Embed Size (px)
Citation preview

Emergency g yCare Institute
NSW
Abdominal pain
Objectives
Abdominal PainObjectives
Common abdominal problemsA di i i Appendicitis
Hernia Gastrointestinal foreign bodies Gastrointestinal foreign bodies Gastrointestinal haemorrhage
UpperL Lower
Renal colic Urinary retentiony
Index

Emergency Abdominal PainPeritoneumPeritoneum
Index
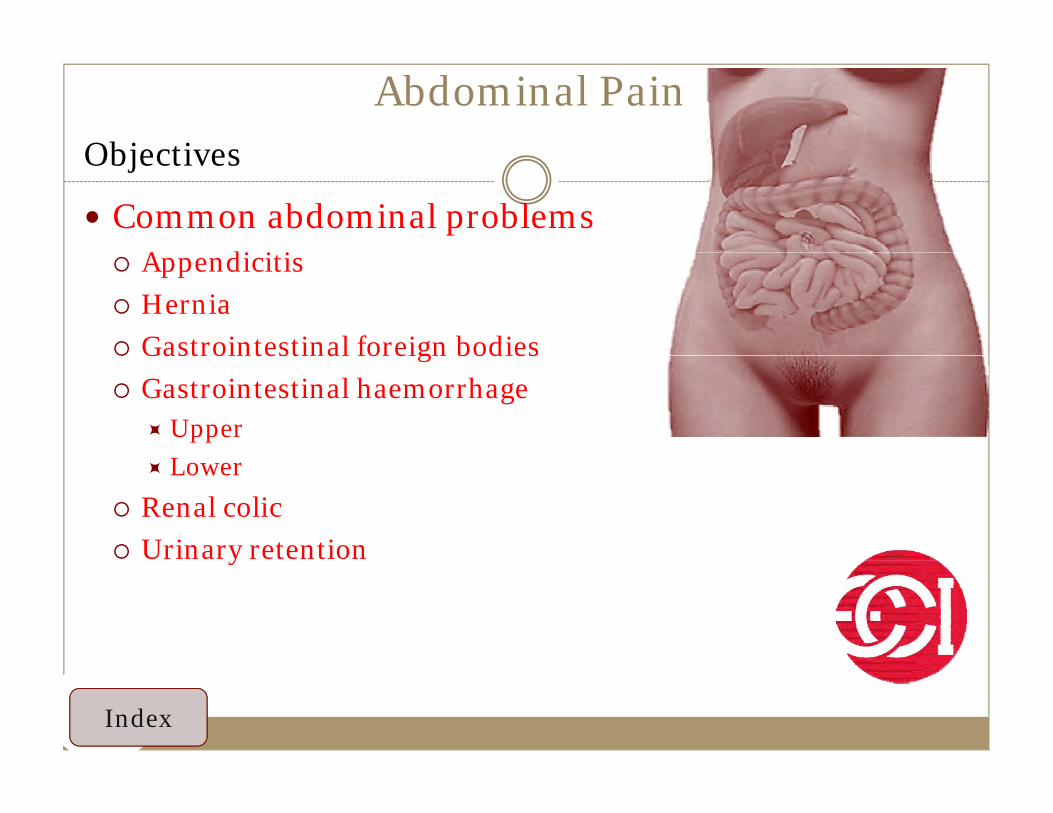
Common abdominal presentationsHistoryStereotypes of pain onset and associated pathologies
Sudden onset (full pain in Rapid onset (minutes - hours) Gradual onset (hours)( pseconds)
p ( ) ( )
Perforated ulcer Strangulated hernia Appendicitis
Mesenteric infarction Volvulus Strangulated hernia
Ruptured AAA Intussusception Peptic ulcer disease
R t d t i A t titi I fl t b l diRuptured ectopic pregnancy Acute pancreatitis Inflammatory bowel disease
Ovarian torsion or ruptured cyst Biliary colic Mesenteric lymphadenitis
Pulmonary embolism Diverticulitis Cystitis / urinary retention
AMI Ureteric / renal colic Salpingitis / prostatitis

Common abdominal presentationsHistoryPossible causes of pain by location
Location Associated pathologies
Right upper quadrant (RUQ) [Liver, R kidney, gallbladder]
Acute cholecystitis, biliary colic, duodenal ulcer, R lower lobe pneumonia, acute hepatitis
Right lower quadrant (RLQ) [Ascending colon, appendix, fallopian tube, ovary, ureter]
Appendicitis, ectopic pregnancy, tubo-ovarian abscess, ruptured ovarian cyst, ovarian torsion, distal ileitis
Left upper quadrant (LUQ) Gastritis acute pancreatitis splenic pathology L lower lobe pneumoniaLeft upper quadrant (LUQ) [Pancreas, spleen, L kidney]
Gastritis, acute pancreatitis, splenic pathology, L lower lobe pneumonia
Left lower quadrant (LLQ) [Sigmoid / descending colon, fallopian tube,
t ]
Diverticulitis, ectopic pregnancy, tubo-ovarian abscess, ruptured ovarian cyst, ovarian torsion
ovary, ureter]
Midline or periumbilical Appendicitis (early), gastroenteritis, mesenteric adenitis, myocardial ischaemia or infarction. pancreatitis
Flank Abdominal aortic aneurysm leak / rupture, ureteric / renal colic, pyelonephritis
Front to back Acute pancreatitis, abdominal aortic aneurysm leak / rupture, retrocaecal appendicitis Posterior duodenal ulcerappendicitis. Posterior duodenal ulcer
Suprapubic / lower abdominal Ectopic pregnancy, mittelschmerz, ruptured ovarian cyst, pelvic inflammatory disease, endometriosis, urinary tract infection

Common abdominal presentationsHistoryStereotypical location of pain and embryonic derivatives
Location of pain Organs Embryonic derivative Nerve supply
Epigastrium Stomach, first two parts of duodenum, liver,
gallbladder, pancreas
Foregut Vagus nerve (parasymathetic)Greater thoracic gallbladder, pancreas Greater thoracic
splanchnic nerves (sympathetic)
Periumbilical Third and fourth part of Midgut Vagus nerve Periumbilical Third and fourth part of the duodenum, jejunum, ileum, caecum, appendix, ascending colon, first two thirds of transverse colon
Midgut Vagus nerve (parasymathetic)Greater thoracic
splanchnic nerves (sympathetic)
Hypogastrium Distal one third of transverse colon,
descending and sigmoid
Hindgut, genitourinary Pelvic splanchnic nerves (parasymathetic)Lesser thoracic descending and sigmoid
colon, rectum and upper portion of anal canal, reproductive organs
(ovaries, fallopian tubes, uterus, seminal vesicles,
Lesser thoracic splanchnic nerves
(sympathetic)
uterus, seminal vesicles, prostate), bladder
Index

Appendicitis
Common Abdominal PresentationsAppendicitis“…in every case the seat of greatest pain, determined by the pressure of one finger,y p f f g ,has been very exactly between an inch and a half to two inches from the anterior spinousprocess of the ileum on a straight line drawnprocess of the ileum on a straight line drawnfrom that process to the umbilicus. Taken in connection with the history of the case and the other well known signs, I look upon as almost other well known signs, I look upon as almost pathognomonic of appendicitis…”
Charles McBurney, 1889 to the New York Surgical Society
Index

Worrying stats
Abdominal painWorrying stats
Common and urgent surgical illnessl f h h l h h Several manifestations with much overlap with other
clinical syndromes - high degree of suspicion!Si ifi t bidit i i ith di ti Significant morbidity, increasing with diagnostic
delay No single sign symptom or diagnostic test No single sign, symptom, or diagnostic test
accurately confirms the diagnosis of appendicitis in all cases
Peak age 11-20

Worrying stats
Abdominal painWorrying stats
Incidence 25/10,000 (10-17), 1-2/10,000 (<4)f k k f l f f l Lifetime risk 8.6% risk for males, 6.7% for females
Previous similar pain in ~30-70% of cases Perforation rate is -higher among patients <18yrs
and patients >50yrs, possibly because of delays in diagnosisdiagnosis
Appendix perforation associated with a significant increase - in morbidity and mortality ratesincrease in morbidity and mortality rates
Mortality >20% in patients over 70yrs

Worrying stats
Abdominal painWorrying stats
Variable positions (relevant to presentation)l Retrocaecal in 30%
Pelvic in 30% Subcaecal in 2% RUQ in 4% Anterior in 1%

Pathophysiology
Abdominal painPathophysiology
Usually luminal obstruction, possibly following viral GI ill GI illness
Distension due to ongoing epithelial secretionI d i hibit l h ti / Increased pressure inhibits lymphatic / venous
drainage Bacterial invasion Bacterial invasion Progressive oedema with eventual obstruction of
arterial blood flowarterial blood flow

Complications
Abdominal painComplications
Acutef Perforation
Abscess formation Peritonitis Long term Adhesions Infertility (females) Mortality as previously mentioned

History
Abdominal painHistory
Classic history - anorexia + periumbilical pain, f ll d b RLQ i d iti 50%followed by nausea, RLQ pain and vomiting - 50% of cases.
Migration of pain from periumbilical area to RLQ Migration of pain from periumbilical area to RLQ -most discriminating feature of patient's history -sensitivity and specificity ~ 80%sensitivity and specificity 80%

History extremes of age (Bad)
Abdominal painHistory extremes of age (Bad)Children Incidence low in <2
Al ll i i i ll i di d Almost all initially misdiagnosed Perforation rates 90% infants <1 80% aged 1-4g 4 10-20% adolescents Incidence peaks in late teensElderly 5 10% aged over 60yrs 5-10% aged over 60yrs >50% of all deaths Most cases perforated at operation 50% post operative complication rate Fibrosed appendiceal wall Impaired blood flow 2° to atherosclerosis Poor immune system 1/3 complain of constipation 1/3 complain of constipation

Examination
Abdominal painExaminationMost specific physical findings Rebound tenderness - remember you do not have to use traditional (cruel) y ( )
techniques to elicit rebound , use percussion tenderness Rigidity Guarding RLQ tenderness present in 96%, but nonspecific Positive cough sign (sharp pain in the RLQ elicited by a voluntary cough)
?helpful in diagnosis of localised peritonitis RLQ pain in response to percussion of a remote quadrant of the abdomen, or to
firm percussion of the patient's heel, suggests peritoneal inflammation

Examination
Abdominal painExamination Markle sign - pain elicited in the abdomen when standing patient drops from
standing on toes to the heels with a jarring landing - is stated to be very sensitive for localising true peritonitis
Psoas sign - indicator of irritation to hip flexors in the abdomen - psoas lies under appendix; passive extension of the thigh of a patient with knees extended. pain is positive psoas signpain is positive psoas sign
Obturator sign - indicator of irritation to obturator internus in the abdomen -obturator comes into contact with appendix on hip rotation; pain is positive obturator signb g
Rectal examination - inconsistent literature, but not probably not useful in patients with clear history and examination suggesting appendicitis. May be useful in equivocal cases. Paediatric PR examination is left to the surgeon who may operate

Investigation
Abdominal painInvestigationFBC ? 80-85% WBC >10,000 & neutrophilia (NØ) >75% in 78% adults with appendicitis <4% WBC <10,000 & NØ <75% Many nonspecific results with either WBC or NØ changes Inconclusive evidence in elderly and children Inexpensive, rapid, widely available but findings nonspecific; 4% of cases missed Does not rule out appendicitis
CRP ? Acute phase reactant synthesized by the liver in response to bacterial infection. -in 6-12 hrs of acute tissue
inflammation Adults - normal CRP 100% negative predictive value if symptoms >24 hrs Low specificity 50-87%, as CRP does not distinguish between bacterial infections May be used as part of a triple screen (WCC, neutrophilia, CRP) May rule out appendicitis in some patients
Urinalysis ? ~1/3 patients with acute appendicitis complain of dysuria / right flank pain 1 in 7 had pyuria >10 WBC / high power field, and 1 in 6 patients >3 RBC per high power field Diagnosis of appendicitis should not be dismissed due to the presence of urological symptoms
or abnormal urinalysis Does not rule out appendicitis

Investigation
Abdominal painInvestigation CT 3 Varying trial results
N h d CT i 8 % i i % ifi Addi i f IV d l Non-enhanced CT - 211 patients - 87% sensitive, 97% specific. Addition of IV and oral contrast agent increased sensitivity to 96-98%
2004 - pediatric patients, non-enhanced CT 66% sensitive; 90% with IV contrast 2005 - 112 pediatric patients, non-enhanced CT 87.5% sensitive, 98.7% specificity
R di h li l CT i d l 6% i i % ifi Recent studies - noncontrast helical CT in adults - 91-96% sensitive, 92-100% specific Noncontrast CT in children 66% sensitive, increased to 90% with intravenous contrast material Helical CT with rectal contrast in children - sensitivity of 95-97 Reduced negative laparotomy rate and appendiceal perforation rate when pelvic CT used in selected
ipatients Study of asymptomatic volunteers undergoing pelvic CT - 42% "abnormal" appendiceal diameter of >6
mm and 78% did not fill after oral contrast Bottom line - CT is useful, but NOT an ED rule out test, and should NOT delay surgical review
USS -is operator and patient factor dependent. Not seeing an appendix does not rule out appendicitis. Need CT after a negative USS. ?
Plain abdominal X-ray - insensitive, nonspecific, and not cost-effective. X

Management
Abdominal painManagement Watch and wait Antibiotic, watch and wait ( cef and met), this is increasing
S i S i l Semi urgent Surgical Urgent surgical
Fear of the negative laparotomy is almost greater than fear of complications

PROPERTIESAllow user to leave interaction: After viewing all the stepsShow ‘Next Slide’ Button: Show upon completionCompletion Button Label: Next Slide
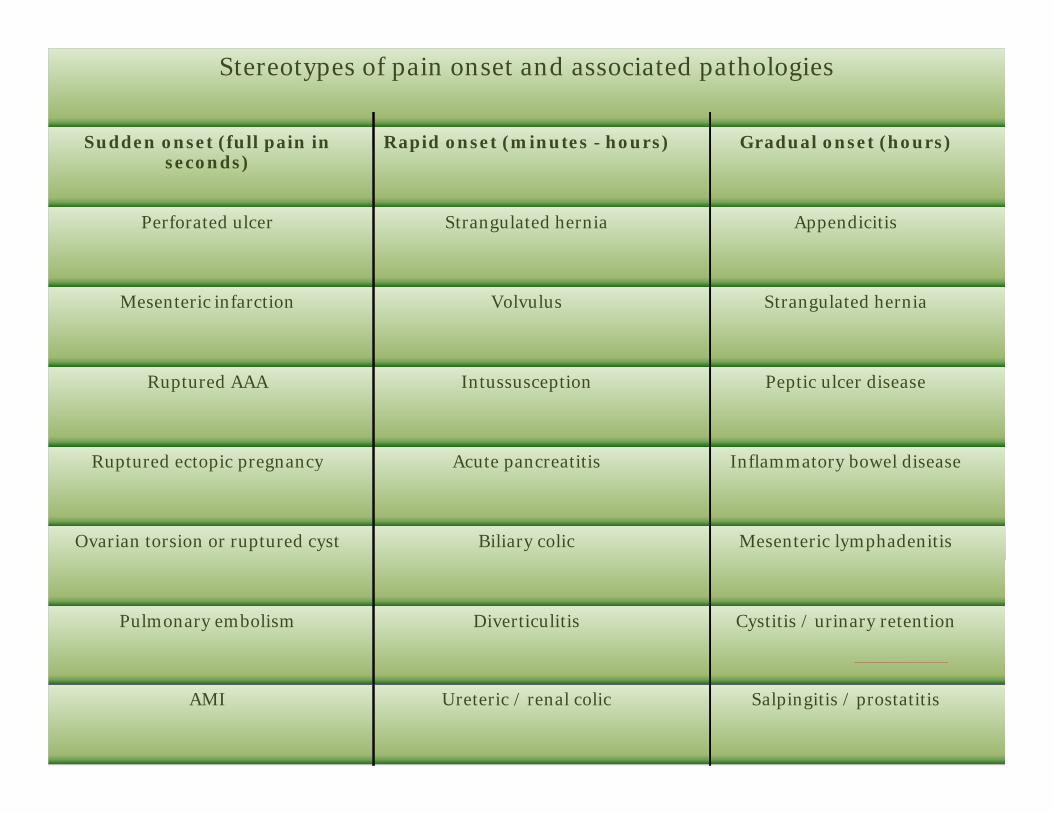
Introduction
CT obdo, showing appendicitis
~ ® Properties.. J Edit in Engage J

PROPERTIESAllow user to leave interaction: After viewing all the stepsShow ‘Next Slide’ Button: Show upon completionCompletion Button Label: Next Slide
(
• Common and urgent surgical illness • Several manifestations with much overlap with other clinical syndromes - high
degree of suspicion! • Significant morbidity, increasing with diagnostic delay
)
• No single sign, symptom, or diagnostic test accurately confirms the diagnosis of appendicitis in all cases
• Peak age 11-20
IS ory
U'll.iil-41fa11r.'!Sr.m-----------------------------1
~ ® Properties.. J Edit in Engage J

Abdominal PainIndex returnIndex-return
Index

PROPERTIESOn passing, 'Finish' button: Goes to Next SlideOn failing, 'Finish' button: Goes to Next SlideAllow user to leave quiz: After user has completed quizUser may view slides after quiz: At any timeUser may attempt quiz: Unlimited times
Pregnant woman RLQ pain t '~PI!NBff r ef r ,.)
A 25 year old woman presents with R lower quadrant pain she is 14 weeks pregnant, she has R lower quadrant tenderness and has anorexia and low grade fever. What investigations do you do? Select the best answers.
D Urinalysis
D FBC, EUC, CRP, LFTs, lipase
D D Dimer
D Pelvic ultrasound and ask tor the radiographer to look tor the apppendix
D Abdominal xray
..... .....
[~ Properties ... J r ~ Edit in QuiZ/Tiaker l I

Hernia
Common Abdominal PresentationsHernia
‘A protrusion of a viscous from its proper cavity. The t d d t ll t i d i lik protruded parts are generally contained in a sac-like
structure, formed by the membrane with which the cavity is naturally lined’ Astley-Cooper 1804cavity is naturally lined Astley Cooper 1804
Several different types of abdominal wall hernia exist, with various names
Usually encountered in routine examination or when complications of hernia occur

Hernia Types of hernia
Common Abdominal PresentationsHernia – Types of hernia
InguinalDi Direct
Indirect
Femoral Femoral Incisional Umbilical / paraumbilical Umbilical / paraumbilical Obturator Spigelian Spigelian

Hernia Types of hernia
Common Abdominal PresentationsHernia – Types of hernia
Clinical presentationd bl Reducible
Irreducible Incarcerated Strangulated

PROPERTIESAllow user to leave interaction: After viewing all the stepsShow ‘Next Slide’ Button: Show upon completionCompletion Button Label: Next Slide
( )
(~~~~~~~~~ ~ Common presentation to ED for evaluation
• Foreign bodies (FBs) in the upper GIT are usually swallowed. purposefully or accidentally
• Presentations range from patient in extremis to patient with subtle I chronic findings with no clear history
• Patients can often localise oropharyngeal and upper 1/3 oesophageal foreign bodies.
• lower 2/3 oesophagus FBs are difficult to localise
• Scratches I abrasions to mucosal surface can create a foreign body sensation
• Chronic foreign bodies or perforations can cause infections in surrounding soft tissues of the throat and neck
• Oesophagus has 3 areas of narrowing -
........... -·
~ ® Properties.. J Edit in Engage J

Common abdominal presentationsClinical indicator Probable upper
GIT sourceProbable lower
GIT source
Gastrointestinal haemorrhageHaematemesis Almost certain Rare
Melaena Probable Possible
Haematochezia Possible Probable
Blood streaked stool Rare Almost certain
Occult blood in stool Possible PossibleOccult blood in stool Possible Possible
PROPERTIESAllow user to leave interaction: After viewing all the stepsShow ‘Next Slide’ Button: Show upon completionCompletion Button Label: Next Slide
( )
(~~~~~~~~~ • -20% of all GIT haemorrhage r.ao«GII~c>l.l!lJ "'
• Mortality dependent on • Age • multi-organ system disease • need for transfusion >5 units • need for surgery • recent physiological stress (trauma. sepsis
etc)
IS ory
--flO! "'
~ ® Properties.. J Edit in Engage J
PROPERTIESAllow user to leave interaction: After viewing all the stepsShow ‘Next Slide’ Button: Show upon completionCompletion Button Label: Next Slide
(
The pain is very severe. and its important not forget that just because we find the diagnosis and treatment options basic that the symptoms are very significant to the patient.
)
The lifetime rate of kidney stones in the general population is approximately 12% for men and 4% for women and this approximately doubles with history of renal colic in a family member. Peak incidence 35-45. Renal failure is not common there are risks for it though: Solitary kidney. diabetes. staghorn calculi. spinal injury, recurrent stones with infection. When renal failure is a c oncern the after risk assessment rehydration is the key for management of this. Studies in animals have suggested that renal damage may begin within 24 hours of a complete obstruc tion and permanent kidney deterioration starts within 5-14 days. agreement in the literature is not good as to the exact time. but we can be comfortable w ith a risk free 3-4 days.
Common causes: • Hypercalciuria • Hyperuricosuria
~ ® Properties.. J Edit in Engage J

Summary
Common Abdominal PresentationsSummary
Careful history including any changes from normal b l h bitbowel habits
Careful examination including full exposure and rectal and vaginal examinations as clinically indicatedand vaginal examinations as clinically indicated
Give adequate analgesia always Continuing observation of trends in pain or physiology Continuing observation of trends in pain or physiology
is one of our best diagnostic tools Err on the side of cautionErr on the side of caution Always advocate for the patient