for neuropathic discomfort
tramadol 50mg po QID PRN for severe discomfort
Case presentation #4Patient did not show for nerve conduction studies and did not return call for initiating PT.
MRI results came back and PCP placed consult to NS.

3/2/2017
41
Lumbar MRI without contrastMay 2016

3/2/2017
42
Neurosurgery ConsultJuly 2016- Presents to clinic with continued low back pain and left leg pain. States pain continues to radiate down the leg to the foot. Denies bowel or bladder changes, urinary retention, perineal or sacral numbness or paresthesia. Prefers surgery.
Exam: Normal 5/5 strengthNormal KJ and AJ reflexesNeg straight leg raise
Plan: Wait and watch. RTC 6 weeks.
Over the next 5 months…There are 6 documented phone calls, appointment cancellations with final decision to proceed with surgery.
Another MRI was scheduled and a preop visit was made.
January 2017…now 9 months after acute herniation
Patient returns to preop clinic with improved but not completely resolved radiculopathy.

3/2/2017
43
MRI reviewed with patient and surgery was cancelled. Patient has been offered steroid injections through pain management.
Studies show that most lumbar disc herniation syndromes resolve without surgical intervention.

3/2/2017
44
Thank You
Citations1. "Brain and Heart labeled images." Cool MRI Stuff.
Turbospinecho , 19 Jan. 2013. Web. 3 Jan. 2017. <https://coolmristuff.wordpress.com/2013/01/19/brain-and-heart-labeled-images/>. Brain Anatomy
2. Greenberg, Mark S., and Mark S. Greenberg. Handbook of neurosurgery. 5th ed. Tampa, FL: Greenberg Graphics, 2001. Print.
3. Hoppenfeld, Stanley, and Richard Hutton. Physical examination of the spine and extremities. New York: Appleton-Century-Crofts, 1976. Print.
4. "Neuroscience: week 2." ProProfs Flashcards. N.p., 19 Jan. 2013. Web. 3 Jan. 2017. <http://www.proprofs.com/flashcards/cardshowall.php?title=neuroscience-week-2>. (855) 776-7763




![Sample Nursing Assessment Form · [ ] nasal feeding tube [ ] impaired swallow reflex [ ] absent or hyperactive gag reflex [ ] reduced level consciousness [ ] infectious saliva from](https://img.pdfslide.us/doc/110x75/5d5a696b88c99355448be1e0/sample-nursing-assessment-form-nasal-feeding-tube-impaired-swallow-reflex.jpg)