Embed Size (px)
Citation preview

Evaluation of Web based Cardiac Rehabilitation (18-month trial
using ‘Activate Your Heart’), in Scotland
Issue Date: November 2016
Anne Reoch Telehealth Advisor TEC & Digital Healthcare Innovation, Scottish Government

AYH Evaluation SCTT AR November 2016 2
INDEX
Page
1 Introduction 3
1.1 Purpose of paper 3
1.2 Background to trial 3
1.3 Trial timescale 4
1.4 Evaluation methods 4
2 Exploration phase 4
3 Pre Planning Phase 5
4 Planning Phase 5
4.1 Financial resource 6
5 Operational Phase 6
5.1 Patient Recruitment 6
5.2 Forth Valley 8
5.3 Lothian 9
6 Technical Challenges 10
7 Patient Feedback 11
7.1 Option of conventional or digital access 11
7.2 Use of digital tool 12
7.3 Most useful areas within digital tool 12
7.4 Challenging areas within the digital tool 12
7.5 Use of other self-management tools 13
7.6 Positive contribution to patient’s rehabilitation? 13
8 Conclusion 14
9 References 14
Appendix 1 Lessons Learned

AYH Evaluation SCTT AR November 2016 3
1 INTRODUCTION
1.1 Purpose The purpose of this paper is to;
provide information to cardiac rehabilitation teams as to whether the 'Activate Your
Heart' (AYH)* digital service provides a valuable contribution to cardiac rehabilitation
services in Scotland;
provide an end of project report for the Scottish Centre for Telehealth and Telecare
(SCTT)/NHS 24, who provided facilitation and evaluation of the trial.
1.2 Background
Although heart disease in the Western World has been decreasing over the last few decades it still causes many deaths. In the UK, around 110 000 men and 65 000 women have an acute myocardial infarction every year, that is equivalent to one every three minutes. 1
Cardiac rehabilitation (CR) is a complex intervention offered to patients diagnosed with heart disease, which includes components of health education, advice on cardiovascular risk reduction, physical activity and stress management. Evidence is increasing which demonstrates that CR reduces mortality, morbidity, unplanned hospital admissions in addition to improvements in exercise capacity, quality of life and psychological well-being. CR is now recommended in all heart disease guidelines, both nationally and internationally.2,3
In the UK, most CR programmes involve physical attendance at face-to-face classes for an average of eight weeks. For some, attendance is difficult for various reasons, for example; having to get time off work to attend, having to rely on others to facilitate their attendance, face to face groups may not be something certain patients are willing to take part in4. CR is now recommended for an increased number of heart related conditions. This has resulted in services in Scotland struggling to find capacity within their current CR teams to provide the rehabilitation to all patients who may benefit from this. In 2012 the Scottish Government Heart Disease Improvement Plan and Audit Scotland’s review of Cardiology Services 5 6, recommended the modernisation of CR, to enable access for more patients. In 2012 SCTT made a successful bid to the Heart Disease National Advisory Committee (NAC), securing £15K to explore solutions to improve patient information on heart disease and digital access to CR. This involved working in collaboration with the Health Information Team (HiS) within NHS 24 and CR specialists across Scotland. The ‘Heart Zone’ within the NHS Inform website www.nhsinform.co.uk, was developed as part of this initiative. This utilised the majority of the available funding. The remaining funding was used to explore possibilities for digital access to CR. This resulted in the trial of AYH.
This paper provides an overview and evaluation of the initial set up, development and operational period of the AYH trial in Scotland and concludes with some recommendations based on the lessons learned.
The project partners involved in the trial were NHS Forth Valley, NHS Lothian, Leicester University Hospital Trust and NHS 24.
*AYH was designed and developed by a specialist team at Leicester University Hospital Trust who continue to be responsible for the on going management and development of the site - www.activateyourheart.org.uk.

AYH Evaluation SCTT AR November 2016 4
1.3 Trial Timescale
The full trial timescale, from concept to completion of evaluation is shown below in Table 1.
Table1. AYH Project Timescale (from bid to explore digital cardiac rehabilitation to the end of the trial period)
Year 2012 2013 2014 2015 2016
NAC Funding bid agreed
Exploration - online HD information & CR
Field visit to AYH
Pre planning phase
Planning phase
Initial trial timescale
Workshop
Trial extension timescale
Evaluation completion
1.4 Evaluation Methods
During the planning phase there was regular communication between the Leicester team, SCTT and the two Scottish CR teams involved (Forth Valley & Lothian).
The operational phase kicked off in August 2014, and for the first six months evaluation information was collated via monthly telephone conferences with the Forth Valley and Lothian CR teams. This was used to establish a comparative baseline, identify in more detail the different processes each clinical team had in place, and enabled lessons learned to be collated and shared. Thereafter bi monthly telephone conferences took place, to which the AYH development team was also invited.
A facilitated workshop was held after nine months, to address challenges around lower levels of patient uptake than originally anticipated.
Nearing the end of the trial, staff focus groups were held in Forth Valley and Lothian, and three patient telephone interviews were undertaken facilitated by a member of the SCTT, who had not been previously involved in the trial.
2. Exploration Phase Specialists in cardiac CR were invited to review existing online CR services. Specialist team: Aynsley Cowie, Consultant specialist physiotherapist in CR, NHS Ayrshire and Arran Frances Divers, Cardiology Nurse Consultant, NHS Lothian Kate Black, Senior Physiotherapist, CR, NHS Lothian (operational phase) Sarah Florida-James, PARCS Project Manager, CHSS Catherine Mondoa, Consultant Cardiology Nurse NHS Forth Valley Lindsay Jamieson, Senior Physiotherapist, CR, NHS Forth Valley (operational phase) Facilitation Team: Anne Reoch, CVD Clinical Lead, SCTT/NHS 24 until 2014 Tracey Cunningham, Project Coordinator, SCTT/NHS 24 The initial plan was to identify Scottish requirements and possibly apply for further funding to design, develop and deliver a bespoke Scottish CR website. A literature review revealed different examples around Europe. Activate Your Heart (AYH) was deemed by the specialist team to be the most relevant option for Scottish patients.

AYH Evaluation SCTT AR November 2016 5
A field visit to the developers of AYH at Leicester University Hospital Trust took place to assess this in more detail. This visit was resourced by the NAC funding held within NHS 24. This allowed the specialist Scottish team full access to the online Programme, helping them to understand the extensive specialist input that was required to design, develop and deliver the Programme, as well as continuing to provide on-going governance for this type of service. The AYH team had carried out a positive pilot phase, which was awaiting publication 4 and were expanding within NHS England. It was agreed the AYH model with four phased Stages for completion and the ability for the patient to have continued access for a full 12 months, was relevant for the Scottish context. However, this could only be replicated in Scotland with a great deal of additional financial and time resource. It was therefore agreed a trial of AYH would be beneficial and the specialists agreed to approach their Health Boards for approval to apply for implementation funding.
Lessons Learned at Exploration Phase
1
Initial thoughts were to design and develop an online CR service for Scotland – this changed to a commissioned trial of an existing product. Lesson: If a suitable product is already available with relevant and supporting evidence and governance, commissioning should be considered in the first instance.
3. Pre Planning Phase Two of the Health Boards represented on the specialist review team, successfully secured internal funding for a trial of one year. NHS Lothian agreed to fund 200 patient licences plus their annual site cost from Improvement Funding and NHS Forth Valley agreed to fund 50 patient licences from Endowment Funding. The remaining annual site cost for Forth Valley had not been agreed through endowments but this was covered by the remaining NAC funding. As web based rehabilitation aligned well with national strategic priorities, NHS 24 agreed to provide input from SCTT to facilitate the establishment of the trial and undertake a small-scale evaluation on completion.
Lessons learned at Pre-planning Stage
1
Some 'seed' funding helped the start up of the AYH trial (and Heart Zone development). Lesson: Building ‘seed’ funding into explorative activities should be considered.
2
SCTT working within the HD NAC, highlighted the need for a digital trial within CR Lesson: National strategic clinical groups should routinely explore the option of technical solutions as part of service change/improvement.
4. Planning Phase SCTT negotiated the commissioning of AYH for the trial. This involved English Enterprise and the Central Legal Office in Scotland. NHS 24 was able to act as a representative for the territorial Health Boards, signing the contract on behalf of Scotland. This supported a single procurement with territorial Health Board reimbursement to NHS 24.
AYH Evaluation SCTT AR November 2016 6
Staff advised they felt part of project planning at both sites, although some Lothian staff reported not being involved until the planning phase was complete. Both CR teams were relatively small, which meant it was easy to pass information to all members of the team. Both teams found that outwith their clinical time it was difficult to find time to plan for the change in service. Both teams were open to the idea of using technology to support self-management activities, although some expressed concerns about how this might impact on their existing workload. Time for training in particular, was a problem for both sites. A training day was set up in Lothian for stakeholders from both geographical areas. The room booking was organised by the Lothian CR team. However there was a problem with the room allocated, which did not allow individual access to a computer terminal. This resulted in only a few staff being able to work through the online Programme while the AYH trainer was present. ‘Cascade’ training then had to take place at a later date. Staff reported that once operational, this had a negative impact on their confidence in using the system and may have impacted on their ‘marketing’ of AYH as a viable option to patients in the initial operational stage. 4.1 Financial Resource Table 2
Requirement Cost Ongoing revenue agreed
Agreed Source
Patient licence FV £ 3.25 k no Endowments
Annual site cost FV* £ 2.1 k no NHS 24 (NAC)
Patient Licence Loth. £13 k no Improvement Funding
Annual site cost Loth.* £ 2.1 k no Improvement Funding
*Only one annual charge was required per site for the 18-month trial.
Lessons Learned at Planning Stage
1
Clinical teams require dedicated training time and training resource. Lesson: Training time and resource for clinical teams should be identified at the outset. This ultimately involves some time out of clinical work for operational teams.
2
Training for staff on web-based systems requires individual 'hands on' access to a computer. Lesson: Identify room / IT accessibility for individual training prior to event – ensure access to external websites is possible.
3
A good understanding of how to ‘market’ a digital service to patients may have helped patient recruitment. Lesson: The clinical staff-training period, should include how to ‘market’ this type of service to patients.
4
A single commissioning approach facilitated each Board to make quicker progress on implementing the trial. Lesson: NHS 24 have expertise in negotiating and commissioning digital services for multiple use as part of a collaborative approach. This could be used in similar activities.

AYH Evaluation SCTT AR November 2016 7
5. Operational Phase
5.1 Patient Recruitment The main challenge for both teams was the sustained recruitment and retention of patients, see fig 1. Recruitment on a quarterly basis was lower than expected, n=20 in Forth Valley and n=74 in Lothian. At both sites, less than 1% of patients with heart disease eligible for rehabilitation chose AYH. This was in contrast to 20% of eligible patients choosing AYH three years into the service going live in Leicester. The Leicester team explained it had taken time for their numbers to increase, putting it down to good patient feedback, confidence of staff and financial resource to support a change in their working pattern.
Fig. 1 Recruitment numbers over the trial period
Participants in the focus groups outlined scenarios and factors that might affect a patient’s willingness to participate and engage with CR generally, including;
the individual experience of each cardiac patient and their own feelings of
vulnerability, denial or anxiety;
the personal demands of family and / or informal carers;
fear of exercise and rehabilitation;
the desire to return to work
Staff stated “it is a good system if you are IT literate”. However, there was uncertainty in both local teams on the ability of health professionals to accurately gauge a patient’s computer literacy. Staff asked the patient questions such as, “do you use email, do you ‘go online’, and do you shop online?” Although the answers were useful they were considered not necessarily indicative that a person could and would complete an online rehabilitation programme, especially if difficulties were encountered. Both teams assessed patients as they would have for conventional classes using the following measurements and questionnaires: • Exercise capacity using (the ISWT) • Quality of Life • Anxiety & Depression (HAD score) • Smoking status • Previous exercise habits • Diet & BMI • Blood pressure & heart rate/ECG
0 2 4 6 8
10 12 14 16 18
Ju
n-1
4
Au
g-1
4
Oct-
14
Dec-1
4
Fe
b-1
5
Ap
r-1
5
Ju
n-1
5
Au
g-1
5
Oct-
15
Dec-1
5
Fe
b-1
6
Ap
r-1
6
Lothian Total Recruitment
Forth Valley Total Recruitment

AYH Evaluation SCTT AR November 2016 8
In both Health Boards, patients who completed AYH had comparable outcome measures to patients completing the conventional classes. Both teams recognised “suitability” and lifestyle” could be indicative of whether the AYH programme would be completed, citing anecdotally the example of a patient wanting to get back to work quickly, as more likely to complete. Both teams followed the algorithm set out by AYH, and followed up those who did not activate their code or ‘move’ through the Programme in the timescale they were expected to. This involved telephone and email prompting. By the fourth month, both Health Boards raised concerns that all patient licences might not get used within the trial year. The AYH team were contacted and confirmed licences could be used after the trial period but that on going annual site costs would be required. However, by the end of the initial trial period the AYH development team agreed to prolong the use of the licences for as long as each site required, with no further site costs. AYH advised that this was primarily due to the useful feedback the teams had provided over the trial year (Table 3).
5.3 Forth Valley All Forth Valley cardiac inpatients were visited by a CR team member pre-discharge and assessed to determine what options from the cardiac rehabilitation menu would be suitable for them. This included the CR exercise and education programme and AYH. All programmes can start at four weeks post discharge. An initial individual assessment was undertaken for the AYH candidates including a 6-minute walk test. The patient was given the login password and was shown what AYH entailed. This took between 60-90 minutes, up to 30-60 minutes longer than assessment for a conventional class. However staff advised that patients in the conventional class have on-going assessment, which would balance out the extra staff time taken to complete an assessment at the initial appointment. Forth Valley staff reported they were enthusiastic and ‘open’ about the trial and, although a ‘champion’ was identified who could also cascade training, initially all the team ‘pushed’ AYH recruitment (Fig.1). The initial cohort included four of the five patients who did not complete the Programme. Retrospectively, the team considered these patients perhaps not the most suitable for the digital option; they reported their own assessment of suitability became better as the trial
progressed. However, there was an overall 70% completion rate (fig. 2), this was
comparable with the AYH development site. (Completion can be at Stage three or four of the AYH Programme, depending on the patient’s own assessment of reaching their goal). Fig. 2 Forth Valley total recruitment numbers n = 20
0
5
14
1
Total completed
Total not completed
Still active
AYH Evaluation SCTT AR November 2016 9
Initially staff logged in once a week to check a patient’s progress. Over the first year this remained the same and it became part of the rehabilitation team’s weekly routine. If a patient looked like they weren’t progressing with the Programme, an email was sent by the team to encourage continuation and completion.
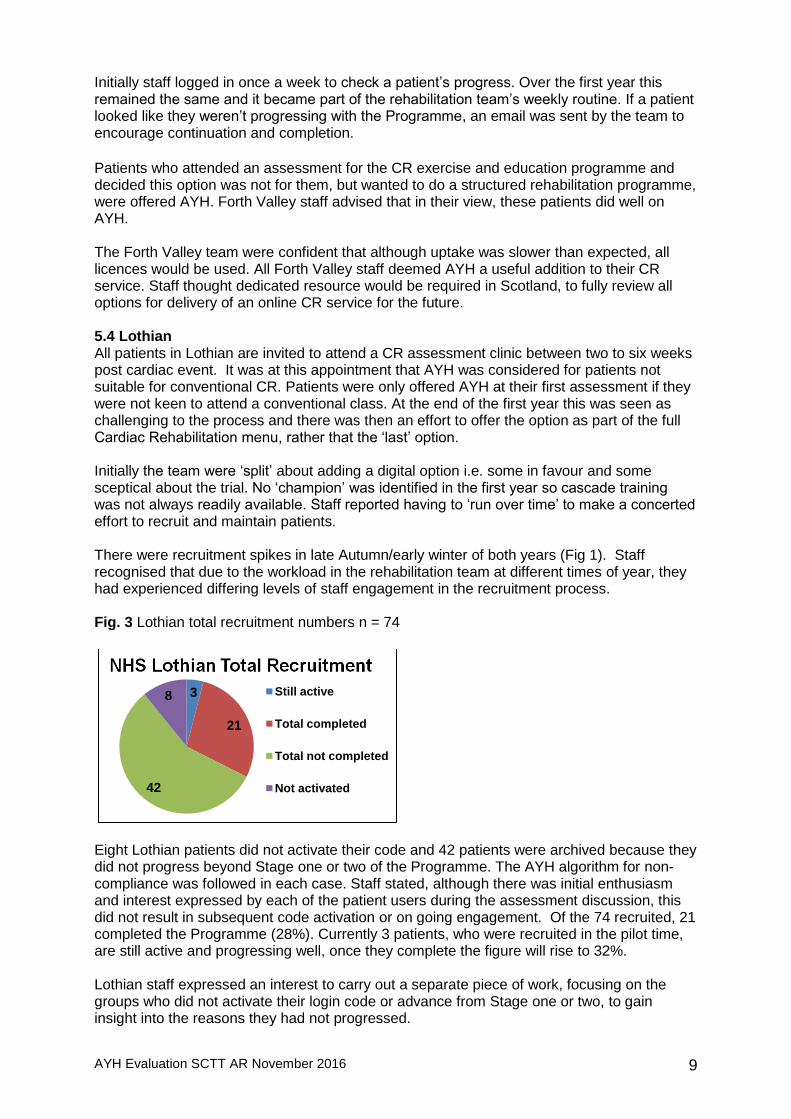
Patients who attended an assessment for the CR exercise and education programme and decided this option was not for them, but wanted to do a structured rehabilitation programme, were offered AYH. Forth Valley staff advised that in their view, these patients did well on AYH. The Forth Valley team were confident that although uptake was slower than expected, all licences would be used. All Forth Valley staff deemed AYH a useful addition to their CR service. Staff thought dedicated resource would be required in Scotland, to fully review all options for delivery of an online CR service for the future. 5.4 Lothian All patients in Lothian are invited to attend a CR assessment clinic between two to six weeks post cardiac event. It was at this appointment that AYH was considered for patients not suitable for conventional CR. Patients were only offered AYH at their first assessment if they were not keen to attend a conventional class. At the end of the first year this was seen as challenging to the process and there was then an effort to offer the option as part of the full Cardiac Rehabilitation menu, rather that the ‘last’ option. Initially the team were ‘split’ about adding a digital option i.e. some in favour and some sceptical about the trial. No ‘champion’ was identified in the first year so cascade training was not always readily available. Staff reported having to ‘run over time’ to make a concerted effort to recruit and maintain patients. There were recruitment spikes in late Autumn/early winter of both years (Fig 1). Staff recognised that due to the workload in the rehabilitation team at different times of year, they had experienced differing levels of staff engagement in the recruitment process. Fig. 3 Lothian total recruitment numbers n = 74
Eight Lothian patients did not activate their code and 42 patients were archived because they did not progress beyond Stage one or two of the Programme. The AYH algorithm for non-compliance was followed in each case. Staff stated, although there was initial enthusiasm and interest expressed by each of the patient users during the assessment discussion, this did not result in subsequent code activation or on going engagement. Of the 74 recruited, 21 completed the Programme (28%). Currently 3 patients, who were recruited in the pilot time, are still active and progressing well, once they complete the figure will rise to 32%. Lothian staff expressed an interest to carry out a separate piece of work, focusing on the groups who did not activate their login code or advance from Stage one or two, to gain insight into the reasons they had not progressed.
3
21
42
8 Still active
Total completed
Total not completed
Not activated

AYH Evaluation SCTT AR November 2016 10
Lothian staff also stated the system seemed ‘complex’ and some had been unable to activate their own codes, to allow them to work though the programme first. Some staff reported the system as ‘rigid’ and leading to staff ‘frustration’. There was worry that patient’s felt the same. However all staff recognised that technology was part of our lives and giving patient’s options for access to services that work for them was the ultimate goal.
Overall the Lothian team believed digital access to be an important addition to offering individualised cardiac rehabilitation menus to all patients in the future.
Lessons Learned at Operational Stage
1
Staff require help in identifying levels of computer literacy in patients Lesson: Identification of effective tool/or support mechanism for assessment of patient’s computer literacy is required.
2
Differing times were spent with patients in each Board on first CR assessment, which may have affected engagement Lesson: Allow time to do an initial ‘walkthrough’, when recommending an online patient self management tool such as AYH as this can impact on successful patient engagement
3
Poor completion rate and non activation of codes in Lothian Lesson: A better understanding of patients who did not remain engaged with the Programme is required. This would be useful for all self management services using online access (opportunity for future research).
4
No ‘champion’ identified at an early stage in Lothian Lesson: Identify a champion who understands the digital service and will support cascade training requirements
5
Less than expected number of patients chose the digital option of CR in both sites. Lesson: Need to understand why the digital option was not taken up in the Scottish sites in greater detail. (Opportunity for possible future research and comparison with the NHS England experience).
6.0 Technical Challenges
Whilst learning to use the Programme, both teams stated they initially had a relatively steep learning curve. They expressed concern about the ease and flexibility of the system and that if they were experiencing difficulties with their background of using IT everyday, then patients who have less daily use of IT might have a higher learning curve, thus affecting continued engagement and completion rates. Some technical challenges were experienced see Table 3, but most were addressed after discussion with the Leicester team.
AYH Evaluation SCTT AR November 2016 11
There was a good relationship between the Scottish stakeholders and the AYH development team in Leicester, which helped address technical challenges, although, at times responses were considered “slow”.
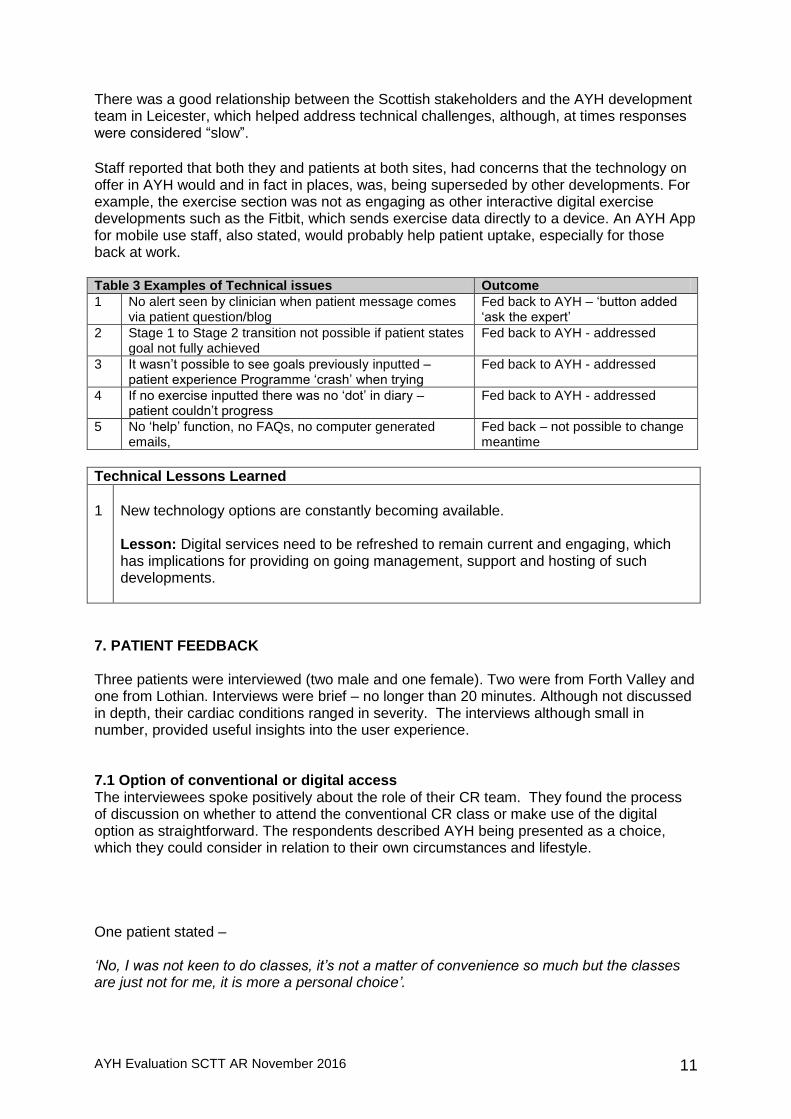
Staff reported that both they and patients at both sites, had concerns that the technology on offer in AYH would and in fact in places, was, being superseded by other developments. For example, the exercise section was not as engaging as other interactive digital exercise developments such as the Fitbit, which sends exercise data directly to a device. An AYH App for mobile use staff, also stated, would probably help patient uptake, especially for those back at work. Table 3 Examples of Technical issues Outcome
1 No alert seen by clinician when patient message comes via patient question/blog
Fed back to AYH – ‘button added ‘ask the expert’
2 Stage 1 to Stage 2 transition not possible if patient states goal not fully achieved
Fed back to AYH - addressed
3 It wasn’t possible to see goals previously inputted – patient experience Programme ‘crash’ when trying
Fed back to AYH - addressed
4 If no exercise inputted there was no ‘dot’ in diary – patient couldn’t progress
Fed back to AYH - addressed
5 No ‘help’ function, no FAQs, no computer generated emails,
Fed back – not possible to change meantime
Technical Lessons Learned
1
New technology options are constantly becoming available. Lesson: Digital services need to be refreshed to remain current and engaging, which has implications for providing on going management, support and hosting of such developments.
7. PATIENT FEEDBACK Three patients were interviewed (two male and one female). Two were from Forth Valley and one from Lothian. Interviews were brief – no longer than 20 minutes. Although not discussed in depth, their cardiac conditions ranged in severity. The interviews although small in number, provided useful insights into the user experience. 7.1 Option of conventional or digital access The interviewees spoke positively about the role of their CR team. They found the process of discussion on whether to attend the conventional CR class or make use of the digital option as straightforward. The respondents described AYH being presented as a choice, which they could consider in relation to their own circumstances and lifestyle. One patient stated – ‘No, I was not keen to do classes, it’s not a matter of convenience so much but the classes are just not for me, it is more a personal choice’.
AYH Evaluation SCTT AR November 2016 12
Another patient’s views were influenced by her husband’s experience of rehabilitation, which he’d found boring and difficult to fit into their own lifestyle. A third patient did not want to attend classes. He was keen to return to work and described the convenience of using the AYH system appealing for his situation, specifically; not having to take time off to go to classes. 7.2 Use of a digital self-management tool All of the interviewees found the tool straightforward to use. When asked about the initial experience using AYH, one patient stated - ‘it was straightforward, I understood what it was for and I got going, my wife and I both looked at it together.’ Another patient had ‘no particular problems’ with the system. A third reported that it was straightforward to work and completed all the stages. 7.3 Areas within the self-help digital tool thought most useful In particular, the interviewees found the advice to support lifestyle change, exercise and goal setting most useful. One patient found the reinforcing element, with reminders sent very useful – to paraphrase, ‘you haven’t used the system for two weeks, you’re stuck on stage three’. The same patient found the Q&A function helpful and the ability to check out stories, which had been heard or read in the media about ‘heart health’, diet or exercise; ‘when a story was in the paper or on the television about food and heart problems, I would use AYH to look up information’ The ‘Blog’ site was also considered useful by this patient. Although they had not directly participated, they had found it useful to read what others were saying about their experiences of CR. 7.4 Areas within the digital self-help tool found challenging / recommended changes The interviewees were asked about any aspects of the system, which they found more difficult to use or, changes they would recommend. The changes suggested were largely focused on making the system more dynamic and responsive. There were areas such as smoking history, which did not allow questions to be skipped once ‘no’ was answered, which one patient highlighted. Another patient had fed her comments back to the local CR team. These were about various exercises, which they felt should be included (they had an active lifestyle and exercised regularly prior to the cardiac event), they also stated a practical point about everyday exercise included in AYH; ‘once you are well enough to go out and exercise - you don’t do 15 minutes of warm up / warm down’. The same patient seemed to have concerns re credibility of information as the ‘big booklet’ provided in hospital was not always consistent with the information within AYH.

AYH Evaluation SCTT AR November 2016 13
One patient wanted to review their ‘quiz’ answers but found that could not go back to them, they thought it would be useful to add this functionality to support self-reflection on the answers provided at an earlier stage. 7.4 Use of other online self-help management tools When asked about using any other online sources for information or advice about self-care since their cardiac event, one patient stated they had not really been a user of online sites for advice, in their view they were ‘not entirely helpful’ and ‘not specific enough’. Only one patient reported that they had used other online self-help service since their cardiac event,. This was the British Heart Foundation website and was used ‘mainly to look up recipes’. 7.5 Did the digital self-management tool make a positive contribution to rehabilitation? All patients felt AYH had been a positive part of their rehabilitation. One patient stated that it was definitely of benefit to them; ‘useful, fitting in with my lifestyle and working well’ Another patient stated that they went through all of the stages, which gave them a feeling of accomplishment; ‘Yes. It was positive, because it gave me a regime to follow and it worked for me. I lost weight, walking regularly and checked my weight daily. Losing approximately 1 stone.’ A third patient stated; ‘I would certainly recommend it to someone else, if it fitted into their lifestyle.’ In particular, the respondent said it would be- ‘ useful to help other people make commitments to do exercise regularly and setting goals was especially helpful in the early days of rehabilitation. One patient had had further cardiac symptoms and had used AYH to read about them, stating; ‘even though they cannot diagnose online, it’s reassuring there is someone there’. While it may be assumed that AYH will be particularly useful for people who are returning to work or have other commitments, which make attending classes more difficult, the respondents (albeit few) are a mix of working full time, retired and some volunteers. None of these respondents were keen to do classes. Assumptions should not be made about which lifestyle might best respond to AYH. For these users, AYH has provided a positive and useful addition to their rehabilitation. 8. CONCLUSION This small trial demonstrates that although recruitment to a digital self-management service can be challenging, for some patients it is an effective option. Within the trial, 33 patients completed the digital CR programme who may not have undertaken CR if this option had not

AYH Evaluation SCTT AR November 2016 14
been available. However, assumptions should not be made at this stage about which lifestyle might best respond to a digital option. To increase compliance or completion rates, investment in staff facilitation may be an option. If a higher percentage of patients use a commissioned digital option such as AYH, there may be a need for more financial resource upfront. However, once staff confidence improves both in the use of a digital tool and the management of patients using the tool, the process should become more streamlined, which may result in cost neutrality or more effective targeting of resources. In 2014 a Scottish Government CR Clinical Champion was appointed, to drive forward the CR modernisation agenda. The main focus was around the need for robust individual assessment, with interventions based on each patient’s individual need, culminating in a CR 2020 Vision statement that included digital online options being available in all Boards as part of the CR menu, depending on patient requirements. The CR Champion is hopeful that the work recorded in this evaluation is not ‘lost’, also that further studies are undertaken to build on this work and to strengthen the current evidence base around digital CR options, which currently show the same outcomes for home based access compared to conventional face to face access7. Recently HIS has published the Draft SIGN Guideline for Cardiac Rehabilitation (Nov 2016), which recommends; “Technology-based interventions may be considered for patients participating in cardiac rehabilitation8.” The CR teams are keen to continue with AYH until all licences are used. In addition, a team has been identified (including technical expertise) to look at all other digital CR options currently available and identify where straight forward signposting for certain parts of the CR menu can be used to meet an individual’s needs. The CR representatives are keen to involve SCTT in areas of this work in the future. Other areas recommended for future investigation include, gaining a better understanding for non-completion of a digital service and, to identify a suitable tool to identify a patient’s computer literacy.
9.0 References 1. British Heart Foundation. Heart statistics. www.bhf.org.uk/research/heart-statistics
AYH Evaluation SCTT AR November 2016 15
2. British Association for Cardiovascular Prevention and Rehabilitation. BACPR standards and core components for cardiovascular disease prevention and rehabilitation 2012. 2nd ed. UKBACPR, 2012. www.bacpr.com/resources/46C_BACPR_Standards_and_Core_Components_2012.pdf 3. National Institute for Health and Care Excellence. Secondary prevention in primary and secondary
care for patients following a myocardial infarction (clinical guidance 172). NICE, 2013. www.nice.org.uk/guidance/cg172
4. Evaluating the Interactive Web-Based Program, Activate Your Heart, for Cardiac Rehabilitation Patients: A Pilot Study Christopher Brough, Sally Boyce, Linzy Houchen-Wolloff, Louise Sewell, Sally Singh.
J Med Internet Res. 2014 Oct; 16(10): e242 5. Scottish Government. Heart Disease Improvement Plan 2014, www.gov.scot/Resource/0045/00458289.pdf
6. Audit Scotland. Cardiology Services Review. www.audit-scotland.gov.uk
7. Clark RA, Conway A, Poulsen V, Keech W, Tirimacco R, Tideman P. Alternative models of cardiac rehabilitation: a systematic review. Eur J Prev Cardiolog 2015;22(1):35-74. 8. HIS SIGN. Guideline Cardiac Rehabilitation, 2016 (Draft). www.sign.ac.uk/pdf/Cardiac_rehab_PEER_REVIEW.pdf

AYH Evaluation SCTT AR November 2016 16
Appendix one – Lessons Learned AYH Lessons Learned at Exploration Phase
1
Initial thoughts were to design and develop an online CR service for Scotland – this changed to a commissioned trial of an existing product. Lesson: If a suitable product is already available with relevant evidence and governance, commissioning should be considered in the first instance.
Lessons learned at Pre-planning Stage
1
Some 'seed' funding helped the start up of the AYH trial (and Heart Zone development). Lesson: Building ‘seed’ funding into explorative activities should be considered.
2
SCTT working within the HD NAC, highlighted the need for a digital trial within CR Lesson: National strategic clinical groups should routinely explore the option of technical solutions as part of service change/improvement.
Lessons Learned at Planning Stage
1
Clinical teams require dedicated training time and training resource. Lesson: Training time and resource for clinical teams should be identified at the outset. This ultimately involves some time out of clinical work for operational teams.
2
Training for staff on web-based systems requires individual 'hands on' access to a computer. Lesson: Identify room / IT accessibility for individual training prior to event, ensure external access is possible.
3
A good understanding of how to ‘market’ a digital service to patients may have helped patient recruitment. Lesson: The clinical staff-training period should include how to ‘market this type of service to patients.
4
A single commissioning approach facilitated each Board to make quicker progress on implementing the trial. Lesson: NHS 24 has expertise in negotiating and commissioning digital services for multiple use, as part of a collaborative approach. This could be used in similar activities.
Lessons Learned at Operational Stage
1
Staff require help in identifying levels of computer literacy in patients Lesson: Identification of effective tool/or support mechanism for assessment of patient’s computer literacy is required.
2
Differing times were spent with patients in each Board on first CR assessment, which may have affected engagement Lesson: Allow time to do an initial ‘walkthrough’, when recommending an online patient self management tool such as AYH as this can impact on successful patient engagement
3
Poor completion rate and non activation of codes in Lothian Lesson: A better understanding of patients who did not remain engaged with the Programme is required. This would be useful for all self-management services using online access (opportunity for future research).
4
No ‘champion’ identified at an early stage in Lothian Lesson: Identify a champion who understands the digital service and will support cascade training requirements
5
Less than expected number of patients chose the digital option of CR in both sites. Lesson: Need to understand why the digital option was not taken up in the Scottish sites in greater detail. (Opportunity for possible future research and comparison with the NHS England experience).
Technical Lessons Learned
1
New technology options are constantly becoming available. Lesson: Digital services need to be refreshed to remain current and engaging, which has implications for providing ongoing management, support and hosting of such developments.




















![Cardiac Rehabilitation[1]](https://img.pdfslide.us/doc/110x75/577d20a21a28ab4e1e935bc2/cardiac-rehabilitation1.jpg)



![Cardiac Rehabilitation Guideline[1]](https://img.pdfslide.us/doc/110x75/551d0bbf4a795993108b4639/cardiac-rehabilitation-guideline1.jpg)



