Embed Size (px)
Citation preview
Speeding up decisions – the right monitoring tools at the right time
Splanchnic perfusion –Detected but neglected?
___________________________________________
27 th International Symposium on Intensive Care and Emergency Medicine
Brussels 2007
Claus-Georg KRENNDept. of Anaesthesia and General Intensive Care, University Vienna
„Splanchnic Region“_______________________________________________
• METNITZ

Liverdysfunction_____________________________________________
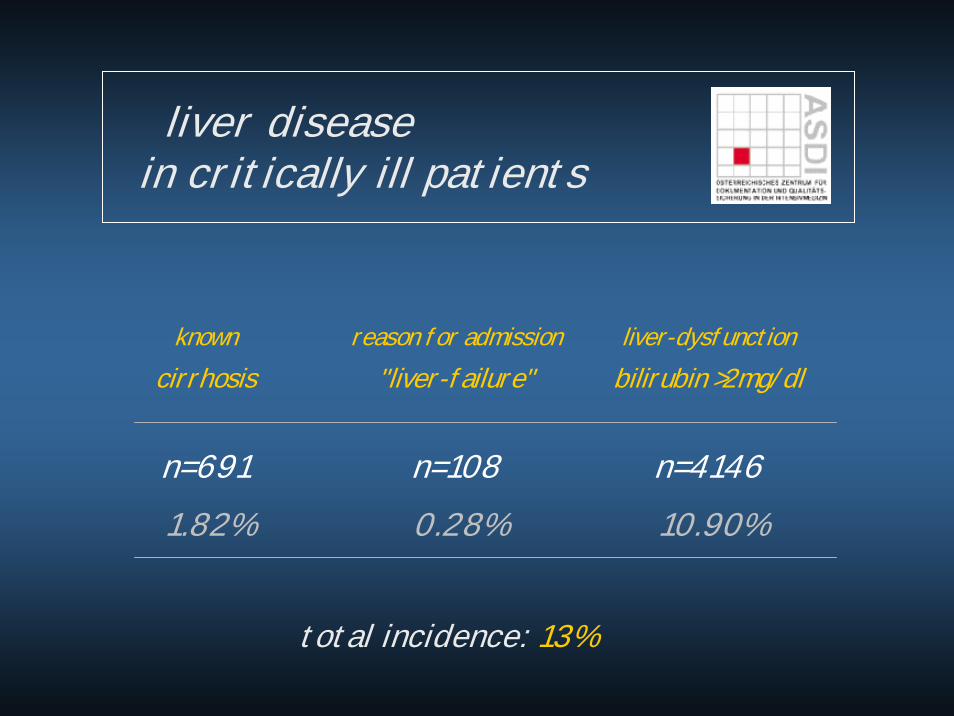
liver diseasein critically ill patients
known cirrhosis
reason for admission "liver-failure"
liver-dysfunction bilirubin >2mg/dl
n=691 n=108 n=4146 1.82% 0.28% 10.90%
total incidence: 13%
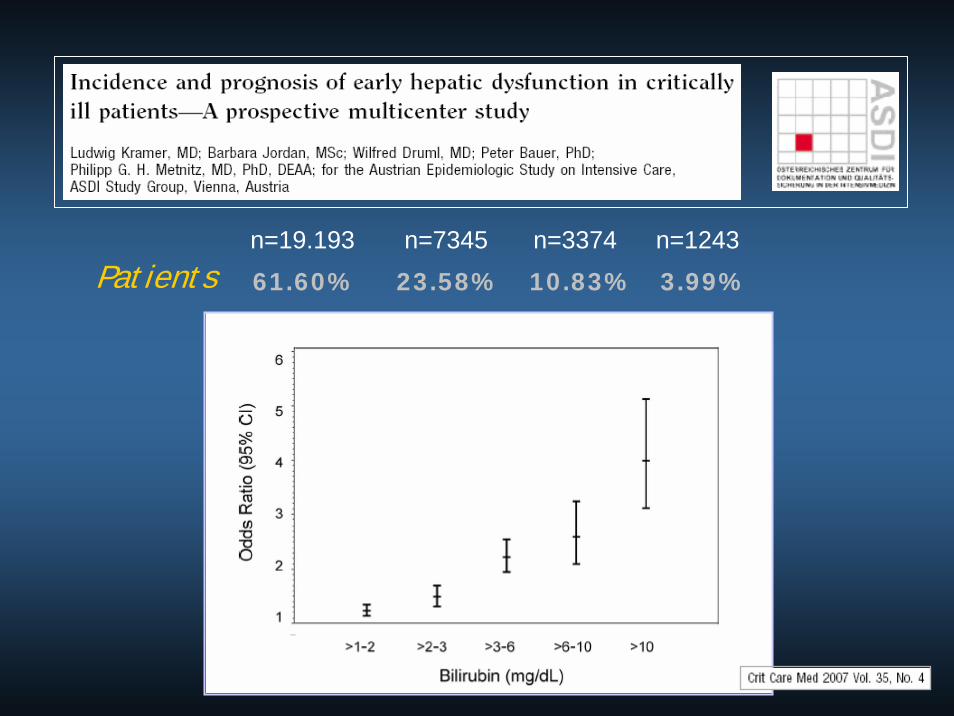
Bilirubin
n=19.193 n=7345 n=3374 n=1243
61.60% 23.58% 10.83% 3.99%
Patients
…virtual round at the ICU___________________________________________________________
Detected but negle
cted?
…virtual round at the ICU_________________________________________________________
HistorySt.p. ACBGSt.p. thoracotomy for bullous cavern
transfer to normal ward
respiratory failure and hypotonia
transfer to Emergency department
Intubation, „hemodynamic stabilization“ and surgery for thoracic empyema
admission to ICU / Reevaluation (hemodynamic stable, homeostasis deranged)
3
2,11,7
1,1 1
0,8
0,177
0,0910,051 0,051
0
1
2
3
4
5
6
7
8
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
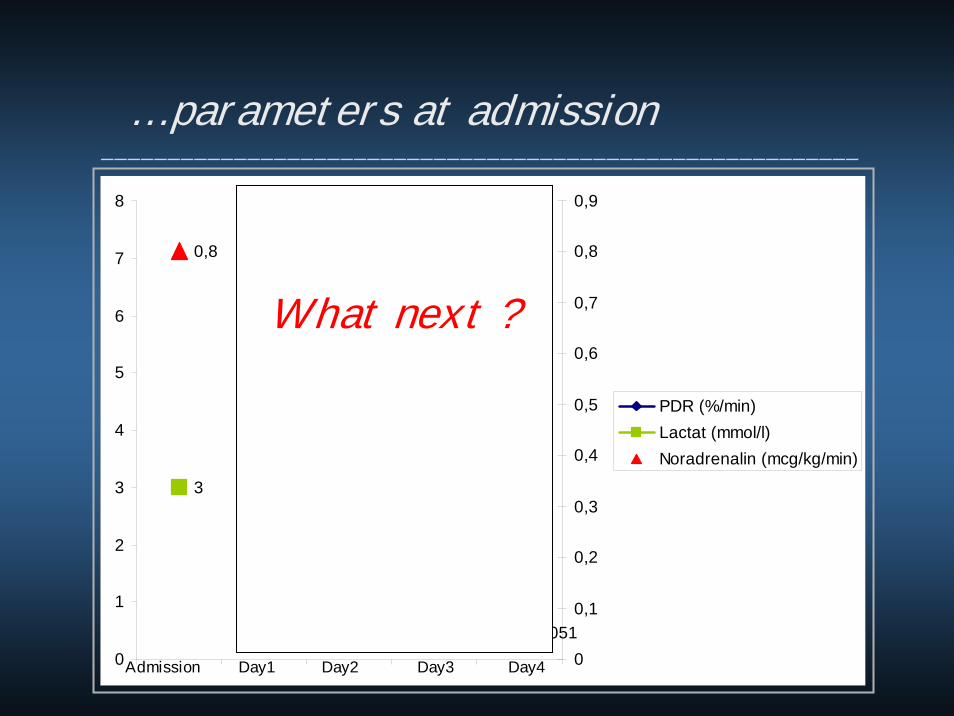
PDR (%/min)Lactat (mmol/l)Noradrenalin (mcg/kg/min)
Admission Day1 Day2 Day3 Day4
… parameters at admission_________________________________________________________
What next ?

3
2,11,7
1,1 1
0,8
0,177
0,0910,051 0,051
0
1
2
3
4
5
6
7
8
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
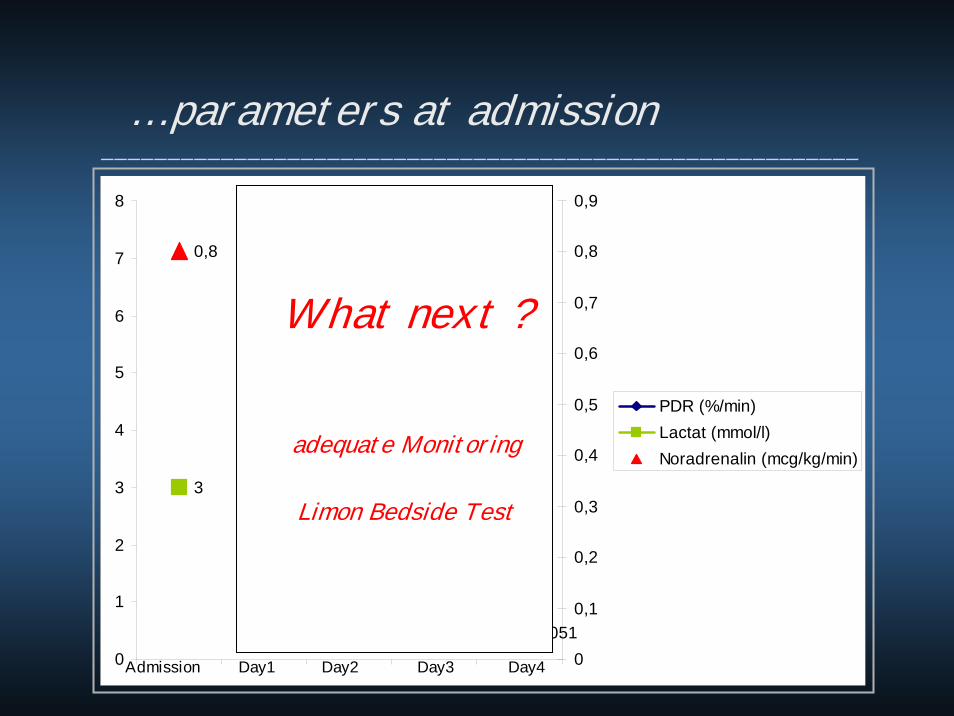
PDR (%/min)Lactat (mmol/l)Noradrenalin (mcg/kg/min)
Admission Day1 Day2 Day3 Day4
… parameters at admission_________________________________________________________
What next ?
adequate Monitoring
3
2,11,7
1,1 1
0,8
0,177
0,0910,051 0,051
0
1
2
3
4
5
6
7
8
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
PDR (%/min)Lactat (mmol/l)Noradrenalin (mcg/kg/min)
Admission Day1 Day2 Day3 Day4
… parameters at admission_________________________________________________________
What next ?
adequate Monitoring
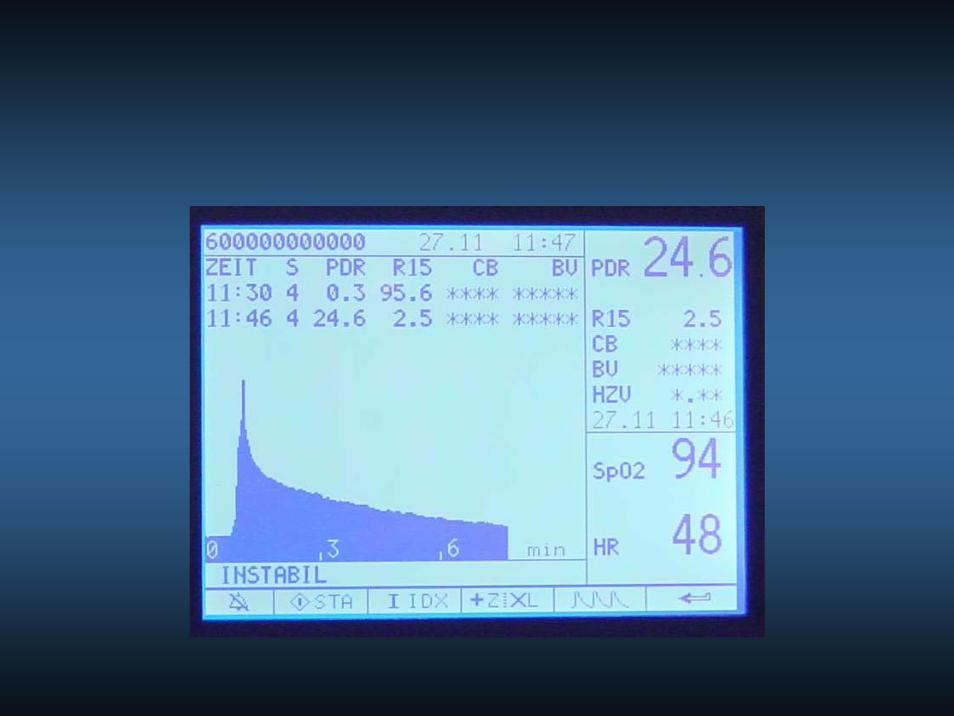
Limon Bedside Test
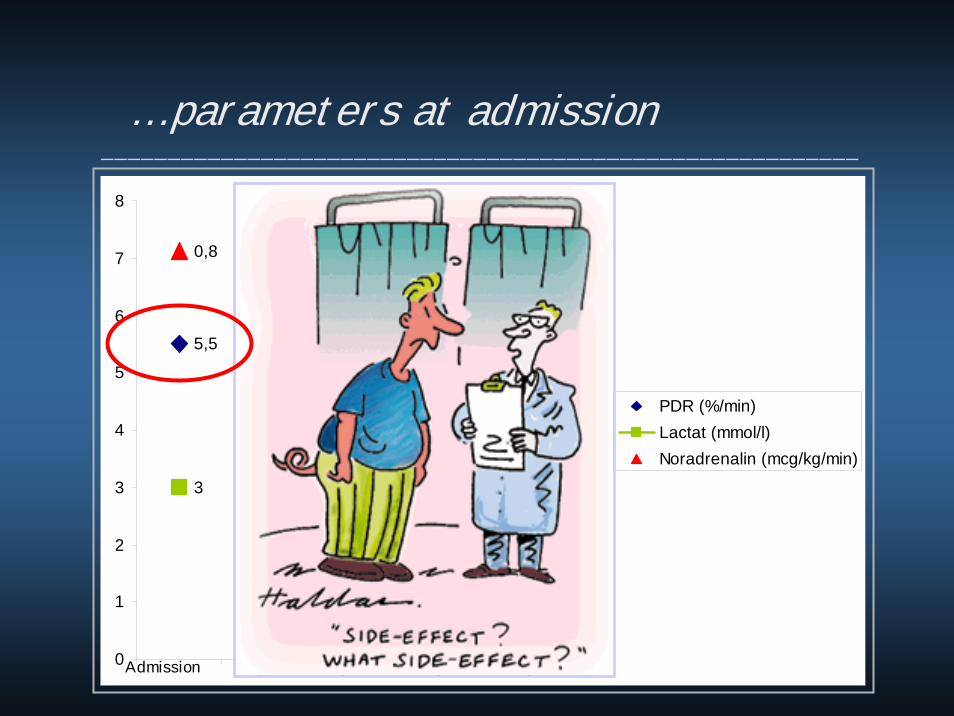
5,55,2
4,2
4,9
7,6
3
2,11,7
1,1 1
0,8
0,177
0,0910,051 0,051
0
1
2
3
4
5
6
7
8
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
PDR (%/min)Lactat (mmol/l)Noradrenalin (mcg/kg/min)
Admission Day1 Day2 Day3 Day4
… parameters at admission_________________________________________________________

5,55,2
4,2
4,9
7,6
3
2,11,7
1,1 1
0,8
0,177
0,0910,051 0,051
0
1
2
3
4
5
6
7
8
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
PDR (%/min)Lactat (mmol/l)Noradrenalin (mcg/kg/min)
Admission Day1 Day2 Day3 Day4
… clinical course_________________________________________________________

2890
2070
958
402
96
23
4946
51
62
0
500
1000
1500
2000
2500
3000
3500
0
10
20
30
40
50
60
70
GOT (U/l)NT (%)
Admission Day1 Day2 Day3 Day4
… clinical course_______________________________________________________

Sometimes …_________________________________________________________

unspecific clinical monitoring_________________________________________________________

Sometimes unspecific clinical monitoring is not enough !______________________________________________________________________________________
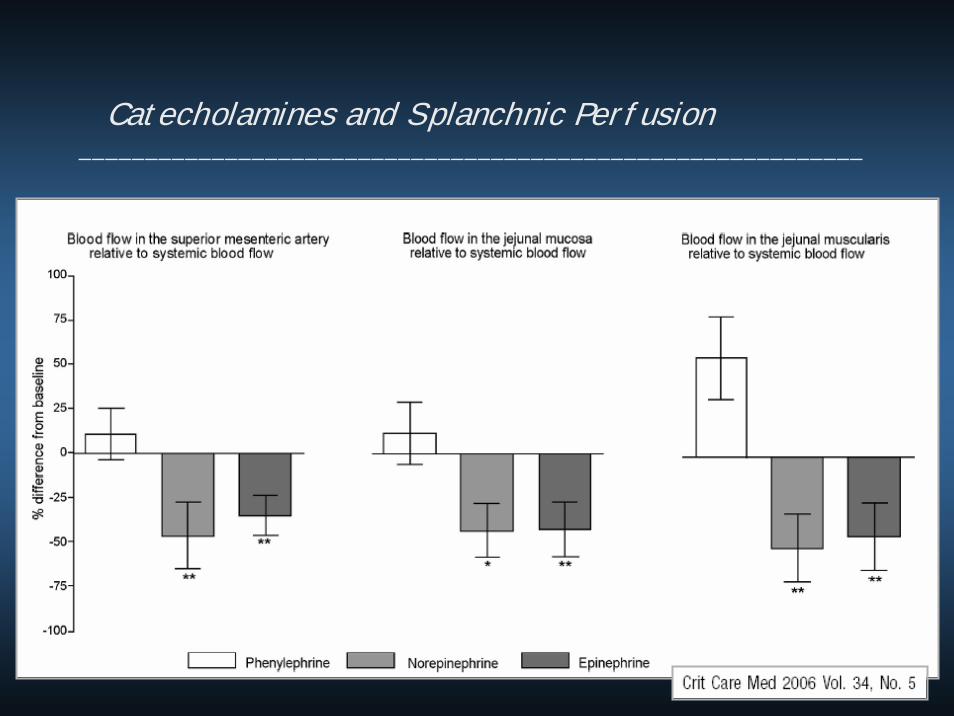
Catecholamines and Splanchnic Perfusion___________________________________________________________

Catecholamines and Splanchnic Perfusion___________________________________________________________
Macrohemodynamics≠
regional blood flow
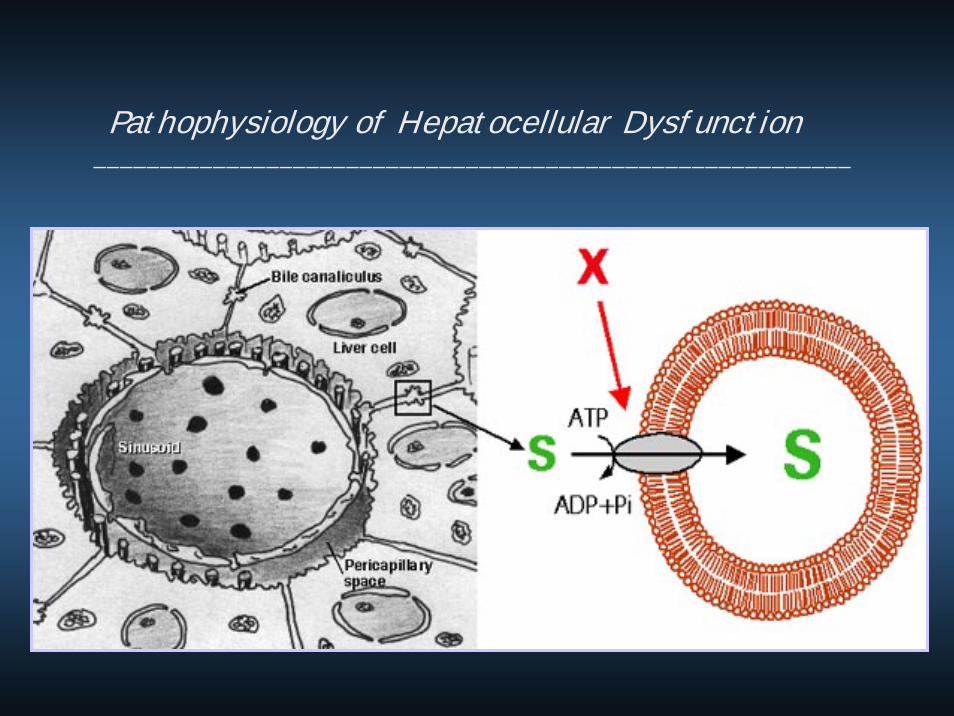
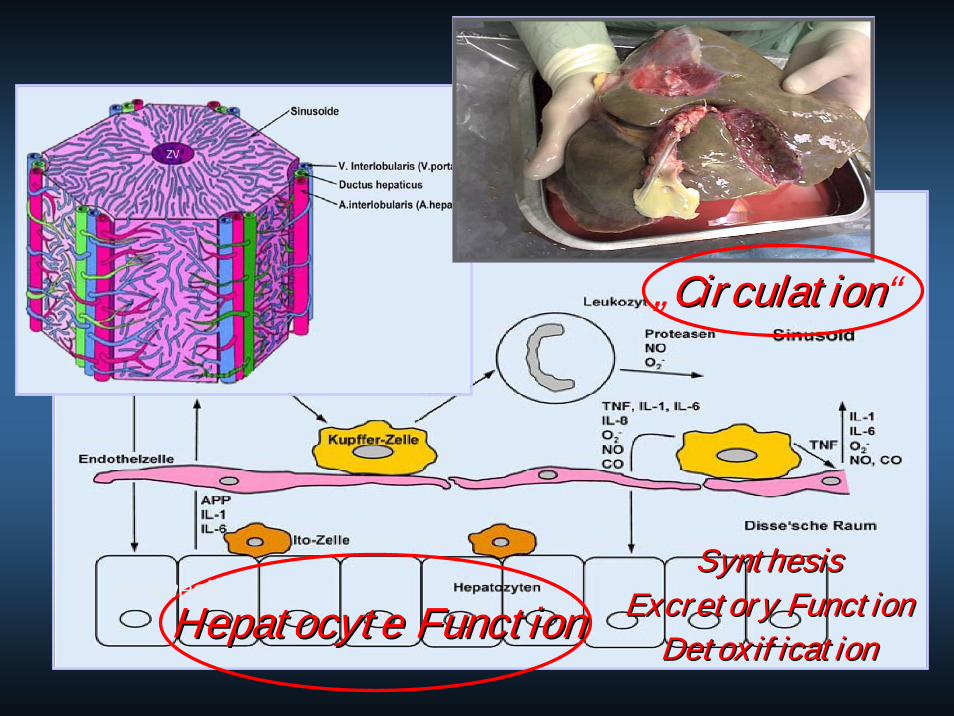
Pathophysiology of Hepatocellular Dysfunction_________________________________________________________
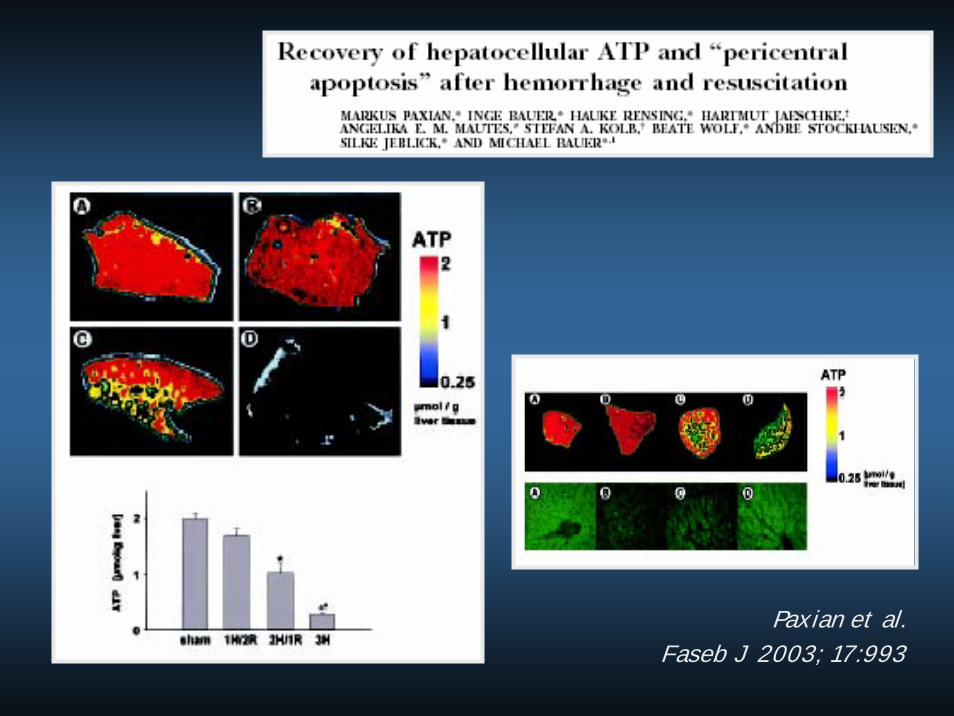
Paxian et al. Faseb J 2003; 17:993

Recovery of hepatocellular ATP and “pericentral apoptosis” afterhemorrhage and resuscitation. Paxian et al., FASEB 2003
Hepatocellular apoptosis can be detected accurately by ICG kineticsand is reversible by early resuscitation
Therapy of I/R induced liver dysfunction____________________________________________________________________________________
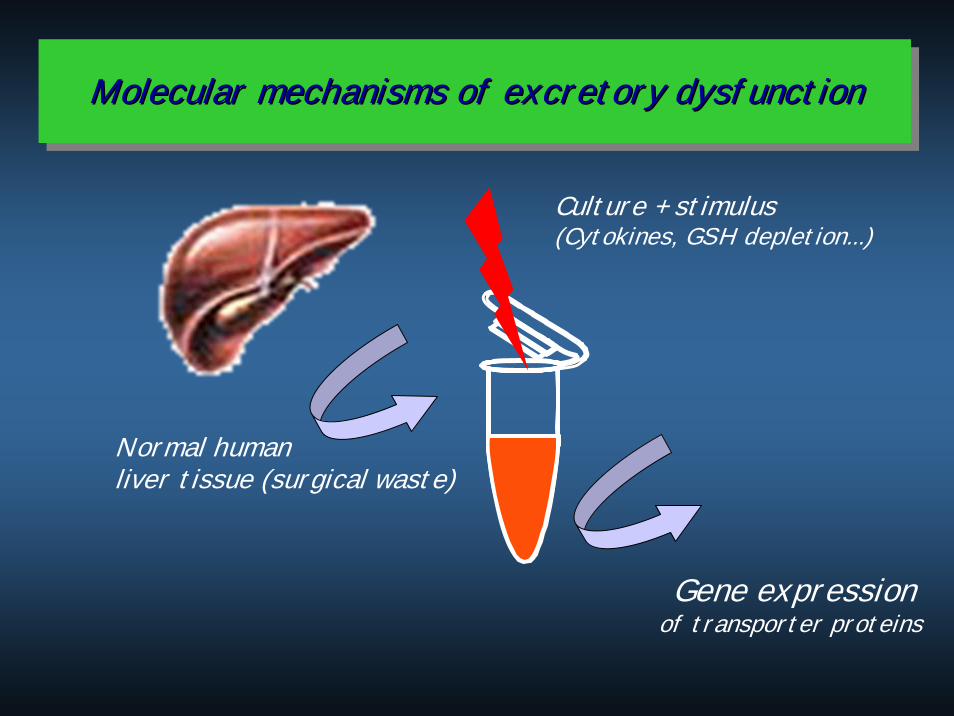
Molecular mechanisms of excretory dysfunctionMolecularMolecular mechanismsmechanisms of of excretoryexcretory dysfunctiondysfunction
Normal human liver tissue (surgical waste)
Culture + stimulus(Cytokines, GSH depletion...)
Gene expressionof transporter proteins
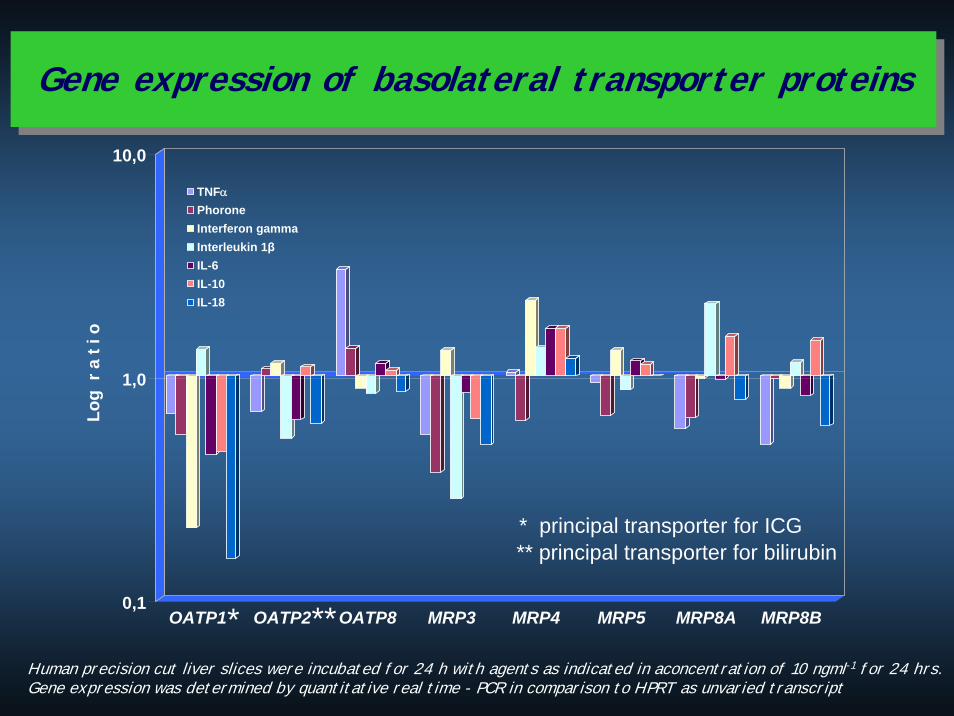
Human precision cut liver slices were incubated for 24 h with agents as indicated in aconcentration of 10 ngml-1 for 24 hrs. Gene expression was determined by quantitative real time - PCR in comparison to HPRT as unvaried transcript
* **
** principal transporter for bilirubin* principal transporter for ICG
0,1
1,0
10,0
Log
r a
t i o
OATP1 OATP2 OATP8 MRP3 MRP4 MRP5 MRP8A MRP8B
TNFαPhoroneInterferon gammaInterleukin 1βIL-6IL-10IL-18
Gene expression of basolateral transporter proteinsGene expression of basolateral transporter proteins
clinical surrogates of
regional blood flow
and metabolism
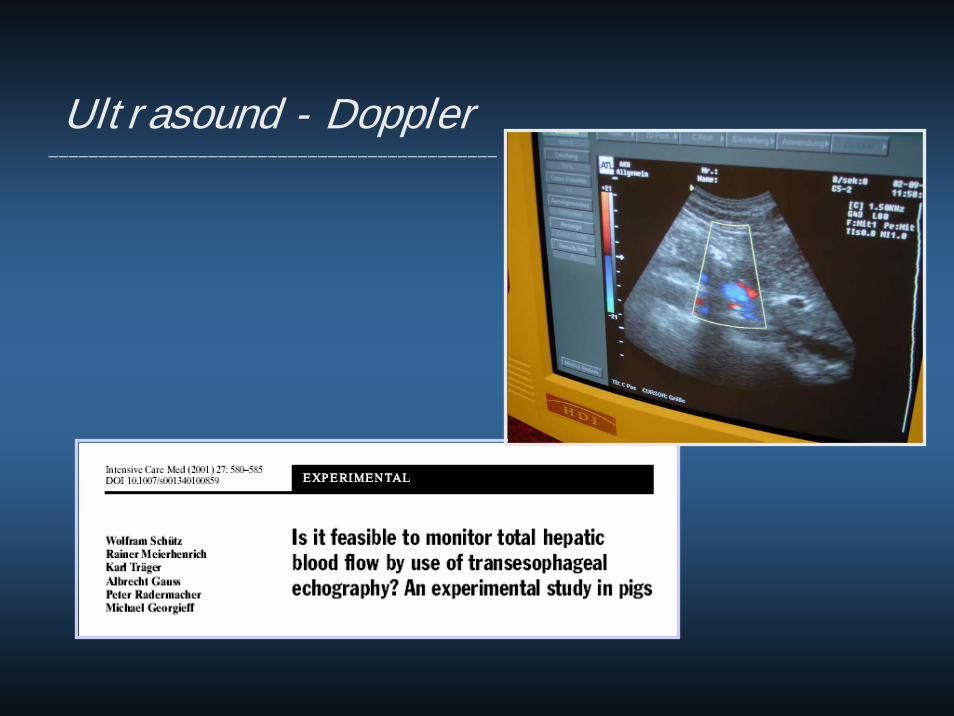
Ultrasound - Doppler_____________________________________________

Dynamic Liverfunction-Testing_______________________________________________________________
J Gastrointest Surg. 2001; 5(3):316-21
Dynamic Liverfunction-Testing_______________________________________________________________
Dynamic Liverfunction-Testing_______________________________________________________________
Dynamic Liverfunction-Testing_______________________________________________________________
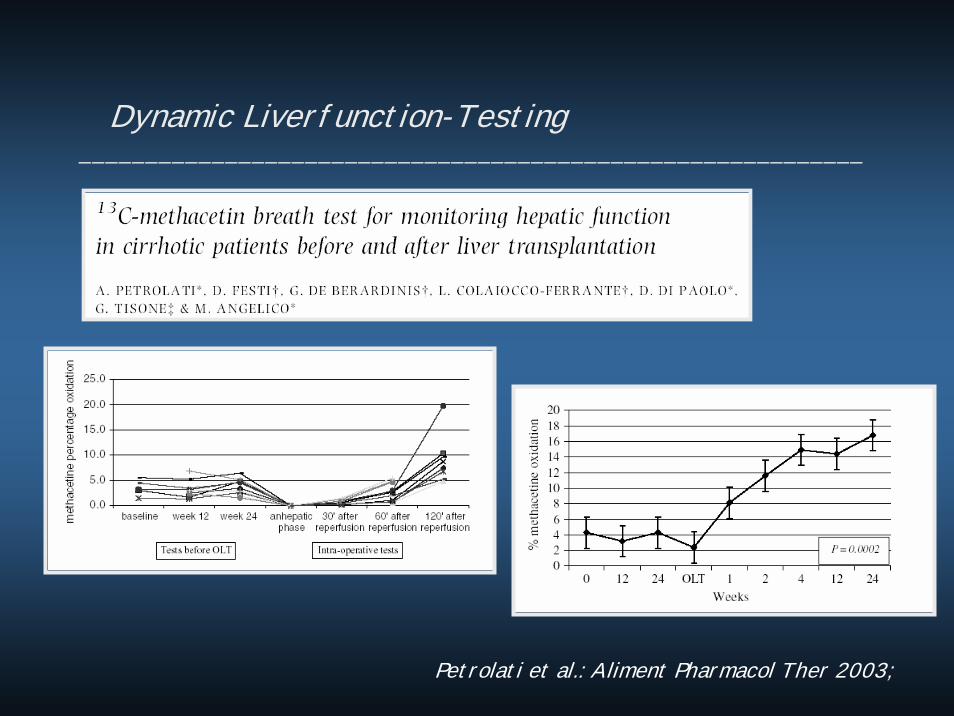
Dynamic Liverfunction-Testing___________________________________________________________
Petrolati et al.: Aliment Pharmacol Ther 2003;
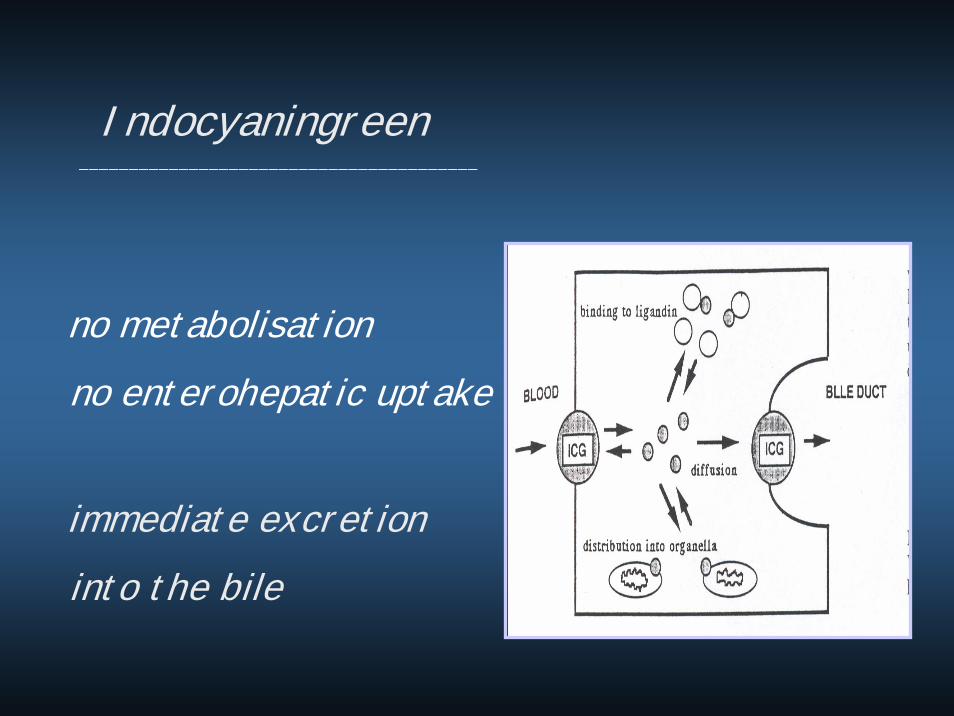
Indocyaningreen________________________________________
no metabolisationno enterohepatic uptake
immediate excretioninto the bile

Measurement________________________________________
Calculation of the halftimeof the elimination rate of ICG
Sequence of re-extrapolation rate
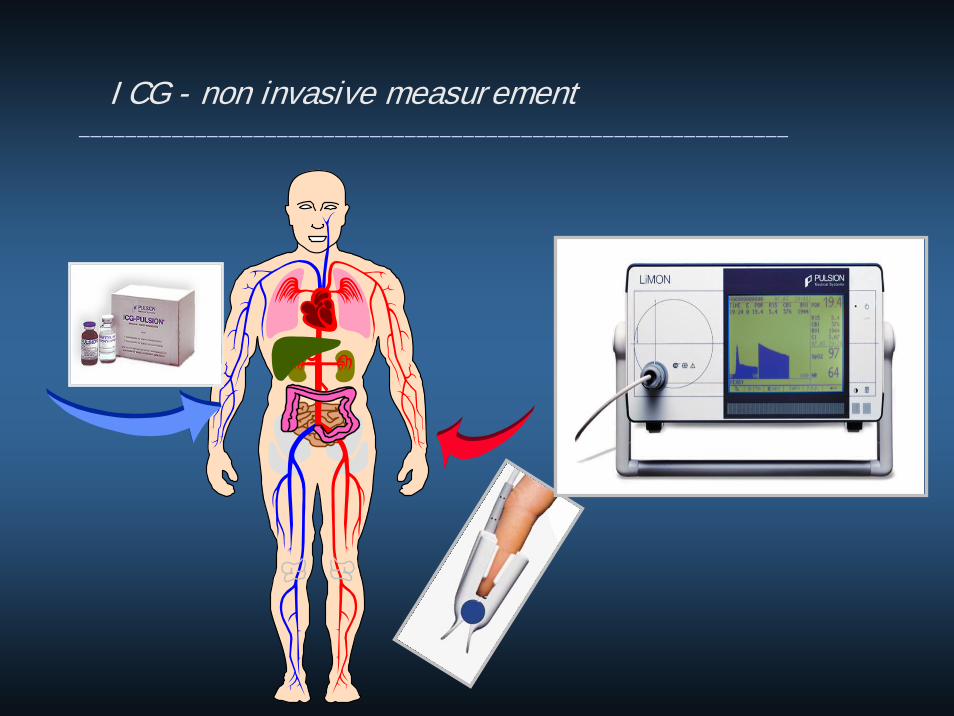
ICG - non invasive measurement_____________________________________________________________
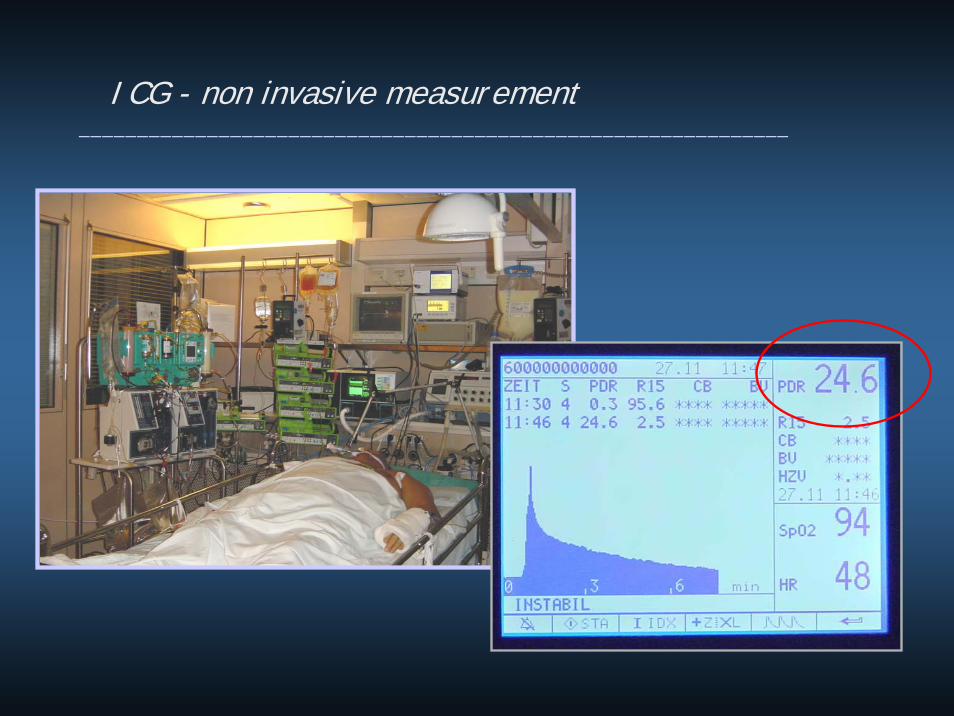
ICG - non invasive measurement_____________________________________________________________
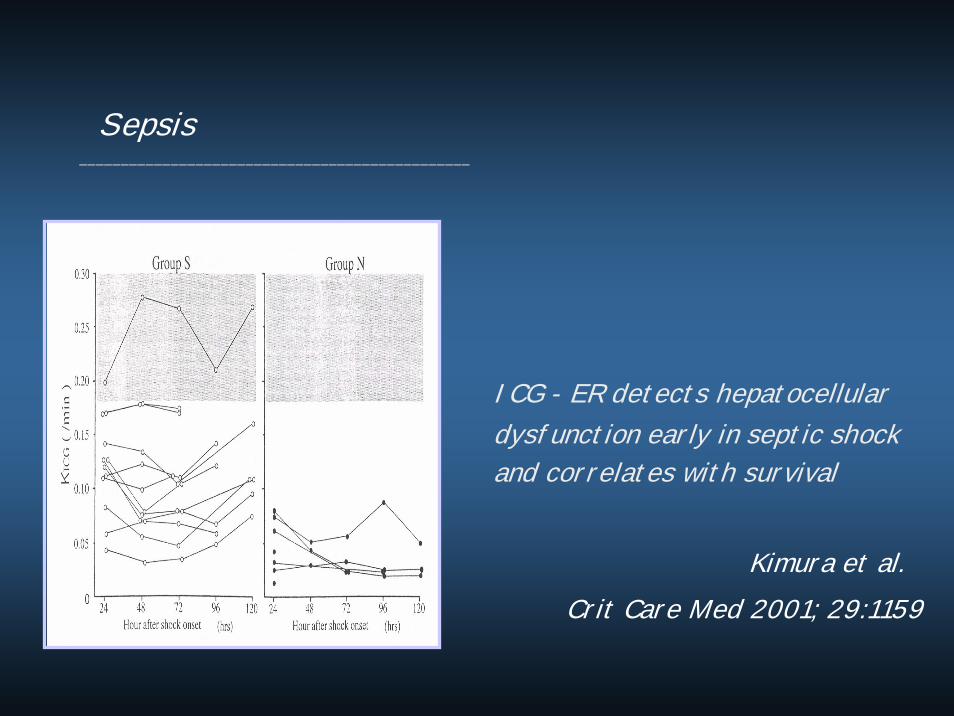
Sepsis_______________________________________________
ICG - ER detects hepatocellulardysfunction early in septic shockand correlates with survival
Kimura et al.Crit Care Med 2001; 29:1159

Prognosis_______________________________________
screen and adapt actual medication !!__________________________________________________
„It may seem a strange principle to enunciateas the very first requirement in a hospital thatit should do the sick no harm.“
Florence NightingaleNotes on hospitals / London 1859
treat „early and goal directed“_______________________________________________________________________


Therapeutic options__________________________________
APOPTOSIS NECROSIS
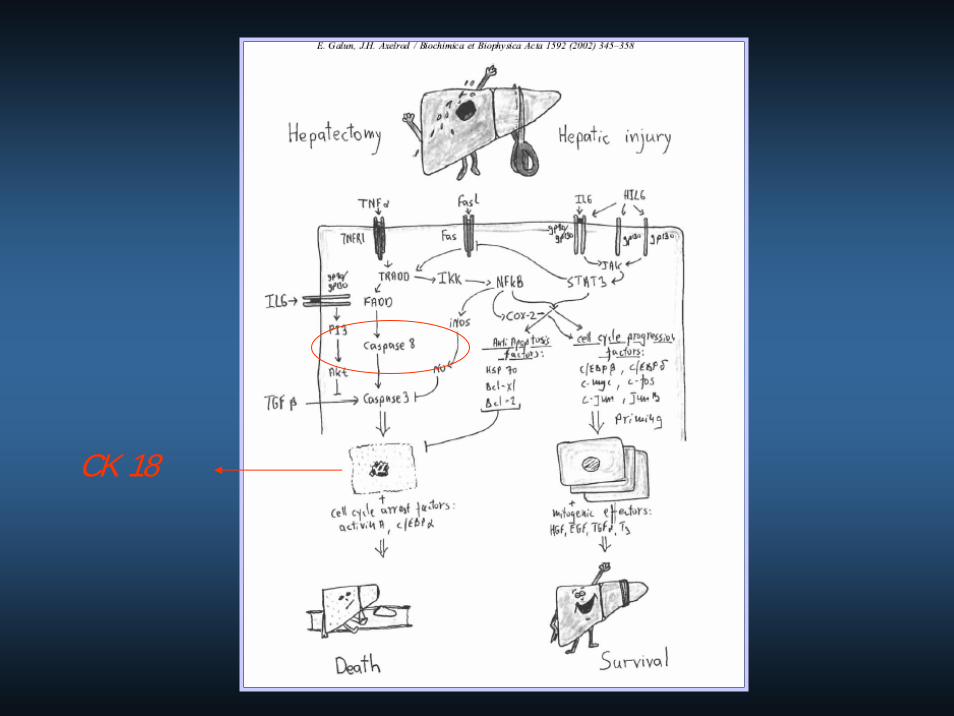
CK 18
the End_______________________________________________
... thank you for your attention


Extracorporeal Detoxification - MARS___________________________________________________________________________________

Apoptosis parameter_______________________________________
-500
0
500
1000
1500
2000
2500
3000
3500
4000
Einh
eite
n
vor
ESLD
control
AOCLF
ALF
Box-DiagrammGetrennt nach: GeneseZeilen-Ausschluß: ck18 alf.xls (importiert).svd
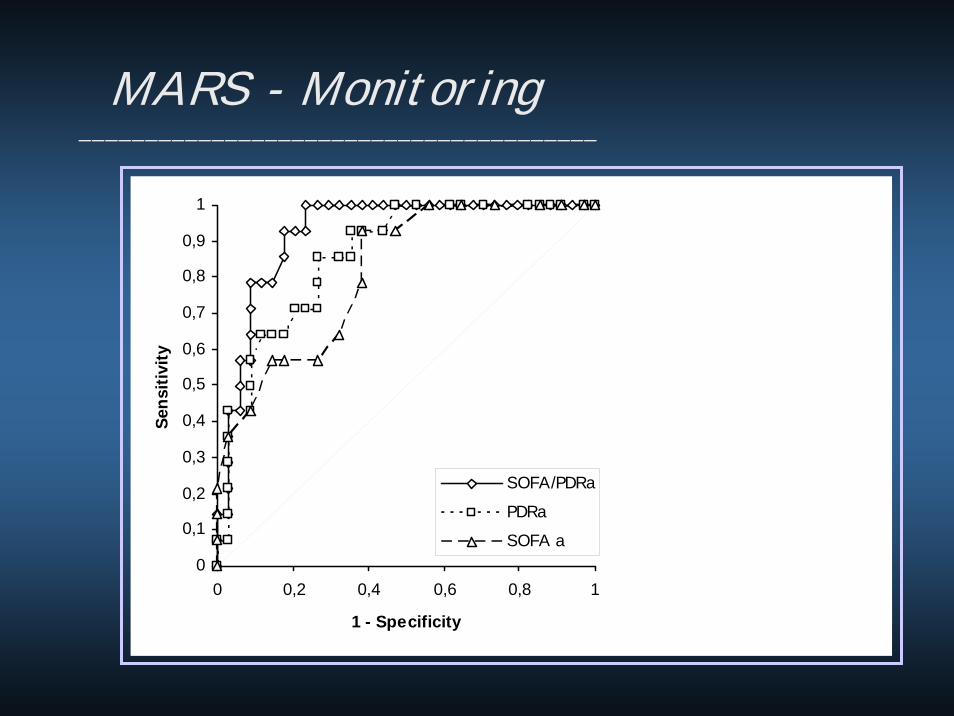
MARS - Monitoring_______________________________________
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 0,2 0,4 0,6 0,8 1
1 - Specificity
Sens
itivi
ty
SOFA/PDRa
PDRa
SOFA a
rely on your clinical judgement____________________________________________________________________
get information about the functional (reserve) capacityand prognosis rather than about the „damage“ !!!the trend of functional monitoring tells you most !!!
ALF MARS_______________________________________________
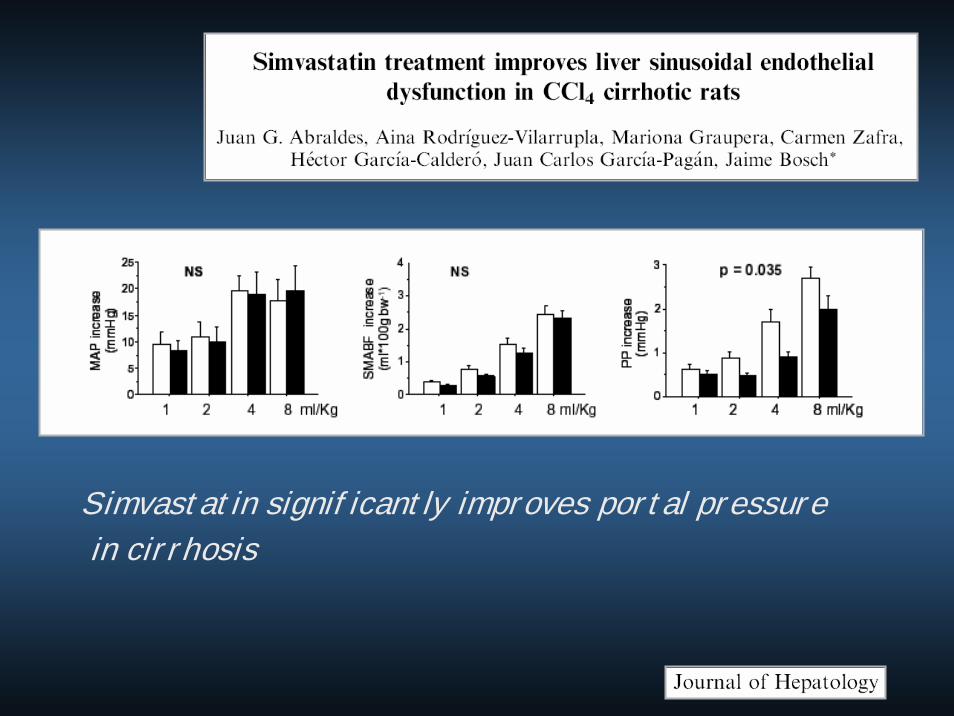
Simvastatin significantly improves portal pressurein cirrhosis

Monitoring______________________________________________
Blood flowFunctionReserve capacity
Prognosis
„…dynamic functional testing“
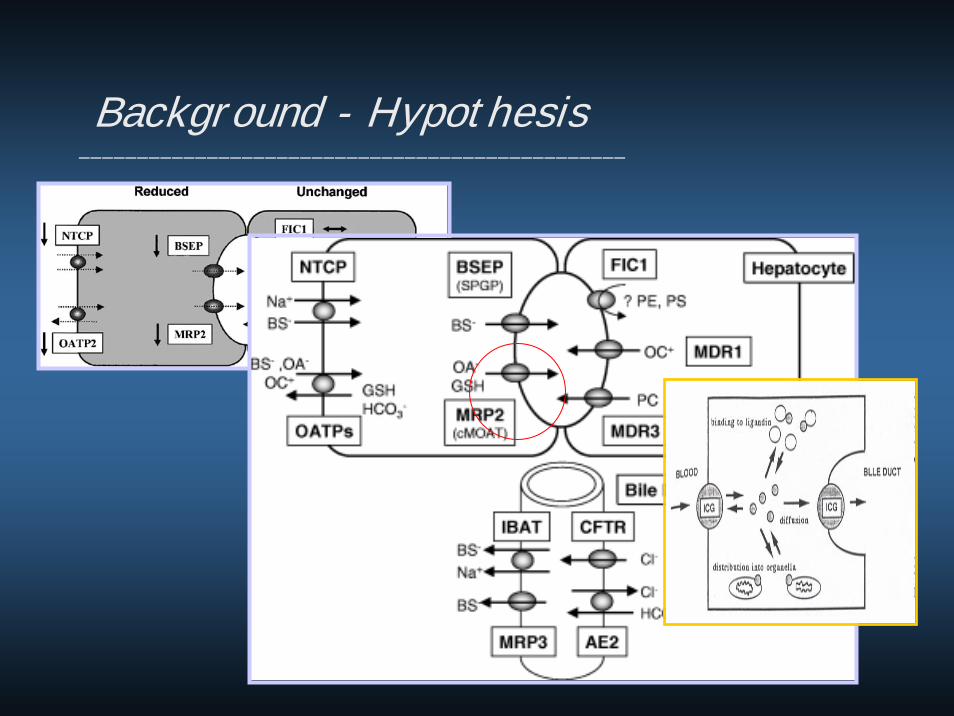
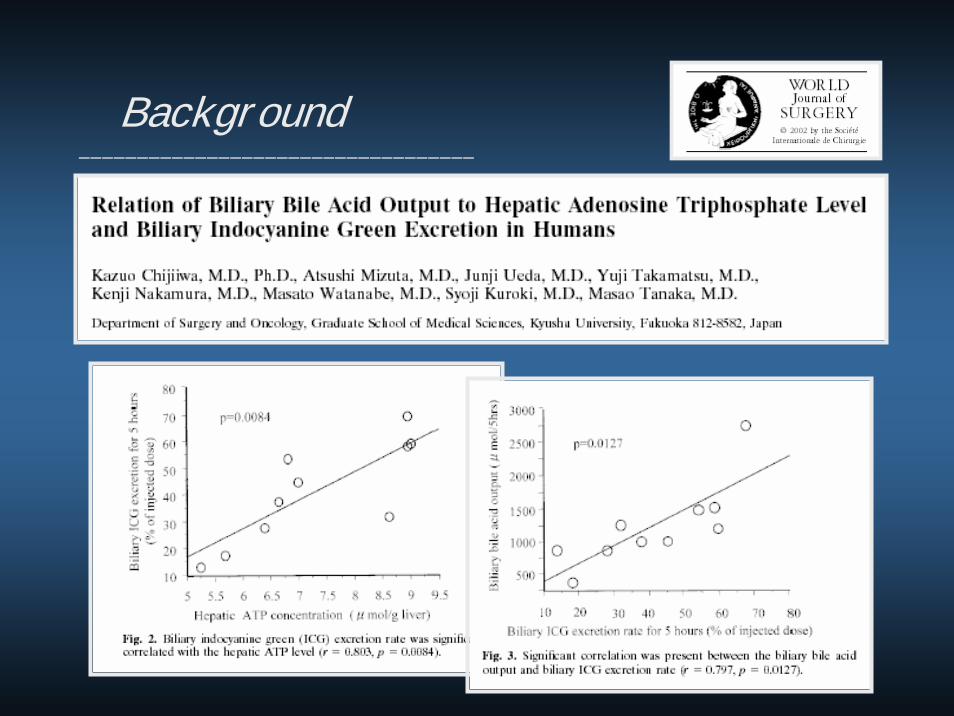
Background - Hypothesis_______________________________________________
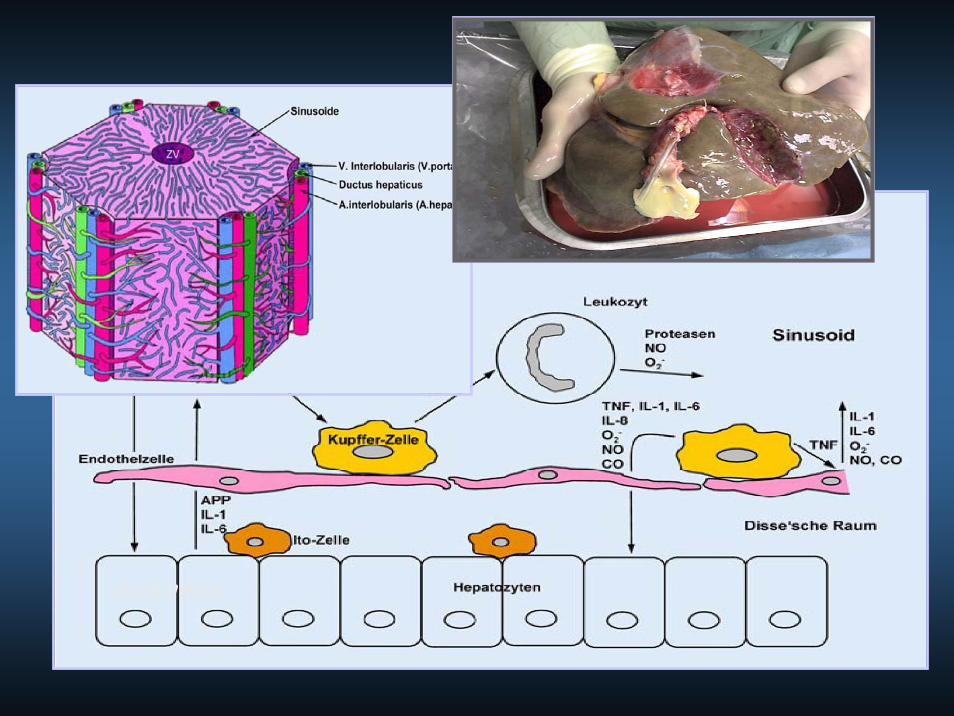
Synthesis,
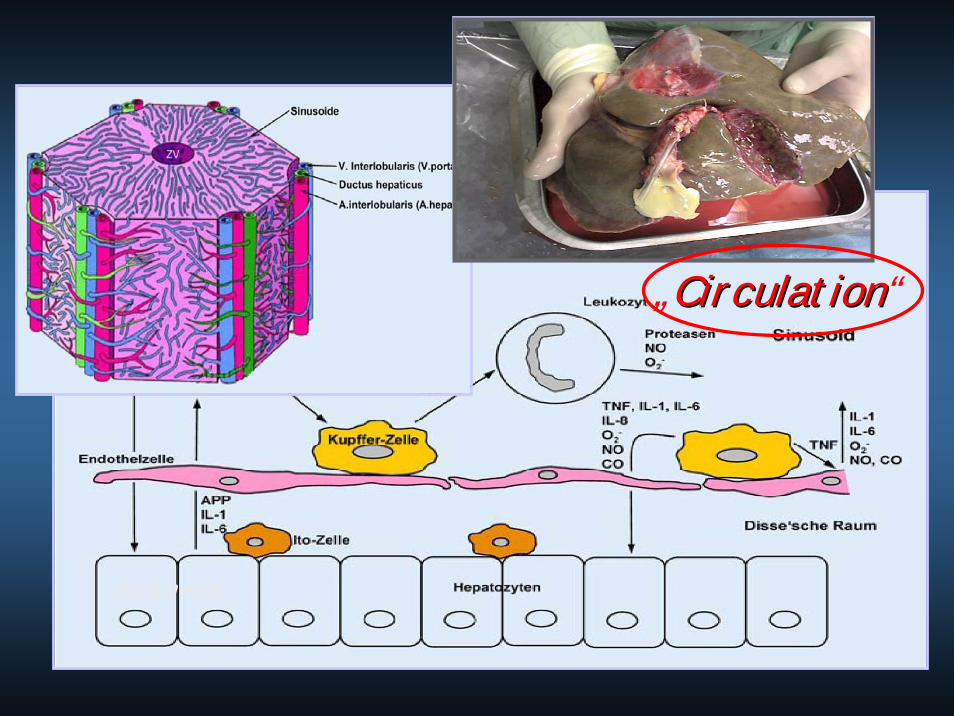
„CirculationCirculation“
Synthesis,
„CirculationCirculation“
Synthesis, HepatocyteHepatocyte FunctionFunction
SynthesisSynthesisExcretoryExcretory FunctionFunction
DetoxificationDetoxification
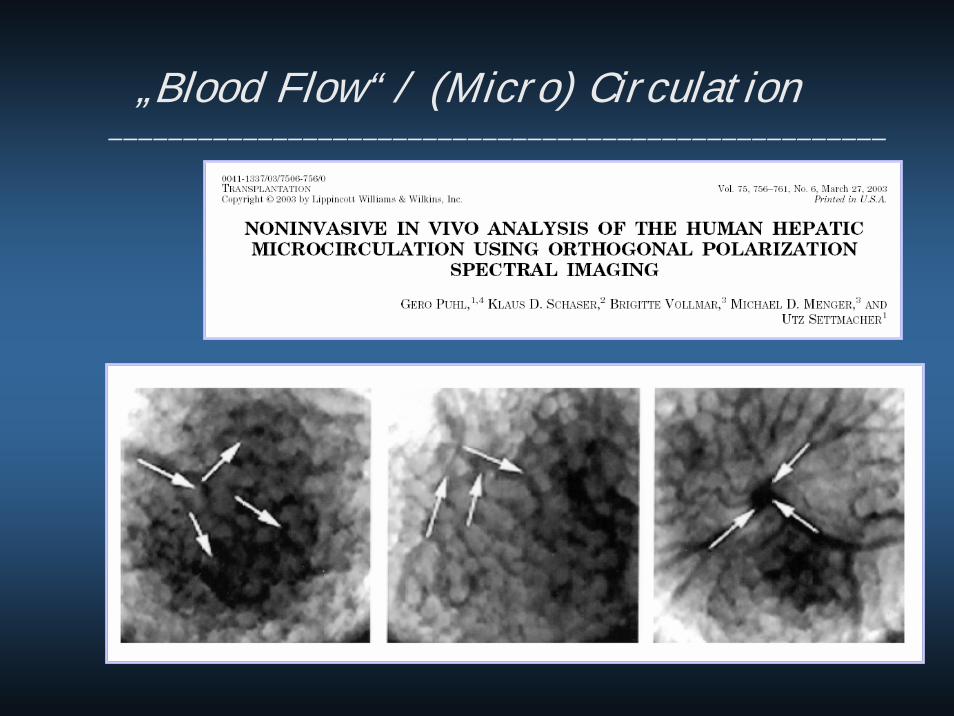
„Blood Flow“ / (Micro) Circulation____________________________________________________
Visualisation - Fluorescence____________________________________________________________

Detoxification________________________________________
graded encephalopathy - I.-IV.branched chained aminoacidsAmmonium
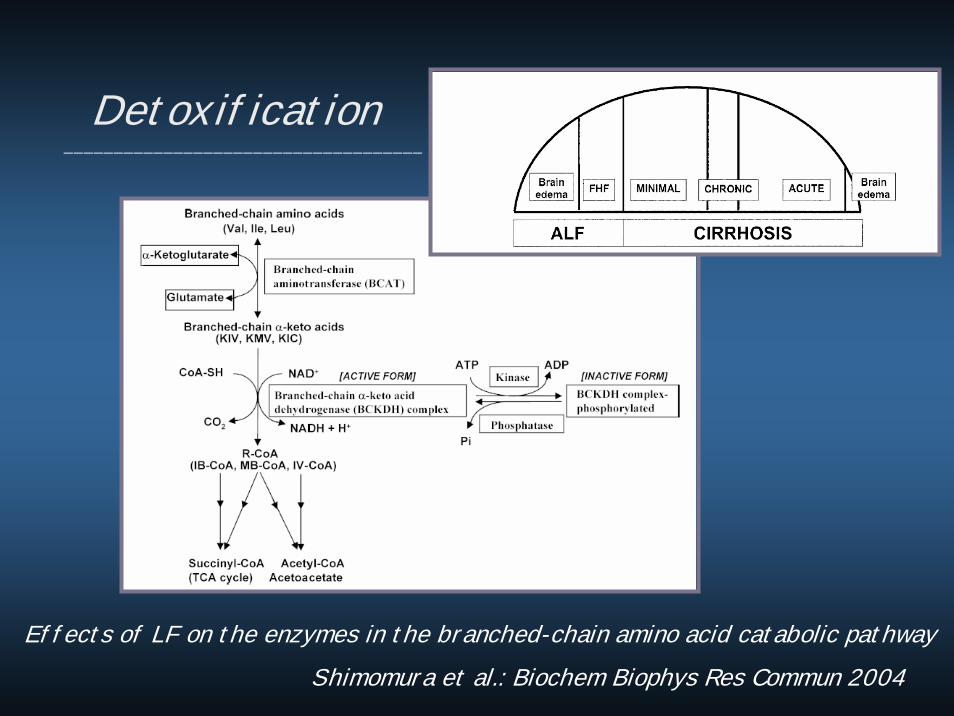
Effects of LF on the enzymes in the branched-chain amino acid catabolic pathwayShimomura et al.: Biochem Biophys Res Commun 2004
Detoxification____________________________________
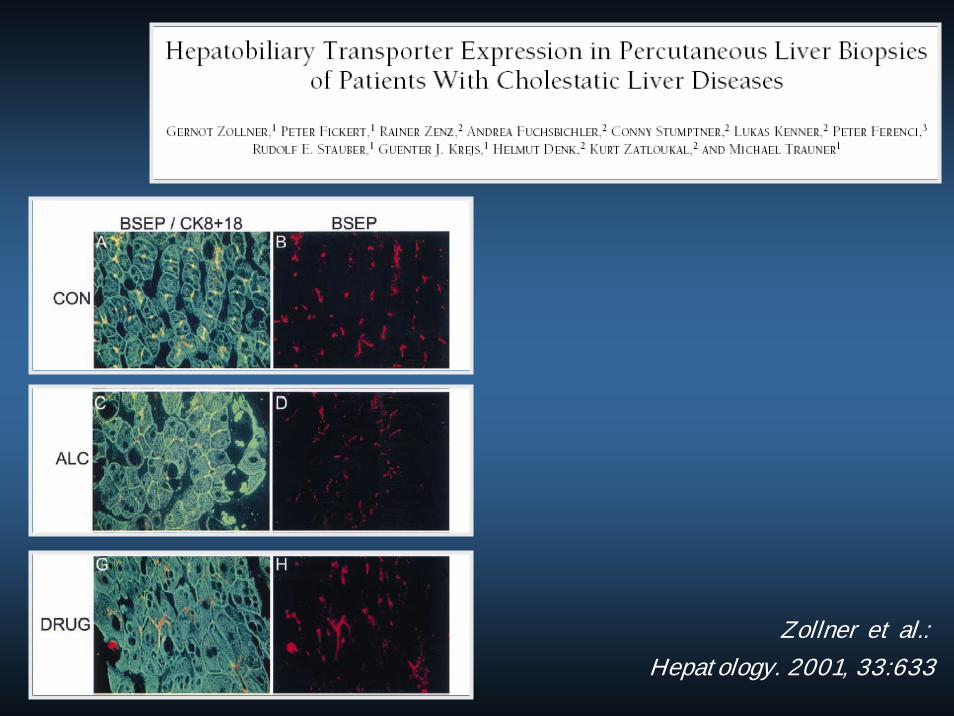
Zollner et al.:Hepatology. 2001, 33:633
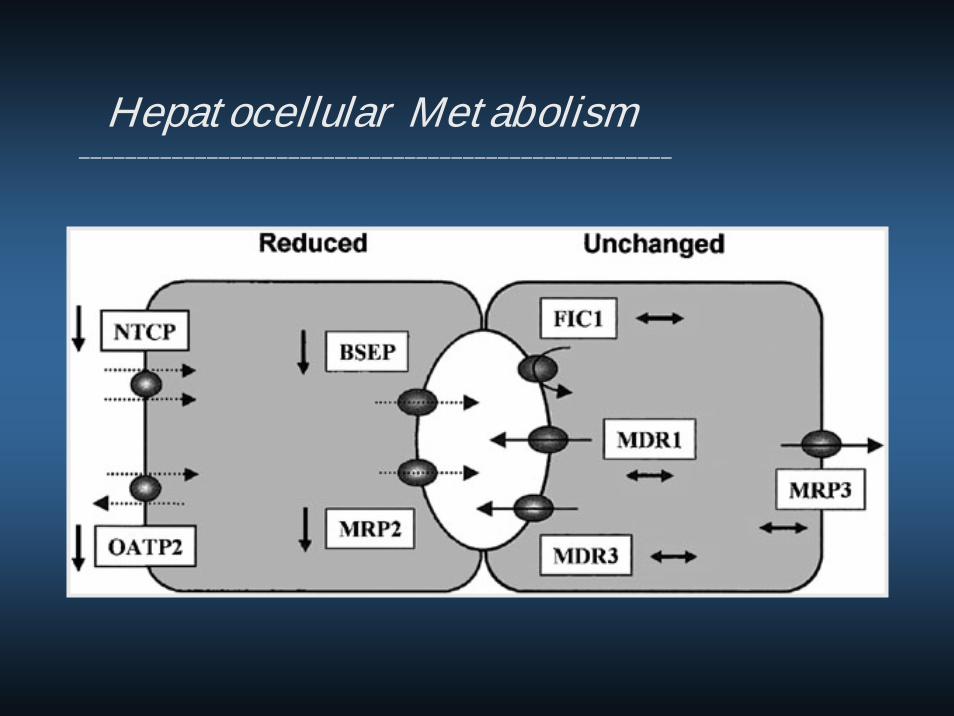
Hepatocellular Metabolism___________________________________________________

Metabolism_______________________________________
Background__________________________________

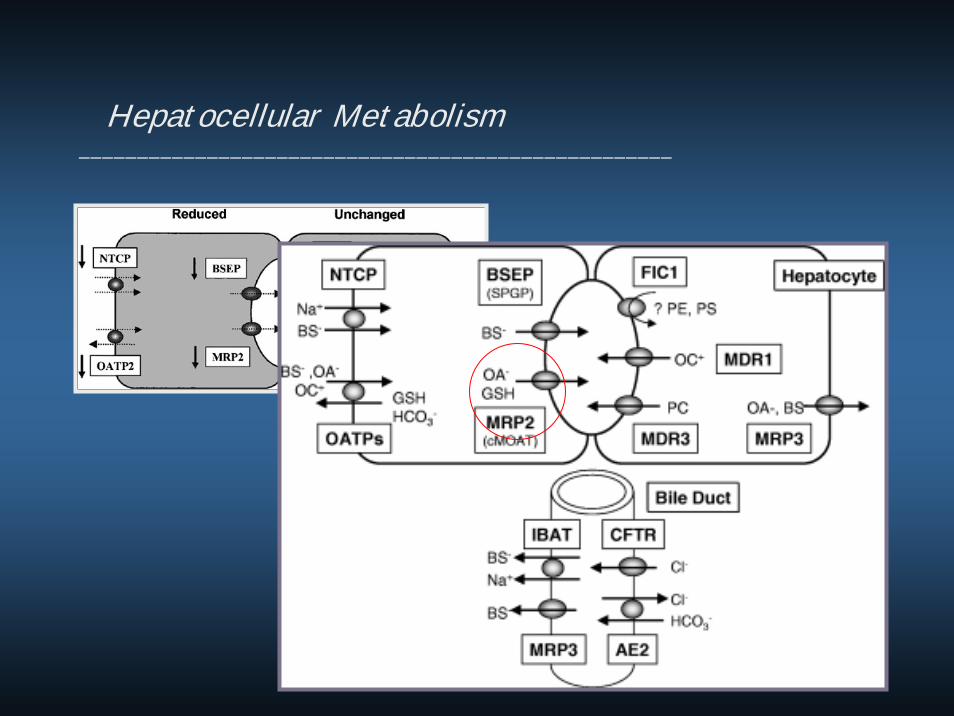
Hepatocellular Metabolism___________________________________________________





























