Embed Size (px)
Citation preview

Abnormal PsychologyAbnormal Psychology
WEBWEB

Anxiety as a Normal and an Abnormal Response
• Some amount of anxiety is “normal” and is associated with optimal levels of functioning.
• Only when anxiety begins to interfere with social or occupational functioning is it considered “abnormal.”

The Bell Curve

Phobic Disorders
• Phobias
1. Specific phobias
2. Social phobia
3. Agoraphobia

Specific Phobias

Social Phobia
• General characteristics
Fear of being in social situations in which one will be embarrassed or humiliated

Panic Disorder With and Without Agoraphobia
• Panic disorder
• Panic versus anxiety
• Agoraphobia
• Agoraphobia without panic

Panic and the Brain

Panic Disorder: The Cognitive Theory of Panic

Treating Anxiety Disorders
• Medications
• Behavioral and cognitive-behavioral treatments

Generalized Anxiety Disorder
• General characteristics
• Prevalence and age of onset
• Comorbidity with other disorders

Generalized Anxiety Disorder:Biological Causal Factors
• Genetic factors
• A functional deficiency of GABA
• Neurobiological differences between anxiety and panic

Obsessive-Compulsive Disorder
• Obsessions- repetitive unwanted ideas that the person recognizes are irrational
• Compulsions- repetitive, often ritualized behavior whose behavior serves to diminish anxiety caused by obsessions

Post-Traumatic Stress Disorder
• Critical Component – Symptoms occurs AFTER a traumatic stressor

Symptoms Categories
• Intrusive– distressing recollections– dreams– flashbacks– psychological trigger reactions– physiological trigger reactions

Symptoms Categories
• Avoidance– avoid thoughts, feelings or discussions– avoid activities, places– memory blocks– anhedonia (without pleasure)– numb– alexithymia (emotions unknown)– feeling of doom

Symptom Categories
• Hyperarousal Symptoms– sleep disturbance– anger problems– concentration– startle response– “on guard” hypervigilence

Mood Disorders
• Major Depressive Disorder
• Bipolar I and Bipolar II
• Cyclothymia– Hypomania
• Dysthymia
• Schizoaffective disorder

Categories of Personality Disorders
• Cluster A– Paranoid– Schizoid– Schizotypal

Personality Disorders
• Paranoid personality disorder
• Schizoid personality disorder
• Schizotypal personality disorder
• Histrionic personality disorder

Categories of Personality Disorders
• Cluster B– Histrionic– Narcissistic– Antisocial– Borderline

Categories of Personality Disorders
• Cluster C– Avoidant– Dependent– Obsessive-compulsive

The Clinical Picture in Schizophrenia
• Positive symptoms– Delusions: fixed firm beliefs with no basis in
reality• Most common are grandiose, persecutory
and referential– Hallucinations: disturbances in perception
• Can occur in any of the five senses– Most common are auditory and visual

The Clinical Picture in Schizophrenia
• Formal Thought Disorder (a positive symptom)
– Disturbances in speech that reflect underlying problems in cognition or thinking
• Most common forms are tangentiality and circumstantiality
• Less common are neologisms, word salad and clang associations

The Clinical Picture in Schizophrenia
• Negative symptoms (Nancy Andreasen)– Avolition– Anhedonia– Alogia– Flat Affect– Asociality

The Classic Subtypes of Schizophrenia
• Undifferentiated type
• Catatonic type
• Disorganized type
• Paranoid type

Graph of HS drug use

Substance-Related Disorders
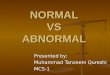
Methods of taking substances:
7 sec
inhaling
20 sec
IV
4 min
snortor
Intramuscularinjection
30 min
oral

When is addiction addiction?
• What is substance use?
• What is substance abuse?
• What is substance dependence?
Where is the line???????

DSM-IV CriteriaSubstance Abuse
leads to impairment or distress
one of these within 1 yr: failure to full fill role
obligations physically hazardous legal problems persistent social
problems
Substance Dependence leads to impairment or
distress 3 of the following:
tolerance withdrawal
delirium tremens (DTs) take more than intended persistent desire fail to control use lots of time spent
obtaining, using, or recovering from
use in place of activities continuing despite physical
or psychological problems

Solomon’s Opponent Process Theory of Addiction
• Basic Premise- People take, abuse and become dependent on drugs because of the effect of these drugs
• The Clements Corollary- noone ever becomes addicted to thorazine– A State- the initial pleasant effect– B State-unpleasant effects occurring as a result
of drug withdrawal

The Clinical Picture of Alcohol Abuse and Dependence
• Alcohol’s effects on the brain
• Physical effects of chronic alcohol use
• Psychosocial effects of abuse and dependence

Alcohol (ETOH)Short-term effects:
absorbed from the stomach into the blood
metabolized by the liver (1 oz/hr)
it is a drug acts within brain to:
stimulate GABA receptors reduces tension
dopamine/serotonin levels pleasurable aspects of
intoxication inhibits glutamate receptors
diminishes cognitive abilities
Long-term effects: reduced food intake
ETOH: no nutrient value impairs food digestion results in vitamin deficiency
B-complex
can lead to brain damage/amnesia kills brain cells leads to loss of gray matter
from the temporal lobes Korsakoff’s Syndrome
suppresses the immune system

Alcohol (ETOH)
A “drink”: 1 oz. Spirits = 1 glass wine = 1 beer
DWI (Driving while intoxicated) takes approximately 2-4 drinks over one hour lighter weight, empty stomach will require less legal blood alcohol limit (.10%)
DUI (Driving under the influence) The CAGE

Alcohol Addiction: Treatment
Admitting the problem a prerequisite for therapy (video clip)
Inpatient Hospital treatment expensive & does not lead to better results may be necessary for safe detoxification
Aversion therapy Antabuse - drug that creates nausea uses operant conditioning principles
Controlled drinking training Self-Help groups
Alcoholics Anonymous