Embed Size (px)
Citation preview

bpgmdwoewfmtrh
pCttatmf
www.AJOG.org
A survey of infection control practices for influenzain mother and newborn units in US hospitals
Munish Gupta, MD, MMSc; DeWayne M. Pursley, MD, MPHutmlsrimtwirparfc
Pregnant women and newborn in-fants are known to be at high risk for
seasonal influenza infection and its com-plications.1 The recent pandemic caused
y the 2009 H1N1 influenza A virus ap-eared to carry particular risks for theseroups, as numerous reports docu-ented high rates of hospitalization and
eath among pregnant and postpartumomen and infants who were �1 yearld.2-5 Given the higher burden of influ-nza in pregnancy, hospitals are facedith the particular challenge of caring
or pregnant women with influenza in aanner that will allow for optimal pa-
ient-centered care, while limiting theisk of infection to the mother herself,er newborn infant, and other patients.During the 2009 H1N1 pandemic,
ublic health agencies, including theenters for Disease Control and Preven-
ion (CDC), offered guidance for hospi-als for infection control practices thatddressed the use of strict isolation andhe use of N95 or equivalent respirator
asks for health care workers who caredor patients with suspected 2009 H1N1.6
Specific guidance for maternal and new-
From the Department of Neonatology, BethIsrael Deaconess Medical Center, andHarvard Medical School, Boston, MA.
Received Dec. 16, 2010; revised Feb. 19,2011; accepted March 2, 2011.
Reprints: Munish Gupta, MD, MMSc, BIDMC–Department of Neonatology, 330 BrooklineAve, Boston, MA [email protected].
Authorship and contribution to the article islimited to the 2 authors indicated. There wasno outside funding or technical assistance withthe production of this article.
Conflict of Interest: none.
Publication of this article was supported by theCenters for Disease Control and Preventionand the Association of Maternal and ChildHealth Programs.
0002-9378/$36.00© 2011 Mosby, Inc. All rights reserved.
doi: 10.1016/j.ajog.2011.03.006born units for the care of pregnantwomen with suspected H1N1 illness wasoffered in July 2009 with the release of“Considerations Regarding Novel H1N1Flu Virus in Obstetric Settings” (Table 1).7
Recommendations included the avoid-ance of close contact between motherand newborn infant while the motherwas febrile, the care of the infant by ahealthy caregiver in a separate roomand the use of expressed breast milk,rather than breastfeeding during thatperiod, and consideration of the new-born infant as potentially infected andthe use of appropriate isolation andprecautions.
After its release, various professionalorganizations raised numerous concernsabout the statement; the concern wasthat separation of mother and newborninfant may not be practical (given con-figuration and staffing of many postpar-tum wards), that current evidence didnot support the possibility of fetal infec-tion and thus, the need to consider thenewborn infant as infected, that theplacement of the newborn infant inother areas of postpartum wards couldincrease exposure to other potentially in-fected individuals, and that separation of
The purpose of this study was to describe inand newborn units in United States hospitaWe conducted surveys of neonatal intensive2010 and requested information on infectioinfluenza seasons. We received 111 responsurvey. In 2009, 58% of respondents restrictillness; 42% did not. Ninety percent of the respan ill mother and her newborn infant, althoughpercent of postpartum units and 89% of nechildren. In 2010, fewer hospitals restricted mpared with 2009. Infection control practicesconsiderably in US hospitals, particularly regnewborn infant. The identification of this variatas future investigations and future guideline d
Key words: infection control, influenza, ma
mother and infant could lead to lactation p
Supplement to JUNE 2011 Am
failure. Recognizing these concerns, otherpublic health agencies released state-ments that modified the CDC recom-mendations. For example, the Massa-chusetts Department of Public Healthrecommended new mothers with influ-enza-like illness be allowed to have theirinfants in their hospital room, with ap-propriate use of face masks, gowns, andcareful hand hygiene.8
Based on the feedback, the CDC issueda revised statement in November 2009(Table 2).9 The new guidelines contin-
ed to recommend temporary separa-ion of the newborn infant from the ill
other in the postpartum period but al-owed for this separation to occur in aeparate room or within the mother’soom with the infant in an incubator orn a bassinet at least 6 feet from the
other. The new guidelines suggestedhat the infant who is born to a motherith confirmed or suspected H1N1
llness should be considered exposed,ather than infected, and that standardrecautions for the newborn infant weredequate if the infant was well. Otherecommendations remained unchangedrom the earlier statement, which in-luded the recommendation for ex-
ion control practices for influenza in motherthe context of the 2009 H1N1 pandemic.
re unit directors in February and Novemberontrol practices during the 2009 and 2010to the initial survey and 48 to the follow-up
breastfeeding by mothers with influenza-likeents maintained physical separation betweenapproaches to this separation varied. Eighty
tal intensive care units restricted access byer-infant contact and children visitation com-influenza in mother and newborn units varying contact between an ill mother and hermay inform best practices in this area, as welllopment.
nal, neonatal
fectls inca
n csesedondthe
onaothforardioneve
ter
ressed breast milk, rather than direct
erican Journal of Obstetrics & Gynecology S77
Gyne
Supplement www.AJOG.org
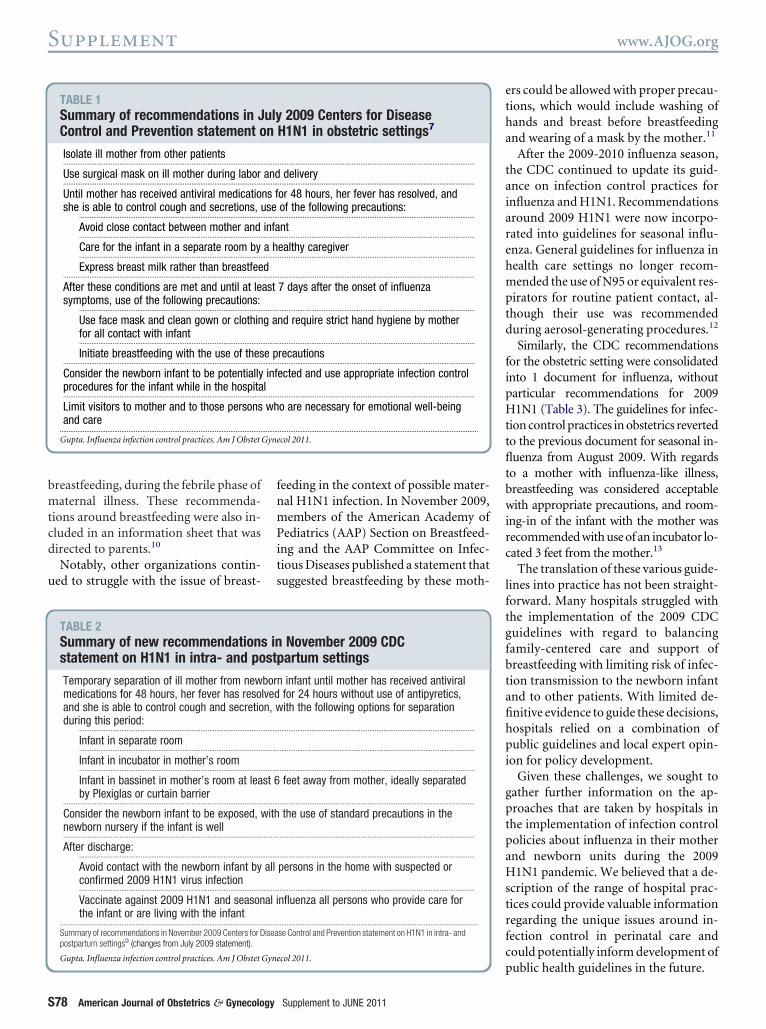
breastfeeding, during the febrile phase ofmaternal illness. These recommenda-tions around breastfeeding were also in-cluded in an information sheet that wasdirected to parents.10
Notably, other organizations contin-ued to struggle with the issue of breast-
TABLE 1Summary of recommendations in JControl and Prevention statement o
Isolate ill mother from other patients.................................................................................................................
Use surgical mask on ill mother during labor.................................................................................................................
Until mother has received antiviral medicatioshe is able to control cough and secretions,
........................................................................................................
Avoid close contact between mother and........................................................................................................
Care for the infant in a separate room by........................................................................................................
Express breast milk rather than breastfee.................................................................................................................
After these conditions are met and until at lesymptoms, use of the following precautions:
........................................................................................................
Use face mask and clean gown or clothinfor all contact with infant........................................................................................................
Initiate breastfeeding with the use of thes.................................................................................................................
Consider the newborn infant to be potentiallyprocedures for the infant while in the hospita.................................................................................................................
Limit visitors to mother and to those personsand care
...................................................................................................................
Gupta. Influenza infection control practices. Am J Obstet
TABLE 2Summary of new recommendationstatement on H1N1 in intra- and po
Temporary separation of ill mother from newmedications for 48 hours, her fever has resoand she is able to control cough and secretioduring this period:
........................................................................................................
Infant in separate room........................................................................................................
Infant in incubator in mother’s room........................................................................................................
Infant in bassinet in mother’s room at leaby Plexiglas or curtain barrier
.................................................................................................................
Consider the newborn infant to be exposed,newborn nursery if the infant is well.................................................................................................................
After discharge:........................................................................................................
Avoid contact with the newborn infant byconfirmed 2009 H1N1 virus infection........................................................................................................
Vaccinate against 2009 H1N1 and seasonthe infant or are living with the infant
...................................................................................................................
Summary of recommendations in November 2009 Centers for Dpostpartum settings9 (changes from July 2009 statement).
Gupta. Influenza infection control practices. Am J Obstet Gyne
S78 American Journal of Obstetrics & Gynecology
feeding in the context of possible mater-nal H1N1 infection. In November 2009,members of the American Academy ofPediatrics (AAP) Section on Breastfeed-ing and the AAP Committee on Infec-tious Diseases published a statement thatsuggested breastfeeding by these moth-
2009 Centers for DiseaseH1N1 in obstetric settings7
................................................................................................................
delivery................................................................................................................
or 48 hours, her fever has resolved, andof the following precautions:
................................................................................................................
nt................................................................................................................
ealthy caregiver................................................................................................................
................................................................................................................
7 days after the onset of influenza
................................................................................................................
nd require strict hand hygiene by mother
................................................................................................................
recautions................................................................................................................
ected and use appropriate infection control
................................................................................................................
o are necessary for emotional well-being
..................................................................................................................
col 2011.
November 2009 CDCpartum settings
n infant until mother has received antiviralfor 24 hours without use of antipyretics,ith the following options for separation
................................................................................................................
................................................................................................................
................................................................................................................
feet away from mother, ideally separated
................................................................................................................
the use of standard precautions in the
................................................................................................................
................................................................................................................
persons in the home with suspected or
................................................................................................................
nfluenza all persons who provide care for
..................................................................................................................
se Control and Prevention statement on H1N1 in intra- and
col 2011.
Supplement to JUNE 2011
ers could be allowed with proper precau-tions, which would include washing ofhands and breast before breastfeedingand wearing of a mask by the mother.11
After the 2009-2010 influenza season,the CDC continued to update its guid-ance on infection control practices forinfluenza and H1N1. Recommendationsaround 2009 H1N1 were now incorpo-rated into guidelines for seasonal influ-enza. General guidelines for influenza inhealth care settings no longer recom-mended the use of N95 or equivalent res-pirators for routine patient contact, al-though their use was recommendedduring aerosol-generating procedures.12
Similarly, the CDC recommendationsfor the obstetric setting were consolidatedinto 1 document for influenza, withoutparticular recommendations for 2009H1N1 (Table 3). The guidelines for infec-tion control practices in obstetrics revertedto the previous document for seasonal in-fluenza from August 2009. With regardsto a mother with influenza-like illness,breastfeeding was considered acceptablewith appropriate precautions, and room-ing-in of the infant with the mother wasrecommended with use of an incubator lo-cated 3 feet from the mother.13
The translation of these various guide-lines into practice has not been straight-forward. Many hospitals struggled withthe implementation of the 2009 CDCguidelines with regard to balancingfamily-centered care and support ofbreastfeeding with limiting risk of infec-tion transmission to the newborn infantand to other patients. With limited de-finitive evidence to guide these decisions,hospitals relied on a combination ofpublic guidelines and local expert opin-ion for policy development.
Given these challenges, we sought togather further information on the ap-proaches that are taken by hospitals inthe implementation of infection controlpolicies about influenza in their motherand newborn units during the 2009H1N1 pandemic. We believed that a de-scription of the range of hospital prac-tices could provide valuable informationregarding the unique issues around in-fection control in perinatal care andcould potentially inform development of
ulyn
.........
and.........
ns fuse.........
infa.........
a h.........
d.........
ast
.........
g a
.........
e p.........
infl.........
wh
.........
s inst
borlvedn, w
.........
.........
.........
st 6
.........
with
.........
.........
all
.........
al i
.........
isea
public health guidelines in the future.

Gyne
www.AJOG.org Supplement
MethodsIn February 2010, we contacted directorsof neonatal intensive care units (NICUs) inthe United States and sought informationon their infection control practices that re-lated to 2009 H1N1 influenza. A listing ofNICU directors was obtained from theAAP Section on Perinatal Pediatrics. Di-rectors were contacted by electronic mail.
Directors were asked about the aver-age number of deliveries at their hospitaleach year, the number of mothers andnewborn infants that were seen at theirinstitution with 2009 H1N1 infection bythe time of the survey, and for informa-tion regarding practices in their hospitalsin 4 areas during the 2009 H1N1 pan-demic: (1) breastfeeding by motherswith influenza-like illness; (2) separationof mother with influenza-like illnessfrom newborn infant; (3) access by chil-dren to the postpartum unit; and (4) ac-cess by children to the NICU.
In November 2010, we surveyed thosedirectors who had responded to the ear-lier query to obtain information onchanges to their infection control prac-tices for the 2010 influenza season. Be-cause the responses to the surveys werenot identified, directors were asked aboutpractices for both the 2009 and 2010 sea-sons to allow for the examination ofchanges within an institution. This sur-vey was conducted by electronic mailand through an online survey tool. Thesurvey was considered exempt from re-view by the institutional review board atour hospital as research that involvedsurvey procedures. The survey was ap-proved by the database committee of theAAP Section on Perinatal Pediatrics.
Results from both surveys were col-lected into a database and analyzed withMicrosoft Excel 2007 software (MicrosoftCorporation, Redmond, WA). Practices in2009 and 2010 were compared with the useof the Fisher’s exact test with the use ofStata software (version 10.0; Stata Corpo-ration, College Station, TX).
ResultsFebruary 2010Surveys were sent by electronic mail to602 NICU directors who were listed inthe AAP database; 39 messages were re-
turned as undeliverable. From the 563 re-maining contacts, 111 responses (20%)were received. The total of the averagenumber of deliveries per year at the hos-pitals was 424,000, with a median of 3000and range of 0 –18,000 deliveries. Threerespondents reported that their hospitalsdid not have labor and delivery services.
The responses to the number of 2009H1N1 infections that were seen at eachinstitution by the time of the survey, asestimated by the NICU directors, aresummarized in Table 4. Eighty-threepercent of the respondents reported atleast 1 infection in mothers; 28% of therespondents reported �5 infections inmothers; 19% of the respondents re-ported having seen at least 1 infection innewborn infants; and only 1% reported�5 infections in infants.
Responses on breastfeeding and sepa-ration of mothers and newborn infants
TABLE 3Summary of recommendations in 2guidance on influenza in obstetric
Use droplet precautions for mothers with influ.................................................................................................................
Use mask and hand hygiene by mother beforbreastfeeding.................................................................................................................
Room-in newborn infant with mother, if poss.................................................................................................................
House newborn infant in incubator, when ava.................................................................................................................
Place incubator 3 feet from mother and 3 fee.................................................................................................................
Use droplet precautions for newborn infant, if.................................................................................................................
Use private room in nursery for newborn infa...................................................................................................................
Summary of recommendations in 2010 Centers for Disease Csettings13 (statement is from August 2009).
Gupta. Influenza infection control practices. Am J Obstet
TABLE 4Mothers and newborn infants with(responses, 106 for each category)
Variable
Mothers with H1N1 infection
...................................................................................................................
Newborn infants with H1N1 infection
...................................................................................................................
Gupta. Influenza infection control practices. Am J Obstet Gyne
Supplement to JUNE 2011 Am
are summarized in Table 5. Fifty-eightpercent of the respondents indicated thatmothers with influenza-like illness werenot allowed to breastfeed directly; 42%of the respondents indicated that breast-feeding was allowed; and 90% of the re-spondents indicated that they would usesome degree of physical separation for amother with influenza-like illness andher newborn infant. Of these, 37%would separate the mother and infant byplacing the infant within the mother’sroom either at a certain distance fromthe mother or in an incubator; 56%would place the infant in a separateroom; and 6% indicated use of bothtypes of separation.
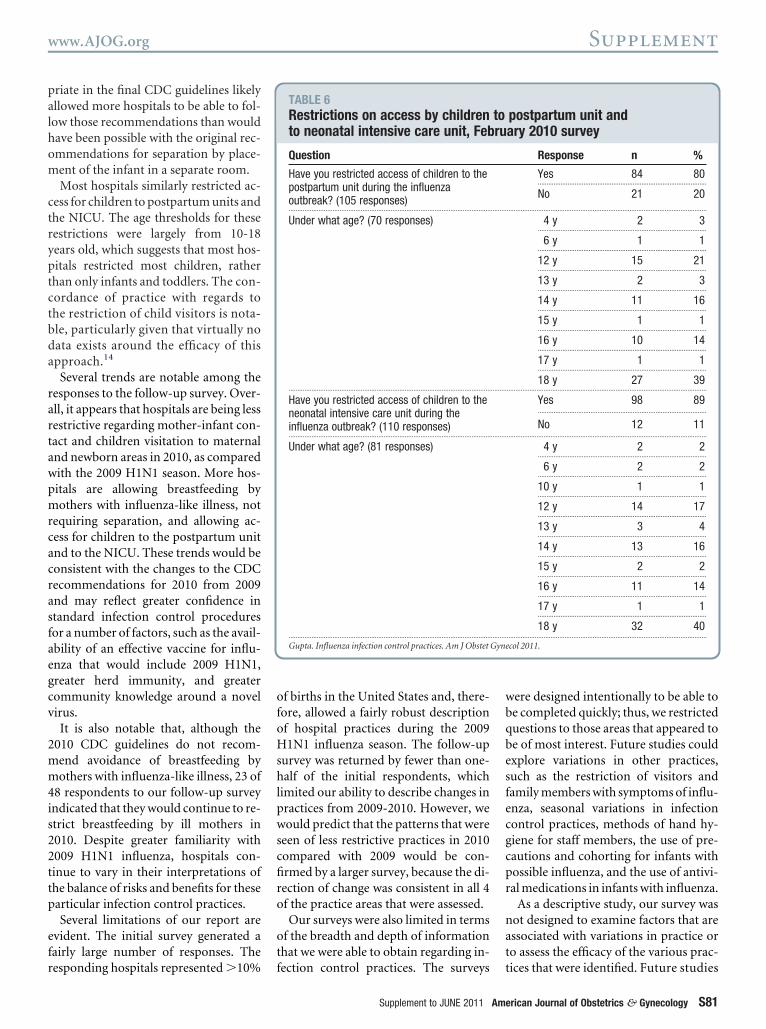
Table 6 summarizes the responses re-garding restriction of access by childrento the postpartum unit or the NICU dur-ing the influenza season. Eighty percent
0 CDCtings
za before, during, and after delivery.................................................................................................................
ntact with newborn infant, including
.................................................................................................................
.................................................................................................................
le.................................................................................................................
m other babies if housed in nursery.................................................................................................................
used in nursery.................................................................................................................
f possible..................................................................................................................
l and Prevention (CDC) guidance on influenza in obstetric
col 2011.
N1 infection
Response n %
None 18 17.............................................................................................................
1 8 8.............................................................................................................
2–5 50 47.............................................................................................................
�5 30 28..................................................................................................................
None 86 81.............................................................................................................
1 10 9.............................................................................................................
2–5 9 8.............................................................................................................
�5 1 1..................................................................................................................
01set
en.........
e co
.........
ible.........
ilab.........
t fro.........
ho.........
nt, i.........
ontro
H1
.........
.........
col 2011.
erican Journal of Obstetrics & Gynecology S79

Gyne
Supplement www.AJOG.org
of the respondents indicated restrictionson access to the postpartum unit; 89%indicated restrictions on access to theNICU. Of these units, 95% extendedthese restrictions to at least some adoles-cents, employing age thresholds of 12years or greater.
November 2010The 111 respondents to the initial surveywere surveyed again in November 2010.Forty-eight responses (43%) were re-ceived. Respondents were asked to indi-cate their practices for both the pastyear’s 2009 H1N1 pandemic influenzaseason and for the current 2010 influ-enza season. The responses are summa-rized in Table 7.
In all areas, significantly fewer hospi-tals were using restrictions on mother-infant contact and children visitation in2010 than in 2009. Eleven of 35 hospitals(31%) that did not allow direct breast-feeding by a mother with influenza-likeillness in 2009 were allowing breastfeed-ing in 2010. Eleven of 35 hospitals (31%)that required separation of a motherwith influenza-like illness and her new-born infant in 2009 were not requiringseparation in 2010. Twelve of 25 hospi-tals (48%) that restricted access by chil-dren to postpartum units in 2009 wereno longer restricting access in 2010. Sev-enteen of 40 hospitals (42%) that re-stricted access by children to the NICUin 2009 were no longer restricting access
TABLE 5Approaches to mothers with influe
Question
Will you allow a mother with influenza-like illnto breastfeed in the first 48 hours after delive(106 responses)...................................................................................................................
Will you physically separate a mother withinfluenza-like illness and her baby? (104responses)...................................................................................................................
If yes, is the separation only within the motheroom, only in a separate room, or in either?
...................................................................................................................
Gupta. Influenza infection control practices. Am J Obstet
in 2010.
S80 American Journal of Obstetrics & Gynecology
CommentObstetric and newborn providers arefaced with unique challenges with re-gards to protecting their patients frominfluenza infection. Pregnant womenand young infants are at high risk forserious complications from influenza,including death, and this risk appearedto have increased during the 2009 H1N1pandemic. Traditional infection controlmeasures cannot be applied easily towomen with influenza during the peri-natal period. Isolating the mother fromthe newborn infant and avoiding directbreastfeeding may minimize the risk ofinfection transmission to the infantbut may not be practical in the hospitaland may not be possible after discharge.Furthermore, this temporary separa-tion may impact other aspects ofmother and newborn care negatively,such as emotional well-being and breast-feeding. The measurement of the bene-fits and risks of these types of inter-ventions is difficult, and no significantevidence exists regarding their potentialor real impact.
The difficulties in balancing the risksand benefits of these interventions wereevident in the various iterations of guide-lines that were produced by the CDCfrom 2009-2010. Although the initialguidance included recommendations forisolating ill mothers from newborn in-fants, for avoiding direct breastfeedingwhile the mother was ill, and for treatingthe well newborn infant who was born to
-like illness, February 2010 survey
Response n %
Yes 44 42............................................................................................
No 62 58..................................................................................................................
Yes 94 90............................................................................................
No 10 10..................................................................................................................
Mother’s room 35 37............................................................................................
Separate room 53 56............................................................................................
Either 6 6..................................................................................................................
col 2011.
a mother with influenza as potentially
Supplement to JUNE 2011
being infected, subsequent statementsrevised all of these recommendations.
Given these challenges, hospitals arecompelled to formulate policies andpractices that best balance availablemedical knowledge, public recommen-dations, and their own clinical expertise.Our survey suggests that this approachled to significant variability in practicesduring the 2009 H1N1 pandemic season.
The most variability was seen in ap-proaches to breastfeeding. Forty-twopercent of the hospitals that were sur-veyed allowed direct breastfeeding bymothers with influenza-like illness; 58%of the hospitals prohibited it. Althoughinfluenza is not thought to be transmit-ted in breast milk, there are increasedrisks for transmission to the infant thatare based on the close contact with themother during breastfeeding. These risksare balanced by the benefits of breastmilk in supporting newborn immunityand the psychologic and developmentalbenefits of breastfeeding for mother andinfant. Provision of expressed breastmilk may preserve some of the benefits ofbreastfeeding, at least with regards toneonatal immunity, but the temporaryprohibition of breastfeeding even withthe provision of expressed breast milkmay still have a negative impact on ma-ternal and neonatal well-being and onlong-term breastfeeding success. Thecomplexity of these considerations is re-flected in the variability of hospital prac-tices and the contrasting guidelines thatwere issued by the CDC and the AAP in2009.
Less variability was seen in the ap-proaches to separation of ill mothers andnewborn infants, with most hospitals us-ing some degree of separation during the2009 H1N1 pandemic season. However,the approach to separation was quitevaried: 37% of the hospitals indicatedthat they would separate the infantwithin the mother’s room; 56% of thehospitals indicated that they would sep-arate the infant in a separate room. Mostlikely, an individual hospital’s approachto this issue is driven in large part bywhat is practical, given staffing limita-tions and the physical design of theirpostpartum units. The identification of
nza
essry?
.........
.........
r’s
.........
both approaches of separation as appro-
Gyne
www.AJOG.org Supplement
priate in the final CDC guidelines likelyallowed more hospitals to be able to fol-low those recommendations than wouldhave been possible with the original rec-ommendations for separation by place-ment of the infant in a separate room.
Most hospitals similarly restricted ac-cess for children to postpartum units andthe NICU. The age thresholds for theserestrictions were largely from 10-18years old, which suggests that most hos-pitals restricted most children, ratherthan only infants and toddlers. The con-cordance of practice with regards tothe restriction of child visitors is nota-ble, particularly given that virtually nodata exists around the efficacy of thisapproach.14
Several trends are notable among theresponses to the follow-up survey. Over-all, it appears that hospitals are being lessrestrictive regarding mother-infant con-tact and children visitation to maternaland newborn areas in 2010, as comparedwith the 2009 H1N1 season. More hos-pitals are allowing breastfeeding bymothers with influenza-like illness, notrequiring separation, and allowing ac-cess for children to the postpartum unitand to the NICU. These trends would beconsistent with the changes to the CDCrecommendations for 2010 from 2009and may reflect greater confidence instandard infection control proceduresfor a number of factors, such as the avail-ability of an effective vaccine for influ-enza that would include 2009 H1N1,greater herd immunity, and greatercommunity knowledge around a novelvirus.
It is also notable that, although the2010 CDC guidelines do not recom-mend avoidance of breastfeeding bymothers with influenza-like illness, 23 of48 respondents to our follow-up surveyindicated that they would continue to re-strict breastfeeding by ill mothers in2010. Despite greater familiarity with2009 H1N1 influenza, hospitals con-tinue to vary in their interpretations ofthe balance of risks and benefits for theseparticular infection control practices.
Several limitations of our report areevident. The initial survey generated afairly large number of responses. The
responding hospitals represented �10%of births in the United States and, there-fore, allowed a fairly robust descriptionof hospital practices during the 2009H1N1 influenza season. The follow-upsurvey was returned by fewer than one-half of the initial respondents, whichlimited our ability to describe changes inpractices from 2009-2010. However, wewould predict that the patterns that wereseen of less restrictive practices in 2010compared with 2009 would be con-firmed by a larger survey, because the di-rection of change was consistent in all 4of the practice areas that were assessed.
Our surveys were also limited in termsof the breadth and depth of informationthat we were able to obtain regarding in-
TABLE 6Restrictions on access by childrento neonatal intensive care unit, Feb
Question
Have you restricted access of children to thepostpartum unit during the influenzaoutbreak? (105 responses)...................................................................................................................
Under what age? (70 responses)
...................................................................................................................
Have you restricted access of children to theneonatal intensive care unit during theinfluenza outbreak? (110 responses)...................................................................................................................
Under what age? (81 responses)
...................................................................................................................
Gupta. Influenza infection control practices. Am J Obstet
fection control practices. The surveys
Supplement to JUNE 2011 Am
were designed intentionally to be able tobe completed quickly; thus, we restrictedquestions to those areas that appeared tobe of most interest. Future studies couldexplore variations in other practices,such as the restriction of visitors andfamily members with symptoms of influ-enza, seasonal variations in infectioncontrol practices, methods of hand hy-giene for staff members, the use of pre-cautions and cohorting for infants withpossible influenza, and the use of antivi-ral medications in infants with influenza.
As a descriptive study, our survey wasnot designed to examine factors that areassociated with variations in practice orto assess the efficacy of the various prac-
postpartum unit andary 2010 survey
Response n %
Yes 84 80................................................................................................
No 21 20..................................................................................................................
4 y 2 3................................................................................................
6 y 1 1................................................................................................
12 y 15 21................................................................................................
13 y 2 3................................................................................................
14 y 11 16................................................................................................
15 y 1 1................................................................................................
16 y 10 14................................................................................................
17 y 1 1................................................................................................
18 y 27 39..................................................................................................................
Yes 98 89................................................................................................
No 12 11..................................................................................................................
4 y 2 2................................................................................................
6 y 2 2................................................................................................
10 y 1 1................................................................................................
12 y 14 17................................................................................................
13 y 3 4................................................................................................
14 y 13 16................................................................................................
15 y 2 2................................................................................................
16 y 11 14................................................................................................
17 y 1 1................................................................................................
18 y 32 40..................................................................................................................
col 2011.
toru
.........
.........
.........
.........
tices that were identified. Future studies
erican Journal of Obstetrics & Gynecology S81

Supplement www.AJOG.org
could investigate whether certain fea-tures of hospitals or NICUs are associ-ated with more or less restrictive infec-tion control practices and whetherdifferent infection control practicesare associated with higher or lowerrates of nosocomial infections in new-born infants.
Despite these limitations, our studydoes offer valuable information on ap-proaches to infection control practicesfor influenza in mother and newbornunits. Given the lack of clear evidence,the survey results can be viewed as asummary of “expert opinion” in thisarea. In the context of the 2009 H1N1epidemic, the concordance of practicesaround restriction of child visitors topostpartum units and NICUs suggests ageneral consensus that avoiding intro-duction of the virus into the units is per-haps the most vital hospital-based in-fection control practice, and that thebenefits of restricting children outweighthe negative impact on family-centeredcare. On the other hand, the lack of con-sensus on the separation of mothers andnewborn infants and the restriction ofdirect breastfeeding reveals the greaterdifficulty in balancing risks and benefitsof these interventions.
Numerous challenges persist in theidentification of the optimal hospitalpractices to limit the risk of influenza for
TABLE 7Responses to November 2010 surv
Question
Direct breastfeeding by mother with influenza
...................................................................................................................
Separation of mother with influenza-like illnes
...................................................................................................................
Restriction of access of children to postpartum
...................................................................................................................
Restriction of access of children to neonatal i
...................................................................................................................
There were 48 total responses. Not all respondents answereda Two-sided Fisher’s exact test that compared 2009-2010 an
Gupta. Influenza infection control practices. Am J Obstet
mothers and newborn infants while sup-
S82 American Journal of Obstetrics & Gynecology
porting family-centered care. At theleast, this report should help providerswho are charged with developing infec-tion control guidelines for the motherand newborn units in their hospitals tounderstand the range of practices thathave been used. In addition, the identifi-cation of the practices with the highestvariation should help inform efforts bypublic health agencies and investigatorsin terms of areas of emphasis for furtherstudy and guideline development. In themeantime, all of us who provide care tomothers and newborn infants shouldcontinue to emphasize those primary in-terventions that we know to be essentialand on which we can have a major im-pact: to encourage universal influenzavaccination of pregnant women andcaregivers and household contacts ofnewborn infants, to ensure meticuloushand hygiene by hospital staff membersand by families, to use restrictions onhealthcare workers with influenza-likeillness to limit exposure to patients andfamilies, and to provide careful educa-tion and discharge preparation to ensuresafe practices in the hospital and athome. f
REFERENCES1. Fiore AE, Shay DK, Broder K, et al. Preven-tion and control of seasonal influenza with vac-
Response
200
n
e illness Yes 13......................................................
No 35.........................................................................................................................
nd newborn infant Yes 35......................................................
No 11.........................................................................................................................
it Yes 25......................................................
No 17.........................................................................................................................
sive care unit Yes 40......................................................
No 7.........................................................................................................................
f the questions.
10-2011.
col 2011.
cines: recommendations of the Advisory Com-
Supplement to JUNE 2011
mittee on Immunization Practices (ACIP), 2009.MMWR Recomm Rep 2009;58:1-52.2. Louie JK, Acosta M, Jamieson DJ, HoneinMA. Severe 2009 H1N1 influenza in pregnantand postpartum women in California. N EnglJ Med 2010;362:27-35.3. Jamieson DJ, Honein MA, Rasmussen SA, etal. H1N1 2009 influenza virus infection duringpregnancy in the USA. Lancet 2009;374:451-8.4. Libster R, Bugna J, Coviello S, et al. Pediatrichospitalizations associated with 2009 pan-demic influenza A (H1N1) in Argentina. N EnglJ Med 2010;362:45-55.5. Louie JK, Gavali S, Acosta M, et al. Childrenhospitalized with 2009 novel influenza A(H1N1)in California. Arch Pediatr Adolesc Med 2010;164:1023-31.6. Centers for Disease Control and Prevention.Interim guidance on infection control measuresfor 2009 H1N1 influenza in healthcare settings,including protection of healthcare personnel.[Internet]. Atlanta: CDC; 2010 [updated July 15,2010; cited October 30, 2010]. Available at:http://www.cdc.gov/h1n1flu/guidelines_infection_control.htm. Accessed Oct. 30, 2010.7. Centers for Disease Control and Prevention.Considerations regarding novel H1N1 flu virusin obstetric settings. [Internet]. Atlanta: CDC;2009 [updated July 6, 2009; cited July 8, 2009;Archived Nov 10, 2009]. Available at: http://www.cdc.gov/h1n1flu/guidance/obstetric.htm.Accessed July 8, 2009.8. Commonwealth of Massachusetts. Fall 2009clinical advisory for new mothers with influenzalike illness who are hospitalized. Boston: De-partment of Public Health; September 29,2009.9. Centers for Disease Control and Prevention.Interim guidance: considerations regarding2009 H1N1 influenza in intrapartum and post-
010 2010–2011
P valuea% n %
27 24 51 .021..................................................................................................................
73 23 49..................................................................................................................
76 23 51 .017..................................................................................................................
24 22 49..................................................................................................................
60 12 29 .008..................................................................................................................
40 29 71..................................................................................................................
85 22 48 .0002..................................................................................................................
15 24 52..................................................................................................................
ey
9–2
-lik.........
......... .........
s a.........
......... .........
un.........
......... .........
nten.........
......... .........
all o
d 20
Gyne
partum hospital settings. [Internet]. Atlanta:

www.AJOG.org Supplement
CDC; 2009 [updated November 10, 2009; citedOctober 30, 2010]. Available at: http://www.cdc.gov/h1n1flu/guidance/obstetric.htm. Ac-cessed Oct. 30, 2010.10. Centers for Disease Control and Preven-tion. 2009 H1N1 flu (swine flu) and feeding yourbaby: what parents should know. [Internet]. At-lanta: CDC; 2009 [updated October 23, 2009;cited October 30, 2010]. Available at: http://www.cdc.gov/h1n1flu/infantfeeding.htm. Ac-
cessed Oct. 30, 2010.11. Lawrence RA, Bradley JS. Breastfeedingadvice for mothers with possible H1N1 infec-tion. AAP News 2009;30:11.12. Centers for Disease Control and Preven-tion. Prevention Strategies for Seasonal Influ-enza in Healthcare Settings. [Internet]. Atlan-ta: CDC; 2010 [updated September 20,2010; cited October 30, 2010]. Available at:ht tp: / /www.cdc.gov/flu/profess iona ls/infectioncontrol/healthcaresettings.htm. Ac-
cessed Oct. 30, 2010.Supplement to JUNE 2011 Am
13. Centers for Disease Control and Prevention.Guidance for Prevention and Control of Influenza inthe Peri- and Postpartum Settings. [Internet]. Atlan-ta: CDC; 2009 [updated August 1, 2009; cited Oc-tober 30, 2010]. Available at: http://www.cdc.gov/flu/professionals/infectioncontrol/peri-post-settings.htm. Accessed Oct. 30, 2010.14. Groothuis J, Bauman J, Malinoski F, Egg-leston M. Strategies for prevention of RSVnosocomial infection. J Perinatol 2008;28:
319-23.erican Journal of Obstetrics & Gynecology S83