Embed Size (px)
Citation preview

ANNALS O F CLINICAL AND LABORATORY SCIEN CE, Vol. 21, No. 5Copyright © 1991, Institu te for Clinical Science, Inc.
A Study of Aspirin Induced Changes in Bleeding Time, Platelet Aggregation, and Sonoclot® Coagulation Analysis in Humans*f$
SATWANT K. SAMRA, M.D.,§ ROBERT L. HARRISON, M.D.,11 DAVID E. BEE, Ph .D.,1
and VICENTE VALERO, M.D.**
Departments o f § Anesthesiology, 11Pathology, and **Internal Medicine, University o f Texas Medical Branch,
Galveston, TX 77550
ABSTRACT
The purpose of this study was to determ ine w hether or not a new er test of p la te le t function, Sonoclot® coagulation analysis, can identify the patients who develop significant prolongation of bleeding tim e after aspirin ingestion. Tem plate bleeding time, platelet aggregation in response to arachidonic acid, collagen, epinephrine, adenosine diphosphate, and ristocetin, and Sonoclot® coagulation analysis were performed before and after ingestion of aspirin in 22 adult volunteers. Mean bleeding tim e increased from 5.32 ± 2.16 min to 7.34 ± 2 .1 min, bu t rem ained w ithin normal range (2.5 to 9 min). There was marked intersubject variability in the effect of aspirin on bleeding time, and difference betw een men and wom en was not significant. T here was significant decrease in p la te le t aggregation in response to arachidonic acid, collagen and epinephrine. Sonoclot® coagulation analysis did not show significant effect of aspirin administration. There was no correlation among changes in bleeding time, p latelet aggregation, and Sonoclot® coagulation analysis. Five patients with known platelet function disorders and prolonged bleeding times (mean = 18.5 min, range 14 to 22) without any other coagulation abnormalities were also studied. In four of these patients who had normal platelet count, Sonoclot® graphs were morphologically similar to those in the volunteers with normal b leeding times, bu t in one patient with thrombocytopenia, morphology was altered. It is our conclusion that Sonoclot® coagulation analysis is unlikely to identify patients with prolonged bleeding time in whom platelet count and other coagulation factors are normal.
* P re se n ted a t th e 64th C ongress o f In terna tional A nesthesia R esearch Society, H ono lu lu , H I, M arch1990.
t S u p p o rted by a g ran t from Sience, Inc ., M orrison, C O 80465.t Sen d re p rin t req u ests to Satw ant K. Sam ra, M .D ., D ep artm en t o f A nesthesio logy, Box 48, 1G323
U niversity H osp ita l, 1500 E . M edical C en te r D rive, A nn Arbor, M I 48109-0048.H D eceased .
3150091-7370/91/0900-0315 $00.00 © Institute for Clinical Science, Inc.

316 SAMRA, HARRISON, BEE, A N D VALERO
Introduction
W hile taking care of surgical patients w ith m ultiple m edical problem s, anesthesiologists have to weigh carefully the risks and benefits of regional vs. general anesthesia. One of the inherent risks of any regional block is hematoma formation secondary to accidental puncture of blood vessels in close proximity to the n e rv e s to b e b lo c k e d . T h is risk is increased in patients with bleeding disorders owing either to intrinsic coagulation disorders or to those secondary to medications. Two such drugs of particular concern to anesthesiologists are aspirin and d ipyridam ole. As a resu lt of recent reports in the literature4,6,7’16 suggesting the value of small doses of aspirin in prevention of myocardial infarction and stroke, anesthesiologists encounter an increasing num ber of elderly surgical patients who are taking “ an aspirin a day” on a regular basis. Regional anesthesia may be the technique of choice in many of these patients, but in light of existing knowledge of the effect of aspirin on platelet function8’10,11,13,19’22 it is desirable that platelet function abnormalities be ruled out in patients taking aspirin prior to adm inistration of regional anesthesia.
Assessm ent of p late le t function p re sents a challenge to the clinicians. There is significant disagreem ent among differen t investigators regarding the efficacy and clinical value of currently available tests of p latelet function.15,21 This is further borne out by the fact that while there is overwhelm ing evidence in medical literature docum enting irreversible inhibition of platelet aggregation even with a s in g le d o se o f a s p ir in , c l in ic a l ly increased bleeding has not been a problem during surgery in patients taking aspirin on a regular basis. On the other h an d , so grave cou ld be the co n se q u e n c e s o f an e p id u ra l / in t r a th e c a l hematoma formation that it behooves an
anesthesiologist to rule out the possibility of prolonged or excessive bleeding b e fo re d o in g a lu m b a r p u n c tu re in patients with potentially altered platelet function. State of the art platelet function tests currently used are platelet aggregation studies and tem plate bleeding time. Results of both these tests are difficult to obtain in most hospitals prior to an em ergency surgery.
An instrum ent, Sonoclot®* is now commercially available. It is a dynamic viscom eter w hich m easures v iscoelastic properties of whole blood or plasma. The viscoelastic m easurem ent of clot formation has been proposed as a bedside test of platelet function23 and its use for intraoperative monitoring of coagulation status in p a tien ts u n d e rg o in g coronary artery bypass,1,24,26 liver transplant,9,20 and th o se w ith p re g n a n c y - in d u c e d hypertension12 has recently been reported. None of the aforem entioned clinical studies has utilized this test for identification of an isolated defect in platelet function (as produced by aspirin ingestion) in the presence of otherwise normal coagulation profile. This clinical investigation was designed by us to evaluate (a) the effect of small dose of aspirin on bleeding time, and (b) the performance of this new instrum ent as a tool to detect the abnormalities of platelet function resulting in prolongation o f b leed ing tim e. Another purpose of this study was to de te rm ine if there is any correla tion among three tests of platelet dysfunction,i.e., tem pla te b leed in g tim e, p la te le t aggregation, and viscoelastic properties of whole blood determ ined by Sonoclot®. The ultimate goal of this study was to determ ine if Sonoclot® coagulation analysis can be u tilized as a bedside test to id en tify those p a tie n ts w ho have developed a sign ificant coagulopathy
* Sienco Inc., 9188 S. T urkey C reek Road, M orrison, C O 80465.

STUDY O F ASPIRIN IN D U C E D CH ANG ES A N D SONOCLOT® COAGULATION 317(p ro lo n g ed b le e d in g tim e) ow ing to ingestion of aspirin or aspirin containing medications.
M aterials and M ethods
T h e I n s t r u m e n t
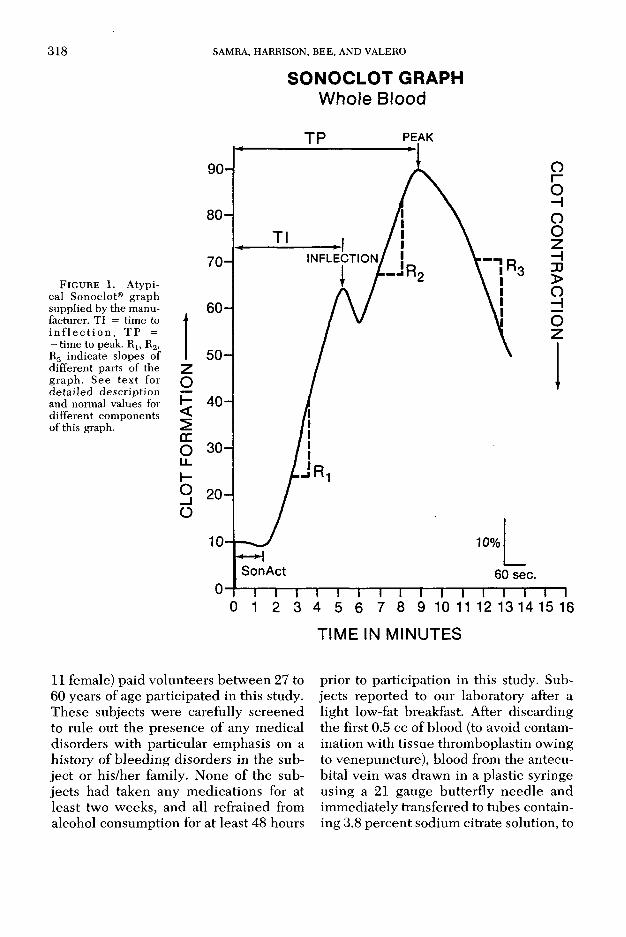
Sonoclot® coagulation analyser m easures dynamic viscosity of a fluid (whole blood or plasma) by immersing an axially vibrating probe in the fluid. The probe oscillates at a frequency of approximately 200 to 250 Hz. Feedback circuitry in the instrum ent constantly adjusts the amount of pow er needed by the oscillator to keep constant the probe’s motion. For a sample w ith increasing viscosity, such as c lo tting b lood , the am ount of pow er needed to operate the oscillating probe increases as a function of time. According to the m anufacturer’s technical manual, the electrical output of the instrum ent is a m easure of this power requirem ent and hence the blood sample’s dynamic viscosity. The instrum ent consists of a heating block to hold the samples at 37°C, a m agnetic stirrer for mixing the sample, a sensitivity or gain control, and an output zeroing adjustm ent. The output signal from the instrum ent can be connected either to an analog recorder or an analog to digital converter for com puterized data acquisition. W hen used with an analog reco rder, th is in s tru m e n t p rov ides a graph similar to the one shown in figure1. Different components of this graph and their interpretation as suggested by the m anufacturer is as follows:
1. Initial flat portion of this curve (Son- Act) is similar to activated clotting time. The acceptable normal range is 60 to 130 seconds.
2. A rapid rise in viscosity is indicated by the upslope of the curve. This increase in viscosity is due to conversion of fibrinogen to fibrin. The rate of rise of this viscosity (Rx) is
determ ined from this curve and the slope of this curve is an indicator of platelet function. Normal range is 15 to 30 percent per minute.
3. This is followed by an “ inflection” in the graph w hich ind icates the beginning of incorporation of the platelets into the fibrin mesh. Time to inflection (TI) is an indirect m easure of Rj.
4. A well defined “peak” (TP) following inflection on this graph, indicates completion of fibrin formation. This is followed by a dow nslope, rate (R3) of which is an indicator of clot retraction. Normal tim e to peak is 5 to 10 m inutes and the normal value for R3 is more than two percent.
T h e T e s t
A small volume (0.4 ml) of e ither fresh whole blood or citrated blood (containing3.8 percent sodium citrate in a blood: citrate ratio of 9:1) can be used. A small plastic cuvette and a cylindrical teflon probe with 0.04 ml capacity are used for processing of the sample. The instrum ent is allowed to warm to 37°C. A strip chart recorder is turned on at a known paper speed. Both the cuvette and teflon probe are inserted at their appropriate positions in the instrument. A sample of blood (0.4 ml), is transferred into the cuvette contain ing kaolin and a m etallic stir-bar. After insuring proper mixing of the sample for 10 seconds, the teflon probe is gently lowered into the sample by closing the plastic head of the instrum ent. Viscosity changes of blood are recorded in the form of a graph which is in terpreted as previously discussed. Results are available w ithin m inutes of drawing the blood sample.
E x p e r i m e n t a l P r o t o c o l
Institutional approval of the protocol was obtained. Twenty-two (11 m ale and
318 SAMRA, HARRISON, BEE , A N D VALERO
SONOCLOT GRAPHW h o le B lo o d
F i g u r e 1. A ty p ica l Sonoclot® g ra p h su p p lied by th e m an u facturer. T I = tim e to i n f l e c t i o n , T P = — tim e to peak. R 1; R2, R3 in d ica te slopes o f d iffe re n t parts o f th e g ra p h . S e e te x t fo r d e ta i le d d e s c r ip t io n an d norm al values for d iffe re n t co m ponen ts o f th is graph.
T IM E IN M IN U T E S
11 female) paid volunteers betw een 27 to 60 years of age participated in this study. These subjects were carefully screened to rule out the presence of any medical disorders with particular emphasis on a history of b leeding disorders in the subject or his/her family. None of the subjects had taken any m edications for at least two weeks, and all refrained from alcohol consumption for at least 48 hours
prior to participation in this study. Subjects reported to our laboratory after a light low-fat breakfast. After discarding the first 0.5 cc of blood (to avoid contamination with tissue throm boplastin owing to venepuncture), blood from the antecu- bital vein was drawn in a plastic syringe using a 21 gauge butterfly needle and immediately transferred to tubes containing 3.8 percent sodium citrate solution, to

STUDY O F ASPIRIN IN D U C E D CH ANGES A N D SONOCLOT® COAGULATION 319obtain a mixture of blood ¡citrate in a ratio of 9:1. This blood was used to perform p late le t aggregation studies and Sono- clot® coagulation analysis.
For perform ing p la te le t aggregation studies, platelet rich plasma (PRP) was obtained by centrifuging whole blood at 160 x g for 10 minutes. Supernatant containing PRP was carefully rem oved and platelet poor plasma (PPP) was then prepared by additional centrifugation for 10 m inutes at 4000 X g. Platelet count for aggregation was adjusted by mixing PRP with PPP to obtain a count of approxim ately 200,000 platelets per |xl. A sample of 0.45 ml of PRP was transferred to an aggregation cuvette to which a stir bar was added. The sample was stirred and allowed to equilibrate to 37°C tem perature for one m inute, and the aggregating agent d iluted in 0.05 ml of normal saline th en was add ed to the cuve tte . T he aggregating agents tested and their concentrations were: arachidonic acid (AA) 500 mg per ml, adenosine diphosphate (ADP) in concentrations of 2.5 and 1.0 |xM per L, epinephrine 10 |xM per L, collagen 1 fxg per ml and ristocetin 1.5 mg per ml. The rationale for using m ultiple aggregating agents was tha t d ifferen t agents test different mechanisms of platele t aggregation. Platelet aggregation was quantitated by measuring the maximum change in light transmission through the sample using a four channel aggregome- ter.* A sample of 0.5 ml PPP was used as the control, and the amount of light transm itted through PPP was considered 100 p e rcen t, ind ica ting com plete p la te le t aggregation. Owing to technical difficulties, p latelet aggregations in four volunteers could not be performed. Therefore data are reported in 18 subjects only.
T e m p la te b le e d in g tim e was p e r formed in duplicate using a disposable
devicet that produces a painless incision one mm in depth and nine mm in length. Incisions were located in a horizontal (parallel to the antecubital crease) plane on the lateral aspect of the volar surface of the forearm, five centim eters below the antecubital crease. Venostasis was achieved by inflation of a blood pressure cuff to 40 mmHg for 30 seconds prior to skin incision and m ain ta ined for the duration of the test. Blood from the incision was blotted once every 30 seconds until all oozing stopped.
Sonoclot® coagulation analyses w ere performed on both freshly draw n as well as citrated blood. Duplicate tests on cit- rated blood were done to establish reproducibility of data. Numerical values for Sonoclot® param eters, i.e., SonAet, R 1; TI, TP and R3, were obtained from the graphs, and the m ean values o f two recordings in each patient are reported. After doing all laboratory tests (bleeding time, platelet aggregation and Sonoclot® analysis) the patients were given 325 mg aspirin? twice a day for two days. The aforementioned tests were repeated after 48 hours, approximately 12 hours after the last dose of aspirin.
F ive p a tien ts w ith know n p la te le t f u n c t io n a b n o rm a l i t ie s w e re a lso included in this study. All these patients had an iso la ted p la te le t d y sfu n c tio n accom panied by m arkedly p ro longed bleeding time (14 to 22 m inutes) in the presence of normal values for prothrom- bine time (PT), activated partial throm bop la s tin tim e (PTT), f ib r in o g e n , and fibrinogen split products. These patients were included to determ ine the usefulness of Sonoclot® analysis in detecting platelet dysfunction in the presence of normal levels of other clotting factors. In these patients, platelet aggregation stud-
* M onitor, IV, H e len a L aboratories, B eaum ont, TX.
t Surgicutt®, A m erican Scientific C orporation , ??. t Bayer C om pany, N ew York, NY.

320 SAMRA, HARRISON, B EE , A N D VALERO
ies w ere om itted and only tem p la te b leeding tim es and Sonoclot® analysis were performed.
S t a t i s t i c a l A n a l y s i s
V alues for p la te le t agg rega tion in response to all aggregating agents were analyzed using a repeated measures analysis of variance to determ ine the effect of asp irin ingestion on abnorm alities of platelet aggregation in response to differen t agents.
N um erical da ta for b le e d in g tim e, p la te le t a g g reg a tio n in re sp o n se to arachidonic acid and collagen, and Sonoclot® param eters TI, TP and R3 w ere subjected to a two factors repeated measures analysis of variance to study the effect of aspirin, sex differences and any interaction betw een the two. These data were also subjected to a correlation analysis to study any correlation betw een the effect of aspirin on bleeding time, p la te le t a g g re g a tio n an d Sonoclot® parameters. A value of p < 0.01 was considered significant.
Results
In table I are shown the data for platelet aggregation in response to five agents tested . N um erical values are for light transmittance through plasma before and after aspirin ingestion. A mean decrease in p la te le t aggregation in response to arachidonic acid, collagen and ep inephrine by 84.2 percent, 68.9 percent, and54.4 percent, respectively, was observed. These changes were statistically significant. P latelet aggregation in response to ristocetin and low er concen tra tion of ADP rem ained nearly unchanged (4 perc e n t and 5.6% in h ib itio n ) , w h ile a decrease of 14.7 percent in response to higher concentration of ADP was seen. In h ib itio n o f p la te le t aggregation in response to ADP and ristocetin was not statistically significant.
Since the m ost p rom inen t effect of aspirin was seen on platelet aggregation in response to AA and collagen, data were included for only these two agents in correlation analysis to study the relatio n sh ip am ong changes in b lee d in g time, platelet aggregation, and Sonoclot® coagulation analysis.
Mean values for b leeding time, platelet aggregation with arachidonic acid and collagen, and Sonoclot® param eters for normal volunteers before and after aspirin are shown in table II. M ean bleeding tim e increased from 5.32 ± 2.16 m inutes to 7.34 ± 2.15 m inutes, a statistically significant increase (P = 0.0001). Considerable variation among subjects was noted. Bleeding time increased by one m inute or less in three subjects, decreased after aspirin ingestion in three, while in three other subjects, it doubled com pared to pre-aspirin values. In terms of absolute values, in only four out of twenty-two subjects an abnorm al value of greater than nine m inutes (normal range in our laboratory is 2.5 to 9 m inutes) was seen. Two out of these four subjects had an abnormally long bleeding time (10 m inutes and 11.4 m inutes) prior to ingestion of aspirin, and a prolongation of only 1.75 m inutes and 1.1 m inute, respectively , was seen after aspirin in these two subjects. None of these subjects had any history of abnormal or excessive bleeding. Prolongation of bleeding tim e was more in males than females (50 percent vs. 25 percent), but this difference was not statistically significant.
Sonoclot® coagulation analysis produced easily in terpretable graphs with both fresh whole blood as well as citrated blood. Num erical values for Sonoclot® parameters reported in this study were obtained using citrated blood because it provided us the opportunity to run this test in duplicate. In figure 2 are shown the Sonoclot® graphs before and after aspirin ingestion, for one representative subject in our study. D espite a 58 percent
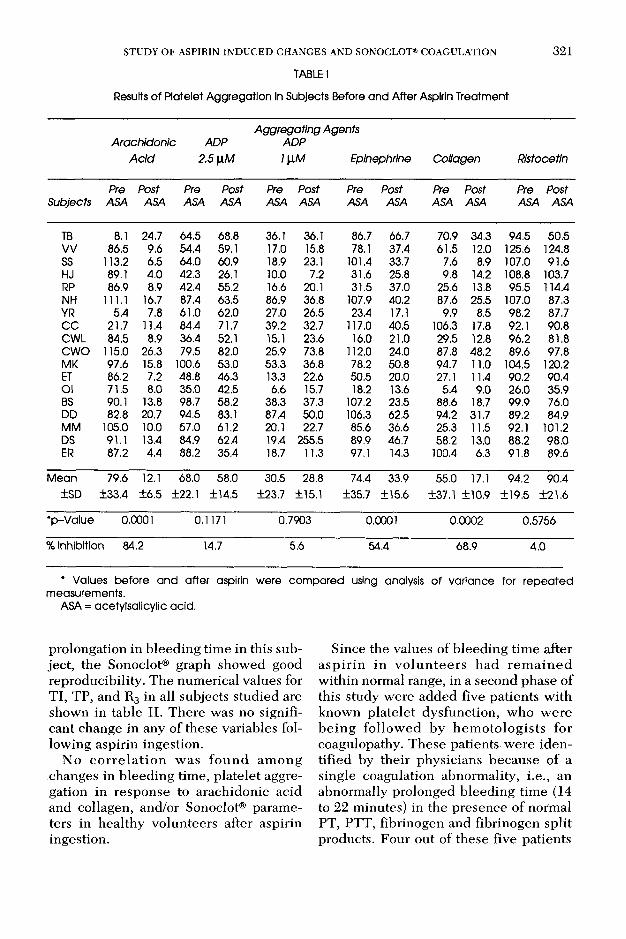
TABLE tResults of Platelet Aggregation In Subjects Before and After Aspirin Treatment
STUDY O F ASPIRIN IN D U C E D CH ANGES A N D SONOCLOT® COAGULATION 321
Arachidonic ADP Acid 2.51xM
Aggregating Agents ADP1 \XM Epinephrine Collagen Ristocetin
SubjectsPre
ASAPostASA
PreASA
PostASA
PreASA
PostASA
PreASA
PostASA
PreASA
PostASA
Pre Post ASA ASA
TB 8.1 24.7 64.5 68.8 36.1 36.1 86.7 66.7 70.9 34.3 94.5 50.5VV 86.5 9.6 54.4 59.1 17.0 15.8 78.1 37.4 61.5 12.0 125.6 124.8SS 113.2 6.5 64.0 60.9 18.9 23.1 101.4 33.7 7.6 8.9 107.0 91.6HJ 89.1 4.0 42.3 26.1 10.0 7.2 31.6 25.8 9.8 14.2 108.8 103.7RP 86.9 8.9 42.4 55.2 16.6 20.1 31.5 37.0 25.6 13.8 95.5 114.4NH 111.1 16.7 87.4 63.5 86.9 36.8 107.9 40.2 87.6 25.5 107.0 87.3YR 5.4 7.8 61.0 62.0 27.0 26.5 23.4 17.1 9.9 8.5 98.2 87.7CC 21.7 11.4 84.4 71.7 39.2 32.7 117.0 40.5 106.3 17.8 92.1 90.8CWL 84.5 8.9 36.4 52.1 15.1 23.6 16.0 21.0 29.5 12.8 96.2 81.8CWO 115.0 26.3 79.5 82.0 25.9 73.8 112.0 24.0 87.8 48.2 89.6 97.8MK 97.6 15.8 100.6 53.0 53.3 36.8 78.2 50.8 94.7 11.0 104.5 120.2ET 86.2 7.2 48.8 46.3 13.3 22.6 50.5 20.0 27.1 11.4 90.2 90.4Ol 71.5 8.0 35.0 42.5 6.6 15.7 18.2 13.6 5.4 9.0 26.0 35.9BS 90.1 13.8 98.7 58.2 38.3 37.3 107.2 23.5 88.6 18.7 99.9 76.0DD 82.8 20.7 94.5 83.1 87.4 50.0 106.3 62.5 94.2 31.7 89.2 84.9MM 105.0 10.0 57.0 61.2 20.1 22.7 85.6 36.6 25.3 11.5 92.1 101.2DS 91.1 13.4 84.9 62.4 19.4 255.5 89.9 46.7 58.2 13.0 88.2 98.0ER 87.2 4.4 88.2 35.4 18.7 11.3 97.1 14.3 100.4 6.3 91.8 89.6
Mean±SD
79.6±33.4
12.1±6.5
68.0±22.1
58.0±14.5
30.5±23.7
28.8±15.1
74.4±35.7
33.9±15.6
55.0±37.1
17.1±10.9
94.2±19.5
90.4±21.6
*p-Value 0.0001 0.1 171 0.7903 0.0001 0.0002 0.5756% Inhibition 84.2 14.7 5.6 54.4 68.9 4.0
* Values before and after aspirin were compared using analysis of variance for repeated measurements.
ASA = acetylsalicylic acid.
prolongation in bleeding time in this subject, the Sonoclot® graph showed good reproducibility. The num erical values for TI, TP, and R3 in all subjects studied are shown in table II. There was no significant change in any of these variables following aspirin ingestion.
No c o rre la t io n w as fo u n d am ong changes in bleeding time, platelet aggregation in response to arachidonic acid and collagen, and/or Sonoclot® parameters in healthy volunteers after aspirin ingestion.
Since the values of bleeding tim e after a sp ir in in v o lu n te e rs had re m a in e d w ithin normal range, in a second phase of this study were added five patients with known p late le t dysfunction, who w ere b e in g fo llow ed by hem oto log ists for coagulopathy. These patients were identified by their physicians because of a single coagulation abnormality, i.e., an abnormally prolonged bleeding time (14 to 22 minutes) in the presence of normal PT, PTT, fibrinogen and fibrinogen split products. Four out of these five patients
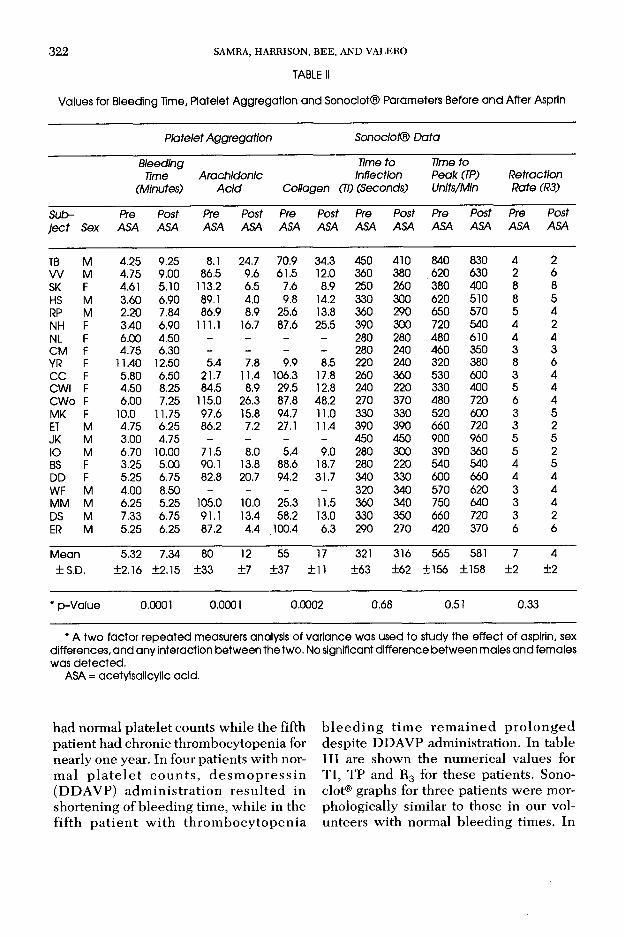
TABLE II322 SAMRA, HARRISON, BEE, A N D VALERO
Values for Bleeding Time, Platelet Aggregation and Sonoclot® Parameters Before and After Asprln
Platelet Aggregation Sonoclot® DataBleeding
Time(Minutes)
ArachidonicAcid Collagen i
Time to Inflection
(TI) (Seconds)Time to Peak (TP) Units/Min
Retraction Rate (R3)
Sub Pre Post Pre Post Pre Post Pre Post Pre Post Pre Postje c t Sex ASA ASA ASA ASA ASA ASA ASA ASA ASA ASA ASA ASA
TB M 4.25 9.25 8.1 24.7 70.9 34.3 450 410 840 830 4 2W M 4.75 9.00 86.5 9.6 61.5 12.0 360 380 620 630 2 6SK F 4.61 5.10 113.2 6.5 7.6 8.9 250 260 380 400 8 8HS M 3.60 6.90 89.1 4.0 9.8 14.2 330 300 620 510 8 5RP M 2.20 7.84 86.9 8.9 25.6 13.8 360 290 650 570 5 4NH F 3.40 6.90 111.1 16.7 87.6 25.5 390 300 720 540 4 2NL F 6.00 4.50 - - - - 280 280 480 610 4 4CM F 4.75 6.30 - - - - 280 240 460 350 3 3YR F 11.40 12.50 5.4 7.8 9.9 8.5 220 240 320 380 8 6CC F 5.80 6.50 21.7 11.4 106.3 17.8 260 360 530 600 3 4CWI F 4.50 8.25 84.5 8.9 29.5 12.8 240 220 330 400 5 4CWo F 6.00 7.25 115.0 26.3 87.8 48.2 270 370 480 720 6 4MK F 10.0 11.75 97.6 15.8 94.7 11.0 330 330 520 600 3 5ET M 4.75 6.25 86.2 7.2 27.1 11.4 390 390 660 720 3 2JK M 3.00 4.75 - - - - 450 450 900 960 5 5IO M 6.70 10.00 71.5 8.0 5.4 9.0 280 300 390 360 5 2BS F 3.25 5.00 90.1 13.8 88.6 18.7 280 220 540 540 4 5DD F 5.25 6.75 82.8 20.7 94.2 31.7 340 330 600 660 4 4WF M 4.00 8.50 - - - - 320 340 570 620 3 4MM M 6.25 5.25 105.0 10.0 25.3 11.5 360 340 750 640 3 4DS M 7.33 6.75 91.1 13.4 58.2 13.0 330 350 660 720 3 2ER M 5.25 6.25 87.2 4.4 100.4 6.3 290 270 420 370 6 6Mean 5.32 7.34 80 12 55 17 321 316 565 581 7 4±S.D. ±2.16 ±2.15 ±33 ±7 ±37 ±11 ±63 ±62 ±156 ±158 ±2 ±2
* p-Value 0.0001 0.0001 0.0002 0.68 0.51 0.33
* A two factor repeated measurers analysis of variance was used to study the effect of aspirin, sex differences, and any interaction between the two. No significant difference between males and females was detected.
ASA = acetylsalicylic acid.
had normal platelet counts while the fifth patient had chronic throm bocytopenia for nearly one year. In four patients with norm al p la te le t c o u n ts , d e s m o p re s s in (DDAVP) ad m in is tra tio n re su lte d in shortening of bleeding time, while in the fifth p a tie n t w ith th ro m b o cy to p en ia
b le e d in g tim e re m a in e d p ro lo n g e d despite DDAVP administration. In tableIII are shown the num erical values for TI, TP and R3 for these patients. Sonoclot® graphs for three patients were morphologically similar to those in our volunteers with normal bleeding times. In

STUDY O F ASPIRIN IN D U C E D CH ANG ES A N D SONOCLOT® COAGULATION 323
F i g u r e 2. Sonoclot® g rap h s b e fo re a n d a fte r a sp irin in one rep re sen ta tive sub ject w hose b le e d in g tim e in c re ased from 3.0 to 4.75 m inutes.
one patient with systemic lupus erythe- matosis, morphology of the graph was normal and num erical values for TI and R3 were w ithin the m ean ± 2 S.D. in our volunteers, while TP was prolonged. In the fourth patient with chronic thrombocytopenia m orphology was som ew hat altered because T I and TP w ere less clearly defined, (even w hen we repeated
this test four times), bu t the num erical values for all param eters w ere w ithin normal range.
Discussion
The primary goal of this investigation was to evaluate the performance of Sonoclot® in d e te c tin g p la te le t function
TABLE IIIValues for Bleeding Time and Sonoclot® Parameters in Patients with Platelet Function Disorders
Subject SexBleeding
Time (In Minutes)
Sonoclot® DATATime to
Injection (TI) (In Seconds)
Time to Peak (TP)(In Seconds)
Retraction Rate (R3) Units/Minute
JM F 21.00 400 1280 5.0STH F 13.75 390 625 5.0PS F 22.00 320 517 5.0ND F 14.50 360 660 3.3CS M 21.00 410 570 10.0
Mean 18.5 384.0 730.4 5.70± S.D. ±4.0 ±46.2 ±312.0 ±2.50
324 SAMRA, HARRISON, BEE, A N D VALERO
abnorm alities induced by ingestion of aspirin, and to compare its performance with an established in vitro laboratory test of platelet function (platelet aggregation) and an in vivo test of hemostasis (bleeding time).
The effect of aspirin on platelet aggregation was tested in response to ADP, (AA), collagen, Ristocetin and epinephrine in this investigation. The magnitude of inhibition of p late le t aggregation in response to different agents (table I) in this study is similar to that reported by Ellis e t a l10 in hum an aspirin studies. They noted 73.4; 78.3, and 61 percent inhibition in response to AA, collagen, and ep in ep h rin e , respectively . T here was minimal inhibition (four percent) of platelet aggregation in response to ADP. The explanation for these findings is that AD P-stim ulated p late le t aggregation is not cyclooxygenase dependent, thus it is not affected by aspirin, while AA and collag en in d u c e d p la te le t ag g re g a tio n involves thromboxane A2, and hence, is significantly affected by aspirin ingestion. Post-aspirin b leeding tim e is significantly prolonged in patients with von- W illebrand’s disease; in many patients, this may be the only initial coagulation abnormality.25 These patients have normal bleeding times prior to aspirin ingestion and only m ild b leeding diathesia, which can be easily overlooked. Ristocetin aggregation was studied to exclude vo lun teer subjects w ith unknow n von W illebrand’s disease.
The tem plate b leed ing tim e is currently the gold standard for assessment of in vivo platelet function.21 A num ber of variables including the venostasis, direction of incision, and type of device can influence the results. This test was performed using a horizontal incision and an automated device, a technique known to be the most sensitive one to measure the effect of aspirin ingestion on bleeding tim e.5,18 A m ean increase in b leeding
tim e a fte r in g e s tio n o f a s p ir in an d marked variation among subjects noted in this study is in keeping with previously published reports.3,518 It has been previously reported2,27 that aspirin prolongs b leeding tim e more in m en than women. Although a greater prolongation of bleeding tim e in males compared to females (50 percent vs. 25 percent) was also observed by us, this difference was not statistically significant. Lack of difference in b leeding tim e values betw een males and females is in agreem ent with other reports5,14 and can be explained by the technique of doing this test. In two investigations show ing significant sex re la ted d ifference, e ith e r a p u n c tu re wound2 or a vertical incision27 was used, while in this study and two other investigations,5,14 which failed to find a significant sex related difference in prolongatio n of b le e d in g tim e by a sp ir in , a horizontal incision was used. Although a significant mean prolongation (138 percent of control) of b leed ing tim e was observed after a sp irin ingestion , the absolute values rem ained w ithin normal range for our laboratory in 18 out of 22 volunteers. These data further confirm the observations of Mielke and co-work- ers17,19 that aspirin has only a mild effect on the b leeding tim e which is insufficient in normal persons to increase blood loss during surgery. However, in a small subset of patients (five to eight percent), b leed in g tim e after asp irin has been reported to prolong three to 10 times the control values and this group needs to be identified prior to surgery.
An attem pt has been made by us to evaluate the Sonoclot® device in this study as an alternative to tem plate b leeding time to identify this group of patients. Aspirin ingestion did not cause a significant change in any o f the Sonoclot® param eters. A lthough six com ponents (SonAct, R 1; TI, R2, TP and R3) were m easured, statistical analysis on only three

STUDY O F ASPIRIN IN D U C E D C H ANG ES A N D SONOCLOT® COAGULATION 325param eters, i.e., TI, TP and R3 was done to avoid m ultiple comparisons. It is our b e lie f that the choice of these three components of the Sonoclot® graph is valid because changes in SonAct, Rj and R2 will be reflected in changes in TI and TP, respectively. No correlation was found betw een increase in bleeding time and changes in Sonoclot® parameters. These results could be interpreted in two ways. One interpretation could be that Sonoclot® is not a good device to detect prolongation in b lee d in g tim e. A nother interpretation could be that although the volunteers showed a statistically significant increase in b leeding time, the value in 18 out of 22 subjects rem ained w ithin the normal range in our laboratory. In other words, if the present authors were not aware of the value of bleeding time prior to aspirin ingestion, as is the case in a clinical setting, these volunteers would have been reported to have a normal b leeding tim e after aspirin ingestion.
It is possible that if the bleeding time had prolonged to more than nine m inutes, Sonoclot® m ight have shown an abnormal graph. This question could be answ ered in one of two ways, (a) by increasing the dose of aspirin to produce prolongation of b leeding tim e in volunteers, or (b) by including patients known to have prolonged bleeding time secondary to abnormal platelet function. It was our choice to study a dose of aspirin comm only used as a “prophylaxis” against stroke and myocardial infarction. Previous studies have shown that prolongation of b leeding tim e after aspirin administration is highly variable and there is no linea r dose response re la tio n sh ip . This m akes se lec tio n of a dose of asp irin which will predictably produce bleeding tim e greater than 9 m inutes, impossible.
Therefore, five patients with known p late le t function disorders with bleeding tim es betw een 14 to 22 m inutes were studied. A platelet function abnormality
was th e on ly s ig n if ic a n t h e m o sta tic defect in these patients, and other in trinsic coagulation factors (PT, PTT, fibrinogen, and fibrinogen degradation product levels) were w ithin normal limits. Mean values for TI, TP and R3 for this group (table III) were similar to those observed in the volunteer group before and after aspirin ingestion. The clinical situation for which this device was being evalua ted , i.e., for d e tec tin g pa tien ts w ith abnormal bleeding tim e owing to aspirin ingestion in small doses prior to adm inistration of spinal/epidural anesthesia, is such that one cannot tolerate any false negative results. So, if normal looking Sonoclot® graphs have been seen in three out of five patients w ith m arked prolongation of bleeding time, then this device cannot be recom m ended as a rep lacem ent for tem plate bleeding tim e which is currently the “gold standard” for detecting defects in primary hemostasis. Four of our patients with prolonged bleeding tim es had normal platelet count, and the Sonoclot® graphs in those patients had a normal morphology. In one patien t with chronic throm bocytopenia and prolonged b leeding tim e (14 m inutes), the Sonoclot® graph was different. It is possible that Sonoclot® graph is more useful in detecting hemostatic abnorm alities associated with thrombocytopenia.
In th e ir original study, Saleem and co-workers23 had proposed, a viscoelastic m easurem ent of clot formation as a new test of platelet function using samples of PRP and PPP. Subsequent clinical studies 1,2°’23’24’26 using Sonoclot® too, have involved patients undergoing either cardiac surgery or liver transplants. Dilu- tional throm bocytopenia is a common occurrence in the postoperative period after these operations. Our findings of Sonoclot® parameters are in partial agreem ent with Stern and co-workers24 who observed no significant difference in the values of TP among patients taking non
326 SAMRA, HARRISON, BEE, A N D VALERO
steroidal antiinflam m atory drugs w hen com pared w ith controls. They d id not report other parameters (TI, R3) included in our study. Goldstein and co-workers12 in a study of pregnant patients had seen good correlation of b leeding tim e with TP of Sonoclot® graph in 15 out of 18 patients. They reported one patient with SLE who had a prolonged bleeding time and norm al Sonoclot® graph and two other patients with normal b leeding time and prolonged TP. Our findings in five patien ts w ith m arked pro longation of bleeding times secondary to an isolated coagulation defect, i.e., p latelet dysfunction, are similar to those of G oldstein.12
In conclusion, in this study, Sonoclot® coagulation analysis could not detect the effect of aspirin in norm al volunteers w hether or not they had m arked prolongation of bleeding time. Even in patients with prolonged bleeding tim e but normal p latelet counts, normal looking Sonoclot® graphs were observed. In order to determ ine the frequency of false negative results while using this instrum ent for id e n tify in g p a tie n ts w ith p ro lo n g ed bleeding time, an investigation involving a large num ber of pa tien ts w ho have abnorm al p late le t function bu t normal platelet count needs to be conducted.
A ckn o w led g m en ts
T hanks are ex ten d ed to Dr. F rank H. G ardner, C hief, D iv ision o f H em otology/O ncology, and his associates for th e ir h e lp in id en tify in g p a tien ts w ith p la te le t function d isorders in c lu d ed in th is study, and perform ance o f tem plate b lee d in g tim e in sp e c ia l h e m a to lo g y lab o ra to ry . T h e ir g u id a n c e in d e s ig n o f th is in v e s tig a tio n is a lso g ra te fu lly acknow ledged .
References
1. A r i l l o t t a , C., S t e r n , M. P., D ia k u n , T. A., ET AL.: C h a n g in g b lo o d p ro d u c t u tiliz a tio n pa tte rn s in cardiac surgery: T h e in flu en ce of coagulation m onito ring in th e o p era tin g room. P r e s e n te d a t th e 11 th A n n u a l m e e t in g o f C ard iovascu lar A nesthesio logists, Seattle , WA, April 16-19, 1989.
2. B a i n , B . and FORSTER, T.: A sex d ifference in th e b le e d in g tim e. T h rom b. H aem ostas. 43: 131-132, 1980.
3. B ic k , R. L., A d a m s , T., a n d S c h m a l h o r s t , W. R.: B leed ing tim es, p la te le t adhesion , and aspirin . A m . J. C lin . Pathol. 65 :69-72, 1976.
4. B o u s s e r , M. G., E c h w e g e , E ., H a g u e n a u , M ., ET AL: “A IC LA ” co n tro lled trial o f asp irin and d ipy ridam ole in th e secondary p rev en tio n o f a thero th rom botic cereb ra l ischem ia. Stroke 14:5-14 , 1983.
5. B u c h a n a n , G., H o l t k a m p , C. A.: A com parative study o f variab les affecting th e b lee d in g tim e using tw o d isp o sab le dev ices. Am. J. C lin . Pathol. 91 :45-51 , 1989.
6. C a i r n s , J. A., G e n t , M., S i n g e r , J., e t a l : A spirin , su lf in p y razo n e or b o th in u n s ta b le angina. N. E ngl. J. M ed. 323:1369—75, 1985.
7. C anad ian C ooperative S tudy G roup: A random ize d tr ia l o f a sp ir in a n d su lf in p y ra z o n e in th rea ten ed stroke. N. E ngl. J. M ed. 299:53—59, 1978.
8. C e r l e t t i , C ., C a r r i e r o , M. R., and G a e t a n o ,G . D.: P la te le t aggregation resp o n se to single or p a ire d agg reg a tin g stim u li a fte r low dose aspirin . N. E ngl. J. M ed. 314:316-317 , 1986.
9. C h a p i n , J. W., B e c k e r , G . L., H u r l b e s t , B . J., ET a l .: C om parison o f th rom boelastog raph and S onoclo t co ag u la tio n a n a ly ze r for a sse ss in g coagulation status d u rin g ortho top ic liver transplanta tion . P re se n ted at T h ird A nnual Sym posium on P erio p era tiv e C are in L iv er T ran sp lan tation , P ittsbu rgh , PA, S ep tem b er 9 -1 0 , 1988.
10. E l l i s , E. F ., W r i g h t , K. F ., Jo n a s , P. S., e t a l .: E ffec t o f oral a sp ir in d o se on p la te le t aggregation ang vascular p rostacyc lin syn thesis in hum ans and rabbits. J. C ardiovasc. Pharm acol. 2 :387-397 , 1980.
11. G a e t a n o , G . D ., C a r l e t t i , C ., D e j a n a , E ., and L a t i n i , R.: Pharm acology o f p la te le t in h ib itio n in hum ans: Im plications o f th e salicy- la te -asp irin in te rac tio n . C ircu la tio n 72:1185- 1193, 1985.
12. G o l d s t e i n , R., S i n a t r a , R., H i n e s , R., e t a l : An evaluation o f p regnancy associated coagulo p a th ies u tiliz in g th e S o n o c lo t co ag u latio n analyzer. P re se n ted a t th e A nnual M ee tin g of th e Society for O bste trical A nesthesia an d P erinatology C are, D enver, C O , 1989.
13. Ja k u b o w s k i , J. M., S t e m p f e r , M. J., V a i l l a n - COURT, R., ET AL: C u m u la tiv e a n tip la te le t effect o f low dose e n te ric coated asp irin . Br. J. H aem at. 60:635-642, 1985.
14. Ka l l m a n n , R ., N i e u w e n h u i s , H . K ., d e - G r OOT, P. G ., e t AL: E ffects o f low doses o f asp irin , 10 m g and 30 m g daily , on b leed in g tim e , th ro m b o x a n e p ro d u c tio n a n d 6 -ke to - P G F 2 a excretion in h ealth y subjects. Throm b. Res. 45 :355-361, 1987.
15. Ki n l o u g h -R a t h b o n e , R. L., P a c k h a m , M . A., and M u s t a r d , J. F.: P la te le t aggregation . In: M e a su re m e n ts o f P la te le t F u n c tio n , vol. 8. H asker, L. A. and Z im m erm an, T., eds. N ew York, C h urch ill L iv ingstone , 1983, pp . 64—87.
16. L e w i s , Jr ., H. D ., D a v i s , J. W., A r c h i b a l d ,D . G ., ET AL: P ro te c tiv e e ffec ts o f a sp ir in against acu te m yocardial infarc tion and death

STUDY O F ASPIRIN IN D U C E D CH ANG ES A N D SONOCLOT® COAGULATION 327in m en w ith u n stab le angina. R esults o f V eteran s A d m in is tra tio n C o o p e ra tiv e S tu d y . N. E ngl. J. M ed. 309:396-403, 1983.
17. M i e l k e , C. H ., Ka n e s h i r o , M . M ., M a h e r ,I . A ., ET AL: T h e s ta n d a r d iz e d n o r m a l iv y b le e d in g t im e a n d its p r o lo n g a t io n b y a sp ir in . B lo o d 34:204-215 , 1969.
18. M lELKE, C. H.: A spirin prolongation of th e tem p la te b le e d in g tim e: In flu en c e o f venostatis an d d irec tio n o f incision. B lood 60:1139-1142,1982.
19. M ie lk e , C. H.: In flu en ce o f asp irin on p la te le ts an d th e b lee d in g tim e. Am. J. M ed. 74:72—78,1983.
20. N e w l a n d , M. C ., K e n n e d y , E . M., C h a p i n , J. W., ET AL: B lood volum e rep lacem en t du ring ped ia tric o rtho top ic liver transp lan tation . P re se n ted a t T h ird Annual Sym posium on P erio p e ra tiv e C are in L iv er T ran sp lan ta tio n , P itts bu rgh , PA, S ep tem b er 9 -1 0 , 1988.
21. P la te le t F u n c tio n T esting : P ro ceed ings from th e w orkshop on p late le ts : T h e Significance of P la te le t F u n c tio n T e s t in th e E v alu a tio n of H em ostatic and T hrom botic T end en cies , h e ld in P h ilad e lp h ia , PA, O ctober 18-19, 1976. Day,H . J., H o lm sen , H ., an d Z u cker, M. B., eds. D H E W P u b lica tion No. (N IH ) 78-1087. W ashing ton , U.S. D ep t, o f H ealth , E du ca tio n and W elfare, P ub lic H ealth Service, N ational In stitu te o f H ealth .
22. P r e s t o n , F. E ., W h i p p s , S., Ja c k s o n , C . A., e t AL: In h ib it io n o f p ro s ta c y c lin a n d p la te le t th ro m b o x an e A2 a fte r lo w -d o se a sp ir in . N. Engl. J. M ed. 304:76-79 , 1981.
23. Sa l e e m , A., B l i f e l d , C., Sa l e h , S . A., e t a l : Viscoelastic m easu rem en t o f clo t form ation: A new te s t o f p la te le t function. Ann. C lin . Lab. Sci. 13:115-124, 1983.
24. S t e r n , M. P ., D e V o s - D o y l e , K. M ., a n d VlGUERA, M. G.: E valuation o f p o st card io p u lm onary bypass Sonoclot® signatu res in p a tien ts taking non-stero idal anti-inflam m atory agents. P re sen ted a t th e T en th A nnual M ee tin g o f th e Society o f C a rd io v ascu la r A n esth esio lo g ists , N ew O rleans, LA, April 10-13, 1988.
25. St u a r t , M . J., M i l l e r , M . L., D a v e y , R., e t a l : T h e post-asp irin b lee d in g tim e: A sc reen ing tes t for evaluating haem ostatic d isorders. Br. J. H aem at. 43 :649-659, 1979.
26. T u m a n , K. J., M c C a r t h y , R. J., Sp i e s s , B. D ., ET AL: C om parison o f v iscoelastic m easu res o f coagulation follow ing card iopulm onary bypass. P re sen ted a t th e 10th A nnual m ee tin g o f C ard io v ascu la r A n e s th e s io lo g is ts , A p ril 1 0 -1 3 , N ew O rleans, LA, 1988.
27. Yo u n g , V. P ., G i l e s , A. R., P a t e r , J., e t a l : Sex d ifferences in b leed in g tim e an d b lo o d loss in norm al subjects follow ing a sp irin ingestion . T hrom b. Res. 20:705-709, 1980.















![Intracranial Aneurysms and Antiplatelet Therapy€¦ · [16]. Given such controversies, there is a need for greater effort to establish a clear effect of aspirin on re-bleeding, since](https://img.pdfslide.us/doc/110x75/5f024b1e7e708231d4038c37/intracranial-aneurysms-and-antiplatelet-therapy-16-given-such-controversies.jpg)