Embed Size (px)
Citation preview

A Very Early Rehabilitation Trial (AVERT):
What we know, what we think and what’s
to come
The AVERT Trial Collaboration group
Joshua Kwant, Blinded Assessor
17th May 2016
NIMAST

Disclosure
• Nothing to disclose

AVERT: A pragmatic, ‘real world’ trial
Design International, multicentre, parallel group, randomised controlled trial testing efficacy and safety of a very early (<24h) frequent, higher dose out of bed (very early mobilisation) protocol compared to usual care post stroke.
Protocol Bernhardt IJS 2006; Bernhardt IJS 2015 SAP
Clinical hypotheses
1. Improve functional outcome (mRS 0-2) at 3 months 2. Lead to fewer immobility complications at 3 months post stroke 3. Lead to more patients regaining the ability to walk early 4. Improve quality of life at 12 months 5. Be cost effective
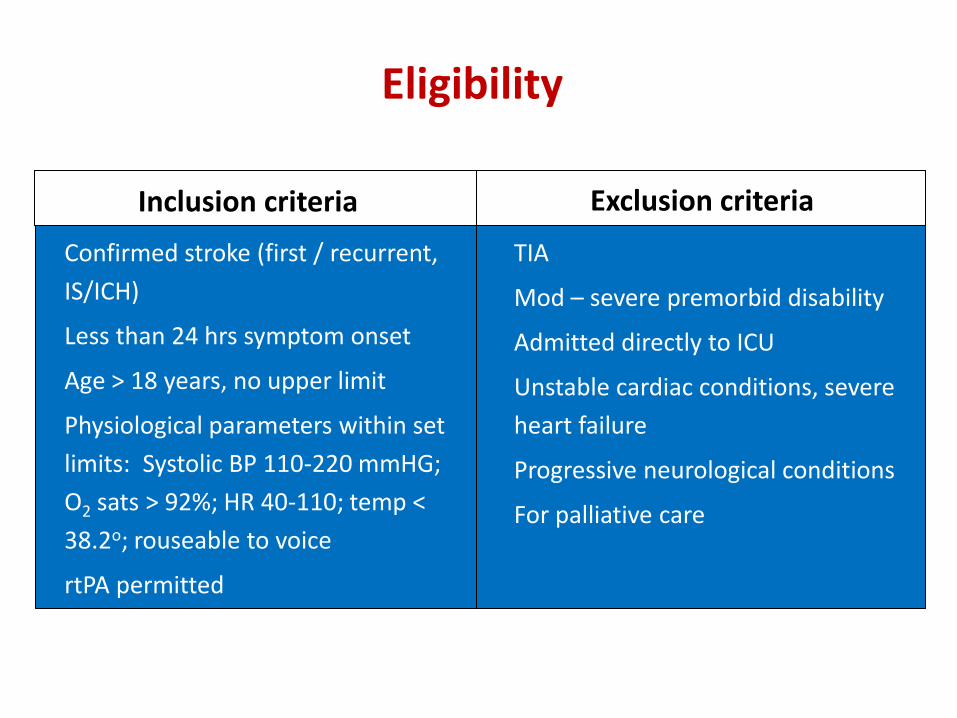
Eligibility
Confirmed stroke (first / recurrent,
IS/ICH)
Less than 24 hrs symptom onset
Age > 18 years, no upper limit
Physiological parameters within set
limits: Systolic BP 110-220 mmHG;
O2 sats > 92%; HR 40-110; temp <
38.2o; rouseable to voice
rtPA permitted
TIA
Mod – severe premorbid disability
Admitted directly to ICU
Unstable cardiac conditions, severe
heart failure
Progressive neurological conditions
For palliative care
Inclusion criteria Exclusion criteria

What was Very Early Mobilisation (VEM)?
• Out of bed, sitting, standing and walking, task specific activity – guided by a detailed protocol
• VEM had 4 levels of intervention, dependant on functional ability and adjusted or with recovery
Rehabilitation treatment package: 1) Time to first mobilisation, 2) frequency per day, 3) amount per day
Sitting out of bed: resting time in/out of bed not measured What VEM was not
With intervention monitoring we achieved significant differences between groups in each of the criteria: time, frequency, amount

Trial pathway
Stroke
Stratified by
stroke severity & site
Arrive hospital, screened, recruited <
24 hrs
12 month Ax
Very Early Mobilisation + Usual Care
First intervention, < 24 hrs PT /Nurse team, 6 days/wk
3 month Ax 1o outcome
1o Efficacy endpoint Favourable outcome (mRS 0-2)
Safety outcomes: death, SAEs, immobility, neurological
Day 14 Treatment ceases
Usual stroke unit care
Sample size, n=2104
3+ additional sessions out of bed activity

Key elements of Protocol
• commenced within 24 hours
• focus on ‘out of bed’ mobilisation activities, and
• provided at least three additional (to UC) out of bed sessions per day
• Continued for 14 days or until discharge from stroke unit care
Visit by blinded assessor or telephone to assess: • mRS • SAEs
• Barthel Index
• Rivermead
• Irritability, depression and anxiety (IDA) scale
• Assessment of Quality of Life (AQoL)
• Montreal Cognitive Assessment (MoCA)
• Comprehensive cost questionnaire

Methods: Key analyses
Efficacy Primary: Favourable outcome mRS 0-2 Secondary: Assumption free ordinal shift analysis Time to walking unassisted 50 metres Exploratory: Subgroups – age (<65; 65–79; >80), stroke severity (mild: NIHSS<7; moderate: 8–16; and severe: >16), stroke type (infarct, haemorrhage), rtPA, time to first mobilisation (<12 h; 12–24 h; >24 h)
Safety Death at 3 months Serious adverse events with separate review of immobility-related, neurological
Dose of intervention (time to start, frequency, amount) Change in dose over time
Bernhardt IJS 2015 Statistical Analysis Plan

25,237 admitted <24 hours of stroke onset
1054 very early mobilisation
23,133 ineligible 5588 premorbid mRS>2 1136 other clinical trial 7080 medically unstable/unwell 7414 no recruiter/weekend 8151 other exclusion reason 446 refused
2104 enrolled
12 never mobilised 21 not stroke
2104 randomised
1050 usual care
14 never mobilised 13 not stroke
1038 assessed at 3 months 950 alive 88 dead
6 unknown 10 refused follow up
1045 assessed at 3 months 973 alive 72 dead
5 refused follow up
1054 included in intention-to-treat primary analysis
1050 included in intention-to-treat primary analysis
Figure 1: Trial profile
Trial Performance
56 sites 5 countries: Australia New Zealand Malaysia Singapore UK
July 06 – October 14
Follow up complete in
2083 patients (99%)
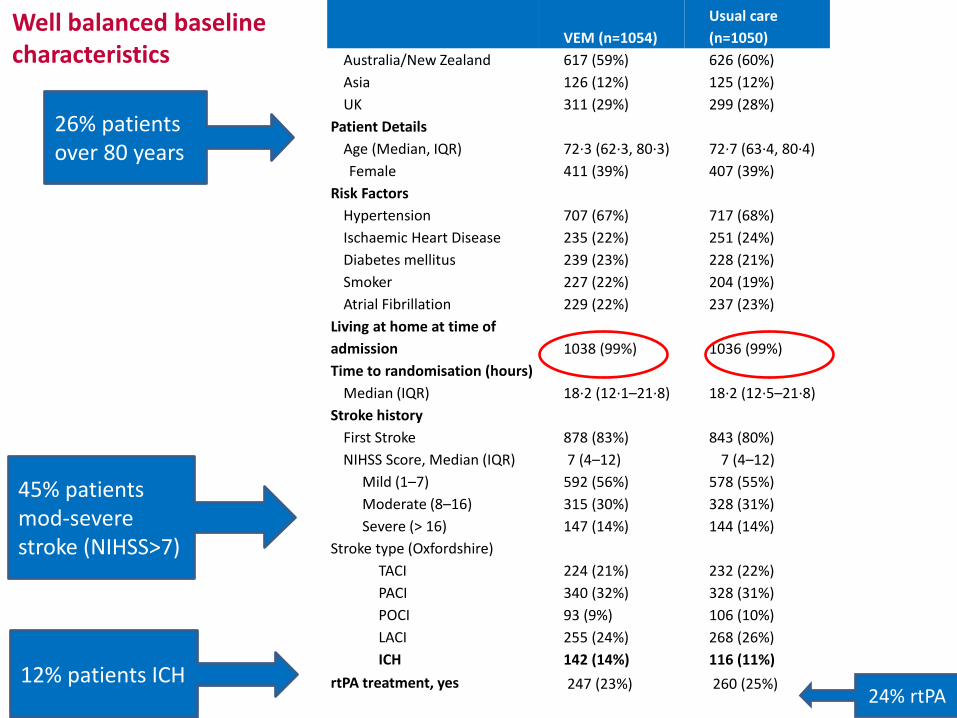
VEM (n=1054)
Usual care
(n=1050)
Australia/New Zealand 617 (59%) 626 (60%)
Asia 126 (12%) 125 (12%)
UK 311 (29%) 299 (28%)
Patient Details
Age (Median, IQR) 72·3 (62·3, 80·3) 72·7 (63·4, 80·4)
Female 411 (39%) 407 (39%)
Risk Factors
Hypertension 707 (67%) 717 (68%)
Ischaemic Heart Disease 235 (22%) 251 (24%)
Diabetes mellitus 239 (23%) 228 (21%)
Smoker 227 (22%) 204 (19%)
Atrial Fibrillation 229 (22%) 237 (23%)
Living at home at time of
admission 1038 (99%) 1036 (99%)
Time to randomisation (hours)
Median (IQR) 18·2 (12·1–21·8) 18·2 (12·5–21·8)
Stroke history
First Stroke 878 (83%) 843 (80%)
NIHSS Score, Median (IQR) 7 (4–12) 7 (4–12)
Mild (1–7) 592 (56%) 578 (55%)
Moderate (8–16) 315 (30%) 328 (31%)
Severe (> 16) 147 (14%) 144 (14%)
Stroke type (Oxfordshire)
TACI 224 (21%) 232 (22%)
PACI 340 (32%) 328 (31%)
POCI 93 (9%) 106 (10%)
LACI 255 (24%) 268 (26%)
ICH 142 (14%) 116 (11%)
rtPA treatment, yes 247 (23%) 260 (25%)
Well balanced baseline characteristics
26% patients over 80 years
45% patients mod-severe stroke (NIHSS>7)
12% patients ICH 24% rtPA

Intervention achieved significant differences
VEM Usual Care
median, IQR n=1054 n=1050 p value
median shift (95%
CI)
Time to first mobilisation
(hrs) 18·5 (12·8–22·3) 22·4 (16·5–29·3)
<0·000
1 4·8 (4·1–5·7)
n=1042;
missing=12
n=1036;
missing=14
Frequency per person
(median daily sessions
of out of bed activity)
6·5 (4·0–9·5) 3 (2·0–4·5) <0·000
1 3 (3–3·5)
Daily amount per
person*
(median minutes per day
spent in out of bed activity)
31 (16·5–50·5) 10 (0–18) <0·000
1 21·0 (20–22·5)
Total amount per person
(mins over the intervention
period)
201·5 (108–340) 70 (32–130) <0·000
1 117 (107–128) * Minutes derived from physiotherapy data only
Time reduced by 28mins/year 95% CI 11·3–44·6, p=0·001
75% of all patients started out of bed activity <24 hours

9.2
8.7
19.5
19.3
21.5
18.2
20.9
22.9
12.2
13.5
9.9
8.8
6.9
8.4
Usual care
VEM
mRS=0 mRS=1 mRS=2 mRS=3 mRS=4 mRS=5 mRS=6
Favourable outcome (mRS 0-2)
480, 46%
525, 50%
OR 0.73, 95% CI 0.59–0.90, p=0.004
VEM
Usual care

9.2
8.7
19.5
19.3
21.5
18.2
20.9
22.9
12.2
13.5
9.9
8.8
6.9
8.4
Usual care
VEM
mRS=0 mRS=1 mRS=2 mRS=3 mRS=4 mRS=5 mRS=6
Assumption free ordinal analysis (GenOR 0.94, 95% CI 0.85–1.03, p=0.193)
Favourable outcome (mRS 0-2)

Time to walking 50 metres unassisted
0.0
00.2
50.5
00.7
51.0
0
1051 342 263 215 198 0VEM:
1049 359 276 231 200 0Usual care:
Number at risk
0 20 40 60 80 100Analysis time
Usual care VEM
Kaplan-Meier failure estimates
Days post stroke
Number of patients who had not achieved walking
Pro
po
rtio
n w
alk
ing
50
m u
nas
sis
ted
VEM Usual care
HR 1.04 95%CI0.94-1.15, p=0.459

UK
AUST/NZ
ASIA
Recruitment Region
>24h
12-24h
<12h
Time to firs t mobilisation
Yes
No
rtPA treated
Haemorrhage
Infarct
Stroke Type
Severe
Mod
Mild
Stroke Severity
>80
65-80
<65
Age
Subgroup
601
1238
244
515
1194
374
503
1580
255
1828
291
635
1157
545
924
614
pts
No.
0.74 (0.51, 1.08)
0.73 (0.55, 0.96)
0.74 (0.40, 1.35)
0.78 (0.42, 1.43)
0.56 (0.42, 0.75)
1.02 (0.62, 1.68)
0.71 (0.46, 1.09)
0.74 (0.58, 0.94)
0.48 (0.25, 0.92)
0.77 (0.62, 0.97)
0.35 (0.11, 1.18)
0.76 (0.53, 1.08)
0.75 (0.57, 0.98)
0.76 (0.50, 1.14)
0.70 (0.52, 0.96)
0.74 (0.49, 1.11)
exp(b) (95% CI)
1 2.5 4.25 8.125
Favours UC Favours VEM
n OR
Favours Usual care Favours VEM
Outcome by subgroup (mRS 0-2)
No significant treatment by group interactions p>0.05

Safety VEM Usual Care Analysis
n (%) n (%) (Adjusted baseline NIHSS, age)
N=1048 N=1050 OR (95% CI) p value
Death
88 (8·4%)
72 (6·9%) 1·34 (0·93–1·93) 0·113
Non-fatal SAEs IRR (95% CI) p value
None 853 (80·9%) 842 (80·2%)
0·88 (0·72–1·07) 0·194
1 157 (14·9%) 146 (13·9%)
2 32 (3·0%) 41 (3·9%)
3 10 (1·0%) 16 (1·5%)
4 2 (0·2%) 4 (0·4%)
5 0 (0%) 1 (0·1%)
Immobility SAEs
None 1000 (94·9%) 997 (95·0%)
0·92 (0·62–1·35) 0·665 1 50 (4·7%) 46 (4·4%)
2 4 (0·4%) 5 (0·5%)
3 0 (0%) 2 (0·2%)
≥4 0 (0%) 0 (0%)
Neurological SAEs
None 947 (89·9%) 967 (92·1%)
1·26 (0·95–1·66) 0·108 1 104 (9·9%) 78 (7·4%)
2 3 (0·3%) 4 (0·4%)
3 1 (0·1%) 1 (0·1%)
4 0 (0%) 0 (0%)
Main causes of death (64% of total) VEM UC Stroke progression 31 19 Pneumonia 19 15 Recurrent stroke 11 7

What ‘dose’ of mobilisation improves
outcome?
Pre-specified dose response analysis
of A Very Early Rehabilitation Trial
Julie Bernhardt, Leonid Churilov, Richard Lindley, Peter
Langhorne, Helen Dewey, Amanda Thrift, Marjorie Moodie,
Geoffrey Donnan on behalf of The AVERT Trial
Collaboration group
@AVERTtrial

Bernhardt et al IJS 2015 SAP
1. Regression models: Efficacy: intervention criteria, 3 months mRS (0-2), walking (% and time to walking), baseline NIHSS & age
Safety: intervention criteria, death, SAEs (immobility and neurological)
2. Classification and regression tree CART®
analyses
Prespecified dose response analysis – all patients, no group
Key intervention criteria: 1) Time to first mobilisation (hours after stroke onset) 2) Frequency, median sessions per day (nurse, PT data) 3) Amount activity out of bed, median minutes per day (PT only)
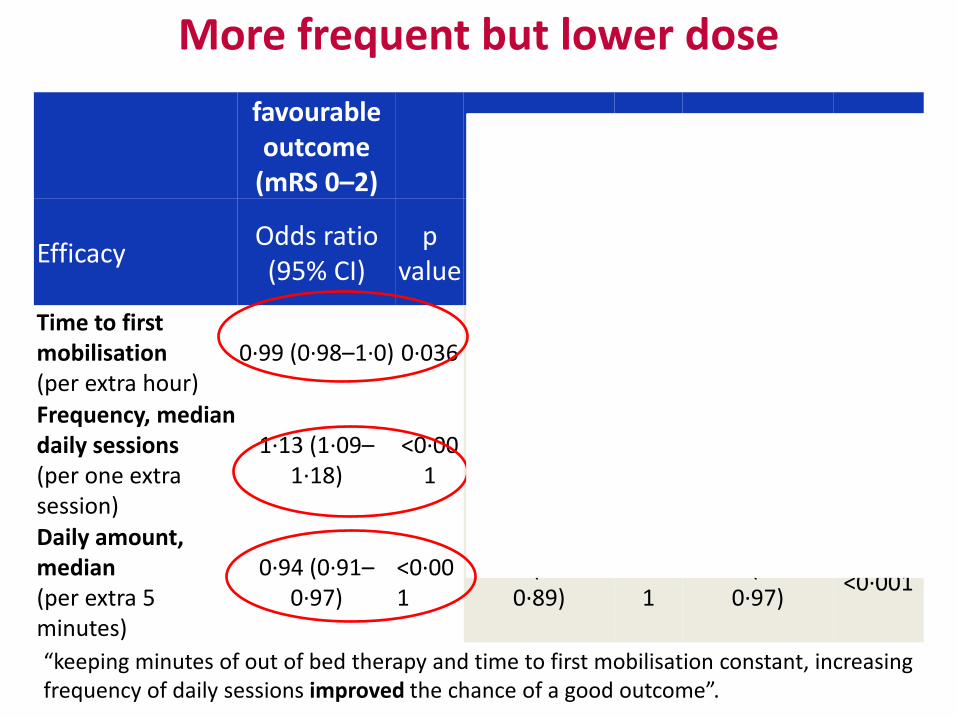
favourable outcome
(mRS 0–2)
Walking unassisted
Efficacy Odds ratio (95% CI)
p value
Binary Odds ratio (95%
CI)
p value
Cox Hazard ratio (95%
CI) p value
Time to first mobilisation (per extra hour)
0·99 (0·98–1·0) 0·036 1·0 (0·99–1·0) 0·40 0·99 (0·98–
0·99) <0·001
Frequency, median daily sessions (per one extra session)
1·13 (1·09–1·18)
<0·001
1·66 (1·53–1·80)
<0·001
1·10 (1·09–1·13)
<0·001
Daily amount, median (per extra 5 minutes)
0·94 (0·91–0·97)
<0·001
0·85 (0·81–0·89)
<0·001
0·96 (0·94–0·97)
<0·001
More frequent but lower dose
“keeping minutes of out of bed therapy and time to first mobilisation constant, increasing frequency of daily sessions improved the chance of a good outcome”.
13% improvement each additional session

favourable outcome
(mRS 0–2)
Walking unassisted
Efficacy Odds ratio (95% CI)
p value
Binary Odds ratio (95%
CI)
p value
Cox Hazard ratio (95%
CI) p value
Time to first mobilisation (per extra hour)
0·99 (0·98–1·0) 0·036 1·0 (0·99–1·0) 0·40 0·99 (0·98–
0·99) <0·001
Frequency, median daily sessions (per one extra session)
1·13 (1·09–1·18)
<0·001
1·66 (1·53–1·80)
<0·001
1·10 (1·09–1·13)
<0·001
Daily amount, median (per extra 5 minutes)
0·94 (0·91–0·97)
<0·001
0·85 (0·81–0·89)
<0·001
0·96 (0·94–0·97)
<0·001
More frequent but lower dose
66% improved odds

Deaths Non-fatal Serious Adverse Events
(SAEs)
Neurological SAEs Fatal/non-fatal
Binary Odds ratio
p value
Incident Rate Ratio (IRR)
p value
IRR p value
Time to first mobilisation (per extra hour)
0·99 (0·98–1·0)
0·07 1·0 (0·99–1·0) 0·71 1·0 (0·99–1·0) 0·45
Frequency, median daily sessions (per one extra session)
0·78 (0·7–0·88)
<0·001
0·99 (0·95–1·03)
0·55 0·89 (0·84–0·95)
0·001
Daily amount, median (per extra 5 minutes per day)
0·96 (0·89–1·04)
0·3 0·96 (0·93–0·99)
0·01 1·03 (0·99–1·08)
0·168
More frequent but lower dose
“keeping minutes of out of bed activity and time to first mobilisation constant, increasing frequency of daily sessions reduced the odds of death”.
80% did NOT have a non-fatal SAE, 90% patients did NOT have
a neurological SAE

What we know • Trial Protocol was met • Mobilisation within 24hrs was seen in both groups and is
safe- though more is not necessarily better. • Very early mobilisation may need to be more considered
especially in severe strokes or those with ICH • More frequent activity with lower duration may be of more
benefit in the first 24 hours, improving the chance of a favourable outcome and reducing the chance of dying
• This requires fundamental change to the organisation and method of therapy delivery in comparison with standard methods
• Large rehab studies are feasible and provide the best method of informing our care

What we think
• Possible physiological factors
• Possible psychological, emotional or other physical factors
• Possible organisational issues
• We don’t know
• Further study is needed to try and extract which components are feeding in to a poorer outcome in VEM

What’s to come
• AVERT DOSE- What does the future hold?
• Due in 2017 pending funding provision
• To examine the nursing and therapy hypotheses looking at optimal dose and frequency
• Further investigation based on current pending data analyses
• They need YOU!
• @AVERTtrial
Publications Efficacy and safety of very early mobilisation within 24 h of stroke onset (AVERT): a randomised controlled trial http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(15)60690-0/abstract
Prespecified dose-response analysis for A Very Early Rehabilitation Trial (AVERT) http://www.neurology.org/content/early/2016/02/17/WNL.0000000000002459.short
AVERT2 (a very early rehabilitation trial, a very effective reproductive trigger): retrospective observational analysis of the number of babies born to trial staff http://www.bmj.com/content/351/bmj.h6432.full
Exploring threats to generalisability in a large international rehabilitation trial (AVERT) http://bmjopen.bmj.com/content/5/8/e008378.full
Economic Evaluation Plan (EEP) for A Very Early Rehabilitation Trial (AVERT): An international trial to compare the costs and cost-effectiveness of commencing out of bed standing and walking training (very early mobilization) within 24 h of stroke onset with usual stroke unit care http://wso.sagepub.com/content/early/recent
Statistical Analysis Plan (SAP) for a Very Early Rehabilitation Trial (AVERT): An International Trial to Determine the Efficacy and Safety of Commencing out of Bed Standing and Walking Training (Very Early Mobilization) within 24 h of Stroke Onset vs. Usual Stroke Unit Care http://wso.sagepub.com/content/10/1/23.long

AVERT Collaboration





























