Embed Size (px)
Citation preview
HEALTH AND HEALTHCARE IN INDIA- RESPONDING TO THE
CHANGING SCENARIO
RAVI DUGGAL
Background Paper prepared for the Observer Research Foundation and
Center for Development Alternatives
January 28, 2004
PDF created with pdfFactory Pro trial version www.pdffactory.com

Health and Healthcare in India Responding to the Changing Scenario
Ravi Duggal Introduction We are into year 2004 but where is “Health For All” as vowed by WHO member nations at Alma Ata in 1978? Year 2000 was selected to be that magical year by when all people of this world were projected to have not only universal access to primary health care but more importantly “health for all”.1 Since then the situation has barely changed. The countries that could not provide basic health care to its people then, continue to be unable to do so even today. It is not as if there is a lack of resources – more drugs are produced, the private health sector has grown geometrically, people are spending much more out of pocket, newer technologies are available etc – but those not having access to primary health care have increased in numbers. In 1946 we had a very well worked out plan and strategy for health for all, the Health Survey and Development Committee Report (popularly called the Bhore Committee Report). It was a comprehensive plan that guaranteed universal access to health care 15 years down the line. But the first Health Ministers Conference in 1947 scuttled it saying that it was unaffordable. The Bhore plan demanded only about 1.33% of GNP, including capital expenditures (or Rs.2.98 per capita at 1945 prices).2 This wasn’t a very difficult thing to achieve considering that it would be a very fruitful investment in people who would then be able to contribute fully to the new emerging and growing economy. We opted instead for a selective program-based approach, perhaps an influence of the American community development model, which had become the cornerstone of our development policy in the early years of planning. Many of these were vertical programs that had their own bureaucracy and which over time developed into “empires”. No doubt this approach had some well known successes like the eradication of small pox by 1976, good control over malaria by mid-sixties (but this was messed up due to complacency, and malaria since then continues to be a menace), reasonable control over leprosy by mid-eighties and more recently the pulse polio program. However, basic health care and access to it, especially in the rural areas, is still unavailable to a large majority. This is so despite a large expansion of rural health infrastructure in the seventies and eighties under the Minimum Needs Program. While this infrastructure is in place in many states it does not meet the health care needs of the people. People need basic curative and preventive care but the existing system is obsessed with providing family
1 The Alma Ata Declaration defined primary health care as “…essential health care based on practical, scientifically sound and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost that the community and the country can afford to maintain at every stage of their development in the spirit of self reliance and self determination.” (WHO, 1978: Alma-Ata 1978 – Primary Health Care, Geneva) 2 GOI, 1946: Health Survey and Development Committee Report, Delhi, Vol. II pg. 510
PDF created with pdfFactory Pro trial version www.pdffactory.com

planning and related services. From the 3rd Five Year Plan onwards family planning has remained the main concern of the Ministry of Health and Family Welfare.3 Since then nomenclatures may have changed from maternal and child health to child survival and safe-motherhood and presently reproductive and child health under international patronage, but the underlying emphasis of the health program is family planning or population control. As a consequence even the poor have to seek primary care from the private health providers, often from those not qualified in any system of medicine and/or from non-allopaths who practice allopathy. Despite this we do see improvement in measurable indicators like longevity, infant mortality, crude death rates etc. over the years. But these figures reflect more the improvement in the quality of life of the top 20% and/or the concerted efforts in health care in states like Kerala and Tamil Nadu. Overall the miseries of the bottom 50-60% continue and this is adequately reflected in disaggregated figures of these same indicators in the BIMARU states (now called Empowered Action Group (EAG) states). Poverty and Health Poverty is the real context of India. Three-fourths of people live below or at subsistence levels. This means 70-90% of their incomes goes to food and related consumption. In such a context social security support for health, education, housing etc. becomes critical. Ironically, India has one of the largest private health sectors in the world with over 80% of ambulatory care being supported through out-of-pocket expenses. The public health services are very inadequate. The public curative and hospital services are mostly in the cities where only 25% of the one billion population resides. Rural areas have mostly preventive and promotive services like family planning and immunisation. The private sector has virtual monopoly of ambulatory curative services in both rural and urban areas and over half of hospital care. Further, a very large proportion of private providers are not qualified to provide modern health care because they are either trained in other systems of medicine (traditional Indian systems like ayurveda, unani and siddha, and homoeopathy) or worse do not have any training, and these are the providers who the poor are most likely to seek health care from. This adds to the risk faced by the already impoverished population. The health care market in India, like in the USA, is based on a supply-induced demand and keeps growing geometrically, especially in the context of new technologies. The cost of seeking such care is also increasing. This means that the already difficult scenario of access to health care is getting worse, and not only the poor but also the middle
3 Infact, in 1966 a UN Advisory Mission strongly advised “The directorate (Health) should be relieved from other responsibilities such as maternal and child health and nutrition. It is undoubtedly important for family planning to be integrated with MCH in the field , particularly in view of the ‘loop’ program , but until the family planning campaign has picked up momentum and made real progress in the states, the Director General concerned should be responsible for family planning only. This recommendation is reinforced by the fear that the program may be otherwise used in some states to expand the much needed and neglected MCH services.” (UN Advisory Mission, 1966: Report of the Family Planning Program in India, United Nations , New York)
PDF created with pdfFactory Pro trial version www.pdffactory.com

classes get severely affected.4 Thus India has a large, unregulated, poor quality, expensive and dominant private health sector, and an inadequately resourced, selectively focused and declining public health sector despite its poverty, with the former having curative monopoly and the latter carrying the burden of preventive services. Given the above context the lack of right to healthcare is the main reason why health status of the Indian population is unsatisfactory. Health indicators across the board are close to the worst and within the country inequities across classes are very severe. For example, the disparity between the top 18% (socio-economically high) households and the bottom 36% (socio-economically low) households, favouring the former, in infant and child mortality rates is of the magnitude of 2 ½ times5, prevalence of malaria 3 times, prevalence of tuberculosis 4 times, access to antenatal care nearly 4 times, completed immunisation 2 times, childbirth by doctor 4 times, malnourishment amongst women in reproductive age-group 3 times.6 . This is clearly due to inadequate access to healthcare services, because even in conditions of poverty if access to primary healthcare is universal then it can become a leveler of healthcare outcomes. In the case of nutritional outcomes the disparities are even wider as this is more closely a function of income poverty. Unlike healthcare social intervention for nutrition is only done during a severe crisis. The unfortunate reality is that even during crises this does not happen today, and shamefully we experience starvation deaths in many places in India despite having overflowing godowns of reserved food-stocks under state control. With such inequities prevailing it is evident that the healthcare and food distribution systems are biased in favour of those with purchasing power and hence such a system is grossly discriminatory. Health Policy and Plans A historical review of policy and plans is relevant here to understand the trajectory of the development of the healthcare system in India, especially the shaping of public healthcare. It was not until 1983 that India adopted a formal or official National Health Policy. Prior to that health activities of the State were formulated through the Five year Plans and recommendations of various Committees. For the Five Year Plans the health sector constituted schemes that had targets to be fulfilled. Each plan period had a number of schemes and every subsequent plan added more and dropped a few.
4 The 52nd Round NSS data reveals that for inpatient care 46% of poorer classes and 34% of the richer classes either sold assets or took loans to pay for treatment. And those using private hospitals were 16% more likely to get into indebtedness than those using public hospitals. (NSS-1996 : Report No. 441, 52nd Round, NSSO, New Delhi, 2000) 5 It is estimated that 2 million children under 5 years of age die every year because of the high child mortality rate. If the entire country experienced the child mortality rate of Kerala the number of such deaths each year would fall by a whopping 1.6 million (Shukla A, 2001: Right to Health Care, Health Action, May 2001) 6 NFHS-1998, 2000: National Family Health Survey –2: India, IIPS, Mumbai
PDF created with pdfFactory Pro trial version www.pdffactory.com

In the fifties and sixties the entire focus of the health sector in India was to manage epidemics. Mass campaigns were started to eradicate the various diseases. These separate countrywide campaigns with a techno-centric approach were launched against malaria, smallpox, tuberculosis, leprosy, filaria, trachoma and cholera. Cadres of workers were trained in each of the vertical programmes. The National Malaria Eradication Programme (NMEP) alone required the training of 150,000 workers spread over in 400 units in the prevention and curative aspects of malaria control.7 The policy of going in for mass campaigns was in continuation of the policy of colonialists who subscribed to the percepts of modern medicine that health could be looked after if the germs which were causing it were removed. But the basic cause of the various diseases is social, i.e. inadequate nutrition, clothing, and housing, and the lack of a proper environment. These were ignored. National programs were launched to eradicate the diseases. The NMEP was started in 1953 with aid from the Technical Cooperation Mission of the U.S.A. and technical advice of the W.H.O. Malaria at that period was considered an international threat. DDT spraying operations was one of the most important activities of the programme. The tuberculosis programme involved vaccination with BCG, T.B. clinics, and domiciliary services and after care. The emphasis however was on prevention through BCG. These programmes depended on international agencies like UNICEF, WHO and the Rockefeller Foundation for supplies of necessary chemicals and vaccines. The policy with regard to communicable diseases was dictated by the imperialist powers as in the other sectors of the economy. Along with financial aid came political and ideological influence. Experts of various international agencies decided the entire policy framework, programme design, and financial commitments etc. During the first two Five Year Plans the basic structural framework of the public health care delivery system remained unchanged. Urban areas continued to get over three-fourth of the medical care resources whereas rural areas received "special attention" under the Community Development Program (CDP). History stands in evidence to what this special attention meant. The CDP was failing even before the Second Five Year Plan began. The governments own evaluation reports confessed this failure. The health sector organization under CDP was to have a primary health unit (a very much diluted form from what was suggested by the Bhore Committee) per development Block (in the fifties this was about 70,000 population spread over 100 villages) supported by a Secondary health unit (hospital with mobile dispensary) for every three such primary health units. The aim of this health organization was "the improvement of environmental hygiene, including provision and protection of water supply; proper disposal of human and animal wastes; control of epidemic diseases such as malaria, cholera, small pox, TB etc.; 7 Banerji, 1985…
PDF created with pdfFactory Pro trial version www.pdffactory.com

provision of medical aid along with appropriate preventive measures, and education of the population in hygienic living and in improved nutrition".8 It is clear from the above statement of objectives of the health organization under CDP that medical care had no priority within the structure of such an organization. In contrast, in the urban areas (which developed independent of CDP) hospitals and dispensaries, which provided mainly curative services (medical care) proliferated. Thus at the start of the third Five year Plan there was only one Primary Health Unit per 140,000 rural population (14 times, less than what the Bhore Committee recommended) in addition to one hospital per 320,000 rural population. In sharp contrast urban areas had one hospital per 36,000 urban population and one hospital bed per 440 urban residents (rural areas had 1 hospital bed per 7000 rural population). This rural-urban differential is the foundation of the discriminatory healthcare system which continues to exist in India even today. To evaluate the progress made in the first 2 plans and to make recommendation for the future path of development of health services the Mudaliar Committee was set up in 1959. The report of the committee recorded that the disease control programmes had some substantial achievements in controlling certain virulent epidemic diseases. Malaria was considered to be under control. Deaths due to malaria, cholera, smallpox etc. were halved or sharply reduced and the overall morbidity and mortality rates had declined. The death rate had fallen to 21.6% for the period 1956-61. The expectation of life at birth had risen to 42 years. However, the tuberculosis program lagged behind. The report also stated that for a million and half estimated open cases of tuberculosis there were not more than 30,000 beds available. The Mudaliar Committee further admitted that basic health facilities had not reached atleast half the nation. The PHC programme was not given the importance it should have been given right from the start. There were only 2800 PHCs existing by the end of 1961. Instead of the "irreducible minimum in staff" recommended by the Bhore Committee, most of the PHC's were understaffed, large numbers of them were being run by ANM's or public health nurses in charge.9 The fact was that the doctors were going into private practice after training at public expense. The emphasis given to individual communicable diseases programme was given top priority in the first two plans. But primary health centers through which the gains of the former could be maintained were given only tepid support.10
8 FYP 1, 227 (citations from Five Year Plans are noted as FYP 1 through 10 followed by page number - FYP 1 – 10, various years: Five Year Plans – First to Tenth, Planning Commission, GOI, New Delhi) 9Mudaliar Committee, 1961: Health Survey and Planning Committee, MoHFW, New Delhi 10Batliwala, Srilatha, 1978: The Historical Development of Health Services in India, FRCH, Bombay
PDF created with pdfFactory Pro trial version www.pdffactory.com
The Mudaliar Committee with regard to medical human-power suggested measures to improve the service condition of doctors and other personnel in order to attract them to rural areas. The committee makes a mention that except for the substantial increase in the number of doctors, number of other categories of health personnel was still woefully short of the requirement. Inspite of this the committee insisted that medical education should get a large share of public health resources. This was in clear contradiction to the committee's findings that doctors were not willing to go to rural areas. The decade scrutinised by the Mudaliar Committee had crystallized the trends and failings in the health system, yet the Committee held on to the belief that improvement in the technical excellence of medical care and substantial addition to medical humanpower would ultimately succeed in changing the country's health status. This is precisely what happened in the next two plan periods - allocations for training of doctors, especially specialists, increased. This was reflected in a large increase in medical college seats with outturn doubling in just one plan period. The outturn of nurses and other auxiliary personnel continued to stagnate. The third Five Year Plan launched in 1961 discussed the problems affecting the provision of PHCs, and directed attention to the shortage of health personnel, delays in the construction of PHCs, buildings and staff quarters and inadequate training facilities for the different categories of staff required in the rural areas.11 The Third Five Year Plan highlighted inadequacy of health care institutions, doctors and other personnel in rural areas as being the major shortcomings at the end of the second Five Year Plan.12 The doctor syndrome loomed large in the minds of planners, and increase in supply of humanpower in health meant more doctors and not other health personnel. While the 3rd plan did give serious consideration to the need for more auxiliary personnel no mention was made of any specific steps to reach this goal. Only lip service was paid to the need for increasing auxiliary personnel but in the actual training and establishment of institutions for these people, inadequate funding became the constant obstacle. On the other hand, the proposed outlays for new Medical Colleges, establishment of preventive and social medicine and psychiatric departments, completion of the All India Institute of Medical Sciences and schemes for upgrading departments in Medical Colleges for post graduate training and research continued to be high.13 In 1963 the Chadha Committee14 had recommended the integration of health and family planning services and its delivery through one male and one female multipurpose worker per 10,000 population. India was the first country in the world to adopt a policy of reducing population growth through a government sponsored family planning programme in 1951. In the first two plans the FP programme was mainly run through voluntary organizations, under the aegis of FPAI. Faced with a rising birth rate and a falling death rate the 3rd plan stated 11 FYP 3, 657 12 Ibid, 652 13 Batliwala, Srilatha, 1978, op.cit. 14 Chadha Committee, 1963: Special Committtee for NMEP Maintenance Phase, MoHFW, GOI, New Delhi
PDF created with pdfFactory Pro trial version www.pdffactory.com

that "the objective of stabilizing the growth of population over a reasonable period must therefore be at the very center of planned development". It was during this period that the camp approach was tried out and government agencies began to actively participate in pushing population control. This was also the time when family planning became an independent department in the Ministry of health. This was a fundamental change in India's health policy. This policy change, though it had its own inner compulsions, was more so due to the influence of foreign agencies. To endorse this strategy The Special Committee to Review the Staffing Pattern and Financial Provision under Family Planning was appointed (Mukherjee Committee). This committee indicated that the camp approach had failed to give the family planning program a mass character and hence the coming in of IUCD (loop) was a great opportunity. This committee also recommended introduction of target fixation, payments for motivation and incentives to acceptors. It suggested reorganization of the FP program into a vertical program like malaria and recommended addition of one more Health visitor per PHC who would specifically supervise the ANMs for the targets of this program. Also the Committee recommended retaining of private practitioners for a fee of Rs. 100 pm for 6 hours work per week plus payment of Rs. 10 per sterilization and Rs. 2 per IUCD insertion.15 The 4th Plan which began in 1969 with a 3 year plan holiday continued on the same line as the 3rd plan. It quoted extensively from the FYP II about the socialist pattern of society16 but its policy decisions and plans did not reflect socialism. Infact the 4th plan is probably the most poorly written plan document. It does not even make a passing comment on the social, political and economic upheaval during the plan Holiday period (1966-1969). These 3 years of turmoil indeed brought about significant policy changes on the economic front and this, the 4th plan ignored completely. It lamented on the poor progress made in the PHC programme and recognized again the need to strengthen it. It pleaded for the establishment of effective machinery for speedy construction of buildings and improvement of the performance of PHCs by providing them with staff, equipment and other facilities.17 For the first time PHCs were given a separate allocation. It was reiterated that the PHC's base would be strengthened along with, sub-divisional and district hospitals, which would be referral centers for the PHCs. The importance of PHCs was stressed to consolidate the maintenance phase of the communicable diseases programme. This acknowledgement was due to the fact that the entire epidemiological trend was reversed in 1966 with the spurt in incidence of malaria which rose from 100,000 cases annually between 1963-65, to 149,102 cases.18 The planning commission admitted this. FP continued to get even a greater emphasis with 42% of health sector (Health + FP) plan allocation going to it. It especially highlighted the fact that population growth was the 15 Mukherjee Committee, 1966: Committee to Review Staffing Pattern and Financial Provision under Family Planning Programme, MoHFW, New Delhi 16 FYP 4, 1-4 17ibid, 390 18ibid.
PDF created with pdfFactory Pro trial version www.pdffactory.com

central problem and used phrases like "crippling handicap", "very serious challenge" and an anti-population growth policy as an "essential condition of success"19 to focus the government's attention to accord fertility reduction "as a program of the highest priority".20 It was in the 5th Plan that the government ruefully acknowledged that despite advances in terms of infant mortality rate going down, life expectancy going up, the number of medical institutions, functionaries, beds, health facilities etc, were still inadequate in the rural areas. This shows that the government acknowledged that the urban health structure had expanded at the cost of the rural sectors.21 This awareness is clearly reflected in the objectives of 5th Five Year Plan which were as follows : 1) Increasing the accessibility of health services to rural areas through the Minimum Needs Programme (MNP) and correcting the regional imbalances. 2) Referral services to be developed further by removing deficiencies in district and sub-division hospitals. 3) Intensification of the control and eradication of communicable diseases. 4) Affecting quality improvement in the education and training of health personnel. 5) Development of referral services by providing specialists attention to common diseases in rural areas.22 The methods by which these goals were to be achieved were through the MNP, the MPW training scheme, and priority treatment to backward and tribal areas. Major innovations took place with regard to the health policy and method of delivery of health care services. The reformulation of health programmes was to consolidate past gains in various fields of health such as communicable diseases, medical education and provision of infrastructure in rural areas. This was envisaged through the MNP which would "receive the highest priority and will be the first charge on the development outlays under the health sector.23 It was an integrated packaged approach to the rural areas. The plan further envisaged that the delivery of health care services would be through a new category of health personnel to be specially trained as multi-purpose health assistants. However, the infrastructure target still remained one PHC per CDP Block (as in the FYPI but the average Block's population was now 125000!) The Kartar Singh Committee in 1973 recommended the conversion of uni-purpose workers, including ANMs, into multi-purpose male and female workers. It recommended that each pair of such worker should serve a population of 19 FYP 4, 31-32 20 ibid, 391 21 FYP 5, 234 22 Ibid, 234 23 Ibid, 234
PDF created with pdfFactory Pro trial version www.pdffactory.com
10,000 to 12,000. Hence the multi-purpose worker scheme was launched with the objective to retrain the existing cadre of vertical programme workers and the various vertical programmes were to be fully integrated into the primary health care package for rural areas.24 Another major innovation in the health strategy was launched in 1977 by creating a cadre of village based health auxiliaries called the Community Health workers. These were part time workers selected by the village, trained for 3 months in simple promotive and curative skills both in allopathy and indigenous systems of medicine. They were to be supervised by MPWs, and the programme was started in 777 selected PHCs where MPWs were already in place. This scheme was adopted on the recommendations of the Shrivastava Committee, which was essentially a committee to look into medical education and support manpower. The committee proposed to rectify the dearth of trained manpower in rural areas. The committee pointed out that "the over-emphasis on provision of health services through professional staff under state control has been counter productive. On the one hand it is devaluing and destroying the old traditions of part-time semi-professional workers, which the community used to train and throw up and proposed that with certain modifications can continue to provide the foundation for the development of a national programme of health services in our country. On the other hand the new professional services provided under state control are inadequate in quantity and unsatisfactory in quality".25 This very direct statement from the committee which was set up to review medical education and its related components assumes significance because it showed that the investment on health care has not been going to the people. The main recommendation of the committee was to have part-time health personnel selected by the community from within the community. They would act as a link between the MPW at the sub-centers and the community. With regard to medical education the committee cried for a halt to opening of new medical colleges. The committee emphasized that there was no point in thinking that doctors would go to rural areas because there were a number of socio-economic dimensions to this issue. Thus their option for rural areas was the CHW scheme. This attitude was clearly supportive of the historical paradigm that rural and urban areas had different health care needs – that urban populations need curative care and rural populations preventive. This also is discriminatory since inherent in this paradigm is deprivation for the rural masses. In the middle of the 5th Plan a State of National Emergency was proclaimed and during this period (1975-77) population control activities were stepped up with compulsion, force and violence now characterizing the FP program. In the midst of all this the National Population Policy was announced whose core aim was a
24Kartar Singh Committee, 1973: Committee on Multipurpose Worker under Health and Family Planning, MoHFW, New Delhi 25Shrivastava Committee, 1975: Report of the Group on Medical Education and Support Manpower, MoHFW, New Delhi
PDF created with pdfFactory Pro trial version www.pdffactory.com

“direct assault on the problem of population rise as a national commitment”26, this clearly contradicting the statement India made at the Bucharest Population summit that “development is the best contraceptive”, ironically by the same health minister! One of the recommendations included was legislation by state governments for compulsory sterilization. With the end of the Emergency and a new government in power this policy was sent to the freezer. The Sixth Plan was to a great extent influenced by the Alma Ata declaration of Health For All by 2000 AD and the ICSSR - ICMR report.27 The plan conceded that "there is a serious dissatisfaction with the existing model of medical and health services with its emphasis on hospitals, specialization and super specialization and highly trained doctors which is availed of mostly by the well to do classes. It is also realized that it is this model which is depriving the rural areas and the poor people of the benefits of good health and medical services".28 The plan emphasized the development of a community based health system. The strategies advocated were : a) provision of health services to the rural areas on a priority basis. b) the training of a large cadre of first level health workers selected from the community and supervised by MPWs and medical officers of the PHCs. c) No further linear expansion of curative facilities in urban areas; this would be permitted only in exceptional cases dictated by real felt need or priority.29 The plan emphasized that horizontal and vertical linkages had to be established among all the interrelated programmes, like water supply, environmental sanitation, hygiene, nutrition, education, family planning and MCH. The objective of achieving a net reproduction rate of 1 by 1995 was reiterated. This plan and the seventh plan too, like the earlier ones make a lot of radical statements and have recommend progressive measures. But the story is the same - progressive thinking and inadequate action. Whatever new schemes are introduced the core of the existing framework and ideology remains untouched. The underprivileged get worse off and the already privileged get better off. The status quo of the political economy is maintained. However, the Sixth and the Seventh plans are different from the earlier ones in one respect. They no longer talk of targets. The keywords are efficiency and quality and the means to realize them is privatisation. Privatisation is the global characteristic of the eighties and the nineties and it has made inroads everywhere and especially in the socialist countries. The Sixth and Seventh Five Year Plans state clearly : ".......... the success of the plan depends crucially on the efficiency, quality and texture of implementation. 26Karan Singh, 1976: National Population Policy, NIHAE Bull, IX,2, 155-160 27ICMR-ICSSR, 1980: Health For All – An Alternative Strategy, IIE, ICSSR, Pune 28 FYP 6, Vol. III, 250 29Ibid, 251-252
PDF created with pdfFactory Pro trial version www.pdffactory.com
...... a greater emphasis in the direction of competitive ability, reduced cost and greater mobility and flexibility in the development of investible resources in the private sector (by adapting) flexible policies to revive investor interest in the capital markets".30 "Our emphasis must be on greater efficiency, reduction of cost and improvement of quality. This calls for absorption of new technology, greater attention to economies of scale and greater competition".31 The National Health Policy of 1983 was announced during the Sixth plan period. It was in no way an original document. It accepted in principle the ICMR-ICSSR Report's (1981) recommendations as is evidenced from the large number of paragraphs that are common to both documents. But beyond stating the policy there was no subsequent effort at trying to change the health situation for the better. The National Health Policy (NHP) in light of the Directive Principles of the constitution of India recommends, "Universal, comprehensive primary health care services which are relevant to the actual needs and priorities of the community at a cost which people can afford".32 Providing universal health care as a goal is a welcome step because this is the first time after the Bhore Committee that the government is talking of universal comprehensive health care. A policy document is essentially the expression of ideas of those governing to establish what they perceive is the will of the people. These may not necessarily coincide for various reasons and influences that impinge upon both the rulers and the ruled. Implementing a policy, especially if it seeks to significantly change the status quo, necessarily requires a political will. Whether the political will is expressed through action depends on both the levels of conscientisation of the electorate and the social concerns of those occupying political office. A health policy is thus the expression of what the health care system should be so that it can meet the health care needs of the people. The health policies of Independent India, adopted by the First Health Ministers’ Conference in 1948 were the recommendations of the Bhore Committee. However, with the advent of planning the levels of health care as recommended by the Bhore Committee were diluted by subsequent committees and the Planning Commission. In fact, until 1983 there was no formal health policy, the latter being reflected in the discussions of the National Development Council and the Central Council of Health and Family Welfare, and the Five Year Plan documents and/or occasional committee reports as discussed above. As a consequence of the global debate on alternative strategies during the seventies, the signing of the Alma Ata Declaration on primary health care and the recommendations of the ICMR-ICSSR
30FYP 6, 1980, xxi and 86 31 FYP 7, 1985, vol. 1, vi 32MoHFW, 1983 : National Health Policy, Govt. of India, Ministry of Health & Family Welfare, p 3-4, New Delhi
PDF created with pdfFactory Pro trial version www.pdffactory.com
Joint Panel, the government decided that the above fora may have served the needs in the past but a new approach was now required,
"It is felt that an integrated, comprehensive approach towards the future development of medical education, research and health services requires to be established to serve the actual health needs and priorities of the country. It is in this context that the need has been felt to evolve a National Health policy,"33
The salient features of the 1983 health policy were:
(a) It was critical of the curative-oriented western model of health care, (b) It emphasised a preventive, promotive and rehabilitative primary health care
approach, (c) It recommended a decentralised system of health care, the key features of
which were low cost, deprofessionalisation (use of volunteers and paramedics), and community participation,
(d) It called for an expansion of the private curative sector which would help reduce the government's burden,
(e) It recommended the establishment of a nationwide network of epidemiological stations that would facilitate the integration of various health interventions, and
(f) It set up targets for achievement that were primarily demographic in nature. There are three questions that must now be answered. Firstly, were the tasks enlisted in the 1983 NHP fulfilled as desired? Secondly, were these tasks and the actions that ensued adequate enough to meet the basic goal of the 1983 NHP of providing "universal, comprehensive primary health care services, relevant to actual needs and priorities of the community"?34 And thirdly, did the 1983 NHP sufficiently reflect the ground realities in health care provision? During the decade following the 1983 NHP rural health care received special attention and a massive program of expansion of primary health care facilities was undertaken in the 6th and 7th Five Year Plans to achieve the target of one PHC per 30,000 population and one subcentre per 5000 population. This target has more or less been achieved, though few states still lag behind. However, various studies looking into rural primary health care have observed that, though the infrastructure is in place in most areas, they are grossly underutilised because of poor facilities, inadequate supplies, insufficient effective person-hours, poor managerial skills of doctors, faulty planning of the mix of health programs and lack of proper monitoring and evaluatory mechanisms. Further, the system being based on the health team concept failed to work because of the mismatch of training and the work allocated to health workers, inadequate transport facilities, non-availability of appropriate accommodation for the health team and an unbalanced distribution of work-time for various activities. In fact, many studies
33 ibid., 1 34 ibid., 3-4
PDF created with pdfFactory Pro trial version www.pdffactory.com
have observed that family planning, and more recently immunisation, get a disproportionately large share of the health workers' effective work-time. Among the other tasks listed by the 1983 health policy, decentralisation and deprofessionalisation have taken place in a limited context but there has been no community participation. This is because the model of primary health care being implemented in the rural areas has not been acceptable to the people as evidenced by their health care seeking behaviour. The rural population continues to use private care and whenever they use public facilities for primary care it is the urban hospital they prefer. Let alone provision of primary medical care, the rural health care system has not been able to provide for even the epidemiological base that the NHP of 1983 had recommended. Hence, the various national health programs continue in their earlier disparate forms, as was observed in the NHP. As regards the demographic and other targets set in the NHP, only crude death rate and life expectancy have been on schedule. The others, especially fertility and immunisation related targets are much below expectation (despite special initiatives and resources for these programs over the last two decades), and those related to national disease programs are also much below the expected level of achievement. In fact, we are seeing a resurgence of communicable diseases. With regard to the private health sector the NHP clearly favours privatization of curative care. It talks of a cost that "people can afford", thereby implying that health care services will not be free. Further statements in the NHP about the private health sector leave no room for doubt that the NHP is pushing privatisation. NHP adopts the stance that curative orientation must be replaced by the preventive and promotive approach so that the entire population can benefit. The NHP suggests that curative services should be left to the private sector because the state suffers from a "constraint of resources". It recommends, "with a view to reducing governmental expenditure and fully utilizing untapped resources, planned programmes may be devised, related to the local requirements and potentials, to encourage the establishment of practice by private medical professionals, increased investment by non-governmental agencies in establishing curative centers and by offering organized logistical, financial and technical support to voluntary agencies active in the health field ... and in the establishment of centers equipped to provide specialty and super specialty services ... efforts should be made to encourage private investments in such fields so that the majority of such centers, within the governmental set-up, can provide adequate care and treatment to those entitled to free care, the affluent sectors being looked after by the paying clinics".35 Thus the NHP 1983 had set the agenda for the future of the health sector in India. The development of health care services post-NHP provide a clear evidence
35MoHFW, 1983, 7-8, op.cit.
PDF created with pdfFactory Pro trial version www.pdffactory.com

that privatisation and private sector expansion in the health sector has occurred rapidly, that in the name of primary health care the state has still kept the periphery without adequate curative services (while the states' support to curative services in urban areas continues to remain strong) and that the state health sectors' priority program still continues to be population control (as recommended in NHP).36 The expansion of the private health sector in the last two decades has been phenomenal thanks to state subsidies in the form of medical education, soft loans to set up medical practice etc. The private health sector's mainstay is curative care and this is growing over the years (especially during the eighties and nineties) at a rapid pace largely due to a lack of interest of the state sector in non-hospital medical care services, especially in rural areas. Various studies show that the private health sector accounts for over 70% of all primary care treatment sought, and over 40% of all hospital care. This is not a very healthy sign for a country where over three-fourths of the population lives at or below subsistence levels. The above analysis clearly indicates that the 1983 NHP did not reflect the ground realities adequately. The tasks enunciated in the policy were not sufficient to meet the demands of the masses, especially those residing in rural areas. "Universal, comprehensive, primary health care services", the 1983 NHP goal, is far from being achieved. The present paradigm of health care development has in fact raised inequities, and in the current scenario of structural adjustment the present strategy is only making things worse. The current policy of selective health care, and a selected target population has got even more focused since the 1993 World Development Report: Investing in Health. In this report the World Bank has not only argued in favour of selective primary health care but has also introduced the concept of DALYs (Disability Adjusted Life Year’s) and recommends that investments should be made in directions where the resources can maximise gains in DALYs. That is, committing increasing resources in favour of health priorities where gains in terms of efficiency override the severity of the health care problems, questions of equity and social justice. So powerful has been the World Bank's influence, that the WHO too has taken an about turn on its Alma Ata Declaration. WHO in its "Health For All in the 21st Century" agenda too is talking about selective health care, by supporting selected disease control programs and pushing under the carpet commitments to equity and social justice. India's health policy too has been moving increasingly in the direction of selective health care - from a commitment of comprehensive health care on the eve of Independence, and its reiteration in the 1983 health policy, to a narrowing down of concern only for family planning, immunisation and control of selected diseases. Hence, one has to view with seriousness the continuance of the current paradigm and make policy changes which would make primary health care as per
36 Ibid., 4
PDF created with pdfFactory Pro trial version www.pdffactory.com

the needs of the population a reality and accessible to all without any social, geographical and financial inequities. The 7th Five-Year Plan accepted the above NHP advice. It recommended that "development of specialties and super-specialties need to be pursued with proper attention to regional distribution"37 and such "development of specialised and training in super specialties would be encouraged in the public and the private sectors"38. This plan also talks of improvement and further support for urban health services, biotechnology and medical electronics and non-communicable diseases39. Enhanced support for population control activities also continues40. The special attention that AIDS, cancer, and coronary heart diseases are receiving and the current boom of the diagnostic industry and corporate hospitals is a clear indication of where the health sector priorities lie. On the eve of the Eighth Five Year Plan the country went through a massive economic crisis. The Plan got pushed forward by two years. But despite this no new thinking went into this plan. Infact, keeping with the selective health care approach the eighth plan adopted a new slogan – instead of Health for All by 2000 AD it chose to emphasize Health for the Underprivileged41. Simultaneously it continued the support to privatization, “In accordance with the new policy of the government to encourage private initiatives, private hospitals and clinics will be supported subject to maintenance of minimum standards and suitable returns for the tax incentives42.” The 9th Five-Year Plan by contrast provides a good review of all programs and has made an effort to strategise on achievements hitherto and learn from them in order to move forward. There are a number of innovative ideas in the ninth plan. It is refreshing to see that reference is once again being made to the Bhore Committee report and to contextualise today’s scenario in the recommendations the Bhore Committee had made43. In its analysis of health infrastructure and human resources the Ninth Plan says that consolidation of PHCs and SCs and assuring that the requirements for its proper functioning are made available is an important goal under the Basic Minimum Services program. Thus, given that it is difficult to find physicians to work in PHCs and CHCs the Plan suggests creating part-time positions which can be offered to local qualified private practitioners and/or offer the PHC and CHC premises for after office hours practice against a rent. Also it suggests putting in place mechanisms to strengthen referral services.
37FYP 7, vol II, 273 38 Ibid., II, 277 39 Ibid, II. 273-276 40 Ibid., II. 279-287 41 FYP 8, 322 42 ibid, 324 43 FYP 9, 446
PDF created with pdfFactory Pro trial version www.pdffactory.com
Another unique suggestion is evolving state specific strategies because states have different scenarios and are at different levels of development and have different health care needs44. The Ninth Plan also shows concern for urban health care, especially the absence of primary health care and complete reliance on secondary and tertiary services even for minor ailments. This needs to be changed through provision of primary health care services, especially in slums, and providing referral linkages at higher levels45. During the Eighth Plan resources were provided to set up the Education Commission for Health Sciences, and afew states have even set up the University for Health Sciences as per the recommendations of the Bajaj committee report of 1987. This initiative was to bring all health sciences together, provide for continuing medical education and improve medical and health education through such integration. The Ninth Plan has made provisions to speed up this process46. During the 8th Plan period a committee to review public health was set up. It was called the Expert Committee on Public Health Systems. This committee made a thorough appraisal of public health programs and found that we were facing a resurgence of most communicable diseases and there was need to drastically improve disease surveillance in the country. The Ninth Plan proposed settting up at district level a strong detection come response system for rapid containment of any outbreaks that may occur. Infact, the recommendations of this committee have formed the basis of the Ninth Plan health sector strategy to revitalize the public health system in the country to respond to its health care needs in these changed times47. Also the Plan has proposed horizontal integration of all vertical programs at district level to increase their effectiveness as also to facilitate allocative efficiencies. What is also interesting is that the 9th Plan also reviews the 1983 National Health Policy in the context of its objectives and goals and concludes that a reappraisal and reformulation of the NHP is necessary so that a reliable and relevant policy framework is available for not only improving health care but also measuring and monitoring the health care delivery systems and health status of the population in the next two decades48. In this context the 9th Plan is critical of the poor quality of data management and recommends drastic changes to develop district level databases so that more relevant planning is possible49. Taking lead from the 9th Plan the Ministry of Health and Family Welfare took up the task of formulating a new health policy.
44 Ibid, 458 45 Ibid, 460 46ibid, 468 47 Ibid, 499 48 Ibid, 503 49Ibid, 472
PDF created with pdfFactory Pro trial version www.pdffactory.com

On the eve of the 10th Plan, the draft National Health Policy 2001 was announced and for the first time feedback invited from the public. "Universal, comprehensive, primary health care services", the NHP 1983 goal, is not even mentioned in the NHP 2001 but the latter bravely acknowledges that the public health care system is grossly short of defined requirements, functioning is far from satisfactory, that morbidity and mortality due to easily curable diseases continues to be unacceptably high, and resource allocations generally insufficient -“It would detract from the quality of the exercise if, while framing a new policy, it is not acknowledged that the existing public health infrastructure is far from satisfactory. For the out-door medical facilities in existence, funding is generally insufficient; the presence of medical and para-medical personnel is often much less than required by the prescribed norms; the availability of consumables is frequently negligible; the equipment in many public hospitals is often obsolescent and unusable; and the buildings are in a dilapidated state. In the in-door treatment facilities, again, the equipment is often obsolescent; the availability of essential drugs is minimal; the capacity of the facilities is grossly inadequate, which leads to over-crowding, and consequentially to a steep deterioration in the quality of the services.”50 The main objective of NHP 2001 is to achieve an acceptable standard of good health amongst the general population of the country51. The goals given in Box IV of the policy document are laudable but how their achievement in the specified time frame will happen has not been supported adequately in the policy document. For instance, goal number 10 “ Increase utilization of public health facilities from current level of <20 to >75%” is indeed remarkable. What it means is a reversal of existing utilization patterns. While we support this goal to the hilt we are worried that many prescriptions of the policy favour strengthening of the private health sector and hence is contrary to this goal. In sum NHP 2001 is a mere collection of unconnected statements, is a dilution of the role of public health services envisaged in the earlier policy and is unabashedly promoting the private health sector. The Ninth Plan also reviews the population policy and the family planning program. In this review too it goes back to the Bhore Committee report and says that the core of this program is maternal and child health services. Assuring antenatal care, safe delivery and immunization are critical to reducing infant and maternal mortality and this in turn has bearing on contraception use and fertility rates. This is old logic which the family planning program has used, only earlier their emphasis was on sterilization. In the early sixties the setting up of subcentres and employing ANMs was precisely for the MCH program but at the field level the family planning program hijacked this. This story continues through the seventies and eighties. MCH became Safe Motherhood, and expanded Program of Immunization and the latter using a mission approach under Sam
50 NHP-2001: Draft National Health Policy, Ministry of Health and Family Welfare, GOI, para 2.4.1 New Delhi 51 ibid. para 3.1
PDF created with pdfFactory Pro trial version www.pdffactory.com

Pitroda became Universal Program of Immmunisation. In the 7th Plan this got combined again to become Child Survival and Safe Motherhood, but the essential emphasis remained on family planning. But since the 8th Plan and into the 9th Plan CSSM acquired a genuine seriousness and presently it is transformed into the RCH program on the basis of the ICPD-Cairo agenda and receives multi-agency external funding support to provide need based, demand driven, high quality integrated reproductive and child health care. In the midst of all this the National Population Policy was announced with a lot of fanfare in the middle of 2000. It is definitely an improvement from its predecessors but the underlying element remains population control and not population welfare. The major concern is with counting numbers and hence its goals are all demographic. But I said earlier that there is improvement from the past because the demographic goals are placed in a larger social context and if that spirit is maintained in practice then we would definitely move forward. We are now through with the 9th Five-year Plan and a review of all its innovative suggestions shows that we have once again failed at the ground level. We have been unable to translate these ideas into practice. And despite all these efforts one can see the public health system weakening further. The answer is found in the 9th Plan itself. It laments that all these years we have failed to allocate even two percent of plan resources to the health sector. The same reason has killed the initiative shown in the 9th Plan process at the start itself by continuing the story of inadequate resource allocations for the health sector. The approach paper to the 10th Five-year Plan maintains the continuum from the 9th Plan. It does talk about reorganization and restructuring of the health infrastructure and linking it to a responsibility system on the basis of residence with a referral system for higher levels of care. The 10th Plan also says that the commitment to primary health care, emergency and life-saving services and the national programs must continue free of cost but puts in a rider of user charges for those above poverty line, and in the same breadth it quotes the NSS 52nd Round which reveals that even middle classes go into severe indebtedness for hospitalization and something towards risk-pooling needs to be developed.52 In the above review of plans and policies an issue of concern is the influence of international agencies in policymaking and program design both within and outside the plans. Right from the First plan onwards one can see the presence of international aid agencies that with a small quantum of money are able to inject large doses of ideology. It cannot be a coincidence that almost every health 52 The Draft Tenth Plan adopts the following contradictory stance: In view of the importance of health as a critical input for human development there will be continued commitment to provide: * essential primary health care, emergency life saving services, services under the National Disease Control programmes and the National Family Welfare Programme totally free of cost to all individuals and * essential health care service to people below poverty line based on their need and not on their ability to pay for the services. ... Available funds will be utilized to make all the existing institutions fully functional by providing needed equipment, consumables, diagnostics and drugs. In addition to funds from the centre, state, externally aided projects, locally generated funds from user charges and donations will be used for maintenance and repair to ensure optimal functional status and improve quality of services. (10th Plan approach paper, Planning Commission, GOI, pages 39-40, New Delhi)
PDF created with pdfFactory Pro trial version www.pdffactory.com

program the Indian government has taken up since the first plan has been anticipated by some international donor agency. Whether it was the CDP in the fifties, IUCD and malaria in the sixties or RCH and AIDS in the nineties, most health programs have been shaped through external collaboration. Historically, though there is a qualitative and quantitative difference. Upto the eighties the influence came through advice and ideology and hence its penetration was limited but post-eighties there is a lot of money also coming in, mostly as soft loans and along with conditionalities, and if we continue without making a paradigm shift and making structural changes, we will be transferring a burden to the next generation which it may be unable to carry!53 The larger dependence on external assistance in the health sector began with the India Population Projects (IPP) of the World Bank, which were essentially soft loans and not grants as in the past from bilateral and multilateral donors. The first five IPP’s focused on development of the health infrastructure, especially in rural areas dove-tailing with the Minimum Needs Program and did make a significant impact in strengthening the infrastructure but the subsequent IPPs changed the strategy to supporting recurring expenditure and this led to disaster because the dependence on World Bank and various bilateral donors like ODA (now DFID), USAID, DANIDA, NORAD, SIDA etc. for running various health programs reduced the governments’ own funding of these programs and that’s where the decline of the public health system began and continues to this day. The big international donors now are World Bank, European Union, USAID, and DFID and all follow a more or less similar strategy, that is supporting selective health programs targeted at specific population groups. This approach is unsustainable and can only distort further the healthcare system of the country and moving further away from the rights framework. This does not mean that international donor organizations do not have a role to play. The Rio Declaration had mandated that the developed world be obligated to provide development grants to the tune of 0.72% of their GDP. The international treaty organizations have failed in securing this obligation from developed countries. These grants are important in assisting the less developed countries in meeting obligations to assure rights that state parties have agreed to respect, protect and fulfill under various international covenants and treaties. But the developed world is no where close to realizing this obligation and the less developed world instead has to face the humiliation of indebtedness to these very developed countries and institutions like the World Bank, the Asia Development Bank etc.
53 Prior to the eighties external assistance was mostly grants and very insignificant in volume. During the entire decade of the seventies about $85 million per year of external assistance in the health sector was being received, largely as grants but after World Bank entered the picture in the eighties with IPP projects the scenario changed significantly with the annual average varying between $300 million and $600 million during eighties and nineties and mostly as loans with World Bank dominating with over two-thirds of such funds coming from it by end of the eighties (Gupta, D and A Gumber, 2002: External Assistance to the Health Sector and its Contributions – Problems and Prognosis, ICRIER, New Delhi)
PDF created with pdfFactory Pro trial version www.pdffactory.com
The above historical review of health policy and planning reveals the failure of the Indian State to assure health and healthcare as a right. What we see is that some earnest efforts at the policy level were made but they failed miserably in practice because of inadequate resource support and a lack of political will to back the cause of healthcare as a right. More than half a century’s experience of waiting for the policy route to assure respect, protection and fulfillment for healthcare is now behind us. The Bhore Committee recommendations which had the potential for this assurance were assigned to the back-burner due to the failure of the state machinery to commit a mere 2% of the Gross Domestic Product at that point of time for implementation of the Bhore Plan. In the review of the evolution of health policy we have seen that each plan and/or health committee contributed to the dilution of the comprehensive and universal access approach by developing selective schemes or programs, and soon enough the Bhore plan was archived and forgotten about. So our historical experience tells us that we should abandon the policy approach and adopt the human rights route to assuring universal access to all people for healthcare. We are today talking of health sector reform and hence it is the right time to switch gears and move in the direction of right to health and healthcare. The Healthcare System The political economy of health care services in India has various dimensions. Multiple systems, various types of ownership patterns and different kinds of delivery structures make up a complex plurality that makes the development of an organised system difficult. Allopathy, ayurveda, homoeopathy, unani, siddha, among others, are different systems of medicine available in the country. However, allopathy is the dominant system of medicine. Its domineering influence is evidenced by the fact that practitioners of the other systems of medicine also primarily practice allopathy. National surveys done by NSSO and NCAER and other small-scale studies clearly bring this out. As regards ownership, while the broad characterisation could be made as public and private, there are various intricacies involved. The public sector ownership is divided between central and state governments, and municipal and panchayat local governments. The facilities include teaching hospitals, secondary level hospitals, first level referral hospitals (CHCs or rural hospitals), dispensaries, PHCs and sub centres, and health posts. Apart from this there are public facilities for selected occupational groups like ESIS, defense, CHGS, railways, post and telegraph, mines etc.. These are usually hospitals of various capacities and dispensaries or clinics. Private ownership is of two kinds, for-profit and not-for-profit. The former could be self-employed or individual ownership or various other forms of ownership like partnership, cooperative or corporate. The not-for-profit is usually a Trust or a Society, many of these also being called NGOs. These again could be teaching
PDF created with pdfFactory Pro trial version www.pdffactory.com

hospitals, hospitals and nursing homes of various sizes and kinds of care, clinics and dispensaries, and diagnostic facilities. Public health facilities appear to be organised into some sort of a system. They are even allocated on the basis of population-based norms and/or on basis of specific geographic units. Thus for primary care there are dispensaries and health centres which provide largely ambulatory care. Rural areas have mostly health centres like Primary Health Centres and sub centres through which preventive and promotive care is provided, largely through paramedics. Presently there are about 24,000 PHCs and 140,000 sub centres in the country catering to about 700 million rural population. In addition in the public sector there are about 4000 rural dispensaries and about 2950 rural hospitals, which provide medical care and first level referral care. In urban areas public health services are largely of a curative nature being provided through dispensaries and hospitals of varying sizes and types of facilities. Taluka and other small towns usually have only dispensaries and a basic hospital. The district towns and larger towns and cities have dispensaries and one or more secondary level hospitals depending on their population size and these may be owned by either state and/or local governments; some of them may even have a teaching hospital and/or special hospitals. Compared to rural areas the urban areas are much better endowed with public health facilities (Table 1). Another special feature of public health services is that there are mass health care programs, largely of a preventive and promotive nature, like selected disease control programs (malaria, tuberculosis, leprosy, AIDS etc..), family planning and maternal and child health programs (contraception, immunisation, ante-natal care, etc..). Private health care is much larger and more widespread than public health services. Individual practitioners in their clinics provide ambulatory care, which may often be within their residence. Data on the private sector is a major problem. For practitioners the only information available is the registration data from the various medical councils but this data has various limitations. The actual practitioners are much more than the registered numbers because due to lack of regulation all kinds of persons set up medical practice on one hand and different kinds of practitioners indulge in large-scale cross-practice across different systems of medicine. The number of registered practitioners is estimated to be about 12 lakhs across the country with large concentrations in states like Maharashtra, Gujarat and the southern states. Eighty percent are in the private sector. The allopathic doctors constitute about 45 percent of total registered practitioners and are located mostly in urban areas, whereas the non-allopaths are mostly located in the smaller towns and rural areas. With regard to private hospitals the data gaps are similar. There is no proper registration process for private hospitals and hence the data available is a gross underestimate as revealed by surveys in Maharashtra and Andhra Pradesh54. The latest estimate reveals that nearly 70% of all hospitals and 40% of all hospital beds in the country are in the private sector with over 80% of them being in urban
54 See Nandraj, Sunil and Ravi Duggal, 1996 : Physical Standards in the Private Health Sector, Radical Journal of Health (New Series) II-2/3
PDF created with pdfFactory Pro trial version www.pdffactory.com

areas. A peculiar characteristic of private health services is that unlike the public health sector they provide almost entirely only curative care. Utilization and Healthcare Expenditures Comparison of utilization and health expenditure data across the 42nd (1987) and 52nd (1996) Rounds of NSS shows a very alarming trend. There is upto 30% decline in use of public healthcare facilities in both rural and urban areas over the decade. Why is this so? Partly the answer is within the same data set. The cost of seeking treatment even in public hospitals has increased over five-fold (in private it is nearly seven times). During the same period the purchasing power of the poorer classes has not changed in any substantial way and as a consequence the 52nd Round shows higher levels of untreated morbidity, especially amongst the poorer groups. The other part of the answer is the declining investment and expenditures in the public health sector. It can be argued that these trends are closely linked with a wide spectrum of changes in the economy since the mid-eighties, which have led to privatization of services, deregulation of drug prices, increased reliance on market mechanisms to address welfare needs, and weakening of public health systems. Thus the main hurdles to healthcare access are poverty and the changing political economy and the inequities associated with it. While data on the number of public health care facilities is available, the data about its use is not available in any systematic manner. The service statistics lack an epidemiological basis and are reported more in terms of targets and achievements, which have little meaning for the purposes of any analysis. State Performance Budgets do give some relevant utilisation data but these documents are not easily available nor the health statistics authorities compile data from them. In case of the private health sector data is conspicuous by its absence. However, in recent years national surveys, like the NSSO utilisation surveys in 1987 and 1996, the NCAER surveys in 1990 and 1993, NFHS surveys in 1993 and 1999, and the RCH rapid household survey in 1999, apart from the smaller studies, have provided reasonably good estimates of utilisation of health services and healthcare expenditures (Table 2). The NSSO data reveals that the share of outpatient services provided by public institutions has declined from 26% to 23% in rural areas over the decade (1986-1996) and from 27% to 22% in urban areas. This decline has been mainly in use of OPD of public hospitals, as the use of PHCs and dispensaries has remained the same in the overall proportion. This also means that the weight of PHCs, CHCs and dispensaries in public provision of OPD services has increased significantly, perhaps a result of expansion of the primary health care sector, especially in the rural areas. Thus the share of PHCs, CHCs and dispensaries in public facilities for OPD care increased from 31% to 42% in the rural areas during this period and in the urban areas from 11% to 15% (Table 3). In case of inpatient care the public sector is still a major provider but here too a declining trend is seen. The NSSO data indicates that in 1986-87 the public institutions accounted for 60% of all hospitalisations and this
PDF created with pdfFactory Pro trial version www.pdffactory.com
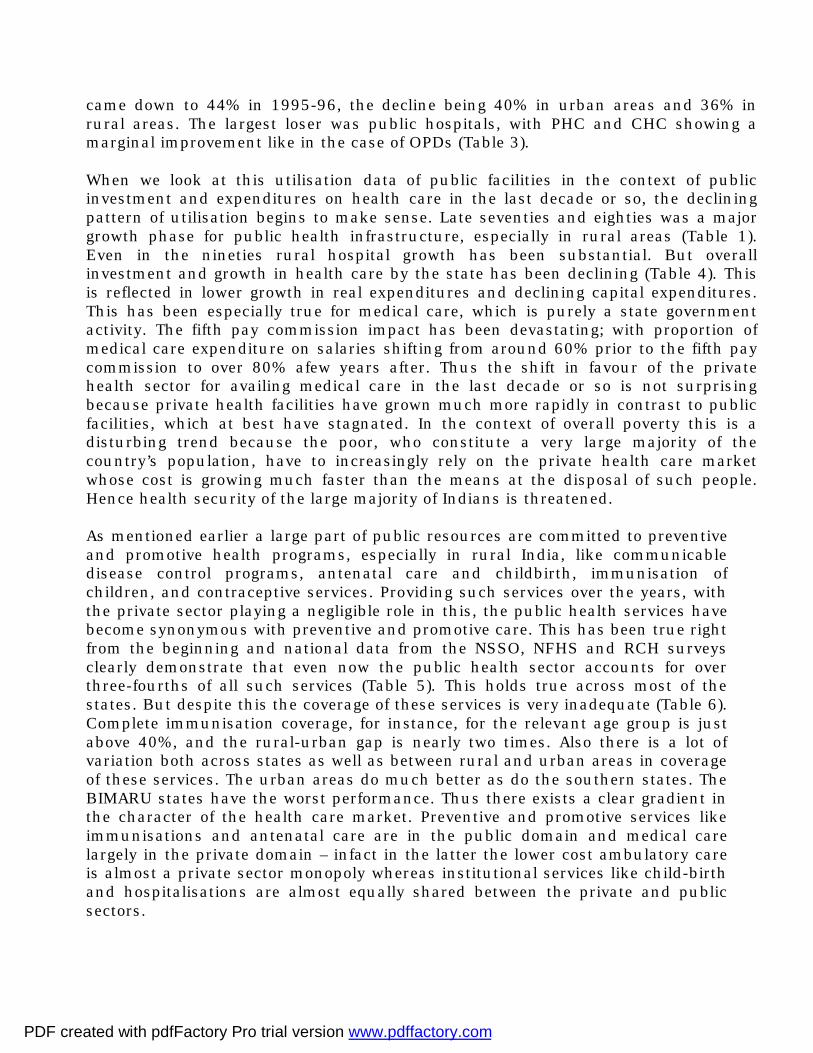
came down to 44% in 1995-96, the decline being 40% in urban areas and 36% in rural areas. The largest loser was public hospitals, with PHC and CHC showing a marginal improvement like in the case of OPDs (Table 3). When we look at this utilisation data of public facilities in the context of public investment and expenditures on health care in the last decade or so, the declining pattern of utilisation begins to make sense. Late seventies and eighties was a major growth phase for public health infrastructure, especially in rural areas (Table 1). Even in the nineties rural hospital growth has been substantial. But overall investment and growth in health care by the state has been declining (Table 4). This is reflected in lower growth in real expenditures and declining capital expenditures. This has been especially true for medical care, which is purely a state government activity. The fifth pay commission impact has been devastating; with proportion of medical care expenditure on salaries shifting from around 60% prior to the fifth pay commission to over 80% afew years after. Thus the shift in favour of the private health sector for availing medical care in the last decade or so is not surprising because private health facilities have grown much more rapidly in contrast to public facilities, which at best have stagnated. In the context of overall poverty this is a disturbing trend because the poor, who constitute a very large majority of the country’s population, have to increasingly rely on the private health care market whose cost is growing much faster than the means at the disposal of such people. Hence health security of the large majority of Indians is threatened. As mentioned earlier a large part of public resources are committed to preventive and promotive health programs, especially in rural India, like communicable disease control programs, antenatal care and childbirth, immunisation of children, and contraceptive services. Providing such services over the years, with the private sector playing a negligible role in this, the public health services have become synonymous with preventive and promotive care. This has been true right from the beginning and national data from the NSSO, NFHS and RCH surveys clearly demonstrate that even now the public health sector accounts for over three-fourths of all such services (Table 5). This holds true across most of the states. But despite this the coverage of these services is very inadequate (Table 6). Complete immunisation coverage, for instance, for the relevant age group is just above 40%, and the rural-urban gap is nearly two times. Also there is a lot of variation both across states as well as between rural and urban areas in coverage of these services. The urban areas do much better as do the southern states. The BIMARU states have the worst performance. Thus there exists a clear gradient in the character of the health care market. Preventive and promotive services like immunisations and antenatal care are in the public domain and medical care largely in the private domain – infact in the latter the lower cost ambulatory care is almost a private sector monopoly whereas institutional services like child-birth and hospitalisations are almost equally shared between the private and public sectors.
PDF created with pdfFactory Pro trial version www.pdffactory.com
Two decades ago the private sector’s share of hospital services was barely 20% but with declining state investment in the hospital sector since mid-eighties the scenario has altered drastically in favour of the private sector. Data on hospital care shows that there is a sharp class gradient in occurrence of such events and utilisation of such services. The lowest quintile contradictorily experiences a hospitalisation rate which is nearly 7 times less than the richest quintile, and what is worse that the richest quintile also has proportionately a utilisation rate of public hospitals which is four times that of the poorest quintile. Of course within the class the poor are larger users of public hospitals. Such a scenario is due to the poor physical access on one hand and on the other the paucity of resources in the poorer classes to demand and access what exists. If we convert the hospitalisation rates and usage of public hospitals across classes into subsidies then we see a pro-rich gradient with the richest quintile amassing one-third of the public hospital resources and the poorest quintile only one-tenth!
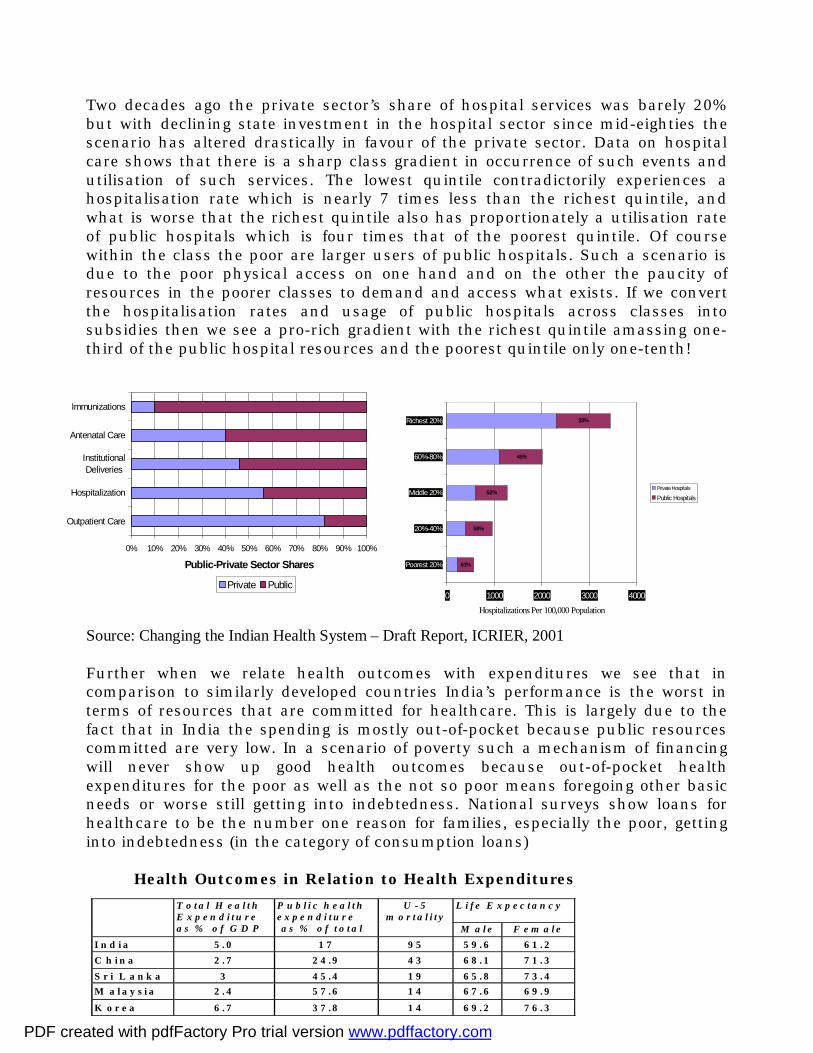
Source: Changing the Indian Health System – Draft Report, ICRIER, 2001 Further when we relate health outcomes with expenditures we see that in comparison to similarly developed countries India’s performance is the worst in terms of resources that are committed for healthcare. This is largely due to the fact that in India the spending is mostly out-of-pocket because public resources committed are very low. In a scenario of poverty such a mechanism of financing will never show up good health outcomes because out-of-pocket health expenditures for the poor as well as the not so poor means foregoing other basic needs or worse still getting into indebtedness. National surveys show loans for healthcare to be the number one reason for families, especially the poor, getting into indebtedness (in the category of consumption loans) Health Outcomes in Relation to Health Expenditures
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Outpatient Care
Hospitalization
InstitutionalDeliveries
Antenatal Care
Immunizations
Public-Private Sector Shares
Private Public
61%
58%
52%
45%
33%
0 1000 2000 3000 4000
Poorest 20%
20%-40%
Middle 20%
60%-80%
Richest 20%
Hospitalizations Per 100,000 Population
Private Hospitals
Public Hospitals
L i f e E x p e c t a n c y
T o t a l H e a l t h E x p e n d i t u r e a s % o f G D P
P u b l i c h e a l t h e x p e n d i t u r e a s % o f t o t a l
U - 5 m o r t a l i t y
M a l e F e m a l e I n d i a 5 . 0 1 7 9 5 5 9 . 6 6 1 . 2 C h i n a 2 . 7 2 4 . 9 4 3 6 8 . 1 7 1 . 3 S r i L a n k a 3 4 5 . 4 1 9 6 5 . 8 7 3 . 4 M a l a y s i a 2 . 4 5 7 . 6 1 4 6 7 . 6 6 9 . 9
K o r e a 6 . 7 3 7 . 8 1 4 6 9 . 2 7 6 . 3
PDF created with pdfFactory Pro trial version www.pdffactory.com
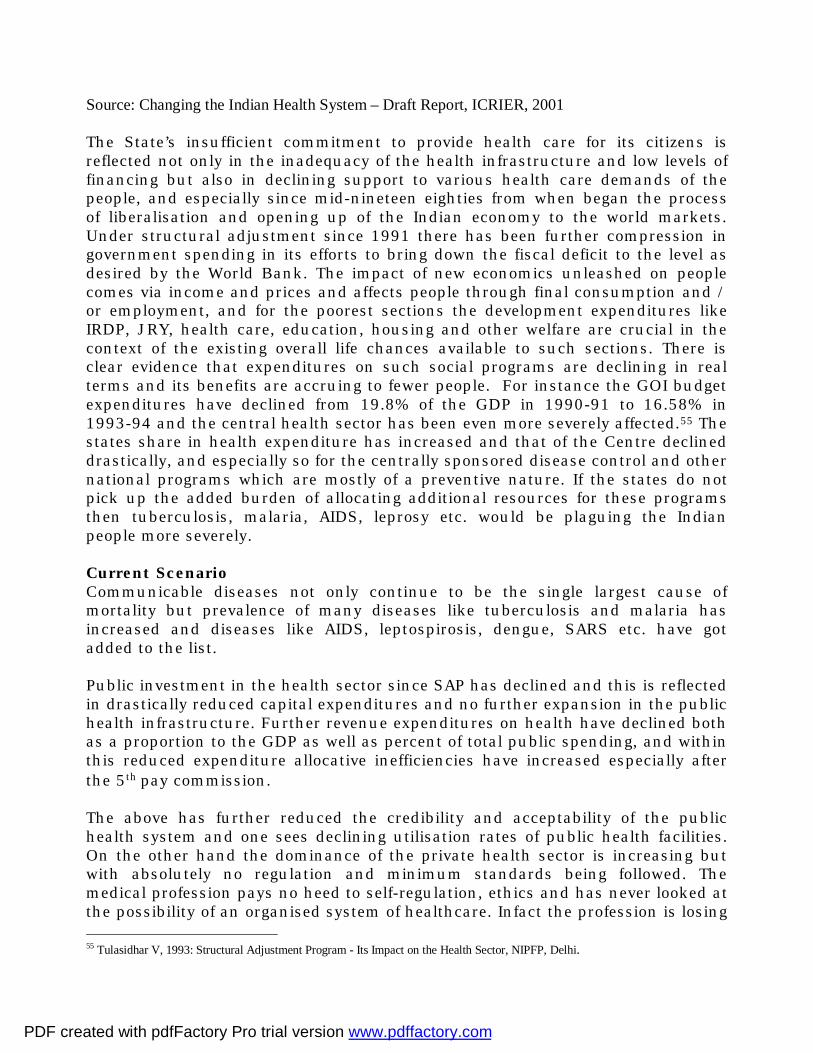
Source: Changing the Indian Health System – Draft Report, ICRIER, 2001 The State’s insufficient commitment to provide health care for its citizens is reflected not only in the inadequacy of the health infrastructure and low levels of financing but also in declining support to various health care demands of the people, and especially since mid-nineteen eighties from when began the process of liberalisation and opening up of the Indian economy to the world markets. Under structural adjustment since 1991 there has been further compression in government spending in its efforts to bring down the fiscal deficit to the level as desired by the World Bank. The impact of new economics unleashed on people comes via income and prices and affects people through final consumption and / or employment, and for the poorest sections the development expenditures like IRDP, JRY, health care, education, housing and other welfare are crucial in the context of the existing overall life chances available to such sections. There is clear evidence that expenditures on such social programs are declining in real terms and its benefits are accruing to fewer people. For instance the GOI budget expenditures have declined from 19.8% of the GDP in 1990-91 to 16.58% in 1993-94 and the central health sector has been even more severely affected.55 The states share in health expenditure has increased and that of the Centre declined drastically, and especially so for the centrally sponsored disease control and other national programs which are mostly of a preventive nature. If the states do not pick up the added burden of allocating additional resources for these programs then tuberculosis, malaria, AIDS, leprosy etc. would be plaguing the Indian people more severely. Current Scenario Communicable diseases not only continue to be the single largest cause of mortality but prevalence of many diseases like tuberculosis and malaria has increased and diseases like AIDS, leptospirosis, dengue, SARS etc. have got added to the list. Public investment in the health sector since SAP has declined and this is reflected in drastically reduced capital expenditures and no further expansion in the public health infrastructure. Further revenue expenditures on health have declined both as a proportion to the GDP as well as percent of total public spending, and within this reduced expenditure allocative inefficiencies have increased especially after the 5th pay commission. The above has further reduced the credibility and acceptability of the public health system and one sees declining utilisation rates of public health facilities. On the other hand the dominance of the private health sector is increasing but with absolutely no regulation and minimum standards being followed. The medical profession pays no heed to self-regulation, ethics and has never looked at the possibility of an organised system of healthcare. Infact the profession is losing 55 Tulasidhar V, 1993: Structural Adjustment Program - Its Impact on the Health Sector, NIPFP, Delhi.
PDF created with pdfFactory Pro trial version www.pdffactory.com

control to the corporate sector, which is now looking beyond the hospital sector at not only diagnostics but also consultant services and general practice. Such a scenario is bound to impact on costs and increase the burden of the patients. Such a situation is not good for 70% of the country’s population that lives in poverty or at subsistence level. The health status indicators amply testify to the poor state of health and healthcare in India. Our trajectory has been worse than the low-income country average over the years and we reached that level only in the nineties and we are stagnating at that level. Infant and child mortality rates which had shown substantial improvements in the eighties with stepped up public health investment under the MNP, especially in the rural areas, are presently not only stagnating but the rural – urban gap which was narrowing down is again getting wider.
IMR Trends in India and Low-income Countries 1960-1995
0306090
120150180
1960 1970 1980 1990 1995 2000Years
Per 1
000
live
birt
hs
India
Low-incomecountriesIndia Urban
India Rural
Decline in Rate of IMR and U-5 Mortality 1971-2001
0.05.0
10.015.020.025.030.035.040.0
1971-81 1981-91 1991-01
Years
Perc
enta
ges
Infant Mortalitydecline
Under-5Mortalitydecline
Source: SRS Bulletins and UNDP HDRs
PDF created with pdfFactory Pro trial version www.pdffactory.com

Apart from the rural-urban divide, there are issues in health and healthcare related to various vulnerable sections of the population and these are not only related to poverty and class concerns but also social concerns. Both access and health outcomes for women, dalits, adivasis, and other minority communities, show clear differentials in terms of adversities in health and healthcare. NFHS and NSSO data provide strong evidence for this.
Selected Health Outcomes Across Social Classes
Source: NFHS 2
Nutritional Outcomes Across Social Classes Source: NFHS 2
Social Group
No ANC
TFR
IMR
U-5 Mortality
Completed Immunisatn
Delivery by Doctor
LOW 45.1 3.37 88.8 130.0 30.4 15.8 Medium 32.8 2.85 70.3 94.6 43.2 31.1 HIGH 12.4 2.10 42.7 51.5 64.7 60.9 ALL 34.0 2.85 73.0 101.4 42.0 30.3 SC 38.2 3.15 83.0 119.3 40.2 23.5 ST 43.1 3.06 84.2 126.6 26.4 14.5 OBC 34.8 2.83 76.0 103.1 43.0 31.8 OTHER 27.9 2.66 61.8 82.6 46.8 37.3
Percent Women 15-49 Children < 3 yrs % below -3SD
Social Group
Below 145
Below BMI 18.5kg/m2
Any Anemia
Wt. For Age
Ht. For Age
Wt. For Height
LOW 17.7 48.1 60.2 25.3 29.8 3.9 Medium 12.5 35.6 50.3 16.5 22.4 2.4 HIGH 7.5 17.3 41.9 6.7 10.7 1.5 SC 17.0 42.1 56.0 27.2 27.5 3.0 ST 13.5 46.3 64.9 26.0 27.6 4.4 OBC 13.5 35.8 50.7 18.3 23.1 3.4 OTHER 10.9 30.5 47.6 13.8 19.4 1.8 ALL 13.2 35.8 51.8 18.0 23.0 2.8
PDF created with pdfFactory Pro trial version www.pdffactory.com
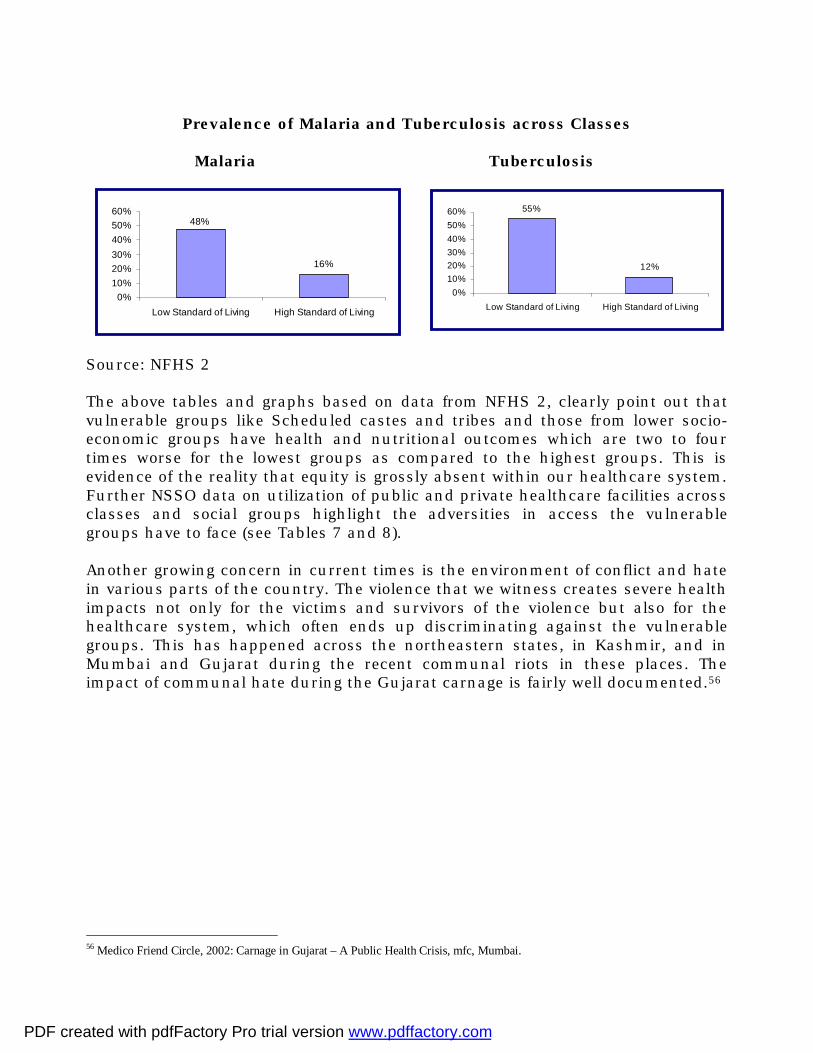
Prevalence of Malaria and Tuberculosis across Classes
Malaria Tuberculosis
Source: NFHS 2 The above tables and graphs based on data from NFHS 2, clearly point out that vulnerable groups like Scheduled castes and tribes and those from lower socio-economic groups have health and nutritional outcomes which are two to four times worse for the lowest groups as compared to the highest groups. This is evidence of the reality that equity is grossly absent within our healthcare system. Further NSSO data on utilization of public and private healthcare facilities across classes and social groups highlight the adversities in access the vulnerable groups have to face (see Tables 7 and 8). Another growing concern in current times is the environment of conflict and hate in various parts of the country. The violence that we witness creates severe health impacts not only for the victims and survivors of the violence but also for the healthcare system, which often ends up discriminating against the vulnerable groups. This has happened across the northeastern states, in Kashmir, and in Mumbai and Gujarat during the recent communal riots in these places. The impact of communal hate during the Gujarat carnage is fairly well documented.56
56 Medico Friend Circle, 2002: Carnage in Gujarat – A Public Health Crisis, mfc, Mumbai.
16%
48%
0%10%20%30%40%50%60%
Low Standard of Living High Standard of Living
55%
12%
0%10%20%30%40%50%60%
Low Standard of Living High Standard of Living
PDF created with pdfFactory Pro trial version www.pdffactory.com

The Changing Political Economy India is knocking at global markets. Since the mid-eighties India has rapidly integrated with the world economy and now faces not only the ups but also the downs as protection of the internal economy has become a thing of the past. The globalisation of India was speeded up under the Structural Adjustment Program designed with World Bank’s assistance to reform India’s economy. A large part of the middle class has certainly benefited from the SAP and related initiatives but overall poverty has not declined - if at all it has added to the misery of the already impoverished masses. Health sector reforms did not stay far behind. But the question is, were they reforms in the positive or progressive sense? In the name of reforms, again under the aegis of the World Bank, and other bilateral and multilateral agencies like USAID, DFID, WHO, UNICEF etc. public health investment became even more selective and targeted at selected populations. Thus family planning and immunisation services, and selective disease programs like HIV-AIDS, acquired an even more central position in public health care and other concerns like curative services, hospital care, malaria, tuberculosis, maternity services, etc. lost further ground. The new priorities were not priorities determined by those who needed health care but by global agents of change who were in the business of adjusting India to the world economy! Economic reforms towards liberalisation began in the early eighties. This is important to note because most often there is a tendency to look only at the post-1991 period. Data available upto now clearly shows that economic performance of the eighties far outweighs that in the nineties. And the underlying fact about this is that in the eighties there was no structural adjustment or World Bank dictat. The classical 'Hindu' rate of growth in the eighties had doubled from 3% to 6%, without much inflation and with declining levels of poverty. Thus we were already liberalising our economy and speeding up growth without the World Bank running the show. Infact, the post (1991)-reform period slowed down growth, increased poverty and inflation, and reversed many trends of the eighties. No doubt it caught up towards the mid-nineties, but it has not yet surpassed the achievements of the eighties. Thus in the eighties India was developing rapidly with a gradual globalisation process and with the advantage of its inner strength which insulated it from global shocks. In the nineties there was rapid globalisation that exposed India to global fluctuations; if India survived the Asian shock, which destroyed Indonesia and other Southeast Asian economies, it was because of its sheer size and the strengths of its own local markets. Another fact to contend with is the as yet dependence of over two-thirds of the population on agriculture and 70% of the population living in rural areas. Since the larger impact of macro-economic reforms is on the urban-industrial sector, which integrates globally with much ease, the rural population in a sense still has relative protection from global impacts. Further, it is the consistent good performance of agriculture that has
PDF created with pdfFactory Pro trial version www.pdffactory.com
helped ward off the severities of SAP, which many other countries have faced. In addition, India's strong investments in the past in rural development, especially employment guarantee programs and agricultural subsidies aided in reducing the adverse impact of SAP. And this is not likely to change thanks to the strong farm lobby that is in fact demanding greater investments and subsidies for the rural economy. Thus at one level India is much more exposed to the global market with increasing vulnerability. But at another level it continues to enjoy an inner strength and autonomy because of its sheer size, its large rural-agricultural population and a large local market of its own, despite the fact that politically the situation is very fluid. This background is important for understanding the impact and changes in the health sector. Impact Of Changing Political Economy While the existing situation is very dismal, the changing political economy does not show too much promise of change for the betterment of health and healthcare; unless of course there is a radical transformation in the political commitment. For this to happen the support of civil society pressures and demands for a transformation of the healthcare dispensation will be needed. The changing political economy demands reduced state participation in the economic sphere both in terms of policy and intervention. But at the same time the new political economy has failed to strengthen the welfare role of the state. Under SAP and other related measures, the states intervention in the economy declined but so have investments, expenditures and interests in the social sectors. This trajectory of growth has worsened the situation for the poor and subsistent population of the country. One very clear impact is declining state investments in the health sector. With rising debt burdens of the state the social sectors are the first to receive the axe. There has been a declining trend since 1991 in social sector expenditures, especially by the Central government and this is best reflected in compression of grants to the states for social sector expenditures. Health care expenditures too have been affected both in quantitative terms (declining real expenditures) and qualitative terms (increasing proportion of establishment costs and declining proportion on medicines, equipment, maintenance and new investments). IMPACT OF CHANGING POLITICAL ECONOMY..
Another very striking impact is the rapidly rising cost of medicines. With a large dependence on the private health sector even by the poor this has meant extreme hardship. With the drug price control virtually on its way out and with India having signed the WTO treaty on IPR we are moving closer to international prices of drugs. The combined effect of the above facts makes a deadly mixture that results in reduced access of the poor to health care. We have seen above the historical dominance of the private health care sector in India in provision of ambulatory care and rising costs could spell disaster for the poor given the fact that the State is gradually reducing its responsibilities in provision of health care. Since the poor too have been active users of private health care their dependence
PDF created with pdfFactory Pro trial version www.pdffactory.com
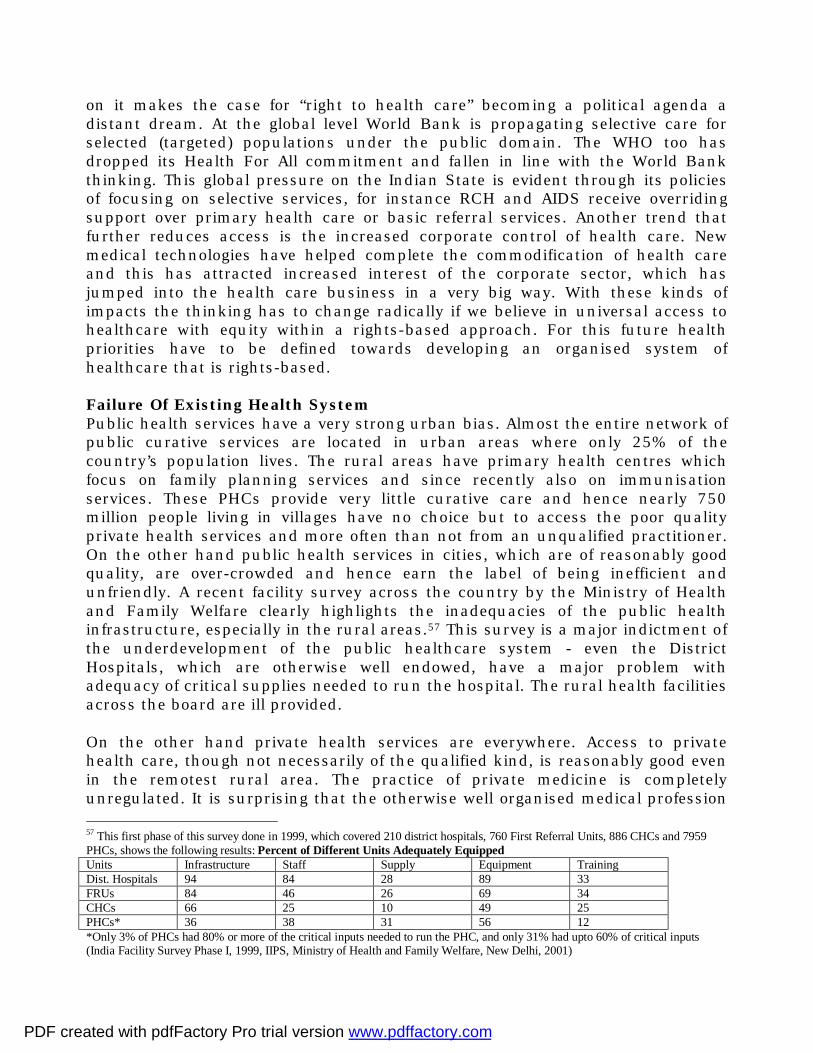
on it makes the case for “right to health care” becoming a political agenda a distant dream. At the global level World Bank is propagating selective care for selected (targeted) populations under the public domain. The WHO too has dropped its Health For All commitment and fallen in line with the World Bank thinking. This global pressure on the Indian State is evident through its policies of focusing on selective services, for instance RCH and AIDS receive overriding support over primary health care or basic referral services. Another trend that further reduces access is the increased corporate control of health care. New medical technologies have helped complete the commodification of health care and this has attracted increased interest of the corporate sector, which has jumped into the health care business in a very big way. With these kinds of impacts the thinking has to change radically if we believe in universal access to healthcare with equity within a rights-based approach. For this future health priorities have to be defined towards developing an organised system of healthcare that is rights-based. Failure Of Existing Health System Public health services have a very strong urban bias. Almost the entire network of public curative services are located in urban areas where only 25% of the country’s population lives. The rural areas have primary health centres which focus on family planning services and since recently also on immunisation services. These PHCs provide very little curative care and hence nearly 750 million people living in villages have no choice but to access the poor quality private health services and more often than not from an unqualified practitioner. On the other hand public health services in cities, which are of reasonably good quality, are over-crowded and hence earn the label of being inefficient and unfriendly. A recent facility survey across the country by the Ministry of Health and Family Welfare clearly highlights the inadequacies of the public health infrastructure, especially in the rural areas.57 This survey is a major indictment of the underdevelopment of the public healthcare system - even the District Hospitals, which are otherwise well endowed, have a major problem with adequacy of critical supplies needed to run the hospital. The rural health facilities across the board are ill provided. On the other hand private health services are everywhere. Access to private health care, though not necessarily of the qualified kind, is reasonably good even in the remotest rural area. The practice of private medicine is completely unregulated. It is surprising that the otherwise well organised medical profession 57 This first phase of this survey done in 1999, which covered 210 district hospitals, 760 First Referral Units, 886 CHCs and 7959 PHCs, shows the following results: Percent of Different Units Adequately Equipped Units Infrastructure Staff Supply Equipment Training Dist. Hospitals 94 84 28 89 33 FRUs 84 46 26 69 34 CHCs 66 25 10 49 25 PHCs* 36 38 31 56 12 *Only 3% of PHCs had 80% or more of the critical inputs needed to run the PHC, and only 31% had upto 60% of critical inputs (India Facility Survey Phase I, 1999, IIPS, Ministry of Health and Family Welfare, New Delhi, 2001)
PDF created with pdfFactory Pro trial version www.pdffactory.com
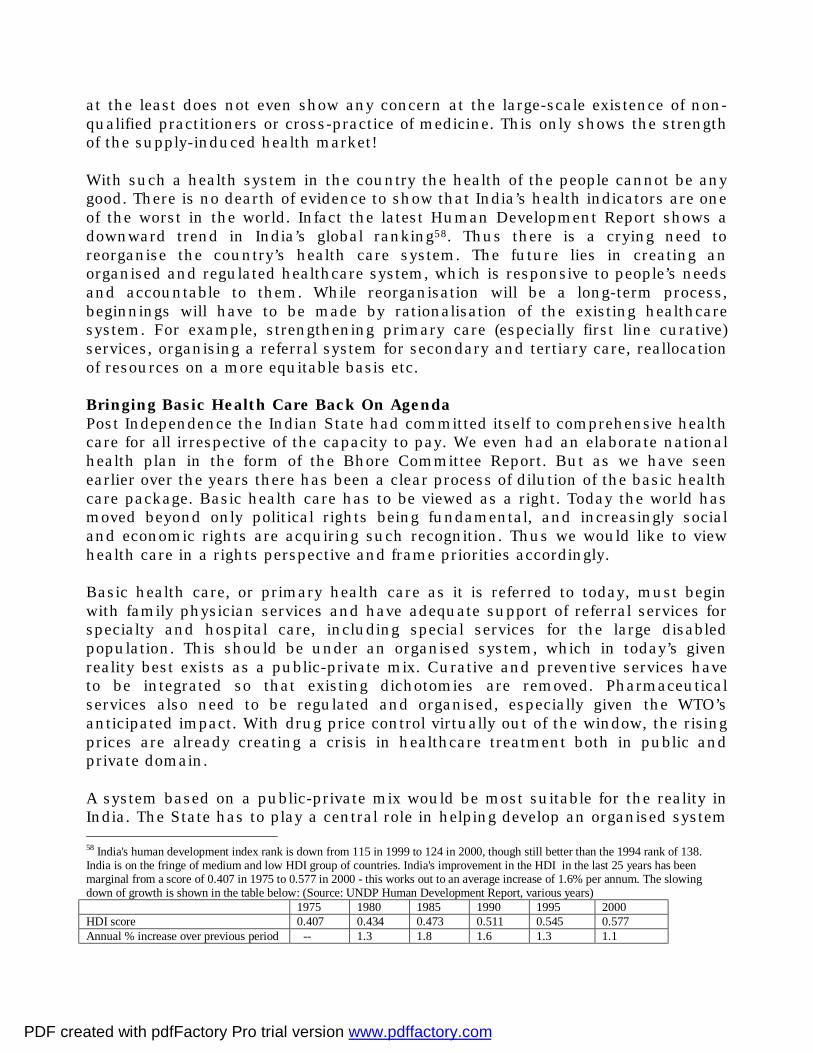
at the least does not even show any concern at the large-scale existence of non-qualified practitioners or cross-practice of medicine. This only shows the strength of the supply-induced health market! With such a health system in the country the health of the people cannot be any good. There is no dearth of evidence to show that India’s health indicators are one of the worst in the world. Infact the latest Human Development Report shows a downward trend in India’s global ranking58. Thus there is a crying need to reorganise the country’s health care system. The future lies in creating an organised and regulated healthcare system, which is responsive to people’s needs and accountable to them. While reorganisation will be a long-term process, beginnings will have to be made by rationalisation of the existing healthcare system. For example, strengthening primary care (especially first line curative) services, organising a referral system for secondary and tertiary care, reallocation of resources on a more equitable basis etc. Bringing Basic Health Care Back On Agenda Post Independence the Indian State had committed itself to comprehensive health care for all irrespective of the capacity to pay. We even had an elaborate national health plan in the form of the Bhore Committee Report. But as we have seen earlier over the years there has been a clear process of dilution of the basic health care package. Basic health care has to be viewed as a right. Today the world has moved beyond only political rights being fundamental, and increasingly social and economic rights are acquiring such recognition. Thus we would like to view health care in a rights perspective and frame priorities accordingly. Basic health care, or primary health care as it is referred to today, must begin with family physician services and have adequate support of referral services for specialty and hospital care, including special services for the large disabled population. This should be under an organised system, which in today’s given reality best exists as a public-private mix. Curative and preventive services have to be integrated so that existing dichotomies are removed. Pharmaceutical services also need to be regulated and organised, especially given the WTO’s anticipated impact. With drug price control virtually out of the window, the rising prices are already creating a crisis in healthcare treatment both in public and private domain. A system based on a public-private mix would be most suitable for the reality in India. The State has to play a central role in helping develop an organised system 58 India's human development index rank is down from 115 in 1999 to 124 in 2000, though still better than the 1994 rank of 138. India is on the fringe of medium and low HDI group of countries. India's improvement in the HDI in the last 25 years has been marginal from a score of 0.407 in 1975 to 0.577 in 2000 - this works out to an average increase of 1.6% per annum. The slowing down of growth is shown in the table below: (Source: UNDP Human Development Report, various years) 1975 1980 1985 1990 1995 2000 HDI score 0.407 0.434 0.473 0.511 0.545 0.577 Annual % increase over previous period -- 1.3 1.8 1.6 1.3 1.1
PDF created with pdfFactory Pro trial version www.pdffactory.com

of health care as against the prevailing laissez-faire approach. The existing health care services will have to be restructured under a defined system and its financing organised and controlled by an autonomous body. To facilitate such restructuring a well defined system of rules and regulations will have to be put in place so that minimum standards and quality care are assured under such a system. There will be a lot of resistance to implementing such a system but it is here that the State will have to demonstrate its guts. Experience across the world shows that wherever near universal access exists, the system is a public-private mix organised under a single umbrella, well regulated and with fiscal control with a monopolistic and autonomous agency or group of agencies. The best examples are Canada, Britain, Sweden, Germany, Costa Rica and South Korea, among others. Public spending on health care is barely 1% of GDP as it stands today. This infact is a decline over earlier years, especially the mid-eighties when it was 1.27% of GDP. Nearly 70% of state spending goes to urban areas, mostly for hospitals. The balance 30% in rural areas is spent mostly on family planning services. Private out-of-pocket expenditures on health care are not available in any organised way. At best estimates can be made based on sample surveys of household expenditures and indirectly by extrapolating on the basis of the strength of the private health sector. It is today estimated to be over 4% of GDP, more than double that of estimates available for the sixties and seventies. A restructured public-private mix would need much less resources. Estimates calculated for the basic health care package, including existing public secondary and tertiary services would cost around 3% of the GDP. This would mean a whopping saving of 40% of what is spent overall now and coupled with much better quality and more effective services. In terms of sharing costs the public share would definitely need to go up and private resources would be channelised through employers, employees and insurance funds. The State would have to raise additional resources through earmarked taxes and cesses for the health sector. This would mean a greater burden on those with capacity to pay but there would be an overall saving of out-of-pocket expenses for all but especially for the poor. Thus the new strategy should focus both on strengthening the state-sector and at the same time also plan for a regulated growth and involvement of the private health sector. There is a need to recognise that the private health sector is huge and has cast its nets, irrespective of quality, far wider than the state-sector health services. Through regulation and involvement of the private health sector an organised public-private mix could be set up which can be used to provide universal and comprehensive care to all. What we are trying to say is that the need of the hour is to look at the entire health care system in unison to evolve
PDF created with pdfFactory Pro trial version www.pdffactory.com

some sort of a national system. The private and public health care services need to be organised under a common umbrella to serve one and all. A framework for basic minimum level of care needs to be spelt out in clear terms and this should be accessible to all without direct cost to the patient at the time of receiving care. Today we are at the threshold of another transition which will probably bring about some of the changes like regulation, price control, quality assurance, rationality in practice etc.. This is the coming of private health insurance that will lay rules of the game for providers to suit its own for-profit motives. While this may improve quality and accountability to some extent it will be of very little help to the poor and the underserved who will anyway not have access to this kind of a system. Worldwide experience shows that private insurance only pushes up costs and serves the interests of the haves. If equity in access to basic health care must remain the goal then the State cannot abdicate its responsibility in the social sectors. The state need not become the primary provider of health care services but this does not mean that it has no stake in the health sector. As long as there are poor the state will have to remain a significant player, and interestingly enough, as the experience of most developed countries show, the state becomes an even stronger player when the number of poor becomes very small!59 While reorganisation of the health sector will take its own time, certain positive changes are possible within the existing setup through macro policy initiatives - the medical councils should be directed at putting their house in order by being strict and vigilant about assuring that only those qualified and registered should practice medicine, continuing medical education (CME) should be compulsory and renewal of registration must be linked to it, medical graduates passing out of public medical schools must put in compulsory public service of atleast five years of which three years must be at PHCs and rural hospitals (this should be assured not through bonds or payments but by providing only a provisional license to do supervised practice in state health care institutions and also by giving the right to pursue postgraduate studies only to those who have completed their three years of rural medical service), regulating the spread of private clinics and hospitals through a strict locational policy whereby the local authority should be given the right to determine how many doctors or how many hospital beds they need in their area (norms for family practice, practitioner : population and bed : population ratios, fiscal incentives for remote and underserved areas and strong disincentives and higher taxes for urban and over-served areas etc.. can be used), regulating the quality of care provided by hospitals and practitioners by setting up minimum standards to be followed, putting in place compulsory health insurance for the organised sector employees (restructuring the existing ESIS and merging it with the common national health care system where each employee has equal rights and cover but contributes as per earning capacity, for example if 59 Data from OECD countries clearly shows that the State is a major player in health financing and over three-fourths of the resources for the health sector in these countries, except USA, comes from the public exchequer; even in the USA it is over 40% but in India the State contributes less than one-fifth, the balance coming out of pocket of households. (OECD, 1990: Health Systems in Transition, Organisation for Economic Cooperation and Development, Paris)
PDF created with pdfFactory Pro trial version www.pdffactory.com

each employee contributes 2% of their earnings and the employer adds another 3% then nearly Rs.100 billion could be raised through this alone), special taxes and cesses for health can be charged to generate additional resources (alcohol, cigarettes, property owners, vehicle owners etc.. are well known targets and something like one percent of sales turnover for the products and a value tax on the asset could bring in substantial resources), allocation of existing resources can be rationalised better through preserving acceptable ratios of salary : non-salary spending and setting up a referral system for secondary and tertiary care. These are only some examples of setting priorities within the existing system for its improvement. However, an organised and universal healthcare system would be possible only under a rights perspective. Right to health and healthcare is a fundamental social and economic right recognised by the International Covenant on Economic Social and Cultural Rights. But such a demand is not on the political agenda in India. The Peoples’ Health Assembly initiative (called Jan Swasthya Abhiyan in India)60 has voiced such a demand but this requires a widespread awareness campaign and participation of many more civil society groups. On the other end of the spectrum the medical profession needs to be educated not only about self-regulation and the need to organise for minimum standards for quality healthcare but also about the benefits of an organised public-private mix healthcare system. Only such an approach can lead us closer towards a system that guarantees universal access. Healthcare will have to be viewed in the context of social security. The latter becomes even more urgent under the changing political economy. To support this, new public management systems and innovations in health financing to raise additional resources will be needed. We are at a stage in history where political will to do something progressive is conspicuous by its absence. We may have constitutional commitments and backing of international law but without political will nothing will happen. To reach the goals of right to health and healthcare discussed above civil society will have to be involved in a very large way and in different ways. The initiative to bring healthcare on the political agenda will have to be a multi-pronged one and fought on different levels. The idea here is not to develop a plan of action but to indicate the various steps and involvements which will be needed
60 The People's Health Campaign is a unique grassroots-to-global movement for 'Health for All’, a campaign for better health. This innovative campaign has been active since July 99, to enquire into the current state of health services and to demand better health care The background to this campaign is a global wake-up call being given to governments around the world, reminding them of their promise and pledge made in 1978 to provide 'Health for All by 2000 AD'. India took the lead in this campaign and over 2000 health, science, womens' and other organisations and NGOs, including 19 national networks, in 20 states are involved in the Peoples Health Assembly (PHA) process.
PDF created with pdfFactory Pro trial version www.pdffactory.com
to build a consensus and struggle for right to healthcare. We make the following suggestions:
• Policy level advocacy for creation of an organized system for universal healthcare
• Research to develop the detailed framework of the organized system • Lobbying with the medical profession to build support for universal
healthcare and regulation of medical practice • Filing a public interest litigation on right to healthcare to create a basis for
constitutional amendment • Lobbying with parliamentarians to demand justiciability of directive
principles • Holding national and regional consultations on right to healthcare with
involvement of a wide array of civil society groups • Running campaigns on right to healthcare with networks of peoples
organizations at the national and regional level • Bringing right to healthcare on the agenda of political parties to incorporate
it in their manifestoes • Pressurizing international bodies like WHO, Committee of ESCR, UNCHR,
as well as national bodies like NHRC, NCW to do effective monitoring of India’s state obligations and demand accountability
• Preparing and circulating widely shadow reports on right to healthcare to create international pressure
The above is not an exhaustive list. The basic idea is that there should be widespread dialogue, awareness raising, research, documentation and legal/constitutional discourse. To conclude, it is evident that the neglect of the public health system is an issue larger than government policy making. The latter is the function of the overall political economy. Under capitalism only a well-developed welfare state can meet the basic needs of its population. Given the backwardness of India the demand of public resources for the productive sectors of the economy (which directly benefit capital accumulation) is more urgent (from the business perspective) than the social sectors, hence the latter get only a residual attention by the state. The policy route to comprehensive and universal healthcare has failed miserably. It is now time to change gears towards a rights-based approach. The opportunity exists in the form of constitutional provisions and discourse, international laws to which India is a party, and the potential of mobilizing civil society and creating a socio-political consensus on right to healthcare. There are a lot of small efforts towards this end all over the country. Synergies have to be created for these efforts to multiply so that people of India can enjoy right to health and healthcare.61
61 Duggal, Ravi: Health and Development in India – Moving Towards Right to Healthcare, Draft paper for Harvard School of Public Health initiative on Right to Development, 2002
PDF created with pdfFactory Pro trial version www.pdffactory.com

Table 1: HEALTH AND HEALTHCARE DEVELOPMENT IN INDIA 1951-2000
1951 1961 1971 1981 1991 1995 1996 1997 1998 2000
1 Hospitals Total 2694 3054 3862 6805 11174 15097 15170 15188 17,000 % Rural 39 34 32 27 31 34 34 %Private 43 57 68 68 68
2 Hospital & dispensary beds
Total 117000 229634 348655 504538 806409 849431 892738 896767 1,000000
% Rural 23 22 21 17 20 23 23 %Private 28 32 36 37 37
3 Dispensaries 6600 9406 12180 16745 27431 28225 25653 25670 % Rural 79 80 78 69 43 41 40 % Private 13 60 61 57 56
4 PHCs 725 2695 5131 5568 22243 21693 21917 22446 23179 24,000 5 Sub-centres 27929 51192 131098 131900 134931 136379 137006 140,000
6 Doctors Allopaths 60840 83070 153000 266140 395600 459670 475780 492634 503947 550,000
All Systems 156000 184606 450000 665340 920000 1080173 1133470 1,250000 7 Nurses 16550 35584 80620 150399 311235 562966 565700 607376 700,000
8 Medical colleges Allopathy 30 60 98 111 128 165 165 165 170 9 Out turn Grads 1600 3400 10400 12170 13934 * * * * 20,000
P. Grads 397 1396 3833 3139 3656 5,000
10 Pharmaceutical production
Rs. in billion 0.2 0.8 3 14.3 38.4 79.4 91.3 104.9 120.7 165.0
11 Health outcomes IMR/000 134 146 138 110 80 74/69 72 71 72 70
CBR/000 41.7 41.2 37.2 33.9 29.5 29 27 27 27 26 CDR/000 22.8 19 15 12.5 9.8 10 9 8.9 9 8.7 Life Expectancy years 32.08 41.22 45.55 54.4 59.4 62 62.4 63.5 64 65 Births attended by
trained practitioners Percent 18.5 21.9 28.5 42.3
12 Health Expenditure Rs. Billion
Public Private@
CSO estimate pvt.
0.22 1.05
1.08 3.04 2.05
3.35 8.15 6.18
12.86 43.82 29.70
50.78 173.60
82.61
82.17 233.47 279.00
101.65
329.00
113.13 399.84 373.00
126.27
459.00
178.00
833.00 Health Expenditure
as percent of GDP Public
Private CSO 0.25 0.71
1.34 0.84 1.56
1.05 2.43
0.92 1.73
0.95 3.25
0.91 2.95
0.88 2.94
0.81 2.98
0.87 4.07
Health Expenditure as % to Govt. Total
Public 2.69 5.13 3.84 3.29 2.88 2.13 2.98 2.94 2.7 2.9
@ Data from - 1951:NSS 1st Round 1949-50; 1961: SC Seals All India District Surveys,1958; 1971: NSS 28th Round 1973-74; 1981: NSS 42nd Round 1987; 1991 and 1995: NCAER – 1990; 1995: NSS 52nd Round 1995-96; 1997: CEHAT 1996-97 (Madhiwala et.al. 2000) *Data available is grossly under-reported, hence not included Notes: The data on hospitals, dispensaries and beds are underestimates, especially for the private sector because of under-reporting. Rounded figures for year 2000 are rough estimates. Source : 1. Health Statistics / Information of India, CBHI, GOI, various years; 2. Census of India Economic Tables, 1961, 1971, 1981, GOI 3.OPPI Bulletins and Annual reports of Min. of Chemicals and Fertilisers for data on Pharmaceutical Production 4. Finance Accounts of Central and State Governments, various years 5. National Accounts Statistics, CSO, GOI, various years 6. Statistical Abstract of India, GOI, various years 7. Sample Registration System - Statistical Reports, various years 8. NFHS - 2, India Report, IIPS, 2000
PDF created with pdfFactory Pro trial version www.pdffactory.com
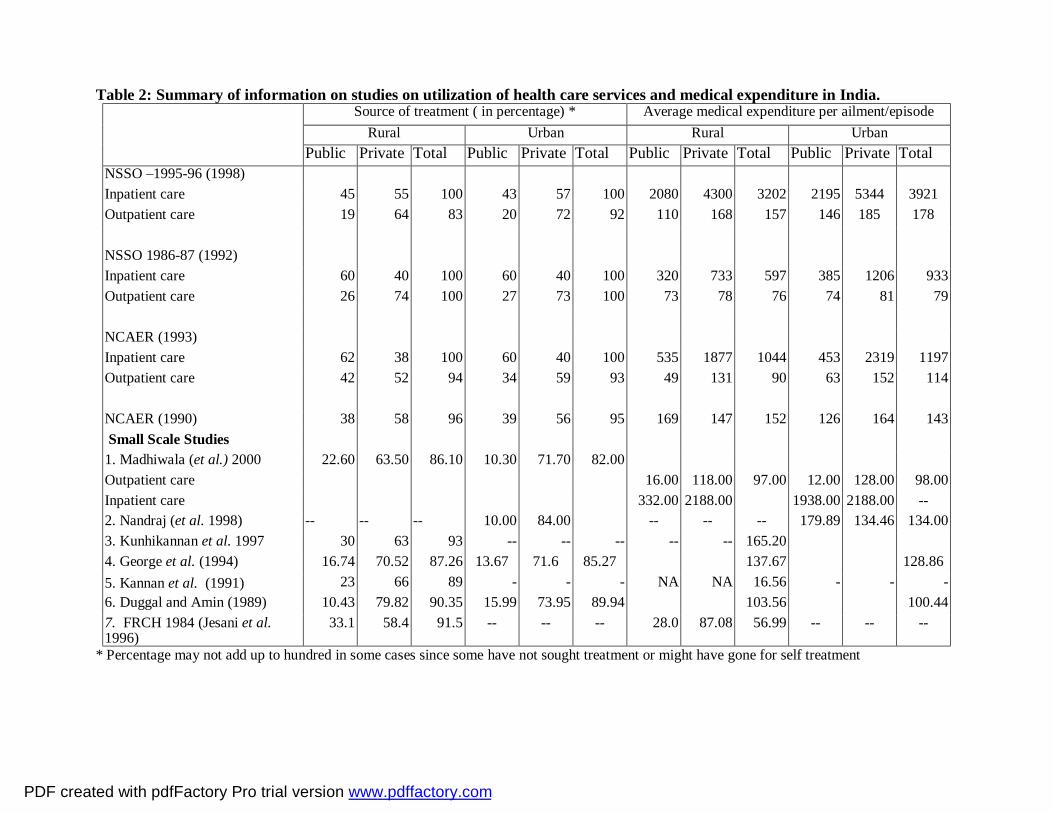
Table 2: Summary of information on studies on utilization of health care services and medical expenditure in India. Source of treatment ( in percentage) * Average medical expenditure per ailment/episode Rural Urban Rural Urban Public Private Total Public Private Total Public Private Total Public Private Total
NSSO –1995-96 (1998) Inpatient care 45 55 100 43 57 100 2080 4300 3202 2195 5344 3921 Outpatient care 19 64 83 20 72 92 110 168 157 146 185 178 NSSO 1986-87 (1992) Inpatient care 60 40 100 60 40 100 320 733 597 385 1206 933 Outpatient care 26 74 100 27 73 100 73 78 76 74 81 79 NCAER (1993) Inpatient care 62 38 100 60 40 100 535 1877 1044 453 2319 1197 Outpatient care 42 52 94 34 59 93 49 131 90 63 152 114 NCAER (1990) 38 58 96 39 56 95 169 147 152 126 164 143 Small Scale Studies 1. Madhiwala (et al.) 2000 22.60 63.50 86.10 10.30 71.70 82.00 Outpatient care 16.00 118.00 97.00 12.00 128.00 98.00 Inpatient care 332.00 2188.00 1938.00 2188.00 -- 2. Nandraj (et al. 1998) -- -- -- 10.00 84.00 -- -- -- 179.89 134.46 134.00 3. Kunhikannan et al. 1997 30 63 93 -- -- -- -- -- 165.20 4. George et al. (1994) 16.74 70.52 87.26 13.67 71.6 85.27 137.67 128.86 5. Kannan et al. (1991) 23 66 89 - - - NA NA 16.56 - - - 6. Duggal and Amin (1989) 10.43 79.82 90.35 15.99 73.95 89.94 103.56 100.44 7. FRCH 1984 (Jesani et al. 1996)
33.1 58.4 91.5 -- -- -- 28.0 87.08 56.99 -- -- --
* Percentage may not add up to hundred in some cases since some have not sought treatment or might have gone for self treatment
PDF created with pdfFactory Pro trial version www.pdffactory.com
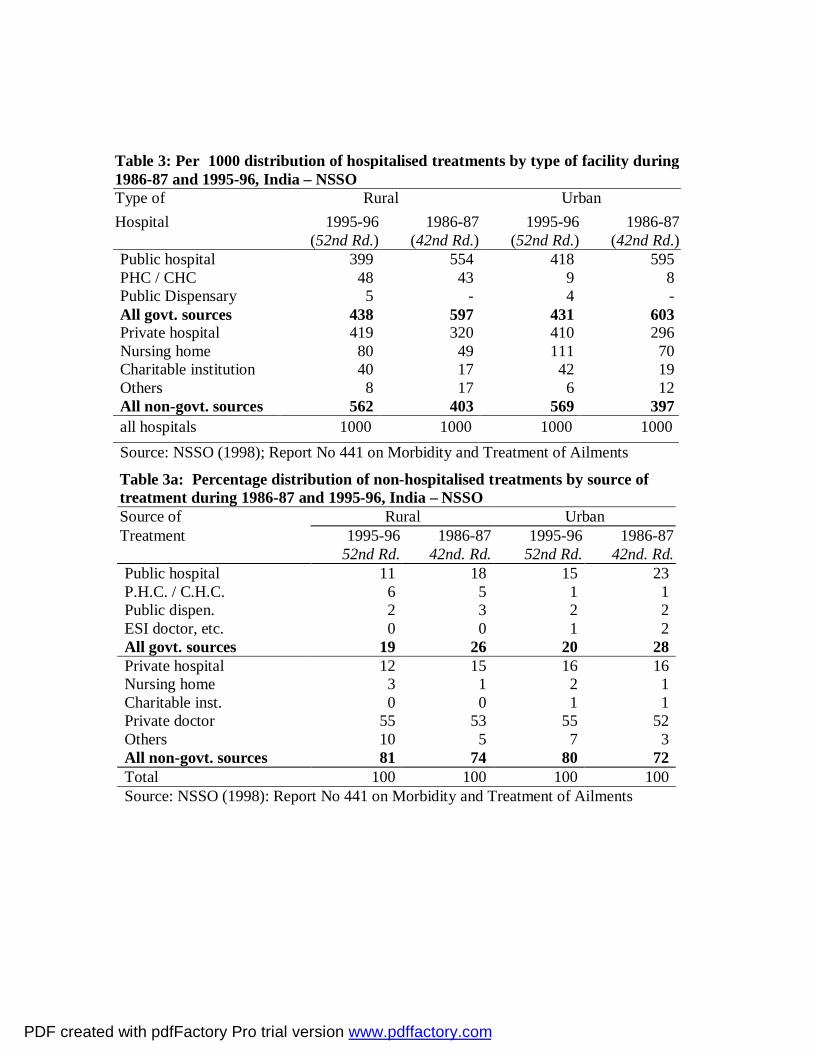
Table 3a: Percentage distribution of non-hospitalised treatments by source of treatment during 1986-87 and 1995-96, India – NSSO Source of Rural Urban Treatment 1995-96
52nd Rd. 1986-87
42nd. Rd. 1995-96
52nd Rd. 1986-87
42nd. Rd. Public hospital 11 18 15 23 P.H.C. / C.H.C. 6 5 1 1 Public dispen. 2 3 2 2 ESI doctor, etc. 0 0 1 2 All govt. sources 19 26 20 28 Private hospital 12 15 16 16 Nursing home 3 1 2 1 Charitable inst. 0 0 1 1 Private doctor 55 53 55 52 Others 10 5 7 3 All non-govt. sources 81 74 80 72 Total 100 100 100 100 Source: NSSO (1998): Report No 441 on Morbidity and Treatment of Ailments
Table 3: Per 1000 distribution of hospitalised treatments by type of facility during 1986-87 and 1995-96, India – NSSO Type of Rural Urban Hospital 1995-96
(52nd Rd.) 1986-87
(42nd Rd.) 1995-96
(52nd Rd.) 1986-87
(42nd Rd.) Public hospital 399 554 418 595 PHC / CHC 48 43 9 8 Public Dispensary 5 - 4 - All govt. sources 438 597 431 603 Private hospital 419 320 410 296 Nursing home 80 49 111 70 Charitable institution 40 17 42 19 Others 8 17 6 12 All non-govt. sources 562 403 569 397 all hospitals 1000 1000 1000 1000 Source: NSSO (1998); Report No 441 on Morbidity and Treatment of Ailments
PDF created with pdfFactory Pro trial version www.pdffactory.com

Table 4: Ministry Of Health And Family Welfare Expenditures 1991-2000 CATEGORY 1990-91 1991-92 1992-93 1993-94 1994-
95 1995-96 1996-97 1997-98 1998-99
RE 1999-00 BE
Total 5078 5639 6464 7518 8217 10165 11313 12627 16303 17854 Central 493 558 705 744 1068 1210 1346 1354 1907 2309
All India Health expenditure at current prices in Rs. crores
State 4585 5081 5759 6774 7149 8955 9967 11273 14396 15545 Health expenditure at 1981-82 prices in Rs. crores
2775 2711 2822 3031 2988 3434 3591 3826 4631 4891
Real Growth Rate of health Expenditure %
-2.3 4.1 7.4 -1.4 14.9 4.6 6.5 21 5.6
Share of state govt. in total Health expenditure %
90.3 90.1 89.1 90.1 87.0 88.1 88.1 89.3 88.3 87.1
Grant in Aid component from Centre in state Health expenditure %
17.0 16.2 18.9 20.7 18.8 14.8 14.1 15.6 16.1
Health expenditure to total govt. expenditure %
2.88 3.11 2.88 2.91 2.13 2.98 2.94 2.7 2.9 3.0
Health expenditure as % of GDP 0.94 0.91 0.91 0.93 0.85 0.91 0.88 0.81 0.86 0.87
Percapita health expenditure in Rs./year 60.02 65.34 73.45 83.90 89.9 109.07 119.08 130.3 165.0 177.3
Source: Budget Papers of the Union Government; The RBI Bulletin; (various years)
PDF created with pdfFactory Pro trial version www.pdffactory.com
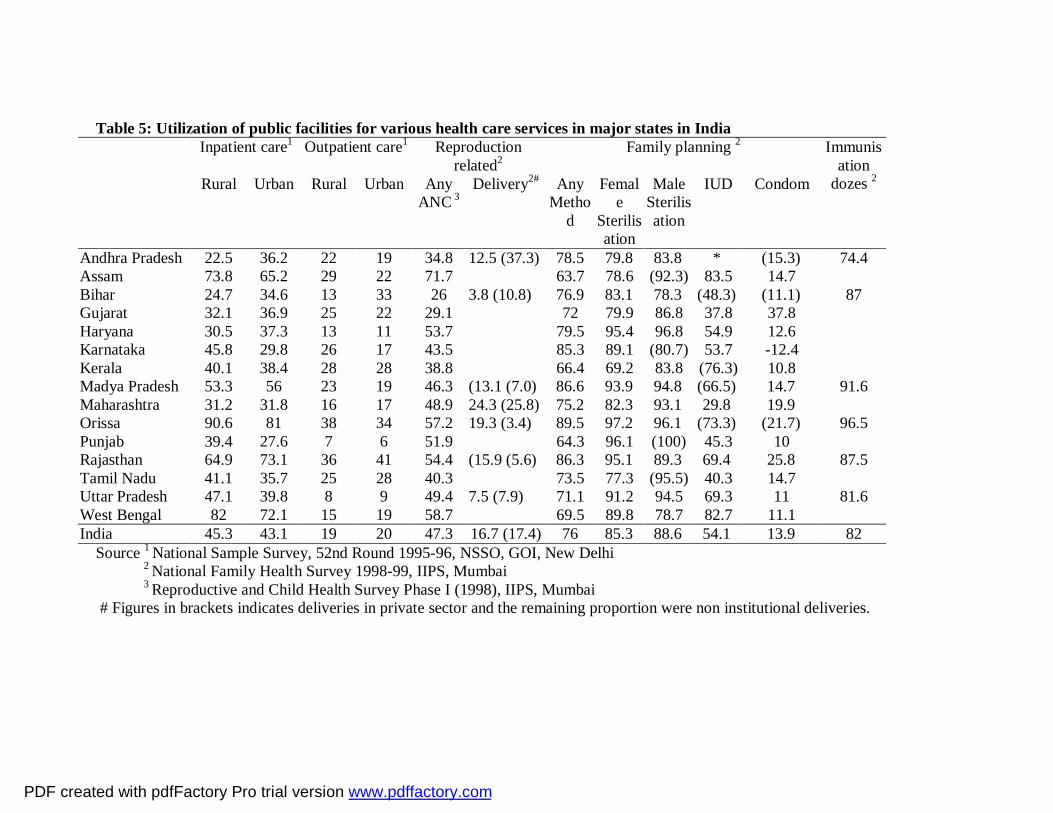
Table 5: Utilization of public facilities for various health care services in major states in India Inpatient care1 Outpatient care1 Reproduction
related2 Family planning 2
Rural Urban Rural Urban Any ANC 3
Delivery2# Any Metho
d
Female
Sterilisation
Male Sterilisation
IUD Condom
Immunisation
dozes 2
Andhra Pradesh 22.5 36.2 22 19 34.8 12.5 (37.3) 78.5 79.8 83.8 * (15.3) 74.4 Assam 73.8 65.2 29 22 71.7 63.7 78.6 (92.3) 83.5 14.7 Bihar 24.7 34.6 13 33 26 3.8 (10.8) 76.9 83.1 78.3 (48.3) (11.1) 87 Gujarat 32.1 36.9 25 22 29.1 72 79.9 86.8 37.8 37.8 Haryana 30.5 37.3 13 11 53.7 79.5 95.4 96.8 54.9 12.6 Karnataka 45.8 29.8 26 17 43.5 85.3 89.1 (80.7) 53.7 -12.4 Kerala 40.1 38.4 28 28 38.8 66.4 69.2 83.8 (76.3) 10.8 Madya Pradesh 53.3 56 23 19 46.3 (13.1 (7.0) 86.6 93.9 94.8 (66.5) 14.7 91.6 Maharashtra 31.2 31.8 16 17 48.9 24.3 (25.8) 75.2 82.3 93.1 29.8 19.9 Orissa 90.6 81 38 34 57.2 19.3 (3.4) 89.5 97.2 96.1 (73.3) (21.7) 96.5 Punjab 39.4 27.6 7 6 51.9 64.3 96.1 (100) 45.3 10 Rajasthan 64.9 73.1 36 41 54.4 (15.9 (5.6) 86.3 95.1 89.3 69.4 25.8 87.5 Tamil Nadu 41.1 35.7 25 28 40.3 73.5 77.3 (95.5) 40.3 14.7 Uttar Pradesh 47.1 39.8 8 9 49.4 7.5 (7.9) 71.1 91.2 94.5 69.3 11 81.6 West Bengal 82 72.1 15 19 58.7 69.5 89.8 78.7 82.7 11.1 India 45.3 43.1 19 20 47.3 16.7 (17.4) 76 85.3 88.6 54.1 13.9 82
Source 1 National Sample Survey, 52nd Round 1995-96, NSSO, GOI, New Delhi 2 National Family Health Survey 1998-99, IIPS, Mumbai 3 Reproductive and Child Health Survey Phase I (1998), IIPS, Mumbai # Figures in brackets indicates deliveries in private sector and the remaining proportion were non institutional deliveries.
PDF created with pdfFactory Pro trial version www.pdffactory.com

Table 6: Coverage of Selected Preventive/Promotive Health Programs Activity Urban Rural All 1. Completed Vaccinations
60.5 36.6 42.0
2. BCG 86.8 67.1 71.6 3. DPT-3 73.4 49.8 55.1 4. Polio – 3 78.2 58.3 62.8 5. Measles 69.2 45.3 50.7 6. No vaccinations dozes
6.4 16.7 14.4
7.ANC 86.4 60.2 66.0 8. TT 2+ (ANC) 81.9 62.5 66.8 9. Iron Folic Acid 75.7 52.5 57.6 Note: Vaccinations for children aged 12-23 months Source: National Family Health Survey 1998-99, IIPS, Mumbai
PDF created with pdfFactory Pro trial version www.pdffactory.com

Table 7: Per 1000 distribution of treatments (not treated as an inpatient of hospital) during the last 15 days by source of treatment for each fractile-group of m p c e and social group, India, 1995-96.
Type of m .p c e f r a c t i l e g r o u p social group Total Hospital 0 -
10 10 - 20
20 - 40
40– 60
60 - 80
80 - 90
90 – 100
S t. s.c. others
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) Rural
Public hospital 78 101 75 100 121 101 109 115 106 97 101 p.h.c 118 49 69 46 50 47 21 111 40 49 52 Public dispensary 9 15 17 19 14 51 11 44 9 20 19 Private hospital 71 95 88 77 121 122 167 113 94 115 110 Nursing home 36 39 38 23 16 17 17 63 21 21 24 Charitable inst. 1 3 3 2 3 3 7 2 3 4 3 ESI doct/ AMA etc 5 1 5 1 2 3 2 5 4 2 3 Private doctor 406 476 487 510 485 486 504 320 507 499 488 Others 123 106 97 82 82 73 65 127 77 83 85 NR 153 115 118 141 106 96 96 100 139 109 115 Total 1000 1000 1000 1000 1000 1000 1000 1000 1000 1000 1000
Urban Public hospital 199 161 141 135 155 105 90 211 170 128 136 p.h.c 9 5 13 7 8 3 2 14 9 6 7 Public dispensary 13 13 18 13 20 11 7 9 19 14 14 Private hospital 106 150 145 156 139 151 138 131 122 147 143 Nursing home 42 36 20 19 21 16 19 11 13 24 22 Charitable inst. 26 4 9 4 9 4 5 0 13 7 8 ESI doct/ AMA etc 2 7 6 12 12 11 7 3 6 10 9 Private doctor 409 492 490 500 504 567 510 423 497 506 502 Others 104 65 63 81 54 66 51 67 76 65 66 NR 90 67 94 73 77 65 171 130 76 93 91 Total 1000 1000 1000 1000 1000 1000 1000 1000 1000 1000 1000 Source: NSSO (1998): Report No 441 on Morbidity and Treatment of Ailments
PDF created with pdfFactory Pro trial version www.pdffactory.com

Table 8 : Per 1000 distribution of hospitalisation cases during last 365 days by fractile-group of mpce and social group for each facility, India 1995-96.
Type of m .p c e f r a c t i l e g r o u p social group Total Hospital 0 -
10 10 - 20
20 - 40
40– 60
60 - 80
80 - 90
90 – 100
S t. s.c. Others
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) Rural
Public hospital 27 55 149 164 227 146 231 84 243 672 1000 p.h.c 56 61 209 216 258 100 100 150 252 594 1000 Public dispensary 11 73 143 136 244 176 217 82 291 628 1000 Private hospital 19 20 69 106 217 182 388 40 160 800 1000 Nursing home 20 26 107 158 228 166 295 19 205 775 1000 Charitable inst. 37 74 112 198 197 122 260 63 259 677 1000 Others 26 25 71 153 383 246 97 54 147 798 1000 any hospital 25 39 113 141 233 157 293 63 203 733 1000
Urban Public hospital 94 95 191 204 195 98 123 41 185 773 1000 P.H.C 179 97 226 201 119 43 134 99 209 692 1000 Public dispensary 113 30 210 140 279 166 61 - 280 720 1000 Private hospital 36 40 129 177 205 165 248 23 100 877 1000 Nursing home 17 50 119 166 209 168 271 21 112 867 1000 Charitable inst. 29 45 129 163 264 148 221 28 141 830 1000 Others 18 151 213 178 196 80 164 3 277 720 1000 any hospital 59 65 155 189 203 134 194 31 141 827 1000 Source: NSSO (1998): Report No 441 on Morbidity and Treatment of Ailments
PDF created with pdfFactory Pro trial version www.pdffactory.com
References for Tables 1 and 2 Duggal, Ravi and S Amin, 1989 : Cost of Health Care, Foundation for Research in Community Health, Bombay George, Alex et.al., 1992 : Household Health Expenditure in Madhya Pradesh, FRCH, Bombay Jesani, Duggal, & Gupte, 1996 – NGOs in Rural Health Care, FRCH, Pune Kannan KP et.al., 1991 : Health and Development in Rural Kerala, Kerala Shastra Sahitya Parishad, Trivandrum Kunhikannan et al.1999: Changes in the Health Status of Kerala 1987-1997, KSSP, Thiruvananthapuram Madhiwala, Neha et.al., 2000: Health, Households and Women’s Lives, CEHAT, Mumbai NCAER – 1990- all India: NCAER – Household survey of Medical Care, NCAER, New Delhi, 1992 NCAER 1995: Household Survey of Health Care Utilisation and Expenditure Working paper No. 53, New Delhi NSSO -1987 : Morbidity and Utilisation of Medical Services, 42nd Round, Report No. 384, National Sample Survey Organisation, New Delhi, 1990 NSSO -1996 : Report No. 441 – 52nd Round, NSSO, New Delhi ,1998
PDF created with pdfFactory Pro trial version www.pdffactory.com









![RAVI COLTRANE: QUARTET – Contract Rider: Quartet: Ravi ...P... · RAVI COLTRANE: QUARTET – Contract Rider: [Current: May 2012] Quartet: Ravi Coltrane (Saxophone) + Guitar, Bass,](https://img.pdfslide.us/doc/110x75/5ab9fb537f8b9a28468eab6a/ravi-coltrane-quartet-contract-rider-quartet-ravi-pravi-coltrane.jpg)




















